 Pilar Montesó-Curto1,2*†
Pilar Montesó-Curto1,2*† Loren Toussaint3†
Loren Toussaint3† Angela Kueny4†Ilga Ruschak5,6
Angela Kueny4†Ilga Ruschak5,6 Shannon Lunn7Lluís Rosselló8Carme Campoy9Stephanie Clark10Connie Luedtke10Alessandra Queiroga Gonçalves11,12Carina Aguilar Martín11,13‡Ann Vincent10‡Arya B. Mohabbat10‡
Shannon Lunn7Lluís Rosselló8Carme Campoy9Stephanie Clark10Connie Luedtke10Alessandra Queiroga Gonçalves11,12Carina Aguilar Martín11,13‡Ann Vincent10‡Arya B. Mohabbat10‡- 1Primary Care, Institut Català de la Salut (ICS), Tortosa, Spain
- 2Department of Medicine, Rovira i Virgili University, Reus, Spain
- 3Department of Psychology, Luther College, Decorah, IA, United States
- 4Department of Nursing, Luther College, Decorah, IA, United States
- 5Internal Medicine Unit, Sant Pau i Santa Tecla Hospital, Tarragona, Spain
- 6Faculty and Department of Nursing, Rovira i Virgili University, Tarragona, Spain
- 7Research Division, United Hospital Allina Health, Minneapolis, MN, United States
- 8Santa Maria Hospital, Lleida, Spain
- 9Faculty of Nursing and Physiotherapy, Lleida University, Lleida, Spain
- 10Mayo Clinic, Division of General Internal Medicine, Rochester, MN, United States
- 11Unitat de Suport a la Recerca Terres de l’Ebre, Institut Universitari d’Investigació en Atenció Primària (IDIAP) Jordi Gol, Tortosa, Spain
- 12Unitat Docent de Medicina de Família i Comunitària Tortosa-Terres de L‘Ebre, Institut Català de la Salut, Tortosa, Spain
- 13Unitat d’Avaluació, Direcció d’Atenció Primària Terres de l’Ebre, Institut Català de la Salut, Tortosa, Spain
Introduction: Gender roles may impact men with fibromyalgia, causing a high number of negative emotional states and affective disorders. There are few studies that detect men’s high emotional suffering. This study examined the emotional experience of men with fibromyalgia.
Methods: A qualitative cross-cultural study utilized inductive thematic analysis was performed at the Fibromyalgia and Chronic Fatigue Unit Santa Maria University Hospital in Spain, the Fibromyalgia and Chronic Fatigue Clinic at Mayo Clinic in the US, and volunteers from the Winneshiek County in the US A total of 17 participants, 10 men from Spain and 7 men from the US were included.
Results: Three themes related to feelings/emotions emerged: (1) psychological level; (2) social level; and (3) physical level. Men with fibromyalgia from Spain and the US experienced many negative emotions. Men often experience negative emotions that are worsened by common misunderstandings and social biases/stigma about their condition.
Conclusion/implications: A proper assessment of emotions when evaluating the global health of men with fibromyalgia as well as the provision of emotional support would improve their mental health and therefore their overall physical health. Emotional management should be incorporated into all treatment protocols for fibromyalgia, especially for men given the gender stigma. Health policies designed by legislators, policymakers, and support agencies must be accompanied by education in gender role concepts to improve the emotions of men with FMS. The mass media will be essential for the disclosure of the emotional suffering of male patients so that society might better understand them.
1 Introduction
Fibromyalgia syndrome (FMS) is characterized by chronic widespread pain along with fatigue, sleep difficulties, cognitive disturbances, and mood disorders. Prevalence ranges from 2 to 8% of the world population (1). Women have a high predominance of FMS cases, approximately 80–96% (2, 3). The American College of Rheumatology states that diagnosis is based on clinical evaluation and patient reports, as there are no reliable biomarkers to identify this disease (4). All this leads to frustration on the part of patients but also health professionals, family, friends, and co-workers (5). Differences between men and women in FMS prevalence may be linked to misdiagnosis or underdiagnosis in men due to the social stigma that this is a “female disease” (6). FMS is associated with a high prevalence of emotional and affective disorders (7). Patients with FMS tend to frequently experience feelings of anger that they repress, which often leads to the inability to implement strategies to regulate their emotional state (8). It is often considered atypical if a man complains about pain, compared to a woman. Hopefully, these attitudes are changing (9). Gender differences have been difficult to study because of relatively fewer men being diagnosed with FMS (10–13). There is a high prevalence of pain, fatigue, and other common FMS symptoms among women, while the frequency of neuropsychiatric symptoms is higher among men (14).
The concept of emotion has multiple definitions. The lack of an agreed upon definition is a constant source of misunderstandings and a series of debates, mostly unproductive, between different disciplines (15). A feeling can trigger an emotion or be the response to one. In everyday language, emotions and feelings are often used interchangeably (16). It is known that emotions impact the management of FMS (17), its symptomatology (18), functioning, and adjustment (19). Emotion management can suppress or reverse negative emotions and consequently improve the experience of pain (20). Furthermore, high levels of emotional intelligence are also related to better social interaction (20, 21). However, there are very few studies on the impact of emotions in men with FMS, but the few that exist detect men’s emotional discomfort. There have been several qualitative studies exploring experiences of illness due to FMS (22–26). Moreover, there are also other mixed methods and quantitative studies of men which analyze the impact of FMS and, in turn, emotions (12, 13, 27, 28). Additionally, men reported emotions of anger, depression, anxiety, post-traumatic stress syndrome, and irritability in the setting of FMS (28).
The purpose of this study is to add to our understanding of emotional experiences in men with FMS. Additionally, we seek to understand men’s emotional experiences resulting from FMS in the context of culture, and as such, we include men from Spain and United States in our study. These cultures have considerably different healthcare systems and approaches to treating FMS and these macro-causal factors may uniquely impact the emotional experience of men with FMS.
2 Methods
2.1 Design
The design of this study was qualitative and cross-cultural, including men from Spain and the United States (US). Men with FMS provided qualitative data on their emotional experiences through focus groups and in-depth interviews (29). To facilitate the understanding of the question on emotions, we asked: What feelings/emotions do you experience because of fibromyalgia?
2.2 Participants and settings
The sample was purposive (30) and was composed of outpatients attending FMS units of medical facilities in Spain and the US. A total of 17 participants were obtained, 10 from Spain and 7 from the US. Collaboration of these two specialized FMS centers started through the contact of two universities, one in Spain and the other in the US, for the specific purpose of cross-cultural research projects in FMS. Shared interests centered around examining FMS from a biopsychosocial perspective where cultural and gender factors, health policies developed in each country and the organization of health systems were of considered of great importance to understand this condition.
To protect participants’ identities, we used fictitious names in reporting our results. The current study was approved by the Ethics and Research Committee of the Primary Care University Institute Jordi Gol i Gurina from Barcelona, code: 4R18/223,, and the Mayo Clinic Human Subjects Review Board, code: 10429.010. Informed consent was obtained from all participants.
2.3 Data collection
2.3.1 Spain
Participants were selected from a list provided by the Fibromyalgia and Chronic Fatigue Clinic from Lleida, Spain and were contacted by phone. The focus groups conducted in this clinic were divided into 2, 1 month apart in 2018 (May and June). They were conducted by two health professionals trained in focus groups and a third observer familiar with the study. Each group interview took about 120 minutes, was audio-recorded, and later transcribed by two of the researchers who attended these sessions.
2.3.2 US
Participants were recruited from a list provided by the Fibromyalgia and Chronic Fatigue Clinic at Mayo Clinic (Rochester, USA) and were contacted by phone, and from voluntary contact in response to public regional advertisements of the study in Luther College (Decorah, USA) in August 2018. Due to logistical difficulties in coordinating appropriate times for group sessions in the US, focus groups were not conducted and instead one-to-one interviews were deemed the best option. Two men completed a joint interview, while five men completed individual interviews in 2018 (August). Two health professionals conducted the interviews at Mayo Clinic. The individual interviews lasted between 45 and 60 min, while the joint interview lasted 120 min. The interviews were audio-recorded for accuracy and later transcribed.
2.4 Data analysis
Qualitative data were analyzed according to the established methods of inductive thematic analysis through a reduction process to manage and classify the data (31). All recorded data were transcribed by three members of the research team and then independently reviewed by three other researchers to verify the accuracy of the data. Then, four team researchers generated codes and grouped them into categories. The categories were organized into themes with the consensus of the whole group. Biopsychosocial and gender perspectives were analyzed (32). The data were analyzed separately in each country, but the two lead researchers had ongoing conversations to ensure standard coding criteria were in place at each site.
3 Results
The patient’s characteristics are shown in Table 1. Regarding the emotional experience in men with FMS, three emotional themes emerged: (1) psychological level; (2) social level; and (3) physical level (Table 2).
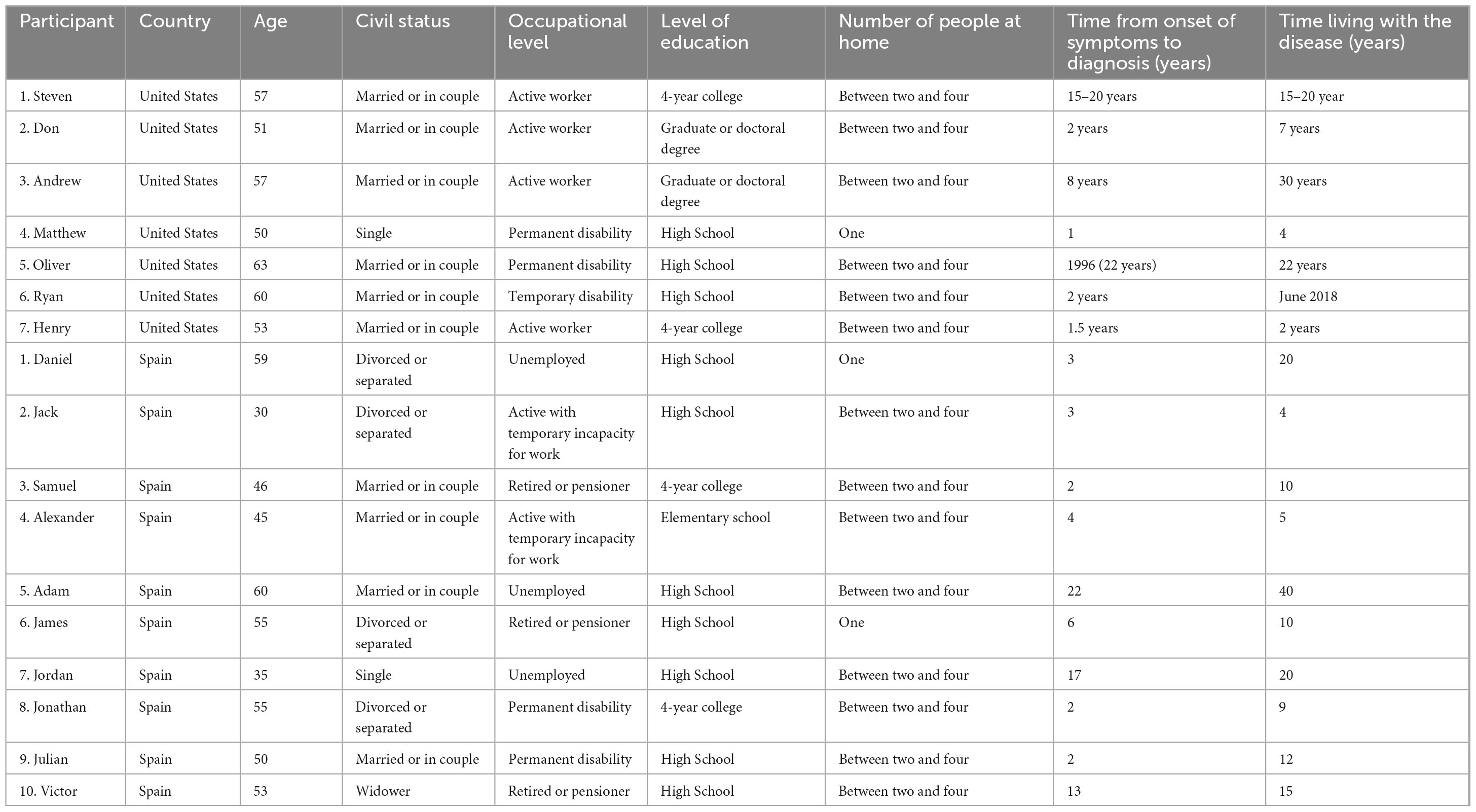
Table 1. Participant characteristics.
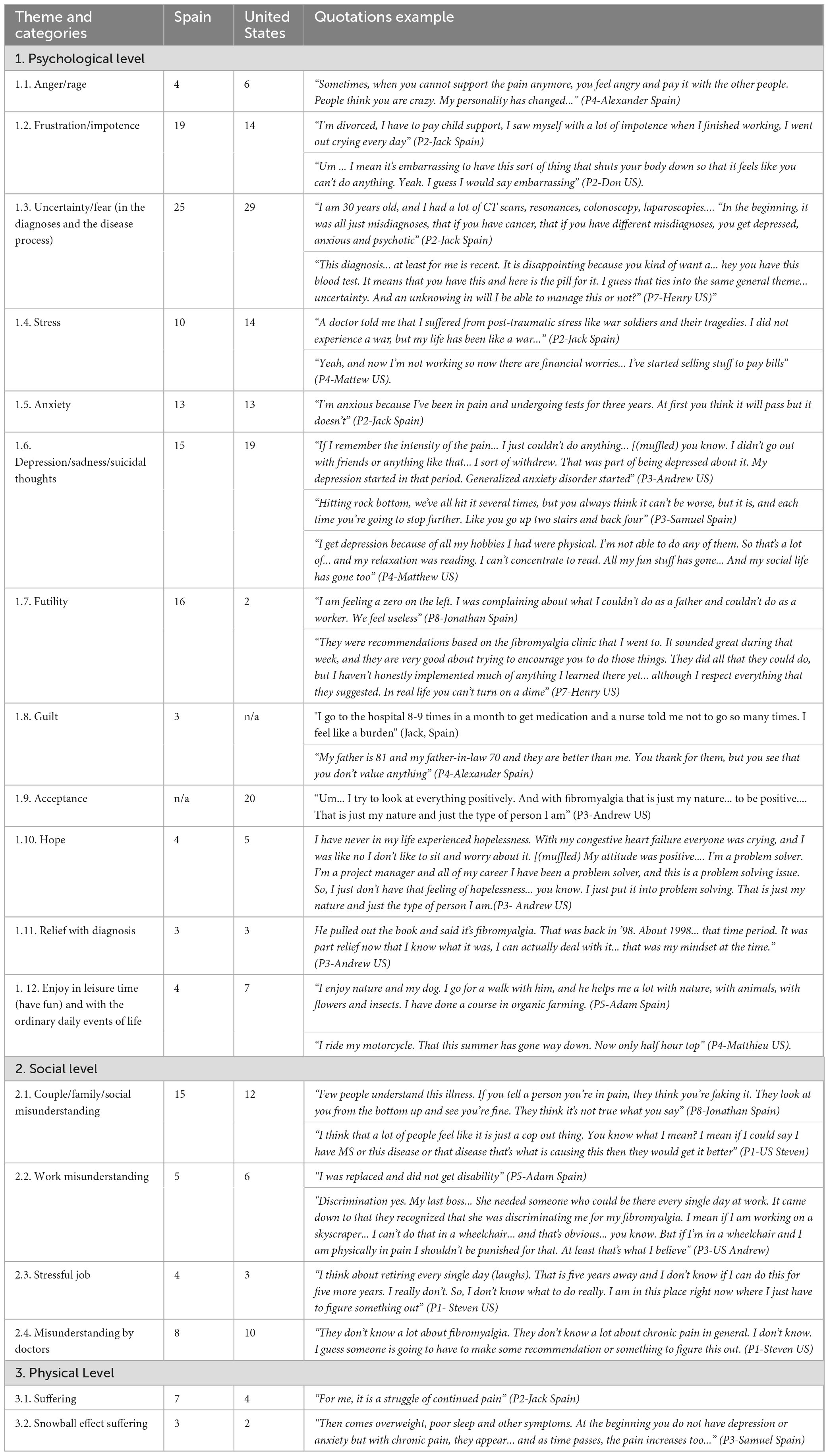
Table 2. Themes, categories on feelings/emotions in men with fibromyalgia.
3.1 Theme 1: psychological level
Most of the emotions that emerged were negative in both Spanish and US men. These negative emotions included anger/rage, frustration/impotence, uncertainty, stress, anxiety, depression/sadness/suicidal thoughts, futility, and guilt. Positive emotions were acceptance, hope, relief with diagnosis, and enjoy in leisure time.
3.1.1 Anger/rage
Due to the lack of understanding of the disease by the people around them and even by the health system, men with FMS experience a great deal of anger and rage.
”You continually feel impotence, anger, and social pressure, because those around you don’t understand the disease” (P3- Spain).
“Overall, I do hate it… I’ll tell you that up front. I can get mad at it for having it… so you get the emotional anger, frustration…” (P3- US).
3.1.2 Frustration/impotence
Men with FMS experience frustration and feelings of impotence because some health providers seem to not understand the condition of FMS. Men have difficulty doing chores, daily life activities, and hobbies; even the simplest tasks are difficult. Men struggle in supporting their families due to the disease’s impact on employment. Moreover, men are frustrated because it took them a long time to be diagnosed and they feel they are not getting better. They are also frustrated due to the lack of a cure or effective treatment.
”You climb 2 steps and backward. Pressure, incomprehension plus impotence…” (P3- Spain).
“If you have pain or fatigue or fogginess and you knew it was for a week, then you can manage it, but if you knew it was forever… that weighs on you” (P7- US).
3.1.3 Uncertainty/fear (in the diagnosis and in the disease process)
The symptoms that appear are unpredictable and often take a considerable amount of time to diagnose. Participants have undergone numerous medical examinations and diagnostic evaluations. Many believe that they may have a serious disease such as cancer. This leads to significant feelings of fear, uncertainty, anxiety, and depression. Furthermore, they are concerned about how the disease will evolve and whether they will be able to manage the disease.
“From the onset of symptoms to having the diagnosis I had to wait 13 years…” (P10- Spain).
“I guess I do have a fear if it gets worse at some point that I would become disabled or not be able to work.” (P2- US).
3.1.4 Stress
Participants consistently identified job stress. Some experience very high levels of stress similar to post-traumatic stress. They describe job stress when working and if not working financial concerns.
“I did the work of 4 people before I was diagnosed with this disease, alone and working 10 h every day” (P6- Spain).
“I identify the cause of FM with other previous diseases and especially work stress” (P1- Spain).
3.1.5 Anxiety
Pain and sleep difficulties lead to anxiety in men with FMS. Although some of them have learned to manage it.
“My sleep has gotten worse, I have insomnia, I wake up suddenly with anxiety, nightmares…” (P10- Spain).
“Well, I have certainly had more anxiety. Anxiety level is decent right now too” (P5- US).
3.1.6 Depression/sadness/suicidal thoughts
Men reach the limit of their emotional strength due to physical pain, economic problems, healthcare mistreatment, lack of symptomatic improvement, lack of hope in a cure, suicidal thoughts in some cases, and obsessive thoughts. Loss of social life and hobbies contributes to these feelings as well. Many believe that they are too young for the physical limitations caused by FMS. In addition, the fact of thinking that the illness is for the rest of their lives also may cause them to become depressed.
“They sent me to the psychiatrist, because with so many pains, I hit bottom at the level of committing suicide, of not being able to take more or endure more” (P10- Spain).
*Asked if he experienced hope in his recovery* “Not anymore.” “I am only 57 years old. It’s depressing.” “The whole idea of living like this for the rest of my life is just more than I can take sometimes…” (P1- US).
3.1.7 Futility
Men feel lots of futile because they are not able to do the same things they used to do; most of them don’t work and their body doesn’t respond as it should. Spanish men presented more feelings of futility. Feelings of futility because men are young, and they can’t do the same things as young people or the older adult/adults.
“When I went to the gym, I saw older people doing stretches that I couldn’t do” (P7- Spain).
”During the early years of being diagnosed, I didn’t have the depression and irritability and all those things that are going on right now. It’s like my body has reached its limits” (P5- US).
3.1.8 Guilt
Spanish men feel guilty that their family members have to put up with them (i.e., burden). In addition, they cannot fulfill the role of parent or breadwinner and they feel bad about it. US men didn’t identify guilt as a feeling or emotion.
“We complain about not doing what has been assigned to us and we feel bad about it” (P3- Spain).
3.1.9 Acceptance
Acceptance of FMS occurred in US men versus Spanish men. Spanish men didn’t identify guilt as a feeling or emotion.
“… but then you realize well… that’s not helping me. Right now, they don’t have a cure for it. I have got to deal with it” (P3- US).
3.1.10 Hope
A common experience for men is to cling to hope. For some, it seems the only solution.
”The doctors burned me the starry ganglion and it took away my pain for 3 days, it’s not worth it, but there is a hope… something can be done” (P3-Samuel Spain).
”Hope and… well there is always hope…. Again, I was just given the word fibromyalgia a couple weeks ago by Dr. XXX in Rheumatology. I was told it was an autoimmune disease… rheumatoid arthritis. Now I am told it is fibromyalgia. I’m not sure about that. Obviously, I’m not a doctor. I want to learn more. I have looked at it a little on my phone. I’m not a big I.T. guy. I don’t learn well from reading” (P6- US).
3.1.11 Relief with diagnosis
The positive aspects of the disease emerged more in US men. As it is a condition that remains permanent and cannot be completely cured, they believe that they have no other solution but to accept and adapt to it. Others remark that they are more positive and put the problems on aside.
When they were diagnosed, participants felt relief, and now some of them are able to cope with the disease.
“Before we knew what we had, we suffered torments. I think we went through an ordeal of numerous diagnoses before we knew what we really had” (P3- Spain).
3.1.12 Enjoy in leisure time (have fun) and with the ordinary daily events of life
Men with FMS attempt to maintain their hobbies. They do well going for a walk with their dog, having contact with nature, and controlling their breathing. However, some are no longer capable of engaging in their hobbies, which leads to significant mood changes. This emotion has not been included together with the positive emotions as it concerns only leisure time.
“We know how to enjoy many more things because it gives us the energy to continue” (P3- Spain).
“I do voice work for a radio station here in Cedar Rapids…I do it about once a week. I always look forward to and have been enjoying” (P2- US).
3.2 Theme 2: social level
Similar codes about feelings of misunderstanding appeared in the US and Spain. Regarding work-life, Spanish men were not currently working but referred to the difficulties perceived during their working lives.
3.2.1 Couple/family/social misunderstanding
Men with FMS do not believe that those around them understand the condition. As a result of their normal external appearance, participants often feel embarrassed and ashamed, or that they might be faking an illness. Another reason is the social pressure they have to do the housework if they are the ones who stay at home and the wife works.
“I do the housework and my wife Works” (P3- Spain).
“Back home a lot of people don’t know about the disease, so when I tell them what I have they are like oh what’s that? So, they don’t realize that it is mostly women” (P4- US).
3.2.2 Work misunderstanding
Men have lost many jobs due to frequent illness-related absences. Colleagues mocked them because they did not believe that their suffering was real. Some felt discriminated at work.
“I have had many job losses, people laughed, they said I was cheating” (P8- Spain).
”I have had to miss work a couple of times where it was more substantial…my coworkers noticed, and my boss noticed. I feel like there were decisions made about my role at that time that wouldn’t have been made had I been there” (P2- US).
3.2.3 Stressful job
Some have stopped working and others are waiting for the opportunity to leave work since they do not know how long they will be capable.
3.2.4 Role reversal
“I was autonomous, I had workers under my charge. I had to quit work and since then I have been the mother and my wife the father of the house” (P3- Spain).
3.2.5 Inability to diagnose appropriately
Some clinicians inaccurately believe that they understand the disease. Other clinicians actually do have a better understanding of patients with FMS. For FMS to be identified, patients go through numerous evaluations. They have the belief that clinicians doubt if the disease exists, that not much is known about it, and that further research is needed.
“I’ve been explaining to doctors for many years, but they’re not interested. (P10- Spain).
”Started with neurology. Went to cardiology. Went to rheumatology. The doctor in rheumatology… Dr. XXX was the first to give me… to put any kind of label of anything on it. Dr. XXX was the first thing and that started out as autoimmune… rheumatoid arthritis. If doctors don’t agree with it and only a certain set of doctors whether it is just rheumatologists or whatever that’s it” (P6- US).
3.3 Theme 3: physical level
Similar codes about feelings of physical suffering appeared in US and Spanish men. Pain is the main symptom that makes it difficult for them to perform activities. There is a snowball effect, and the symptoms are chained one after another. The pain appears, leading to decreased physical activity, weight changes, sleeping difficulties, and mood changes (“snowball effect”). For some, as time goes by, the pain increases.
3.3.1 Suffering
Chronic generalized pain is the main aspect of physical suffering identified. It makes it difficult to perform physical exercise.
“Pain that penetrates to the soul” (P8- Spain).
“I have to get down to the ground a lot sometimes. I avoid it now a lot if I don’t need to” (P1- US).
3.3.2 Snowball effect suffering
First, the pain comes, and then other symptoms appear, such as difficulty sleeping, being overweight, anxiety, and depression. It is like a snowball that is increasing.
”Part of this is because it’s all a big snowballing effect, right? I like to do walking if I can for exercise because I need to lose weight, but the more I do the more I hurt. Then you don’t walk, and you don’t do things because you hurt. So, then the weight comes and then you know I don’t sleep well and then that causes more things. It’s a big snowball effect where then I turn into this hot mess (laughs)”(P1- US).
4 Discussion
Our findings highlighted that men with FMS experienced so many negative emotions due to the changes in their physiology but also because they had to make numerous changes to adapt their lives to the onset of FMS. It’s difficult to make these adjustments. Their bodies are imprisoned by pain and other crippling symptoms, and they have been suffering from many failed treatments (25). These emotions were associated with different events due to the nature of the disease itself, psychological factors, and the cultural and social contexts in the men’s lives. Despite these different contexts in terms of emotions between the US and Spain, more similarities than differences were found. However, US men expressed more feelings of positive emotions (mostly acceptance) and enjoyment of leisure time. Spanish men showed more feelings of futility and guilt.
Overall, men feel anger, frustration, helplessness, depression, sadness, and impotence because of the difficulty in performing the tasks of daily life, at work, and in their own families. Men also felt frustration for not being the father or spouse they used to be, due to an inability to support their family (33). The more traditional expectation for men is that they develop a conservative role within the family, as the main breadwinner. The inability to do this has a direct impact on men as they are unable to fulfill this gender mandate produces negative emotions such as worthlessness, depression, sadness, and suicidal thoughts (34). They felt futility and depression due to inability to work, engage in recreational activities, or participate in basic daily activities (32). Most of the Spanish participants were not active workers while most US participants were currently working. Patients in Spain are allowed to exempt themselves from work by receiving a small pension, while men in the US describe fewer options to leave their jobs. The Spanish health and social system provide healthcare coverage and pension provision (27). Participants in our study also identified negative emotions like anger, frustration, and impotence experiences with the misunderstandings by some healthcare professionals with did not contribute to their improvement (11, 22, 23). The misunderstanding of the disease and lack of empathy on the part of family, friends, and health professionals caused emotions of anger, rage, frustration, and helplessness (11, 25). Also, men reported the lack of recognition of FMS in men has such a strong influence on men who are affected because it is not believed that men can suffer from it, as it is mostly associated with the female sex (35).
The difficulty in diagnosis creates negative emotions such as uncertainty, fear, stress, and anxiety (26), and it was clearly observed that men endure a lot of pain and fear of being seen as complainers (24). Men with FMS stated the difficulty for men to express their feelings in order not to be labeled as inferior men, as culturally, men’s complaints may challenge their socially constructed masculinity (23).
Men in Spain felt that life was futile and they felt guilty about their condition. This is because they were not able to fulfill the traditional gender role of being a breadwinner for their household. More commonly men were unemployed, retired (pensioner), or on permanent disability. The concept of “gender” refers to culturally accepted norms, attitudes, and beliefs about what it is to be male or female. In contrast to the old-school term “gender role,” (36) gender should be understood as an ongoing process and not as a fixed entity or outcome, and that it is linguistically constructed and contextually situated. Deviating from norms can be subject to negative stigmatization and, even worse, social exclusion (37). The construction of masculinity from cultural achievement, such as sport or manual labor means that gender is vulnerable if performance cannot be sustained due to illness or physical disability (38).
Psychosocial support is needed to improve the quality of life of men with FMS (25). Pain impacts a wide variety of experiences both physically and emotionally (24). When the pain was intense, they unloaded the tension with their closest relatives (25). Both depression and FMS challenged the traditional male identity and thus had a demasculinizing effect (39, 40). There are some key limitations to the study. First, the sample size was small. Second, fewer men are diagnosed with FMS, and as such, many men may not have wanted to make themselves visible in their communities.
5 Conclusion
The emotional experience associated with men with FMS was largely negative (anger, frustration, helplessness, uncertainty, fear, worthlessness, futility, stress, anxiety, depression, sadness, and suicidal thoughts). Spanish men had more futility and guilt than US men. In smaller amounts, there were also positive emotions such as acceptance, hope, and relief. Acceptance and enjoyment in leisure time were more present in US men. At the social level, there is incomprehension among partners, family, health professionals, employers, and coworkers. Men also described wanting to quit or escape from work. At the physical level, a generalized and unbearable sensation of pain provokes a cascade of negative emotions at the psychological and physical levels. Clinicians should also be trained in emotional management from a gender perspective in which men are significantly stigmatized due to FMS. Findings from this study might inform health policy design by legislators, policymakers, and support agencies as they work to improve the visibility of the emotional difficulties experienced by men with FMS and improve men’s social support and therapeutic relationships with professionals.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The current study was approved by the Ethics and Research Committee of the Primary Care University Institute Jordi Gol I Gurina from Barcelona, code: CEIC- P18/073, and Mayo Clinic, IRB 10429.010. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
PM-C: Writing – review and editing, Writing – original draft, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization. LT: Writing – review and editing, Writing – original draft, Visualization, Validation, Supervision, Resources, Methodology, Investigation, Formal analysis, Conceptualization. AK: Supervision, Writing – review and editing, Writing – original draft, Validation, Software, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. IR: Writing – original draft, Investigation, Formal analysis. SL: Writing – original draft, Project administration, Investigation, Formal analysis. LR: Writing – review and editing, Supervision, Project administration, Investigation, Funding acquisition, Conceptualization. CC: Writing – original draft, Investigation, Formal analysis. SC: Writing – review and editing, Project administration, Investigation. CL: Writing – original draft, Project administration, Investigation. AG: Writing – review and editing, Formal analysis. CA: Writing – review and editing, Writing – original draft, Project administration. AV: Writing – review and editing, Writing – original draft, Project administration, Investigation. AM: Resources, Writing – review and editing, Project administration, Investigation.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Foundation Rovira i Virgili. Centre for Technology Transfer. No: T18250S. 2018Mecenes-01: La fibromyalgia en hombres, la gran desconocida [Fibromyalgia in men, the great unknown], 09/01/2018-09/30/2020. Crowdfunding PRECIPITA Platform. FECYT (Spanish foundation for science and technology). No: T20061S. September 3rd to December 3th, 2019. https://www.youtube.com/watch?v=hsT2NYEwbeM.
Acknowledgments
We would like to thank the study participants for their valuable contributions to this research and Mayo Clinic support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Gündüz N, Erzıncan E, Polat A. The relationship of intimate partner violence with psychiatric disorders and severity of pain among female patients with fibromyalgia. Arch Rheumatol. (2019) 34:245–52. doi: 10.5606/ArchRheumatol.2019.7090
2. Atzeni F, Talotta R, Masala IF, Giacomelli C, Conversano C, Nucera V, et al. One year in review 2019: Fibromyalgia. Clin Exp Rheumatol. (2019) 37:3–10.
3. Queiroz LP. Worldwide epidemiology of fibromyalgia. Curr Pain Headache Rep. (2013) 17:356. doi: 10.1007/s11916-013-0356-5
4. American College of Rheumatology. Fibromyalgia. (2019). Available online at: https://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Fibromyalgia (accessed September 10, 2022).
5. Rosselló L. Que hay de nuevo en la fibromialgia? In: P Montesó-Curto, L Rosselló editors. Compartir experiencias combatir el dolor Una visión de la fibromialgia desde el ámbito “bio-psico-social”. Tarragona: URV (2017).
6. Miró E, Martínez MP, Sánchez AI, Prados G, Lupiáñez J. Men and women with fibromyalgia: Relation between attentional function and clinical symptoms. Br J Health Psychol. (2015) 20:632–47. doi: 10.1111/bjhp.12128
7. Galvez-Sánchez CM, Duschek S, Del Paso GAR. Psychological impact of fibromyalgia: Current perspectives. Psychol Res Behav Manag. (2019) 12:117–27. doi: 10.2147/PRBM.S178240
8. Trucharte A, Leon L, Castillo-Parra G, Magán I, Freites D, Redondo M. Emotional regulation processes: Influence on pain and disability in fibromyalgia patients. Clin Exp Rheumatol. (2020) 123:40–6.
9. Úbeda-D’ocasar E, Gallego-Sendarrubias GM, Guodemar-Pérez J, Hervás-Pérez JP. Differences between men and women with fibromyalgia | unterschiede zwischen männern und frauen mit fibromyalgie. Physikal Med Rehabil Kurortmed. (2020) 30:272–82. doi: 10.1055/a-1089-8152
10. Arout CA, Sofuoglu M, Bastian LA, Rosenheck RA. Gender differences in the prevalence of fibromyalgia and in concomitant medical and psychiatric disorders: A national veterans health administration study. J Womens Health. (2018) 27:1035. doi: 10.1089/jwh.2017.6622
11. Ruschak I, Toussaint L, Rosselló L, Martín CA, Fernández-Sáez J, Montesó-Curto P. Symptomatology of fibromyalgia syndrome in men: A mixed-method pilot study. Int Int J Environ Res Public Health. (2022) 19:1724. doi: 10.3390/ijerph19031724
12. Ruschak I, Montesó-Curto P, Rosselló L, Aguilar Martín C, Sánchez-Montesó L, Toussaint L. Fibromyalgia syndrome pain in men and women: A scoping review. Healthcare. (2023) 11:223. doi: 10.3390/healthcare11020223
13. Jiao J, Cheng Z, Wang W, Zhao Y, Jiang Q. Demographic characteristics and clinical features of fibromyalgia in China: A cross-sectional study. Rheumatol Ther. (2021) 8:817. doi: 10.1007/s40744-021-00303-1
14. Iannuccelli C, Lucchino B, Gioia C, Dolcini G, Rabasco J, Venditto T, et al. Gender influence on clinical manifestations, depressive symptoms and brain-derived neurotrophic factor (BDNF) serum levels in patients affected by fibromyalgia. Clin Rheumatol. (2022) 41:2171–8. doi: 10.1007/s10067-022-06133-y
15. Mulligan K, Scherer KR. Toward a working definition of emotion. Emot Rev. (2012) 4:345–57. doi: 10.1177/175407391244581
16. Jiménez-Herrera MF, Llauradó-Serra M, Acebedo-Urdiales S, Bazo-Hernández L, Font-Jiménez I, Axelsson C. Emotions and feelings in critical and emergency caring situations: A qualitative study. BMC Nurs. (2020) 19:60. doi: 10.1186/s12912-020-00438-6
17. van Middendorp H, Lumley MA, Jacobs JWG, van Doornen LJP, Bijlsma JWJ, Geenen R. Emotions and emotional approach and avoidance strategies in fibromyalgia. J Psychosom Res. (2008) 64:159–67. doi: 10.1016/j.jpsychores.2007.08.009
18. Pinto AM, Geenen R, Wager TD, Lumley MA, Häuser W, Kosek E, et al. Emotion regulation and the salience network: A hypothetical integrative model of fibromyalgia. Nat Rev Rheumatol. (2022) 19:44–60. doi: 10.1038/s41584-022-00873-6
19. Varallo G, Suso-Ribera C, Ghiggia A, Veneruso M, Cattivelli R, Usubini AG, et al. Catastrophizing, kinesiophobia, and acceptance as mediators of the relationship between perceived pain severity, self-reported and performance-based physical function in women with fibromyalgia and obesity. J Pain Res. (2022) 15:3017–29. doi: 10.2147/JPR.S370718
20. Luque-Reca O, Pulido-Martos M, Gavilán-Carrera B, García-Rodríguez IC, McVeigh JG, Aparicio VA, et al. Emotional intelligence impairments in women with fibromyalgia: Associations with widespread pain. J Health Psychol. (2021) 26:1901–12. doi: 10.1177/1359105319890916
21. Bartkowska W, Samborski W, Mojs E. Cognitive functions, emotions and personality in woman with fibromyalgia. Anthropol Anz. (2018) 75:271–7.
22. Paulson M, Norberg A, Danielson E. Men living with fibromyalgia-type pain: Experiences as patients in the Swedish health care system. J Adv Nurs. (2002) 40:87–95. doi: 10.1046/j.1365-2648.2002.02343.x
23. Paulson M, Danielson E, Söderberg S. Struggling for a tolerable existence: The meaning of men’s lived experiences of living with pain of fibromyalgia type. Qual Health Res. (2002) 12:238–49. doi: 10.1177/104973202129119865
24. Paulson M, Danielson E, Larsson K, Norberg A. Men’s descriptions of their experience of nonmalignant pain of fibromyalgia type. Scand J Car Sci (2001) 15:54–9. doi: 10.1046/j.1471-6712.2001.1510054.x
25. Sallinen M, Mengshoel AM. “I just want my life back!”-Men’s narratives about living with fibromyalgia. Disabil Rehabil. (2017) 4:422–9. doi: 10.1080/09638288.2017.1395085
26. Sallinen M, Mengshoel AM, Solbrække KN. “I can’t have it; I am a man. A young man!” – men, fibromyalgia and masculinity in a Nordic context. Int J Qual Stud Health Well Being. (2019) 14:1676974. doi: 10.1080/17482631.2019.1676974
27. Kueny A, Montesó-Curto P, Lunn S, Mohabbat AB, Clark S, Luedtke C, et al. Fibromyalgia pain and fatigue symptoms in Spanish and U.S. men. Pain Manag Nurs. (2021) 22:423–8. doi: 10.1016/j.pmn.2020.12.003
28. Muraleetharan D, Fadich A, Stephenson C, Garney W. Understanding the impact of fibromyalgia on men: Findings from a nationwide survey. Am J Mens Health. (2018) 12:952–60. doi: 10.1177/1557988317753242
29. Redmond R, Curtis E. Focus groups: Principles and process. Nurse Res. (2009) 16:57–69. doi: 10.7748/nr2009.04.16.3.57.c6946
31. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
32. Montesó-Curto P, García-Martinez M, Romaguera S, Mateu ML, Cubí-Guillén MT, Sarrió-Colas L, et al. Problems and solutions for patients with fibromyalgia: Building new helping relationships. J Adv Nurs. (2018) 74:339–49. doi: 10.1111/jan.13412
33. Samulowitz A, Gremyr I, Eriksson E, Hensing G. “Brave men” and “emotional women”: A theory-guided literature review on gender bias in health care and gendered norms towards patients with chronic pain. Pain Res Manag. (2018) 2018:6358624. doi: 10.1155/2018/6358624
34. Ferguson M. The workplace lives of men with fibromyalgia: A qualitative study. Bloomington: Indiana University (2014).
35. Katz JD, Mamyrova G, Guzhva O, Furmark L. Gender bias in diagnosing fibromyalgia. Gend Med. (2010) 7:19–27. doi: 10.1016/j.genm.2010.01.003
37. Fleming PJ, Agnew-Brune C. Current trends in the study of gender norms and health behaviors. Curr Opin Psychol. (2015) 5:72–7. doi: 10.1016/j.copsyc.2015.05.001
38. Connell R, Messerschmidt JW. Hegemonic mas-culinity; Rethinking the concept. Gender Soc. (2005) 19:829–59.
39. Bernardes SF, Lima ML. Being less of a man or less of a woman: Perceptions of chronic pain patients’ gender identities. Eur J Pain. (2010) 14:194–9. doi: 10.1016/j.ejpain.2009.04.009
Keywords: emotional experience, gender role, fibromyalgia syndrome, cross-cultural studies, qualitative study
Citation: Montesó-Curto P, Toussaint L, Kueny A, Ruschak I, Lunn S, Rosselló L, Campoy C, Clark S, Luedtke C, Gonçalves AQ, Aguilar Martín C, Vincent A and Mohabbat AB (2024) Emotional experiences and gender roles of men with fibromyalgia syndrome: a cross-cultural qualitative study. Front. Med. 11:1286729. doi: 10.3389/fmed.2024.1286729
Received: 17 October 2023; Accepted: 23 April 2024;
Published: 20 May 2024.
Edited by:
Aswathy Sreedevi, Amrita Vishwa Vidyapeetham University, IndiaReviewed by:
Aravind B. Chandru, State Health Systems Resource Centre Kerala (SHSRC-K), IndiaChythra R. Rao, Manipal Academy of Higher Education, India
Copyright © 2024 Montesó-Curto, Toussaint, Kueny, Ruschak, Lunn, Rosselló, Campoy, Clark, Luedtke, Gonçalves, Aguilar Martín, Vincent and Mohabbat. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pilar Montesó-Curto, bWFyaWFwaWxhci5tb250ZXNvQHVydi5jYXQ=
†These authors have contributed equally to this work and share first authorship
‡These authors share senior authorship