 Cheng-Wei Lin1†
Cheng-Wei Lin1† I-Chan Lin
I-Chan Lin
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Med. , 28 February 2024
Sec. Ophthalmology
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1305579
This article is part of the Research Topic Dry Eye Disease Syndrome - Volume II View all 8 articles
Dry eye disease (DED) is a common multifactorial disease affecting a substantial proportion of the population worldwide. Objective tests and subjective symptoms evaluation are necessary to assess DED. Although various treatments have been introduced, accurately evaluating the efficacy of those treatments is difficult because of the disparity between diagnostic tests and patient-reported symptoms. We reviewed the questionnaires used to evaluate DED and the improvements of quality of life with various treatments. In addition, we highlighted the importance of patient-reported outcomes (PRO) assessments for evaluating the effect of DED treatments. Given that the assessment of DED treatment effectiveness substantially relies on individual ocular experiences, acquiring qualitative PRO data is essential for comprehensive evaluation and optimal treatment management. Clinicians should not only focus on improving objective symptoms but also prioritize the well-being of patients in clinical management.
Dry eye disease (DED) is a common ocular surface disease that affects a substantial proportion of the population worldwide. The prevalence of DED varies across different regions, ranging from 4.6% in North America to 47.9% in Africa (1). In Asian countries, approximately 20.1% of individuals develop DED (2). Moreover, in some industrialized Asian countries, such as Taiwan (3), Korea (4), and Japan (5), over a quarter of the population is affected.
DED is a multifactorial disease characterized by an imbalance between insufficient aqueous production (6) and excessive tear evaporation (7). Decreased tear production by the lacrimal gland results in less eye surface lubrication, and decreased oil secretion by the meibomian gland leads to excessive tear evaporation (8). The decreased wettability type of DED is characterized by a short tear film break-up time (TBUT), normal tear production, and minimal or no staining. This type results from the deficiency or abnormality of membrane-associated mucin, causing impaired corneal surface wettability (9). The most common risk factors with the strongest contribution for DED include female sex, contact lens usage, prolonged computer use, thyroid abnormalities, hypertension, antidepressant use, and antihistamine use (2). Other risk factors include Asian ethnicity (10), hormonal dysfunction and replacement therapy (11), Sjögren’s syndrome (12, 13), lifestyle factors (14), aging (2, 15, 16), medication usage, and cataract surgery (17, 18). These factors contribute to tear film instability, hyperosmolarity, ocular surface inflammation, and subsequent ocular discomfort (19).
Previously, DED was mainly attributed to aqueous insufficiency and ocular surface inflammation. Recent research has indicated meibomian gland dysfunction (MGD) as the leading cause of DED, particularly evaporative DED, and aqueous-deficient dry eye may be caused by MGD (5, 7). Thus, new diagnostic assessments and therapeutic interventions have been developed to address MGD (5, 20, 21) and restore the homeostasis of the tear film.
Objective tests and subjective symptom examination are mandatory for the accurate diagnosis of DED. However, disparities between diagnostic tests and patient-reported symptoms have been reported because of varied etiologies and clinical presentations (22–24). By evaluating patients’ symptoms and quality of life (QoL), the effect of the disease on individuals can be determined. Currently, no single test is available that can precisely predict and evaluate an individual’s response to treatment. Therefore, a standardized classification system that combines objective measurements with subjective symptom assessment and functional lifestyle evaluation through the use of well-designed questionnaires has been recommended to guide treatment strategies (19, 24, 25).
Various questionnaires have been developed to examine patient-reported outcomes (PROs) and the subjective symptoms of DED. Herein, we review the efficacy of conventional and advanced therapies as well as procedures (punctual occlusion, thermal pulsation, and intense pulsed light) in alleviating clinical signs and patient-reported symptoms. In addition, we evaluated questionnaires used to examine subjective ocular symptoms and QoL.
In this review, we evaluated the literature on the effect of current DED treatments on subjective outcomes. Given that subjective symptoms do not consistently correlate with objective clinical advancements, we focused on investigating the effects of treatments on the basis of patients’ self-reported improvements, encompassing self-reported symptoms, and satisfaction levels and by using validated questionnaires. By examining patients’ subjective responses to various treatment modalities, we intended to provide practitioners with valuable references for making informed treatment decisions. In our data search for clinical-trial-based articles, we initially employed specific commercial products or ingredients as primary search terms. Subsequently, we complemented our search by including the terms “dry eye” and “subjective” to refine and identify targeted search results. We comprehensively searched reputable databases, such as PubMed, Medline, and Web of Science, for relevant published studies related to DED treatments and their subjective impact. All articles meeting our search criteria that were published between 2000 and November 2022 (n = 9,050) were meticulously analyzed to identify clinical-trial-based publications focusing on assessment of QoL and subjective outcomes in human (in vivo) studies. With careful consideration, relevant articles investigating DED treatments and subjective assessments were selected, and their full contents were thoroughly evaluated (n = 255). The subsequent sections elucidate specific treatments for DED, including a detailed evaluation of their effects on QoL and patient satisfaction. We included not only original research papers but also other types of papers, such as trials and reviews, examining treatments for DED and questionnaires used to evaluate the QoL of patients with DED. We review studies on questionnaires and assessment tools for DED, and discuss the treatment options for DED. In addition, we discuss the advantages and disadvantages of possible treatment options for DED through comparative analysis.
PROs are highly valuable references because they directly capture the patient’s perspective without any interpretation from clinicians or third parties (26). Quantitative measurements alone may not always provide a definitive diagnosis of DED (27). Therefore, well-designed PRO instruments can provide complementary information and a more comprehensive understanding of patients’ condition (28). In addition to investigating the effect of DED or the effectiveness of its treatment, evaluating treatment satisfaction on the basis of direct patient feedback is essential. This evaluation can determine the effectiveness of treatment in alleviating symptoms as well as its convenience and accessibility.
Our review revealed various questionnaires and assessment tools that have been employed to differentiate patients with DED from those with normal ocular health and to capture subjective treatment outcomes. We categorized these questionnaires into two groups on the basis of their intended purpose: subjective ocular symptom measurement and QoL assessment. Because both groups of questionnaires rely on the subjective responses of individual patients, we compiled a table to differentiate the characteristics and purposes of each questionnaire (Table 1).
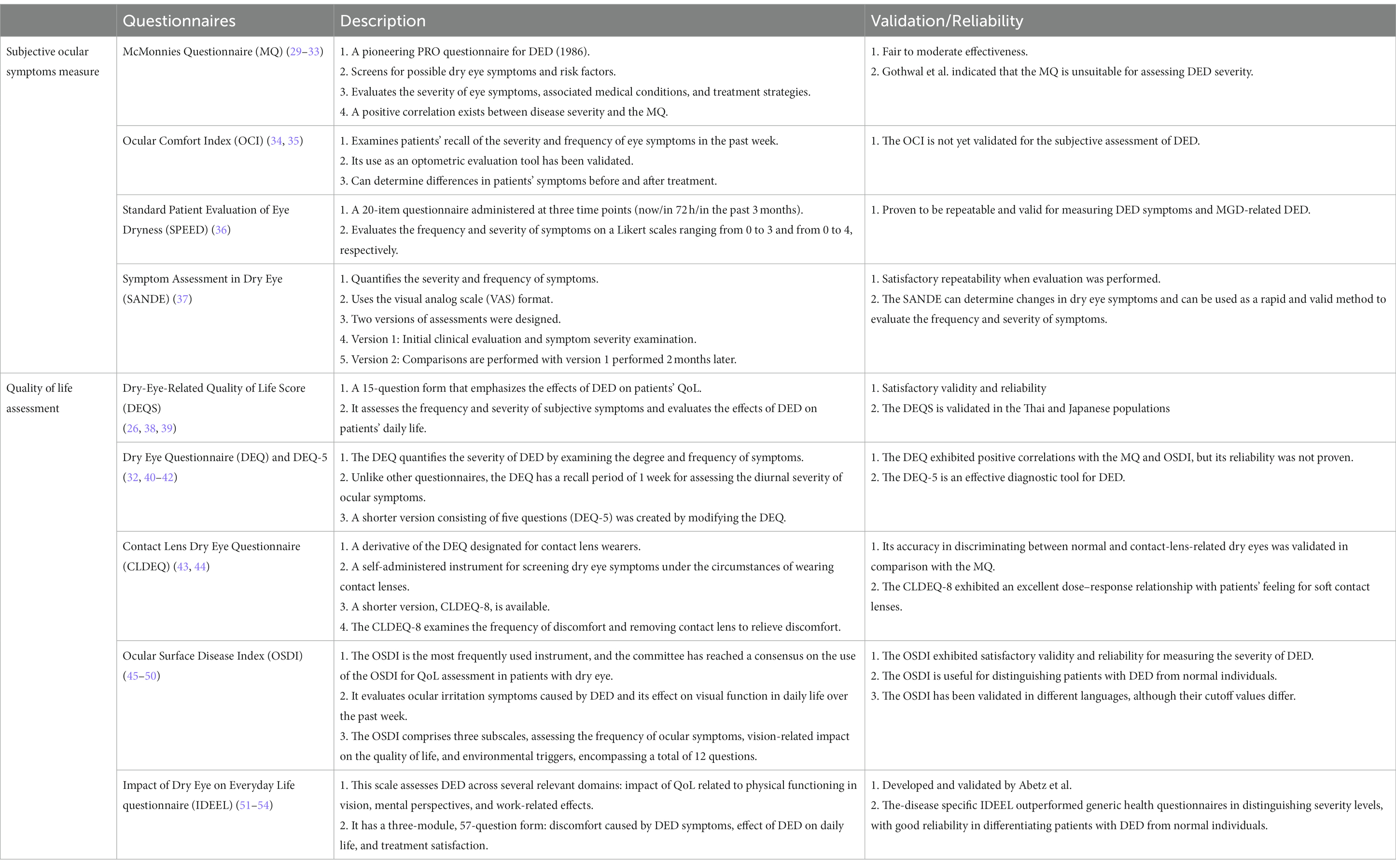
Table 1. Questionnaires and assessment tools for DED and ocular symptoms.
AT and ointments are commonly used as first-line therapy 1 (55, 56). They are available in various formulations with different active ingredients, electrolyte compositions, osmolarity, and viscosities (57). These formulations may contain viscosity-enhancing agents, electrolytes, osmoprotectants, oily compounds, antioxidants, and preservatives. Oily agents and surfactants supplement the tear film lipid layer. Antioxidants, such as vitamin A and vitamin E, are integrated to address oxidative stress associated with DED (58, 59).
Polymeric composites are commonly incorporated into artificial tears due to their hygroscopic and mucoadhesive properties. One advantage is the enhancement of tear viscosity, which prolongs the duration of tear retention on the ocular surface and maintains smooth tear distribution (60). Among the listed ophthalmic demulcents, carbomer, also known as polyacrylic acid, is an earlier additive used to increase the viscosity of artificial tears; its capacity to prolong ocular hydration has been reported (61). Enhancing the tear remnant improves TBUT and fluorescein test results, reduces subjective symptoms (62, 63), and improves patients’ QoL (64, 65). Since then, polymeric composites have been used to alleviate the symptoms of DED (Table 2).
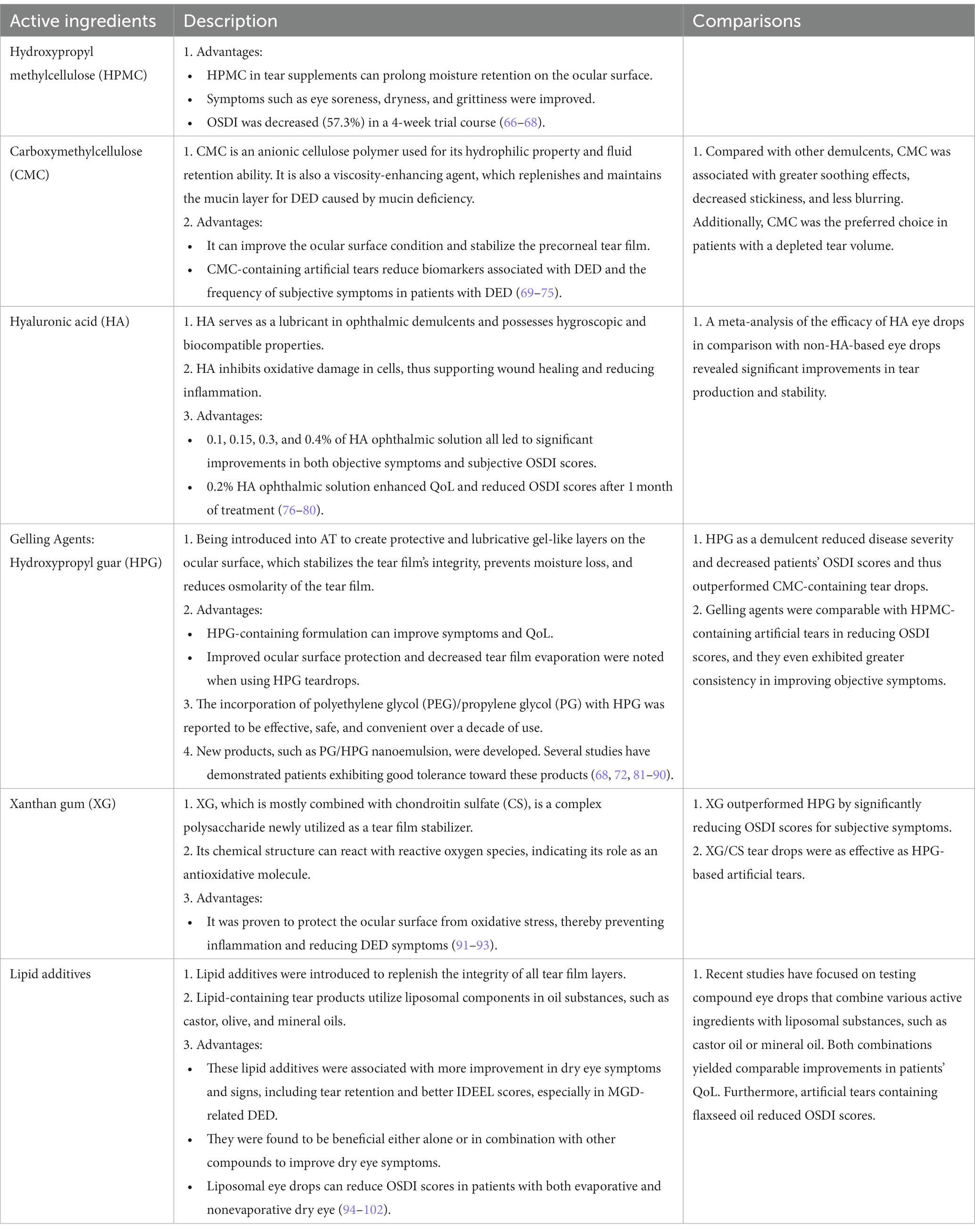
Table 2. Tear supplement: active ingredients.
The hyperosmolarity of the tear film enhances inflammatory responses, leading to the morphological damage of ocular surface cells such as apoptosis of cells of the conjunctiva and cornea. The hyperosmolarity also triggers inflammatory cascades that contribute to further cell death, including loss of mucin-producing goblet cells. These reactions exacerbate DED symptoms (112). Conventional methods for addressing hyperosmolarity in DED involve the use of hypotonic tear substitutes, which exhibit a relatively brief duration for 1-2 minutes. Recently, new formulations of artificial tears have been created, incorporating one or more osmoprotectants. Table 3 contains the types of osmoprotectants that have been utilized.
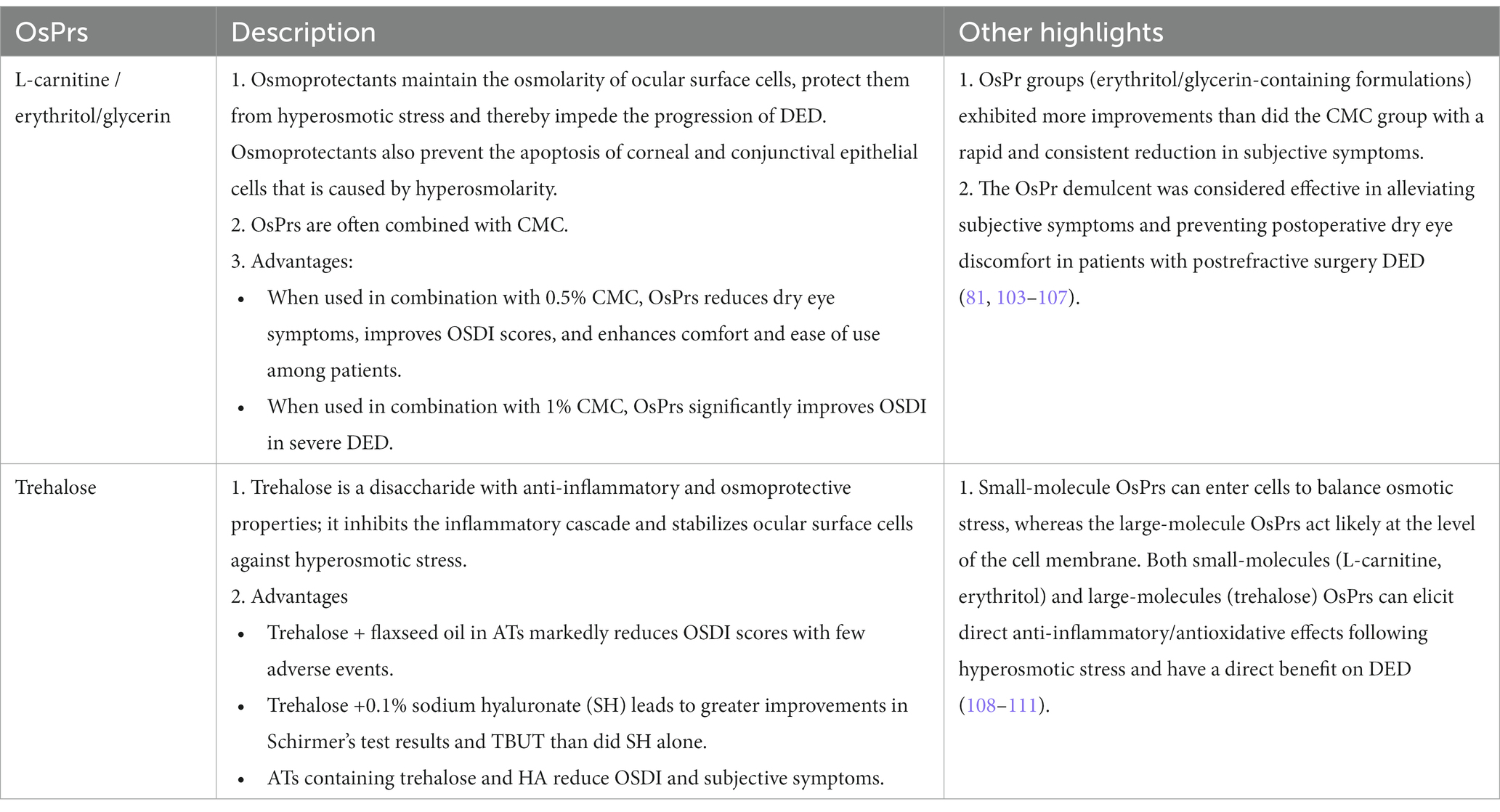
Table 3. Types of osmoprotectants (OsPrs).
Topical immunomodulators have been used because of their ability to disrupt the inflammation pathway (Table 4) (140). Although topical corticosteroids can effectively disrupt the inflammatory and immune response cycle of DED, their long-term use can cause complications, such as ocular hypertension and opportunistic infections (141, 142). Tetracyclines are broad-spectrum antibiotics that possess anti-inflammatory properties. They are occasionally prescribed to treat disorders associated with DED. However, the long-term risks and safety of their use are still not well understood (141). Table 5 lists the effective topical immunomodulators, which had been applied clinically.
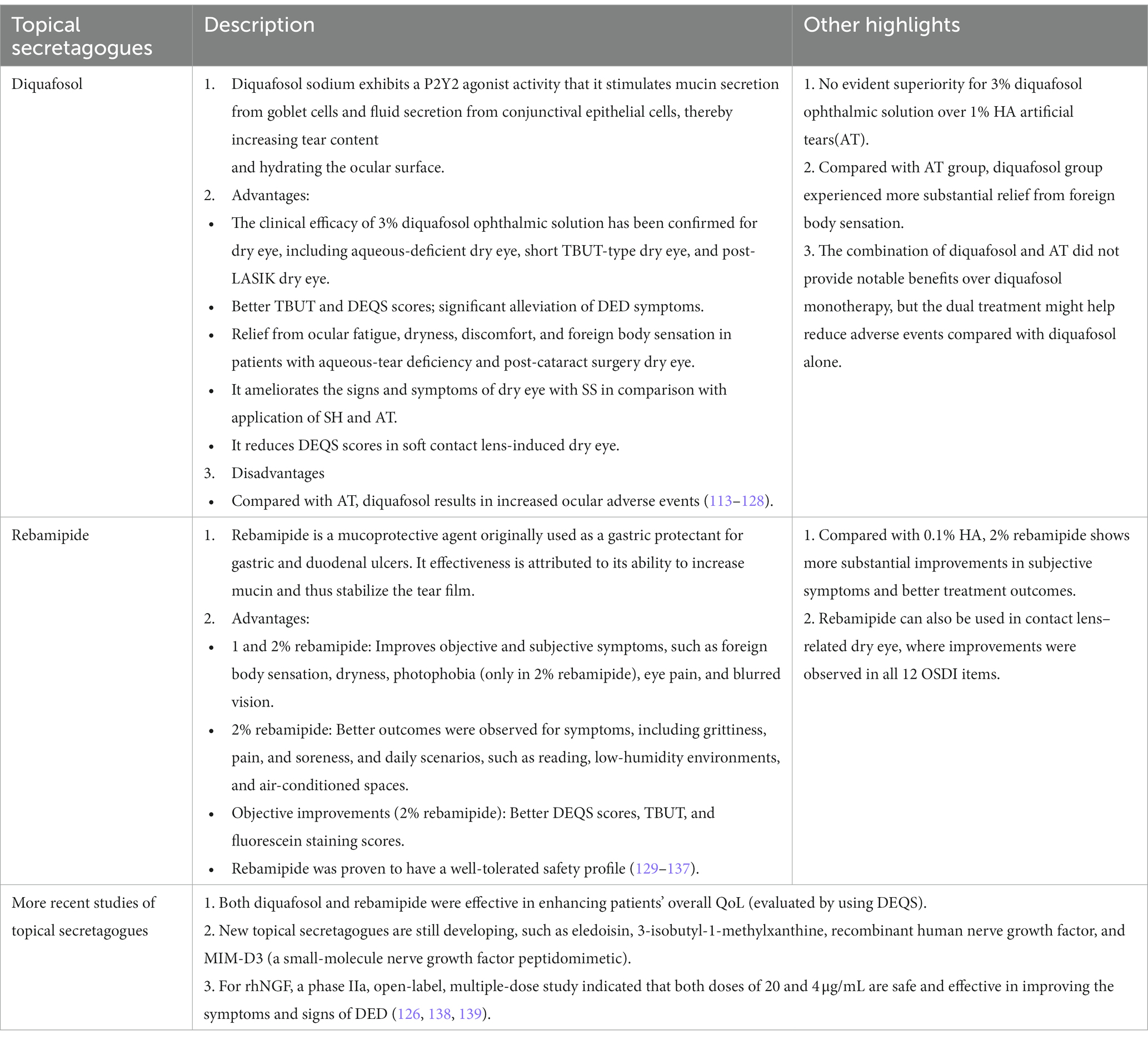
Table 4. Topical secretagogues.
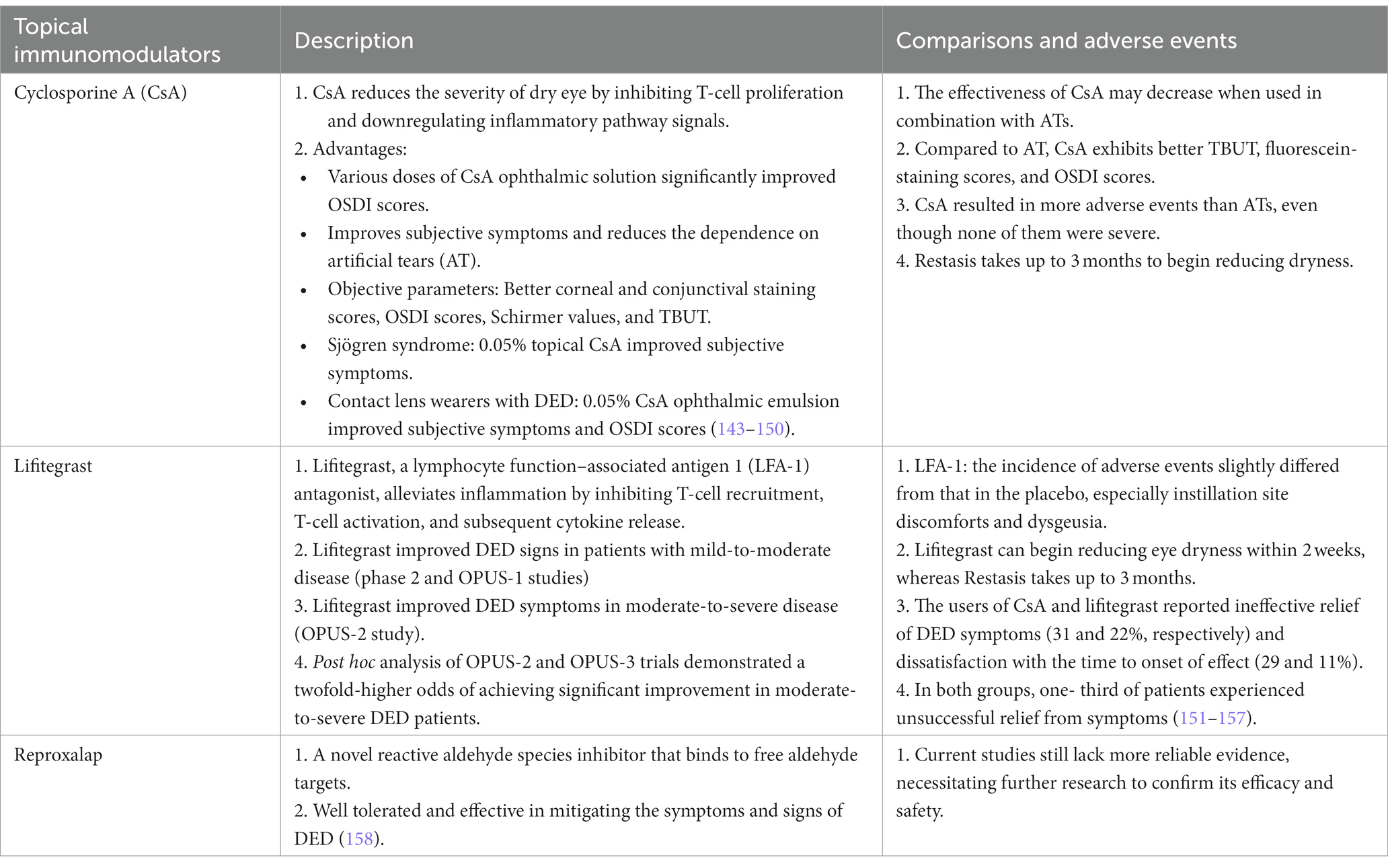
Table 5. Topical immunomodulators.
Blood-derived topical products were first used to treat ocular surface disease by Ralph et al. in 1979 (159). Since then, serum eye tears have been used to treat DED in clinical practice (Table 6).
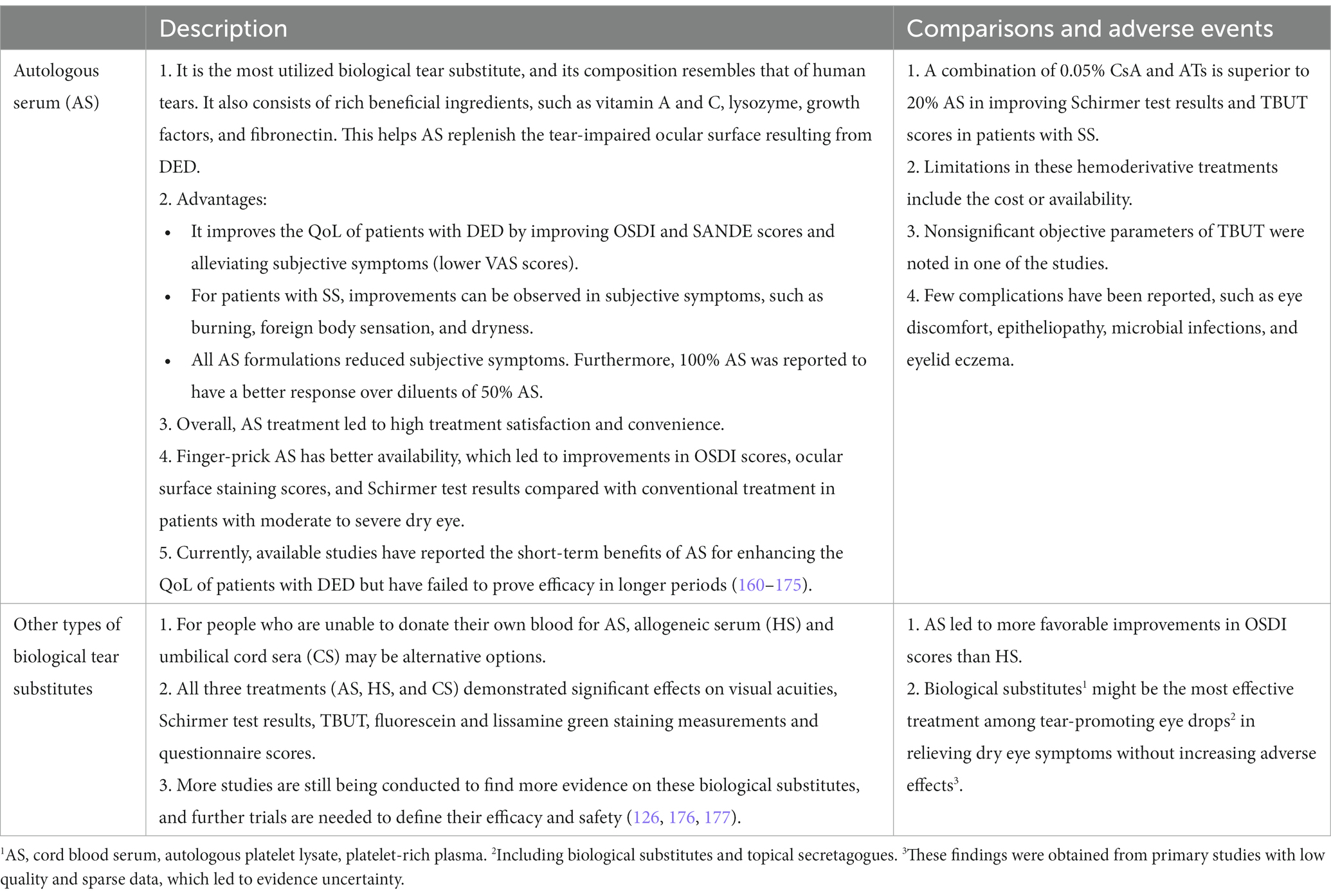
Table 6. Biological tear substitutes.
Previous studies have explored the use of nutritional strategies to improve DED. A novel botanical combination of lutein ester; zeaxanthin; and extracts from blackcurrant, chrysanthemum, and goji berry was designed to treat adults with eye fatigue. This formula ameliorated eye soreness, blurred vision, dry eye, foreign body sensation, and increased tearing, resulting in enhanced scores on questionnaires used to evaluate dry eye conditions (178).
Punctal occlusion can reduce the drainage of tears into the lacrimal ducts, thereby conserving tears, providing lubrication, and alleviating dry eye symptoms (179). Many types of plugs, including those made of silicone and collagen, have been investigated. Improvements in irritative symptoms, as well as reductions in central, superior, nasal, and temporal corneal staining were noted DED patients with bilateral punctal plug insertion (Table 7).
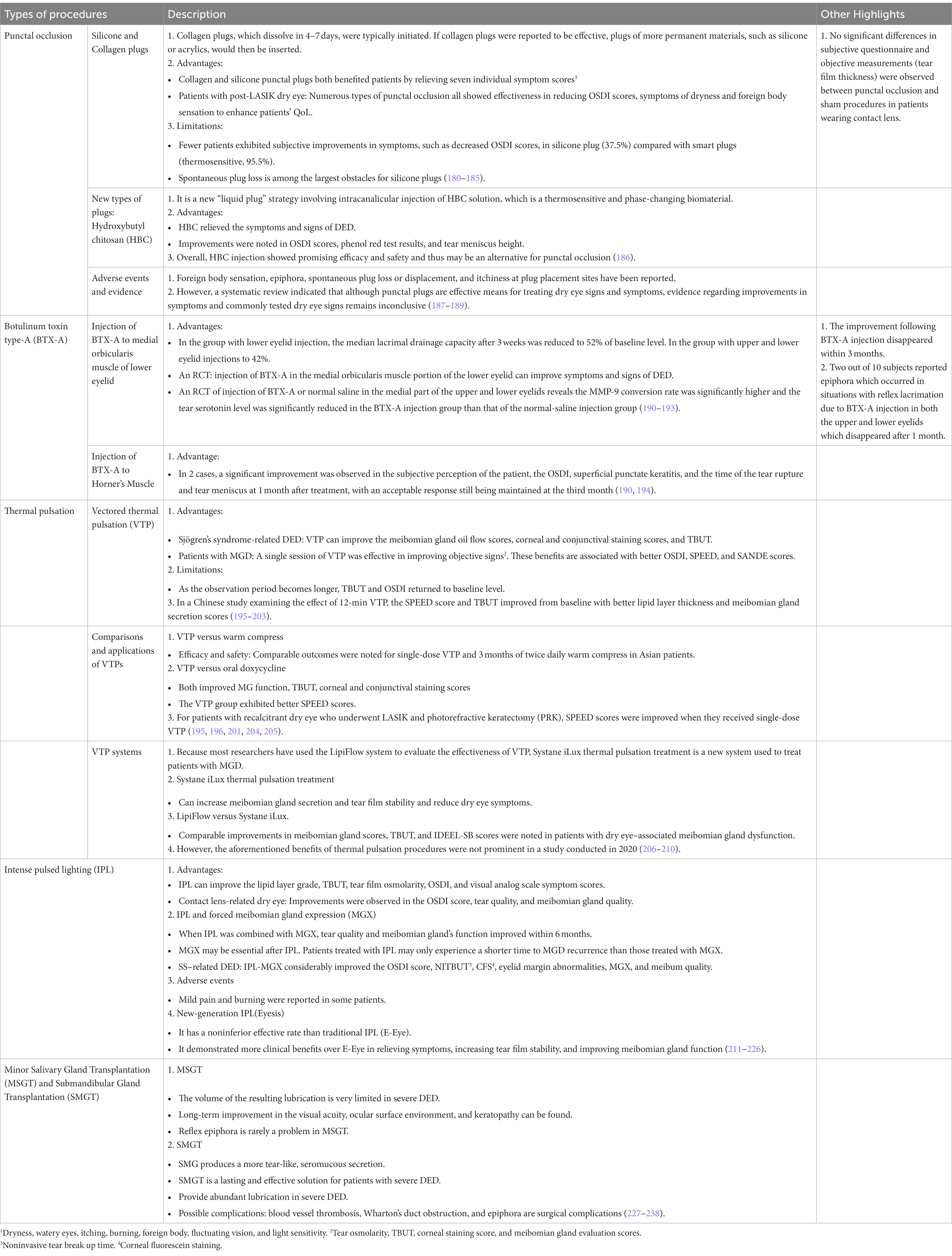
Table 7. Procedure options for DED.
Botulinum toxin type A injection in the medial part of the lower eyelid is considered an alternative method of punctal occlusion to reduce lacrimal drainage (239). Botulin toxin type-A (BTX-A) can demonstrate less lacrimal clearance by denervating lacrimal part of orbicularis oculi muscle. This procedure can be done by injecting BTX-A into upper or lower eyelids. Injection in the lower eyelid alone showed better improvements than injection in both the upper and lower eyelids. However, the effect cannot last long in most patient with a range of 3 months (240).
Vector thermal pulsation (VTP) can provide warm compress to the eyelids and meibomian gland (241). Thermal pulsation has many advantages, with potentially the longest-lasting per-treatment effect for MGD (206). Intense pulsed lighting involves the application of highly intensified pulses of polychromatic light across a broad wavelength range (515–1,200 nm) for eliminating superficial capillary vessels in the periocular region, reducing the release of tear inflammatory cytokines, and improving the outflow of the meibomian gland (211). However, because of the paucity of high-quality research, the effectiveness and safety of long-term intense pulsed lighting treatment for MGD remain uncertain, necessitating further research (242).
Salivary gland transplantation should be considered to treat severe DED. Submandibular gland transplantation (SMGT) and minor salivary gland transplantation (MSGT) are the most commonly used procedure, while parotid gland was proved to be non-beneficial for severe DED (227, 228). Previous studies demonstrated autologous microvascular SMGT improved objective signs and subjective symptoms of severe DED (229, 230, 243). Su et al. conducted a prospective study and revealed that the significant improvement of life quality and satisfaction of DED patients after SMGT (231). Although SMGT and MSGT provided benefits for severe DED patients, SMGT should be recommended to treat end-stage refractory DED (232). Table 8 compiles a summary of various treatment options for DED, encompassing tear supplements, osmoprotectants, secretagogues, immunomodulators, biological tear substitutes, and procedures.
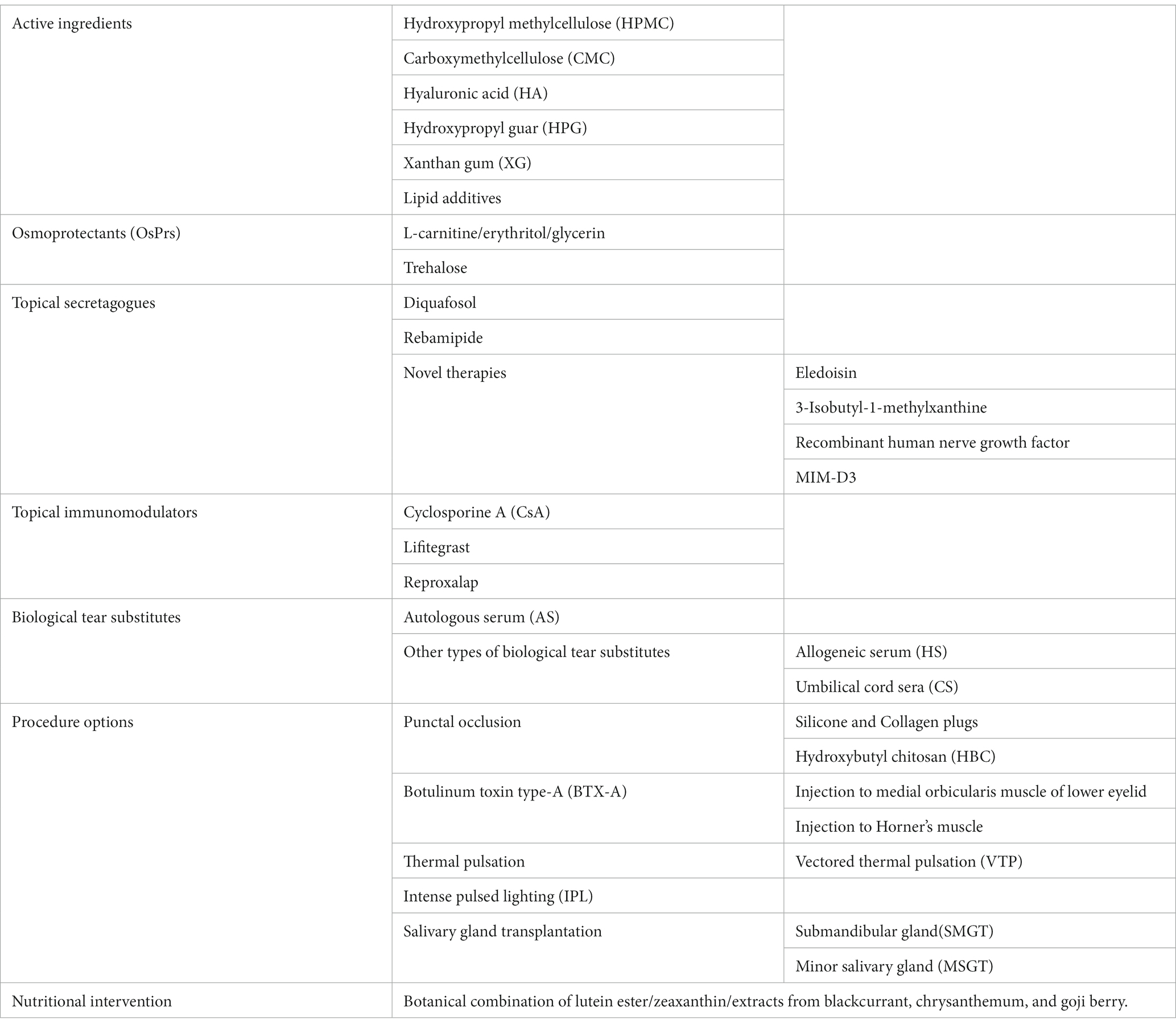
Table 8. Treatment options for DED.
In our investigation of various treatments and questionnaires for DED, we found multiple validated questionnaires designed to collect PROs. Although inconsistencies exist between questionnaires and clinical findings, they provide valuable information in the initial evaluation and monitoring of DED treatments. However, the lack of standardized measures and intergroup conversion causes difficulty in cross-comparison.
The initial therapy of DED involves the use of artificial tears. Over-the-counter formulations containing ingredients, such as CMC and HA, and osmoprotectants, such as trehalose, aim to restore hydration and lubrication, thereby alleviating dry eye symptoms (69, 244). However, in advanced cases of moderate-to-severe dry eyes, artificial tears might not be effective (245). Liposomal tear drops are beneficial for both evaporative and non-evaporative DED (94), and secretagogue drops can improve the QoL of patients with short TBUT or aqueous deficient-type DED (113).
Immunomodulators provide rapid symptom relief, and most patients with DED report the effectiveness and high satisfaction rate of cyclosporine A (CsA) and lifitegrast (246–248). However, trials have consistently reported adverse events, such as irritation or pain at the instillation site, which may affect patient compliance and therapy efficacy (249, 250).
Patients who received autologous serum (AS) treatments reported high satisfaction and expressed eagerness to continue the therapy (251). However, well-established production and storage protocols are still needed for their clinical use (160, 161). Punctual occlusion has been performed to either temporarily or permanently block tear drainage from the lacrimal punctum. However, this procedure is associated with a higher complication rate (even up to 60%) (252), making it a less favorable option for treating DED (239). BTX-A serving as a temporary solution for DED, it can significantly improve symptoms within 3 months by reducing lacrimal drainage (240).
VTP is a novel therapy option, particularly for DED caused by MGD (195, 253). VTP offers a convenient solution for individuals with MGD-related dry eye, representing an alternative treatment option for patients with modern busy lifestyles (254). Intense pulsed light(IPL) also has proven to be effective for treating evaporative dry eye caused by MGD (255), with 93% of patients reporting posttreatment satisfaction without any severe adverse effects. Multiple studies have confirmed the efficacy of combining IPL treatment with meibomian gland manipulation (256).
In severe DED cases, SMGT offers a promising approach for tear film restoration (243). Previous studies demonstrated autologous SMGT has a high success rate, and it significantly improved quality of life and satisfaction (231).
Overall, patient satisfaction and QoL evaluations often improved after different DED treatment modalities. This review highlights the importance of PRO assessments for evaluating the effect of DED treatments on subjective symptoms and QoL. Given that the assessment of DED treatment effectiveness substantially relies on individual ocular experiences, acquiring qualitative PRO data is essential for comprehensive evaluation and optimal treatment management. Clinicians should not only focus on improving objective symptoms but also prioritize the well-being of patients in clinical settings.
C-WL: Investigation, Writing – original draft. M-YL: Conceptualization, Formal analysis, Supervision, Visualization, Writing – review & editing. J-WH: Conceptualization, Formal analysis, Methodology, Resources, Writing – review & editing. T-JW: Writing – original draft, Investigation, Methodology, Project administration, Visualization. I-CL: Methodology, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported in part by a grant from Taipei Medical University (TMU112-AE1-B04).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Papas, EB. The global prevalence of dry eye disease: a Bayesian view. Ophthalmic Physiol Opt. (2021) 41:1254–66. doi: 10.1111/opo.12888
2. Zaiy, H. Dry eye syndrome risk factors: a systemic review. Saudi J Ophthalmol. (2021) 35:131–9. doi: 10.4103/1319-4534.337849
3. Kuo, YK, Lin, IC, Chien, LN, Lin, TY, How, YT, Chen, KH, et al. Dry eye disease: a review of epidemiology in Taiwan, and its clinical treatment and merits. J Clin Med. (2019) 8:1227. doi: 10.3390/jcm8081227
4. Han, SB, Hyon, JY, Woo, SJ, Lee, JJ, Kim, TH, and Kim, KW. Prevalence of dry eye disease in an elderly Korean population. Arch Ophthalmol. (2011) 129:633–8. doi: 10.1001/archophthalmol.2011.78
5. Uchino, M, Dogru, M, Yagi, Y, Goto, E, Tomita, M, Kon, T, et al. The features of dry eye disease in a Japanese elderly population. Optom Vis Sci. (2006) 83:797–802. doi: 10.1097/01.opx.0000232814.39651.fa
6. Lemp, MA. Report of the National eye Institute/industry workshop on clinical trials in dry eyes. CLAO J. (1995) 21:221–32.
7. Nichols, KK, Foulks, GN, Bron, AJ, Glasgow, BJ, Dogru, M, Tsubota, K, et al. The international workshop on meibomian gland dysfunction: executive summary. Invest Ophthalmol Vis Sci. (2011) 52:1922–9. doi: 10.1167/iovs.10-6997a
9. Tsubota, K, Yokoi, N, Watanabe, H, Dogru, M, Kojima, T, Yamada, M, et al. A new perspective on dry eye classification: proposal by the Asia dry eye society. Eye Contact Lens. (2020) 46:S2–S13. doi: 10.1097/ICL.0000000000000643
10. Chan, TCY, Chow, SSW, Wan, KHN, and Yuen, HKL. Update on the association between dry eye disease and meibomian gland dysfunction. Hong Kong Med J. (2019) 25:38–47. doi: 10.12809/hkmj187331
11. Knop, E, Knop, N, Millar, T, Obata, H, and Sullivan, DA. The international workshop on meibomian gland dysfunction: report of the subcommittee on anatomy, physiology, and pathophysiology of the meibomian gland. Invest Ophthalmol Vis Sci. (2011) 52:1938–78. doi: 10.1167/iovs.10-6997c
12. Whitcher, JP, Shiboski, CH, Shiboski, SC, Heidenreich, AM, Kitagawa, K, Zhang, S, et al. A simplified quantitative method for assessing keratoconjunctivitis sicca from the Sjogren's syndrome international registry. Am J Ophthalmol. (2010) 149:405–15. doi: 10.1016/j.ajo.2009.09.013
13. Liew, MS, Zhang, M, Kim, E, and Akpek, EK. Prevalence and predictors of Sjogren's syndrome in a prospective cohort of patients with aqueous-deficient dry eye. Br J Ophthalmol. (2012) 96:1498–503. doi: 10.1136/bjophthalmol-2012-301767
14. Moss, SE, Klein, R, and Klein, BE. Prevalence of and risk factors for dry eye syndrome. Arch Ophthalmol. (2000) 118:1264–8. doi: 10.1001/archopht.118.9.1264
15. de Paiva, CS. Effects of aging in dry eye. Int Ophthalmol Clin. (2017) 57:47–64. doi: 10.1097/IIO.0000000000000170
16. Wang, MTM, Muntz, A, Mamidi, B, Wolffsohn, JS, and Craig, JP. Modifiable lifestyle risk factors for dry eye disease. Cont Lens Anterior Eye. (2021) 44:101409. doi: 10.1016/j.clae.2021.01.004
17. Toda, I. Dry eye after LASIK. Invest Ophthalmol Vis Sci. (2018) 59:DES109-DES15. doi: 10.1167/iovs.17-23538
18. Iglesias, E, Sajnani, R, Levitt, RC, Sarantopoulos, CD, and Galor, A. Epidemiology of persistent dry eye-like symptoms after cataract surgery. Cornea. (2018) 37:893–8. doi: 10.1097/ICO.0000000000001491
19. Craig, JP, Nichols, KK, Akpek, EK, Caffery, B, Dua, HS, Joo, CK, et al. TFOS DEWS II definition and classification report. Ocul Surf. (2017) 15:276–83. doi: 10.1016/j.jtos.2017.05.008
20. Korb, DR, and Blackie, CA. Meibomian gland diagnostic expressibility: correlation with dry eye symptoms and gland location. Cornea. (2008) 27:1142–7. doi: 10.1097/ICO.0b013e3181814cff
21. Maskin, SL. Intraductal meibomian gland probing relieves symptoms of obstructive meibomian gland dysfunction. Cornea. (2010) 29:1145–52. doi: 10.1097/ICO.0b013e3181d836f3
22. Nichols, KK, Nichols, JJ, and Mitchell, GL. The lack of association between signs and symptoms in patients with dry eye disease. Cornea. (2004) 23:762–70. doi: 10.1097/01.ico.0000133997.07144.9e
23. Johnson, ME. The association between symptoms of discomfort and signs in dry eye. Ocul Surf. (2009) 7:199–211. doi: 10.1016/S1542-0124(12)70187-8
24. Giannaccare, G, and Di Zazzo, A. Special issue "diagnosis and Management of dry eye Disease and Ocular Surface Inflammation". Medicina (Kaunas). (2022) 58:764. doi: 10.3390/medicina58060764
25. Behrens, A, Doyle, JJ, Stern, L, Chuck, RS, McDonnell, PJ, Azar, DT, et al. Dysfunctional tear syndrome: a Delphi approach to treatment recommendations. Cornea. (2006) 25:900–7. doi: 10.1097/01.ico.0000214802.40313.fa
26. U.S. Department of Health and Human Services FDA Center for Drug Evaluation and Research; U.S. Department of Health and Human Services FDA Center for Biologics Evaluation and Research; U.S. Department of Health and Human Services FDA Center for Devices and Radiological Health. Guidance for industry: Patient-reported outcome measures: use in medical product development to support labeling claims: draft guidance. Health Qual Life Outcomes. (2006) 4:79. doi: 10.1186/1477-7525-4-79
27. Bartlett, JD, Keith, MS, Sudharshan, L, and Snedecor, SJ. Associations between signs and symptoms of dry eye disease: a systematic review. Clin Ophthalmol. (2015) 9:1719–30. doi: 10.2147/OPTH.S89700
28. Begley, CG, Caffery, B, Chalmers, RL, and Mitchell, GLDry Eye Investigation Study G. Use of the dry eye questionnaire to measure symptoms of ocular irritation in patients with aqueous tear deficient dry eye. Cornea. (2002) 21:664–70. doi: 10.1097/00003226-200210000-00007
29. Nichols, KK, Nichols, JJ, and Mitchell, GL. The reliability and validity of McMonnies dry eye index. Cornea. (2004) 23:365–71. doi: 10.1097/00003226-200405000-00010
30. Lu, F, Tao, A, Hu, Y, Tao, W, and Lu, P. Evaluation of reliability and validity of three common dry eye questionnaires in Chinese. J Ophthalmol. (2018) 2018:1–6. doi: 10.1155/2018/2401213
31. Guo, Y, Peng, R, Feng, K, and Hong, J. Diagnostic performance of McMonnies questionnaire as a screening survey for dry eye: a multicenter analysis. J Ophthalmol. (2016) 2016:1–6. doi: 10.1155/2016/6210853
32. Simpson, TL, Situ, P, Jones, LW, and Fonn, D. Dry eye symptoms assessed by four questionnaires. Optom Vis Sci. (2008) 85:692–9. doi: 10.1097/OPX.0b013e318181ae36
33. Gothwal, VK, Pesudovs, K, Wright, TA, and McMonnies, CW. McMonnies questionnaire: enhancing screening for dry eye syndromes with Rasch analysis. Invest Ophthalmol Vis Sci. (2010) 51:1401–7. doi: 10.1167/iovs.09-4180
34. Johnson, ME, and Murphy, PJ. Measurement of ocular surface irritation on a linear interval scale with the ocular comfort index. Invest Ophthalmol Vis Sci. (2007) 48:4451–8. doi: 10.1167/iovs.06-1253
35. McAlinden, C, Gao, R, Wang, Q, Zhu, S, Yang, J, Yu, A, et al. Rasch analysis of three dry eye questionnaires and correlates with objective clinical tests. Ocul Surf. (2017) 15:202–10. doi: 10.1016/j.jtos.2017.01.005
36. Facchin, A, and Boccardo, L. Italian translation, validation, and repeatability of standard patient evaluation of eye dryness (SPEED) questionnaire. Cont Lens Anterior Eye. (2022) 45:101497. doi: 10.1016/j.clae.2021.101497
37. Schaumberg, DA, Gulati, A, Mathers, WD, Clinch, T, Lemp, MA, Nelson, JD, et al. Development and validation of a short global dry eye symptom index. Ocul Surf. (2007) 5:50–7. doi: 10.1016/S1542-0124(12)70053-8
38. Sakane, Y, Yamaguchi, M, Yokoi, N, Uchino, M, Dogru, M, Oishi, T, et al. Development and validation of the dry eye-related quality-of-life score questionnaire. JAMA Ophthalmol. (2013) 131:1331–8. doi: 10.1001/jamaophthalmol.2013.4503
39. Tananuvat, N, Tansanguan, S, Wongpakaran, N, and Wongpakaran, T. Reliability, validity, and responsiveness of the Thai version of the dry eye-related quality-of-life score questionnaire. PLoS One. (2022) 17:e0271228. doi: 10.1371/journal.pone.0271228
40. Begley, CG, Chalmers, RL, Mitchell, GL, Nichols, KK, Caffery, B, Simpson, T, et al. Characterization of ocular surface symptoms from optometric practices in North America. Cornea. (2001) 20:610–8. doi: 10.1097/00003226-200108000-00011
41. Chalmers, RL, Begley, CG, and Caffery, B. Validation of the 5-item dry eye questionnaire (DEQ-5): discrimination across self-assessed severity and aqueous tear deficient dry eye diagnoses. Cont Lens Anterior Eye. (2010) 33:55–60. doi: 10.1016/j.clae.2009.12.010
42. Akowuah, PK, Adjei-Anang, J, Nkansah, EK, Fummey, J, Osei-Poku, K, Boadi, P, et al. Comparison of the performance of the dry eye questionnaire (DEQ-5) to the ocular surface disease index in a non-clinical population. Cont Lens Anterior Eye. (2022) 45:101441. doi: 10.1016/j.clae.2021.101441
43. Nichols, JJ, Mitchell, GL, Nichols, KK, Chalmers, R, and Begley, C. The performance of the contact lens dry eye questionnaire as a screening survey for contact lens-related dry eye. Cornea. (2002) 21:469–75. doi: 10.1097/00003226-200207000-00007
44. Chalmers, RL, Begley, CG, Moody, K, and Hickson-Curran, SB. Contact Lens dry eye Questionnaire-8 (CLDEQ-8) and opinion of contact lens performance. Optom Vis Sci. (2012) 89:1435–42. doi: 10.1097/OPX.0b013e318269c90d
45. Walt, J, Rowe, M, and Stern, K. Evaluating the functional impact of dry eye: the ocular surface disease index. Drug Inf J. (1997) 31:b5
46. Grubbs, JR Jr, Tolleson-Rinehart, S, Huynh, K, and Davis, RM. A review of quality of life measures in dry eye questionnaires. Cornea. (2014) 33:215–8. doi: 10.1097/ICO.0000000000000038
47. Ozcura, F, Aydin, S, and Helvaci, MR. Ocular surface disease index for the diagnosis of dry eye syndrome. Ocul Immunol Inflamm. (2007) 15:389–93. doi: 10.1080/09273940701486803
48. Schiffman, RM, Christianson, MD, Jacobsen, G, Hirsch, JD, and Reis, BL. Reliability and validity of the ocular surface disease index. Arch Ophthalmol. (2000) 118:615–21. doi: 10.1001/archopht.118.5.615
49. Okumura, Y, Inomata, T, Iwata, N, Sung, J, Fujimoto, K, Fujio, K, et al. A review of dry eye questionnaires: measuring patient-reported outcomes and health-related quality of life. Diagnostics (Basel). (2020) 10:559. doi: 10.3390/diagnostics10080559
50. Wolffsohn, JS, Arita, R, Chalmers, R, Djalilian, A, Dogru, M, Dumbleton, K, et al. TFOS DEWS II diagnostic methodology report. Ocul Surf. (2017) 15:539–74. doi: 10.1016/j.jtos.2017.05.001
51. Guillemin, I, Begley, C, Chalmers, R, Baudouin, C, and Arnould, B. Appraisal of patient-reported outcome instruments available for randomized clinical trials in dry eye: revisiting the standards. Ocul Surf. (2012) 10:84–99. doi: 10.1016/j.jtos.2012.01.007
52. Abetz, L, Rajagopalan, K, Mertzanis, P, Begley, C, Barnes, R, Chalmers, R, et al. Development and validation of the impact of dry eye on everyday life (IDEEL) questionnaire, a patient-reported outcomes (PRO) measure for the assessment of the burden of dry eye on patients. Health Qual Life Outcomes. (2011) 9:111. doi: 10.1186/1477-7525-9-111
53. Rajagopalan, K, Abetz, L, Mertzanis, P, Espindle, D, Begley, C, Chalmers, R, et al. Comparing the discriminative validity of two generic and one disease-specific health-related quality of life measures in a sample of patients with dry eye. Value Health. (2005) 8:168–74. doi: 10.1111/j.1524-4733.2005.03074.x
54. Recchioni, A, Aiyegbusi, OL, Cruz-Rivera, S, Rauz, S, and Slade, A. A systematic review assessing the quality of patient reported outcomes measures in dry eye diseases. PLoS One. (2021) 16:e0253857. doi: 10.1371/journal.pone.0253857
55. Schirra, F, and Ruprecht, KW. Dry eye. An update on epidemiology, diagnosis, therapy and new concepts. Ophthalmologe. (2004) 101:10–8. doi: 10.1007/s00347-003-0958-0
56. Hakim, FE, and Farooq, AV. Dry eye disease: an update in 2022. JAMA. (2022) 327:478–9. doi: 10.1001/jama.2021.19963
58. Augustin, AJ, Spitznas, M, Kaviani, N, Meller, D, Koch, FH, Grus, F, et al. Oxidative reactions in the tear fluid of patients suffering from dry eyes. Graefes Arch Clin Exp Ophthalmol. (1995) 233:694–8. doi: 10.1007/BF00164671
59. Labetoulle, M, Benitez-Del-Castillo, JM, Barabino, S, Herrero Vanrell, R, Daull, P, Garrigue, JS, et al. Artificial tears: biological role of their ingredients in the management of dry eye disease. Int J Mol Sci. (2022) 23:2434. doi: 10.3390/ijms23052434
60. Calles, JA, Bermúdez, J, Vallés, E, Allemandi, D, and Palma, S. Polymers in ophthalmology In: F Puoci, editor. Advanced Polymers in Medicine. Switzerland: Springer International Publishing (2014). 147–76.
61. Oechsner, M, and Keipert, S. Polyacrylic acid/polyvinylpyrrolidone bipolymeric systems. I. Rheological and mucoadhesive properties of formulations potentially useful for the treatment of dry-eye-syndrome. Eur J Pharm Biopharm. (1999) 47:113–8. doi: 10.1016/S0939-6411(98)00070-8
62. Bron, AJ, Daubas, P, Siou-Mermet, R, and Trinquand, C. Comparison of the efficacy and safety of two eye gels in the treatment of dry eyes: Lacrinorm and Viscotears. Eye (Lond). (1998) 12:839–47. doi: 10.1038/eye.1998.215
63. Sullivan, LJ, McCurrach, F, Lee, S, Taylor, HR, Rolando, M, Marechal-Courtois, C, et al. Efficacy and safety of 0.3% carbomer gel compared to placebo in patients with moderate-to-severe dry eye syndrome. Ophthalmology. (1997) 104:1402–8. doi: 10.1016/S0161-6420(97)30124-9
64. Smolle, M, Keller, C, Pinggera, G, Deibl, M, Rieder, J, and Lirk, P. Clear hydro-gel, compared to ointment, provides improved eye comfort after brief surgery. Can J Anaesth. (2004) 51:126–9. doi: 10.1007/BF03018770
65. de Araujo, DD, Silva, DVA, Rodrigues, CAO, Silva, PO, Macieira, TGR, and Chianca, TCM. Effectiveness of nursing interventions to prevent dry eye in critically ill patients. Am J Crit Care. (2019) 28:299–306. doi: 10.4037/ajcc2019360
66. Toda, I, Shinozaki, N, and Tsubota, K. Hydroxypropyl methylcellulose for the treatment of severe dry eye associated with Sjogren's syndrome. Cornea. (1996) 15:120–8. doi: 10.1097/00003226-199603000-00003
67. Prabhasawat, P, Tesavibul, N, and Kasetsuwan, N. Performance profile of sodium hyaluronate in patients with lipid tear deficiency: randomised, double-blind, controlled, exploratory study. Br J Ophthalmol. (2007) 91:47–50. doi: 10.1136/bjo.2006.097691
68. Maharana, PK, Raghuwanshi, S, Chauhan, AK, Rai, VG, and Pattebahadur, R. Comparison of the efficacy of carboxymethylcellulose 0.5%, hydroxypropyl-guar containing polyethylene glycol 400/propylene glycol, and hydroxypropyl methyl cellulose 0.3% tear substitutes in improving ocular surface disease index in cases of dry eye. Middle East Afr J Ophthalmol. (2017) 24:202–6. doi: 10.4103/meajo.MEAJO_165_15
69. Kaercher, T, Buchholz, P, and Kimmich, F. Treatment of patients with keratoconjunctivitis sicca with Optive: results of a multicenter, open-label observational study in Germany. Clin Ophthalmol. (2009) 3:33–9.
70. Simmons, PA, and Vehige, JG. Clinical performance of a mid-viscosity artificial tear for dry eye treatment. Cornea. (2007) 26:294–302. doi: 10.1097/ICO.0b013e31802e1e04
71. Bruix, A, Adan, A, and Casaroli-Marano, RP. Efficacy of sodium carboxymethylcellulose in the treatment of dry eye syndrome. Arch Soc Esp Oftalmol. (2006) 81:85–92. doi: 10.4321/s0365-66912006000200008
72. Davitt, WF, Bloomenstein, M, Christensen, M, and Martin, AE. Efficacy in patients with dry eye after treatment with a new lubricant eye drop formulation. J Ocul Pharmacol Ther. (2010) 26:347–53. doi: 10.1089/jop.2010.0025
73. Martin, E, Oliver, KM, Pearce, EI, Tomlinson, A, Simmons, P, and Hagan, S. Effect of tear supplements on signs, symptoms and inflammatory markers in dry eye. Cytokine. (2018) 105:37–44. doi: 10.1016/j.cyto.2018.02.009
74. Noecker, RJ. Comparison of initial treatment response to two enhanced-viscosity artificial tears. Eye Contact Lens. (2006) 32:148–52. doi: 10.1097/01.icl.0000181819.63425.a6
75. Essa, L, Laughton, D, and Wolffsohn, JS. Can the optimum artificial tear treatment for dry eye disease be predicted from presenting signs and symptoms? Cont Lens Anterior Eye. (2018) 41:60–8. doi: 10.1016/j.clae.2017.07.007
76. Milas, M, and Rinaudo, M. Characterization and properties of hyaluronic acid (Hyaluronan). Polysaccharides. (2004) 1:535–50. doi: 10.1201/9781420030822.ch22
77. Pinto-Fraga, J, Lopez-de la Rosa, A, Blazquez Arauzo, F, Urbano Rodriguez, R, and Gonzalez-Garcia, MJ. Efficacy and safety of 0.2% hyaluronic acid in the Management of dry eye Disease. Eye Contact Lens. (2017) 1:57–63. doi: 10.1097/ICL.0000000000000236
78. Park, Y, Song, JS, Choi, CY, Yoon, KC, Lee, HK, and Kim, HS. A randomized multicenter study comparing 0.1, 0.15, and 0.3% sodium hyaluronate with 0.05% cyclosporine in the treatment of dry eye. J Ocul Pharmacol Ther. (2017) 33:66–72. doi: 10.1089/jop.2016.0086
79. Aragona, P, Benitez-Del-Castillo, JM, Coroneo, MT, Mukherji, S, Tan, J, Vandewalle, E, et al. Safety and efficacy of a preservative-free artificial tear containing Carboxymethylcellulose and hyaluronic acid for dry eye disease: a randomized, controlled, multicenter 3-month study. Clin Ophthalmol. (2020) 14:2951–63. doi: 10.2147/OPTH.S256480
80. Yang, YJ, Lee, WY, Kim, YJ, and Hong, YP. A meta-analysis of the efficacy of hyaluronic acid eye drops for the treatment of dry eye syndrome. Int J Environ Res Public Health. (2021) 18:2383. doi: 10.3390/ijerph18052383
81. Labetoulle, M, Messmer, EM, Pisella, PJ, Ogundele, A, and Baudouin, C. Safety and efficacy of a hydroxypropyl guar/polyethylene glycol/propylene glycol-based lubricant eye-drop in patients with dry eye. Br J Ophthalmol. (2017) 101:487–92. doi: 10.1136/bjophthalmol-2016-308608
82. Christensen, MT, Cohen, S, Rinehart, J, Akers, F, Pemberton, B, Bloomenstein, M, et al. Clinical evaluation of an HP-guar gellable lubricant eye drop for the relief of dryness of the eye. Curr Eye Res. (2004) 28:55–62. doi: 10.1076/ceyr.28.1.55.23495
83. Hartstein, I, Khwarg, S, and Przydryga, J. An open-label evaluation of HP-guar gellable lubricant eye drops for the improvement of dry eye signs and symptoms in a moderate dry eye adult population. Curr Med Res Opin. (2005) 21:255–60. doi: 10.1185/030079905X26252
84. Rolando, M, Autori, S, Badino, F, and Barabino, S. Protecting the ocular surface and improving the quality of life of dry eye patients: a study of the efficacy of an HP-guar containing ocular lubricant in a population of dry eye patients. J Ocul Pharmacol Ther. (2009) 25:271–8. doi: 10.1089/jop.2008.0026
85. Jacobi, C, Kruse, FE, and Cursiefen, C. Prospective, randomized, controlled comparison of SYSTANE UD eye drops versus VISINE INTENSIV 1% EDO eye drops for the treatment of moderate dry eye. J Ocul Pharmacol Ther. (2012) 28:598–603. doi: 10.1089/jop.2012.0066
86. Labetoulle, M, Schmickler, S, Galarreta, D, Bohringer, D, Ogundele, A, Guillon, M, et al. Efficacy and safety of dual-polymer hydroxypropyl guar-and hyaluronic acid-containing lubricant eyedrops for the management of dry-eye disease: a randomized double-masked clinical study. Clin Ophthalmol. (2018) 12:2499–508. doi: 10.2147/OPTH.S177176
87. Srinivasan, S, and Manoj, V. A decade of effective dry eye disease management with Systane ultra (polyethylene glycol/propylene glycol with Hydroxypropyl guar) lubricant eye drops. Clin Ophthalmol. (2021) 15:2421–35. doi: 10.2147/OPTH.S294427
88. Silverstein, S, Yeu, E, Tauber, J, Guillon, M, Jones, L, Galarreta, D, et al. Symptom relief following a single dose of propylene glycol-Hydroxypropyl guar Nanoemulsion in patients with dry eye disease: a phase IV, multicenter trial. Clin Ophthalmol. (2020) 14:3167–77. doi: 10.2147/OPTH.S263362
89. Srinivasan, S, and Williams, R. Propylene glycol and Hydroxypropyl guar Nanoemulsion-safe and effective lubricant eye drops in the management of dry eye disease. Clin Ophthalmol. (2022) 16:3311–26. doi: 10.2147/OPTH.S377960
90. Yeu, E, Silverstein, S, Guillon, M, Schulze, MM, Galarreta, D, Srinivasan, S, et al. Efficacy and safety of phospholipid Nanoemulsion-based ocular lubricant for the Management of Various Subtypes of dry eye disease: a phase IV, Multicenter Trial. Clin Ophthalmol. (2020) 14:2561–70. doi: 10.2147/OPTH.S261318
91. Amico, C, Tornetta, T, Scifo, C, and Blanco, AR. Antioxidant effect of 0.2% xanthan gum in ocular surface corneal epithelial cells. Curr Eye Res. (2015) 40:72–6. doi: 10.3109/02713683.2014.914542
92. Llamas-Moreno, JF, Baiza-Duran, LM, Saucedo-Rodriguez, LR, and Alaniz-De la, OJ. Efficacy and safety of chondroitin sulfate/xanthan gum versus polyethylene glycol/propylene glycol/hydroxypropyl guar in patients with dry eye. Clin Ophthalmol. (2013) 7:995–9. doi: 10.2147/OPTH.S46337
93. Perez-Balbuena, AL, Ochoa-Tabares, JC, Belalcazar-Rey, S, Urzua-Salinas, C, Saucedo-Rodriguez, LR, Velasco-Ramos, R, et al. Efficacy of a fixed combination of 0.09% xanthan gum/0.1% chondroitin sulfate preservative free vs polyethylene glycol/propylene glycol in subjects with dry eye disease: a multicenter randomized controlled trial. BMC Ophthalmol. (2016) 16:164. doi: 10.1186/s12886-016-0343-9
94. Fogagnolo, P, Quisisana, C, Caretti, A, Marchina, D, Dei Cas, M, Melardi, E, et al. Efficacy and safety of Visu Evo((R)) and Cationorm((R)) for the treatment of evaporative and non-evaporative dry eye disease: a multicenter, double-blind, cross-over, Randomized Clinical Trial. Clin Ophthalmol. (2020) 14:1651–63. doi: 10.2147/OPTH.S258081
95. Garrigue, JS, Amrane, M, Faure, MO, Holopainen, JM, and Tong, L. Relevance of lipid-based products in the Management of dry eye Disease. J Ocul Pharmacol Ther. (2017) 33:647–61. doi: 10.1089/jop.2017.0052
96. Simmons, PA, Carlisle-Wilcox, C, Chen, R, Liu, H, and Vehige, JG. Efficacy, safety, and acceptability of a lipid-based artificial tear formulation: a randomized, controlled, multicenter clinical trial. Clin Ther. (2015) 37:858–68. doi: 10.1016/j.clinthera.2015.01.001
97. Lim, P, Han, TA, and Tong, L. Short-term changes in tear lipid layer thickness after instillation of lipid containing eye drops. Transl Vis Sci Technol. (2020) 9:29. doi: 10.1167/tvst.9.8.29
98. Lee, SY, and Tong, L. Lipid-containing lubricants for dry eye: a systematic review. Optom Vis Sci. (2012) 89:1654–61. doi: 10.1097/OPX.0b013e31826f32e0
99. Chung, SH, Lim, SA, and Tchach, H. Efficacy and safety of Carbomer-based lipid-containing artificial tear formulations in patients with dry eye syndrome. Cornea. (2016) 35:181–6. doi: 10.1097/ICO.0000000000000660
100. Baudouin, C, Galarreta, DJ, Mrukwa-Kominek, E, Bohringer, D, Maurino, V, Guillon, M, et al. Clinical evaluation of an oil-based lubricant eyedrop in dry eye patients with lipid deficiency. Eur J Ophthalmol. (2017) 27:122–8. doi: 10.5301/ejo.5000883
101. Jerkins, G, Greiner, JV, Tong, L, Tan, J, Tauber, J, Mearza, A, et al. A comparison of efficacy and safety of two lipid-based lubricant eye drops for the management of evaporative dry eye disease. Clin Ophthalmol. (2020) 14:1665–73. doi: 10.2147/OPTH.S256351
102. Downie, LE, Hom, MM, Berdy, GJ, El-Harazi, S, Verachtert, A, Tan, J, et al. An artificial tear containing flaxseed oil for treating dry eye disease: a randomized controlled trial. Ocul Surf. (2020) 18:148–57. doi: 10.1016/j.jtos.2019.11.004
103. Baudouin, C, Cochener, B, Pisella, PJ, Girard, B, Pouliquen, P, Cooper, H, et al. Randomized, phase III study comparing osmoprotective carboxymethylcellulose with sodium hyaluronate in dry eye disease. Eur J Ophthalmol. (2012) 22:751–61. doi: 10.5301/ejo.5000117
104. Lievens, C, Berdy, G, Douglass, D, Montaquila, S, Lin, H, Simmons, P, et al. Evaluation of an enhanced viscosity artificial tear for moderate to severe dry eye disease: a multicenter, double-masked, randomized 30-day study. Cont Lens Anterior Eye. (2019) 42:443–9. doi: 10.1016/j.clae.2018.12.003
105. Simmons, PA, Liu, H, Carlisle-Wilcox, C, and Vehige, JG. Efficacy and safety of two new formulations of artificial tears in subjects with dry eye disease: a 3-month, multicenter, active-controlled, randomized trial. Clin Ophthalmol. (2015) 9:665–75. doi: 10.2147/OPTH.S78184
106. Labetoulle, M, Chiambaretta, F, Shirlaw, A, Leaback, R, and Baudouin, C. Osmoprotectants, carboxymethylcellulose and hyaluronic acid multi-ingredient eye drop: a randomised controlled trial in moderate to severe dry eye. Eye (Lond). (2017) 31:1409–16. doi: 10.1038/eye.2017.73
107. Hazarbassanov, RM, Queiroz-Hazarbassanov, NGT, Barros, JN, and Gomes, JAP. Topical osmoprotectant for the management of postrefractive Surgery-Induced dry eye symptoms: a randomised controlled double-blind trial. J Ophthalmol. (2018) 2018:1–6. doi: 10.1155/2018/4324590
108. Panigrahi, T, Shivakumar, S, Shetty, R, D'Souza, S, Nelson, EJR, Sethu, S, et al. Trehalose augments autophagy to mitigate stress induced inflammation in human corneal cells. Ocul Surf. (2019) 17:699–713. doi: 10.1016/j.jtos.2019.08.004
109. Iturriaga, G, Suarez, R, and Nova-Franco, B. Trehalose metabolism: from osmoprotection to signaling. Int J Mol Sci. (2009) 10:3793–810. doi: 10.3390/ijms10093793
110. Luyckx, J, and Baudouin, C. Trehalose: an intriguing disaccharide with potential for medical application in ophthalmology. Clin Ophthalmol. (2011) 5:577–81. doi: 10.2147/OPTH.S18827
111. Chiambaretta, F, Doan, S, Labetoulle, M, Rocher, N, Fekih, LE, Messaoud, R, et al. A randomized, controlled study of the efficacy and safety of a new eyedrop formulation for moderate to severe dry eye syndrome. Eur J Ophthalmol. (2017) 27:1–9. doi: 10.5301/ejo.5000836
112. Baudouin, C, Aragona, P, Messmer, EM, Tomlinson, A, Calonge, M, Boboridis, KG, et al. Role of hyperosmolarity in the pathogenesis and management of dry eye disease: proceedings of the OCEAN group meeting. Ocul Surf. (2013) 11:246–58. doi: 10.1016/j.jtos.2013.07.003
113. Koh, S. Clinical utility of 3% diquafosol ophthalmic solution in the treatment of dry eyes. Clin Ophthalmol. (2015) 9:865–72. doi: 10.2147/OPTH.S69486
114. Tauber, J, Davitt, WF, Bokosky, JE, Nichols, KK, Yerxa, BR, Schaberg, AE, et al. Double-masked, placebo-controlled safety and efficacy trial of diquafosol tetrasodium (INS365) ophthalmic solution for the treatment of dry eye. Cornea. (2004) 1:784–92. doi: 10.1097/01.ico.0000133993.14768.a9
115. Matsumoto, Y, Ohashi, Y, Watanabe, H, and Tsubota, K. Diquafosol ophthalmic solution phase 2 study G. Efficacy and safety of diquafosol ophthalmic solution in patients with dry eye syndrome: a Japanese phase 2 clinical trial. Ophthalmology. (2012) 119:1954–60. doi: 10.1016/j.ophtha.2012.04.010
116. Kamiya, K, Nakanishi, M, Ishii, R, Kobashi, H, Igarashi, A, Sato, N, et al. Clinical evaluation of the additive effect of diquafosol tetrasodium on sodium hyaluronate monotherapy in patients with dry eye syndrome: a prospective, randomized, multicenter study. Eye (Lond). (2012) 26:1363–8. doi: 10.1038/eye.2012.166
117. Gong, L, Sun, X, Ma, Z, Wang, Q, Xu, X, Chen, X, et al. A randomised, parallel-group comparison study of diquafosol ophthalmic solution in patients with dry eye in China and Singapore. Br J Ophthalmol. (2015) 99:903–8. doi: 10.1136/bjophthalmol-2014-306084
118. Shigeyasu, C, Yamada, M, Akune, Y, and Tsubota, K. Diquafosol sodium ophthalmic solution for the treatment of dry eye: clinical evaluation and biochemical analysis of tear composition. Jpn J Ophthalmol. (2015) 59:415–20. doi: 10.1007/s10384-015-0408-y
119. Utsunomiya, T, Kawahara, A, Hanada, K, and Yoshida, A. Effects of diquafosol ophthalmic solution on quality of life in dry eye assessed using the dry eye-related quality-of-life score questionnaire: effectiveness in patients while reading and using visual display terminals. Cornea. (2017) 36:908–14. doi: 10.1097/ICO.0000000000001241
120. Koh, S, Ikeda, C, Takai, Y, Watanabe, H, Maeda, N, and Nishida, K. Long-term results of treatment with diquafosol ophthalmic solution for aqueous-deficient dry eye. Jpn J Ophthalmol. (2013) 57:440–6. doi: 10.1007/s10384-013-0251-y
121. Yokoi, N, Sonomura, Y, Kato, H, Komuro, A, and Kinoshita, S. Three percent diquafosol ophthalmic solution as an additional therapy to existing artificial tears with steroids for dry-eye patients with Sjogren's syndrome. Eye (Lond). (2015) 29:1204–12. doi: 10.1038/eye.2015.125
122. Toda, I, Ide, T, Fukumoto, T, Ichihashi, Y, and Tsubota, K. Combination therapy with diquafosol tetrasodium and sodium hyaluronate in patients with dry eye after laser in situ keratomileusis. Am J Ophthalmol. (2014) 157:616–622.e1. doi: 10.1016/j.ajo.2013.11.017
123. Mori, Y, Nejima, R, Masuda, A, Maruyama, Y, Minami, K, Miyata, K, et al. Effect of diquafosol tetrasodium eye drop for persistent dry eye after laser in situ keratomileusis. Cornea. (2014) 33:659–62. doi: 10.1097/ICO.0000000000000136
124. Baek, J, Doh, SH, and Chung, SK. The effect of topical diquafosol tetrasodium 3% on dry eye after cataract surgery. Curr Eye Res. (2016) 41:1281–5. doi: 10.3109/02713683.2015.1122813
125. Shigeyasu, C, Yamada, M, Akune, Y, and Fukui, M. Diquafosol for soft contact Lens dryness: clinical evaluation and tear analysis. Optom Vis Sci. (2016) 93:973–8. doi: 10.1097/OPX.0000000000000877
126. Jongkhajornpong, P, Anothaisintawee, T, Lekhanont, K, Numthavaj, P, McKay, G, Attia, J, et al. Short-term efficacy and safety of biological tear substitutes and topical Secretagogues for dry eye disease: a systematic review and network Meta-analysis. Cornea. (2022) 41:1137–49. doi: 10.1097/ICO.0000000000002943
127. Eom, Y, and Kim, HM. Clinical effectiveness of diquafosol ophthalmic solution 3% in Korean patients with dry eye disease: a multicenter prospective observational study. Int J Ophthalmol. (2021) 14:1518–26. doi: 10.18240/ijo.2021.10.07
128. Ohashi, Y, Munesue, M, Shimazaki, J, Takamura, E, Yokoi, N, Watanabe, H, et al. Long-term safety and effectiveness of diquafosol for the treatment of dry eye in a real-world setting: a prospective observational study. Adv Ther. (2020) 37:707–17. doi: 10.1007/s12325-019-01188-x
129. Urashima, H, Okamoto, T, Takeji, Y, Shinohara, H, and Fujisawa, S. Rebamipide increases the amount of mucin-like substances on the conjunctiva and cornea in the N-acetylcysteine-treated in vivo model. Cornea. (2004) 23:613–9. doi: 10.1097/01.ico.0000126436.25751.fb
130. Kinoshita, S, Awamura, S, Oshiden, K, Nakamichi, N, Suzuki, H, Yokoi, N, et al. Rebamipide (OPC-12759) in the treatment of dry eye: a randomized, double-masked, multicenter, placebo-controlled phase II study. Ophthalmology. (2012) 119:2471–8. doi: 10.1016/j.ophtha.2012.06.052
131. Kinoshita, S, Oshiden, K, Awamura, S, Suzuki, H, Nakamichi, N, Yokoi, N, et al. A randomized, multicenter phase 3 study comparing 2% rebamipide (OPC-12759) with 0.1% sodium hyaluronate in the treatment of dry eye. Ophthalmology. (2013) 120:1158–65. doi: 10.1016/j.ophtha.2012.12.022
132. Kinoshita, S, Awamura, S, Nakamichi, N, Suzuki, H, Oshiden, K, Yokoi, N, et al. A multicenter, open-label, 52-week study of 2% rebamipide (OPC-12759) ophthalmic suspension in patients with dry eye. Am J Ophthalmol. (2014) 157:576–583.e1. doi: 10.1016/j.ajo.2013.11.010
133. Igarashi, T, Fujita, M, Yamada, Y, Kobayashi, M, Fujimoto, C, Takahashi, H, et al. Improvements in signs and symptoms of dry eye after instillation of 2% rebamipide. J Nippon Med Sch. (2015) 82:229–36. doi: 10.1272/jnms.82.229
134. Shrivastava, S, Patkar, P, Ramakrishnan, R, Kanhere, M, and Riaz, Z. Efficacy of rebamipide 2% ophthalmic solution in the treatment of dry eyes. Oman J Ophthalmol. (2018) 11:207–12. doi: 10.4103/ojo.OJO_29_2017
135. Simsek, C, Dogru, M, Shinzawa, M, Den, S, Kojima, T, Iseda, H, et al. The efficacy of 2% topical Rebamipide on conjunctival squamous metaplasia and goblet cell density in dry eye disease. J Ocul Pharmacol Ther. (2019) 35:350–8. doi: 10.1089/jop.2018.0130
136. Igarashi, T, Kobayashi, M, Yaguchi, C, Fujimoto, C, Suzuki, H, and Takahashi, H. Efficacy of Rebamipide instillation for contact Lens discomfort with dry eye. Eye Contact Lens. (2018) 44:S137–42. doi: 10.1097/ICL.0000000000000438
137. Sakane, Y, Yamaguchi, M, and Shiraishi, A. Retrospective observational study on Rebamipide ophthalmic suspension on quality of life of dry eye disease patients. J Ophthalmol. (2019) 2019:1–8. doi: 10.1155/2019/8145731
138. Sacchetti, M, Lambiase, A, Schmidl, D, Schmetterer, L, Ferrari, M, Mantelli, F, et al. Effect of recombinant human nerve growth factor eye drops in patients with dry eye: a phase IIa, open label, multiple-dose study. Br J Ophthalmol. (2020) 104:127–35. doi: 10.1136/bjophthalmol-2018-312470
139. Shimazaki, J, Seika, D, Saga, M, Fukagawa, K, Sakata, M, Iwasaki, M, et al. A prospective, randomized trial of two mucin Secretogogues for the treatment of dry eye syndrome in office workers. Sci Rep. (2017) 7:15210. doi: 10.1038/s41598-017-13121-9
140. Pflugfelder, SC. Anti-inflammatory therapy of dry eye. Ocul Surf. (2003) 1:31–6. doi: 10.1016/S1542-0124(12)70005-8
141. Jones, L, Downie, LE, Korb, D, Benitez-Del-Castillo, JM, Dana, R, Deng, SX, et al. TFOS DEWS II management and therapy report. Ocul Surf. (2017) 15:575–628. doi: 10.1016/j.jtos.2017.05.006
142. Abidi, A, Shukla, P, and Ahmad, A. Lifitegrast: a novel drug for treatment of dry eye disease. J Pharmacol Pharmacother. (2016) 7:194–8. doi: 10.4103/0976-500X.195920
143. el Asrar, AM, Tabbara, KF, Geboes, K, Missotten, L, and Desmet, V. An immunohistochemical study of topical cyclosporine in vernal keratoconjunctivitis. Am J Ophthalmol. (1996) 121:156–61. doi: 10.1016/S0002-9394(14)70579-3
144. Sall, K, Stevenson, OD, Mundorf, TK, and Reis, BL. Two multicenter, randomized studies of the efficacy and safety of cyclosporine ophthalmic emulsion in moderate to severe dry eye disease. CsA phase 3 study group. Ophthalmology. (2000) 107:631–9. doi: 10.1016/S0161-6420(99)00176-1
145. Stevenson, D, Tauber, J, and Reis, BL. Efficacy and safety of cyclosporin a ophthalmic emulsion in the treatment of moderate-to-severe dry eye disease: a dose-ranging, randomized trial. The Cyclosporin a phase 2 study group. Ophthalmology. (2000) 107:967–74. doi: 10.1016/S0161-6420(00)00035-X
146. Straub, M, Bron, AM, Muselier-Mathieu, A, and Creuzot-Garcher, C. Long-term outcome after topical ciclosporin in severe dry eye disease with a 10-year follow-up. Br J Ophthalmol. (2016) 100:1547–50. doi: 10.1136/bjophthalmol-2015-306930
147. Deveci, H, and Kobak, S. The efficacy of topical 0.05% cyclosporine a in patients with dry eye disease associated with Sjogren's syndrome. Int Ophthalmol. (2014) 34:1043–8. doi: 10.1007/s10792-014-9901-4
148. Kang, MJ, Kim, YH, Chou, M, Hwang, J, Cheon, EJ, Lee, HJ, et al. Evaluation of the efficacy and safety of a novel 0.05% Cyclosporin a topical Nanoemulsion in primary Sjogren's syndrome dry eye. Ocul Immunol Inflamm. (2020) 28:370–8. doi: 10.1080/09273948.2019.1587470
149. Mullick, R, Annavajjhala, S, Thakur, P, Mohapatra, A, Shetty, R, and D'Souza, S. Efficacy of topical cyclosporine 0.05% and osmoprotective lubricating eye drops in treating dry eye disease and inflammation. Indian J Ophthalmol. (2021) 69:3473–7. doi: 10.4103/ijo.IJO_3822_20
150. Tuan, HI, Chi, SC, and Kang, YN. An updated systematic review with Meta-analysis of randomized trials on topical Cyclosporin a for dry-eye disease. Drug Des Devel Ther. (2020) 14:265–74. doi: 10.2147/DDDT.S207743
151. Semba, CP, and Gadek, TR. Development of lifitegrast: a novel T-cell inhibitor for the treatment of dry eye disease. Clin Ophthalmol. (2016) 10:1083–94. doi: 10.2147/OPTH.S110557
152. Semba, CP, Torkildsen, GL, Lonsdale, JD, McLaurin, EB, Geffin, JA, Mundorf, TK, et al. A phase 2 randomized, double-masked, placebo-controlled study of a novel integrin antagonist (SAR 1118) for the treatment of dry eye. Am J Ophthalmol. (2012) 153:1050–1060.e1. doi: 10.1016/j.ajo.2011.11.003
153. Sheppard, JD, Torkildsen, GL, Lonsdale, JD, D'Ambrosio, FA Jr, McLaurin, EB, Eiferman, RA, et al. Lifitegrast ophthalmic solution 5.0% for treatment of dry eye disease: results of the OPUS-1 phase 3 study. Ophthalmology. (2014) 121:475–83. doi: 10.1016/j.ophtha.2013.09.015
154. Tauber, J, Karpecki, P, Latkany, R, Luchs, J, Martel, J, Sall, K, et al. Lifitegrast ophthalmic solution 5.0% versus placebo for treatment of dry eye disease: results of the randomized phase III OPUS-2 study. Ophthalmology. (2015) 122:2423–31. doi: 10.1016/j.ophtha.2015.08.001
155. Holland, EJ, Luchs, J, Karpecki, PM, Nichols, KK, Jackson, MA, Sall, K, et al. Lifitegrast for the treatment of dry eye disease: results of a phase III, randomized, double-masked, placebo-controlled trial (OPUS-3). Ophthalmology. (2017) 124:53–60. doi: 10.1016/j.ophtha.2016.09.025
156. Li, JX, Tsai, YY, Lai, CT, Li, YL, Wu, YH, and Chiang, CC. Lifitegrast ophthalmic solution 5% is a safe and efficient Eyedrop for dry eye disease: a systematic review and meta-analysis. J Clin Med. (2022) 11:5014. doi: 10.3390/jcm11175014
157. Shen Lee, B, Toyos, M, Karpecki, P, Schiffbauer, J, and Sheppard, J. Selective pharmacologic therapies for dry eye disease treatment: efficacy, tolerability, and safety data review from preclinical studies and pivotal trials. Ophthalmol Ther. (2022) 11:1333–69. doi: 10.1007/s40123-022-00516-9
158. Clark, D, Sheppard, J, and Brady, TC. A randomized double-masked phase 2a trial to evaluate activity and safety of topical ocular Reproxalap, a novel RASP inhibitor, in dry eye disease. J Ocul Pharmacol Ther. (2021) 37:193–9. doi: 10.1089/jop.2020.0087
159. Ralph, RA, Doane, MG, and Dohlman, CH. Clinical experience with a mobile ocular perfusion pump. Arch Ophthalmol. (1975) 93:1039–43. doi: 10.1001/archopht.1975.01010020815015
160. Katsakoulas, I, Lougovoi, C, Paraskevopoulou, P, and Vougioukas, N. Protocol of blood serum eye drops. Int J Pharm Compd. (2015) 19:252–60.
161. Lagnado, R, King, AJ, Donald, F, and Dua, HS. A protocol for low contamination risk of autologous serum drops in the management of ocular surface disorders. Br J Ophthalmol. (2004) 88:464–5. doi: 10.1136/bjo.2003.025528
162. Bradley, JC, Bradley, RH, McCartney, DL, and Mannis, MJ. Serum growth factor analysis in dry eye syndrome. Clin Experiment Ophthalmol. (2008) 36:717–20. doi: 10.1111/j.1442-9071.2008.01895.x
163. Tsubota, K, Goto, E, Fujita, H, Ono, M, Inoue, H, Saito, I, et al. Treatment of dry eye by autologous serum application in Sjogren's syndrome. Br J Ophthalmol. (1999) 83:390–5. doi: 10.1136/bjo.83.4.390
164. Nelson, JD, and Gordon, JF. Topical fibronectin in the treatment of keratoconjunctivitis sicca. Chiron Keratoconjunctivitis Sicca Study Group. Am J Ophthalmol. (1992) 114:441–7. doi: 10.1016/S0002-9394(14)71856-2
165. Franchini, M, Cruciani, M, Mengoli, C, Marano, G, Capuzzo, E, Pati, I, et al. Serum eye drops for the treatment of ocular surface diseases: a systematic review and meta-analysis. Blood Transfus. (2019) 17:200–9. doi: 10.2450/2019.0080-19
166. Creuzot-Garcher, C, Lafontaine, PO, Brignole, F, Pisella, PJ, d'Athis, P, Bron, A, et al. Treating severe dry eye syndromes with autologous serum. J Fr Ophtalmol. (2004) 27:346–51. doi: 10.1016/S0181-5512(04)96139-6
167. Kojima, T, Ishida, R, Dogru, M, Goto, E, Matsumoto, Y, Kaido, M, et al. The effect of autologous serum eyedrops in the treatment of severe dry eye disease: a prospective randomized case-control study. Am J Ophthalmol. (2005) 139:242–6. doi: 10.1016/j.ajo.2004.08.040
168. Urzua, CA, Vasquez, DH, Huidobro, A, Hernandez, H, and Alfaro, J. Randomized double-blind clinical trial of autologous serum versus artificial tears in dry eye syndrome. Curr Eye Res. (2012) 37:684–8. doi: 10.3109/02713683.2012.674609
169. Cho, YK, Huang, W, Kim, GY, and Lim, BS. Comparison of autologous serum eye drops with different diluents. Curr Eye Res. (2013) 38:9–17. doi: 10.3109/02713683.2012.720340
170. Rocha, EM, Pelegrino, FS, de Paiva, CS, Vigorito, AC, and de Souza, CA. GVHD dry eyes treated with autologous serum tears. Bone Marrow Transplant. (2000) 25:1101–3. doi: 10.1038/sj.bmt.1702334
171. Ogawa, Y, Okamoto, S, Mori, T, Yamada, M, Mashima, Y, Watanabe, R, et al. Autologous serum eye drops for the treatment of severe dry eye in patients with chronic graft-versus-host disease. Bone Marrow Transplant. (2003) 31:579–83. doi: 10.1038/sj.bmt.1703862
172. Pan, Q, Angelina, A, Marrone, M, Stark, WJ, and Akpek, EK. Autologous serum eye drops for dry eye. Cochrane Database Syst Rev. (2017) 2017:CD009327. doi: 10.1002/14651858.CD009327.pub3
173. Berhuni, M, Istek, S, and Tiskaoglu, NS. 20% autologous serum vs. 0.05% cyclosporine and preservative-free artificial tears in the treatment of Sjogren related dry eye. Arq Bras Oftalmol. (2022) 87:S0004-27492022005011217. doi: 10.5935/0004-2749.2022-0192
174. Hassan, A, Balal, S, Cook, E, Dehbi, HM, Pardhan, S, Bourne, R, et al. Finger-prick autologous blood (FAB) eye drops for dry eye disease: single masked multi-Centre randomised controlled trial. Clin Ophthalmol. (2022) 16:3973–9. doi: 10.2147/OPTH.S384586
175. Erikitola, OO, Williams, O, Fern, A, and Lyall, D. Fingerprick autologous blood in the treatment of severe dry eyes and ocular surface disease. Cornea. (2021) 40:1104–9. doi: 10.1097/ICO.0000000000002624
176. van der Meer, PF, Verbakel, SK, Honohan, A, Lorinser, J, Thurlings, RM, Jacobs, JFM, et al. Allogeneic and autologous serum eye drops: a pilot double-blind randomized crossover trial. Acta Ophthalmol. (2021) 99:837–42. doi: 10.1111/aos.14788
177. Rodriguez Calvo-de-Mora, M, Dominguez-Ruiz, C, Barrero-Sojo, F, Rodriguez-Moreno, G, Antunez Rodriguez, C, Ponce Verdugo, L, et al. Autologous versus allogeneic versus umbilical cord sera for the treatment of severe dry eye disease: a double-blind randomized clinical trial. Acta Ophthalmol. (2022) 100:e396–408. doi: 10.1111/aos.14953
178. Kan, J, Wang, M, Liu, Y, Liu, H, Chen, L, Zhang, X, et al. A novel botanical formula improves eye fatigue and dry eye: a randomized, double-blind, placebo-controlled study. Am J Clin Nutr. (2020) 112:334–42. doi: 10.1093/ajcn/nqaa139
179. Barnard, NA. Punctal and intracanalicular occlusion—a guide for the practitioner. Ophthalmic Physiol Opt. (1996) 16:S15–22. doi: 10.1016/0275-5408(95)00135-2
180. Altan-Yaycioglu, R, Gencoglu, EA, Akova, YA, Dursun, D, Cengiz, F, and Akman, A. Silicone versus collagen plugs for treating dry eye: results of a prospective randomized trial including lacrimal scintigraphy. Am J Ophthalmol. (2005) 140:88–93. doi: 10.1016/j.ajo.2005.02.031
181. Nava-Castaneda, A, Tovilla-Canales, JL, Rodriguez, L, Tovilla, YPJL, and Jones, CE. Effects of lacrimal occlusion with collagen and silicone plugs on patients with conjunctivitis associated with dry eye. Cornea. (2003) 22:10–4. doi: 10.1097/00003226-200301000-00003
182. Said, AM, Farag, ME, Abdulla, TM, Ziko, OA, and Osman, WM. Corneal sensitivity, ocular surface health and tear film stability after punctal plug therapy of aqueous deficient dry eye. Int J Ophthalmol. (2016) 9:1598–607. doi: 10.18240/ijo.2016.11.10
183. Geldis, JR, and Nichols, JJ. The impact of punctal occlusion on soft contact lens wearing comfort and the tear film. Eye Contact Lens. (2008) 34:261–5. doi: 10.1097/ICL.0b013e31817fa604
184. Alfawaz, AM, Algehedan, S, Jastaneiah, SS, Al-Mansouri, S, Mousa, A, and Al-Assiri, A. Efficacy of punctal occlusion in management of dry eyes after laser in situ keratomileusis for myopia. Curr Eye Res. (2014) 39:257–62. doi: 10.3109/02713683.2013.841258
185. Yung, YH, Toda, I, Sakai, C, Yoshida, A, and Tsubota, K. Punctal plugs for treatment of post-LASIK dry eye. Jpn J Ophthalmol. (2012) 56:208–13. doi: 10.1007/s10384-012-0125-8
186. Lin, T, Wang, W, Lu, Y, and Gong, L. Treatment of dry eye with Intracanalicular injection of Hydroxybutyl chitosan: a prospective randomized clinical trial. Front Med (Lausanne). (2021) 8:769448. doi: 10.3389/fmed.2021.769448
187. Burgess, PI, Koay, P, and Clark, P. Smart plug versus silicone punctal plug therapy for dry eye: a prospective randomized trial. Cornea. (2008) 27:391–4. doi: 10.1097/ICO.0b013e318160d030
188. Slusser, TG, and Lowther, GE. Effects of lacrimal drainage occlusion with nondissolvable intracanalicular plugs on hydrogel contact lens wear. Optom Vis Sci. (1998) 75:330–8. doi: 10.1097/00006324-199805000-00022
189. Ervin, AM, Law, A, and Pucker, AD. Punctal occlusion for dry eye syndrome. Cochrane Database Syst Rev. (2017) 2017:CD006775. doi: 10.1002/14651858.CD006775.pub3
190. Sahlin, S, Chen, E, Kaugesaar, T, Almqvist, H, Kjellberg, K, and Lennerstrand, G. Effect of eyelid botulinum toxin injection on lacrimal drainage. Am J Ophthalmol. (2000) 129:481–6. doi: 10.1016/S0002-9394(99)00408-0
191. Serna-Ojeda, JC, and Nava-Castaneda, A. Paralysis of the orbicularis muscle of the eye using botulinum toxin type a in the treatment for dry eye. Acta Ophthalmol. (2017) 95:e132–7. doi: 10.1111/aos.13140
192. Choi, MG, Yeo, JH, Kang, JW, Chun, YS, Lee, JK, and Kim, JC. Effects of botulinum toxin type a on the treatment of dry eye disease and tear cytokines. Graefes Arch Clin Exp Ophthalmol. (2019) 257:331–8. doi: 10.1007/s00417-018-4194-3
193. Alsuhaibani, AH, and Eid, SA. Botulinum toxin injection and tear production. Curr Opin Ophthalmol. (2018) 29:428–33. doi: 10.1097/ICU.0000000000000506
194. Diaz, AL, Chaparro, TA, Tello, A, Coy, H, Frederick, GA, and Parra, MM. Application of botulinum toxin in Horner's muscle for the treatment of dry eye. Arch Soc Esp Oftalmol (Engl Ed). (2018) 93:617–20. doi: 10.1016/j.oftal.2018.04.013
195. Finis, D, Hayajneh, J, Konig, C, Borrelli, M, Schrader, S, and Geerling, G. Evaluation of an automated thermodynamic treatment (Lipi flow (R)) system for meibomian gland dysfunction: a prospective, randomized, observer-masked trial. Ocul Surf. (2014) 12:146–54. doi: 10.1016/j.jtos.2013.12.001
196. Godin, MR, Stinnett, SS, and Gupta, PK. Outcomes of thermal pulsation treatment for dry eye syndrome in patients with Sjogren disease. Cornea. (2018) 37:1155–8. doi: 10.1097/ICO.0000000000001621
197. Greiner, JV. A single Lipi flow(R) thermal pulsation system treatment improves meibomian gland function and reduces dry eye symptoms for 9 months. Curr Eye Res. (2012) 37:272–8. doi: 10.3109/02713683.2011.631721
198. Greiner, JV. Long-term (12-month) improvement in meibomian gland function and reduced dry eye symptoms with a single thermal pulsation treatment. Clin Experiment Ophthalmol. (2013) 41:524–30. doi: 10.1111/ceo.12033
199. Greiner, JV. Long-term (3 year) effects of a single thermal pulsation system treatment on Meibomian gland function and dry eye symptoms. Eye Contact Lens. (2016) 42:99–107. doi: 10.1097/ICL.0000000000000166
200. Kim, MJ, Stinnett, SS, and Gupta, PK. Effect of thermal pulsation treatment on tear film parameters in dry eye disease patients. Clin Ophthalmol. (2017) 11:883–6. doi: 10.2147/OPTH.S136203
201. Zhao, Y, Veerappan, A, Yeo, S, Rooney, DM, Acharya, RU, Tan, JH, et al. Clinical trial of thermal pulsation (Lipi flow) in Meibomian gland dysfunction with Preteatment Meibography. Eye Contact Lens. (2016) 42:339–46. doi: 10.1097/ICL.0000000000000228
202. Hura, AS, Epitropoulos, AT, Czyz, CN, and Rosenberg, ED. Visible Meibomian gland structure increases after vectored thermal pulsation treatment in dry eye disease patients with Meibomian gland dysfunction. Clin Ophthalmol. (2020) 14:4287–96. doi: 10.2147/OPTH.S282081
203. Meng, Z, Chu, X, Zhang, C, Liu, H, Yang, R, Huang, Y, et al. Efficacy and safety evaluation of a single thermal pulsation system treatment (Lipiflow((R))) on meibomian gland dysfunction: a randomized controlled clinical trial. Int Ophthalmol. (2023) 43:1175–84. doi: 10.1007/s10792-022-02516-x
204. Hagen, KB, Bedi, R, Blackie, CA, and Christenson-Akagi, KJ. Comparison of a single-dose vectored thermal pulsation procedure with a 3-month course of daily oral doxycycline for moderate-to-severe meibomian gland dysfunction. Clin Ophthalmol. (2018) 12:161–8. doi: 10.2147/OPTH.S150433
205. Schallhorn, CS, Schallhorn, JM, Hannan, S, and Schallhorn, SC. Effectiveness of an eyelid thermal pulsation procedure to treat recalcitrant dry eye symptoms after laser vision correction. J Refract Surg. (2017) 33:30–6. doi: 10.3928/1081597X-20161006-05
206. Lam, PY, Shih, KC, Fong, PY, Chan, TCY, Ng, AL, Jhanji, V, et al. A review on evidence-based treatments for Meibomian gland dysfunction. Eye Contact Lens. (2020) 46:3–16. doi: 10.1097/ICL.0000000000000680
207. Schanzlin, D, Owen, JP, Klein, S, Yeh, TN, Merchea, MM, and Bullimore, MA. Efficacy of the Systane iLux thermal pulsation system for the treatment of Meibomian gland dysfunction after 1 week and 1 month: a prospective study. Eye Contact Lens. (2022) 48:155–61. doi: 10.1097/ICL.0000000000000847
208. Wesley, G, Bickle, K, Downing, J, Fisher, B, Greene, B, Heinrich, C, et al. Systane iLux thermal pulsation system in the treatment of Meibomian gland dysfunction: a post-hoc analysis of a 12-month, randomized, multicenter study. Clin Ophthalmol. (2022) 16:3631–40. doi: 10.2147/OPTH.S379484
209. Wesley, G, Bickle, K, Downing, J, Fisher, B, Greene, B, Heinrich, C, et al. Comparison of two thermal pulsation Systems in the Treatment of Meibomian gland dysfunction: a randomized, multicenter study. Optom Vis Sci. (2022) 99:323–32. doi: 10.1097/OPX.0000000000001892
210. Tauber, J. A 6-week, prospective, randomized, single-masked study of Lifitegrast ophthalmic solution 5% versus thermal pulsation procedure for treatment of inflammatory Meibomian gland dysfunction. Cornea. (2020) 39:403–7. doi: 10.1097/ICO.0000000000002235
211. Choi, M, Han, SJ, Ji, YW, Choi, YJ, Jun, I, Alotaibi, MH, et al. Meibum expressibility improvement as a therapeutic target of intense pulsed light treatment in Meibomian gland dysfunction and its association with tear inflammatory cytokines. Sci Rep. (2019) 9:7648. doi: 10.1038/s41598-019-44000-0
212. Craig, JP, Chen, YH, and Turnbull, PR. Prospective trial of intense pulsed light for the treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. (2015) 56:1965–70. doi: 10.1167/iovs.14-15764
213. Yurttaser Ocak, S, Karakus, S, Ocak, OB, Cakir, A, Bolukbasi, S, Erden, B, et al. Intense pulse light therapy treatment for refractory dry eye disease due to meibomian gland dysfunction. Int Ophthalmol. (2020) 40:1135–41. doi: 10.1007/s10792-019-01278-3
214. Fan, Q, Pazo, EE, You, Y, Zhang, C, Zhang, C, Xu, L, et al. Subjective quality of vision in evaporative dry eye patients after intense pulsed light. Photobiomodul Photomed Laser Surg. (2020) 38:444–51. doi: 10.1089/photob.2019.4788
215. Karaca, EE, Evren Kemer, O, and Ozek, D. Intense regulated pulse light for the meibomian gland dysfunction. Eur J Ophthalmol. (2020) 30:289–92. doi: 10.1177/1120672118817687
216. Albietz, JM, and Schmid, KL. Intense pulsed light treatment and meibomian gland expression for moderate to advanced meibomian gland dysfunction. Clin Exp Optom. (2018) 101:23–33. doi: 10.1111/cxo.12541
217. Rong, B, Tang, Y, Liu, R, Tu, P, Qiao, J, Song, W, et al. Long-term effects of intense pulsed light combined with Meibomian gland expression in the treatment of Meibomian gland dysfunction. Photomed Laser Surg. (2018) 36:562–7. doi: 10.1089/pho.2018.4499
218. Rong, B, Tang, Y, Tu, P, Liu, R, Qiao, J, Song, W, et al. Intense pulsed light applied directly on eyelids combined with Meibomian gland expression to treat Meibomian gland dysfunction. Photomed Laser Surg. (2018) 36:326–32. doi: 10.1089/pho.2017.4402
219. Arita, R, Fukuoka, S, and Morishige, N. Therapeutic efficacy of intense pulsed light in patients with refractory meibomian gland dysfunction. Ocul Surf. (2019) 17:104–10. doi: 10.1016/j.jtos.2018.11.004
220. Huang, X, Qin, Q, Wang, L, Zheng, J, Lin, L, and Jin, X. Clinical results of Intraductal Meibomian gland probing combined with intense pulsed light in treating patients with refractory obstructive Meibomian gland dysfunction: a randomized controlled trial. BMC Ophthalmol. (2019) 19:211. doi: 10.1186/s12886-019-1219-6
221. Iradier, MT, Del Buey, MA, Peris-Martinez, C, Cedano, P, and Pinero, DP. Characterization and prediction of the clinical outcome of intense pulsed light-based treatment in dry eye associated to Meibomian gland dysfunction. J Clin Med. (2021) 10:3573. doi: 10.3390/jcm10163573
222. Leng, X, Shi, M, Liu, X, Cui, J, Sun, H, and Lu, X. Intense pulsed light for meibomian gland dysfunction: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. (2021) 259:1–10. doi: 10.1007/s00417-020-04834-1
223. Jiang, X, Yuan, H, Zhang, M, Lv, H, Chou, Y, Yang, J, et al. The efficacy and safety of new-generation intense pulsed light in the treatment of Meibomian gland dysfunction-related dry eye: a multicenter, randomized, patients-blind, parallel-control, non-inferiority clinical trial. Ophthalmol Ther. (2022) 11:1895–912. doi: 10.1007/s40123-022-00556-1
224. Yang, L, Pazo, EE, Zhang, Q, Wu, Y, Song, Y, Qin, G, et al. Treatment of contact lens related dry eye with intense pulsed light. Cont Lens Anterior Eye. (2022) 45:101449. doi: 10.1016/j.clae.2021.101449
225. Huo, Y, Wan, Q, Hou, X, Zhang, Z, Zhao, J, Wu, Z, et al. Therapeutic effect of intense pulsed light in patients with Sjogren's syndrome related dry eye. J Clin Med. (2022) 11:1377. doi: 10.3390/jcm11051377
226. Xue, AL, Wang, MTM, Ormonde, SE, and Craig, JP. Randomised double-masked placebo-controlled trial of the cumulative treatment efficacy profile of intense pulsed light therapy for meibomian gland dysfunction. Ocul Surf. (2020) 18:286–97. doi: 10.1016/j.jtos.2020.01.003
227. Singh, S, Basu, S, and Geerling, G. Salivary gland transplantation for dry eye disease: indications, techniques, and outcomes. Ocul Surf. (2022) 26:53–62. doi: 10.1016/j.jtos.2022.07.013
228. Geerling, G, and Sieg, P. Transplantation of the major salivary glands. Dev Ophthalmol. (2008) 41:255–68. doi: 10.1159/000131094
229. Zhang, L, Su, JZ, Cai, ZG, Lv, L, Zou, LH, Liu, XJ, et al. Factors influencing the long-term results of autologous microvascular submandibular gland transplantation for severe dry eye disease. Int J Oral Maxillofac Surg. (2019) 48:40–7. doi: 10.1016/j.ijom.2018.07.006
230. Yu, GY, Zhu, ZH, Mao, C, Cai, ZG, Zou, LH, Lu, L, et al. Microvascular autologous submandibular gland transfer in severe cases of keratoconjunctivitis sicca. Int J Oral Maxillofac Surg. (2004) 33:235–9. doi: 10.1006/ijom.2002.0438
231. Su, JZ, Zheng, B, Liu, XJ, Xie, Z, Sun, D, Cai, ZG, et al. Quality of life and patient satisfaction after submandibular gland transplantation in patients with severe dry eye disease. Ocul Surf. (2019) 17:470–5. doi: 10.1016/j.jtos.2019.04.007
232. Su, JZ, Zheng, B, Wang, Z, Liu, XJ, Cai, ZG, Zhang, L, et al. Submandibular gland transplantation vs minor salivary glands transplantation for treatment of dry eye: a retrospective cohort study. Am J Ophthalmol. (2022) 241:238–47. doi: 10.1016/j.ajo.2022.05.019
233. Vazirani, J, Bhalekar, S, Amescua, G, Singh, S, and Basu, S. Minor salivary gland transplantation for severe dry eye disease due to cicatrising conjunctivitis: multicentre long-term outcomes of a modified technique. Br J Ophthalmol. (2021) 105:1485–90. doi: 10.1136/bjophthalmol-2020-316611
234. Su, JZ, Cai, ZG, and Yu, GY. Microvascular autologous submandibular gland transplantation in severe cases of keratoconjunctivitis sicca. Maxillofac Plast Reconstr Surg. (2015) 37:5. doi: 10.1186/s40902-015-0006-4
235. Wang, DK, Zhang, SE, Su, YX, Zheng, GS, Yang, WF, and Liao, GQ. Microvascular submandibular gland transplantation for severe Keratoconjunctivitis sicca: a single-institution experience of 61 grafts. J Oral Maxillofac Surg. (2018) 76:2443–52. doi: 10.1016/j.joms.2018.05.008
236. Borrelli, M, Schroder, C, Dart, JK, Collin, JR, Sieg, P, Cree, IA, et al. Long-term follow-up after submandibular gland transplantation in severe dry eyes secondary to cicatrizing conjunctivitis. Am J Ophthalmol. (2010) 150:894–904. doi: 10.1016/j.ajo.2010.05.010
237. Schroder, C, Sieg, P, Framme, C, Honnicke, K, Hakim, SG, and Geerling, G. Transplantation of the submandibular gland in absolute dry eyes. Effect on the ocular surface. Klin Monatsbl Augenheilkd. (2002) 219:494–501. doi: 10.1055/s-2002-33582
238. Wakamatsu, TH, Sant'Anna, A, Cristovam, PC, Alves, VAF, Wakamatsu, A, and Gomes, JAP. Minor salivary gland transplantation for severe dry eyes. Cornea. (2017) 36:S26–33. doi: 10.1097/ICO.0000000000001358
239. Bukhari, AA. Botulinum neurotoxin type a versus punctal plug insertion in the management of dry eye disease. Oman J Ophthalmol. (2014) 7:61–5. doi: 10.4103/0974-620X.137142
240. Victoria, AC, and Pino, A. Botulinum toxin type a and its uses in dry eye disease. Plast Reconstr Surg. (2012) 130:209e–10e. doi: 10.1097/PRS.0b013e31825500ba
241. Food and Drug Administration HHS. Medical devices; ophthalmic devices; classification of the eyelid thermal pulsation system. Final rule. Fed Regist. (2011) 76:51876–8.
242. Cote, S, Zhang, AC, Ahmadzai, V, Maleken, A, Li, C, Oppedisano, J, et al. Intense pulsed light (IPL) therapy for the treatment of meibomian gland dysfunction. Cochrane Database Syst Rev. (2020) 3:CD013559. doi: 10.1002/14651858.CD013559
243. Geerling, G, Sieg, P, Bastian, GO, and Laqua, H. Transplantation of the autologous submandibular gland for most severe cases of keratoconjunctivitis sicca. Ophthalmology. (1998) 105:327–35. doi: 10.1016/S0161-6420(98)93406-6
244. Nichols, KK, Bacharach, J, Holland, E, Kislan, T, Shettle, L, Lunacsek, O, et al. Impact of dry eye disease on work productivity, and Patients' satisfaction with over-the-counter dry eye treatments. Invest Ophthalmol Vis Sci. (2016) 57:2975–82. doi: 10.1167/iovs.16-19419
245. Lopez-de la Rosa, A, Pinto-Fraga, J, Blazquez Arauzo, F, Urbano Rodriguez, R, and Gonzalez-Garcia, MJ. Safety and efficacy of an artificial tear containing 0.3% hyaluronic acid in the Management of Moderate-to-Severe dry eye Disease. Eye Contact Lens. (2017) 43:383–8. doi: 10.1097/ICL.0000000000000284
246. Stonecipher, K, Perry, HD, Gross, RH, and Kerney, DL. The impact of topical cyclosporine a emulsion 0.05% on the outcomes of patients with keratoconjunctivitis sicca. Curr Med Res Opin. (2005) 21:1057–63. doi: 10.1185/030079905X50615
247. Trattler, W, Katsev, D, and Kerney, D. Self-reported compliance with topical cyclosporine emulsion 0.05% and onset of the effects of increased tear production as assessed through patient surveys. Clin Ther. (2006) 28:1848–56. doi: 10.1016/j.clinthera.2006.11.016
248. White, DE, Zhao, Y, Jayapalan, H, Machiraju, P, Periyasamy, R, and Ogundele, A. Treatment satisfaction among patients using anti-inflammatory topical medications for dry eye disease. Clin Ophthalmol. (2020) 14:875–83. doi: 10.2147/OPTH.S233194
249. Ames, P, and Galor, A. Cyclosporine ophthalmic emulsions for the treatment of dry eye: a review of the clinical evidence. Clin Investig (Lond). (2015) 5:267–85. doi: 10.4155/cli.14.135
250. Haber, SL, Benson, V, Buckway, CJ, Gonzales, JM, Romanet, D, and Scholes, B. Lifitegrast: a novel drug for patients with dry eye disease. Ther Adv Ophthalmol. (2019) 11:251584141987036. doi: 10.1177/2515841419870366
251. Jirsova, K, Brejchova, K, Krabcova, I, Filipec, M, Al Fakih, A, Palos, M, et al. The application of autologous serum eye drops in severe dry eye patients; subjective and objective parameters before and after treatment. Curr Eye Res. (2014) 39:21–30. doi: 10.3109/02713683.2013.824987
252. Fouda, SM, and Mattout, HK. Comparison between botulinum toxin a injection and lacrimal Punctal plugs for the control of post-LASIK dry eye manifestations: a prospective study. Ophthalmol Ther. (2017) 6:167–74. doi: 10.1007/s40123-017-0079-5
253. Blackie, CA, Coleman, CA, and Holland, EJ. The sustained effect (12 months) of a single-dose vectored thermal pulsation procedure for meibomian gland dysfunction and evaporative dry eye. Clin Ophthalmol. (2016) 10:1385–96. doi: 10.2147/OPTH.S109663
254. Baumann, A, and Cochener, B. Meibomian gland dysfunction: a comparative study of modern treatments. J Fr Ophtalmol. (2014) 37:303–12. doi: 10.1016/j.jfo.2013.12.007
255. Vora, GK, and Gupta, PK. Intense pulsed light therapy for the treatment of evaporative dry eye disease. Curr Opin Ophthalmol. (2015) 26:314–8. doi: 10.1097/ICU.0000000000000166
Keywords: dry eye diseases, quality of life, patient-reported outcomes, treatment, impact
Citation: Lin C-W, Lin M-Y, Huang J-W, Wang T-J and Lin I-C (2024) Impact of dry eye disease treatment on patient quality of life. Front. Med. 11:1305579. doi: 10.3389/fmed.2024.1305579
Edited by:
Yonathan Garfias, National Autonomous University of Mexico, MexicoReviewed by:
Angel Nava-Castañeda, Instituto de Oftalmología Fundación de Asistencia Privada Conde de Valenciana, IAP, MexicoCopyright © 2024 Lin, Lin, Huang, Wang and Lin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: I-Chan Lin, aWNoYW5saW5AZ21haWwuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.