 Borja Perez-Dominguez1*
Borja Perez-Dominguez1* Sara Perpiña-Martinez2
Sara Perpiña-Martinez2 Isabel Escobio-Prieto3,4
Isabel Escobio-Prieto3,4 Marta de la Fuente-Costa5
Marta de la Fuente-Costa5 Alvaro Manuel Rodriguez-Rodriguez5
Alvaro Manuel Rodriguez-Rodriguez5 Maria Blanco-Diaz5
Maria Blanco-Diaz5- 1Department of Physiotherapy, Exercise Intervention for Health Research Group, University of Valencia, Valencia, Spain
- 2Faculty of Health Sciences, Pontifical University of Salamanca, Madrid, Spain
- 3Department of Physiotherapy, Faculty of Nursing, Physiotherapy and Podiatry, University of Seville, Seville, Spain
- 4Research group CTS-1043: Health, Physiotherapy and Physical Activity, Institute of Biomedicine of Seville (IBIS), Seville, Spain
- 5Faculty of Medicine and Health Sciences, Physiotherapy and Translational Research Group, Institute of Health Research of the Principality of Asturias, University of Oviedo, Oviedo, Spain
Introduction: Some patients with rotator cuff injuries do not report significant changes in pain-related outcomes. Pain self-efficacy, which is commonly assessed using the Pain Self-Efficacy Questionnaire, may contribute toward this outcome. However, a Spanish adaptation of this questionnaire is currently lacking. Therefore, this study’s purpose was developing the Spanish version of this questionnaire, and assess its psychometric properties.
Methods: The Spanish version of the Pain Self-Efficacy Questionnaire was translated and culturally adapted, and a sample of 107 patients with rotator cuff injuries completed the questionnaire to examine its convergent validity (analyzing its correlation with the Tampa Scale of Kinesiophobia), its test–retest reliability, for which a subset of 40 participants completed again the questionnaire, and its internal consistency.
Results: Translation was conducted without any problems, and 107 participants completed the study. Mean scores for the Pain Self-Efficacy Questionnaire were 45.2 points (standard deviation, 11.4). The Pain Self-Efficacy Questionnaire showed a moderate negative correlation with the Tampa Scale of Kinesiophobia (Pearson’s correlation index r = −0.48) supporting its convergent validity. High test–retest reliability (Intraclass Correlation Coefficient of 0.90) and excellent internal consistency (Cronbach’s α value of 0.92) were also found.
Discussion: The Spanish version of the Pain Self-Efficacy Questionnaire presents high validity, test–retest reliability, and internal consistency to assess pain self-efficacy in patients suffering rotator cuff injuries in Spanish-speaking settings.
1. Introduction
Rotator cuff injuries account for 80% of primary care consultations for shoulder pain (1), and their incidence increases with age (2). These injuries, among other problems such as weakness and loss of function, can cause significant levels of pain that are crucial when deciding treatment strategies (3). Despite the development of many effective interventions to improve symptoms, around 30% of the patients report no significant change in pain-related outcomes, and psychosocial, occupational and lifestyle factors have been identified as possible reasons for this (1).
One of these factors is pain self-efficacy. Originally defined by Albert Bandura, self-efficacy is one’s confidence or belief in their capacity goal achievement or activity performance (4). Higher levels of self-efficacy are suggested as predictors of better prognosis in patients with musculoskeletal pain (5), less disability, pain, fatigue, or emotional distress (6). Self-efficacy, therefore, determines the willingness to persist when obstacles are faced, avoids shying away from a complicated task, and shows commitment to achieving a goal (7).
The assessment of self-efficacy, as it is a belief, must be self-administered. To assess self-efficacy, many tools have been developed. Some of them are specific to a condition, such as the Arthritis Self-Efficacy Scale (ASES) or the Chronic Disease Self-Efficacy Scale, and some are related to pain and altered pain states, such as the Chronic Pain Self-Efficacy Scale or the Pain Self-Efficacy Scale (PSEQ) (8, 9). When dealing with clinical settings involving musculoskeletal disorders, the PSEQ is the preferred scale used by clinicians (10). It is a short and comprehensive questionnaire composed with 10 items first developed in English, aimed to assess the confidence or ability people with pain have to achieve activities despite their pain (11). The PSEQ assesses several dimensions, including physical functioning, social interaction, and participation in activities of the daily living when pain is present (11).
Translated and adapted versions of the PSEQ have assessed its psychometric properties in several languages, such as Amharic (7), Arabic (12), Canadian-French (1), Catalan (13), Chinese-Hong Kong (14), Chinese-Mainland (15), Danish (16), Italian (17), Farsi (18), Japanese (19), Marathi (20), Mongolian (21), Portuguese-Brazilian (22), Portuguese-European (23), and Yoruba (24). All of these translations were performed rigorously, and several of them adapted items from the questionnaire to their culture. Despite this, a validated version of this questionnaire in Spanish is lacking, limiting its access to healthcare professionals who develop their practice in Spanish-speaking settings. Therefore, this study aimed to translate and culturally adapt the Spanish version of the PSEQ, and examine its psychometric properties.
2. Materials and methods
2.1. Participants
This cross-sectional study was conducted at a private practice Hospital in Valencia, Spain, and included a sample of patients with rotator cuff injuries that were considered for surgical repair. Recruitment of participants was conducted between March and May 2023. Participants were included based on the following eligibility criteria: (1) adults >18 years old, (2) with a medically diagnosed rotator cuff injury considered for surgical repair, and (3) willingness to participate in the study. Participants were excluded if they had any cognitive impairments that could interfere with the completion of the assessment or if they were illiterate in Spanish. A briefing on the purpose of the study was given to the participants by a member of the research team during consultation with the surgeon, and gave written consent before being considered for enrollment in this study.
2.2. Measures
Baseline demographic characteristics from the sample were obtained for descriptive purposes, including sex, age, if the involved side was dominant or not, educational level (uneducated, primary, high school, college) and work status (part-time, full-time, unemployed, or retired).
The PSEQ is a 10-item questionnaire aimed to assess the confidence or ability people with pain have to achieve activities despite their pain. It includes lifestyle, social and daily activity questions the participant has to rate from 0 (not at all confident) to 6 (completely confident) in a Likert-style scale. Scores range from 0 to 60, with higher values indicating stronger self-efficacy levels (11). The psychometric properties, such as a high internal consistency, a high degree of stability, and construct validity of this assessment tool have been previously reported (7, 10).
The Tampa Scale of Kinesiophobia (TSK) was used as a validity criterion. It assesses fear-avoidance behaviors related to pain, and it has been previously translated and adapted in Spanish (25). In each item, patients have to answer in a 4-item Likert-style scale if they strongly agree (1) or strongly disagree (4) with the given statement. The total score ranges from 17 to 68 points, with higher values indicating stronger fear-avoidance behaviors. The preliminary Spanish version of the TSK was reviewed by a group of bilingual experts, including healthcare professionals and researchers familiar with the target population. They assessed the clarity, comprehensibility, and appropriateness of the translated items in the Spanish context. Any necessary modifications or adjustments were made based on their feedback and consensus.
2.3. Procedures
2.3.1. Translation and cultural adaptation
Before starting the translation and cross-cultural adaptation process, the original developer of the PSEQ (Professor Michael K. Nicholas) was contacted for the permission to translate and adapt the original English version of the PSEQ into Spanish. Established guidelines must be followed to translate and culturally adapt a questionnaire to a new language and cultural setting (26). The following steps were followed in the translation process: (1) The first author, bilingual in Spanish and English, translated every item from its original English version to Spanish, (2) a forward translation was then conducted twice by two independent authors who were also fluent in both languages, and to solve any differences between those authors, consensus was obtained. Finally (3) a back translation from Spanish to English was conducted twice by two independent authors fluent in both languages. Once the final version of the Spanish translation was approved by every member in the research team through consensus, a preliminary testing for cognitive debriefing was conducted in a small sample of 30 patients with rotator cuff injuries to assess comprehensiveness and clarity of the translated items.
2.3.2. Data collection
Data collection was carried out by two experienced physiotherapist members of the research team from March to May 2023, and was registered in a spreadsheet for further analysis. During their medical visit, participants were asked to complete a short form with their sociodemographic and clinical information, the Spanish version of the PSEQ, and the TSK. To assess test–retest reliability, a subset of 40 participants was asked to complete again the PSEQ within a week after completing it for the first time.
2.4. Statistical analysis
To conduct statistical analyses, SPSS Statistics (IBM, Armonk, NY, United States) software, in its 23.0 version for MacOS was used. Baseline demographic information was described as means (standard deviations) for continuous data, and counts (percentages) for categorical data. The Kolmogorov–Smirnov test was used to check for data normal distribution. Missing values were handled using mean imputation. This method involved replacing missing values with the mean value of the available data for each respective variable. Floor and ceiling effects were established and determined by calculating if >15% of the responses given by participants corresponded to the minimum possible score of 0 or the maximum possible score of 60 (27).
2.4.1. Sample size estimation
Published guidelines with established requirements for the validation of a survey-like instrument were followed to conduct the sample size estimation (10 participants per item in the tool) (28). Also, the COSMIN recommendation for the selection of health-status measurement instruments were followed (29), establishing that the sample should at least be seven times the total number of items and ≥ 100. A sample of a minimum of 100 respondents was required, as the PSEQ is a 10-item questionnaire.
2.4.2. Validity
An exploratory factor analysis (EFA) was conducted to assess validity through an exploratory principal component analysis (PCA) with Varimax rotation, establishing the number of generated domains using the Scree test criteria (30). Keyser-Meyer-Olkin (KMO) measure was used for sampling adequacy at >0.8 to be considered good, and the Bartlett test for sphericity was used to determine the level of significance (31, 32). Similar to what previous studies have reported (1, 11–19, 22, 23), a one-factor solution is hypothesized to be found in the factorial analysis.
Additionally, convergent validity was also assessed, and it is defined as how close a measurement tool is related to other measurement tools that assess the same (or similar) constructs. To conduct convergent validity analysis, our a priori hypothesis was that the PSEQ would have a significant negative correlation with fear-avoidance behaviors related to pain, assessed through the Tampa Scale of Kinesiophobia (TSK) (25), as shown in similar studies (12, 15, 17). This outcome has been previously associated with pain-self efficacy, and has been also recommended as a core pain-related assessment in pain clinical trials (33). Pearson’s correlation coefficient was used to establish correlation levels between these tools. As reported in similar studies that aimed to validate a translated version of the PSEQ (14, 18), absolute values above 0.3 are sufficient to support the tool’s validity.
2.4.3. Test–retest reliability
Stability over time is assessed by conducting a test–retest reliability analysis, by assessing the same outcome twice in the same group of people and establishing the level of correlation between responses. To assess test–retest reliability, the Intraclass Correlation Coefficient (ICC) was used (model alpha, 2-way random effects model). ICC establishes a coefficient that ranges from 0 to 1, being 0 no correlation and 1 the highest correlation possible. Scores ranging from 0 to 0.4 are considered to have low correlation, from 0.4 to 0.6 moderate correlation, 0.6 to 0.8 average correlation and scores above 0.8 show excellent correlation (34). A subset of 40 participants was asked to complete again the PSEQ within a week after completing it for the first time. Additionally, a Bland–Altman graph was also created to plot the mean differences of the measurements with their limits of average difference corresponding limits ± the standard deviation’s difference (35).
Absolute reliability measures were also calculated through the standard error of measurement (SE) and the minimal detectable change (MDC). The MDC represents the smallest change in scores that can be considered beyond measurement error and is required to confidently conclude that a meaningful change has occurred in an individual’s pain self-efficacy. To calculate the SE, the following formula was used: SD × √(1-R), where SD is the Standard Deviation and R is the reliability coefficient of the instrument (36). To calculate the MDC, the following formula was used: 1.96 × √2× SE.
2.4.4. Internal consistency
Internal consistency is the degree of relatedness between the items of an assessment tool (12). To assess the internal consistency of the PSEQ, Cronbach’s α was calculated. Cronbach’s α values range between 0 and 1, and an α value >0.9 was considered excellent, > 0.8 was considered good, and > 0.7 was considered acceptable (37). Corrected-total item correlation was also assessed to establish association levels between the items and the total score of the PSEQ.
3. Results
107 participants completed the questionnaire. Researchers in charge of the translation reached an agreement during the translation and adaptation process of the PSEQ into Spanish (PSEQ-Sp) and in a Spanish context. None of the items of the original were removed during the translation process.
3.1. Descriptive statistics
Demographic and clinical data of the study sample is shown in Table 1. Data was normally distributed. 112 participants met inclusion criteria and were enrolled in the study. However, 5 of them failed to complete all of the outcome measures and were excluded from the final analyses, leaving a total final sample of 107 participants. The sample included 48 males and 59 females, and the mean age was 49.4 years (SD 12.9). The vast majority of participants had a high educational level (97% had at least a High School degree), and were currently employed (91%).
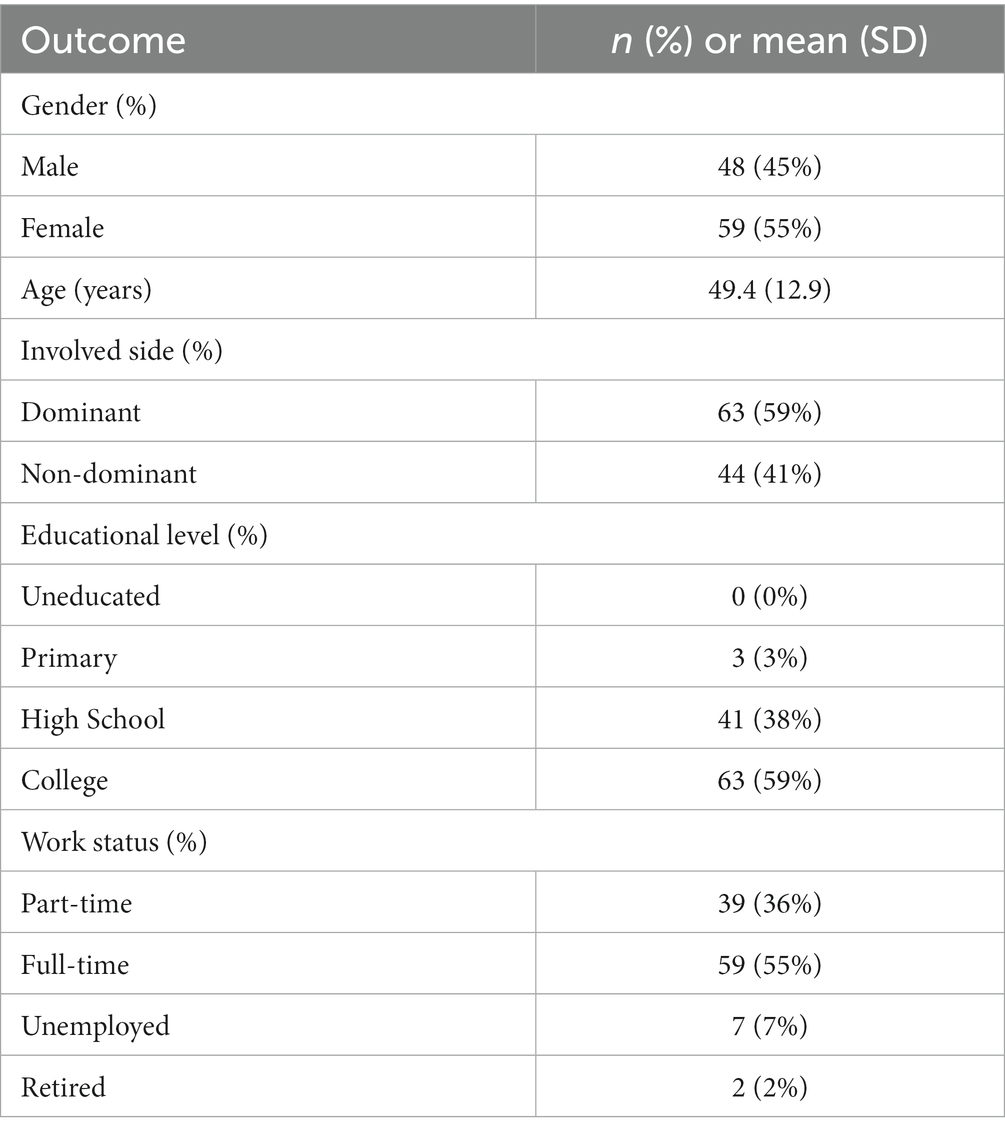
Table 1. Baseline demographic characteristics from the sample.
The PSEQ-Sp mean score was 45.2 points (SD 11.4), and the TSK mean score was 46.6 points (SD 8.2). The PSEQ ranges from 0 to 60, and the TSK ranges from 17 to 68 points. None of the participants reported the lowest possible score 0, and only 3 (3%) of them reported the maximum score possible 60, so no significant floor and ceiling effects were found.
3.2. Validity
Results for the EFA are presented in Table 2. The value for the KMO assessing sampling adequacy was 0.90 and the score for Bartlett’s test was X2 = 1,866.08 (p < 0.001), suggesting that sampling was adequate, and data was appropriate for factor analysis. The exploratory factor analysis yielded for the PSEQ-Sp a one-factor solution, which accounted for 66% of the variance, as every item’s factor loading was >0.5. Additionally, every participant completed the PSEQ-Sp and the TSK measures, and the convergent validity analysis found a significant moderate negative correlation between the PSEQ-Sp and the TSK (Pearson’s correlation index r = −0.48, p < 0.001).
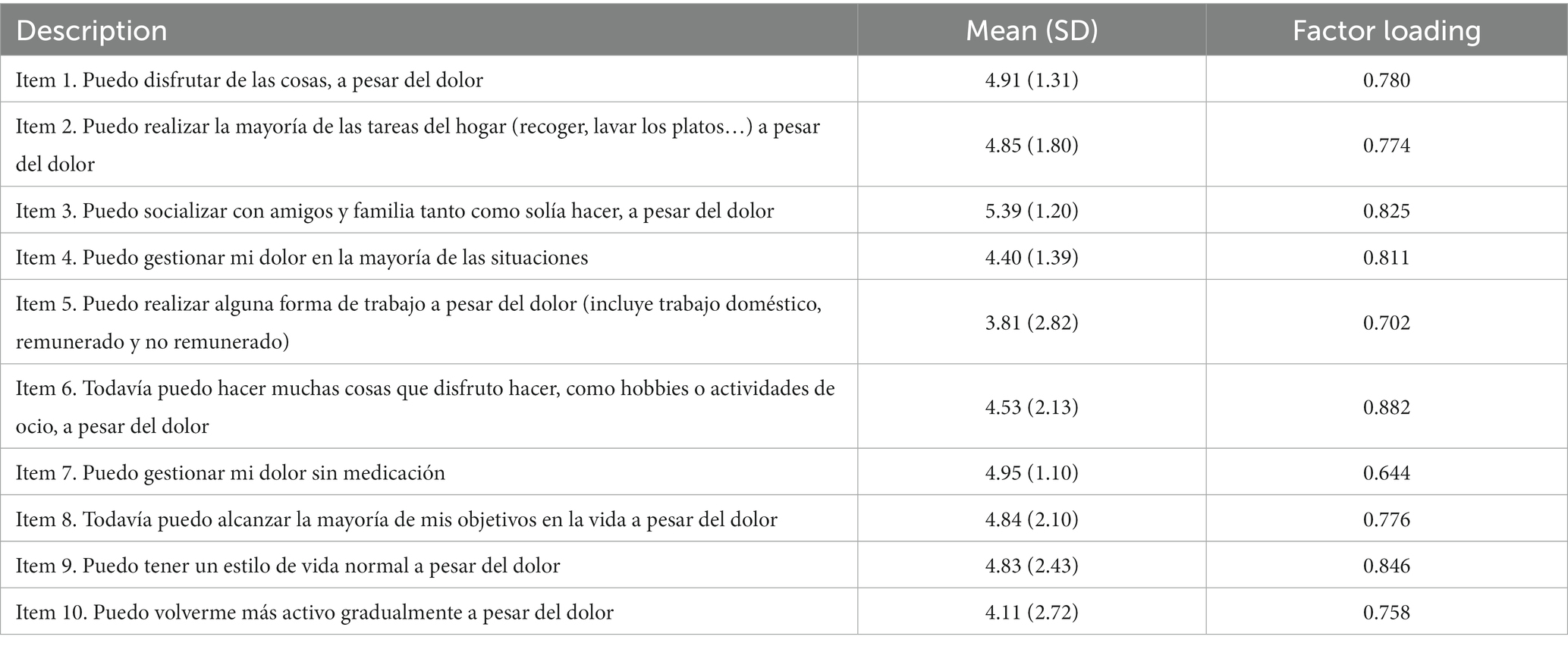
Table 2. Exploratory factor analysis results of the Spanish version of the PSEQ.
3.3. Test–retest reliability
Results for the test–retest reliability analysis are shown in Table 3. Every participant invited to respond to the PSEQ-Sp for a second time completed the questionnaire. The overall ICC for the PSEQ was 0.90 (95% CI 0.88–0.93), showing excellent correlation levels. ICC’s for each individual item ranged from 0.77 to 0.86. The SE was 1.23 and the MDC was 3.05 points, respectively. Additionally, most of the pair differences are between the agreement limits, as shown in the Bland–Altman plot graph (Figure 1). This implies that test–retest measure of the PSEQ-Sp have a high concordance.
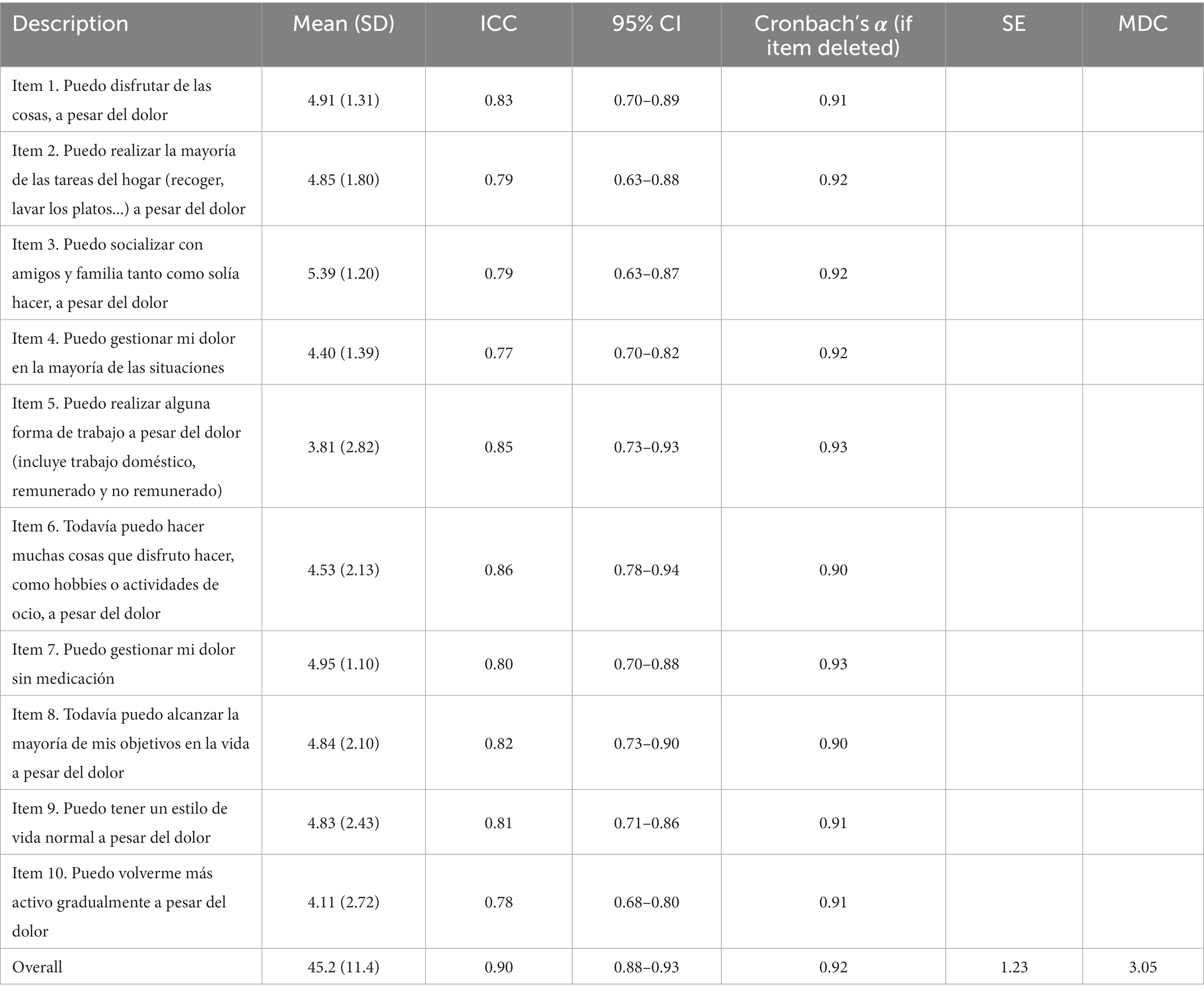
Table 3. Descriptive statistics, internal consistency values, and intraclass correlations of the items in the PSEQ.

Figure 1. Results for the Bland-Altman plot graph.
3.4. Internal consistency
Results for the internal consistency analysis are shown in Table 3. The PSEQ-Sp showed overall excellent internal consistency, with a Cronbach’s α value of 0.92. Moreover, the Corrected-item total correlation values for Cronbach’s α if an item was deleted were also excellent, ranging from 0.90 to 0.93. These findings indicate that there is a strong association between the items and the total score.
4. Discussion
The aim of the present study was to translate and culturally adapt the Spanish version of the PSEQ, and examine its psychometric properties, being this the first study to perform such translation and analysis. Our results show that PSEQ-Sp has excellent test–retest reliability and excellent internal consistency. Also, our hypothesis stating that the PSEQ-Sp and the TSK were associated was confirmed, supporting the validity of the PSEQ-Sp.
The PSEQ is a relatively short and feasible questionnaire that can easily be administered during a regular assessment, and can provide valuable information to understand the patient’s clinical presentation from a biopsychosocial perspective. Authors have discussed its form and how can it be improved. For instance, respondents in the study conducted by Chala et al. (7) suggested to include every possible number in the scale, instead of including numbers only at every limit. However, authors in this study decided that such modification would have a significant influence in the performance of the scale, and opted not to conduct such modification.
The exploratory factor analysis yielded a one-factor solution, coinciding with previous studies (1, 11–19, 22, 23). Contrary to this, several studies did not report results for factorial analysis (20, 21, 24) and one study (7) showed a two-factor solution instead, alluding there may have been underlying factors in the cultural setting they assessed their translated version in Ethiopia. Also, the construct convergent validity of the PSEQ-Sp was assessed by performing a correlation analysis with the TSK. The moderate negative correlation found in our study between the PSEQ-Sp and the TSK is consistent with other studies that conducted the same analysis. Chiarotto et al. (17), Almutairi et al. (12), and Yang et al. (15) found moderate negative correlations of r = −0.48, −0.41, −0.45, respectively. All of these studies conducted their validity analysis in patients that suffered low back pain, unlike our study, but we can consider this positively, as the correlation between these tools seems to be consistent despite the clinical condition. However, our validity analysis could have been further developed by correlating the PSEQ with other tools that similar studies used, such as the Short-Form 36 (SF-36) assessing health-related quality of life (7, 12, 14, 18, 19, 23), or other indices of validity, such as discriminant (13), or factorial (7, 18) validity. Future studies could consider these analyses.
Both the Bland–Altman plot and ICC values showed excellent reliability levels for the PSEQ-Sp. Other studies have also used the ICC to establish correlation values for the PSEQ. The Arabic and Chinese-Hong Kong versions (12, 14) found average ICC correlation values of 0.79 and 0.75, respectively, and the Amharic, Canadian-French, Danish, Farsi, Italian, Japanese, and Marathi versions (1, 7, 16, 20) found high ICC correlation values that ranged from 0.80 to 0.96. However, we have to consider the possible incurring in a recall bias, as the high test–retest reliability might’ve been influenced by the interval between assessments.
The level of internal consistency of the PSEQ-Sp was excellent. Other language translations of the PSEQ have found excellent internal consistency levels too. The Amharic (7), Arabic (12), and Portuguese-Brazilian (22) versions had internal consistencies of α = 0.90, the Canadian-French (1) version of α = 0.91, the original English (11), Catalan (13), and Farsi (18) versions of α = 0.92, the Chinese-Hong Kong (14), and Marathi (20) versions of α = 0.93, the Italian (17), Japanese (19), and Mongolian (21) versions of α = 0.94, and the Chinese-Mainland (15) version of α = 0.95. The Portuguese-European (23) and Danish (16) versions had good levels of internal consistency, both α = 0.88. Only the Yoruba (24) version had inferior, but still acceptable levels of consistency of α = 0.79. Therefore, this tendency appears to be a psychometric property of the PSEQ across different languages and cultural contexts.
Limitations were also present in our study. First, results from this study are limited to patients suffering rotator cuff injuries, so conclusions should be interpreted cautiously. Also, our sample was of convenience, it was not randomly selected from the general population, meaning the generalizability cannot be assumed for all patients suffering rotator cuff injuries. Finally, we translated and cross-culturally adapted the PSEQ in Spain, and even though the version is easily understood by any Spanish speaker, cross-cultural adaptations to other Spanish-speaking countries, as the ones in South America, could report different results. Additional limitations to be considered include response biases, as our assessment was self-administered, and the potential recall bias on the test–retest assessment.
However, our study also presents strong points. This is the first translation of the PSEQ in Spanish, the world’s second most spoken native language, and the official language in 20 countries. Therefore, the development of the PSEQ-Sp could imply an important addition for so many clinicians and researchers. Future research could conduct cross-cultural adaptations of the PSEQ-Sp in different Spanish-speaking countries to explore potential variations in psychometric properties and cultural influences. Cross-cultural adaptations of the PSEQ-Sp in different Spanish-speaking countries to explore potential variations in psychometric properties and cultural influences.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee of University of Valencia (protocol code 2537824 and date of approval March 9, 2023). The patients/participants provided their written informed consent to participate in this study.
Author contributions
BP-D and MB-D contributed to the conception and design of the study. SP-M and IE-P organized the database. AR-R performed the statistical analysis. BP-D wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Dubé, MO, Roos, M, Desmeules, F, and Roy, JS. Reliability, validity, and responsiveness of a Canadian French adaptation of the pain self-efficacy questionnaire (PSEQ). Disabil Rehabil. (2022):1–8. doi: 10.1080/09638288.2022.2102254
2. Kirkley, A, Alvarez, C, and Griffin, S. The development and evaluation of a disease-specific quality-of-life questionnaire for disorders of the rotator cuff: the western ontario rotator cuff index. Clin J Sport Med. (2003) 13:84–92. doi: 10.1097/00042752-200303000-00004
3. Sahoo, S, Ricchetti, ET, Zajichek, A, Cleveland Clinic Shoulder Group, Evans, PJ, Farrow, LD, et al. Associations of preoperative patient mental health and sociodemographic and clinical characteristics with baseline pain, function, and satisfaction in patients undergoing rotator cuff repairs. Am J Sports Med. (2020) 48:432–43. doi: 10.1016/j.jse.2020.08.003
4. Bandura, A . Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. (1977) 84:191–215. doi: 10.1037//0033-295x.84.2.191
5. Martinez-Calderon, J, Zamora-Campos, C, Navarro-Ledesma, S, and Luque-Suarez, A. The role of self-efficacy on the prognosis of chronic musculoskeletal pain: a systematic review. J Pain. (2018) 19:10–34. doi: 10.1016/j.jpain.2017.08.008
6. Martinez-Calderon, J, Flores-Cortes, M, Morales-Asencio, JM, Fernandez-Sanchez, M, and Luque-Suarez, A. Which interventions enhance pain self-efficacy in people with chronic musculoskeletal pain? a systematic review with meta-analysis of randomized controlled trials, including over 12 000 participants. J Orthop Sports Phys Ther. (2020) 50:418–30. doi: 10.2519/jospt.2020.9319
7. Chala, MB, Donnelly, C, Wondie, Y, Ghahari, S, and Miller, J. Cross-cultural translation, adaptation, and validation of the Amharic version pain self-efficacy questionnaire in people with low back pain in Ethiopia. BMC Musculoskelet Disord. (2021) 22:111. doi: 10.1186/s12891-021-03985-4
8. Miles, CL, Pincus, T, Carnes, D, Taylor, SJC, and Underwood, M. Measuring pain self-efficacy. Clin J Pain. (2011) 27:461–70. doi: 10.1097/AJP.0b013e318208c8a2
9. Vergeld, V, and Utesch, T. Pain-related self-efficacy among people with back pain: a systematic review of assessment tools. Clin J Pain. (2020) 36:480–94. doi: 10.1097/AJP.0000000000000818
10. Dubé, MO, Langevin, P, and Roy, JS. Measurement properties of the pain self-efficacy questionnaire in populations with musculoskeletal disorders: a systematic review. Pain Rep. (2021) 6:e972. doi: 10.1097/PR9.0000000000000972
11. Nicholas, MK . The pain self-efficacy questionnaire: taking pain into account. Eur J Pain. (2007) 11:153–63. doi: 10.1016/j.ejpain.2005.12.008
12. Almutairi, BA, Al Odaibi, FA, Alnahdi, AH, Omar, M, Algashami, A, and Alonazi, M. Cross-cultural adaptation, and validation of the Arabic version of the pain self-efficacy questionnaire in Arab people with chronic low back pain. Physiother Theory Pract. (2023) 39:182–92. doi: 10.1080/09593985.2021.2005196
13. Castarlenas, E, Solé, E, Galán, S, Racine, M, Jensen, MP, and Miró, J. Construct validity and internal consistency of the Catalan version of the pain self-efficacy questionnaire in young people with chronic pain. Eval Health Prof. (2020) 43:213–21. doi: 10.1177/0163278718820410
14. Lim, HS, Chen, PP, Wong, TCM, Gin, T, Wong, E, Chan, ISF, et al. Validation of the chinese version of pain self-efficacy questionnaire. Anesth Analg. (2007) 104:918–23. doi: 10.1213/01.ane.0000255731.24092.a5
15. Yang, Y, Yang, M, Bai, J, Zhao, J, Chen, K, Zhou, X, et al. Validation of simplified chinese version of the pain self-efficacy questionnaire (SC-PSEQ) and SC-PSEQ-2 for patients with nonspecific low back pain in Mainland China. Spine. (2019) 44:E1219–26. doi: 10.1097/BRS.0000000000003099
16. Rasmussen, MU, Rydahl-Hansen, S, Amris, K, Danneskiold Samsøe, B, and Mortensen, EL. The adaptation of a Danish version of the pain self-efficacy questionnaire: reliability and construct validity in a population of patients with fibromyalgia in Denmark. Scand J Caring Sci. (2016) 30:202–10. doi: 10.1111/scs.12232
17. Chiarotto, A, Vanti, C, Ostelo, RW, Ferrari, S, Tedesco, G, Rocca, B, et al. The pain self-efficacy questionnaire: cross-cultural adaptation into Italian and assessment of its measurement properties. Pain Pract. (2015) 15:738–47. doi: 10.1111/papr.12242
18. Asghari, A, and Nicholas, MK. An investigation of pain self-efficacy beliefs in Iranian chronic pain patients: a preliminary validation of a translated English-language scale. Pain Med. (2009) 10:619–32. doi: 10.1111/j.1526-4637.2009.00623.x
19. Adachi, T, Nakae, A, Maruo, T, Shi, K, Shibata, M, Maeda, L, et al. Validation of the Japanese version of the pain self-efficacy questionnaire in Japanese patients with chronic pain. Pain Med. (2014) 15:1405–17. doi: 10.1111/pme.12446
20. Rajan, P, Leaver, A, Refshauge, K, Patil, A, Kalkonde, Y, Lincoln, M, et al. Cross-cultural adaptation, reliability, and validity of the Marathi versions of the back beliefs questionnaire and pain self-efficacy questionnaire in people living with chronic low back pain. Disabil Rehabil. (2022) 44:646–52. doi: 10.1080/09638288.2020.1773942
21. Tuck, NL, Khuvtsagaan, B, Rashid, U, Aamir, T, Goucke, R, Regjii, B, et al. The adaptation of pain assessment tools from high-income to low- and middle-income countries: psychometric properties of a set of chronic pain questionnaires in Mongolian and New Zealand Patient Samples. Pain Med. (2021) 22:948–60. doi: 10.1093/pm/pnaa267
22. Sardá, J, Nicholas, MK, Pimenta, CAM, and Asghari, A. Pain-related self-efficacy beliefs in a Brazilian chronic pain patient sample: a psychometric analysis. Stress Health. (2007) 23:185–90. doi: 10.1016/j.ejpain.2008.03.008
23. Ferreira-Valente, MA, Pais-Ribeiro, JL, and Jensen, MP. Psychometric properties of the Portuguese version of the pain self-efficacy questionnaire. Acta Reumatol Port. (2011) 36:260–7.
24. Fatoye, F, Mbada, CE, Oladayo TO, Idowu, OA, Oyewole, OO, Fatoye, C, et al. Validation of the yoruba version of the pain self-efficacy questionnaire in patients with chronic low back pain. Spine. (2021) 46:E528–33. doi: 10.1097/BRS.0000000000003870
25. Gómez-Pérez, L, López-Martínez, AE, and Ruiz-Párraga, GT. Psychometric properties of the Spanish version of the Tampa scale for Kinesiophobia (TSK). J Pain. (2011) 12:425–35. doi: 10.1016/j.jpain.2010.08.004
26. Beaton, DE, Bombardier, C, Guillemin, F, and Ferraz, MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. (2000) 25:3186–91. doi: 10.1097/00007632-200012150-00014
27. Terwee, CB, Bot, SDM, De Boer, MR, Van Der Windt, DAWM, Knol, DL, Dekker, J, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. (2007) 60:34–42. doi: 10.1016/j.jclinepi.2006.03.012
28. Tsang, S, Royse, C, and Terkawi, A. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J Anaesth. (2017) 11:80–S89. doi: 10.4103/sja.SJA_203_17
29. Mokkink, LB, De Vet, HCW, Prinsen, CAC, Patrick, DL, Alonso, J, Bouter, LM, et al. COSMIN risk of Bias checklist for systematic reviews of patient-reported outcome measures. Qual Life Res. (2018) 27:1171–9. doi: 10.1007/s11136-017-1765-4
30. Cattell, RB . The Scree test for the number of factors. Multivar Behav Res. (1966) 1:245–76. doi: 10.1207/s15327906mbr0102_10
31. Kaiser, HF . An index of factorial simplicity. Psychometrika. (1974) 39:31–6. doi: 10.1007/BF02291575
32. Bartlett, MS . A note on the multiplying factors for various χ2 approximations. J R Stat Soc Ser B Methodol. (1954) 16:296–8. doi: 10.1111/j.2517-6161.1954.tb00174.x
33. Keefe, FJ, Rumble, ME, Scipio, CD, Giordano, LA, and Perri, LM. Psychological aspects of persistent pain: current state of the science. J Pain. (2004) 5:195–211. doi: 10.1016/j.jpain.2004.02.576
34. Koo, TK, and Li, MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. (2016) 15:155–63. doi: 10.1016/j.jcm.2016.02.012
35. Bland, JM, and Altman, DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet Lond Engl. (1986) 327:307–10. doi: 10.1016/S0140-6736(86)90837-8
36. Stratford, PW . Getting more from the literature: estimating the standard error of measurement from reliability studies. Physiother Can. (2004) 56:027. doi: 10.2310/6640.2004.15377
Keywords: cross-cultural adaptation, pain self-efficacy questionnaire, reliability, Spain, validity
Citation: Perez-Dominguez B, Perpiña-Martinez S, Escobio-Prieto I, de la Fuente-Costa M, Rodriguez-Rodriguez AM and Blanco-Diaz M (2023) Psychometric properties of the translated Spanish version of the Pain Self-Efficacy Questionnaire. Front. Med. 10:1226037. doi: 10.3389/fmed.2023.1226037
Edited by:
Emma K. Ho, The University of Sydney, AustraliaReviewed by:
Pawel Kiper, San Camillo IRCCS S.r.l. Società Unipersonale, ItalyOlga Velasco, University of the Balearic Islands, Spain
Copyright © 2023 Perez-Dominguez, Perpiña-Martinez, Escobio-Prieto, de la Fuente-Costa, Rodriguez-Rodriguez and Blanco-Diaz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Borja Perez-Dominguez, Zi5ib3JqYS5wZXJlekB1di5lcw==