 María Estevan-Ortega1Cristina de la Encarnación Castellano2Alberto Mendiola-López2Lucy A. Parker3,4Juan Pablo Caballero-Romeu2,5Blanca Lumbreras3,4*
María Estevan-Ortega1Cristina de la Encarnación Castellano2Alberto Mendiola-López2Lucy A. Parker3,4Juan Pablo Caballero-Romeu2,5Blanca Lumbreras3,4*- 1Pharmacy Faculty, University Miguel Hernández de Elche, Alicante, Spain
- 2Department of Urology, University General Hospital of Alicante, Alicante, Spain
- 3Department of Public Health, University Miguel Hernández de Elche, Alicante, Spain
- 4CIBER de Epidemiología y Salud Pública (CIBERESP), Madrid, Spain
- 5Alicante Institute for Health and Biomedical Research (ISABIAL), Alicante, Spain
Background: Recent guidelines on opportunistic prostate cancer screening conclude that the decision to screen with prostate-specific antigen should be made by each patient individually together with the clinician. However, there is evidence of a lack of clinicians’ awareness of prostate cancer screening. This study sought to assess the recent evidence of clinicians’ knowledge, beliefs, and practice regarding opportunistic prostate cancer screening comparing urologists and generals practitioners.
Methods: A systematic search was conducted in 3 online databases: MEDLINE, Web of Science and EMBASE (from January 1, 2015, to January 9th, 2023). Studies that explored clinicians’ knowledge, beliefs, and practices regarding opportunistic prostate cancer screening were included. Studies were assessed for quality reporting according to the Strengthening the Reporting of Observational studies in Epidemiology guidelines.
Results: A total of 14 studies met the inclusion criteria: ten studies included primary care health professionals, three studies included urologists, and one study included both. Studies involving general practitioners showed a generally low level of awareness of the recommended uses of the test, and urologists showed a greater knowledge of clinical practice guidelines. General practitioners’ opinion of prostate-specific antigen was generally unfavourable in contrast to urologists’ who were more likely to be proactive in ordering the test. Less than half of the included studies evaluated shared-decision making in practice and 50% of clinicians surveyed implemented it.
Conclusion: General practitioners had less knowledge of prostate cancer risk factors and clinical practice guidelines in the use of PSA than urologists, which makes them less likely to follow available recommendations. A need to carry out education interventions with trusted resources based on the available evidence and the current guidelines was identified.
1 Introduction
Screening for prostate cancer (PCa) using prostate-specific antigen (PSA) seeks to detect PCa at an early stage to reduce disease-specific mortality (1). Data from the European Randomised study of Screening for Prostate Cancer (ERSPC) (2), which included 182,160 men, showed that PSA screening significantly reduced prostate cancer–specific mortality by 20% at 16 years of follow-up. Although the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening trial failed to show a reduction in PCa–specific mortality (3), a recent modelling analysis on the data from ERSPCA and PLCO trials showed a reduction of approximately 25–32% in PCa mortality (4). Nevertheless, there are controversies regarding its use as a screening test, as it is also associated with false-positive results and a high frequency of overdiagnosis (5).
Weighing the benefits and harms of PSA, the U.S. Preventive Services Task Force (USPSTF) updated its recommendations in 2017. They stated that opportunistic screening may be useful for men aged 55–69 years, but the decision to screen should be made by each patient individually together with the clinician after the patient has understood the benefits and risks of screening (6). The European Association of Urology (EAU) (7) updated their recommendations in 2015 and more recently in 2021. They stated that clinicians should offer an individualized early detection strategy to inform patients aged over 50 years old with a good functional status and a life expectancy of at least 10–15 years, to African American patients and patients with a family history of PCa aged over 45 years and to men carrying BRCA2 mutations over 40 years old. In addition, they have recently published recommendations for the use of PSA testing as part of a risk-adapted strategy aimed at tackling the present situation in most countries in the European Union (EU). Nevertheless, PSA testing is being prescribed for men over 50 as well as those over 70 in a yet unorganized or on-request service (8), which results in a high rate or false positive results and overdiagnosis. Recently, the European Union published Europe’s Beating Cancer Plan (9), which proposes the introduction of PCa screening with prostate-specific antigen (PSA) testing for men up to 70 years old in combination with additional magnetic resonance imaging (MRI) scanning as a follow-up test.
Healthcare providers play a crucial role in influencing PCa screening uptake among men, providing them with essential information on related risks, potential benefits and uncertainties (10). However, discrepancies in the approach to PSA testing and adherence to PCa screening guidelines are reported between general practitioners (GPs) and urologists. GPs, compared to urologists, may: perceive the PSA test as less useful, show a less proactive approach in informing men about PSA, and exhibit less familiarity with screening guidelines (11). Knowledge gaps among GPs have been found (12), and this point is relevant since the knowledge and attitudes of primary healthcare providers may influence their approach to PCa screening and their implementation of SDM. In this sense, a study in the United States revealed suboptimal practice of SDM among some GPs involved in PCa screening with PSA (13). Controversy surrounding PCa screening and the recent updating of the available guidelines could influence lack of knowledge among GPs and thus, their uneven handling of PSA testing.
Previous research showed a significant decline in the use of PSA screening among men aged 50 and above following the release of the 2012 US Preventive Services Task Force (USPSTF) guidelines (14). Despite this overall reduction, PSA screening continues to be performed at levels that seemingly contradict the USPSTF recommendation. This discrepancy raises questions about the potential influence of the guidelines on the clinicians’ practice (15).
Although there is evidence on clinicians’ knowledge, beliefs and practices before the updating of the available guidelines (16), there has not been an analysis of this information since the last updates of the European Association of Urology guidelines (from 2015 onwards) and USPSTF (after 2017). Moreover, no evidence has been published regarding clinicians’ familiarity with the guideline statements and their opinions about them since the recent updates for both GPs and urologists.
This study, therefore, aims to fill this gap by comparing the recent evidence of GPs and urologists’ (population) about: a) knowledge, b) beliefs, and c) practice (outcomes) regarding opportunistic PCa screening with PSA determination (intervention/exposure). This knowledge will be useful for designing targeted strategies to provide education for clinicians following the recent European Union Cancer Plan.
2 Methods
This review was reported according to the PRISMA statement (Preferred Reporting Items for Systematic Reviews and MetaAnalyses) (17) (protocol in Supplementary Table S1).
2.1 Inclusion and exclusion criteria
The population, intervention, comparator and outcomes (PICO) framework (18) was used to define the eligibility criteria. Studies reporting original research that met the following criteria were included:
• Population— Clinicians: general practitioners and urologists.
• Intervention/exposure— opportunistic screening of prostate cancer based on PSA test.
• Comparison—none.
• Outcomes—clinicians’ knowledge (urologists and GPs), beliefs and practice regarding opportunistic prostate cancer screening with PSA determination.
Observational studies published in English or Spanish that assessed clinicians’ knowledge, beliefs and practices regarding opportunistic PCa screening with PSA determination were included. We restricted to those published after 2015.
2.2 Search strategy
We searched the following databases by 9th of January, 2023, MEDLINE (through PubMed), Web of Science and EMBASE using terms referring to the population (health professionals), intervention (knowledge, beliefs and practice) and outcome (screening request) as descriptors or keywords.
Searches for descriptors were carried out in English and combined by Boolean operators (OR and AND) in four blocks: clinicians; prostate cancer; screening; knowledge, beliefs, practices. The descriptors in each block were combined by the Boolean operator OR. The combination between the blocks was done using the AND operator. Forward and backward citation searching was performed on included papers. The detailed search strategy is outlined in Supplementary Table S2.
To assess risk of bias due to missing results, we also checked for publication in other languages and there were no studies that met the eligibility criteria.
2.3 Study selection
All records retrieved from the search were imported into EndNote, deduplicated and then imported into Rayyan for screening (19). Two reviewers (MEO and BL) independently screened each reference title and abstract (if available) for relevance to this review and eliminated duplicates. This first screening excluded editorials, letters to the editor, systematic reviews, study protocols and any study that did not include original data.
The full article of the selected studies in the first screening was then reviewed. The second round of screening involved two reviewers (MEO and BL) independently and was based on the application of the selection criteria. Any discrepancies in the two screenings between the two reviewers were discussed with two other reviewers (CEC, AM, two urologists with expertise in the field). Study investigators or published studies were not contacted for more additional information.
2.4 Data extraction, variables included and quality assessment
The following data from each study were obtained: country and date of publication, objective, study design, study population (inclusion and exclusion criteria, sample size, and classified into GPs or urologists), sociodemographic characteristics of the population included (sex, age), procedure, main results (knowledge, beliefs and practice), conclusions and limitations.
Studies were assessed for reporting quality according to the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidelines (20).
For both the extraction of the main variables and the quality assessment, three of the authors (MEO, CEC and AML) reviewed the studies independently, and disagreements were resolved by discussion and consensus with other reviewer (BL). Cohen’s kappa coefficient between the reviewers was 1.00.
2.5 Data synthesis and analysis
Data were collated and synthesised using narrative and descriptive summaries. No attempt at meta-analysis was made given the heterogeneity in target population, study design and outcome measures across included studies. To improve conceptual clarity and comprehensiveness, two independent researchers (BL and MEO) synthesized for each report the knowledge, attitudes, beliefs and practice (and their analysis) for the different population (i.e., GPs, urologists).
3 Results
3.1 Literature search
The systematic searches yielded 918 potentially relevant citations, of which 80 were duplicates. A systematic screening process was used (Figure 1) to screen titles, abstracts, and full-text publications, resulting in 81 eligible studies. The reason for the exclusion of full texts was mainly that the results were unrelated to the aim of the study. Finally, 14 studies met the inclusion criteria (11, 21–33).
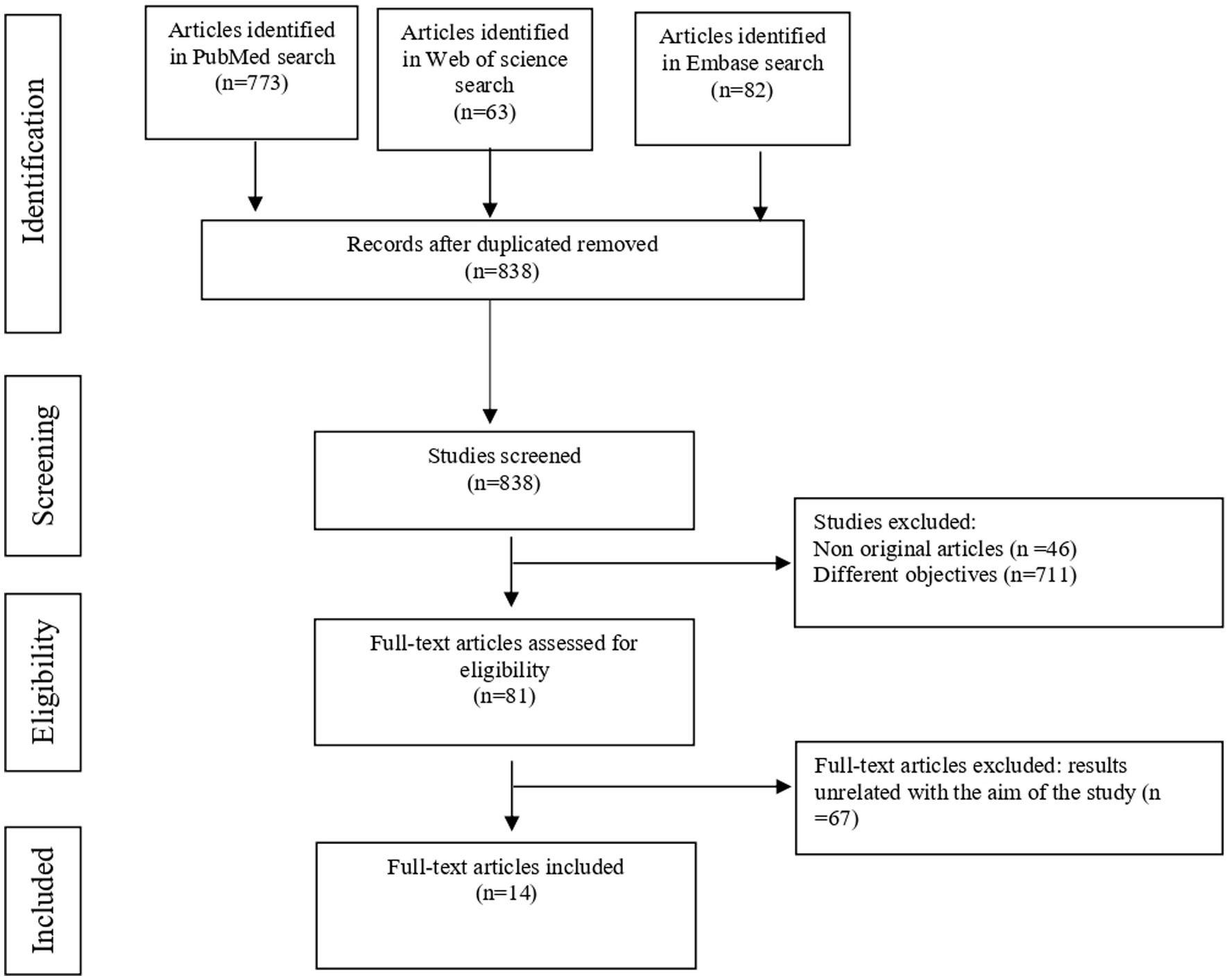
Figure 1. Flowchart describing study selection and excluded studies, according to PRISMA recommendations.
3.2 Evaluation of quality reporting
The median compliance with the 22 criteria applied was 17.5 (IQR 16.8–20) (Supplementary Tables S3, S4).
All studies described the criteria related to the description of the background (item 2), key elements of the study design (item 4), selection of participants (item 6), quantitative variables (item 11), description of the main results (items 13–15), and discussion of the limitations (item 19) and interpretation of results (item 19). However, criteria related to sensitivity analysis (item 17), explanation of how the study size was arrived (item 10) and how quantitative variables were handled in the analyses, were only described in 4 (28.6%), 8 (57.1%) and 8 (57.1%) studies, respectively.
There were three studies (14.3%) below the first quartile (11, 23, 30) and four studies (28.6%) between the median and the first quartile (11, 24, 31, 32). Miller et al’s study (23) did not include relevant aspects such as a detailed description of the setting, thereby limiting the external validity of the results. Furthermore, the study failed to adequately articulate the outcomes and exposure variables, and the methodology for determining the study size was not clearly outlined, potentially introducing biases. Benedict Moa et al.’s study (30) did not provide an explanation for the origin of various variables. In the case of Kappen S et al.’s study (11), the research objectives were not explicitly stated, and there was a lack of effort to address potential sources of bias. Additionally, the study did not detail how the study size was determined and failed to provide a comprehensive description of the statistical analysis.
Concordance among the reviewers was 95.4%.
3.3 Characteristics of identified studies
All articles were cross-sectional, and 7 of them (50%) were published between 2015 and 2017. Most of them were carried out in the USA (5, 35.7%) (21, 23, 25, 29, 31), 2 (14.3%) in Spain (24, 26), and the rest in countries such as Malaysia (22), Saudi Arabia (27), Netherlands (28), South Africa (30), Caribbean (32), Switzerland (33), and Germany (11) (Table 1).
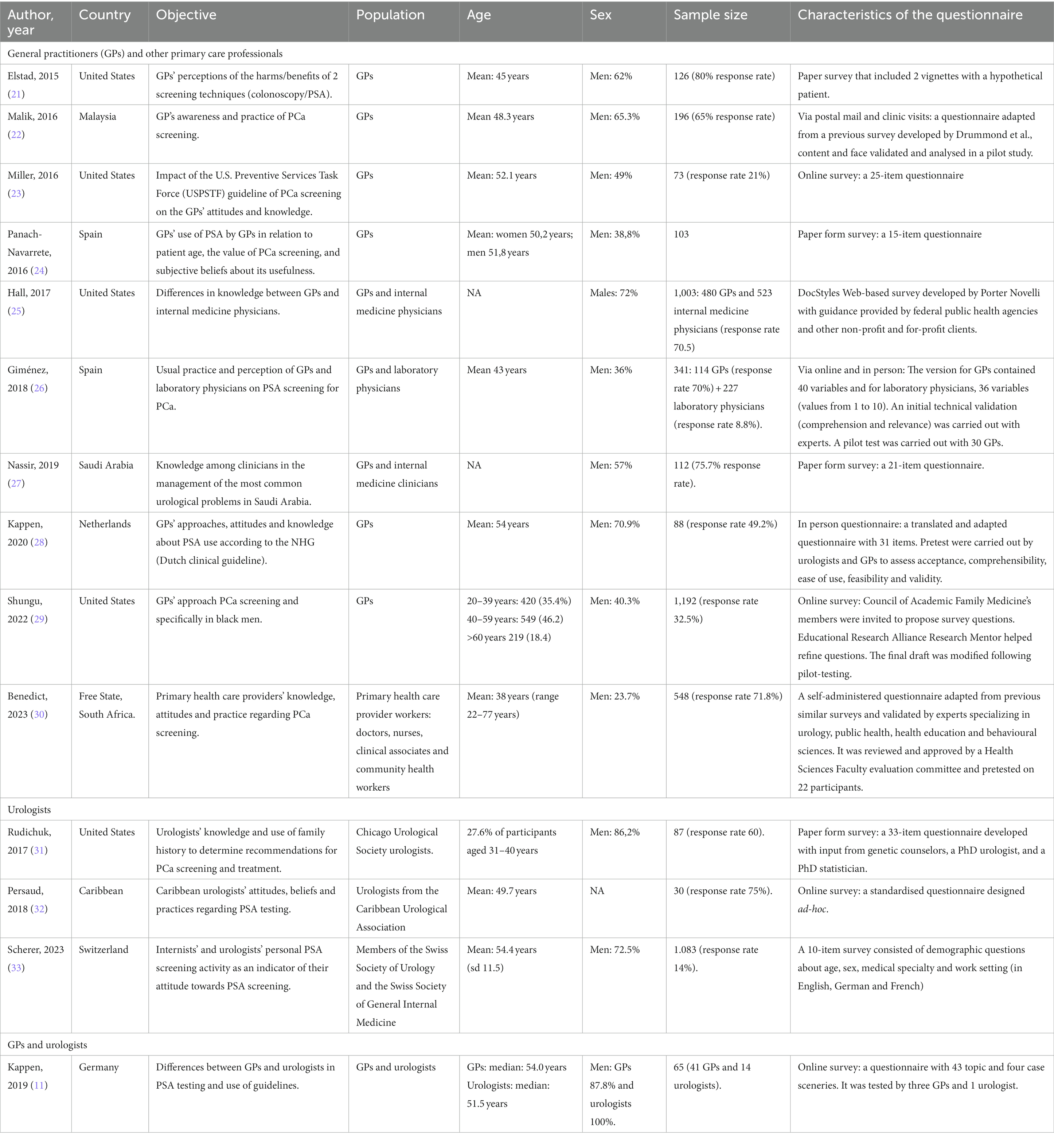
Table 1. Description of the main characteristics of the 14 studies included in the review.
In 10 of the articles (71.4%) (21–30), the study population comprised general practitioners (GPs) and other primary care health professionals [laboratory clinicians (26), nurses, clinical associates and community health workers (30)]; in 3 articles (21.4%) (31–33), urologists were included, and in one, urologists and GPs (11). The mean age of the participants was 49.5 years. The mean sample size was 285, ranging between 30 and 1,192.
3.4 Procedural characteristics of the included studies
Data collection was carried out by questionnaire or survey: 9 studies (64.2%) (11, 22, 23, 25, 26, 29, 30, 32, 33) requested the information by e-mail, online, etc., and 3 of them also solicited information directly from participants in person (22, 26, 30). The remaining articles (21, 24, 27, 28) included in person participation in the questionnaires/surveys. The questionnaires/surveys used were mostly designed ad hoc for the study, and 3 of the articles (21.4%) (22, 28, 30) included previously used questionnaires. However, only three of the studies indicated that the questionnaire was previously validated (22, 26, 30), and others were previously tested by clinicians (11, 28, 29) (Table 1).
3.5 Clinicians’ knowledge, beliefs and use in practice on PCa screening with PSA
The results are described below according to the main topics covered in the studies and in accordance with the clinical specialty (Table 2).
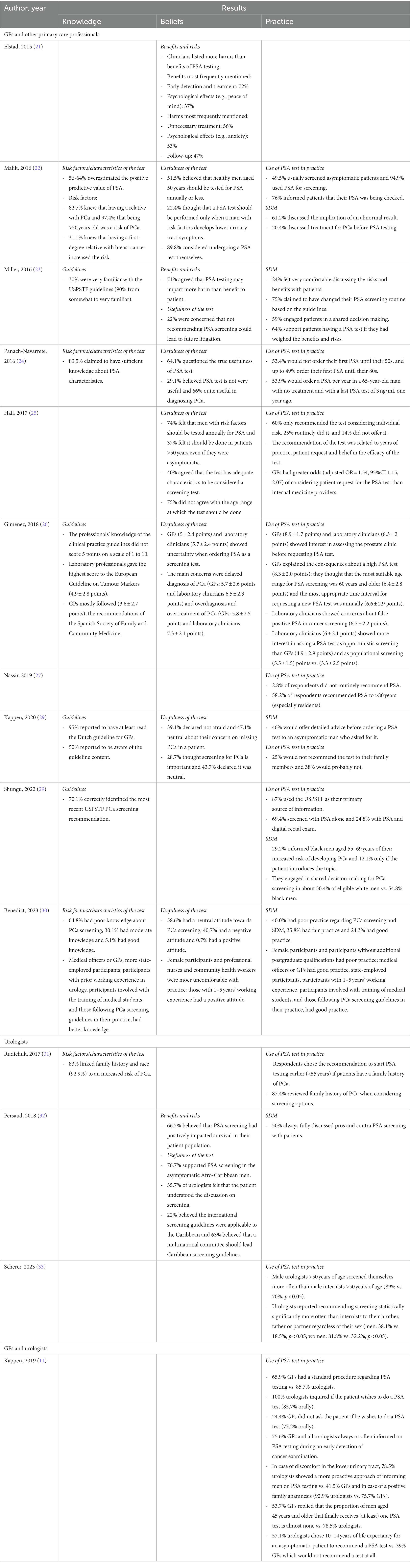
Table 2. Analysis of the main results obtained from the 14 studies included in the review according to the following categories: knowledge, beliefs and practice.
3.5.1 Knowledge of PSA, risk factors and available guidelines
Clinicians’ knowledge about risk factors and PSA test characteristics was covered in 4 articles (22, 24, 30, 31). In addition, 4 studies focused on clinicians’ knowledge about the use of clinical practice guidelines (23, 26, 28, 29).
a. Clinicians’ knowledge about risk factors and PSA test characteristics: Studies involving GPs showed a generally low level of awareness of the recommended uses of the test. In Malaysia (22), only 31% of respondents knew that having a first-degree relative with breast cancer was also a risk factor for PCa, and most of the GPs interviewed overestimated the predictive value of the test. A study carried out in Spain (24) showed that clinicians who had a greater knowledge of PSA tended to request testing in older patients and more frequently questioned the usefulness of the test. In South Africa (30), only 5.1% of the primary health care provider workers had good knowledge about PCa and medical officers or GPs had better knowledge compared with other professionals. Urologists (31) showed a greater knowledge risk factors associated to PCa than GPs.
b. Clinicians’ knowledge about the use of clinical practice guidelines: In relation to clinicians’ knowledge regarding clinical practice guidelines, in a study carried out among GPs in the Netherlands (28), only half of the interviewees stated that they were aware of the available recommendations, but these GPs followed them. In another study among GPs in Spain, although they were not aware of clinical practice guidelines, they stated that they would like to have more information related to PSA testing (26). In another study carried out by GPs in a hospital in the USA (23), 90% of those interviewed were familiar with the existing guidelines, although they did not follow them in routine practice.
3.5.2 Beliefs regarding the usefulness, benefits, and risks of the test
Eight of the included studies (22–26, 28, 30, 32) assessed clinicians’ opinions about the usefulness of PSA, and three of them included an evaluation of its benefits and risks (21, 23, 32).
a. Clinicians’ opinions about the usefulness of PSA: In general, GPs’ opinion of PSA was unfavourable. In a study (25) conducted in the USA, only 40% of GPs acknowledged that the test was a useful screening test. In another study carried out in the Netherlands (28), more than 60% of the GPs interviewed indicated that they would probably not recommend the test to their relatives. In a study in Spain (24), more than 60% of clinicians questioned the usefulness of the biomarker, and nearly 30% of them did not consider it useful for diagnosing PCa. In another study performed in South Africa (30), 40.7 of the surveyed primary health care provider workers had a negative attitude towards PCa screening, and this percentage was higher in nurses and community health workers compared with other professionals.
b. Clinicians’ evaluation of PSA benefits and risks: In other studies (21, 23), GPs indicated that the risks related to PSA outweighed the benefits.
Urologists showed a positive opinion about PCa screening with PSA, mainly those whose patients were Afro-Caribbeans (32) with a higher risk of PCa.
3.5.3 Use of PSA in routine practice
Six studies (22, 23, 28–30, 32) addressed the issue of shared decision-making with the patient, and eight (11, 22, 24–27, 29, 31, 33) evaluated how clinicians used PSA in routine practice.
a. SDM with patient: In primary care, 50% of surveyed GPs engaged in SDM for PCa. In a study carried out in the USA (23), more than 50% of surveyed GPs carried out shared decision-making with the patient but only 24% felt comfortable discussing the risks and benefits of PSA with patients. Similarly, in another study (22), 61.2% of GPs discussed the implication of an abnormal result, but only 20.4% discussed treatment for PCa before PSA testing. In a study carried out in the Netherlands (28), less than 50% of surveyed GPs would offer detailed advice before ordering a PSA test to an asymptomatic man who asked for it. In the USA (29), GPs performed SDM in 50.4% of white men and 54.8% black me, and in South Africa (30) 40% of GPs had poor practice regarding SDM in PCa screening.
A similar percentage was seen in urologists (32), who 50% discussed pros and contras of PSA screening with patients.
a. Use of PSA in practice: In general, screening was recommended in primary care for patients with risk factors for PCa. One of the studies carried out in the USA (25) showed that most GPs only recommended the test considering individual risk, and a smaller percentage of them never offered it. Similarly, in the Saudi Arabian study (27), only 2.8% of GPs did not routinely recommend PSA. In a study carried out in the Netherlands (28), most GPs only recommended screening in patients with risk factors. In contrast, in other studies, GPs did not take risk factors into account when recommending the test: a study in the USA (29) involving GPs indicated that only 29% of them informed their black patients of the risks involved and tended not to have shared decision-making discussions. Several studies showed that GPs disagreed with the age recommendations for PSA testing. In the Saudi Arabian study (27) approximately 60% of GPs recommended screening in patients over 80 years old. In a Spanish study (26), 75% of GPs disagreed with the age range at which the test was offered and most of them thought that the most appropriate time interval for requesting a new test was annually.
A study comparing practices between GPs and urologists in Germany (11) showed a more proactive practice among urologists; 75% of GPs and 100% of urologists informed patients om PSA testing during an early detection of cancer examination. Urologists were in favor of starting screening at an earlier age if the patient had a family history (31). In addition, since being Afro-Caribbean was an important factor to consider, some urologists performed PSA at an early age (40 years) and up to 75 years (32) in these patients. Urologists indicated that existing guidelines were not adapted to Afro-Caribbean patients.
4 Discussion
The review’s main findings reveal that GPs exhibited a lower level of knowledge concerning PCa risk factors and clinical practice guidelines for PSA usage than urologists. This knowledge gap contributes to GPs being less inclined to adhere to available recommendations. In addition, there were differences in opinion on the usefulness of the PSA test. Volk et al. (34) noted that medical specialty was a variable related to the probability of screening, with GPs more likely to use PSA test than internal medicine clinicians. This discrepancy may be attributed to the practice setting, as some clinicians, such as urologists, typically work in inpatient settings where preventive care is less implemented. In addition, only near 50% of GPs and urologists carried out SDM with patients for PCa screening with PSA test.
Most studies included in this review indicated that the main reason for GPs to screen patients with recognized PCa risk factors was their knowledge of these factors. However, studies involving GPs consistently showed a generally lower awareness of recommended PSA test applications and the associated PCa risk factors than urologists.
Most of the surveyed clinicians, aligned with previous studies conducted in Ireland and the USA (35), knew that having a relative with PCa and being older than 50 years old were risk factors for PCa. However, a low percentage of clinicians knew that having a first-degree relative with breast cancer increased the risk for PCa, even though in 2020, the EAU incorporated the recommendation to offer early PSA testing to well-informed men aged over 40 with BRCA2 mutations. In line with previous studies (36), a significant finding in this review was that more than 50% of surveyed GPs tended to overestimate the positive predictive value of PSA (22), possibly indicating a lack of awareness among clinicians, potentially resulting in excessive screening and inadequate information provided to patients about the PSA test.
Some studies reported disagreement among GPs regarding the age range at which the test should be offered (26). In contrast, urologists, demonstrated a more proactive stance (11) expressing a willingness to initiate screening at an earlier age for patients with a family history of PCa (31). A previous study carried out in the United States found no differences between urologists and primary care clinicians in the number of PSA tests carried out (37), which could be explained by the differences in health care systems.
Clinicians’ awareness of clinical practice guidelines was generally low, and even those who were aware did not consistently follow them in routine practice (23). Previous research also showed that clinicians generally had favorable attitudes toward clinical guidelines, but that only one-third used them very often or often (38). This lack of adherence could be attributed to the constant updates and lack of consensus in guidelines, which lead to confusion (26). Some GPs, although unaware of clinical practice guidelines, expressed a desire for more information related to PSA testing (26). Urologists, on the other hand, argued that existing guidelines were not adapted to high-risk patients, such as Afro-Caribbean patients (32).
Previous studies indicated that clinicians’ insufficient knowledge was linked to variation in PSA testing practices (39, 40). This systematic review further revealed that clinicians with lower PSA knowledge tended to request testing in younger patients and were less likely to question the test’s usefulness. Overall, GPs exhibited an unfavorable opinion of PSA, half of them stating that they would probably not recommend the test to their relatives, emphasizing perceived risks outweighing benefits. In contrast, urologists generally held a positive opinion of PCa screening with PSA, especially for patients at higher risk of PCa.
Less than half of the included studies assessed the implementation of SPM in practice. Both GPs and urologists were found to involve patients in SPM on PCa screening at a rate of 50% or less, highlighting a potential gap in this context. The lack of shared decision-making when ordering PSA screening is of relevant concern. Evidence suggests that clinicians have traditionally underestimated the adverse impact of PSA determination (11), and consequently, it is rarely explained to patients (41), although several studies show that most wish to be informed (26). In this review, it was shown that GPs rarely discussed PSA screening with their patients, although it is critical to help them to make informed decisions regarding screening. Major professional organizations have strongly recommended that patients be fully informed about the pros, cons, and uncertainties of PSA screening, enabling them to make a decision based on their specific clinical and personal characteristics (42). Information regarding test properties such as the likelihood of having a false-positive result or overdiagnosis are not frequently explained to patients (43) and should be explained in the context of their characteristics.
The findings of this systematic review shed some light on the complexity of decision making in oncology, which leads patients and clinicians to consider the benefits and risks of an increasing number of clinical options. Patients and clinicians evaluate the options differently, and therefore, all relevant information and personal preferences are needed to make a decision. This review has also shown that a clinician’s personal beliefs and specialization can influence the use of PSA testing (32), leading to significant variability in practice. These results are consistent with those observed prior to the guideline update, indicating that physicians’ knowledge, beliefs and practices regarding PSA testing have not been influenced by the available recommendations. Hence, and in accordance with the recent recommendations from the European Association of Urology (EAU) (6), clinicians should receive more training in PSA testing.
The overarching strength of this study was the comparison between urologists and GPs given the different roles of these clinicians in opportunistic PCa screening. In addition, the different analyses of the clinicians’ knowledge, beliefs and practice allow us to evaluate different aspects that may influence the recommendation for opportunistic PCa screening.
This systematic review has, however, some limitations. The review was restricted by some terms, e.g., and some relevant studies may not have been included. However, in relation to the language limitation, although we restricted the search to English and Spanish, we also checked for publication in other languages and there were no studies that met the eligibility criteria. This review did not identify studies that evaluated clinicians’ knowledge on the use of genetic biomarkers together with PSA detection for PCa screening. However, the use of additional tests, such as certain genes or molecules shed into urine—TMPTSS2:ERG gene fusions or PCA3 mRNA—has been suggested as a way to reduce overdiagnosis (33). However, GPs usually considered the presence of patient risk factors such as race, age or family history when ordering a PSA, although they were less in favour of carrying out PSA determination than urologists. Thus, they could also support the inclusion of other risk factors, such as genetic risk stratification, which will allow them to advance toward personalized management of the patient. We did not register the protocol of this systematic review in PROSPERO (44). Registration minimizes unintentional duplication of systematic reviews and enhance transparency in the review process, thereby mitigating reporting bias. However, this systematic review conforms to reporting Guidelines PRISMA and a protocol has also included. The adherence to the 22 STROBE criteria demonstrated a high median compliance, with only three studies falling below the first quartile. Most unmet criteria were associated with conducting sensitivity analyses, reporting the estimation of the sample size, and handling quantitative variables. Importantly, these criteria are not directly linked to information bias in the selection process, suggesting that their omission may have minimal impact on the precision of the results.
5 Conclusion
From the findings of this review and considering the new recommendations published by the European Commission and Urologist Associations (5–8), we identify the need to carry out education interventions with trusted resources based on the available evidence and the current guidelines, mainly in the implementation in practice of SDM. This knowledge will allow health professionals to develop shared decision-making with patients when ordering a PSA.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
ME-O: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft. CC: Data curation, Methodology, Writing – review & editing. AM-L: Data curation, Methodology, Writing – review & editing. LP: Data curation, Formal analysis, Methodology, Writing – review & editing. JC-R: Data curation, Formal analysis, Methodology, Writing – review & editing. BL: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Research funded by the research project of the Instituto de Salud Carlos III, code 267 PI20/01334, Principal Investigator BL Lacarra, co-financed with FEDER funds from the European Union “A way of doing Europe”. CIBER in Epidemiology and Public Health, CIBERESP.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2024.1283654/full#supplementary-material
References
1. Vickers, AJ. Prostate Cancer screening: time to question how to optimize the ratio of benefits and harms. Ann Intern Med. (2017) 167:509–10. doi: 10.7326/M17-2012
2. Hugosson, J, Roobol, MJ, Månsson, M, Månsson, M, Tammela, TLJ, Zappa, M, et al. A 16-yr follow-up of the European randomized study of screening for prostate Cancer. Eur Urol. (2019) 76:43–51. doi: 10.1016/j.eururo.2019.02.009
3. Pinsky, PF, Prorok, PC, Yu, K, Kramer, BS, Black, A, Gohagan, JK, et al. Extended mortality results for prostate cancer screening in the PLCO trial with median follow-up of 15 years. Cancer. (2017) 123:592–9. doi: 10.1002/cncr.30474
4. Tsodikov, A, Gulati, R, Heijnsdijk, EAM, Pinsky, PF, Moss, SM, Qiu, S, et al. Reconciling the effects of screening on prostate Cancer mortality in the ERSPC and PLCO trials. Ann Intern Med. (2017) 167:449–55. doi: 10.7326/M16-2586
5. Heijnsdijk, EAM, Bangma, CH, Borràs, JM, de Carvalho, TM, Castells, X, Eklund, M, et al. Summary statement on screening for prostate cancer in Europe. Int J Cancer. (2018) 142:741–6. doi: 10.1002/ijc.31102
6. US Preventive Services Task ForceGrossman, DC, Curry, SJ, Owens, DK, Bibbins-Domingo, K, Caughey, AB, et al. Screening for prostate Cancer: US preventive services task force recommendation statement. JAMA. (2018) 319:1901–13. doi: 10.1001/jama.2018.3710
7. Mottet, N, van den Bergh, RCN, Briers, E, van den Broeck, T, Cumberbatch, MG, de Santis, M, et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate Cancer-2020 update. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. (2021) 79:243–62. doi: 10.1016/j.eururo.2020.09.042
8. Van Poppel, H, Hogenhout, R, Albers, P, van den Bergh, RCN, Barentsz, JO, and Roobol, MJ. Early detection of prostate Cancer in 2020 and beyond: facts and recommendations for the European Union and the European Commission. Eur Urol. (2021) 79:327–9. doi: 10.1016/j.eururo.2020.12.010
9. Council on recommendation on strengthening prevention through early detection: a new EU approach on cancer screening, Sept 2022. Available at: https://ec.europa.eu/commission/presscorner/detail/en/QANDA_22_5584
10. Eales, OO, and Smith, S. Do socio-economically disadvantaged patients prefer shared decision-making? S Afr Fam Pract. (2021) 63:e1–6. doi: 10.4102/safp.v63i1.5293
11. Kappen, S, Jürgens, V, Freitag, MH, and Winter, A. Early detection of prostate cancer using prostate-specific antigen testing: an empirical evaluation among general practitioners and urologists. Cancer Manag Res. (2019) 11:3079–97. doi: 10.2147/CMAR.S193325
12. Drummond, FJ, Carsin, AE, Sharp, L, and Comber, H. Factors prompting PSA-testing of asymptomatic men in a country with no guidelines: a national survey of general practitioners. BMC Fam Pract. (2009) 10:3. doi: 10.1186/1471-2296-10-3
13. Leyva, B, Persoskie, A, Ottenbacher, A, Hamilton, JG, Allen, JD, Kobrin, SC, et al. Do men receive information required for shared decision making about PSA testing? Results from a national survey. J Cancer Educ. (2016) 31:693–701. doi: 10.1007/s13187-015-0870-8
14. Jemal, A, Fedewa, SA, Ma, J, Siegel, R, Lin, CC, Brawley, O, et al. Prostate Cancer incidence and PSA testing patterns in relation to USPSTF screening recommendations. JAMA. (2015) 314:2054–61. doi: 10.1001/jama.2015.14905
15. Squiers, LB, Bann, CM, Dolina, SE, Tzeng, J, McCormack, L, and Kamerow, D. Prostate-specific antigen testing: men’s responses to 2012 recommendation against screening. Am J Prev Med. (2014) 314:182, 2054–2189. doi: 10.1016/j.amepre.2013.04.005
16. Tasian, GE, Cooperberg, MR, Cowan, JE, Keyashian, K, Greene, KL, Daniels, NA, et al. Prostate specific antigen screening for prostate cancer: knowledge of, attitudes towards, and utilization among primary care physicians. Urol Oncol. (2012) 30:155–60. doi: 10.1016/j.urolonc.2009.12.019
17. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
18. Schardt, C, Adams, MB, Owens, T, Keitz, S, and Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak. (2007) 7:16. doi: 10.1186/1472-6947-7-16
19. Ouzzani, M, Hammady, H, Fedorowicz, Z, and Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
20. von Elm, E, Altman, DG, Egger, M, Pocock, SJ, Gøtzsche, PC, Vandenbroucke, JP, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. (2007) 370:1453–7. doi: 10.1016/S0140-6736(07)61602-X
21. Elstad, EA, Sutkowi-Hemstreet, A, Sheridan, SL, Vu, M, Harris, R, Reyna, VF, et al. Clinicians' perceptions of the benefits and harms of prostate and colorectal cancer screening. Med Decis Mak. (2015) 35:467–76. doi: 10.1177/0272989X15569780
22. Tun Firzara, AM, and Ng, CJ. Knowledge and practice of prostate cancer screening among general practitioners in Malaysia: a cross-sectional study. BMJ Open. (2016) 6:e011467. doi: 10.1136/bmjopen-2016-011467
23. Miller, A, Yates, J, Epstein, MM, Fantasi, J, Frendl, D, Afiadata, A, et al. Impact of 2012 USPSTF screening PSA guideline statement: changes in primary care provider practice patterns and attitudes. Urol Pract. (2017) 4:126–31. doi: 10.1016/j.urpr.2016.04.003
24. Panach-Navarrete, J, Gironés-Montagud, A, Sánchez-Cano, E, Doménech-Pérez, C, and Martínez-Jabaloyas, JM. Use of prostatic specific antigen in primary care (PSA). SEMERGEN. (2017) 43:189–95. doi: 10.1016/j.semerg.2016.04.023
25. Hall, IJ, Rim, SH, Massetti, GM, Thomas, CC, Li, J, and Richardson, LC. Prostate-specific antigen screening: an update of physician beliefs and practices. Prev Med. (2017) 103:66–9. doi: 10.1016/j.ypmed.2017.08.004
26. Giménez, N, Filella, X, Gavagnach, M, Allué, JA, Pedrazas, D, and Ferrer, F. Grupo de Estudio sobre Cribado en Cáncer de Próstata. Prostate cancer screening using prostate-specific antigen: the views of general and laboratory physicians. Semergen. (2018) 44:409–19. doi: 10.1016/j.semerg.2018.02.001
27. Nassir, AM, Baazeem, A, Saada, H, Elkoushy, MA, Badr, H, Bahuwyrith, M, et al. Urological knowledge among primary health care physicians in Saudi Arabia. Saudi Med J. (2019) 40:483–9. doi: 10.15537/smj.2019.5.24080
28. Kappen, S, Koops, L, Jürgens, V, Freitag, MH, Blanker, MH, Timmer, A, et al. General practitioners' approaches to prostate-specific antigen testing in the north-east of the Netherlands. BMC Fam Pract. (2020) 21:270. doi: 10.1186/s12875-020-01350-3
29. Shungu, N, Diaz, VA, Perkins, S, and Kulshreshtha, A. Physician attitudes and self-reported practices toward prostate Cancer screening in Black and White men. Fam Med. (2022) 54:30–7. doi: 10.22454/FamMed.2022.474827
30. Rudichuk, L, Vogel, KJ, Wang, CH, Helfand, BT, and Selkirk, CG. Urologists' current practices in screening and treating men with a family history of prostate Cancer. Urology. (2017) 99:180–5. doi: 10.1016/j.urology.2016.07.032
31. Persaud, S, and Aiken, WD. Prostate-specific antigen-based screening in afro-Caribbean men: a survey of members of the Caribbean urological association. Ecancermedicalscience. (2018) 12:842. doi: 10.3332/ecancer.2018.842
32. Briss, P, Rimer, B, Reilley, B, Coates, RC, Lee, NC, Mullen, P, et al. Task force on community preventive services. Promoting informed decisions about cancer screening in communities and healthcare systems. Am J Prev Med. (2004) 26:67–80. doi: 10.1016/j.amepre.2003.09.012
33. Hoffmann, TC, and Del Mar, C. Patients' expectations of the benefits and harms of treatments, screening, and tests: a systematic review. JAMA Intern Med. (2015) 175:274–86. doi: 10.1001/jamainternmed.2014.6016
34. Volk, RJ, Linder, SK, Kallen, MA, Galliher, JM, Spano, MS, Mullen, PD, et al. Primary care physicians' use of an informed decision-making process for prostate cancer screening. Ann Fam Med. (2013) 11:67–74. doi: 10.1370/afm.1445
35. Tasian, GE, Cooperberg, MR, Potter, MB, Cowan, JE, Greene, KL, Carroll, PR, et al. PSA screening: determinants of primary-care physician practice patterns. Prostate Cancer Prostatic Dis. (2012) 15:189–94. doi: 10.1038/pcan.2011.59
36. Mistry, K, and Cable, G. Meta-analysis of prostate-specific antigen and digital rectal examination as screening tests for prostate carcinoma. J Am Board Fam Pract. (2003) 16:95–101. doi: 10.3122/jabfm.16.2.95
37. Zavaski, ME, Meyer, CP, Sammon, JD, Hanske, J, Gupta, S, Sun, M, et al. Differences in prostate-specific antigen testing among urologists and primary care physicians following the 2012 USPSTF recommendations. JAMA Intern Med. (2016) 176:546–7. doi: 10.1001/jamainternmed.2015.7901
38. Birrenbach, T, Kraehenmann, S, Perrig, M, Berendonk, C, and Huwendiek, S. Physicians’ attitudes toward, use of, and perceived barriers to clinical guidelines: a survey among Swiss physicians. Adv Med Educ Pract. (2016) 7:673–80. doi: 10.2147/AMEP.S115149
39. Pucheril, D, Dalela, D, Sammon, J, Sood, A, Sun, M, Trinh, QD, et al. The influence of physician recommendation on prostate-specific antigen screening. Urol Oncol. (2015) 33:424.e1–7. doi: 10.1016/j.urolonc.2015.06.013
40. Clements, A, Watson, E, Rai, T, Bukach, C, Shine, B, and Austoker, J. The PSA testing dilemma: GPs’ reports of consultations with asymptomatic men: a qualitative study. BMC Fam Pract. (2007) 8:35. doi: 10.1186/1471-2296-8-35
41. Wilt, TJ, Jones, KM, Barry, MJ, Andriole, GL, Culkin, D, Wheeler, T, et al. Follow-up of prostatectomy versus observation for early prostate Cancer. N Engl J Med. (2017) 377:132–42. doi: 10.1056/NEJMoa1615869
42. Martínez-González, NA, Neuner-Jehle, S, Plate, A, Rosemann, T, and Senn, O. The effects of shared decision-making compared to usual care for prostate cancer screening decisions: a systematic review and meta-analysis. BMC Cancer. (2018) 18:1015. doi: 10.1186/s12885-018-4794-7
43. Ankolekar, A, Dekker, A, Fijten, R, and Berlanga, A. The benefits and challenges of using patient decision aids to support shared decision making in health care. JCO Clin Cancer Inform. (2018) 2:1–10. doi: 10.1200/CCI.18.00013
Keywords: prostate cancer, screening, knowledge, urologists, general practitioner (GP)
Citation: Estevan-Ortega M, de la Encarnación Castellano C, Mendiola-López A, Parker LA, Caballero-Romeu JP and Lumbreras B (2024) Urologists’ and general practitioners’ knowledge, beliefs and practice relevant for opportunistic prostate cancer screening: a PRISMA-compliant systematic review. Front. Med. 11:1283654. doi: 10.3389/fmed.2024.1283654
Edited by:
Alexander Winter, University Hospital for Urology, GermanyReviewed by:
Sakineh Hajebrahimi, Tabriz University of Medical Sciences, IranMatthias May, Klinikum St. Elisabeth Straubing GmbH, Germany
Copyright © 2024 Estevan-Ortega, de la Encarnación Castellano, Mendiola-López, Parker, Caballero-Romeu and Lumbreras. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Blanca Lumbreras, blumbreras@umh.es