
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 27 November 2023
Sec. Precision Medicine
Volume 10 - 2023 | https://doi.org/10.3389/fmed.2023.1284689
This article is part of the Research Topic Precision Treatments for Patients with Obesity View all 6 articles
 Saúl Caicedo-Trujillo1,2
Saúl Caicedo-Trujillo1,2 Rodrigo Torres-Castro3,4*
Rodrigo Torres-Castro3,4* Luis Vasconcello-Castillo3
Luis Vasconcello-Castillo3 Lilian Solis-Navarro3,5
Lilian Solis-Navarro3,5 Diana Sanchez-Ramirez6
Diana Sanchez-Ramirez6 Rodrigo Núñez-Cortés3,7
Rodrigo Núñez-Cortés3,7 Roberto Vera-Uribe3Isabel Muñoz-Muñoz8
Roberto Vera-Uribe3Isabel Muñoz-Muñoz8 Marisol Barros-Poblete9Juan Eduardo Romero3
Marisol Barros-Poblete9Juan Eduardo Romero3 Jordi Vilaró5
Jordi Vilaró5Introduction: Obesity is a chronic medical condition that affects, among others, the cardiovascular and respiratory systems. Interventions for its treatment focus on sustained weight reduction and general health improvement, leaving respiratory management aside. Our objective was to determine the effects of inspiratory muscle training (IMT) in patients with obesity.
Methods: A systematic review was performed in Embase, Cochrane Library (CENTRAL), CINAHL, Web of Science, and PubMed/MEDLINE on June 26, 2023. Randomized clinical trials (RCTs), and quasi-randomized clinical trials investigating the effects of IMT in people with obesity were included. Selected studies were screened by two independent reviewers who extracted data and assessed the quality of the evidence.
Results: The initial search returned 705 potential studies were included. Ultimately, eight studies met the criteria for eligibility and were included in the review. IMT improves physical capacity [6-minute walk test (6MWT): 44.5 m, 95% CI: 30.5 to 58.5; p < 0.0001] and the strength of the inspiratory muscles [maximal inspiratory pressure (MIP): −28.4 cm H2O, 95% CI: −41.9 to −14.8; p < 0.0001] compared to the controls, without differences in the pulmonary function, body mass index (BMI) and metabolic parameters.
Conclusion: Inspiratory muscle training improves physical capacity and inspiratory muscle strength without significant changes in lung function, BMI, and metabolic parameters.
Systematic review registration: PROSPERO, identifier CRD42023439625, https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023439625Obesity is a chronic medical condition characterized by excessive accumulation of body fat, leading to adverse health outcomes (1). It is a major global health concern, increasing worldwide prevalence (2). According to the World Health Organization (WHO), the number of individuals with obesity has nearly tripled since 1975 (3). In 2016, the global prevalence of overweight and obesity was indeed significant. More than 1.9 billion adults were classified as overweight, and over 650 million were classified as obese (3). These alarming statistics highlight the urgent need for effective interventions to combat obesity and its associated health risks.
Obesity not only affects the body’s metabolic and cardiovascular systems but also places a significant burden on the respiratory system (4, 5). Excess weight can lead to decreased lung volumes, reduced lung compliance, and increased work of breathing (4, 6). It can also lead to the development or exacerbation of respiratory conditions such as obstructive sleep apnea, obesity, hypoventilation syndrome, and asthma (7–9). The compromised respiratory function in individuals with obesity contributes to impaired exercise tolerance, increased breathlessness, and a higher risk of respiratory complications (5, 10).
The treatment of obesity involves a multidisciplinary approach to achieve sustained weight loss and improve overall health (11). Pharmacological interventions, such as orlistat and liraglutide, may be prescribed to diminishing weight by reducing appetite or inhibiting fat absorption (12). Surgical interventions, especially bariatric surgery, are considered for individuals with severe obesity or obesity-related comorbidities (13). Dietary interventions, including calorie restriction and balanced macronutrient distribution, are crucial in weight management (14). Additionally, regular physical activity and exercise are essential components of obesity treatment, promoting energy expenditure and maintaining muscle mass (15). Specific exercises that target the respiratory muscles, such as inspiratory muscle training (IMT), have shown potential benefits in improving respiratory function in individuals with obesity (16, 17).
In addition to its potential role in obesity, respiratory muscle training has been explored as an alternative therapeutic option for various respiratory, cardiac, and metabolic conditions (18–20). It has been shown to improve respiratory muscle strength, endurance, and breathing efficiency, enhancing exercise capacity and quality of life (20, 21). Patients with chronic obstructive pulmonary disease, heart failure, and metabolic disorders have experienced significant benefits from respiratory muscle training (18, 20, 21).
Although IMT has demonstrated positive effects in managing various chronic conditions, its effectiveness in obesity is not yet fully understood. Given the compromised respiratory function in individuals with obesity and the potential benefits of respiratory muscle training, it is critical to investigate the effectiveness of respiratory muscle training in subjects with obesity is crucial. By determining the effects of such training on respiratory muscle strength, pulmonary function, exercise tolerance, and overall health outcomes, we can gain valuable insights into the potential benefits of this intervention in managing individuals with obesity.
A systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (22). The review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) CRD42023439625.
Randomized clinical trials (RCTs), and quasi-randomized clinical trials, that investigated the effects of IMT in people with obesity were included. The studies should report on respiratory muscle strength, physical capacity, pulmonary function, or quality of life. The search approach was formulated using the PICO framework (population: people with obesity; intervention: IMT; control: no intervention; and outcome: physical capacity, pulmonary function, quality of life). All observational studies (retrospective, prospective, cross-sectional, longitudinal, case–control, and cohort), editorials, letters, conference publications, review articles, systematic reviews, meta-analyses, and in vivo and in vitro studies were excluded.
Records were retrieved from Embase, Cochrane Library (CENTRAL), CINAHL, Web of Science, and PubMed/MEDLINE databases on June 26, 2023. Manual searches with the following terms: [(Obesity) OR (Obese)] AND [(Inspiratory muscle training) OR (Breathing exercises) OR (respiratory muscle training)] AND [(Pulmonary function) OR (Spirometry) OR (Maximal inspiratory pressure) OR (Maximal expiratory pressure) OR (MIP) OR (MEP) OR (Physical capacity) OR (6MWT) OR (CPET) OR (cardiopulmonary exercise test) OR (Dyspnea) OR (Fatigue) OR (Weight loss) OR (BMI)] were conducted. No language or publication restrictions were imposed. A manual search of the references list of the selected studies was also conducted. All references were analyzed using Rayyan web software (23).
Two researchers with experience in meta-analysis and training in literature review independently assessed the articles. Initially, two investigators reviewed the titles and abstracts of all identified studies (SCT-LSN). Studies that were considered irrelevant based on the title and abstract review were excluded. In case of any disagreements, a third reviewer (RTC) resolved them. Subsequently, the full-text versions of the articles selected in the initial step were thoroughly examined against the eligibility criteria by the same reviewers (RTC-LSN). Any further discrepancies were addressed by involving a third reviewer (JV). Finally, additional unpublished data were obtained from study authors when possible. Two review authors extracted the data independently (LV-RTC). A third reviewer (JV) solved any disagreements in data extraction.
The methodological quality of the included articles was evaluated using the quality assessment tools provided by the National Heart, Lung, and Blood Institute (NHLBI) (24). Each tool contains criteria for evaluating internal validity and risk of bias. The criteria were assessed using categories of “yes,” “no,” or “other” (indicating items like “not reported,” “not applicable,” or “not determinable”). An overall rating was assigned to each study, considering the items with affirmative answers: ≥ 75% was categorized as good, 50–75% as fair, and < 50% as poor. This evaluation was performed independently by two authors (SCT-LSN), and discrepancies were resolved through consensus. If disagreements could not be resolved, a third author (RTC) was consulted. Additionally, the overall certainty of the evidence was assessed independently by two reviewers (RTC, LSN) using the GRADE approach (25). Disagreements were solved by consensus. Publication bias was assessed by visualizing a funnel plot and Begg’s and Egger’s tests for the possible existence of study bias using the Jamovi software (version 2.3) (26).
Information relating to author, country, study design, number, and characteristics of patients included was collected and summarized in Table 1, characteristics of IMT interventions were collected and summarized in Table 2. Summaries of the association between the outcomes for each study in terms of mean differences (MD) or standard mean differences (SMD) were reported using Review Manager 5 (RevMan, Copenhagen: The Nordic Cochrane Center, The Cochrane Collaboration, 2014). Absolute values and obtained combined measures of the effect of each primary outcome through meta-analysis with a random-effect model due to the expected heterogeneity between studies were calculated (27). Statistical heterogeneity was measured with the I2 statistic and classified as negligeable (I2 = 0−40%), moderate (I2 = 30–60%), substantial (I2 = 50–90%), or considerable (I2 = 75–100%) (27).
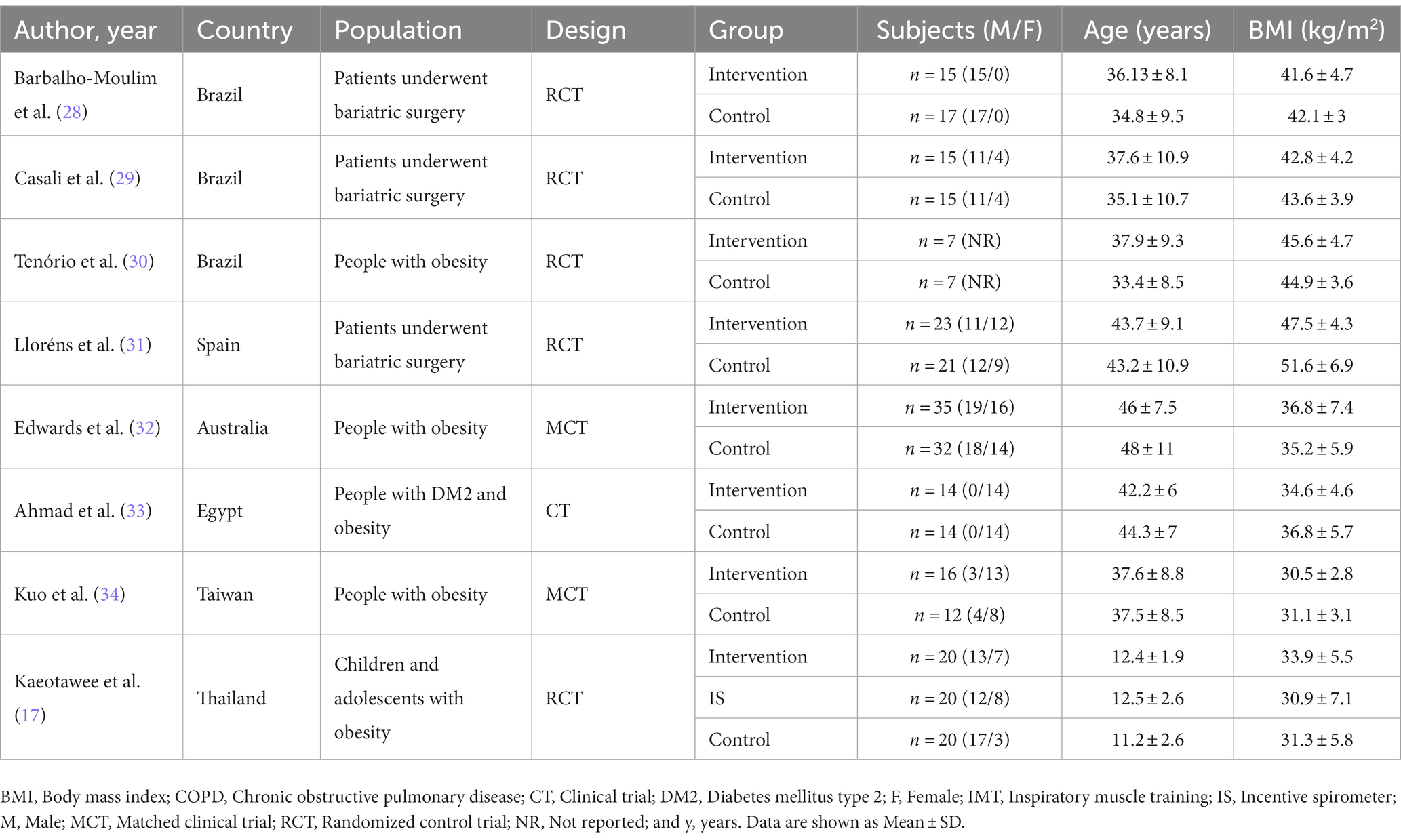
Table 1. Characteristics of included studies.
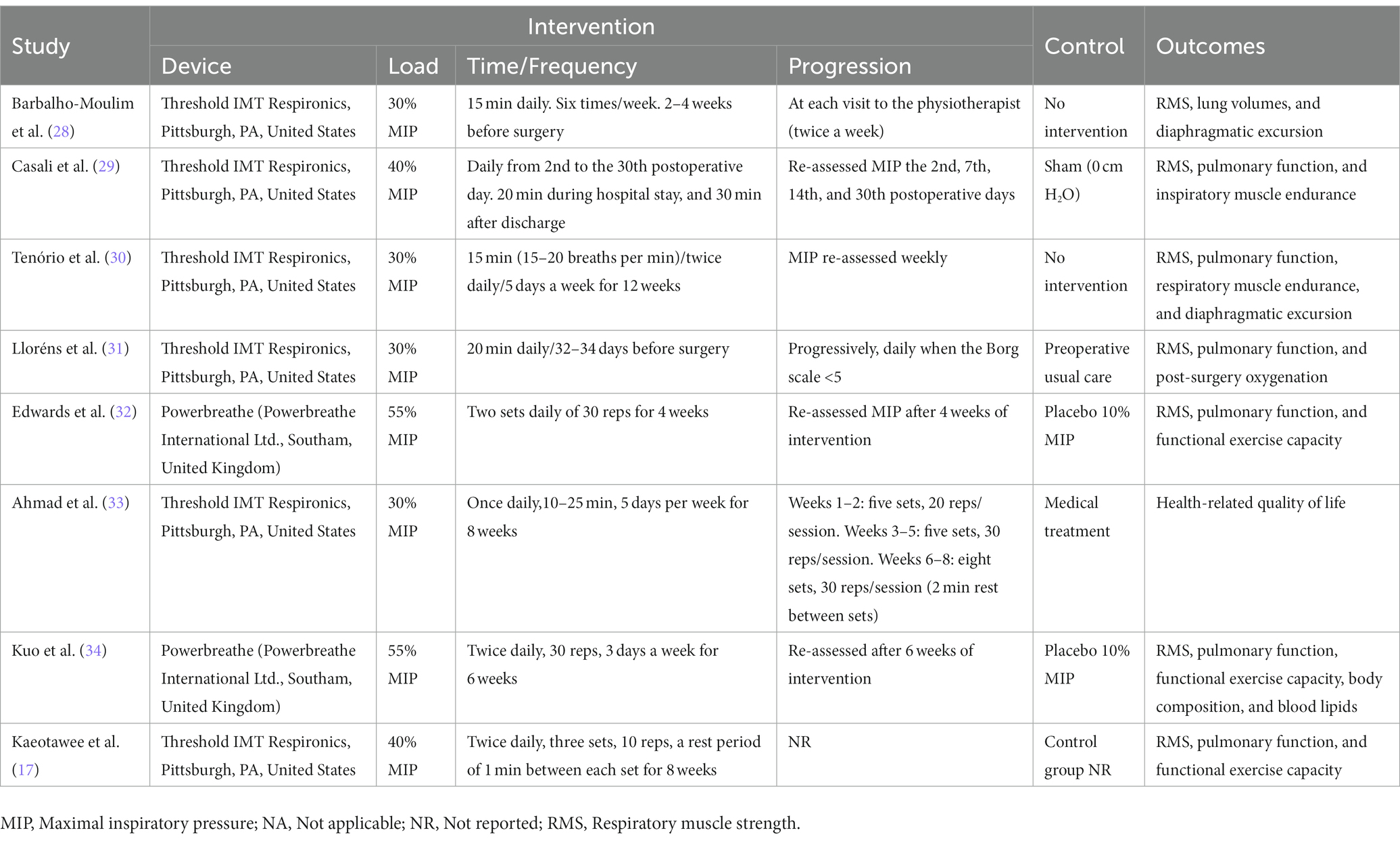
Table 2. Characteristics of interventions.
The initial search yielded 705 potential studies. In total, 133 duplicate records were deleted. Five hundred seventy-two titles and abstracts were screened, and 543 records that did not meet our inclusion criteria were excluded. Twenty-nine of these were assessed as full-text. Of these, 10 were excluded for wrong intervention, seven for conference abstract, two for wrong population, and two for wrong study design. Ultimately, eight studies met the criteria for eligibility and were included in the review (17, 28–34). The flowchart of the study selection process is shown in Figure 1.
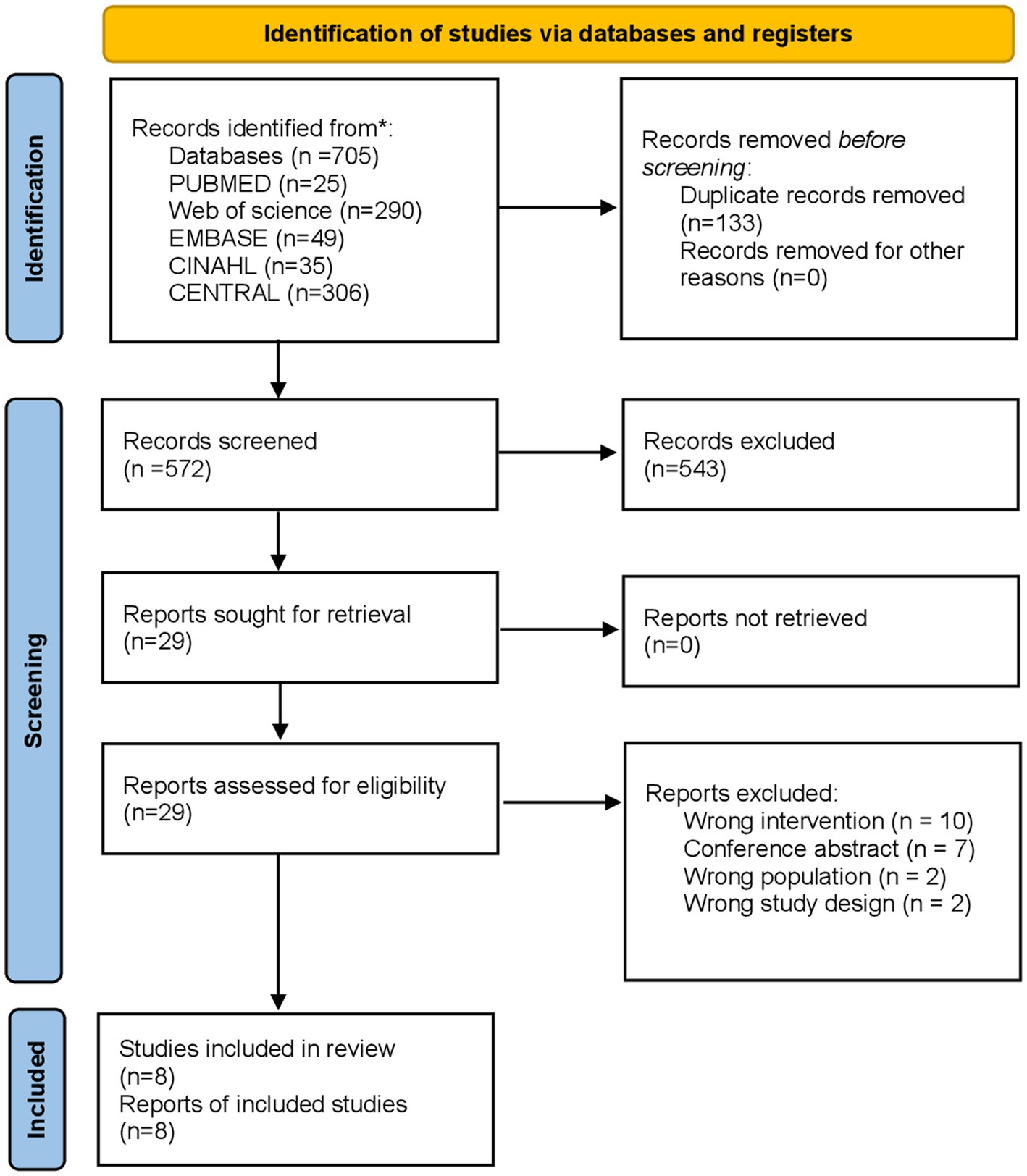
Figure 1. Study selection process.
Three studies were conducted in Brazil (28–30), one in Spain (31), Australia (32), Egypt (33), Taiwan (34), and Thailand (17). All studies were published after 2011. Table 1 displays the attributes and features of the studies that have been incorporated in the analysis.
A total of 283 participants with obesity were analyzed (145 in the intervention group and 138 in the control group). Sample sizes varied from 14 (30) to 67 (32) participants. The studies included 151 (56%) males and 118 (44%) females, with mean ages varying between 11.2 ± 2.6 (17) and 48 ± 11 (32) years. One study did not report the male/female distribution (30). The body mass index (BMI) varied between 30.5 ± 2.8 (34) and 51.6 ± 6.9 kg/m2 (Table 1) (31). The studies were conducted in adults (28–34), except one study that focused on children and adolescents (17). Additionally, some studies specifically targeted groups undergoing bariatric surgery (28, 29, 31), while others investigated important health conditions such as type 2 diabetes (33).
The duration of training varied between 2 (28) and 12 weeks (30). The most commonly used load was 30% of maximal inspiratory pressure (MIP) (28, 30, 31, 33), two studies used 40% (17, 29), and two studies used loads of 55% (32, 34). Regarding the protocol, five studies were trained by time (28–31, 33), and three were trained by repetitions (17, 32, 34). The frequency varied from 3 (34) to 7 days per week (17, 28–32). The devices used were Powerbreathe (Powerbreathe, Southam, United Kingdom) (32, 34) or Threshold IMT (Respironics, Pittsburgh, PA, United States) (17, 28–31, 33). The control group received no intervention (28, 33), 10% MIP (32, 34), placebo (30), sham (29), preoperative usual care (31), or incentive spirometer (17).
Only one of the RCT selected (12.5%) was rated as “good” (i.e., >75 affirmative answers), three (37.5%) were “fair” (50–75% affirmative answers), and four (50) were “poor” (<50% affirmative answers). The quality assessment results for the individual studies obtained using the NHLBI quality assessment tool are presented in the Supplementary material. In the estimation of the effect of IMT on MIP, the result of the Egger’s test suggests the presence of publication bias in the studies (p = 0.045), while the Begg’s test does not show solid evidence of such bias (p = 0.233).
Seven studies reported MIP (Table 2) (17, 28–32, 34). These studies compared 81 participants in the intervention group (IG) vs. 77 in the control group (CG). Patients in the IG had −28.4 cm H2O (95%CI -41.9 to −14.8) higher than CG (p < 0.0001; Figure 2). Substantial heterogeneity of the comparison was identified (I2 = 76%). We could only meta-analyze five studies (17, 28, 30, 31, 34); however, the two non-meta-analyzed studies reported increased MIP (29, 32). According to the GRADE methodology, the certainty of evidence was very low. Only one study reported on endurance, demonstrating that the intervention effectively improved it (29).
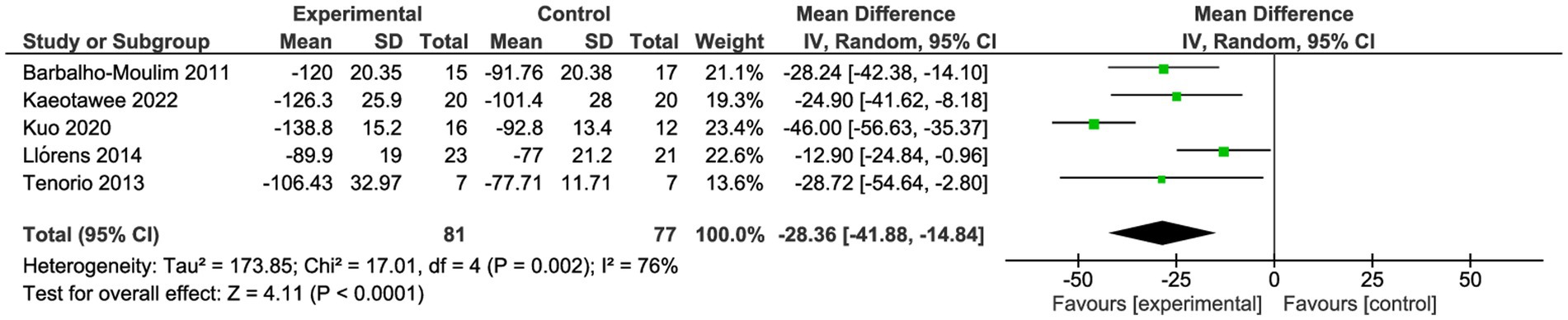
Figure 2. Forest plot for maximal inspiratory pressure.
Three studies reported physical capacity pre- and post-intervention (Table 2) (17, 32, 34). The outcome reported was the distance walked in the 6-min walk test (6MWD) (17, 32, 34). These studies compared 55 participants in the IG vs. 52 in the CG. Patients in the IG walked 44.5 m (95%CI 30.5–58.5) more compared to CG (p < 0.0001; Figure 3). The heterogeneity of the comparison was negligeable (I2 = 0%). The certainty of evidence, according to the GRADE methodology, was low.

Figure 3. Forest plot for physical capacity.
Seven studies reported lung function pre- and post-intervention (Table 2) (17, 28–32, 34). These studies compared 131 participants in the IG vs. 122 in the CG. Both groups had similar forced vital capacity (FVC; SMD 0.13; 95%CI −0.12 to 0.38, p = 0.31, I2: 1%) and similar forced expiratory volume in the first second (FEV1; SMD 0.10; 95%CI −0.16 to 0.35, p = 0.46, I2: 4%; Figures 4, 5). One study reported maximal voluntary ventilation with significant changes in IG (30). The certainty of evidence, according to the GRADE methodology, was low.
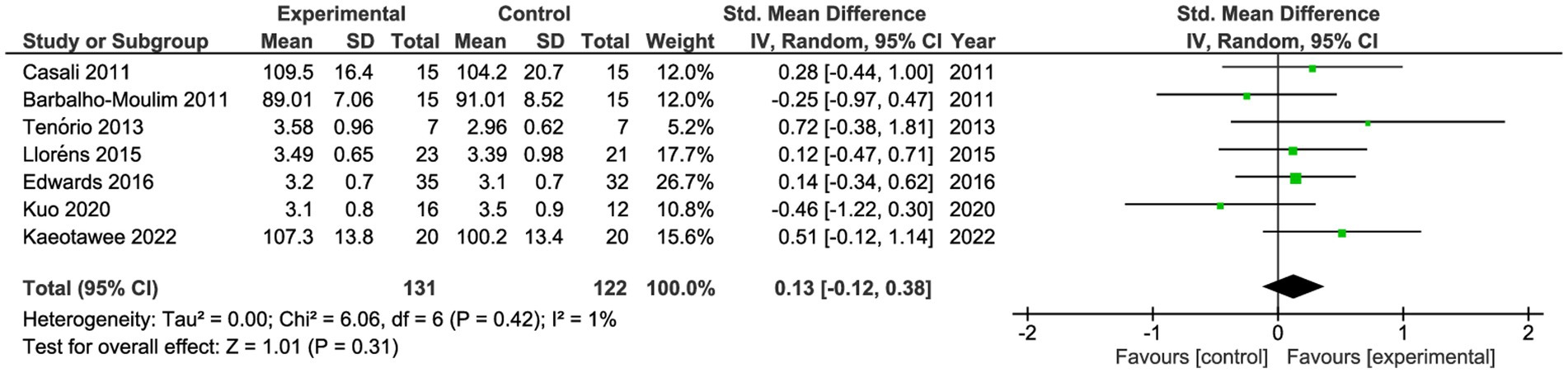
Figure 4. Forest plot for forced vital capacity.
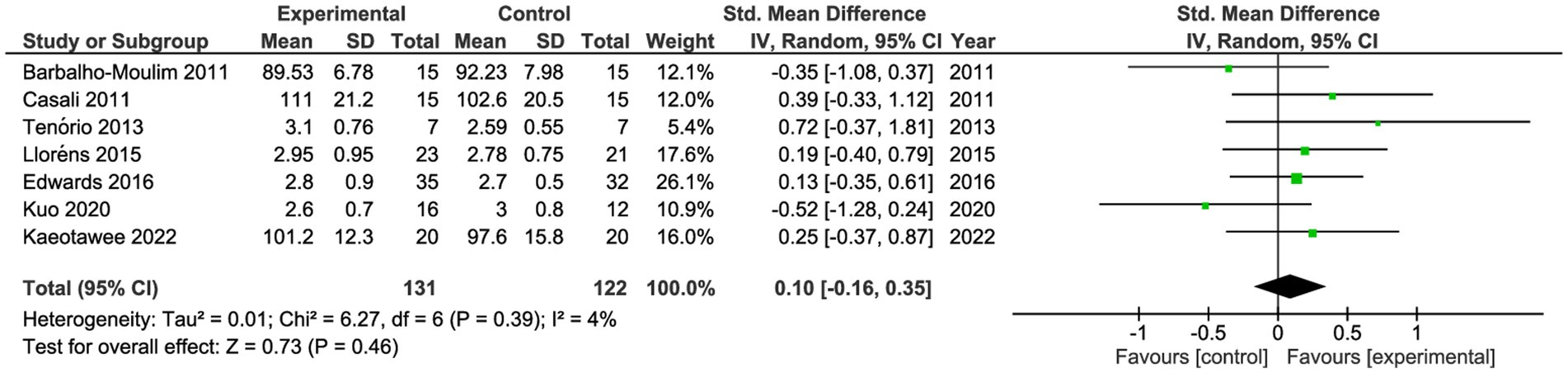
Figure 5. Forest plot for forced expiratory volume in the first second.
Only one study assessed post-intervention BMI without finding significant differences after the intervention (34). The same authors also evaluated the lipid profile, finding no changes in cholesterol, triglycerides, high-density lipoprotein, or low-density lipoprotein (34). Another author assessed post-intervention glucose levels in 26 diabetic women who trained for 8 weeks at low intensity. They found no significant differences between the groups (33).
Additional outcomes reported pre- and post-intervention included quality of life (QoL) and dyspnea. Significant differences in QoL were found in a cohort of 26 diabetic women assessed with the SF-36 (33). On the other hand, no differences in post-exercise dyspnea were identified when assessed with the Borg scale (32).
Our main findings indicated that the IMT improves respiratory muscle strength and physical capacity without changing lung function in people with obesity.
Similarly to what has been observed in other conditions, IMT led to improvements in MIP since it targets the specific inspiratory muscles and utilizes flow-independent devices that adhere to training principles (35, 36). The suggested mechanisms contributing to this finding could involve an increase in the proportion and size of type II muscle fibers (34, 37, 38), promotion of diaphragm hypertrophy, attenuation of the respiratory muscle metaboreflex, and enhanced respiratory muscle economy (17). It is suggested that enhanced respiratory muscle strength increases respiratory capacity, facilitates muscle oxygenation, diminishes respiratory muscle fatigue, and improves individual performance for cardiopulmonary functioning during physical activity (28, 37, 39).
Physical capacity improved in three reviewed studies (17, 32, 34), although only two could be meta-analyzed due to their small sample size (17, 34). The improvement of respiratory muscle function directly impacts physical capacity since it partly depends on ventilation (40). By enhancing ventilatory capacity through the strength of respiratory muscles, patients can walk more while ventilating the same or less (40). Improved respiratory muscle strength enhances respiratory capacity, facilitates muscle oxygenation, lowers lactate production by respiratory muscles, and ultimately decreases respiratory muscle fatigue, improving exercise functional fitness (37, 39, 41). From a clinical point of view, despite the small sample sizes studied, the improvements exceeded the Minimal Clinically Important Difference (MCID) of 30 m in the 6MWT reported for patients with respiratory and cardiovascular diseases, suggesting that this intervention is effective for this outcome (42, 43).
Lung function remained unchanged, as seen in other conditions (19, 44). It is essential to highlight that this outcome can be of interest, especially considering that patients with obesity may develop a restrictive pattern (4). On the other hand, only one study evaluated maximal voluntary ventilation (MVV) and showed improvement suggesting that this intervention could be effective for this outcome (30). Although this test measures ventilation, it has been described in the literature as an assessment scale for the endurance of respiratory muscles (45).
Contrary to expectations, only one study reported variables related to body composition or metabolic parameters linked to obesity which are essential components to include in evaluating any patient with obesity and found no post-intervention changes (34). Similarly to some studies that have shown improvements in quality of life, only one of the analyzed studies found a significant improvement in QoL in subjects with obesity (33).
Three studies included patients eligible for bariatric surgery, making this potential group of interest. Lloréns et al. (31) reported that preoperative IMT enhanced postoperative oxygenation and raised inspiratory muscular strength among morbidly obese patients who underwent laparoscopic bariatric surgery. Similarly, Casali et al. (29) observed that IMT improves inspiratory muscle strength and endurance and accounts for earlier recovery of pulmonary airflows in morbidly obese patients submitted to bariatric surgery. Both studies confirm the improvement in post-surgical outcomes, suggesting the use of IMT in this subgroup of individuals.
Our study has some limitations. First, the selected studies are few and do not allow for a sub-analysis according to obesity severity or training loads. Second, a common feature of the studies is their small sample sizes. Third, regarding the interventions, the intensities and the time/frequency used in the included studies are so heterogeneous and provably low or short to achieve higher inspiratory muscle strength improvements. Fourth, the methodology quality is generally poor to consider the obtained evidence so strong to extrapolate their results to an obese general population. Finally, in the case of MIP, the Egger’s test’s result suggests publication bias in the studies, while the Begg’s test does not show solid evidence of such bias. In these cases, the validity and reliability of the meta-analysis should be considered with caution, as the presence of publication bias can affect the results and conclusions of the study.
Inspiratory muscle training improves physical capacity, inspiratory muscle strength without significant changes in lung function, BMI, and metabolic parameters. Further studies are needed to improve the quality of the present evidence.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
SC-T: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. RT-C: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. LV-C: Formal analysis, Investigation, Methodology, Software, Supervision, Writing – original draft, Writing – review & editing. LS-N: Conceptualization, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. DS-R: Investigation, Validation, Writing – review & editing. RN-C: Conceptualization, Formal analysis, Methodology, Supervision, Validation, Writing – review & editing. RV-U: Conceptualization, Methodology, Validation, Writing – review & editing. IM-M: Data curation, Validation, Visualization, Writing – review & editing. MB-P: Formal analysis, Investigation, Writing – review & editing. JER: Methodology, Supervision, Writing – review & editing. JV: Conceptualization, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2023.1284689/full#supplementary-material
1. Jastreboff, AM, Kotz, CM, Kahan, S, Kelly, AS, and Heymsfield, SB. Obesity as a disease: the Obesity Society 2018 position statement. Obesity. (2019) 27:7–9. doi: 10.1002/oby.22378
2. Reilly, JJ, El-Hamdouchi, A, Diouf, A, Monyeki, A, and Somda, SA. Determining the worldwide prevalence of obesity. Lancet. (2018) 391:1773–4. doi: 10.1016/S0140-6736(18)30794-3
3. Bentham, J, Di Cesare, M, Bilano, V, Bixby, H, Zhou, B, Stevens, GA, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. (2017) 390:2627–42. doi: 10.1016/S0140-6736(17)32129-3
4. Peters, U, and Dixon, AE. The effect of obesity on lung function. Expert Rev Respir Med. (2018) 12:755–67. doi: 10.1080/17476348.2018.1506331
5. Rabec, C, de Lucas, RP, and Veale, D. Respiratory complications of obesity. Arch Bronconeumol. (2011) 47:252–61. doi: 10.1016/j.arbres.2011.01.012
6. Grassi, L, Kacmarek, R, and Berra, L. Ventilatory mechanics in the patient with obesity. Anesthesiology. (2020) 132:1246–56. doi: 10.1097/ALN.0000000000003154
7. Dixon, AE, and Que, LG. Obesity and asthma. Semin Respir Crit Care Med. (2022) 43:662–74. doi: 10.1055/s-0042-1742384
8. Masa, JF, Pépin, JL, Borel, JC, Mokhlesi, B, Murphy, PB, and Sánchez-Quiroga, MÁ. Obesity hypoventilation syndrome. Eur Respir Rev. (2019) 28:180097. doi: 10.1183/16000617.0097-2018
9. Bonsignore, MR. Obesity and obstructive sleep apnea. Handb Exp Pharmacol. (2022) 274:181–201. doi: 10.1007/164_2021_558
10. Atlantis, E, Langford, K, Piya, M, Ho, V, Skelsey, K, Rickards, L, et al. Physical capacity outcomes in patients with severe obesity after 12 months of physician-led multidisciplinary team care: a case series from a public hospital clinical obesity service. Clin Obes. (2019) 9:e12337. doi: 10.1111/cob.12337
11. Bray, GA, and Ryan, DH. Evidence-based weight loss interventions: individualized treatment options to maximize patient outcomes. Diabetes Obes Metab. (2021) 23:50–62. doi: 10.1111/dom.14200
12. Kushner, RF. Weight loss strategies for treatment of obesity: lifestyle management and pharmacotherapy. Prog Cardiovasc Dis. (2018) 61:246–52. doi: 10.1016/j.pcad.2018.06.001
13. Eisenberg, D, Shikora, SA, Aarts, E, Aminian, A, Angrisani, L, Cohen, RV, et al. 2022 American Society of Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of obesity and metabolic disorders (IFSO) indications for metabolic and bariatric surgery. Obes Surg. (2023) 33:3–14. doi: 10.1007/s11695-022-06332-1
14. Chao, AM, Quigley, KM, and Wadden, TA. Dietary interventions for obesity: clinical and mechanistic findings. J Clin Invest. (2021) 131:e140065. doi: 10.1172/JCI140065
15. Olateju, IV, Opaleye-Enakhimion, T, Udeogu, JE, Asuquo, J, Olaleye, KT, Osa, E, et al. A systematic review on the effectiveness of diet and exercise in the management of obesity. Diabetes Metab Syndr. (2023) 17:102759. doi: 10.1016/j.dsx.2023.102759
16. Ramos-Barrera, GE, DeLucia, CM, and Bailey, EF. Inspiratory muscle strength training lowers blood pressure and sympathetic activity in older adults with OSA: a randomized controlled pilot trial. J Appl Physiol. (2020) 129:449–58. doi: 10.1152/japplphysiol.00024.2020
17. Kaeotawee, P, Udomittipong, K, Nimmannit, A, Tovichien, P, Palamit, A, Charoensitisup, P, et al. Effect of threshold inspiratory muscle training on functional fitness and respiratory muscle strength compared to incentive spirometry in children and adolescents with obesity: a randomized controlled trial. Front Pediatr. (2022) 10:942076. doi: 10.3389/fped.2022.942076
18. De, ANS, Peixoto De, NM, Callegaro, CC, Trevisan, ME, and Jaenisch, RB. Effects of inspiratory muscle training in type 2 diabetes: A systematic review. Br J Cardiovasc Surg. (2023) 38:e20220366. doi: 10.21470/1678-9741-2022-0366
19. Lista-Paz, A, Bouza Cousillas, L, Jácome, C, Fregonezi, G, Labata-Lezaun, N, Llurda-Almuzara, L, et al. Effect of respiratory muscle training in asthma: a systematic review and meta-analysis. Ann Phys Rehabil Med. (2023) 66:101691. doi: 10.1016/j.rehab.2022.101691
20. Li, H, Tao, L, Huang, Y, Li, Z, and Zhao, J. Inspiratory muscle training in patients with heart failure: a systematic review and meta-analysis. Front Cardiovasc Med. (2022) 9:993846. doi: 10.3389/fcvm.2022.993846
21. Beaumont, M, Forget, P, Couturaud, F, and Reychler, G. Effects of inspiratory muscle training in COPD patients: a systematic review and meta-analysis. Clin Respir J. (2018) 12:2178–88. doi: 10.1111/crj.12905
22. Moher, D, Liberati, A, Tetzlaff, J, and Altman, DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. (2009) 151:264–9. doi: 10.7326/0003-4819-151-4-200908180-00135
23. Ouzzani, M, Hammady, H, Fedorowicz, Z, and Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
24. NHLBI (2023). Study quality assessment tools | NHLBI, NIH. [WWW document]. Available at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
25. Guyatt, GH, Oxman, AD, Vist, GE, Kunz, R, Falck-Ytter, Y, Alonso-Coello, P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. (2008) 336:924–6. doi: 10.1136/bmj.39489.470347.AD
27. Higgins, J, Thomas, J, Chandler, J, and Al, E. Cochrane handbook for systematic reviews of interventions version 6.3. Cochrane (2022).
28. Barbalho-Moulim, MC, Miguel, GPS, Forti, EMP, Campos, FDA, and Costa, D. Effects of preoperative inspiratory muscle training in obese women undergoing open bariatric surgery: respiratory muscle strength, lung volumes, and diaphragmatic excursion. Clinics. (2011) 66:1721–7. doi: 10.1590/S1807-59322011001000009
29. Casali, CCC, Pereira, APM, Martinez, JAB, de Souza, HCD, and Gastaldi, AC. Effects of inspiratory muscle training on muscular and pulmonary function after bariatric surgery in obese patients. Obes Surg. (2011) 21:1389–94. doi: 10.1007/s11695-010-0349-y
30. Tenório, LHS, Santos, AC, Câmara Neto, JB, Amaral, FJ, Passos, VMM, Lima, AMJ, et al. The influence of inspiratory muscle training on diaphragmatic mobility, pulmonary function and maximum respiratory pressures in morbidly obese individuals: a pilot study. Disabil Rehabil. (2013) 35:1915–20. doi: 10.3109/09638288.2013.769635
31. Lloréns, J, Rovira, L, Ballester, M, Moreno, J, Hernández-Laforet, J, Santonja, FJ, et al. Preoperative inspiratory muscular training to prevent postoperative hypoxemia in morbidly obese patients undergoing laparoscopic bariatric surgery. A randomized clinical trial. Obes Surg. (2015) 25:1003–9. doi: 10.1007/s11695-014-1487-4
32. Edwards, AM, Graham, D, Bloxham, S, and Maguire, GP. Efficacy of inspiratory muscle training as a practical and minimally intrusive technique to aid functional fitness among adults with obesity. Respir Physiol Neurobiol. (2016) 234:85–8. doi: 10.1016/j.resp.2016.09.007
33. Ahmad, A, and Ali, H. Low-intensity inspiratory loaded exercises improve physical health perception in women with type 2 diabetes. Physiother Q. (2020) 28:9–14. doi: 10.5114/pq.2020.92472
34. Kuo, Y-C, Chang, H-L, Cheng, C-F, Mündel, T, and Liao, Y-H. Six-week inspiratory resistance training ameliorates endurance performance but does not affect obesity-related metabolic biomarkers in obese adults: A randomized controlled trial. Respir Physiol Neurobiol. (2020) 273:103285. doi: 10.1016/j.resp.2019.103285
35. Padula, CA, and Yeaw, E. Inspiratory muscle training: integrative review. Res Theory Nurs Pract. (2006) 20:291–304. doi: 10.1891/rtnp-v20i4a005
36. Romer, LM, and McConnell, AK. Specificity and reversibility of inspiratory muscle training. Med Sci Sports Exerc. (2003) 35:237–44. doi: 10.1249/01.MSS.0000048642.58419.1E
37. Illi, SK, Held, U, Frank, I, and Spengler, CM. Effect of respiratory muscle training on exercise performance in healthy individuals: a systematic review and meta-analysis. Sports Med. (2012) 42:707–24. doi: 10.1007/BF03262290
38. Bisschop, A, Gayan-Ramirez, G, Rollier, H, Gosselink, R, Dom, R, de Bock, V, et al. Intermittent inspiratory muscle training induces fiber hypertrophy in rat diaphragm. Am J Respir Crit Care Med. (1997) 155:1583–9. doi: 10.1164/ajrccm.155.5.9154861
39. Frank, I, Briggs, R, and Spengler, CM. Respiratory muscles, exercise performance, and health in overweight and obese subjects. Med Sci Sports Exerc. (2011) 43:714–27. doi: 10.1249/MSS.0b013e3181f81ca2
40. Romer, LM, and Polkey, MI. Exercise-induced respiratory muscle fatigue: implications for performance. J Appl Physiol. (2008) 104:879–88. doi: 10.1152/japplphysiol.01157.2007
41. Villiot-Danger, J-C, Villiot-Danger, E, Borel, J-C, Pépin, J-L, Wuyam, B, and Vergès, S. Respiratory muscle endurance training in obese patients. Int J Obes. (2011) 35:692–9. doi: 10.1038/ijo.2010.191
42. Shoemaker, MJ, Curtis, AB, Vangsnes, E, and Dickinson, MG. Clinically meaningful change estimates for the six-minute walk test and daily activity in individuals with chronic heart failure. Cardiopulm Phys Ther J. (2013) 24:21–9. doi: 10.1097/01823246-201324030-00004
43. Holland, AE, and Nici, L. The return of the minimum clinically important difference for 6-minute-walk distance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. (2013) 187:335–6. doi: 10.1164/rccm.201212-2191ED
44. Woods, A, Gustafson, O, Williams, M, and Stiger, R. The effects of inspiratory muscle training on inspiratory muscle strength, lung function and quality of life in adults with spinal cord injuries: a systematic review and Meta-analysis. Disabil Rehabil. (2023) 45:2703–14. doi: 10.1080/09638288.2022.2107085
45. Otto-Yáñez, M, Sarmento da Nóbrega, AJ, Torres-Castro, R, Araújo, PRS, Carvalho de Farias, CA, Dornelas de Andrade, AF, et al. Maximal voluntary ventilation should not be estimated from the forced expiratory volume in the first second in healthy people and COPD patients. Front Physiol. (2020) 11:537. doi: 10.3389/fphys.2020.00537
Keywords: inspiratory muscle training, obesity, physical capacity, maximal inspiratory pressure, lung function
Citation: Caicedo-Trujillo S, Torres-Castro R, Vasconcello-Castillo L, Solis-Navarro L, Sanchez-Ramirez D, Núñez-Cortés R, Vera-Uribe R, Muñoz-Muñoz I, Barros-Poblete M, Romero JE and Vilaró J (2023) Inspiratory muscle training in patients with obesity: a systematic review and meta-analysis. Front. Med. 10:1284689. doi: 10.3389/fmed.2023.1284689
Edited by:
Héctor Isaac Rocha-González, Escuela Superior de Medicina (IPN), MexicoReviewed by:
Manuel Alberto Guerrero Gutierrez, Autonomous University of Baja California, MexicoCopyright © 2023 Caicedo-Trujillo, Torres-Castro, Vasconcello-Castillo, Solis-Navarro, Sanchez-Ramirez, Núñez-Cortés, Vera-Uribe, Muñoz-Muñoz, Barros-Poblete, Romero and Vilaró. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rodrigo Torres-Castro, cm9kcml0b3JyZXNAdWNoaWxlLmNs
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.