 Hailing Liu
Hailing Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 12 April 2024
Sec. Infectious Diseases: Pathogenesis and Therapy
Volume 11 - 2024 | https://doi.org/10.3389/fmed.2024.1301105
Objective: To analyze the clinical characteristics and correlation of Fournier’s gangrene induced by sodium-glucose cotransporter protein-2 (SGLT-2) inhibitors, providing references for safe clinical drug use.
Methods: The CNKI, WanFang, and PubMed databases were searched, and relevant documents were collected and statistically analyzed. The basic information of patients, drug use information, adverse reactions and outcomes were extracted and analyzed.
Results: A total of 12 patients (8 males and 4 females) were included, with an average age of 55.6 years (ranging from 34 to 72 years). SGLT-2 inhibitors associated with Fournier’s gangrene include empagliflozin (5 cases), dapagliflozin (5 cases), and canagliflozin (2 cases). Among them, 10 cases reported the time of first medication, ranging from 1 month to 6 years for the occurrence of adverse reactions. The most common concomitant drug was metformin (7 cases). Adverse reactions mainly manifested as redness, swelling and pain in the buttocks, perineum, perianal, scrotum and other positions, accompanied by an increased white blood cell count. Following surgery and antibiotic treatment, all patients showed improved.
Conclusion: Fournier’s gangrene induced by SGLT-2 inhibitors is rare. If patients using SGLT-2 inhibitors are suspected of having Fournier’s gangrene, it is recommended to discontinue the drugs immediately and initiate active treatment to ensure clinical safety.
SGLT-2 are common hypoglycemic drugs in clinical practice and are among the cornerstone drugs in the treatment of heart failure. SGLT-2 inhibitors reduce glucose and sodium reabsorption by inhibiting SGLT-2 in the proximal convoluted tubular epithelial cell membrane, thereby excreting large amounts of glucose in the urine (1). However, an increased urinary glucose concentration can elevate the risk of urethral and genital infections (2).
Fournier’s gangrene (FG) is one of the rare but highly progressive adverse reactions. FG, also known as perineal necrotizing fasciitis, can penetrate soft tissue structures and destroy subcutaneous fat and muscle, leading to necrosis of perineal, perianal, and genitourinary areas, and the case fatality rate can be as high as 50% (3). The most common pathogenic cause of FG is infection of adjacent tissues, such as abscesses, anal fissure, and colonic perforation.
In 2018, the Food and Drug Administration (FDA) issued a safety warning on SGLT-2 inhibitors regarding FG in patients with type 2 diabetes. In January 2022, the American Diabetes Association identified 491 cases of FG associated with SGLT-2 inhibitors (3). Despite the issuance of a warning for the risk of FG with SGLT-2 inhibitors, the number of related cases continued to rise (3). Therefore, this study conducted a comprehensive analysis by searching relevant case reports for the reference of clinical users.
Literature search for Fournier’s gangrene caused by SGLT-2 inhibitors included databases such as CNKI, Wanfang, and PubMed. English search terms comprised “Fournier’s gangrene,” “SGLT-2,” “SGLT,” “empagliflozin,” “dapagliflozin,” “canagliflozin,” “ipragliflozin,” “ertugliflozin,” “luseogliflozin,” “ofogliflozin,” and “Sodium-Glucose Cotransporter-2 Inhibitors.” The search was completed as of February 12, 2023.
Inclusion criteria: We collected original case reports of FG caused by SGLT-2 inhibitors.
Exclusion criteria: Reviews, repeated cases, cases where the causal relationship between SGLT-2 inhibitors and FG cannot be determined, and cases lacking full texts were excluded.
Read the included literature in detail and record the patient’s age, gender, Region, chief complaint, past history, white blood cell count (WBC), C-reactive protein, hemoglobin, glycosylated hemoglobin, glucose, bacterial culture, culture sample, treatment process, time of first medication and adverse reaction, outcome and other information.
A total of 24 articles were retrieved, and 12 articles were screened based on the inclusion criteria and exclusion criteria, resulting in a total of 12 cases.
A total of 12 patients were included, including 8 men and 4 women, with a median age of 55.6 years (range 34–72) (Table 1). Among them, 5 patients were treated with empagliflozin, 5 with dapagliflozin, and 2 with canagliflozin. Ten patients reported the time of first medication, with the shortest duration being 1 month and the longest 5 years, occurring more than 6 months after medication. Five patients reported the specific dosage of SGLT-2 inhibitors, including empagliflozin at dose of 10 mg, 12.5 mg, and 25 mg/d, dapagliflozin at 10 mg/d, and canagliflozin at 100 mg/d. Following treatment, all patients showed improvement.
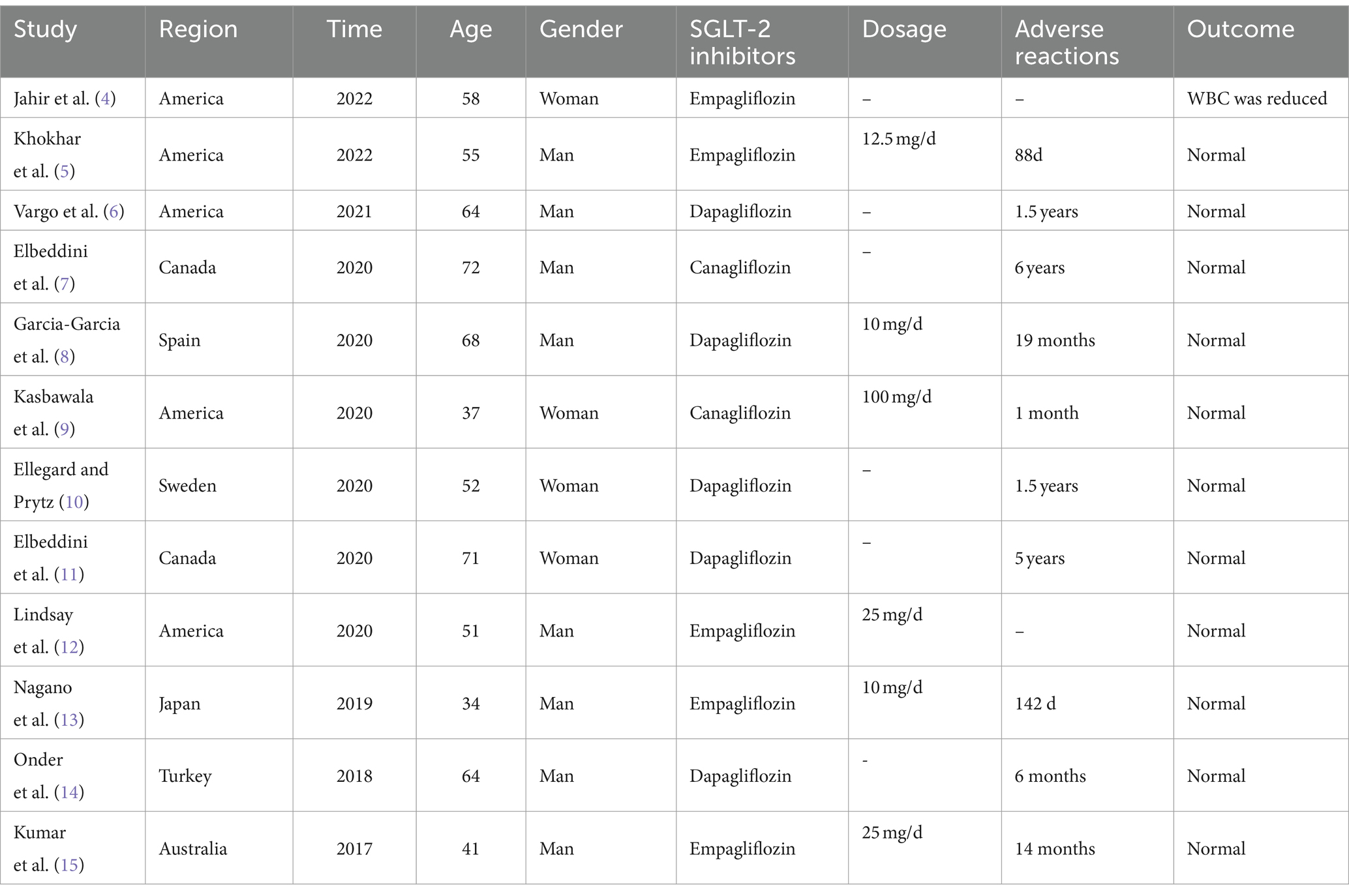
Table 1. The basic information of the 12 included patients.
The main manifestations of adverse reactions include redness and pain in the buttocks, perineum, perianal, scrotum, and other positions, accompanied by an increase in white blood cell count (Tables 2, 3). Pain affects sleep and may even lead to fever, requiring timely intervention and treatment.
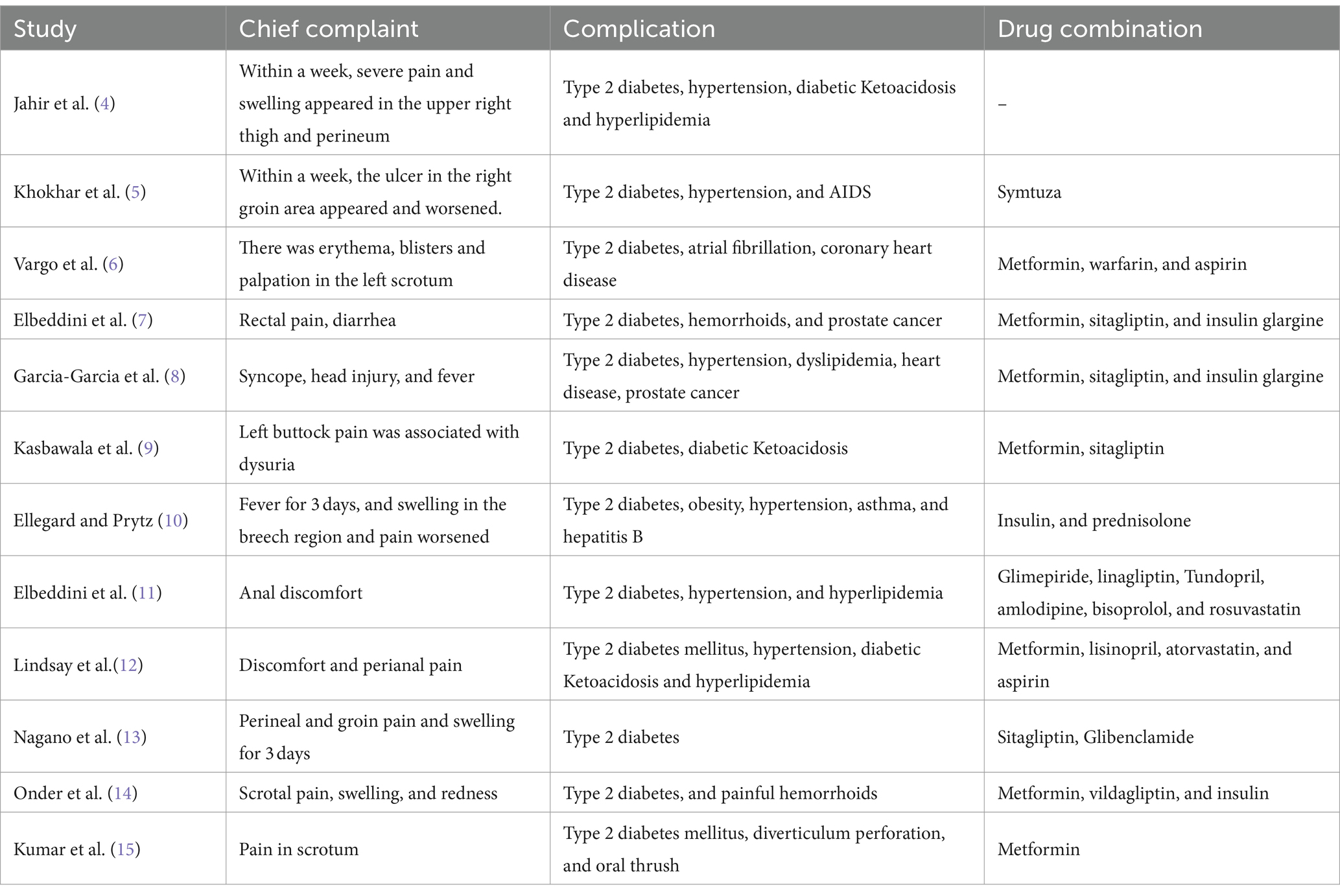
Table 2. Chief complaint, complications, and drug combinations of the 12 included patients.
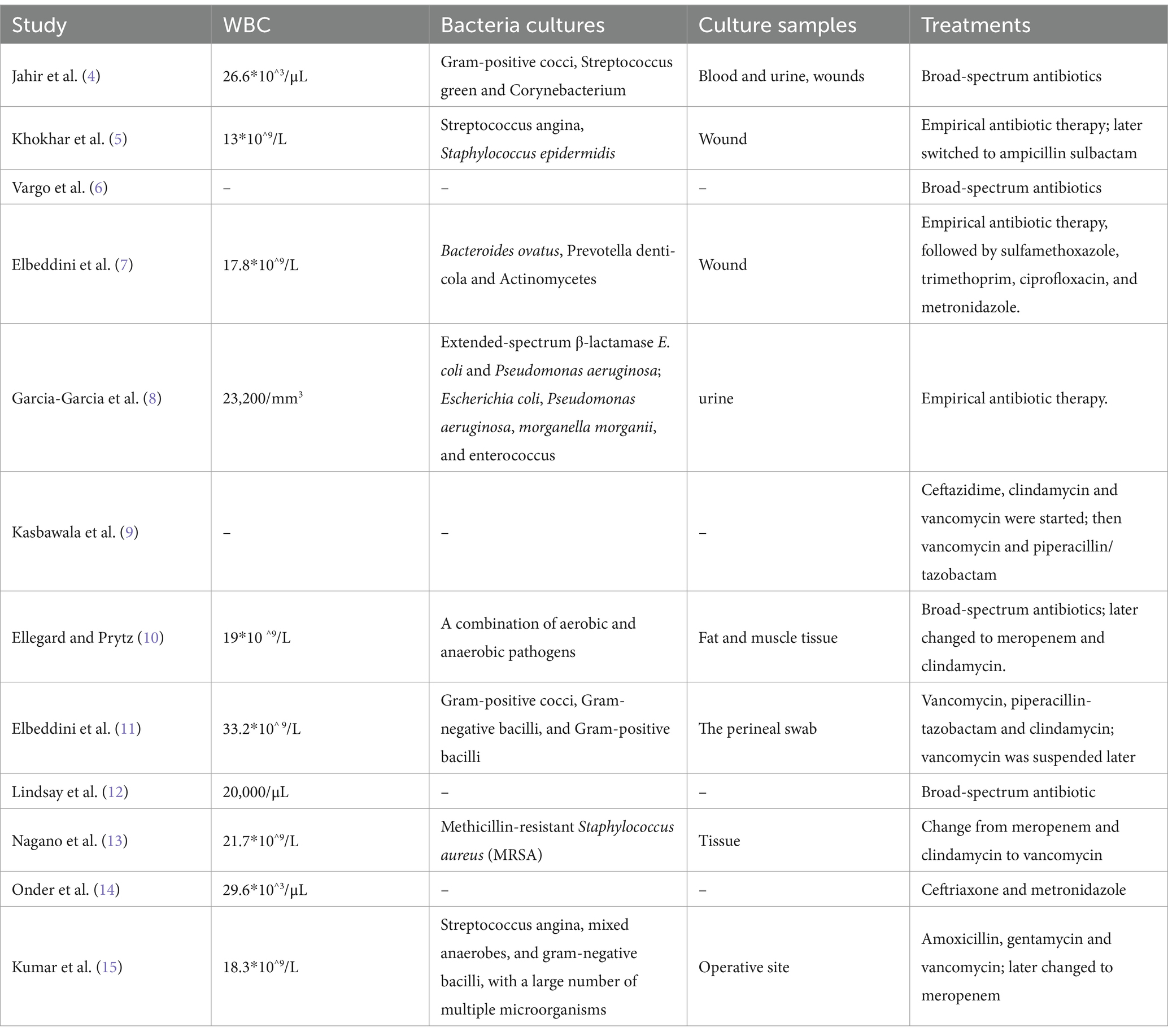
Table 3. Treatments of the 12 included patients.
All cases were diabetic patients. In addition, the most common complications were hypertension, hyperlipidemia, diabetic ketoacidosis, prostate cancer, and obesity, with 6, 4, 3, 2, 2 cases, respectively. Out of the 12 patients, 11 were taking concomitant medications, of which 7 were prescribed metformin (Table 2). When combining these diseases or using metformin in combination, it is important to monitor patients for any adverse reactions.
Laboratory tests are summarized in Table 4. Nine cases reported elevated glycated hemoglobin levels, with eight exceeding the normal range. Seven cases reported blood glucose and six of them were higher than the normal range. When patients experience FG, blood sugar management is inadequate.
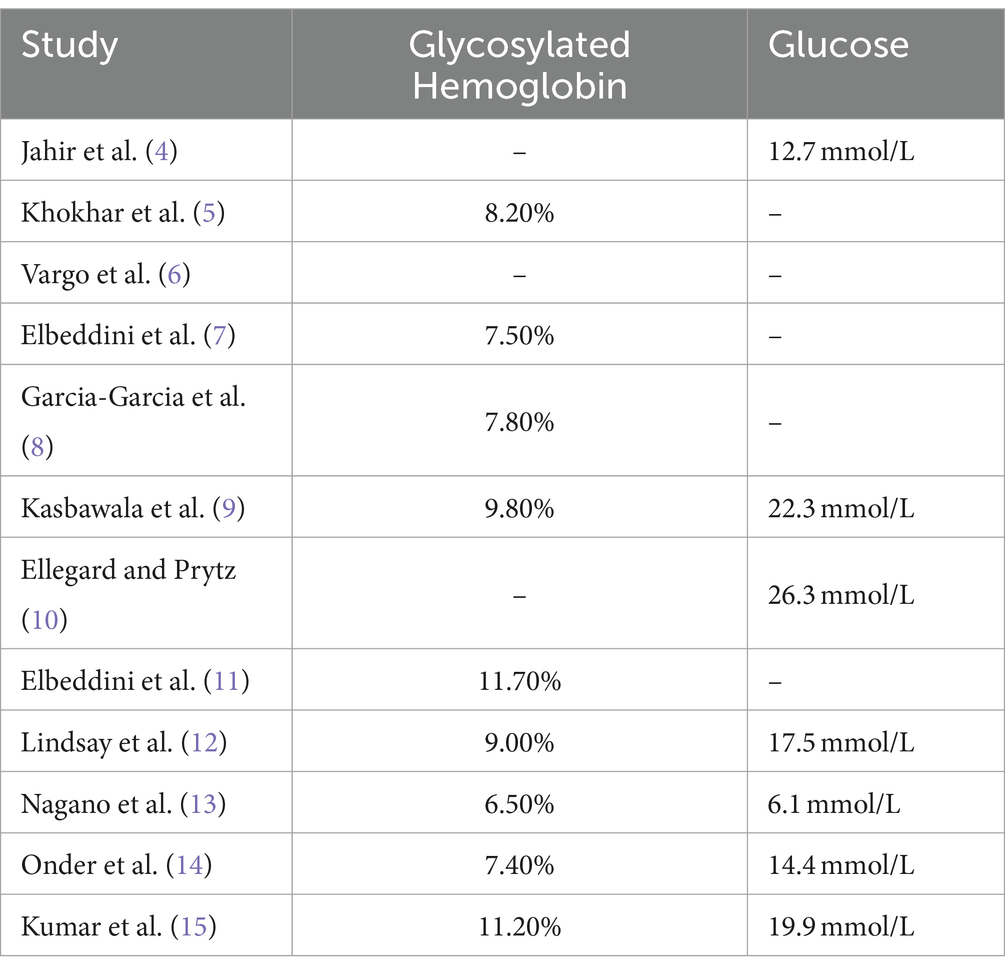
Table 4. Laboratory tests of the 12 included patients.
Treatment involves discontinuation of the medication, urgent and aggressive surgical exploration with debridement of necrotic tissue, and administration of broad-spectrum antibiotics, among other measures (16). All patients underwent surgical debridement. White blood cell count was reported in 10 patients, all above normal values (9.5 × 10^9/L) (Table 3). Bacteria cultures were performed in eight patients. Culture samples involved blood samples, urine samples, wound sampling, perineal swabs, and surgical site sampling; a variety of bacterial species were cultured, including Gram-positive cocci and Gram-negative rods (Table 3). The patient was admitted immediately admitted on empirical antibiotic intravenous therapy including vancomycin, meropenem, clindamycin, ampicillin sulbactam, daptomycin, ceftazidime, piperacillin/tazobactam, ceftriaxone, metronidazole, amoxicillin, and gentamicin. Later, the medication was adjusted according to the patient’s condition and the results of bacterial culture, and the type of antibiotics or prescription were changed.
FG, also known as perineal necrotizing fasciitis, is a urinary emergency characterized by progressive necrotic infection of the external genitalia or perineum, local skin purple-black or brown, exuding large amounts of purulent fluid, accompanied by a foul odor, subcutaneous spasm, rare but rapid onset. Diabetes is an important predisposing factor, along with obesity, cancer, advanced age, and other immunosuppressive diseases (17). Management relies on early identification. Treatment includes discontinuation of medication, urgent and aggressive surgical exploration with debridement of necrotic tissue, and administration of broad-spectrum antibiotics, among other measures (16).
SGLT-2 inhibitors, including canagliflozin, dapagliflozin, empagliflozin, and ertugliflozin, were first approved in 2013 for adults with type 2 diabetes. They exert a hypoglycemic effect by promoting the excretion of sugar through the kidneys. Both the UK Medicines and Healthcare Products Regulatory Agency (MHRA) (18) and the US FDA (19) have concluded that the risk of FG for SGLT-2 inhibitors is warranted based on received case reports. The cases included in this study were reported from 2017 to 2022, totaling 12 cases. Bershoff-Matcha et al. identified a total of 55 cases meeting the inclusion criteria in the FAERS database, with a median age of 56 years, 39 males, and 16 females. The average time to event was 9 months (range: 5 days to 49 months). Reported complications included diabetic ketoacidosis, and all patients underwent surgical debridement (20). As of January 2022, the American Diabetes Association identified a total of 491 cases of FG associated with SGLT-2 inhibitors, of which 162 were caused by canagliflozin, 101 cases of dapagliflozin, and 223 cases of empagliflozin and found a statistically significant increase in the risk of FG hospitalization with SGLT2i treatment compared to the use of two or more non-SGLT2 inhibitors or insulin therapy alone (3). Bao Anh Tran et al. reported a median age of 54 years and 52 years in cases from the FAERS database and literature review, respectively. In both datasets, the incidence of FG was higher in males than females. Other reported data included clinical outcomes and concomitant antihyperglycemic medications, which are consistent with the findings of my study. In addition, the number of associated cases continues to rise despite the issuance of a FG risk warning for SGLT-2 inhibitors (3). Therefore, both physicians and patients should be concerned about the adverse effects of SGLT-2 inhibitors. SGLT-2 inhibitors’ mechanism in causing Fournier’s gangrene (FG) is still unclear, potentially associated with the stimulation of urinary glucose excretion (1), SGLT-2 inhibitors function by inhibiting the renal tubular reabsorption of glucose, leading to a significant excretion of glucose in the urine. This high concentration of urinary glucose can create an ideal environment for bacterial growth, thereby increasing the risk of gangrene (2). Additionally, the presence of urinary glucose may lead to localized osmotic changes, contributing to bacterial infection (21). On the other hand, SGLT-2 inhibitors might exert some influence on the immune system, but the specific mechanism remains unclear (22). Of the 12 patients included in this review, all had diabetes, and 11 of them exhibited poor glycemic control at the onset of FG (glycosylated hemoglobin, HbAlc >7.0%), so there was still a risk of FG despite good glycemic management with SGLT-2 inhibitors.
According to the guidelines for the clinical application of antimicrobial drugs issued in 2015, the selection of antibacterial drug varieties should in principle be determined according to the results of bacterial drug susceptibility tests, and the corresponding qualified specimens should be retained in time before starting antimicrobial treatment for pathogenic testing. Among the cases included in this paper, 8 patients underwent bacterial culture, and the culture rate accounted for only 66.7%, suggesting that the awareness of bacterial drug susceptibility testing among medical workers should be strengthened. In this study, cultures showed that patients with FG were monocultures or a combination of bacteria of aerobic, anaerobic, or facultative anaerobic bacteria. In mixed infection, aerobic bacteria can provide a suitable growth environment for anaerobic bacteria after consuming oxygen, while producing leukocyte toxins to avoid phagocytosis of white blood cells, and its metabolites can also lead to endarteritis obliterans, making the skin and subcutaneous tissue ischemic necrosis, resulting in the further spread of pathogenic microorganisms.
This study identified 12 case reports from literature retrieval, which is more than found in any other articles. Furthermore, the study results support previous findings, providing a comprehensive summary of clinical characteristics, and conducting a thorough analysis and discussion. However, due to the nature of being case reports, the level of evidence is relatively low. Additionally, it is challenging to determine whether the occurrence of FG in patients using SGLT2 inhibitors is a direct correlation. Therefore, careful consideration of potential risk factors for FG in patients is warranted.
In summary, FG caused by SGLT-2 inhibitors, despite its low incidence, is rapidly progressive and severe. When SGLT-2 inhibitors are used clinically, the patient’s discomfort during medication should be closely observed, and if FG is suspected, it is recommended to stop the drug immediately and start broad-spectrum antibacterial drugs and surgical debridement combination therapy to ensure clinical safety. For patients progressing to diabetic ketoacidosis, the insulin injections and aggressive fluid resuscitation are also necessary.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
HL: Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Han, Y, Cho, YE, Ayon, R, Guo, R, Youssef, KD, Pan, M, et al. Sglt inhibitors attenuate no-dependent vascular relaxation in the pulmonary artery but not in the coronary artery. Am J Physiol Lung Cell Mol Physiol. (2015) 309:L1027–36. doi: 10.1152/ajplung.00167.2015
2. Dave, CV, Schneeweiss, S, and Patorno, E. Comparative risk of genital infections associated with sodium-glucose co-transporter-2 inhibitors. Diabetes Obes Metab. (2019) 21:434–8. doi: 10.1111/dom.13531
3. Wang, T, Patel, SM, Hickman, A, Liu, X, Jones, PL, Gantz, I, et al. Sglt2 inhibitors and the risk of hospitalization for Fournier's gangrene: a nested case-control study. Diabetes Ther. (2020) 11:711–23. Data sharing is not applicable as no new data were generated during this study. doi: 10.1007/s13300-020-00771-8
4. Jahir, T, Hossain, S, Bagum, M, Saidi, A, Risal, R, and Schmidt, M. A rare but life-threatening case of Fournier's gangrene caused by sodium-glucose Cotransporter-2 (Sglt2) inhibitor, Empagliflozin. Cureus. (2022) 14:e29264. doi: 10.7759/cureus.29264
5. Khokhar, F, Hernandez, C, and Mahapatra, R. Fournier's gangrene in an Hiv-positive patient on Empagliflozin for the treatment of diabetes mellitus. Cureus. (2022) 14:e26083. doi: 10.7759/cureus.26083
6. Vargo, E, Leone, G, Barat, O, Yunker, A, and Parekh, N. A case of Fournier's gangrene following a large-volume hydrocelectomy in a diabetic patient managed with Sglt-2 inhibitor therapy. Urol Case Rep. (2021) 39:101834. doi: 10.1016/j.eucr.2021.101834
7. Elbeddini, A, Gallinger, J, Davey, M, Brassard, S, Gazarin, M, Plourde, F, et al. A case of Fournier's gangrene in a patient taking Canagliflozin for the treatment of type II diabetes mellitus. Am J Case Rep. (2020) 21:e920115. doi: 10.12659/AJCR.920115
8. Garcia-Garcia, A, Galeano-Valle, F, Nuevo-Gonzalez, JA, and Demelo-Rodriguez, P. Fournier's gangrene and Sglt2 inhibitors: a case study. Endocrinol Diabetes Nutr. (2020) 67:423–5. doi: 10.1016/j.endinu.2019.12.007
9. Kasbawala, K, Stamatiades, GA, and Majumdar, SK. Fournier's gangrene and diabetic ketoacidosis associated with sodium glucose co-transporter 2 (Sglt2) inhibitors: life-threatening complications. Am J Case Rep. (2020) 21:e921536. doi: 10.12659/AJCR.921536
10. Ellegard, L, and Prytz, M. Fournier's gangrene under Sglt-2 inhibitor therapy: a literature review and case report. Int J Surg Case Rep. (2020) 77:692–4. doi: 10.1016/j.ijscr.2020.11.100
11. Elbeddini, A, Tayefehchamani, Y, Davey, M, Gallinger, J, Hooda, N, Aly, A, et al. Fournier's gangrene with dapagliflozin in a rural hospital: a case report. BMJ Case Rep. (2021) 14:e237784. doi: 10.1136/bcr-2020-237784
12. Lindsay, PJ, Gibson, LE, Bittner, EA, Berg, S, and Chang, MG. Sodium-glucose cotransporter-2 (Sglt2) inhibitor-induced euglycemic diabetic ketoacidosis complicating the perioperative management of a patient with type 2 diabetes mellitus (T2dm) and Fournier's gangrene: a case report. Int J Surg Case Rep. (2020) 77:463–6. doi: 10.1016/j.ijscr.2020.11.037
13. Nagano, Y, Yakame, NK, Aoki, H, Yamakawa, T, and Kondo, NI. Fournier's gangrene in a patient with type 2 diabetes mellitus treated with Empagliflozin: a case report. Drug Saf Case Rep. (2019) 6:11. doi: 10.1007/s40800-019-0105-8
14. Onder, CE, Gursoy, K, Kuskonmaz, SM, Kocer, U, and Culha, C. Fournier's gangrene in a patient on dapagliflozin treatment for type 2 diabetes. J Diabetes. (2019) 11:348–50. doi: 10.1111/1753-0407.12896
15. Kumar, S, Costello, AJ, and Colman, PG. Fournier's gangrene in a man on empagliflozin for treatment of type 2 diabetes. Diabet Med. (2017) 34:1646–8. doi: 10.1111/dme.13508
16. Singh, A, Ahmed, K, Aydin, A, Khan, MS, and Dasgupta, P. Fournier's gangrene. A clinical review. Arch Ital Urol Androl. (2016) 88:157–64. doi: 10.4081/aiua.2016.3.157
17. Canbaz, H, Caglikulekci, M, Altun, U, Dirlik, M, Turkmenoglu, O, Tasdelen, B, et al. Fournier's gangrene: analysis of risk factors affecting the prognosis and cost of therapy in 18 cases. Ulus Travma Acil Cerrahi Derg. (2010) 16:71–6.
18. The UK warns of the risk of genital or perineal necrotizing fasciitis with Sglt2 inhibitors. J China Prescript Drug. (2019) 17:3.
19. The FDA warns that Sglt2 inhibitors may be associated with serious reproductive infections. J China Prescrip Drug. (2018) 16:3.
20. Bersoff-Matcha, SJ, Chamberlain, C, Cao, C, Kortepeter, C, and Chong, WH. Fournier gangrene associated with sodium-glucose Cotransporter-2 inhibitors: a review of spontaneous postmarketing cases. Ann Intern Med. (2019) 170:764–9. doi: 10.7326/M19-0085
21. Li, D, Wang, T, Shen, S, Fang, Z, Dong, Y, and Tang, H. Urinary tract and genital infections in patients with type 2 diabetes treated with sodium-glucose co-transporter 2 inhibitors: a meta-analysis of randomized controlled trials. Diabetes Obes Metab. (2017) 19:348–55. doi: 10.1111/dom.12825
Keywords: SGLT-2 inhibitor, Fournier’s gangrene, adverse drug reaction, literature analysis, case
Citation: Liu H (2024) Case literature analysis of Fournier’s gangrene caused by sodium-glucose protein-2 inhibitors. Front. Med. 11:1301105. doi: 10.3389/fmed.2024.1301105
Edited by:
Monica Catarina Botelho, Universidade do Porto, PortugalReviewed by:
Yunfang Meng, Shandong Provincial Hospital, ChinaCopyright © 2024 Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hailing Liu, a3h5ajIwMjNAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.