 Salvatore D’Angelo1
Salvatore D’Angelo1 Fabiola Atzeni2
Fabiola Atzeni2 Maurizio Benucci3
Maurizio Benucci3 Gerolamo Bianchi4
Gerolamo Bianchi4 Fabrizio Cantini5
Fabrizio Cantini5 Roberto Felice Caporali6,7Giorgio Carlino8
Roberto Felice Caporali6,7Giorgio Carlino8 Francesco Caso9Alberto Cauli10
Francesco Caso9Alberto Cauli10 Francesco Ciccia11
Francesco Ciccia11 Maria Antonietta D’Agostino12
Maria Antonietta D’Agostino12 Lorenzo Dagna13,14Christian Dejaco15,16Oscar Massimiliano Epis17Maria Grazia Ferrucci18
Lorenzo Dagna13,14Christian Dejaco15,16Oscar Massimiliano Epis17Maria Grazia Ferrucci18 Franco Franceschini19,20
Franco Franceschini19,20 Enrico Fusaro21Marco Gabini22
Enrico Fusaro21Marco Gabini22 Roberto Gerli23
Roberto Gerli23 Roberto Giacomelli24,25
Roberto Giacomelli24,25 Marcello Govoni26
Marcello Govoni26 Elisa Gremese27
Elisa Gremese27 Giuliana Guggino28
Giuliana Guggino28 Annamaria Iagnocco29
Annamaria Iagnocco29 Florenzo Iannone30
Florenzo Iannone30 Bruno Laganà31Ennio Lubrano32
Bruno Laganà31Ennio Lubrano32 Carlomaurizio Montecucco33
Carlomaurizio Montecucco33 Rosario Peluso34
Rosario Peluso34 Roberta Ramonda35
Roberta Ramonda35 Maurizio Rossini36
Maurizio Rossini36 Carlo Salvarani37Gian Domenico Sebastiani38
Carlo Salvarani37Gian Domenico Sebastiani38 Marco Sebastiani39
Marco Sebastiani39 Carlo Selmi40,41Enrico Tirri42
Carlo Selmi40,41Enrico Tirri42 Antonio Marchesoni43,44*
Antonio Marchesoni43,44*- 1Rheumatology Department of Lucania, San Carlo Hospital of Potenza, Potenza, Italy
- 2Rheumatology Unit, Department of Experimental and Internal Medicine, University of Messina, Messina, Italy
- 3Rheumatology Unit, S. Giovanni di Dio Hospital, Florence, Italy
- 4Division of Rheumatology, Department of Medical Specialties, Azienda Sanitaria Locale 3 Genovese, Genova, Italy
- 5Private Practice, Prato, Italy
- 6Division of Clinical Rheumatology, ASST Gaetano Pini-CTO Institute, Milan, Italy
- 7Department of Clinical Sciences and Community Health, University of Milan, Milan, Italy
- 8Rheumatology Service, ASL LE-DSS Casarano and Gallipoli, Gallipoli, Italy
- 9Department of Clinical Medicine and Surgery, University of Naples Federico II, Naples, Italy
- 10Rheumatology Unit, Department of Medicine and Public Health, AOU and University of Cagliari, Cagliari, Italy
- 11Rheumatology Section, Department of Precision Medicine, University of Campania "Luigi Vanvitelli", Naples, Italy
- 12Department of Rheumatology, Catholic University of Sacred Heart, Fondazione Policlinico Universitario A. Gemelli, IRCSS, Rome, Italy
- 13Unit of Immunology, Rheumatology, Allergy and Rare Diseases (UnIRAR), San Raffaele Scientific Institute, Milan, Italy
- 14School of Medicine, Vita-Salute San Raffaele University, Milan, Italy
- 15Department of Rheumatology and Immunology, Medical University of Graz, Graz, Austria
- 16Department of Rheumatology, Teaching Hospital of the Paracelsius Medical University, Brunico Hospital (ASAA-SABES), Brunico, Italy
- 17Division of Rheumatology, Multispecialist Medical Department, ASST Grande Ospedale Metropolitano Niguarda, Milan, Italy
- 18Department of Rheumatology, Azienda Ospedaliera Rummo Benevento, Benevento, Italy
- 19Rheumatology and Clinical Immunology Unit, Dipartimento Continuità di Cure e Fragilità, ASST Spedali Civili di Brescia, Brescia, Italy
- 20Department of Clinical and Experimental Sciences, University of Brescia, Brescia, Italy
- 21Rheumatology Unit, University Hospital AOU Città della Salute e della Scienza di Torino, Turin, Italy
- 22Rheumatology Unit, Santo Spirito Hospital, Pescara, Italy
- 23Rheumatology Unit, Department of Medicine and Surgery, University of Perugia, Perugia, Italy
- 24Research Unit of Immuno-Rheumatology, Department of Medicine, School of Medicine, University of Rome "Campus Biomedico", Rome, Italy
- 25Fondazione Policlinico Campus Bio-Medico, Rome, Italy
- 26Rheumatology Unit, Department of Medical Sciences, Azienda Ospedaliero-Universitaria S. Anna-Ferrara, University of Ferrara, Ferrara, Italy
- 27Clinical Immunology Unit, Department of Geriatrics, Orthopedics and Rheumatology, Fondazione Policlinico Universitario A. Gemelli-IRCCS, Catholic University of the Sacred Heart, Rome, Italy
- 28PROMISE, Università degli studi di Palermo, Palermo, Italy
- 29Academic Rheumatology Centre, Department of Clinical and Biological Sciences, Università degli Studi di Torino, Turin, Italy
- 30DiMePRe-J, Rheumatology Unit, Università degli studi di Bari “Aldo Moro”, Bari, Italy
- 31Department of Clinical and Molecular Medicine, Sapienza University of Rome-S. Andrea University Hospital, Rome, Italy
- 32Academic Rheumatology Unit, Department of Medicine and Health Sciences "Vincenzo Tiberio", Università Degli Studi del Molise, Campobasso, Italy
- 33Department of Internal Medicine and Therapeutics, Rheumatology Unit, University of Pavia, IRCCS Policlinico S. Matteo, Pavia, Italy
- 34Department of Clinical Medicine and Surgery, School of Medicine, University Federico II of Naples, Naples, Italy
- 35Rheumatology Unit+ EULAR Center of Excellence in Rheumatology, Department of Medicine-DIMED, University of Padova, Padua, Italy
- 36Rheumatology Unit, Department of Medicine, University of Verona, Verona, Italy
- 37Azienda USL-IRCCS di Reggio Emilia, Università di Modena e Reggio Emilia, Reggio Emilia, Italy
- 38Rheumatology, Azienda Ospedaliera San Camillo Forlanini, Rome, Italy
- 39Rheumatology Unit, CHIMOMO, University of Modena and Reggio Emilia, Modena, Italy
- 40Department of Biomedical Sciences, Humanitas University, Pieve Emanuele, Italy
- 41Department of Rheumatology and Clinical Immunology, Humanitas Clinical and Research Center-IRCCS, Rozzano, Italy
- 42Rheumatology Unit, Ospedale del Mare, Naples, Italy
- 43Rheumatology, Humanitas San Pio X, Milan, Italy
- 44Ospedale S. Maria Nuova, Reggio Emilia, Italy
Background: Psoriatic arthritis (PsA) is a chronic inflammatory musculoskeletal disease involving several articular and extra-articular structures. Despite the important progresses recently made in all of the aspects of this disease, its management is still burdened by unresolved issues. The aim of this exercise was to provide a set of statements that may be helpful for the management of PsA.
Methods: A group of 38 Italian rheumatologists with recognized expertise in PsA selected and addressed the following four topics: “early PsA,” “axial-PsA,” “extra-articular manifestations and comorbidities,” “therapeutic goals.” Relevant articles from the literature (2016–2022) were selected by the experts based on a PubMed search. A number of statements for each topic were elaborated.
Results: Ninety-four articles were selected and evaluated, 68 out of the 1,114 yielded by the literature search and 26 added by the Authors. Each of the four topic was subdivided in themes as follows: transition from psoriasis to PsA, imaging vs. CASPAR criteria in early diagnosis, early treatment for “early PsA”; axial-PsA vs. axialspondyloarthritis, diagnosis, clinical evaluation, treatment, standard radiography vs. magnetic resonance imaging for “axial PsA”; influence of inflammatory bowel disease on the therapeutic choice, cardiovascular comorbidity, bone damage, risk of infection for “comorbidities and extra-articular manifestations”; target and tools, treat-to-target strategy, role of imaging for “therapeutic goals.” The final document consisted of 49 statements.
Discussion: The final product of this exercise is a set of statements concerning the main issues of PsA management offering an expert opinion for some unmet needs of this complex disease.
1 Introduction
Psoriatic arthritis (PsA) is a chronic inflammatory musculoskeletal disease associated with psoriasis, or a predisposition to this skin disorder, which may involve joints, entheses, and the axial skeleton. In addition, PsA may be associated with extra-articular manifestations such as inflammatory bowel disease (IBD) and uveitis, and with a number of comorbidities, first of all those metabolic in nature.
Articular and extra-articular manifestations, as well as comorbidities, may have a profound impact on the quality of life of patients with PsA and may even be responsible for a shorter life expectancy (1–5). Early diagnosis, comprehensive disease assessment, and proper treatment are the mainstays to guarantee the best outcome of PsA patients, both in the short and long-term. In the past two decades, relevant research progresses have been made in understanding pathophysiology and defining clinical phenotypes (6–11), and therapies targeting new mechanisms of action have been developed (12). Despite these improvements, the management of PsA is still difficult and many unresolved questions in this field await an answer (13).
To provide a guidance in this complex topic, a group of Italian rheumatologists with expertise in PsA (Expert Group: EG) convened to elaborate, through a consensus process, a number of statements addressing some of the main issues of diagnosis, assessment, and treatment of PsA.
2 Methods
Thirty-eight Italian rheumatologists with leading roles and expert in PsA agreed to participate to this consensus study. The expert group was composed on the basis of the following criteria:
• Clinical experience in psoriatic arthritis management.
• Research activity in psoriatic arthritis disease.
• Participation in disease-specific guidelines and scientific committees, indicating a commitment to improving standards of care and promoting best practices in disease management.
• Participation in conferences and congresses as a speaker, demonstrating commitment to the scientific community and the opportunity to share the latest findings and establish collaborative links.
Fifteen of them constituted a steering committee which selected, among several “hot” general topics in the management of PsA considered of interest, the following four for their relevance: early PsA, axial PsA, comorbidities and extra-articular manifestations, and therapeutic goals. The process was then structured in subsequent steps.
In the firststep, the steering committee explored the main issues concerning the four selected topics, evaluated a literature review previously performed, and defined the specific items to be addressed. The literature review was carried out by an independent methodologist in the Medline via PubMed using as searching definition “psoriatic arthritis AND early,” “psoriatic arthritis AND axial,” “psoriatic arthritis AND comorbidity,” “psoriatic arthritis AND extraarticular manifestations,” and “psoriatic arthritis AND therapy.” Only references in English and published within January 1st, 2016 and December 31st, 2021 were selected. The methodologist performed a first screening of the retrieved records by title and summary and excluded all those not relevant to the search question. Duplicates were marked to be removed from the final manuscript count but left for evaluation by any individual subgroups (see below). The remaining records were evaluated by the steering committee, which selected only the manuscript considered of interest. The final selection was then forwarded to the EG, which was subdivided into four subgroups, one for each of the topics previously defined by the steering committee. Finally, as the various consensus rounds were eventually held in 2022, manuscripts published in 2022 and considered of relevance by the components of the EG were also included in the literature evaluation.
For the second step, each of the four subgroups convened online to discuss the themes of interest and elaborate a number of statements relevant to any individual theme. These statements were then evaluated through a Delphi-like process (14). Each of them was voted by the components of the steering committee using a 9-point scale (ranging from 1, strongly disagree to 9, strongly agree). Then, median scores were calculated for each statement: a median score greater than or equal to 7 was considered a positive consensus, between 3 and 7 a neutral opinion, and lower than 3 a negative consensus. Individual responses were anonymous to preserve objectivity. The statements with a negative consensus were discussed, modified if needed, and then voted again until an agreement was reached. The final product for each working group was a document containing the approved statements.
In the third step, the final four documents were submitted for anonymous evaluation to the entire panel of participating rheumatologists and each statement was scored as reported above.
3 Results
The steering committee selected and evaluated 68 of the 1,114 articles originally yielded by the literature search, to which were added another 26 manuscripts published in 2022 and considered relevant to the various topics (Figure 1).
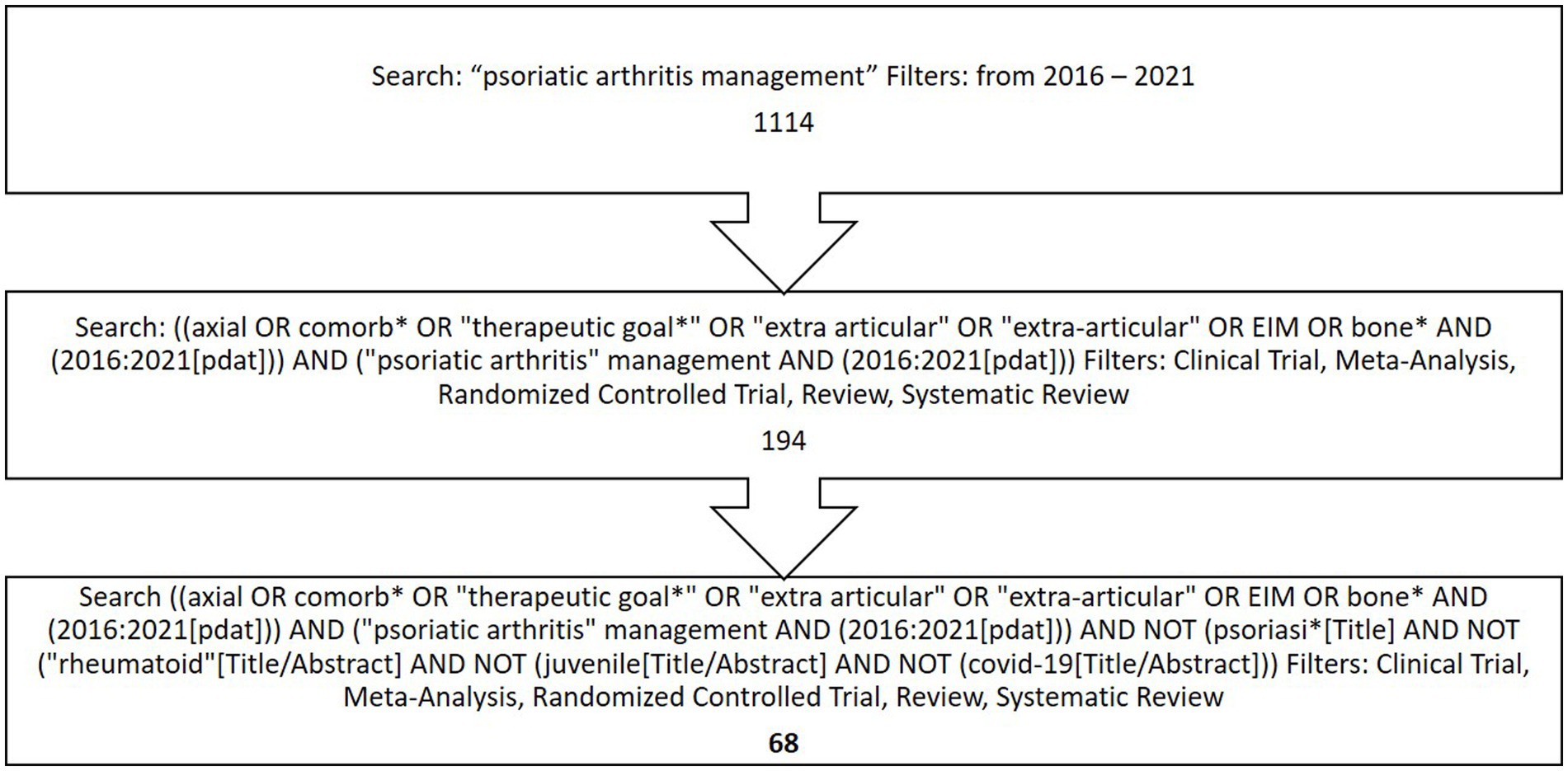
Figure 1. Flowchart describing the literature selection process.
After the various rounds, the final document consisted of 49 statements subdivided as follows: 11 for “early PsA” (Table 1A), 12 for “axial-PsA” (Table 1B), 19 for “comorbidities and extra-articular manifestations” (Table 1C), and 7 for “therapeutic goals” (Table 1D). The themes of interest explored by the EG were the following:
• for “early PsA”: transition from psoriasis to PsA, imaging vs. CASPAR criteria in early diagnosis, and early treatment.
• for “axial PsA”: axial-PsA vs. axial-spondyloarthritis (SpA), diagnosis, clinical evaluation, treatment, and standard radiography vs. MRI.
• for “comorbidities and extra-articular manifestations”: influence of IBD on the therapeutic choice, cardiovascular comorbidity, bone damage, and risk of infection.
• for “therapeutic goals”: target and tools, treat-to-target (T2T) strategy, and role of imaging.

Table 1A. Statements stemming from the discussion of the topic “Early PsA” and the score, out of a 9-point scale, they received from the consensus group.
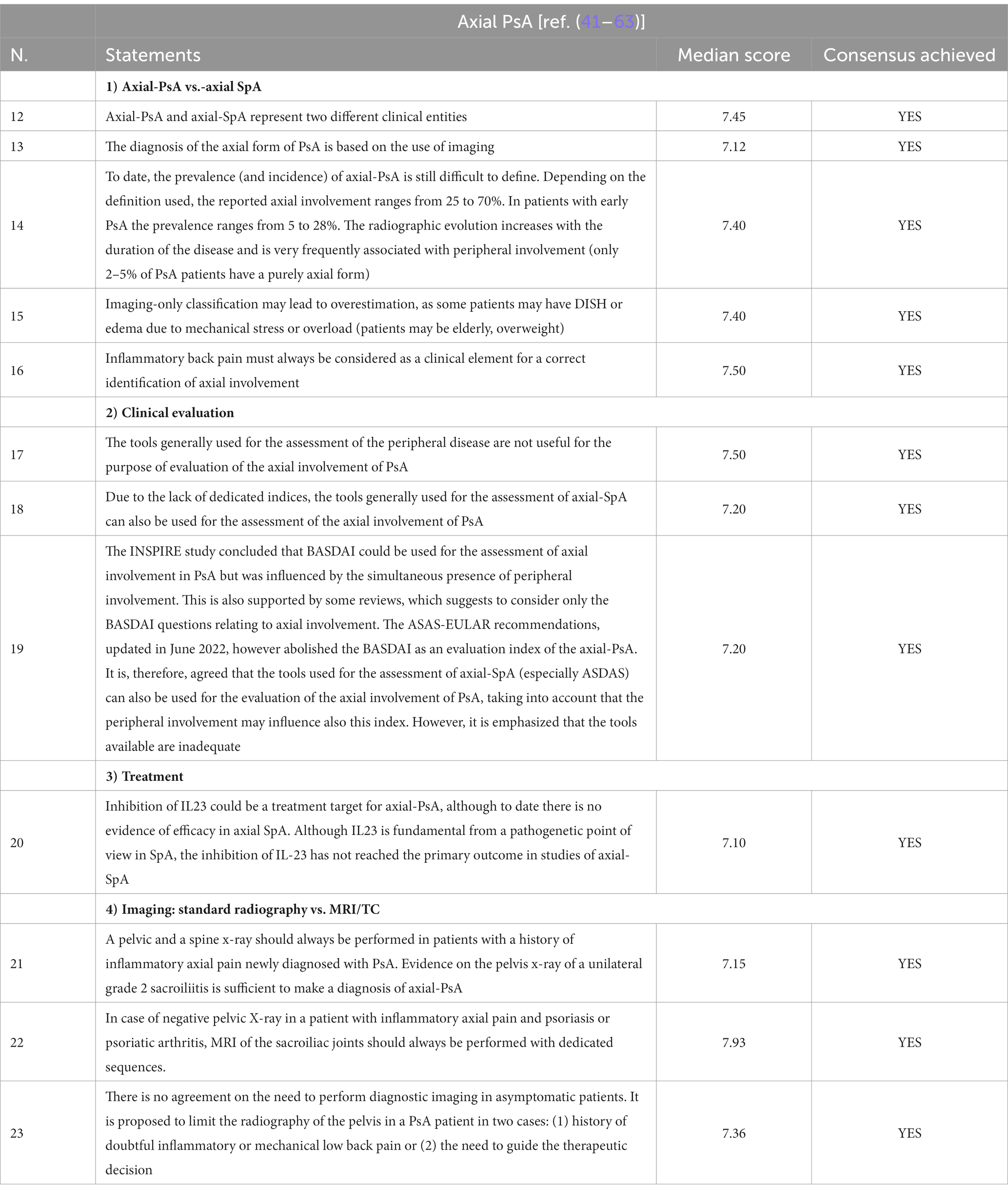
Table 1B. Statements stemming from the discussion of the topic “Axial PsA” and the score, out of a 9-point scale, they received from the consensus group.
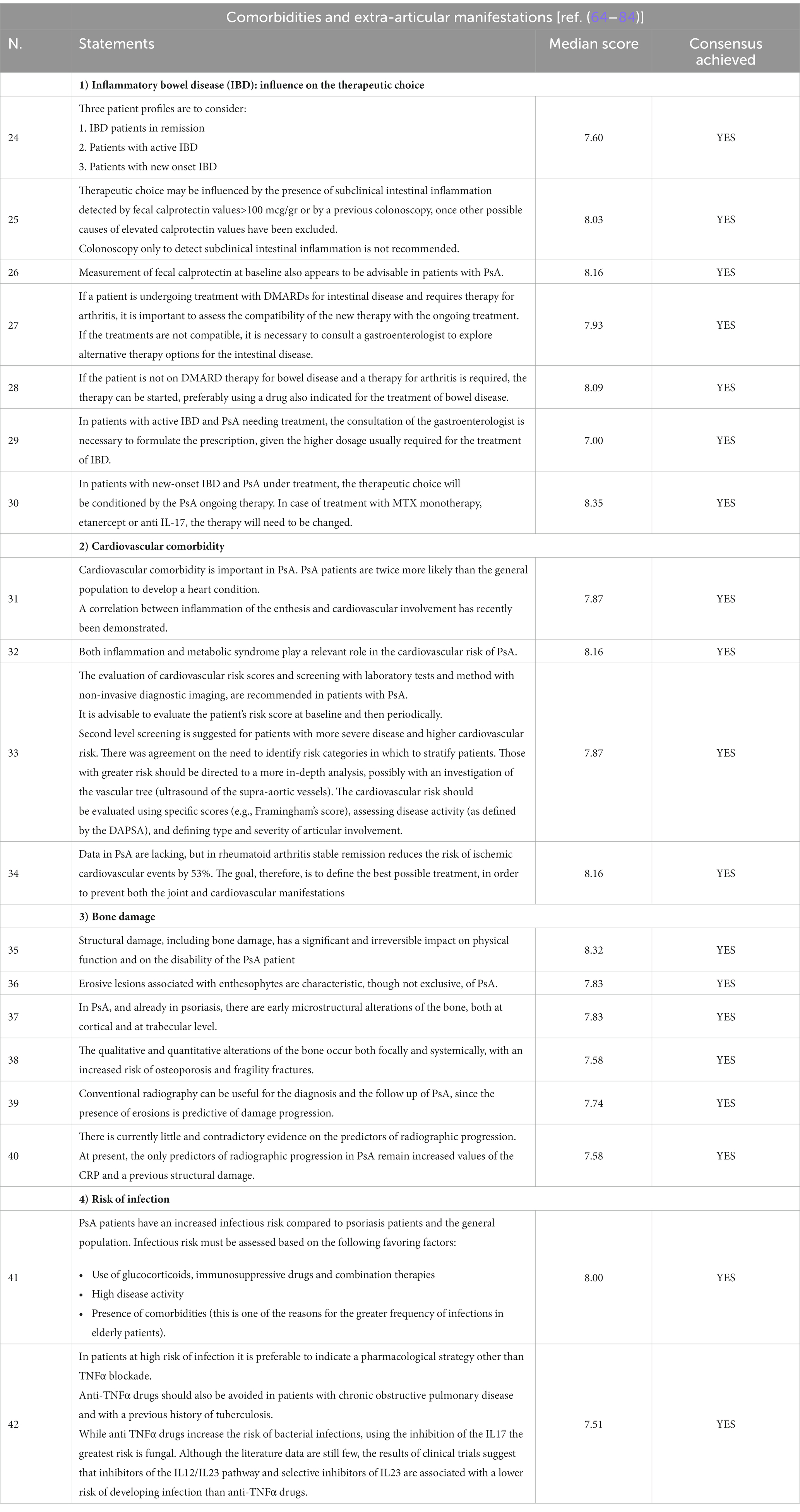
Table 1C. Statements stemming from the discussion of the topic “Comorbidities and extra-articular manifestations” and the score, out of a 9-point scale, they received from the consensus group.
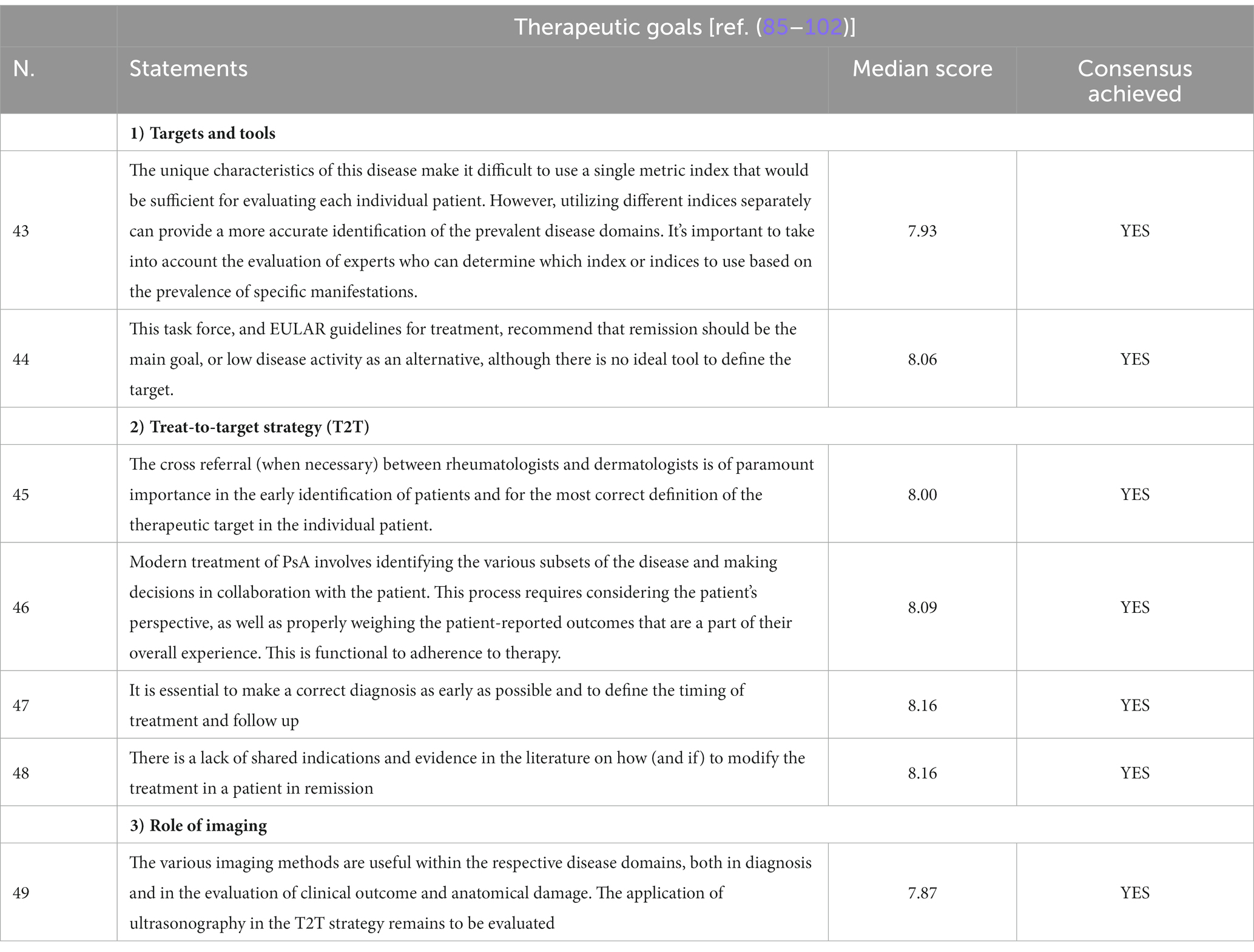
Table 1D. Statements stemming from the discussion of the topic “Therapeutic goals” and the score, out of a 9-point scale, they received from the consensus group.
All of the themes of interest and relative approved statements are reported in Table 1. Results can be summarized for each specific theme as follows: (i) dermatologists are important in detecting PsA and early diagnosis and treatment are likely to be of great benefit, (ii) there are large knowledge gaps in the distinction between axial-PsA and axial-SpA, on how to diagnose axial PsA, its prevalence, how to assess it, and how to treat it; (iii) associated conditions and comorbidities of major clinical relevance include IBD, cardiovascular and metabolic disturbances and bone damage; and (iv) measuring treatment targets in PsA should be based on instruments more suitable for the clinical manifestations of each individual patient.
4 Discussion
The purpose of this consensus study was to provide an expert opinion on some issues concerning the management of patients with PsA. The choice of the topics to be addressed was arbitrarily made by the steering committee of the EG. Many other themes would have been of interest, but the four selected subjects were considered among the most relevant for the clinical management of PsA patients and are all included in the research agenda of the recent recommendations developed by EULAR (62) and GRAPPA (63).
The “early PsA” topic was mainly focused on the transition from psoriasis to PsA and early diagnosis and treatment. It was agreed that, despite the advances in the pathophysiology knowledge (6, 15–21), prediction of the transition at a molecular level is still not possible. Thus, the dermatologist ability to detect the psoriatic patients at risk of PsA should be enhanced as much as possible. Although ultrasound (US) imaging and magnetic resonance imaging (MRI) are not always specific for PsA, their use may help for its early diagnosis, classification and assessment (30–32). However, it is worth noting that the statement on the US and MRI imaging was the one with the lowest agreement (7.25) of this topic, indicating that the role of these imaging techniques in early PsA needs to be studied further. Finally, even if the evidence is scarce, it was underlined that early treatment of PsA may guarantee the best outcome, while more data are needed to prove that treating psoriatic patients with immunosuppressive drugs may prevent the transition to PsA (38–40). Overall, the EG agrees that that dermatologists play an important role in detecting PsA and that early diagnosis and treatment are likely to be of great benefit.
Globally, the topic “axial-PsA,” showed the lowest rate of agreement, with only one statement (“In case of negative pelvic X-ray in a patient with inflammatory axial pain and psoriasis or psoriatic arthritis, MRI of the sacroiliac joints should always be performed with dedicated sequences”) reaching a score of nearly 8. This result likely mirrors the well-known controversies concerning this theme. The first statement about this topic was that axial-PsA and axial-SpA likely represent two different entities. As the evidence on this subject is not conclusive, it could be argued that this statement only reflects personal opinions. However, based on genetic factors and clinical and radiographic findings, a growing number of experts in the field are supporting the concept that axial-PsA and axial-SpA cannot be considered the same entity (42–47). Many other questions on this topic remain unanswered: how to diagnose axial PsA, its prevalence, how to assess it, and how to treat it. As for the diagnosis, it was reasoned that diagnosis should be based on imaging, using radiography as first technique, which, however, should be performed only in symptomatic patients. Inflammatory back pain should always be sought for in patients with PsA. An imaging-driven diagnosis of axial PsA will exclude patients with axial involvement without radiographic or MRI changes. This choice was made to avoid the risk of diagnosing as axial PsA all psoriatic patients with back pain. In addition, it was considered not appropriate to perform axial imaging investigation in all patients, regardless of their symptoms. For the assessment of axial PsA, given the lack of specific instruments, it was indicated that the BASDAI and, preferably, the ASDAS may be used. Finally, for the treatment, as all of the recommendations clearly indicate that anti-TNF-α and IL-17 drugs are the therapy of choice for axial-PsA, only the issue recently arisen of the possible efficacy of anti-IL23 therapies on this disease domain was addressed. The final agreement was that ongoing studies should show whether anti-IL23 therapies are effective to treat axial-PsA (54–56).
The “comorbidity and extra-articular manifestations” topic addressed four themes: IBD, cardiovascular comorbidity, bone damage, and infection risk. As for the IBD, all the various possible clinical occurrences were analyzed. Basically, it was suggested that drugs effective for both the articular and the intestinal disease should be preferred in most cases, to be used with the co-operation of the gastroenterologist whenever needed. Interestingly, it was agreed that the measurement of fecal calprotectin may be advisable in patients with PsA. As there are no data to support this statement, it was only based on the experts’ opinion. It was reckoned that values of fecal calprotectin greater than 100 μg/gr in absence of other possible causes might be due to subclinical intestinal inflammation and thus should be considered for the therapy choice. For the cardiovascular (CV) comorbidity, it was stated that the CV risk should be scored using specific instruments in all patients with PsA and that subjects at elevated risk should undergo in-depth investigations (e.g., supra-aortic vessels ultrasound). Despite the lack of definite evidence, it was felt that proper management of the CV risk factors and of the articular disease should decrease the incidence of CV events. Bone damage was also included in the “comorbidity and extra-articular manifestations” section. The statements on this subject underlined the importance of evaluating the bone damage through standard radiography. Infections are undoubtedly a major concern when immunosuppressive agents are used for the treatment of PsA. It was stated that before starting a therapy, patients should be carefully evaluated particularly for the well-known risk factors of infection and treated accordingly. Although not definitive, the available data indicate that IL-17 and IL-23 inhibitors are less likely to favor bacterial infections than TNF-α blockers (81–85).
The fourth topic, “therapeutic goals,” recorded the highest level of agreement, with most statements reaching a score greater than 8. As indicated by all recent international recommendations (62, 63), remission, or at least a status of minimal disease activity, was considered the goal of the therapy. Given the phenotypic heterogeneity of PsA, it was suggested to assess the disease activity using the instruments more suitable for the clinical manifestations of each individual patient. It was emphasized the importance of cooperating with a dermatologist whenever needed and of considering the patient’s opinion to optimize the adherence. For a personalized T2T approach, it was indicated to define time of intervention and follow-up according to the individual clinical context. The available data on treatment modifications in case of remission were considered not strong enough to provide indications. This opinion is not in line with what indicated in the most recent recommendations on the treatment of PsA, which state that drug tapering, and eventually even drug discontinuation, may be considered in case of disease remission. The EG did not advise against this strategy, but decided that at present the available evidence dot not allow to draw definite conclusions on this issue (100–102). Finally, it was affirmed that imaging is useful to assess disease evolution, but a possible role of the US in a T2T strategy remains to be established.
5 Conclusion
We provide the results of an exercise which, moving from the available literature, resulted in statements on the understanding and management of PsA. The main limitations of this work are that that the period chosen is short and that not all potentially useful literature has been included to answer the research questions, and that the majority of statements are not based on definite evidence and only reflected the opinion of a group of experts, thus being liable to criticism. On the other hand, the purpose of this exercise was to provide an opinion on some unresolved questions regarding the management of PsA and Delphi-like methods are considered acceptable to provide indications when evidence is weak or absent. The choice of the topics to be addressed was arbitrary, yet there was large agreement on their relevance to the practicing rheumatologist.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
SD’A: Formal analysis, Supervision, Writing – original draft, Writing – review & editing. FA: Formal analysis, Supervision, Writing – review & editing. MB: Formal analysis, Writing – review & editing. GB: Formal analysis, Writing – review & editing. FCan: Formal analysis, Writing – review & editing. RC: Formal analysis, Supervision, Writing – review & editing. GC: Formal analysis, Writing – review & editing. FCas: Formal analysis, Writing – review & editing. AC: Formal analysis, Supervision, Writing – review & editing. FCi: Formal analysis, Supervision, Writing – review & editing. MD’A: Formal analysis, Supervision, Writing – review & editing. LD: Formal analysis, Writing – review & editing. CD: Formal analysis, Writing – review & editing. OE: Formal analysis, Writing – review & editing. MF: Formal analysis, Writing – review & editing. FF: Formal analysis, Writing – review & editing. EF: Formal analysis, Writing – review & editing. MGa: Formal analysis, Writing – review & editing. RGe: Formal analysis, Writing – review & editing. RGi: Formal analysis, Supervision, Writing – review & editing. MGo: Formal analysis, Writing – review & editing. EG: Formal analysis, Writing – review & editing. GG: Formal analysis, Writing – review & editing. AI: Formal analysis, Supervision, Writing – review & editing. FI: Formal analysis, Supervision, Writing – review & editing. BL: Formal analysis, Writing – review & editing. EL: Formal analysis, Supervision, Writing – review & editing. CM: Formal analysis, Writing – review & editing. RP: Formal analysis, Writing – review & editing. RR: Formal analysis, Supervision, Writing – review & editing. MR: Formal analysis, Supervision, Writing – review & editing. CSa: Formal analysis, Supervision, Writing – review & editing. GS: Formal analysis, Writing – review & editing. MS: Formal analysis, Writing – review & editing. CSe: Formal analysis, Supervision, Writing – review & editing. ET: Formal analysis, Writing – review & editing. AM: Formal analysis, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The Educational project INSIDE PsA was arranged with an unrestricted educational sponsorship provided by Janssen-Cilag SpA. Editorial support was provided by Dialecticon srl.
Conflict of interest
SD’A received consulting and speaking fees from AbbVie, Amgen, Bristol-Myers Squibb, Janssen, Lilly, Merck Sharp & Dohme, Novartis, Pfizer and UCB. MB had the following financing relationships with subjects with commercial interests in the health sector: BMS, Janseen, Novartis, Lilly, Abbvie, Pfizer, and Galapagos. LD received consultation honoraria from Abbvie, Amgen, Astra-Zeneca, Biogen, Boehringer-Ingelheim, Bristol-Myers Squibb, Celltrion, Eli Lilly and Company, Galapagos, GlaxoSmithKline, Janssen, Kiniksa Pharmaceuticals, Novartis, Pfizer, Roche, Sanofi-Genzyme, Swedish Orphan Biovitrium (SOBI), Takeda, and Vifor Pharmaceuticals. The Unit of Immunology, Rheumatology, Allergy and Rare Diseases (UnIRAR) received unrestricted research/educational grants from Abbvie, Bristol-Myers Squibb, Celgene, GlaxoSmithKline, Janssen, Kiniksa, Merk Sharp & Dohme, Mundipharma Pharmaceuticals, Novartis, Pfizer, Roche, Sanofi-Genzyme, and SOBI. CD has received consulting/speaker’s fees from Abbvie, Eli Lilly, Janssen, Novartis, Pfizer, Roche, Galapagos, Sparrow and Sanofi; grant support from AbbVie and Novartis. FF received consulting/speaker fee or research support from AbbVie, Amgen, Alfa-Sigma, Biogen, Bristol-Myers Squibb, Eli-Lilly, Galapagos, Janssen, Lilly, Novartis, and Pfizer. MGa received consulting and speaking fees from Abbvie, Pfizer, Novartis, Galapagos, Janssen, MSD, Lilly, Astra Zeneca. RGe received consulting and speaking fees from AbbVie, Alfasigma, BMS, MSD, Pfizer, Roche. MGo received consulting and speaking fees from AbbVie, Amgen, Lilly, Novartis, Pfizer. EG received consulting/speaker fee or research support from AbbVie, Eli-Lilly, Galapagos, Janssen, Novartis, and Pfizer. FI received honoraria or consulting fees from Abbvie, Eli-Lilly, Galapagos, Janssen, and Pfizer. BL received speaker fee or research support from AbbVie, Eli-Lilly, Janssen, Novartis, Pfizer, and Bristol. CM received speaker’s bureau or grants from Abbvie, Amgem, BMS, Galapagos, Lilly, Novartis, and Pfizer. RR received consulting/speaker fee or research support from AbbVie, Novartis, Janssen, Eli-Lilly, Amgen, and Pfizer. MR received advisory board honoraria, consultancy fees and/or speaker fees from Abbvie, BMS, Eli-Lilly, Galapagos, Menarini, Novartis, Pfizer, Sandoz, Theramex, UCB. MS received consulting/speaker fees or research support from Bristol-Myers Squibb, Janssen, Eli-Lilly, Pfizer, Galapagos, and Boehringer-Ingheleim. CSe received consulting/speaker fee or research support from AbbVie, Amgen, Alfa-Sigma, Biogen, Eli-Lilly, EUSA-Recordati, Galapagos, Janssen, Novartis, Pfizer, SOBI. AM received consulting/speaker fee from Abbvie, Eli-Lilly, Janssen, Novartis, and UCB.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ritchlin, CT, Colbert, RA, and Gladman, DD. Psoriatic arthritis. N Engl J Med. (2017) 376:957–70. doi: 10.1056/NEJMra1505557
2. Husni, ME, Merola, JF, and Davin, S. The psychosocial burden of psoriatic arthritis. Semin Arthritis Rheum. (2017) 47:351–60. doi: 10.1016/j.semarthrit.2017.05.010
3. Tekin, HG, Wu, JJ, Burge, R, Birt, J, and Egeberg, A. Burden and disease characteristics of patients with psoriatic arthritis: a population-based cross-sectional study. J Rheumatol. (2019) 46:716–20. doi: 10.3899/jrheum.180670
4. de Vlam, K, Steinfeld, S, Toukap, AN, van den Bosch, F, Joos, R, Geysens, P, et al. The burden of psoriatic arthritis in the biologics era: data from the Belgian epidemiological psoriatic arthritis study. Rheumatology. (2021) 60:5677–85. doi: 10.1093/rheumatology/keab233
5. Leung, YY. Is psoriatic arthritis associated with higher risk of mortality? J Rheumatol. (2022) 49:128–31. doi: 10.3899/jrheum.210963
6. Schett, G, Rahman, P, Ritchlin, C, McInnes, IB, Elewaut, D, and Scher, JU. Psoriatic arthritis from a mechanistic perspective. Nat Rev Rheumatol. (2022) 18:311–25. doi: 10.1038/s41584-022-00776-6
7. Najm, A, Goodyear, CS, McInnes, IB, and Siebert, S. Phenotypic heterogeneity in psoriatic arthritis: towards tissue pathology-based therapy. Nat Rev Rheumatol. (2023) 19:153–65. doi: 10.1038/s41584-022-00874-5
8. Kishimoto, M, Deshpande, GA, Fukuoka, K, Kawakami, T, Ikegaya, N, Kawashima, S, et al. Clinical features of psoriatic arthritis. Best Pract Res Clin Rheumatol. (2021) 35:101670. doi: 10.1016/j.berh.2021.101670
9. Richette, P, Vis, M, Ohrndorf, S, Tillett, W, Ramírez, J, Neuhold, M, et al. Identification of PsA phenotypes with machine learning analytics using data from two phase III clinical trials of guselkumab in a bio-naïve population of patients with PsA. RMD Open. (2023) 9:e002934. doi: 10.1136/rmdopen-2022-002934
10. Eder, L, Li, Q, Rahmati, S, Rahman, P, Jurisica, I, and Chandran, V. Defining imaging sub-phenotypes of psoriatic arthritis: integrative analysis of imaging data and gene expression in a PsA patient cohort. Rheumatology. (2022) 61:4952–61. doi: 10.1093/rheumatology/keac078
11. López-Medina, C, Chevret, S, Molto, A, Sieper, J, Duruöz, T, Kiltz, U, et al. Identification of clinical phenotypes of peripheral involvement in patients with spondyloarthritis, including psoriatic arthritis: a cluster analysis in the worldwide ASAS-PerSpA study. RMD Open. (2021) 7:e001728. doi: 10.1136/rmdopen-2021-001728
12. McInnes, IB, Sawyer, LM, Markus, K, LeReun, C, Sabry-Grant, C, and Helliwell, PS. Targeted systemic therapies for psoriatic arthritis: a systematic review and comparative synthesis of short-term articular, dermatological, enthesitis and dactylitis outcomes. RMD Open. (2022) 8:e002074. doi: 10.1136/rmdopen-2021-002074
13. Ng, BCK, and Jadon, DR. Unmet needs in psoriatic arthritis. Best Pract Res Clin Rheumatol. (2021) 35:101693. doi: 10.1016/j.berh.2021.101693
14. Nasa, P, Jain, R, and Juneja, D. Delphi methodology in healthcare research: how to decide its appropriateness. World J Methodol. (2021) 11:116–29. doi: 10.5662/wjm.v11.i4.116
15. Szczerkowska-Dobosz, A, Krasowska, D, Bartosińska, J, Stawczyk-Macieja, M, Walczak, A, Owczarczyk-Saczonek, A, et al. Pathogenesis of psoriasis in the "omic" era. Part IV. Epidemiology, genetics, immunopathogenesis, clinical manifestation and treatment of psoriatic arthritis. Postepy Dermatol Alergol. (2020) 37:625–34. doi: 10.5114/ada.2020.100478
16. Leijten, EF, van Kempen, TS, Olde Nordkamp, MA, Pouw, JN, Kleinrensink, NJ, Vincken, NL, et al. Tissue-resident memory CD8+ T cells from skin differentiate psoriatic arthritis from psoriasis. Arthritis Rheumatol. (2021) 73:1220–32. doi: 10.1002/art.41652
17. van Tok, MN, Na, S, Lao, CR, Alvi, M, Pots, D, van de Sande, MGH, et al. The initiation, but not the persistence, of experimental spondyloarthritis is dependent on Interleukin-23 signaling. Front Immunol. (2018) 9:1550. doi: 10.3389/fimmu.2018.01550
18. Pennington, SR, and FitzGerald, O. Early origins of psoriatic arthritis: clinical, genetic and molecular biomarkers of progression from psoriasis to psoriatic arthritis. Front Med. (2021) 8:723944. doi: 10.3389/fmed.2021.723944
19. Gurke, R, Bendes, A, Bowes, J, Koehm, M, Twyman, RM, Barton, A, et al. Omics and multi-omics analysis for the early identification and improved outcome of patients with psoriatic arthritis. Biomedicine. (2022) 10:2387. doi: 10.3390/biomedicines10102387
20. Boutet, MA, Nerviani, A, Gallo Afflitto, G, and Pitzalis, C. Role of the IL-23/IL-17 axis in psoriasis and psoriatic arthritis: the clinical importance of its divergence in skin and joints. Int J Mol Sci. (2018) 19:530. doi: 10.3390/ijms19020530
21. Bridgewood, C, Sharif, K, Sherlock, J, Watad, A, and McGonagle, D. Interleukin-23 pathway at the enthesis: the emerging story of enthesitis in spondyloarthropathy. Immunol Rev. (2020) 294:27–47. doi: 10.1111/imr.12840
22. Simon, D, Tascilar, K, Kleyer, A, Bayat, S, Kampylafka, E, Sokolova, MV, et al. Association of Structural Entheseal Lesions with an increased risk of progression from psoriasis to psoriatic arthritis. Arthritis Rheumatol. (2022) 74:253–62. doi: 10.1002/art.41239
23. Elliott, A, McGonagle, D, and Rooney, M. Integrating imaging and biomarker assessment to better define psoriatic arthritis and predict response to biologic therapy. Rheumatology. (2021) 60:vi38–52. doi: 10.1093/rheumatology/keab504
24. Gottlieb, AB, and Merola, JF. A clinical perspective on risk factors and signs of subclinical and early psoriatic arthritis among patients with psoriasis. J Dermatolog Treat. (2022) 33:1907–15. doi: 10.1080/09546634.2021.1942423
25. Bilgin, E, Aydin, SZ, Tinazzi, I, Bayindir, Ö, Kimyon, G, Özişler, C, et al. Disease characteristics of psoriatic arthritis patients may differ according to age at psoriasis onset: cross-sectional data from the psoriatic arthritis-international database. Clin Exp Rheumatol. (2021) 39:532–6. doi: 10.55563/clinexprheumatol/ert0p7
26. Perez-Chada, LM, Haberman, RH, Chandran, V, Rosen, CF, Ritchlin, C, Eder, L, et al. Consensus terminology for preclinical phases of psoriatic arthritis for use in research studies: results from a Delphi consensus study. Nat Rev Rheumatol. (2021) 17:238–43. doi: 10.1038/s41584-021-00578-2
27. Karmacharya, P, Wright, K, Achenbach, SJ, Crowson, CS, Ogdie, A, Bekele, D, et al. Time to transition from psoriasis to psoriatic arthritis: a population-based study. Semin Arthritis Rheum. (2022) 52:151949. doi: 10.1016/j.semarthrit.2021.12.013
28. Zabotti, A, Tinazzi, I, Aydin, SZ, and McGonagle, D. From psoriasis to psoriatic arthritis: insights from imaging on the transition to psoriatic arthritis and implications for arthritis prevention. Curr Rheumatol Rep. (2020) 22:24. doi: 10.1007/s11926-020-00891-x
29. Zabotti, A, De Lucia, O, Sakellariou, G, Batticciotto, A, Cincinelli, G, Giovannini, I, et al. Predictors, risk factors, and incidence rates of psoriatic arthritis development in psoriasis patients: a systematic literature review and Meta-analysis. Rheumatol Ther. (2021) 8:1519–34. doi: 10.1007/s40744-021-00378-w
30. Antony, A, Holland, R, D'Agostino, MA, Maksymowych, WP, Bertheussen, H, Schick, L, et al. Measurement properties of radiographic outcome measures in psoriatic arthritis: a systematic review from the GRAPPA-OMERACT initiative. Semin Arthritis Rheum. (2021) 51:367–86. doi: 10.1016/j.semarthrit.2021.01.008
31. Geng, Y, Song, Z, Zhang, X, Deng, X, Wang, Y, and Zhang, Z. Improved diagnostic performance of CASPAR criteria with integration of ultrasound. Front Immunol. (2022) 13:935132. doi: 10.3389/fimmu.2022.935132
32. Crespo-Rodríguez, AM, Sanz Sanz, J, Freites, D, Rosales, Z, Abasolo, L, and Arrazola, J. Role of diagnostic imaging in psoriatic arthritis: how, when, and why. Insights Imaging. (2021) 12:121. doi: 10.1186/s13244-021-01035-0
33. Fassio, A, Matzneller, P, and Idolazzi, L. Recent advances in imaging for diagnosis, monitoring, and prognosis of psoriatic arthritis. Front Med. (2020) 7:551684. doi: 10.3389/fmed.2020.551684
34. van der Heijde, D, Gladman, DD, Kavanaugh, A, and Mease, PJ. Assessing structural damage progression in psoriatic arthritis and its role as an outcome in research. Arthritis Res Ther. (2020) 22:18. doi: 10.1186/s13075-020-2103-8
35. Kampylafka, E, Simon, D, d'Oliveira, I, Linz, C, Lerchen, V, Englbrecht, M, et al. Disease interception with interleukin-17 inhibition in high-risk psoriasis patients with subclinical joint inflammation-data from the prospective IVEPSA study. Arthritis Res Ther. (2019) 21:178. doi: 10.1186/s13075-019-1957-0
36. Nerviani, A, Boutet, MA, Tan, WSG, Goldmann, K, Purkayastha, N, Lajtos, TA, et al. IL-23 skin and joint profiling in psoriatic arthritis: novel perspectives in understanding clinical responses to IL-23 inhibitors. Ann Rheum Dis. (2021) 80:591–7. doi: 10.1136/annrheumdis-2020-218186
37. Rossini, M, Epis, OM, Tinazzi, I, Grembiale, RD, and Iagnocco, A. Role of the IL-23 pathway in the pathogenesis and treatment of enthesitis in psoriatic arthritis. Expert Opin Biol Ther. (2020) 20:787–98. doi: 10.1080/14712598.2020.1737855
38. Zabotti, A, Giovannini, I, McGonagle, D, De Vita, S, Stinco, G, and Errichetti, E. Arthritis interception in patients with psoriasis treated with Guselkumab. Dermatol Ther. (2022) 12:5–8. doi: 10.1007/s13555-021-00650-5
39. Hioki, T, Komine, M, and Ohtsuki, M. Diagnosis and intervention in early psoriatic arthritis. J Clin Med. (2022) 11:2051. doi: 10.3390/jcm11072051
40. Haberman, RH, MacFarlane, KA, Catron, S, Samuels, J, Blank, RB, Toprover, M, et al. Efficacy of guselkumab, a selective IL-23 inhibitor, in preventing arthritis in a multicentre psoriasis at-risk cohort (PAMPA): protocol of a randomised, double-blind, placebo controlled multicentre trial. BMJ Open. (2022) 12, 12:e063650. doi: 10.1136/bmjopen-2022-063650
41. Gladman, DD. Axial psoriatic arthritis. Curr Rheumatol Rep. (2021) 23:35. doi: 10.1007/s11926-021-00999-8
42. Feld, J, Chandran, V, Haroon, N, Inman, R, and Gladman, D. Axial disease in psoriatic arthritis and ankylosing spondylitis: a critical comparison. Nat Rev Rheumatol. (2018) 14:363–71. doi: 10.1038/s41584-018-0006-8.29752461
43. Feld, J, Ye, JY, Chandran, V, Inman, RD, Haroon, N, Cook, R, et al. Is axial psoriatic arthritis distinct from ankylosing spondylitis with and without concomitant psoriasis? Rheumatology. (2020) 59:1340–6. doi: 10.1093/rheumatology/kez457
44. Poddubnyy, D, Jadon, DR, Van den Bosch, F, Mease, PJ, and Gladman, DD. Axial involvement in psoriatic arthritis: an update for rheumatologists. Semin Arthritis Rheum. (2021) 51:880–7. doi: 10.1016/j.semarthrit.2021.06.006
45. Michelena, X, López-Medina, C, Erra, A, Juanola, X, Font-Ugalde, P, Collantes, E, et al. Characterising the axial phenotype of psoriatic arthritis: a study comparing axial psoriatic arthritis and ankylosing spondylitis with psoriasis from the REGISPONSER registry. RMD Open. (2022) 8:e002513. doi: 10.1136/rmdopen-2022-002513
46. Benavent, D, Plasencia, C, Poddubnyy, D, Kishimoto, M, Proft, F, Sawada, H, et al. Unveiling axial involvement in psoriatic arthritis: an ancillary analysis of the ASAS-perSpA study. Semin Arthritis Rheum. (2021) 51:766–74. doi: 10.1016/j.semarthrit.2021.04.018
47. Benavent, D, Plasencia-Rodríguez, C, Franco-Gómez, K, Nieto, R, Monjo-Henry, I, Peiteado, D, et al. Axial spondyloarthritis and axial psoriatic arthritis: similar or different disease spectrum? Ther Adv Musculoskelet Dis. (2020) 12:1759720X20971889. doi: 10.1177/1759720X20971889
48. Feld, J, Ye, JY, Chandran, V, Inman, RD, Haroon, N, Cook, R, et al. Axial disease in psoriatic arthritis: the presence and progression of unilateral grade 2 sacroiliitis in a psoriatic arthritis cohort. Semin Arthritis Rheum. (2021) 51:464–8. doi: 10.1016/j.semarthrit.2021.03.007
49. Giovannini, I, Zabotti, A, Cicciò, C, Salgarello, M, Cereser, L, De Vita, S, et al. Axial psoriatic disease: clinical and imaging assessment of an underdiagnosed condition. J Clin Med. (2021) 10:2845. doi: 10.3390/jcm10132845
50. Gottlieb, AB, and Merola, JF. Axial psoriatic arthritis: an update for dermatologists. J Am Acad Dermatol. (2021) 84:92–101. doi: 10.1016/j.jaad.2020.05.089
51. Poddubnyy, D, Baraliakos, X, Van den Bosch, F, Braun, J, Coates, LC, Chandran, V, et al. Axial involvement in psoriatic arthritis cohort (AXIS): the protocol of a joint project of the assessment of SpondyloArthritis international society (ASAS) and the Group for Research and Assessment of psoriasis and psoriatic arthritis (GRAPPA). Ther Adv Musculoskelet Dis. (2021) 13:1759720X211057975. doi: 10.1177/1759720X211057975
52. Fragoulis, GE, Pappa, M, Evangelatos, G, Iliopoulos, A, Sfikakis, PP, and Tektonidou, MG. Axial psoriatic arthritis and ankylosing spondylitis: same or different? A real-world study with emphasis on comorbidities. Clin Exp Rheumatol. (2022) 40:1267–72. doi: 10.55563/clinexprheumatol/8zn9z8
53. Abdelaziz, MM, Ismail, N, Gamal, AM, Lafy, R, and El-Adly, W. Comparative analysis between ankylosing spondylitis and axial psoriatic arthritis patients. Egypt. Rheumatol. (2022) 44:25–9. doi: 10.1016/j.ejr.2021.07.006
54. Lopez-Medina, C, and Ziade, N. Axial disease in psoriatic arthritis: how can we define it, and does it have an impact on treatment? Mediterr. J. Rheumatol. (2022) 33:142–9. doi: 10.31138/mjr.33.1.142
55. Mease, PJ, Helliwell, PS, Gladman, DD, Poddubnyy, D, Baraliakos, X, Chakravarty, SD, et al. Efficacy of guselkumab on axial involvement in patients with active psoriatic arthritis and sacroiliitis: a post-hoc analysis of the phase 3 DISCOVER-1 and DISCOVER-2 studies. Lancet Rheumatol. (2022) 3:e715–23. doi: 10.1016/S2665-9913(21)00105-3
56. Gladman, DD, Mease, PJ, Bird, P, Soriano, ER, Chakravarty, SD, Shawi, M, et al. Efficacy and safety of guselkumab in biologic-naïve patients with active axial psoriatic arthritis: study protocol for STAR, a phase 4, randomized, double-blinded, placebo-controlled trial. Trials. (2022) 23:743. doi: 10.1186/s13063-022-06589-y
57. Deodhar, A, Gensler, LS, Sieper, J, Clark, M, Calderon, C, Wang, Y, et al. Three multicenter, randomized, double-blind, placebo-controlled studies evaluating the efficacy and safety of Ustekinumab in axial Spondyloarthritis. Arthritis Rheumatol. (2019) 71:258–70. doi: 10.1002/art.40728
58. Mease, P, and van den Bosch, F. IL-23 and axial disease: do they come together? Rheumatology. (2021) 60:iv28–33. doi: 10.1093/rheumatology/keab617
59. Miyagawa, I, Nakayamada, S, Nakano, K, Kubo, S, Iwata, S, Miyazaki, Y, et al. Precision medicine using different biological DMARDs based on characteristic phenotypes of peripheral T helper cells in psoriatic arthritis. Rheumatology. (2019) 58:336–44. doi: 10.1093/rheumatology/key069
60. Lubrano, E, Chan, J, Queiro-Silva, R, Cauli, A, Goel, N, Poddubnyy, D, et al. Management of axial disease in patients with psoriatic arthritis: an updated literature review informing the 2021 GRAPPA treatment recommendations. J Rheumatol. (2023) 50:279–84. doi: 10.3899/jrheum.220309
61. Baraliakos, X, Gossec, L, Pournara, E, Jeka, S, Mera-Varela, A, D'Angelo, S, et al. Secukinumab in patients with psoriatic arthritis and axial manifestations: results from the double-blind, randomised, phase 3 MAXIMISE trial. Ann Rheum Dis. (2021) 80:582–90. doi: 10.1136/annrheumdis-2020-218808
62. Gossec, L, Baraliakos, X, Kerschbaumer, A, de Wit, M, McInnes, I, Dougados, M, et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann Rheum Dis. (2020) 79:700.1–700.712. doi: 10.1136/annrheumdis-2020-217159
63. Coates, LC, Soriano, ER, Corp, N, Bertheussen, H, Callis Duffin, K, Campanholo, CB, et al. Group for research and assessment of psoriasis and psoriatic arthritis (GRAPPA): updated treatment recommendations for psoriatic arthritis 2021. Nat Rev Rheumatol. (2022) 18:465–79. doi: 10.1038/s41584-022-00798-0
64. Gupta, S, Syrimi, Z, Hughes, DM, and Zhao, SS. Comorbidities in psoriatic arthritis: a systematic review and meta-analysis. Rheumatol Int. (2021) 41:275–84. doi: 10.1007/s00296-020-04775-2
65. Ballegaard, C, Skougaard, M, Guldberg-Møller, J, Nissen, CV, Amris, K, Jørgensen, TS, et al. Comorbidities, pain and fatigue in psoriatic arthritis, psoriasis and healthy controls: a clinical cohort study. Rheumatology. (2021) 60:3289–300. doi: 10.1093/rheumatology/keaa780
66. Casciano, F, Pigatto, PD, Secchiero, P, Gambari, R, and Reali, E. T cell hierarchy in the pathogenesis of psoriasis and associated cardiovascular comorbidities. Front Immunol. (2018) 9:1390. doi: 10.3389/fimmu.2018.01390
67. Gialouri, CG, and Fragoulis, GE. Cardiovascular disease in psoriatic arthritis: facts and unmet needs. Rheumatology (Oxford). (2022) 61:1305–6. doi: 10.1093/rheumatology/keab655
68. Cheng, IT, Li, EK, Wong, PC, Law, MY, Yim, IC, Lai, BT, et al. Treat to target and prevention of subclinical atherosclerosis in psoriatic arthritis-which target should we choose? Rheumatology. (2020) 59:2881–92. doi: 10.1093/rheumatology/keaa025
69. Egeberg, A, Gisondi, P, Carrascosa, JM, Warren, RB, and Mrowietz, U. The role of the interleukin-23/Th17 pathway in cardiometabolic comorbidity associated with psoriasis. J Eur Acad Dermatol Venereol. (2020) 34:1695–706. doi: 10.1111/jdv.16273
70. Ramírez, J, Azuaga-Piñango, AB, Celis, R, and Cañete, JD. Update on cardiovascular risk and obesity in psoriatic arthritis. Front Med. (2021) 8:742713. doi: 10.3389/fmed.2021.742713
71. Perez-Chada, LM, and Merola, JF. Comorbidities associated with psoriatic arthritis: review and update. Clin Immunol. (2020) 214:108397. doi: 10.1016/j.clim.2020.108397
72. Atzeni, F, Gerratana, E, Francesco Masala, I, Bongiovanni, S, Sarzi-Puttini, P, and Rodríguez-Carrio, J. Psoriatic arthritis and metabolic syndrome: is there a role for disease modifying anti-rheumatic drugs? Front Med. (2021) 8:735150. doi: 10.3389/fmed.2021.735150
73. Merzel Šabović, EK, Starbek Zorko, M, and Janić, M. Killing two birds with one stone: potential therapies targeting psoriasis and atherosclerosis at the same time. Int J Mol Sci. (2022) 23:6648. doi: 10.3390/ijms23126648
74. Tanase, DM, Gosav, EM, Radu, S, Ouatu, A, Rezus, C, Ciocoiu, M, et al. Arterial hypertension and interleukins: potential therapeutic target or future diagnostic marker? Int J Hypertens. (2019) 2019:3159283. doi: 10.1155/2019/3159283
75. Wang, J, Bhatia, A, Krugliak Cleveland, N, Gupta, N, Dalal, S, Rubin, DT, et al. Rapid onset of inflammatory bowel disease after receiving secukinumab infusion. ACG Case Rep J. (2018) 5:e56. doi: 10.14309/crj.2018.56
76. Ehrlich, D, Jamaluddin, N, Pisegna, J, and Padua, D. A challenging case of severe ulcerative colitis following the initiation of secukinumab for ankylosing spondylitis. Case Rep Gastrointest Med. (2018) 2018:9679287–4. doi: 10.1155/2018/9679287
77. Vernero, M, Astegiano, M, and Ribaldone, DG. New onset of inflammatory bowel disease in three patients undergoing IL-17A inhibitor secukinumab: a case series. Am J Gastroenterol. (2019) 114:179–80. doi: 10.1038/s41395-018-0422-z
78. Ferrante, M, Panaccione, R, Baert, F, Bossuyt, P, Colombel, JF, Danese, S, et al. Risankizumab as maintenance therapy for moderately to severely active Crohn's disease: results from the multicentre, randomised, double-blind, placebo-controlled, withdrawal phase 3 FORTIFY maintenance trial. Lancet. (2022) 399:2031–46. doi: 10.1016/S0140-6736(22)00466-4
79. D'Haens, G, Panaccione, R, Baert, F, Bossuyt, P, Colombel, JF, Danese, S, et al. Risankizumab as induction therapy for Crohn's disease: results from the phase 3 ADVANCE and MOTIVATE induction trials. Lancet. (2022) 399:2015–30. doi: 10.1016/S0140-6736(22)00467-6
80. Sandborn, WJ, D'Haens, GR, Reinisch, W, Panés, J, Chan, D, Gonzalez, S, et al. Guselkumab for the treatment of Crohn's disease: induction results from the phase 2 GALAXI-1 study. Gastroenterology. (2022) 162:1650–1664.e8. doi: 10.1053/j.gastro.2022.01.047
81. Hindson, J. Gasdermin B in IBD and epithelial barrier repair. Nat Rev Gastroenterol Hepatol. (2022) 19:216. doi: 10.1038/s41575-022-00589-8
82. Lortholary, O, Fernandez-Ruiz, M, Baddley, JW, Manuel, O, Mariette, X, and Winthrop, KL. Infectious complications of rheumatoid arthritis and psoriatic arthritis during targeted and biological therapies: a viewpoint in 2020. Ann Rheum Dis. (2020) 79:1532–43. doi: 10.1136/annrheumdis-2020-217092
83. Li, X, Andersen, KM, Chang, HY, Curtis, JR, and Alexander, GC. Comparative risk of serious infections among real-world users of biologics for psoriasis or psoriatic arthritis. Ann Rheum Dis. (2020) 79:285–91. doi: 10.1136/annrheumdis-2019-216102
84. Jin, Y, Lee, H, Lee, MP, Landon, JE, Merola, JF, Desai, RJ, et al. Risk of hospitalization for serious infection after initiation of ustekinumab or other biologics in patients with psoriasis or psoriatic arthritis. Arthritis Care Res. (2022) 74:1792–805. doi: 10.1002/acr.24630
85. Tucker, LJ, Coates, LC, and Helliwell, PS. Assessing disease activity in psoriatic arthritis: a literature review. Rheumatol Ther. (2019) 6:23–32. doi: 10.1007/s40744-018-0132-4
86. Batko, B. Patient-centered care in psoriatic arthritis-a perspective on inflammation, disease activity, and psychosocial factors. J Clin Med. (2020) 9:3103. doi: 10.3390/jcm9103103
87. Hackett, S, and Coates, LC. Outcome measures in psoriatic arthritis: where next? Musculoskeletal Care. (2022) 20:S22–31. doi: 10.1002/msc.1692
88. Coates, LC, Lubrano, E, Perrotta, FM, Emery, P, Conaghan, PG, and Helliwell, PS. What should be the primary target of "treat to target" in psoriatic arthritis? J Rheumatol. (2019) 46:38–42. doi: 10.3899/jrheum.180267
89. Gazitt, T, Elhija, MA, Haddad, A, Lavi, I, Elias, M, and Zisman, D. Implementation of the treat-to-target concept in evaluation of psoriatic arthritis patients. J Clin Med. (2021) 10:5659. doi: 10.3390/jcm10235659
90. Coates, LC, Strand, V, Wilson, H, Revicki, D, Stolshek, B, Samad, A, et al. Measurement properties of the minimal disease activity criteria for psoriatic arthritis. RMD Open. (2019) 5:e001002. doi: 10.1136/rmdopen-2019-001002
91. Gezer, HH, Duruöz, MT, Nas, K, Kılıç, E, Sargın, B, Kasman, SA, et al. Inconsistencies of the disease activity assessment tools for psoriatic arthritis: challenges to rheumatologists. Joint Bone Spine. (2022) 89:105296. doi: 10.1016/j.jbspin.2021.105296
92. Dures, E, Shepperd, S, Mukherjee, S, Robson, J, Vlaev, I, Walsh, N, et al. Treat-to-target in PsA: methods and necessity. RMD Open. (2020) 6:e001083. doi: 10.1136/rmdopen-2019-001083
93. Lu, C, Wallace, BI, Waljee, AK, Fu, W, Zhang, Q, and Liu, Y. Comparative efficacy and safety of targeted DMARDs for active psoriatic arthritis during induction therapy: a systematic review and network meta-analysis. Semin Arthritis Rheum. (2019) 49:381–8. doi: 10.1016/j.semarthrit.2019.06.001
94. Tucker, LJ, Ye, W, and Coates, LC. Novel concepts in psoriatic arthritis management: can we treat to target? Curr Rheumatol Rep. (2018) 20:71. doi: 10.1007/s11926-018-0781-x
95. Kerschbaumer, A, Smolen, JS, Dougados, M, de Wit, M, Primdahl, J, McInnes, I, et al. Pharmacological treatment of psoriatic arthritis: a systematic literature research for the 2019 update of the EULAR recommendations for the management of psoriatic arthritis. Ann Rheum Dis. (2020) 79:778–86. doi: 10.1136/annrheumdis-2020-217163
96. Michielsens, CA, den Broeder, N, van den Hoogen, FH, Mahler, EA, Teerenstra, S, van der Heijde, D, et al. Treat-to-target dose reduction and withdrawal strategy of TNF inhibitors in psoriatic arthritis and axial spondyloarthritis: a randomised controlled non-inferiority trial. Ann Rheum Dis. (2022) 81:1392–9. doi: 10.1136/annrheumdis-2022-222260
97. Michielsens, CAJ, den Broeder, N, Mulder, MLM, van den Hoogen, FHJ, Verhoef, LM, and den Broeder, AA. Tumour necrosis factor inhibitor dose adaptation in psoriatic arthritis and axial spondyloarthritis (TAPAS): a retrospective cohort study. Rheumatology (Oxford). (2022) 61:2307–15. doi: 10.1093/rheumatology/keab741
98. Michielsens, CAJ, Boers, N, den Broeder, N, Wenink, MH, van der Maas, A, Mahler, EAM, et al. Dose reduction and withdrawal strategy for TNF-inhibitors in psoriatic arthritis and axial spondyloarthritis: design of a pragmatic open-label, randomised, non-inferiority trial. Trials. (2020) 21:90. doi: 10.1186/s13063-019-4000-5
99. Gottlieb, AB, and Langholff, W. Safety observations in 12095 patients with psoriasis enrolled in an international registry (PSOLAR): experience with infliximab and other systemic and biologic therapies errata. J Drugs Dermatol. (2020) 19:573–4.
100. Mease, PJ, McInnes, IB, Tam, LS, Eaton, K, Peterson, S, Schubert, A, et al. Comparative effectiveness of guselkumab in psoriatic arthritis: results from systematic literature review and network meta-analysis. Rheumatology. (2021) 60:2109–21. doi: 10.1093/rheumatology/keab119
101. Kwok, TSH, Sutton, M, Ye, JY, Pereira, D, Chandran, V, and Gladman, DD. Prevalence and factors associated with osteoporosis and bone mineral density testing in psoriatic arthritis. Arthritis Care Res. (2022) 74:1006–12. doi: 10.1002/acr.24538
Keywords: psoriatic arthritis, chronic inflammatory musculoskeletal disease, comorbidities, extra-articular manifestations, diagnosis, treatment, consensus process, expert opinion
Citation: D’Angelo S, Atzeni F, Benucci M, Bianchi G, Cantini F, Caporali RF, Carlino G, Caso F, Cauli A, Ciccia F, D’Agostino MA, Dagna L, Dejaco C, Epis OM, Ferrucci MG, Franceschini F, Fusaro E, Gabini M, Gerli R, Giacomelli R, Govoni M, Gremese E, Guggino G, Iagnocco A, Iannone F, Laganà B, Lubrano E, Montecucco C, Peluso R, Ramonda R, Rossini M, Salvarani C, Sebastiani GD, Sebastiani M, Selmi C, Tirri E and Marchesoni A (2023) Management of psoriatic arthritis: a consensus opinion by expert rheumatologists. Front. Med. 10:1327931. doi: 10.3389/fmed.2023.1327931
Edited by:
George E. Fragoulis, Laiko General Hospital of Athens, GreeceReviewed by:
Rubén Queiro, Foundation for Biosanitary Research and Innovation of the Principality of Asturias (FINBA), SpainCopyright © 2023 D’Angelo, Atzeni, Benucci, Bianchi, Cantini, Caporali, Carlino, Caso, Cauli, Ciccia, D’Agostino, Dagna, Dejaco, Epis, Ferrucci, Franceschini, Fusaro, Gabini, Gerli, Giacomelli, Govoni, Gremese, Guggino, Iagnocco, Iannone, Laganà, Lubrano, Montecucco, Peluso, Ramonda, Rossini, Salvarani, Sebastiani, Sebastiani, Selmi, Tirri and Marchesoni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio Marchesoni, bWFyY2hlc29uaUB0aXNjYWxpLml0