
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med., 26 January 2024
Sec. Rheumatology
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1320076
This article is part of the Research TopicNew insights into the role of imaging in large vessel vasculitisView all 11 articles
 Edoardo Conticini1†
Edoardo Conticini1† Paolo Falsetti1†Suhel Gabriele Al Khayyat1†
Paolo Falsetti1†Suhel Gabriele Al Khayyat1† Silvia Grazzini1*†
Silvia Grazzini1*† Caterina Baldi1†Francesca Bellisai1Stefano Gentileschi1†Marco Bardelli1†Claudia Fabiani2Luca Cantarini1†Bhaskar Dasgupta3†Bruno Frediani1†
Caterina Baldi1†Francesca Bellisai1Stefano Gentileschi1†Marco Bardelli1†Claudia Fabiani2Luca Cantarini1†Bhaskar Dasgupta3†Bruno Frediani1†Objectives: Ultrasound has a paramount role in the diagnostic assessment of giant cell arteritis (GCA); Southend halo score (HS), halo count (HC), and OMERACT GCA Ultrasonography Score (OGUS) are the first quantitative scores proposed in this setting. The aim of this study was therefore to assess the diagnostic accuracy of these scores in a real-life scenario, as well as to evaluate their optimal cutoff, also with respect to disease extent, sex, and age.
Methods: We retrospectively collected clinical, serological, and US findings of all patients referred for the first time to our vasculitis clinic in the suspicion of GCA.
Results: A total of 79 patients were included, and a definite diagnosis of GCA was made in 43 patients. For OGUS, the ROC curve showed an optimal cut point of 0.81 (sensitivity 79.07% and specificity 97.22%). For HC and HS, the optimal cutoff values were > 1.5 (sensitivity 76.7% and specificity 97.2%) and > 14.5 (sensitivity 74.4% and specificity 97.2%), respectively. No relevant differences were assessed when patients were stratified according to disease extent, age, and sex. Compression sign (CS) was positive in 34 of 38 patients with cranial GCA and negative in all controls and LV-GCA.
Conclusion: All three scores display good sensitivity and excellent specificity, although the cutoff was slightly different than proposed. In particular, for OGUS, a threshold of 0.81 could be employed for diagnostic purposes, although it was developed solely for monitoring. Due to its high sensitivity and specificity, CS should be always assessed in all patients referred with a suspicion of cranial GCA.
• Southend halo score (HS) and halo count (HC) have a good diagnostic accuracy, which is not influenced by disease extent, age, and sex.
• Even though the OMERACT GCA Ultrasonography Score (OGUS) was developed for disease monitoring, our study suggests its potential diagnostic role.
• Compression sign (CS) has the highest sensitivity and specificity for cranial GCA: Temporal arteries US should always comprise a dynamic evaluation.
Giant cell arteritis (GCA) is a large-vessel vasculitis affecting the aorta and its major branches. Due to the high morbidity arising from irreversible, organ-threatening complications, an early diagnosis and prompt adequate treatment are mandatory. In this regard, in contradistinction to the temporal artery (TA) biopsy advocated in ACR 1990 criteria (1), imaging has a paramount role in the diagnosis and assessment of GCA. An ultrasound (US) of TA and axillary (AxA) arteries, due to its wide availability, rapidity, and lack of ionizing radiation, is most employed for both large vessels (LV) and cranial GCA.
Nevertheless, despite growing evidence supporting its routine use for diagnosis (2) and follow-up (3–6), US has several shortcomings in clinical practice: first the poor training of specialists facing the first symptoms of GCA, including rheumatologists; second, the paucity of studies that include also the LV-GCA phenotype in addition to the more common cranial one (7); third, the lack of validated quantitative scores, which limits its use for clinical trials (8) and multicenter studies.
The first quantitative score reports using the Southend Halo score (HS) (9) found an association with male sex, disease activity, ocular ischemia, and intimal hyperplasia on temporal artery biopsy. Thereafter, the Outcome Measures in Rheumatology (OMERACT) ultrasonography large-vessel vasculitis working group, after defining and testing elementary lesions in GCA (10, 11), has recently developed a novel, provisional score for disease monitoring (12). Both the HS and OMERACT GCA Ultrasonography Score (OGUS) displayed an excellent agreement and proved to be sensitive to changes during follow-up as well as to correlate with markers of inflammation and Birmingham Vasculitis Activity Score (BVAS) in one study (13).
Thus, we aimed to evaluate the quantitative halo scores (9, 12) in a real-life setting in order to assess their diagnostic accuracy and feasibility.
The primary endpoint of the study was a retrospective assessment of the specificity and sensitivity of OGUS, as well as to determine its optimal cutoff values, in a cohort of patients referred to our clinic with suspected GCA.
Secondary endpoints were to retrospectively assess the accuracy of the halo scores with respect to disease extent (LV and cranial) and to compare it with semiquantitative and quantitative scores already employed in our clinical practice.
We retrospectively collected clinical, serological, and US findings of all patients referred to Vasculitis Clinic, Rheumatology Unit, University Hospital of Siena, in the suspicion of GCA from January 2020 to January 2023.
Patients could be referred by other clinicians or through our fast-track pathway, in which patients suffering from sudden visual impairment and/or other symptoms of GCA and an increase in erythrocyte sedimentation rate (ESR) and/or C-reactive protein (CRP) were immediately referred to our clinic.
Inclusion criteria were the availability of the following: a minimum core set of blood examinations (14), including hemoglobin (Hb), ESR, and CRP; US findings, including intima–media thickness (IMT), compressibility, and the presence of “halo sign” in AxA and common temporal, parietal, and frontal branches of both TA; a definite clinical diagnosis, which was performed by a single rheumatologist experienced in vasculitis and expressed as follows: cranial GCA, LV-GCA, cranial and LV-GCA, and no GCA.
Exclusion criteria were the unavailability of the abovementioned findings and a previous diagnosis of GCA in remission at the time of the assessment, as well as concomitant or previous treatment with anti-IL6 agents.
US examination was carried out by two rheumatologists experienced in US employing an Esaote MyLab X8, equipped with two linear (4–15 and 18–22 MHz) probes, and an Esaote MyLab Twice, equipped with two linear (4–13 and 6–18 MHz) probes. The vessels assessed were AxA and common temporal, parietal, and frontal branches of TA, the latter being evaluated only with high-frequency probes. Color Doppler frequency was set at 9–12.3 MHz and pulse repetition frequency at 2–3 KHz, while gain was adjusted at just below the threshold of artifacts. The burden of vascular inflammation was measured through IMT and scored using halo count (HC), HS (9), and OGUS (12). IMT measurements were manually performed evaluating the thickness from the luminal–intimal interface to the medial–adventitial one, in a longitudinal scan during systole and reported in millimeters (15, 16). The occurrence of low compressibility of any branch of TA was also recorded.
A binomial regression analysis was performed to obtain diagnostic cutoffs of different components of OGUS (total, LV, cranial, etc.). Various ROC curves were calculated comparing the halo score components with the diagnosis of GCA as the gold standard.
This study was conducted in accordance with the Declaration of Helsinki and its late amendments and approved by the local ethics committee (Rhelabus, protocol number 22271).
A total of 79 subjects were evaluated with suspicion of GCA, and a clinical diagnosis was made in 43 of them (mean age 76.42 years; 24 women): 29 patients suffered from cranial GCA, 9 presented with involvement of both cranial and extracranial arteries, while 5 had only LV-GCA. Clinical and serological features of the patients, including PET findings, are reported in Table 1.
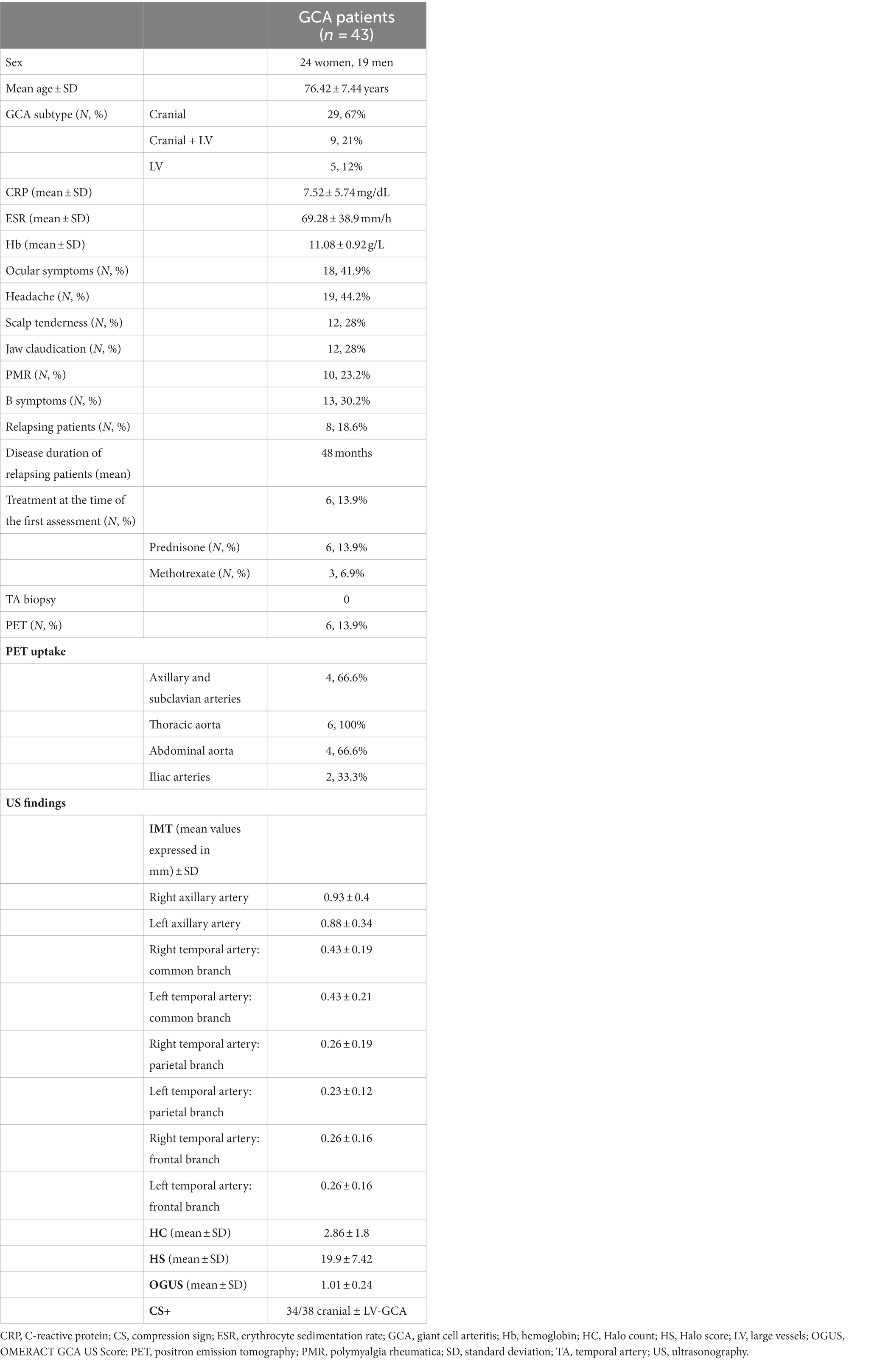
Table 1. Clinical and serological features of GCA patients.
No patient underwent TA biopsy, while PET was requested in 6, in which an involvement of large vessels was suspected: In all of them, imaging displayed a pathological uptake (Meller scale 3) in the territory of the aorta and/or iliac vessels.
The area under the ROC curve (AUROC) for OGUS was 0.980 (95% confidence interval: 0.9534, 1). The ROC curve showed an optimal cut point of 0.81, with a sensitivity of 79.07%, a specificity of 97.22%, and a likelihood ratio (LR) of 28.47. Similar cutoffs were found also when patients were stratified according to disease extent (Table 2), while slightly lower values, although with 100% sensitivity, were reported when our cohort was subdivided for age and sex (Table 3).
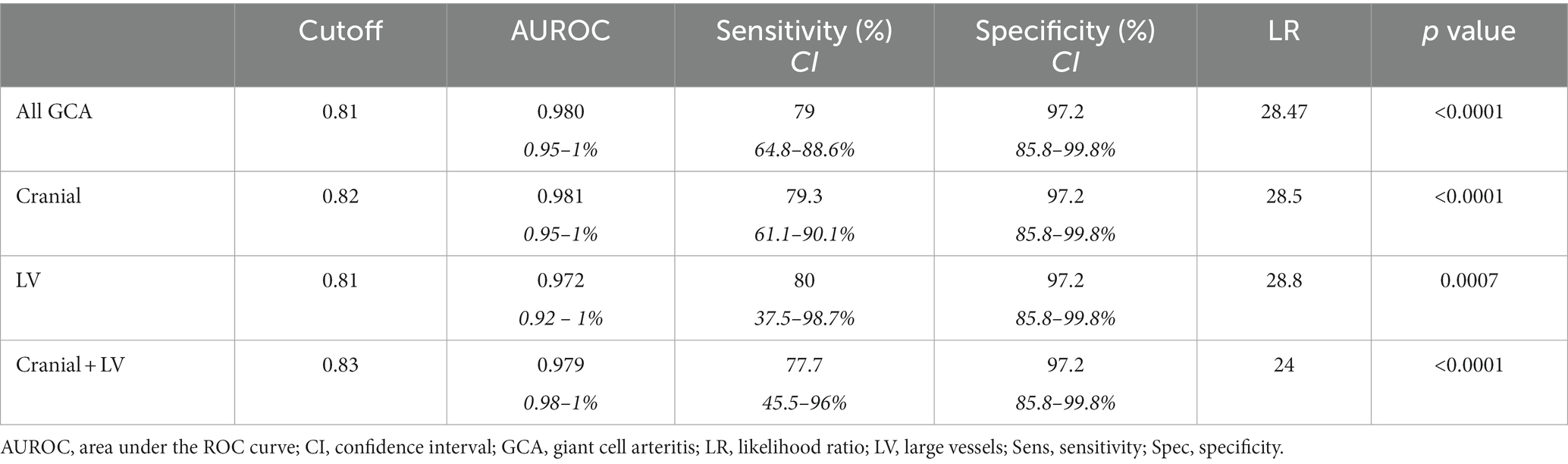
Table 2. OGUS, stratification for GCA type.
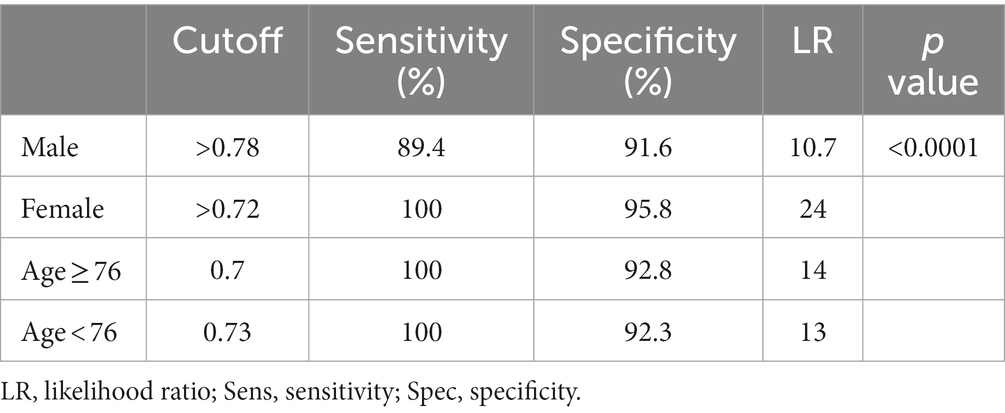
Table 3. OGUS, stratification for sex and age.
For HC, AUROC was 0.979, with a CI of 0.944 to 1 and a p < 0.0001. The optimal cutoff value was set at >1.5 with a sensitivity of 76.7% (CI: 62.2–86.8%), a specificity of 97.2% (CI: 85.8–99.8%), and an LR of 27.63. A lower, although high, LR (17) was assessed with a cutoff >0.5 (sensitivity 100%, specificity 94.44%). The same cutoff (>1.5) was found to be the optimal one also for cranial, LV, and LV + cranial GCA, but the latter had the lowest sensitivity (66.6%), while the highest (100%) was found for cranial (Table 4). As for OGUS, these findings were not influenced by sex or age (Table 5). Finally, a positive, statistically significant correlation was found between HC and OGUS (Pearson’s r: 0.841, p < 0.001).
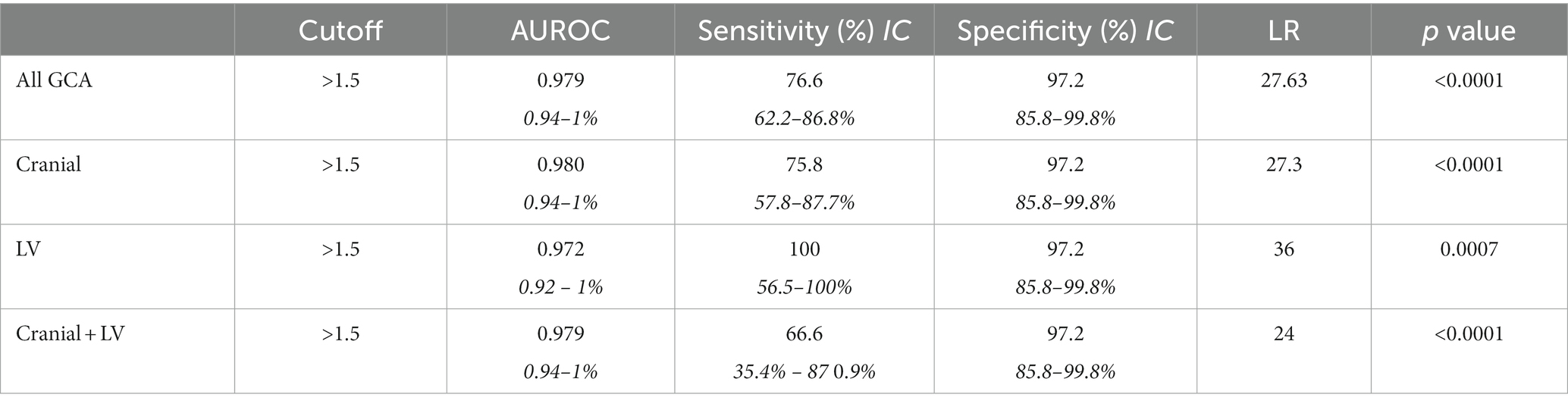
Table 4. Halo count, stratification for GCA type.
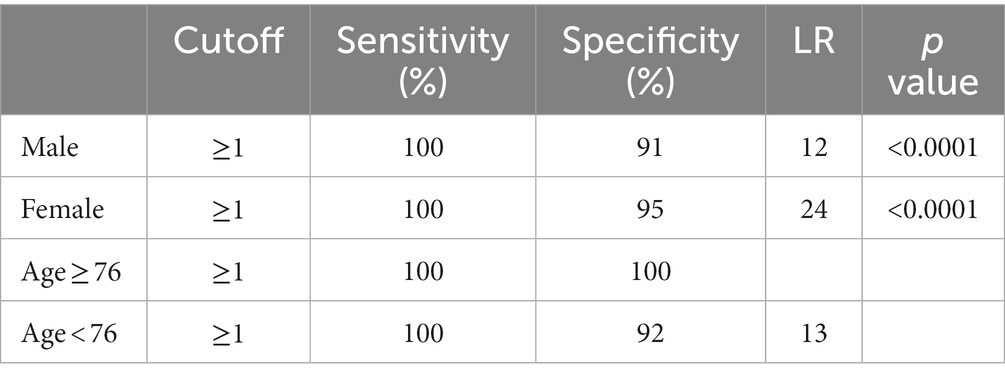
Table 5. Halo count, stratification for sex and age.
For HS, a cutoff of >14.5 (AUROC: 0.95, sensitivity: 74.4%, specificity: 97.2, and LR: 26.7) was found for all GCA patients, but a lower sensitivity (65.5%) was found for cranial ones (Table 6). In contrast to HC and OGUS, a different optimal cutoff was evidenced for men, in whom an HS >8.5 was associated with 100% sensitivity and 83.3% specificity (Table 7).
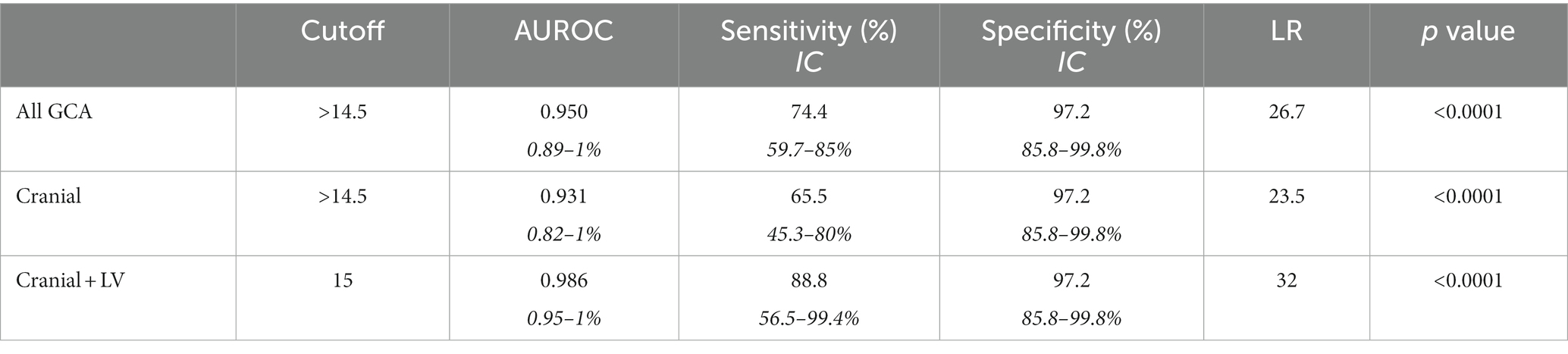
Table 6. Halo score, stratification for GCA type.
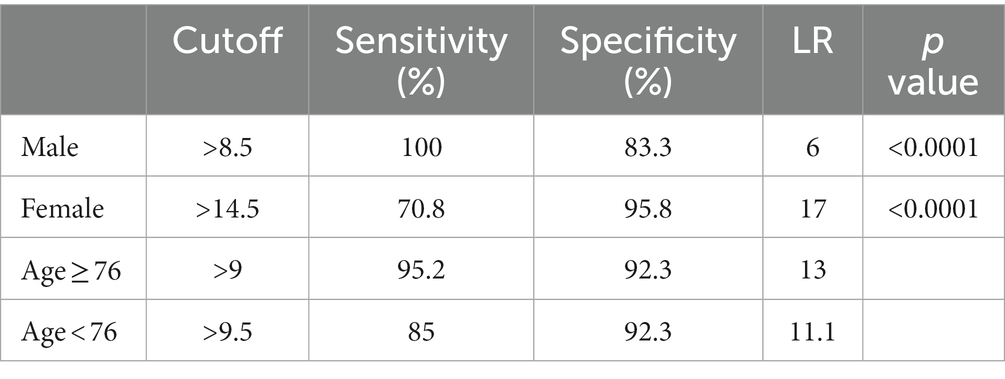
Table 7. Halo score, stratification for sex and age.
Compression signs were positive in 34 of 38 patients with cranial and cranial + LV-GCA, while all controls and LV-GCA displayed negative CS (89% sensitivity and 100% specificity).
The retrospective application of three different US scores to patients with suspected GCA allows for the first time a direct comparison of these methodologies. While some US scores and cutoff values have been proposed, their application is de facto restricted to the cohorts in which they were originally applied (9) and few other ones (6, 18). At the same time, OGUS, specifically designed for clinical trials and disease monitoring, is a consensus-based algorithm and has not been applied yet in clinical practice, except for assessing its sensitivity to change after treatment (13, 17), which appeared comparable to HS and HC, although only for TA.
In our sample population, comprising 79 subjects referred to in the suspicion of GCA, we evidenced positive US findings in the majority of patients who eventually were diagnosed with vasculitis, thus confirming the crucial role of US in its diagnostic work-up. Such findings were not influenced by age nor differed between first diagnosis and relapse; the only relevant difference was according to sex and disease extent, as the only GCA patient in whom US was negative had an exclusive involvement of the aorta. This is not surprising, because men have greater IMT than women (9), and at the same time, some vascular territories (i.e., aorta and iliac arteries) cannot adequately be detected by US and require different imaging procedures, such as PET, MRI, and CT. On the other hand, no patient with a final diagnosis of cranial GCA had a fully negative US.
When separately analyzing the three scores taken for examination, an overall good diagnostic accuracy was assessed, although with cutoffs slightly different than proposed.
In particular, OGUS had the best diagnostic performance at a threshold of 0.81, instead of 1.01: The latter resulted in an excellent specificity (100%) but a poor sensitivity (39.53%), while our cutoff displayed a slightly lower specificity (94.44%) but a significantly higher sensitivity (79.07%) with an LR of 28.47.
This finding was predictable, as OGUS was designed for clinical trials and research and not for being employed in a clinical setting nor for diagnostic purposes: In this context, a lower specificity, thus potentially leading to overtreatment of a patient with suspected vasculitis, should be preferred to a 100% specificity with a poor sensitivity, which in real life may lead to a hazardous and harmful undertreatment of a GCA.
On the other hand, our data confirm the excellent specificity of OGUS, applied for the first time in a real-life cohort, and strongly support its use in drug research and trials, in which the need to exclude mimickers is prevalent. Moreover, even though OGUS was developed only for disease monitoring, our study seems to suggest its potential diagnostic role.
For HC, our findings did not substantially differ from the cutoffs previously proposed: an HC ≥2 provided a 76.74% sensitivity and 97.22% specificity, with an LR of 27.63, which are values de facto comparable to the ones reported by Molina-Collada et al. (18) for an HC > 1 (sensitivity 80%; specificity 95%) and by van der Geest et al. (9) for an HC ≥ 2 in case of TAB positivity (sensitivity 85% and specificity 70%). On the other hand, despite a similar sensitivity (78%), van der Geest et al. (9) reported a much lower specificity (55%), for an optimal cutoff of 1. Curiously, a specificity comparable to ours (95%) was reported only for a cutoff of 6, 3-fold higher than the optimal one calculated in our cohort.
Such discrepancies are not easy to explain but are potentially due to the occurrence of a high HC in two non-GCA patients from the Southend cohort, which differed from ours in terms of F:M ratio (2.86 vs. 1.26).
On the other hand, it is noteworthy that all three cohorts evidenced a similar sensitivity, despite the differences existing among the three populations: the one by van der Geest et al. (9) and ours double the Spanish one (18) and include predominantly GCA patients, while in the latter, the controls are two thirds of the total. Moreover, and more importantly, we included cranial, LV, and cranial plus LV-GCA; the Southend cohort had only subjects with cranial vasculitis (headache was complained in up to 96% of subjects) and focused on the ischemic hazard, while, conversely, only 5 patients from the study by Molina-Collada et al. (18) fulfilled 1990 ACR criteria. Finally, at the time of the US assessment, four patients were relapsing, while both previous studies included only subjects referred for the first time.
That has a paramount importance in clinical terms, which is the ground of this study: Indeed, despite the application of this score in cohorts composed of different patients, comparable only for sex and age, HC presents the same good sensitivity, also for low or very low cutoffs. This confirms the potential application of HC in daily clinical practice, in which the prevention of ischemic complications prevails over the need to minimize the immunosuppressive treatment. In summary, it is not necessary to reach an HC ≥ 6, which can be assessed only in a minority of patients, to reasonably start glucocorticoids in a patient with suspected GCA.
More relevant discrepancies were conversely evidenced for HS: Lower values resulted in very poor specificity, particularly when compared with the cohort by Molina-Collada et al. (18), who reported a sensitivity and specificity of 86.7 and 95.3%, respectively, for HS ≥ 2.
Conversely, our results found an optimal cutoff of 15, displaying an excellent specificity (97.22%) and a good sensitivity (74.22%), far higher than the one (21%) reported by van der Geest et al. (9) for an HC ≥ 10.
Such a difference is not easy to explain but can be presumably determined by the inclusion of relapsing patients in our cohort, therefore presenting a higher IMT of AxA, and by the higher numbers of LV-GCA. A lower HS can be considered prudentially.
However, regardless of the difference existing for the optimal cutoff, which may also be due to the heterogeneity of the patients included in the studies, both HC and HS, as well as OGUS, proved to be reliable US scores, with comparable sensitivity and specificity, suggesting that they can be variously and alternatively employed for the diagnosis of GCA and its relapses (6).
Nevertheless, some difference was assessed when our patients were distinguished according to sex: for OGUS, men displayed poorer specificity and sensitivity, even with an optimal cutoff higher than women.
Conversely, statistical analysis evidenced a lower cutoff value for HS in men, which nevertheless led to a poorer LR and a statistically significant lower specificity.
Those findings presumably mean that in men with suspected GCA, OGUS and HS are by far less specific (and OGUS less sensitive, too) than in women, presumably due to a physiological increase of IMT in men.
On the opposite, no difference was assessed for HC, whose cutoff remained the same, with identical specificity, sensitivity, and LR, in men and women: Regardless of sex and age, an HC ≥1 is strongly associated with a diagnosis of GCA.
When patients were stratified for age, no difference was evidenced for any of the scores: This, at least for HS, is in contradiction with previous findings, displaying a higher IMT in older patients, but can be explained by the reduced age range of our cohort, as well as by the high diagnostic accuracy of US, regardless of age.
When patients were stratified according to disease extent, no relevant differences were assessed for optimal cutoff, which remained the same for HC and HS. At the same time, specificity did not vary for any of the three scores, ranging from 94 to 97%; conversely, at our cutoffs, sensitivity appeared lower for HC and, particularly, HS (65%) in patients affected by cranial GCA.
In this specific subset of patients, the application of compressibility sign resulted, in our cohort, in higher sensitivity (89%) and a 100% specificity. Such findings are substantially in line with previous studies (19–21), which nevertheless did not distinguish between cranial and LV-GCA. Our findings remark that a dynamic US evaluation, comprising compression sign, is mandatory for achieving a higher sensitivity: Reduced compressibility of any segment of TA markedly increases the diagnostic value of US and should be routinely employed in a patient with suspected GCA. Further scores should therefore include compression sign and add it to the assessment of IMT and halo, thus resulting in a semiquantitative score comprehensive in all these three aspects.
Our study has some limitations: First, the relatively low numbers do not allow any definite conclusions. Second, the number of “pure” LV-GCA, is low in comparison with cranial and cranial and LV combination, thus potentially leading to an incorrect assessment of specificity and sensitivity in this subset of patients. Third, we did not evaluate subclavian (22, 23) nor vertebral arteries, which in our clinical practice are assessed only in patients with suspected Takayasu arteritis. Fourth, we employed two different US machines, although from the same factory and with comparable features. Fifth, we did not assess the echo-texture of the vessels: We suspect that in the case of subjects referred for disease relapse or with long-term disease, a chronic thickening of IMT can be misleadingly interpreted as inflammatory, instead of a fibrotic, reparatory process; hence, the inclusion of relapsing patients may be a confounder. Nevertheless, in the context of a real-life study, we could not exclude such an important subtype of patients referred to our centers.
In conclusion, all proposed scores appear feasible and reliable not only for studies or clinical trials but also in clinical practice. The high specificity assessed in all of them confirms the excellent diagnostic value of US in suspected GCA, in a clinical setting like ours which does not employ TA biopsy nor routinely requests radiological imaging procedures, such as MRI or PET, as first-line test for GCA. Despite the lack of direct comparison among OGUS, HS, and HC, the latter could be potentially preferred, as it is not influenced by age or sex.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Comitato Etico Area Vasta Sudest Toscana. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
EC: Conceptualization, Data curation, Methodology, Supervision, Writing – original draft. PF: Conceptualization, Data curation, Methodology, Supervision, Writing – original draft. SA: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft. SiG: Conceptualization, Data curation, Investigation, Writing – review & editing. CB: Investigation, Supervision, Writing – review & editing. FB: Investigation, Validation, Writing – review & editing. StG: Investigation, Supervision, Writing – review & editing. MB: Investigation, Supervision, Writing – review & editing. CF: Supervision, Writing – review & editing. LC: Supervision, Validation, Writing – review & editing. BD: Supervision, Validation, Writing – original draft. BF: Supervision, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The authors declare that this study received funding from AbbVie (protocol number 0068880). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hunder, GG, Bloch, DA, Michel, BA, Stevens, MB, Arend, WP, Calabrese, LH, et al. The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum. (1990) 33:1122–8. doi: 10.1002/art.1780330810
2. Dejaco, C, Ramiro, S, Bond, M, Bosch, P, Ponte, C, Mackie, SL, et al. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice: 2023 update. Ann Rheum Dis. (2023) 7:ard-2023-224543. doi: 10.1136/ard-2023-224543
3. Conticini, E, Falsetti, P, Baldi, C, Bardelli, M, Cantarini, L, and Frediani, B. Superb microvascular imaging in giant cell arteritis. Clin Exp Rheumatol. (2022) 40:860–1. doi: 10.55563/clinexprheumatol/ygcvaz
4. Aschwanden, M, Schegk, E, Imfeld, S, Staub, D, Rottenburger, C, Berger, CT, et al. Concise report vessel wall plasticity in large vessel giant cell arteritis: an ultrasound follow-up study. Rheumatology (Oxford). (2019) 58:792–7. doi: 10.1093/rheumatology/key383
5. Conticini, E, Sota, J, Falsetti, P, Baldi, C, Bardelli, M, Bellisai, F, et al. The role of multimodality imaging in monitoring disease activity and therapeutic response to tocilizumab in Giant cell arteritis. Mediat Inflamm. (2020) 2020:1–9. doi: 10.1155/2020/3203241
6. Conticini, E, Falsetti, P, Baldi, C, Fabiani, C, Cantarini, L, and Frediani, B. Routine color doppler ultrasonography for the early diagnosis of cranial giant cell arteritis relapses. Intern Emerg Med. (2022) 17:2431–5. doi: 10.1007/s11739-022-03110-w
7. Sebastian, A, Coath, F, Innes, S, Jackson, J, Van Der Geest, KSM, and Dasgupta, B. Role of the halo sign in the assessment of giant cell arteritis: a systematic review and meta-analysis. Rheumatol Adv Pract. (2021) 5:rkab059. doi: 10.1093/rap/rkab059
8. Stone, JH, Tuckwell, K, Dimonaco, S, Klearman, M, Aringer, M, Blockmans, D, et al. Trial of tocilizumab in Giant-cell arteritis. N Engl J Med. (2017) 377:317–28. doi: 10.1056/NEJMoa1613849
9. Van Der Geest, KSM, Borg, F, Kayani, A, Paap, D, Gondo, P, Schmidt, W, et al. Novel ultrasonographic halo score for giant cell arteritis: assessment of diagnostic accuracy and association with ocular ischaemia. Ann Rheum Dis. (2020) 79:393–9. doi: 10.1136/annrheumdis-2019-216343
10. Chrysidis, S, Duftner, C, Dejaco, C, Schäfer, VS, Ramiro, S, Carrara, G, et al. Definitions and reliability assessment of elementary ultrasound lesions in giant cell arteritis: a study from the OMERACT large vessel Vasculitis ultrasound working group. RMD Open. (2018) 4:e000598. doi: 10.1136/rmdopen-2017-000598
11. Schäfer, VS, Chrysidis, S, Schmidt, WA, Duftner, C, Iagnocco, A, Bruyn, GA, et al. OMERACT definition and reliability assessment of chronic ultrasound lesions of the axillary artery in giant cell arteritis. Semin Arthritis Rheum. (2021) 51:951–6. doi: 10.1016/j.semarthrit.2021.04.014
12. Dejaco, C, Ponte, C, Monti, S, Rozza, D, Scirè, CA, Terslev, L, et al. The provisional OMERACT ultrasonography score for giant cell arteritis. Ann Rheum Dis. (2023) 82:556–64. doi: 10.1136/ard-2022-223367
13. Nielsen, BD, Therkildsen, P, Keller, KK, Gormsen, LC, Hansen, IT, and Hauge, EM. Ultrasonography in the assessment of disease activity in cranial and large-vessel giant cell arteritis: a prospective follow-up study. Rheumatology (Oxford). (2023) 62:3084–94. doi: 10.1093/rheumatology/kead028
14. Hellmich, B, Agueda, A, Monti, S, Buttgereit, F, De Boysson, H, Brouwer, E, et al. 2018 update of the EULAR recommendations for the management of large vessel vasculitis. Ann Rheum Dis. (2020) 79:19–130. doi: 10.1136/annrheumdis-2019-215672
15. Schäfer, VS, Juche, A, Ramiro, S, Krause, A, and Schmidt, WA. Ultrasound cut-off values for intima-media thickness of temporal, facial and axillary arteries in giant cell arteritis. Rheumatology (Oxford). (2017) 56:1479–83. doi: 10.1093/rheumatology/kex143
16. Ponte, C, Monti, S, Scirè, CA, Delvino, P, Khmelinskii, N, Milanesi, A, et al. Ultrasound halo sign as a potential monitoring tool for patients with giant cell arteritis: a prospective analysis. Ann Rheum Dis. (2021) 80:1475–82. doi: 10.1136/annrheumdis-2021-220306
17. Grazzini, S, Conticini, E, Falsetti, P, D’alessandro, M, Sota, J, Terribili, R, et al. Tocilizumab vs methotrexate in a cohort of patients affected by active GCA: a comparative clinical and ultrasonographic study. Biologics. (2023) 17:151–60. doi: 10.2147/BTT.S431818
18. Molina-Collada, J, Martínez-Barrio, J, Serrano-Benavente, B, Castrejón, I, Motta, LRC, Folguera, LT, et al. Diagnostic value of ultrasound halo count and halo score in giant cell arteritis: a retrospective study from routine care. Ann Rheum Dis. (2020) 81:e175. doi: 10.1136/annrheumdis-2020-218631
19. Aranda-Valera, IC, García Carazo, S, Monjo Henry, I, and De Miguel, ME. Diagnostic validity of Doppler ultrasound in giant cell arteritis. Clin Exp Rheumatol. (2017) 35:123–7.
20. Aschwanden, M, Daikeler, T, Kesten, F, Baldi, T, Benz, D, Tyndall, A, et al. Temporal artery compression sign--a novel ultrasound finding for the diagnosis of giant cell arteritis. Ultraschall Med. (2013) 34:47–50. doi: 10.1055/s-0032-1312821
21. Nakajima, E, Moon, FH, Junior, NC, Macedo, CR, de Souza, AWS, and Iared, W. Accuracy of Doppler ultrasound in the diagnosis of giant cell arteritis: a systematic review and meta-analysis. Adv Rheumatol. (2023) 63:5. doi: 10.1186/s42358-023-00286-3
22. Molina-Collada, J, Martínez-Barrio, J, Serrano-Benavente, B, Castrejón, I, Nieto-González, JC, Caballero Motta, LR, et al. Subclavian artery involvement in patients with giant cell arteritis: do we need a modified halo score? Clin Rheumatol. (2021) 40:2821–7. doi: 10.1007/s10067-020-05577-4
Keywords: ultrasonography, vasculitis, giant cell arteritis, Horton arteritis, diagnosis
Citation: Conticini E, Falsetti P, Al Khayyat SG, Grazzini S, Baldi C, Bellisai F, Gentileschi S, Bardelli M, Fabiani C, Cantarini L, Dasgupta B and Frediani B (2024) Diagnostic accuracy of OGUS, Southend halo score and halo count in giant cell arteritis. Front. Med. 11:1320076. doi: 10.3389/fmed.2024.1320076
Edited by:
Wolfgang Schmidt, Immanuel Hospital Berlin, GermanyReviewed by:
Juan Molina-Collada, Gregorio Marañón Hospital, SpainCopyright © 2024 Conticini, Falsetti, Al Khayyat, Grazzini, Baldi, Bellisai, Gentileschi, Bardelli, Fabiani, Cantarini, Dasgupta and Frediani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Silvia Grazzini, Z3JhenppbmkucmV1bWF0b2xvZ2lhQGdtYWlsLmNvbQ==
†ORCID: Edoardo Conticini orcid.org/0000-0002-3974-6606
Paolo Falsetti orcid.org/0000-0003-2667-4866
Suhel Gabriele Al Khayyat orcid.org/0000-0003-0035-6632
Silvia Grazzini orcid.org/0000-0001-6541-2469
Caterina Baldi orcid.org/0000-0002-3070-5568
Stefano Gentileschi orcid.org/0000-0002-3070-5568
Claudia Fabiani orcid.org/0000-0003-4515-7741
Luca Cantarini orcid.org/0000-0002-7352-1275
Bhaskar Dasgupta orcid.org/0000-0002-7352-1275
Bruno Frediani orcid.org/0000-0002-9375-5984
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.