 Yuehan Ren
Yuehan Ren Junning Zhang
Junning Zhang Weizhen Wu
Weizhen Wu Yi Yuan
Yi Yuan Jiale Wang
Jiale Wang Yi Tang
Yi Tang Yan Liao
Yan Liao Xinmin Liu
Xinmin Liu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 13 December 2023
Sec. Obstetrics and Gynecology
Volume 10 - 2023 | https://doi.org/10.3389/fmed.2023.1268220
Background: Uterine fibroids (UFs) are the most common benign tumors in women of reproductive age. The most effective treatment is myomectomy, but there is no long-term or low-invasive treatment option exists. Acupuncture can be used to treat UFs in a variety of ways. However, there is no meta-analytic synthesis including valid data that explored the efficacy of acupuncture for UFs.
Objective: To assess the efficacy and safety of acupuncture for treating UFs.
Methods: The PRISMA 2020 checklist was used. We identified and extracted the trials through may 2023 from six databases. The quality of the trials was assessed using the risk of bias (2.0). Meta-analysis was performed using RevMan 5.4 software, and it was synthesized using the random-effects model if the included studies were in high heterogeneity. Subgroup and sensitivity analysis were used if necessary.
Results: A total of 1,035 trials were identified, of which 11 were included in the review and meta-analysis. In terms of acupuncture scheme design and fibroid-related symptoms, the trials are highly heterogeneous. All 11 trials have reported acupuncture types, with traditional acupuncture and electroacupuncture being the more representative subgroups. A qualitative review of existing evidence shows that acupuncture has no serious adverse reaction on UFs. Meta-analysis shows that acupuncture can effectively reduce the volume of UFs (MD – 3.89, 95% CI – 5.23 to – 2.56, P < 0.00001) or uterine volume (MD – 16.22, 95% CI – 19.89 To – 12.55, p < 0.00001), reduce the score of fibroid symptoms (MD – 3.03, 95% CI − 3.45 to – 2.60, p < 0.00001), improve the treatment efficiency (RR: 0.19, 95% CI: 0.13 to 0.25, p < 0.00001), and likely do not affect the estrogen level.
Uterine fibroids (UFs), also known as leiomyomas, are benign tumors that arise from the smooth muscle tissue layer (myometrium) of the uterus (1). They are the most common benign tumors in women of reproductive age. The prevalence of UFs is estimated to be between 4.5–80% depending on study populations and diagnostic methods (2–5). Accompanying a high incidence rate, the substantial direct and indirect costs to healthcare payers and society are large. Some studies (6, 7) show that the total costs range from $11,717–25,023 per patient per year, after diagnosis or surgery among patients with UFs.
The exact cause of UFs is unknown, but several risk factors have been identified, including age, race, obesity, and family history. It is worth mentioning that those aged 41–50 or 51–60 years were 10 times more likely to have UFs than those aged 21–30 years (2). Symptoms of UFs can include heavy menstrual bleeding, pelvic pain or pressure, iron deficiency anemia, or urinary frequency, which make a huge impact on women’s quality of life (8).
Treatment options for UFs, such as uterine artery embolization, myomectomy, surgical removal of the uterus (hysterectomy) and high-frequency magnetic resonance-guided focused ultrasound surgery (MRgFUS) (9). However, there are currently no low-invasive treatments that are simple, inexpensive, and effective enough and fertility-preservation (1, 10, 11). Traditional Chinese Medicine (TCM) may provide an alternative option for patients with UFs.
Acupuncture is a key modality based on TCM theory and has been used for thousands of years to treat a wide range of conditions (12, 13). One of the unique features of acupuncture is that it is minimally invasive and has very few side effects when performed by a qualified practitioner. It is also a holistic therapy that aims to treat the underlying causes of disease, rather than just the symptoms. Acupuncture can be used to treat a wide range of conditions, which are commonly used to support fertility and reproductive health (14, 15), as well as to promote overall wellness and balance in the body.
One possible mechanism of acupuncture-treated UFs is through the modulation of the hypothalamic–pituitary-ovarian (HPO) axis (16, 17). The HPO axis plays a critical role in regulating female reproductive function, and it has been linked to the development of UFs (18). Acupuncture has been shown to regulate the HPO axis by modulating the release of gonadotropin-releasing hormone (GnRH) and other hormones involved in reproductive function (19). Another possible mechanism is through the modulation of local blood flow. UFs are known to be highly vascularized (20), and acupuncture has been shown to increase blood flow to the uterus and surrounding tissues (21). This increased blood flow may help to reduce the size and symptoms of UFs. Finally, acupuncture may also have an anti-inflammatory effect. Inflammation has been implicated in the development and progression of UFs, and acupuncture has been shown to reduce levels of pro-inflammatory cytokines in the body (22–25).
Due to the lack of summary evidence for the acupuncture treatment of UFs, we conducted a systematic review and meta-analysis to evaluate the effectiveness and safety of acupuncture treatment of UFs, and to provide evidence-based medicine evidence for clinical decision-makers and guide-makers.
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 checklist was followed. This review had been registered on PROSPERO (ID: CRD42023428921). Considering the actual research situation, some information has been modified.
Randomized controlled trials (RCTs), whether blinded or not, were included.
Patients diagnosed as UFs according to any authoritative clinical guidelines, such as Chinese expert consensus on the diagnosis and treatment of UFs (26).
In our review, the interventions of the treatment group include acupuncture such as traditional acupuncture, electroacupuncture, wrist-ankle acupuncture, abdominal acupuncture, warm acupuncture and moxibustion (a method of fixing moxa sticks on acupuncture needles which seen as a holistic form of therapy) and fire needle therapy.
Comparison interventions include sham acupuncture, traditional Chinese medicine, western medication and no intervention. Both groups of patients could receive routine care. The difference in intervention mode between the two groups was only the specific acupuncture. Trials evaluating acupuncture that made use of nonpenetrating point stimulation, such as acupressure and transcutaneous electrical nerve stimulation (TENS), and trials comparing various acupuncture techniques, were disregarded by the research team.
Primary outcomes were UFs volume or uterine volume. Secondary outcomes included: (i) Quality of life measured using validated scales including The UFs Symptom and Health-Related Quality of Life (UFS-QOL) or other validated TCM syndrome scales; (ii) Estradiol levels during menstruation; (iii) The total effective rate. Improvement of clinical signs and symptoms, and 30% or more reduction of UFs are considered effective; (iv) Safety of the acupuncture intervention including adverse events and withdrawals for any reason.
Six databases were searched from inception to May 23rd, 2023 to identify potentially relevant articles with no restrictions on language. The databases included China National Knowledge Infrastructure (CNKI), Wanfang Database for Chinese Technical Periodicals, PubMed, Web of Science, Embase, and Cochrane Central Registry of Controlled Trials (CENTRAL). The key search terms were (fibroid* or leiomyoma* or fibromyoma* or fibroma*) and (acupuncture or electroacupuncture or acupoint or needling or needle or warm acupuncture and moxibustion or fire needle or wrist-ankle acupuncture). This search contained both MESH and Non-MESH terms. All searches were limited to studies on humans. Reference lists of full text papers were searched, and any relevant articles identified were screened.
The screening was carried out separately by YHR and JNZ. After screening the titles and abstracts of every trial that was searched, the complete texts of any publications that could be pertinent were retrieved and read. Discussions between the two reviewers were used to settle disagreements, occasionally with the help of a third reviewer (WZ W).
Data from included trials were extracted and double-entered into a database for analysis. The following information was extracted and recorded on a standardized data extraction form: publication information (first author, year, title, country), participant characteristics, study design (sample size, age, UFs diagnosis criteria, group assignment, control condition), acupuncture protocol (acupoint formula, technique, treatment session, duration, and frequency), outcomes, time points for assessments, and adverse events. When inadequate data were supplied in the full text, authors were contacted through e-mail to provide extra information on trial details.
Two reviewers (YHR and JNZ) independently assessed the risk of bias using the methods endorsed by The Cochrane Collaboration. This tool appraises trials in seven domains: Random sequence generation (selection bias), Allocation concealment (selection bias), Blinding of participants and personnel (performance bias), Blinding of outcome assessment (detection bias), Incomplete outcome data (attrition bias), Selective reporting (reporting bias), Other bias (acupuncture scheme design bias). Each domain is rated as low risk (of bias), high risk, or unclear risk. Any issues were settled by discussion. The specific detail please review Cochrane Handbook for Systematic Reviews of Interventions.1
Each trial’s acupuncture treatment regimen was analyzed using the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) (27). The STRICTA checklist includes acupuncture rationale, details of needling, treatment regimen, other components of treatment, practitioner background, and comparator interventions.
The meta-analysis was performed using Cochrane Collaboration Review Manager (RevMan 5.4). The continuous data were presented with the mean difference (MD) with 95% confidence intervals (CIs). The dichotomous data were presented using relative risk (RR) with 95% CIs. We analyzed the efficacy differences between therapies by pooling the results of all trials. The I2 statistic was used to assess statistical heterogeneity between trials (28). I2 values of 50% or less indicate no observable heterogeneity, while I2 values of more than 50% indicate significant heterogeneity (29). The random-effects model would be used to synthesize a meta-analysis if there is no significant heterogeneity among the included trials. If heterogeneity was high, we used subgroup analysis or sensitivity analysis to manage data.
The search yielded 1,035 potential titles and abstracts for review, of which 266 were duplicates and 634 were excluded due to ineligible conditions. A total of 135 full-text articles were reviewed for further assessment, of which 122 were excluded for various reasons (see Figure 1). The remaining 11 trials (30–40) were included in our review.
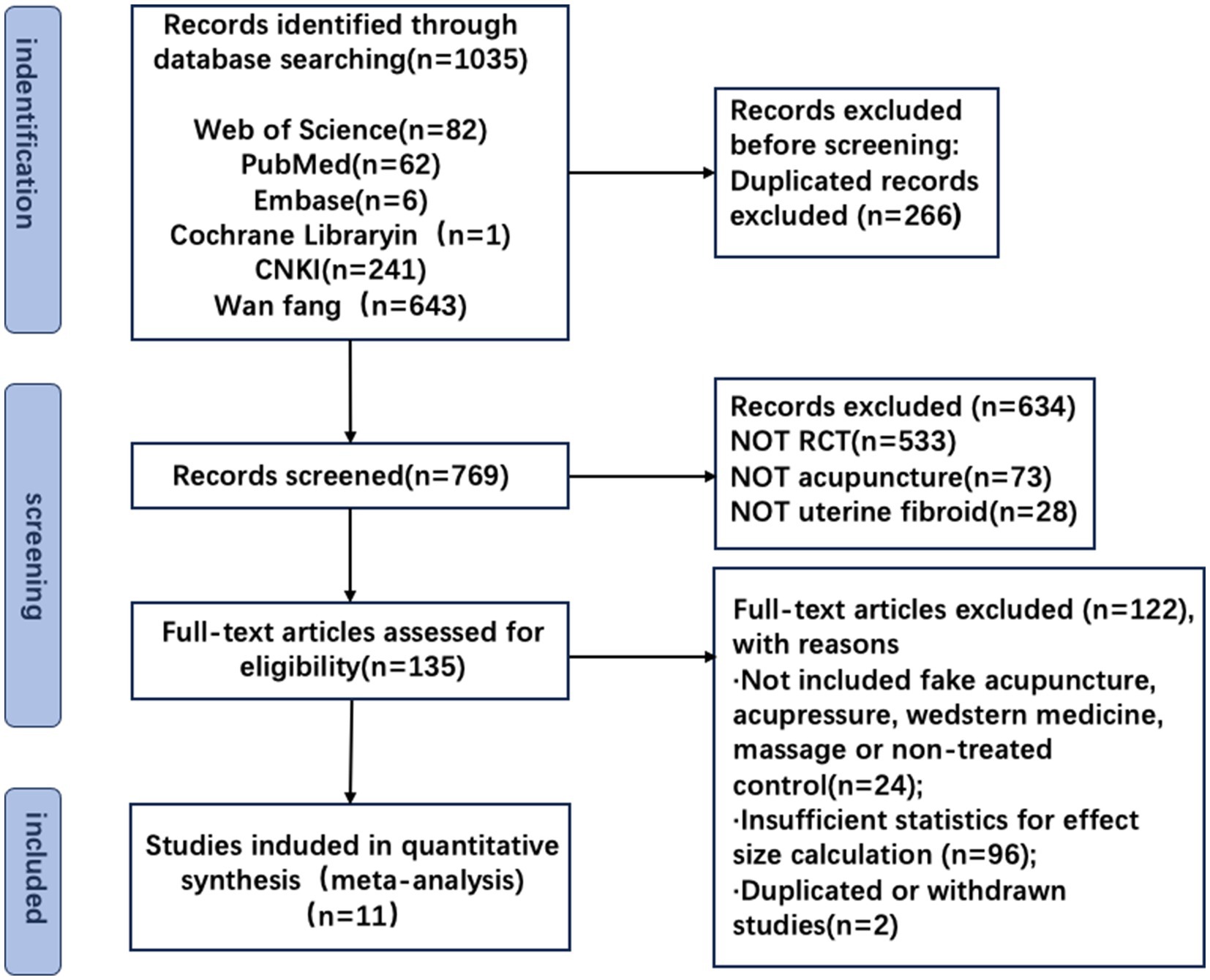
Figure 1. Flowchart of the literature review and selection process.
The summarized characteristics are listed in Table 1. Eleven trials were all published in the Chinese language. Sample size ranged from 60 (31, 32, 37, 39) to 84 (36). The included trials comprised 735 UFs patients (mean age 34 to 48 years). There were 5 participants reported to have withdrawn from included trial (33).

Table 1. Information of the included studies.
All 11 trials enrolled women with UFs and used imaging criteria to determine the diagnosis. Four of the trials (36–38, 40) highlighted clinical symptoms and gynecological tests as supplementary diagnostic tools, such as stomach pain, bladder compression, increased menstrual volume, and longer cycles. Two trials (32, 33) met the criteria for syndrome differentiation of qi stagnation and blood stasis while meeting the diagnosis of UFs, and one trial (39) meet the criteria for syndrome differentiation of blood stasis, as formulated by the Ministry of Health of China in the Guiding Principles for Clinical Research of New Drugs of Traditional Chinese Medicine for UFs.
Of the 11 trials, seven (32–34, 36–38, 40) involved 176 participants using traditional acupuncture, two (31, 35) involved 62 participants using electroacupuncture, one (30) involved 42 participants using warm acupuncture, one (39) involved 30 patients using catgut-embedding therapy (Table 1).
Among the 11 interventions studied, 9 trials used fixed TCM formulas, including Juli Sanjie Pill (30), Shaofu Zhuyu Decoction (31), Fukangle Capsule (32), Xiangling Pill (33), Huoxue Xiaozheng Decoction (37, 38), Guizhi Fuling Capsule (39, 40), and Self formulated decoction (34). One trial (35) selected prescriptions based on syndrome differentiation. One trial (36) used mifepristone (Table 1).
Four trials (30, 32, 33, 39) have set up two control groups. The interventions of the experimental group for these four trials are acupuncture combined with TCM. Only if the control group with only this TCM can show the efficacy of acupuncture. Our review only retained this control group and ignored another control group, which included blank control (39), simple acupuncture (33), mifepristone (30), and unrelated TCM (32).
Figure 2 shows the various biases included in the trials. A graphical summary of the bias risk assessment conducted by the authors based on 7 bias risk areas for the review of 11 included trials is shown in Figure 3. Score 2 points for each item that is high risk, 1 point for items that are ambiguous, and 0 points for those that are low risk. A total score of 1–8 represents little danger, while a score of 9–12 represents high risk. In all domains, no experiment has been judged as having a minimal risk of bias. Our investigation included 11 trials that were all categorized as low risk.
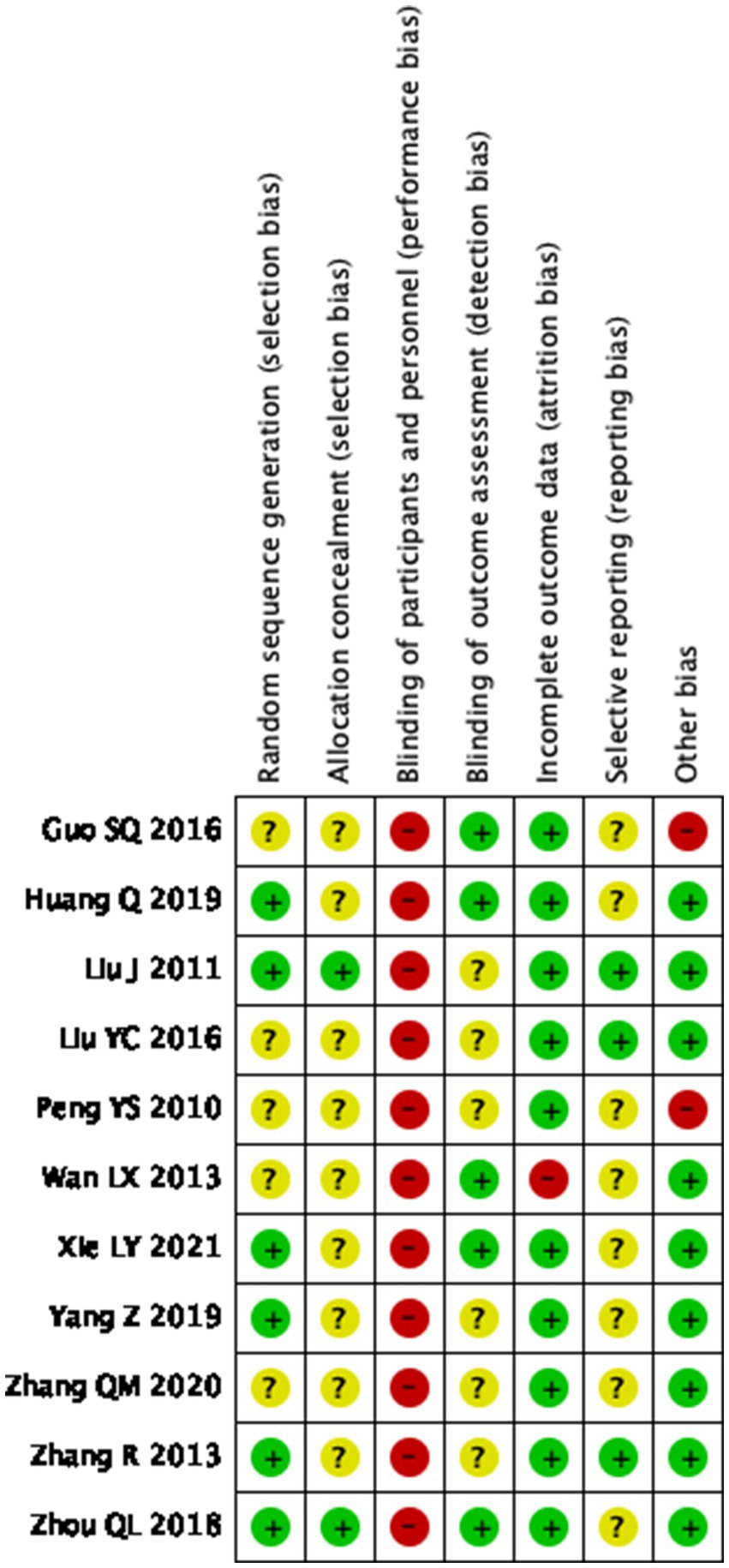
Figure 2. Risk of bias domain for each included study.
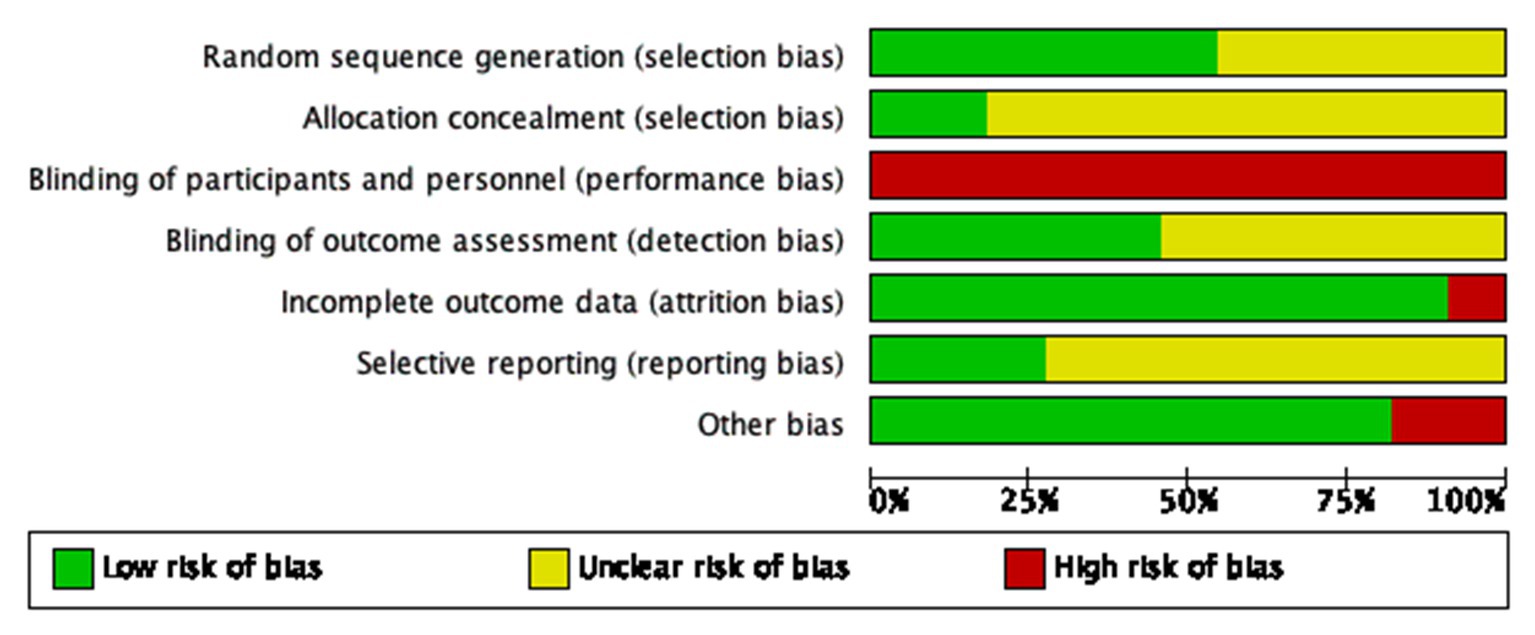
Figure 3. Risk of bias summary.
Six trials (studies 2,3,7,8,10,11) were at low risk of bias for randomization. They mentioned implementation-specific randomization methods, such as random number tables, or random grouping with sequentially numbered, sealed, opaque envelopes. Five trials (studies 1,4,5,6,9) did not describe the method of randomization which was assessed as unclear.
Two trials (studies 3,11) were assessed as low risk of bias for allocation concealment. Jing Liu et al. used a random number table as the method of assigning concealment. Qinglian Zhou et al. use random envelopes to assign concealment. The remaining 9 trials (studies 1,2,4,5,6,7,8,9,10) did not report the method of allocation, so we assessed their risk as unclear.
11 trials involved acupuncture versus oral medication so that participants could not be blinded. We assessed a total of 11 trials as having a high risk for performance bias. Most trials used clinician-rated outcome measures. Five trials (studies 1,2,6,7,11) were rated as having a low risk of detection bias and the remaining six (studies 3,4,5,8,9,10) did not report on blinding of the assessor/clinician, the analyst, or outcome measures, and were rated as unclear risk.
The outcome indicators for trials with only fibroid volume or uterine volume (study 6) are assessed as high-risk. Trials that included other secondary outcome indicators were (studies 1,2,3,4,5,7,8,9,10,11) rated as low risk.
Eight trials (studies 1,2,5,6,7,8,9,11) were rated as unclear risk, owing to no study protocol or trial registration records being available. Three trials (studies 3,4,10) did report data on all included outcomes and were at low risk of bias.
In 9 trials (studies 2,3,4,6,7,8,9,10,11), we rated the risk from other biased sources as low. In two trials (studies 1,5), we evaluated the irrationality of the design of experiments such as acupuncture treatment course and frequency, and these trials were rated as high risk.
Results of 11 trials were summarized to evaluate the clinical efficacy of acupuncture in the treatment of UFs. The volume of UFs was used as the main therapeutic index in 11 trials, the volume of uterus was reported in 3 trials (36, 38, 39), and the estrogen level was included in 2 trials (32, 38). Four trials used a quality-of-life assessment scale, including the UFS-QOL scale (37, 38) and the validated TCM syndrome score (33, 39). Nine trials (30–34, 36, 37, 39, 40) reported effective rates and three (36, 37, 39) reported the occurrence of adverse reactions.
Eleven trials showed that acupuncture was superior to the control group in the volume of UFs, but there was high heterogeneity among them (MD −3.89, 95% CI −5.23 to −2.56, p < 0.00001, I2 = 91%; Supplementary Figure 1). Here, seven trials were divided into two subgroups based on different acupuncture methods and controlled intervention measures. In the subgroup analysis, two trials (studies 2,6) including 124 participants showed that electroacupuncture had better therapeutic effects compared to TCM (MD −6.83, 95% CI −8.79 to −4.86, p < 0.00001, I2 = 8%; Supplementary Figure 2). Five trials (studies 3,4,5,8,11) including 323 participants showed that traditional acupuncture had better effects compared to TCM (MD −0.66, 95% CI −0.87 to −0.44, p < 0.00001, I2 = 31%; Supplementary Figure 2). The remaining four trials (studies 1,7,9,10) were not included in subgroup analysis due to significant differences in acupuncture methods or control intervention measures.
Three trials (studies 7,9,10) involving 208 participants showed that acupuncture has a better therapeutic effect with moderate heterogeneity (MD −16.22, 95% CI −19.89 to −12.55, p < 0.00001, I2 = 59%; Supplementary Figure 3).
In terms of affecting estrogen levels, the therapeutic effect of acupuncture is similar to the control group (MD 3.21, 95% CI – 0.57 to 6.99, p = 0.1, I2 = 34%; Supplementary Figure 4). These data are sourced from two trials (studies 3,9) involving 124 participants.
A meta-analysis was conducted on four trials (studies 4,8,9,10) with 245 participants, and the results showed high heterogeneity (MD −3.03, 95% CI −3.45 to −2.60, p < 0.00001, I2 = 96%; Supplementary Figure 5).
Nine trials (studies 1–5,7,8,10,11) compared the efficacy of acupuncture with other therapies by using effective rates. Five trials (studies 3–5,8,11) found that traditional acupuncture was more effective than conventional Chinese medicine, three trials proved that warm acupuncture and moxibustion (studies 1), acupoint catgut embedding (studies 10), and electroacupuncture (studies 2) were more effective than conventional Chinese medicine, and one trial (studies 3) proved that traditional acupuncture was more effective than mifepristone. In all, the results showed that the efficacy of acupuncture was better than that of the control group (RR: 0.19, 95% CI: 0.13 to 0.25, p < 0.00001, I2 = 0%; Supplementary Figure 6).
Among the three trials that recorded adverse events, one (study 8) did not have any adverse events, while the other (study 10) did not clearly report the specific number of adverse reactions in each group. Only one trial (study 7) reported the specific number and events of adverse reactions, so we did not conduct a meta-analysis of the incidence rate of adverse reactions.
The course of treatment, length of needle retention, and frequency of acupuncture treatment showed diversity in different trials (Supplementary Table 1). Semi-standardized acupuncture protocols were used in two trials (studies 1,5), and standardized methods were used in other trials (studies 2,3,4,6,7,8,9,10,11). The most commonly used acupoints are Guanyuan (RN14), Sanyinjiao (SP6), Zigong (EX-CA1), Xuehai (SP10), Qihai (RN6), Zusanli (ST36), Hegu (LI4), and Taichong (LR3), which have been used more than 5 times. The number of acupoints selected varies from 3 (study 3) to 16 (study 11), with an average of 9.6(SD = 4.2).
Seven trials (studies 3,4,5,7,8,9,11) used traditional acupuncture, two (studies 2,6) used electroacupuncture, one used warm acupuncture and moxibustion (study 1), and one used acupoint catgut embedding (study 10). The frequency of acupuncture is mostly once a day (studies 4,7 8,9), and most patients have been treated for 3 months (studies 1,2,3,6,10,11), with an average duration of 68.7 days (SD = 25.4).
Supplementary Table 2 lists the summary of acupuncture treatment protocol reports using STRICTA standards. All 11 trials reported the style of acupuncture, provided a reason for treatment and comparator interventions in detail. But the details of needling, such as the number and depth of needles inserted, the responses sought, and the needle type, are not detailed enough to meet the STRICTA standard. All trials reported the acupuncture points used, but in two of them (studies 1,7), the acupuncture points were not fixed. Seven trials (studies 1,2,3,4,6,7,11) reported other interventions besides acupuncture, including moxibustion, waveform setting of electroacupuncture instruments, and medical advice during the treatment period. Three trials (studies 3,4,10) reported on the setting and context of treatment and practitioner background.
In assessing the uterine size, we performed a sensitivity analysis by removing data from one trial (39) and found a significant reduction in heterogeneity (I2 = 0%), suggesting that the source of heterogeneity may be the different acupuncture methods.
In assessing the uterine size, the sensitivity analysis results showed that when the last study (study 10) was removed and only the first three studies (studies 4,8,9) were retained, heterogeneity was low, indicating that the therapeutic effect of acupuncture was better than that of the control group (MD −4.68, 95% CI −5.24 to −4.12, p < 0.00001, I2 = 0%; Supplementary Figure 7).
This study reviewed the feasibility, effectiveness, and safety of acupuncture in the treatment of UFs. A total of 11 studies were included in the review and meta-analysis. To our knowledge, this is the first meta-analysis that included studies to solve this specific problem. The preliminary data of the included research shows that acupuncture treatment of UFs has no serious adverse events and is feasible. The sub-group meta-analysis results show that after 1–3 months of treatment, electroacupuncture and traditional acupuncture can reduce the volume of UFs or uterus more effectively than conventional treatment. However, there is not enough high-quality research to conduct subgroup analysis to explore the efficacy of other more diversified acupuncture methods on UFs and evaluate the long-term efficacy.
Study (41) have shown that acupuncture can improve microcirculation and inhibit excessive fibrosis, which may be the effect of treating UFs. However, due to limited clinical trials available, the evidence of acupuncture treatment of UFs is not completely conclusive. Our study comprehensively and systematically reviewed the literature in the databases, identified 11 randomized controlled trials, and provided higher-quality evidence for acupuncture treatment of UFs. The ROB scores of the included trials are all below 9 points. Although according to the high heterogeneity of acupuncture methods and research design, the evidence of using acupuncture to reduce the size of UFs is different, some interesting observations can be found. First of all, each study used the volume of UFs or uterine volume as a therapeutic index, indicating that reducing the volume of UFs is the main treatment goal of patients and doctors in China. Secondly, in approximately half of the studies, patients with TCM syndrome differentiation were recruited, or TCM syndrome differentiation was performed during acupuncture point selection, indicating that acupuncture, as a classic treatment method of TCM, is related to disease types and TCM syndrome types. However, further exploration is needed to determine whether myoma patients can benefit more from syndrome differentiation. Third, UFs are an estrogen-dependent disease. The reduction of estrogen can lead to the reduction of the size of the myoma, this is also the target of western medicine in treating UFs, but acupuncture cannot effectively reduce the estrogen level, which may prove that the mechanism of TCM in treating fibroids is different from western medicine, and the specific molecular pathways affected by acupuncture need further experimental research.
The available research shows that acupuncture is safe in the treatment of UFs. All reported acupuncture-related adverse events were moderate or mild in severity, including dizziness, hot flashes, abdominal pain, etc. All trials indicated normal blood function and normal liver and kidney function, which can help ensure the safety of participants.
In addition, we think it is important to emphasize that acupuncture, as a personalized treatment option, faces some ethical and moral issues as well (42, 43). Here is the premise in the process of diagnosis and treatment, qualified acupuncturists carry out therapeutic operations that are virtually free of side effects and, having informed the patient of the relevant information about the potential risks and benefits prior to the treatment, the patient has the right to decide whether or not to undergo the treatment.
All trials included are effective in terms of methodological quality, but at least one area has been rated as high bias risk. Apart from using sham acupuncture as a controlled study, it is unlikely that blinding procedures will be performed in most trials using an open-label design. Therefore, if the statisticians cannot be blinded, the research results may be affected by selection bias and reduce the credibility of the results.
In addition, the measurement of the results of these trials varies depending on the experiment. As an objective indicator, UFs or uterine volume can directly reflect the curative effect. However, there are still trials that use subjective scales such as symptom scores and psychological status as observation indicators, and most trials do not mention the standardized process of filling out scales, which may affect accuracy to some extent.
The details of the acupuncture treatment plan vary from study to study. Most included trials fail to report sufficient details to meet all STRICTA criteria, which will hinder readers from evaluating the quality of acupuncture treatment. Syndrome differentiation is commonly used in clinical acupuncture treatment, but this personalized diagnostic method is difficult to replicate and evaluate. Standardized acupuncture treatment plans are still the first choice in acupuncture clinical trials. However, many experiments have proven the effectiveness of dialectical treatment, so it is still necessary to find a balance between standardized treatment and flexible personalized treatment.
In conclusion, future research needs to expand the sample size and conduct a more rigorous and effective design of experiments to evaluate the efficacy and safety of acupuncture in the treatment of UFs. The calculation of sample size should be determined based on standardized formulas and previous research. To improve the quality of methodology, future trials should (1) adopt more standardized syndrome differentiation and acupoint selection methods; (2) use standardized scales as outcome indicators (44, 45); (3) comply with STRICTA standards and CONSORT statements; (4) use appropriate blinding methods; and (5) standardize the quality of researchers and the language used in the study.
Due to factors such as acupuncture manipulation and intervention methods in the control group, our review included literature with high heterogeneity. We attempted to reduce heterogeneity through subgroup and sensitivity analysis. First of all, acupuncture techniques (such as traditional acupuncture, electroacupuncture, warm acupuncture and moxibustion, etc.), treatment frequency, and course of treatment are different. These factors may affect the effect measurement and become the source of heterogeneity. Secondly, part of the information in the design of experiments is not comprehensive, such as the specific operation of acupuncture and the background of the researcher are not clear, which greatly limits our evaluation of the quality of the literature. Thirdly, all experiments were conducted in China with strong regional and cultural characteristics, and the risk bias was carefully explained.
Acupuncture has shown great potential in the treatment of UFs, and it may provide an option for conservative alternative therapy for UFs. It is important to clearly emphasize the practical contribution and significance of this study to the future continuation of clinical practice of acupuncture as a minimally invasive adjuvant therapy for UFs. It provides a robust and feasible reference for relevant clinical trials. In the future, more high-quality randomized controlled trials and long-term follow-ups are needed to better verify acupuncture’s effectiveness and safety in treating UFs.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
YR: Writing – original draft, Writing – review & editing. JZ: Writing – original draft, Writing – review & editing. WW: Data curation, Writing – review & editing. YY: Data curation, Formal analysis, Writing – review & editing. JW: Visualization, Writing – original draft. YT: Validation, Writing – original draft. YL: Validation, Writing – original draft. XL: Project administration, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study is funded by Science and Technology Innovation Project of the Chinese Academy of Traditional Chinese Medicine (ref no: C12021A02404). The funding body is not involved in the study design and conduct, data collection, management, analysis, and interpretation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2023.1268220/full#supplementary-material
1. McWilliams, MM, and Chennathukuzhi, VM. Recent advances in uterine fibroid etiology. Semin Reprod Med. (2017) 35:181–9. doi: 10.1055/s-0037-1599090
2. Stewart, EA, Cookson, CL, Gandolfo, RA, and Schulze-Rath, R. Epidemiology of uterine fibroids: a systematic review. BJOG. (2017) 124:1501–12. doi: 10.1111/1471-0528.14640
3. Boosz, AS, Reimer, P, Matzko, M, Römer, T, and Müller, A. The conservative and interventional treatment of fibroids. Dtsch Arztebl Int. (2014) 111:877–83. doi: 10.3238/arztebl.2014.0877
4. Whiteman, MK, Kuklina, E, Jamieson, DJ, Hillis, SD, and Marchbanks, PA. Inpatient hospitalization for gynecologic disorders in the United States. Am J Obstet Gynecol. (2010) 202:541.e1–6. doi: 10.1016/j.ajog.2009.12.013
5. Soriful Islam, M, Protic, O, Giannubilo, SR, Toti, P, Tranquilli, AL, Petraglia, F, et al. Uterine leiomyoma: available medical treatments and new possible therapeutic options. J Clin Endocrinol Metabol. (2013) 98:921–34. doi: 10.1210/jc.2012-3237
6. Soliman, AM, Yang, H, du, EX, Kelkar, SS, and Winkel, C. The direct and indirect costs of uterine fibroid tumors: a systematic review of the literature between 2000 and 2013.[J]. Am J Obstet Gynecol. (2015) 213:141–60. doi: 10.1016/j.ajog.2015.03.019
7. Arip, M, Yap, VL, Rajagopal, M, Selvaraja, M, Dharmendra, K, and Chinnapan, S. Evidence-based Management of Uterine Fibroids with Botanical Drugs-a Review. Front Pharmacol. (2022) 13:878407. doi: 10.3389/fphar.2022.878407
8. Fraser, IS, Critchley, HO, Munro, MG, and Broder, M. A process designed to lead to international agreement on terminologies and definitions used to describe abnormalities of menstrual bleeding. Writing group for this menstrual agreement process. Fertil Steril. (2007) 87:466–76. doi: 10.1016/j.fertnstert.2007.01.023
9. Donnez, J, and Dolmans, MM. Uterine fibroid management: from the present to the future. Hum Reprod Update. (2016) 22:665–86. doi: 10.1093/humupd/dmw023
10. Dolmans, MM, Donnez, J, and Fellah, L. Uterine fibroid management: today and tomorrow. J Obstet Gynaecol Res. (2019) 45:1222–9. doi: 10.1111/jog.14002
11. American College of Obstetricians and Gynecologists. ACOG practice bulletin. Alternatives to hysterectomy in the management of leiomyomas. Obstet Gynecol. (2008) 112:387–400. doi: 10.1097/AOG.0b013e318183fbab
12. Zhu, J, Li, J, Yang, L, and Liu, S. Acupuncture, from the ancient to the current. Anat Rec (Hoboken). (2021) 304:2365–71. doi: 10.1002/ar.24625
13. Chang, S. The meridian system and mechanism of acupuncture-a comparative review. Part 1: the meridian system. Taiwan J Obstet Gynecol. (2012) 51:506–14. doi: 10.1016/j.tjog.2012.09.004
14. Bishop, KC, Ford, AC, Kuller, JA, and Dotters-Katz, S. Acupuncture in obstetrics and gynecology. Obstet Gynecol Surv. (2019) 74:241–51. doi: 10.1097/OGX.0000000000000655
15. Franconi, G, Manni, L, Aloe, L, Mazzilli, F, Giambalvo Dal Ben, G, Lenzi, A, et al. Acupuncture in clinical and experimental reproductive medicine: a review. J Endocrinol Invest. (2011) 34:307–11. doi: 10.1007/BF03347091
16. Yang, L, Xu, HF, Gou, MH, Yang, HS, Feng, YX, Liu, SY, et al. Study on the application of acupuncture for regulating menstruation and promoting pregnancy in the treatment of ovarian function decline. Zhongguo Zhen Jiu. (2022) 42:1200–4. doi: 10.13703/j.0255-2930.20220505-k0002
17. Zhu, H, Nan, S, Suo, C, Zhang, Q, Hu, M, Chen, R, et al. Electro-acupuncture affects the activity of the hypothalamic-pituitary-ovary Axis in female rats. Front Physiol. (2019) 10:466. doi: 10.3389/fphys.2019.00466
18. Syed, YY. Relugolix/estradiol/Norethisterone (Norethindrone) acetate: a review in symptomatic uterine fibroids. Drugs. (2022) 82:1549–56. doi: 10.1007/s40265-022-01790-4
19. Chang, R, Chung, PH, and Rosenwaks, Z. Role of acupuncture in the treatment of female infertility. Fertil Steril. (2002) 78:1149–53. doi: 10.1016/S0015-0282(02)04348-0
20. Henri, M, Florence, E, Aurore, B, Denis, H, Frederic, P, Francois, T, et al. Contribution of contrast-enhanced ultrasound with Sonovue to describe the microvascularization of uterine fibroid tumors before and after uterine artery embolization. Eur J Obstet Gynecol Reprod Biol. (2014) 181:104–10. doi: 10.1016/j.ejogrb.2014.07.030
21. Liu, W, Wang, CC, Lee, KH, Ma, X, and Kang, TL. Research methodology in acupuncture and moxibustion for managing primary dysmenorrhea: a scoping review. Complement Ther Med. (2022) 71:102874. doi: 10.1016/j.ctim.2022.102874
22. Li, N, Guo, Y, Gong, Y, Zhang, Y, Fan, W, Yao, K, et al. The anti-inflammatory actions and mechanisms of acupuncture from Acupoint to target organs via neuro-immune regulation. J Inflamm Res. (2021) 14:7191–224. doi: 10.2147/JIR.S341581
23. Zhang, B, Shi, H, Cao, S, Xie, L, Ren, P, Wang, J, et al. Revealing the magic of acupuncture based on biological mechanisms: a literature review. Biosci Trends. (2022) 16:73–90. doi: 10.5582/bst.2022.01039
24. Yu, WY, Ma, LX, Zhang, Z, Mu, JD, Sun, TY, Tian, Y, et al. Acupuncture for primary dysmenorrhea: a potential mechanism from an anti-inflammatory perspective. Evid Based Complement Alternat Med. (2021) 2021:1907009–12. doi: 10.1155/2021/1907009
25. Cetin, E, Al-Hendy, A, and Ciebiera, M. Non-hormonal mediators of uterine fibroid growth. Curr Opin Obstet Gynecol. (2020) 32:361–70. doi: 10.1097/GCO.0000000000000650
26. Chinese expert consensus expert group on the diagnosis and treatment of uterine fibroid. Chinese expert consensus on the diagnosis and treatment of uterine fibroid. Chinese J Obstetrics and Gynecology. (2017) 12:793–800. doi: 10.3760/cma.j.issn.0529-567x.2017.12.001
27. Mac Pherson, H, Altman, DG, Hammerschlag, R, Li, Y, Wu, T, White, A, et al. Revised standards for reporting interventions in clinical trials of acupuncture (STRICTA)–extending the CONSORT statement. J Altern Complement Med. (2010) 3:140–55. doi: 10.1111/j.1756-5391.2010.01086.x
28. Higgins, JP, Thomas, J, Chandler, J, Cumpston, M, Li, T, Page, MJ, et al. Cochrane handbook for systematic reviews of interventions. US: John Wiley and Sons (2019).
29. Ioannidis, JP, Patsopoulos, NA, and Evangelou, E. Uncertainty in heterogeneity estimates in meta-analyses. BMJ. (2007) 335:914–6. doi: 10.1136/bmj.39343.408449.80
30. Guo, S, Lin, X, Yang, C, He, W, Zhang, Y, and Li, W. Clinical observation on warm acupuncture combined with Juli Sanjie pill in the treatment of uterine fibroids. Shanghai J Acupuncture. (2016) 35:437–9. doi: 10.13460/j.issn.1005-0957.2016.04.0437
31. Huang, Q. Clinical efficacy of electroacupuncture combined with Shaofuzhuyu decoction in the treatment of uterine fibroids and its influence on the volume of fibroids. J Electrocardiography (electronic). (2019) 8:88–9.
32. Liu, J. Clinical observation on the treatment of uterine fibroid by acupuncture with Hefukangle capsule [master, Liaoning medical college]. (2011).
33. Liu, Y. Observation on curative effect of acupuncture combined with traditional Chinese medicine in treating uterine fibroids of qi-stagnation and blood-stasis type [master, Heilongjiang University of Chinese medicine]. (2016).
34. Peng, X, Qian, X, and Peng, G. Clinical study of acupuncture combined with Chinese medicine in the treatment of uterine fibroids. China Medical Guide. (2010) 7:82–3. doi: 10.3969/j.issn.1673-7210.2010.02.050
35. Wan, L. Analysis of curative effect of Chinese medicine, electroacupuncture and acupuncture in the treatment of uterine fibroids. J Mudanjiang Medical College. (2013) 34:69–71. doi: 10.13799/j.cnki.mdjyxyxb.2013.0.013
36. Xie, L, Zhao, X, Li, X, and Shi, L. Effect of acupuncture combined with mifepristone on serum MCP-1, ER and PR in patients with uterine fibroids. Shanghai J Acupuncture. (2021) 40:1353–7. doi: 10.13460/j.issn.1005-0957.2021.11.1353
37. Yang, Z, Li, X, and Li, Q. Clinical study on the treatment of uterine fibroids by acupuncture combined with Huoxue Xiaoshi prescription. Massage and rehabilitation Medicine. (2019) 10:30–2. doi: 10.19787/j.issn.1008-1879.2019.14.013
38. Zhang, Q. Effect of acupuncture combined with Huoxue Xiaoshi prescription on ovarian function and volume of uterine fibroids. Guangming Chinese Med. (2020) 35:1018–20. doi: 10.3969/j.issn.1003-8914.2020.07.022
39. Zhang, R. Clinical observation on therapeutic effect of acupoint embedding and Guizhi Tuckahoe capsule on uterine fibroids [master, Shanxi College of Traditional Chinese Medicine]. (2013).
40. Zhou, Q, Liu, J, Du, Y, and Tao, Y. (2018) A randomized controlled study of acupuncture and drug therapy for uterine fibroids. Hebei traditional Chinese medicine. 40: 1245–1271. doi: 10.3969/j.issn.1002-2619.2018.08.028
41. Liu, S, Wang, R, Luo, D, Xu, Q, Xiao, C, Lin, P, et al. Effects of electroacupuncture on recovery of the electrophysiological properties of the rabbit gastrocnemius after contusion: an in vivo animal study. BMC Complement Altern Med. (2015) 15:69. doi: 10.1186/s12906-015-0601-z
42. Gullo, G, Scaglione, M, Buzzaccarini, G, Laganà, AS, Basile, G, Chiantera, V, et al. Cell-free fetal DNA and non-invasive prenatal diagnosis of Chromosomopathies and pediatric monogenic diseases: a critical appraisal and medicolegal remarks. J personalized medicine. (2022) 13:1. doi: 10.3390/jpm13010001
43. Piergentili, R, Basile, G, Nocella, C, Carnevale, R, Marinelli, E, Patrone, R, et al. Using nc RNAs as tools in Cancer diagnosis and treatment-the way towards personalized medicine to improve Patients' health. Int J Mol Sci. (2022) 23:9353. doi: 10.3390/ijms23169353
44. Long, Y, Liu, B, Mao, S, and Ma, L. Review and prospect of acupuncture standardization in China. Zhongguo Zhen Jiu. (2016) 36:1337–40. doi: 10.13703/j.0255-2930.2016.12.031
Keywords: acupuncture, uterine fibroid, complementary therapy, systematic review, meta-analysis
Citation: Ren Y, Zhang J, Wu W, Yuan Y, Wang J, Tang Y, Liao Y and Liu X (2023) Should acupuncture become a complementary therapy in the treatment of uterine fibroid: a systematic review and meta-analysis of randomized controlled trials. Front. Med. 10:1268220. doi: 10.3389/fmed.2023.1268220
Edited by:
Guanhu Yang, Ohio University, United StatesReviewed by:
Giuseppe Basile, IRCCS Istituto Ortopedico Galeazzi, ItalyCopyright © 2023 Ren, Zhang, Wu, Yuan, Wang, Tang, Liao and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xinmin Liu, Z2FtbGl1eGlubWluQDE2My5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.