
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med., 19 July 2023
Sec. Infectious Diseases: Pathogenesis and Therapy
Volume 10 - 2023 | https://doi.org/10.3389/fmed.2023.1221363
This article is part of the Research TopicClostridioides Difficile InfectionView all 8 articles
 Sarah Jolivet1*†
Sarah Jolivet1*† Jeanne Couturier2,3†
Jeanne Couturier2,3† Patrick Grohs4Aurélie Vilfaillot5,6Jean-Ralph Zahar7
Patrick Grohs4Aurélie Vilfaillot5,6Jean-Ralph Zahar7 Pierre Frange8Anne Casetta9Véronique Moulin10Christine Lawrence11Patricia Baune12Cléo Bourgeois5,6Axel Bouffier5,6Claudine Laussucq4Lydia Sienzonit4Simon Picard4Isabelle Podglajen4Najiby Kassis-Chikhani13
Pierre Frange8Anne Casetta9Véronique Moulin10Christine Lawrence11Patricia Baune12Cléo Bourgeois5,6Axel Bouffier5,6Claudine Laussucq4Lydia Sienzonit4Simon Picard4Isabelle Podglajen4Najiby Kassis-Chikhani13 Frédéric Barbut1,2,3
Frédéric Barbut1,2,3Clostridioides difficile infection (CDI) incidence has increased over the last 20 years. Studies suggest that asymptomatic carriers may be an important reservoir of C. difficile in healthcare settings. We conducted a point prevalence study to estimate the toxigenic C. difficile asymptomatic carriage rate and the associated risk factors in patients >3 years old. Between September 16, 2019 and January 15, 2020, all patients hospitalized in 11 healthcare facilities in the Paris urban area were included in the study. They were screened on the day of the survey for toxigenic C. difficile carriage by rectal swab and interviewed. Isolates were characterized by PCR ribotyping and multiplex PCR targeting toxin genes. A logistic regression model was used to determine the risk factors associated with toxigenic C. difficile asymptomatic carriage using uni- and multivariate analysis in the subpopulation of patients >3 years old. During the study period, 2,389 patients were included and screened. The median age was 62 years (interquartile range 35–78 years) and 1,153 were male (48.3%). Nineteen patients had a previous CDI (0.9%). Overall, 185/2389 patients were positive for C. difficile (7.7%), including 93 toxigenic strains (3.9%): 77 (82.8%) were asymptomatic (prevalence 3.2%) whereas 12 (12.9%) were diarrheic. Prevalences of toxigenic C. difficile were 3.5% in patients >3 years old and 7.0% in ≤3 years old subjects, respectively. Toxigenic strains mainly belonged to PCR ribotypes 106 (n = 14, 15.0%), 014 (n = 12, 12.9%), and 020 (n = 10, 10.8%). Among toxigenic strains, 6 (6.4%) produced the binary toxin. In multivariate analysis, two factors were positively associated with toxigenic C. difficile asymptomatic carriage in patients >3 years old: multidrug-resistant organisms co-carriage [adjusted Odd Ratio (aOR) 2.3, CI 95% 1.2–4.7, p = 0.02] and previous CDI (aOR 5.8, CI 95% 1.2–28.6, p = 0.03). Conversely, consumption of raw milk products were associated with reduced risk of toxigenic C. difficile colonization (aOR 0.5, CI 95% 0.2–0.9, p = 0.01). We showed that there was a low prevalence of asymptomatic toxigenic C. difficile carriage in hospitalized patients. Consumption of raw milk prevents toxigenic C. difficile colonization, probably due to the barrier effect of milk-associated bacteria.
Clostridioides difficile is the leading cause of healthcare-associated diarrhea, accounting for almost half of all nosocomial gastrointestinal infections in hospitals in Europe (1). Exposure to C. difficile can lead to asymptomatic carriage or C. difficile infection (CDI) with a wide range of clinical presentations and outcomes (from mild diarrhea to severe colitis and death). CDI is associated with a substantial morbidity and mortality. In France, the extra cost of CDI in public acute-care hospitals was estimated to 163.1 million per year (2). Prevention of CDI stills remains challenging in both acute care and long-term care facilities. The CDI incidence in hospitalized patients has increased over the last 20 years in France (3). The asymptomatic C. difficile colonization rate is frequent although highly variable across studies (range: 6–18%) (4–8). Main risk factors for asymptomatic C. difficile carriage included previous antibiotic treatment, use of gastric acid suppression therapy, prior hospitalization and history of CDI (4, 9, 10). Risk factors described in the literature vary widely, depending especially on the sampling technique, the C. difficile detection method, the population targeted and the epidemiology situation (outbreak versus endemicity). Colonization is a prerequisite to infection, and asymptomatic carriage is associated with a higher risk of CDI (11). Moreover, asymptomatic carriers of toxigenic strains are an important and hidden reservoir of C. difficile in healthcare settings and could play a key role in the transmission of this spore-forming micro-organism (12). A recent study showed that the environment of asymptomatic C. difficile carriers is as contaminated as that of symptomatic CDI patients (13). A quasi-experimental controlled study revealed that identification and isolation of C. difficile carriers was associated with a decreased incidence of CDI (14). However, screening asymptomatic carrier is not currently recommended in infection control guidelines (15). The aim of the study was to evaluate the prevalence of toxigenic C. difficile asymptomatic carriage and its associated risk factors in order to provide insights into this potential reservoir in healthcare facilities.
The study was performed in 11 sites of Assistance Publique-Hôpitaux de Paris (AP-HP) providing intensive care, acute care for adults, maternity, pediatrics, geriatric and long-term care with a total capacity of 6,454 beds: Hôpital Européen Georges Pompidou (EGP01; acute care), Avicenne (AV02; acute care), Jean Verdier (JV03; maternity and acute care), René Muret (RM04; geriatric long stay), Corentin Celton (CC05; geriatric long stay and reeducation), Vaugirard-Gabriel Pallez (VG06; geriatric long stay), Necker-Enfants malades (NCK07; maternity and acute care for adults and children), Raymond Poincaré (RP08; acute care), Saint-Antoine (SA09; acute care), Cochin (CCH10; maternity and acute care) and Paul Brousse (PB11; liver transplant and geriatrics). This study is an ancillary study of the project CODBAHRE (16), a point prevalence study to estimate the multidrug-resistant organisms (MDRO) fecal carriage rate.
This study was approved by agreement with French regulations (AP-HP project CODBAHRE no. 180561; IDRCB no. 2019-A01226-51).
We conducted a serial cross-sectional survey of C. difficile carriage between September 16, 2019 and January 15, 2020. All patients hospitalized more than 24 h on a given day in one of the 11 facilities (except patients from psychiatric units) who agreed to participate in the survey were eligible to inclusion. A non-opposition form was obtained from each patient included in the study (or from parents/guardians for pediatric patients). Clinical wards and eligible patients were informed by information notes according to the protocol.
Six nurses were specifically recruited and trained to implement the protocol. They interviewed the patients and collected the data. The questionnaire (available as Supplementary Table S1) was completed by the nurses and included demographic data, life conditions, previous treatments and food consumption.
For all included patients, a screening sample was taken using an eSwab® system (COPAN, Brescia, Italy) by the nurse or by the patients themselves. The sample was collected by rectal swabbing, by soaking the swab in the stools or by swabbing an ostomy. All samples were sent to a central microbiology laboratory for subsequent analysis.
All samples were plated on the selective chromogenic medium ChromID® C. difficile agar (bioMérieux®, Marcy-l’Etoile, France). Plates were incubated for 48 h at 37°C in an anaerobic atmosphere. Suspicious colonies (based on black coloration and the morphological aspect) were analyzed using matrix assisted laser desorption ionization time-of-flight (MALDI-TOF) mass spectrometry (Brucker Daltonics, Germany). DNA extraction was performed from colonies grown on Brucella agar (bioMérieux®, Marcy-l’Etoile, France) using the InstaGene Matrix™ kit (Bio-Rad®, Marnes-la-Coquette, France). Strains were characterized by a previously described multiplex PCR assay detecting tpi, tcdA, tcdB, tcdC, cdtA, and cdtB genes coding for the triose phosphate isomerase, toxin A, toxin B, TcdC and the two components of the binary toxin, respectively (17).
Isolates were typed by capillary gel electrophoresis-based PCR ribotyping on an ABI 3500 sequencer (Applied Biosystems, Foster City, CA, United States), using primers described by Bidet et al. (18). After DNA amplification, each PCR product was diluted at 1/200. One microliter of this dilution was mixed with 10.5 μL formamide and 0.5 μL GeneScan LIZ600 (Applied Biosystems®, Foster City, United States). The banding patterns were analyzed with the GeneMapper software (Thermo Fisher Scientific, Villebon-sur-Yvette, France). PCR ribotypes (RT) were assigned using the Webribo database.1
ESwab® samples were also plated onto specific chromogenic culture media: chromID® CARBA SMART, chromID® VRE, and chromID® ESBL-PE (bioMérieux, Craponne, France) to search for the presence of MDRO co-carriage.
Prevalence of C. difficile carriage (including toxigenic and non-toxigenic strains) was reported in the overall study population, by hospitals, by specialties, by age and by time from admission. Results were expressed as median [interquartile range (IQR)] for continuous variables and N (%) for categorical variables.
Risk factors for toxigenic C. difficile asymptomatic carriage in patients >3 years old were investigated by uni- and multivariate analysis. Asymptomatic patients with toxigenic C. difficile were compared with asymptomatic non- C. difficile carriers in patient >3 years old. Asymptomatic patients with toxigenic C. difficile was defined as patient without diarrhea (<3 stools per day for 48 h) and with a rectal sample positive for a toxigenic C. difficile isolate. Patients with diarrhea on the day of inclusion were excluded from the analysis. A logistic regression analysis was used to determine the risk factors associated with asymptomatic carriage of toxigenic C. difficile. Variables with a p < 0.20 in univariable analysis were included in the multivariate logistic regression model. A backward stepwise approach was used to identify independent predictors. Adjusted odds ratios (aOR) and 95% confidence intervals (95% CIs) were calculated for all variables. p < 0.05 were considered statistically significant. Statistical analysis was made using Stata® software, v15 (StataCorp, College Station, Texas, United States).
In the 11 participating hospitals on the day of the study, 4,287 patients were eligible, 2,396 patients were included (55.9%) and 2,389 were tested for C. difficile carriage (Figure 1). In total, 1,193 (50.4%) swabs were collected by patients themselves and 1,176 (49.6%) by nurses. The median age was 62 years (IQR 35–78 years, range 0–106 years), 1,153 patients (48.3%) were male and 2,317 (97.1%) were born in France. Comorbidities were frequent (n = 1,599, 68.2%); in particular, 922 (38.5%) patients had a cardiopathy, 384 (16.1%) were diabetic, 309 (12.9%) had a progressive cancer, 206 (8.6%) had a chronic respiratory failure, 199 (8.3%) had a chronic kidney failure, 137 (5.7%) had a progressive hemopathy, 75 (3.1%) were transplants, 59 (2.5%) had a cirrhosis, 22 (0.9%) had HIV and 18 (0.7%) were under dialysis. One thousand seventy-one (45.7%) patients had a history of hospitalization during the last 12 months, mostly in France (n = 1,036, 44.2%). Four hundred fifty-four (19.6%) traveled abroad in the previous 3 months. Overall, 1,074 (48.4%) patients had received antibiotics during the last 6 months. Nineteen (0.9%) patients reported a previous episode of CDI.
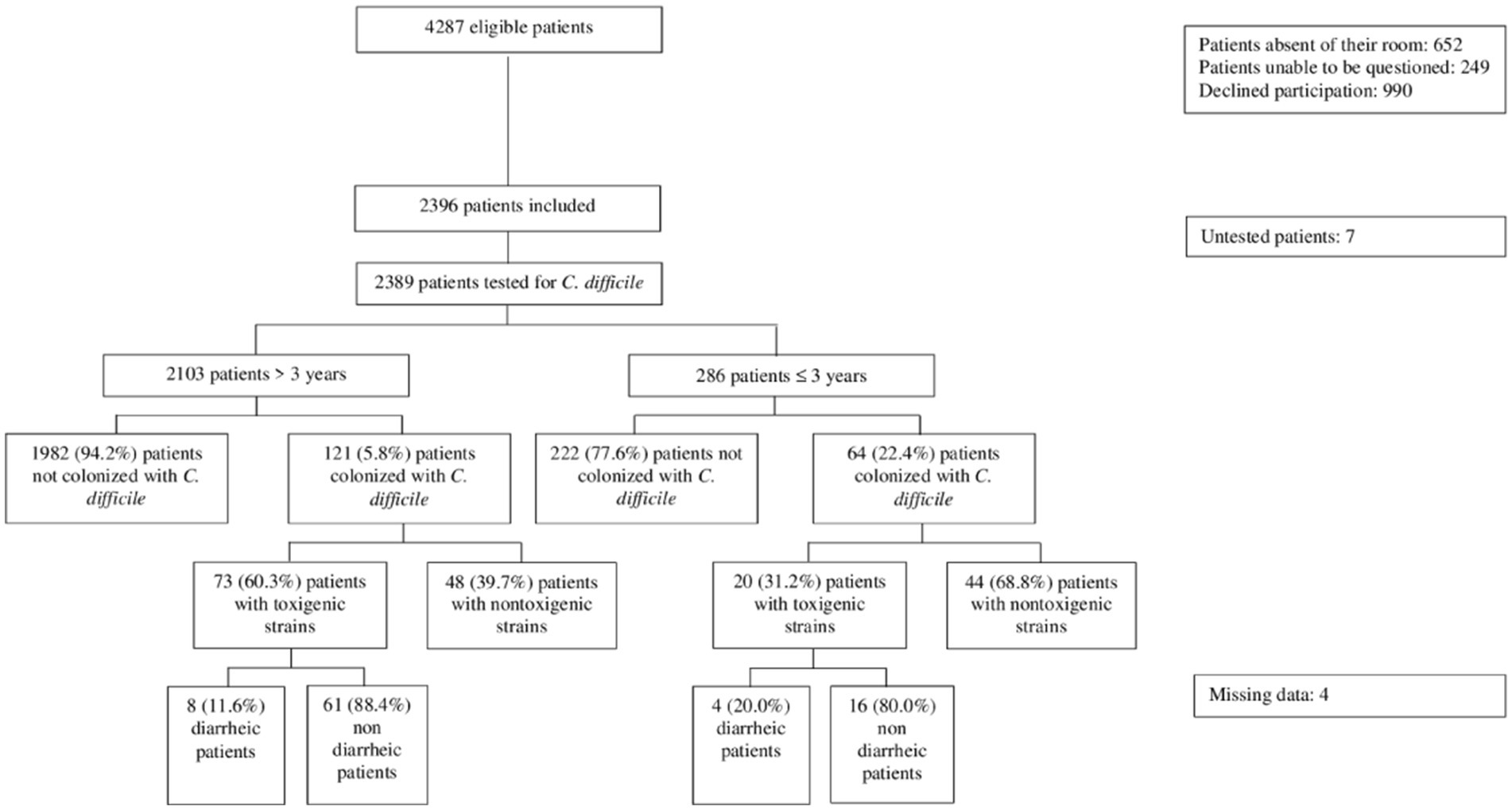
Figure 1. Flow chart of patient recruitment.
Overall, 185 (7.7%) samples were positive for C. difficile including 93 (50.3%) toxigenic strains and 92 (49.7%) nontoxigenic strains. The most prevalent toxigenic RT were 106 (n = 14, 15.0%), 014 (n = 12, 12.9%), and 020 (n = 10, 10.8%). Six of the 14 RT 106 strains were isolated in samples from the NCK07 healthcare facility, from patients <1 year old (n = 4), 3 years old (n = 1) and 14 years old (n = 1), hospitalized in different wards. Among toxigenic strains, 6 (6.4%) were tested positive for the binary toxin genes ctdA and cdtB and belonged to RT 126 (n = 3), 078 (n = 2), and 023 (n = 1). The most frequent nontoxigenic strains were 039 (n = 28, 30.4%), 205 (n = 20, 21.7%), and 010 (n = 17, 18.5%). The distribution of RT is described in the Table 1.
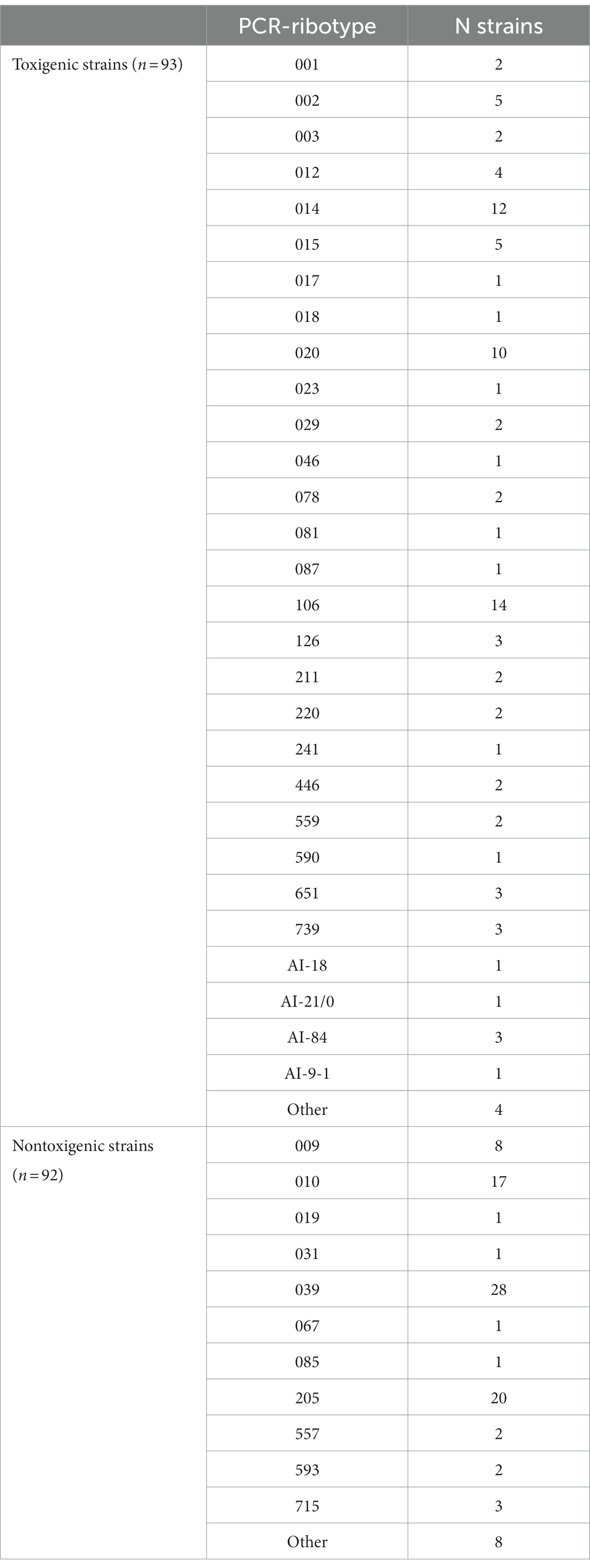
Table 1. Distribution of the PCR-ribotypes of the 185 Clostridioides difficile strains.
Of 93 patients harboring a toxigenic C. difficile strain, 77 (82.8%) were asymptomatic whereas 12 (12.9%) were diarrheic (Figure 1). Among the 12 diarrheic patients, 8 were > 3 years old. The strains isolated from those 8 patients belonged to RT 078, 046, AI-21/0, 106, 015, 211, 014 and 126. Moreover, among toxigenic C. difficile carriers, 18 patients were screened within 3 days of admission.
Prevalences of C. difficile and toxigenic C. difficile were 5.8% (121/2103) and 3.5% (73/2103) in patients >3 years old, respectively; and 22.4% (64/286) and 7.0% (20/286) in youngest subjects, respectively. C. difficile carriage ranged from 2.6% (2/76) to 20.2% (68/336) depending on the hospital, and that of toxigenic strain from 1.0% (3/307) to 7.4% (25/336) (Table 2). The prevalence of C. difficile carriage varied also according to the type of ward, from 0.7% (1/141) in motherhood to 23.4% (40/171) in pediatrics, with rates of 0.7% (1/141) and 9.9% (17/171) respectively for toxigenic C. difficile carriage. The prevalence of toxigenic C. difficile in patient hospitalized ≤3 days and > 3 days were 2.3% (18/769) and 4.6% (73/1578) respectively.

Table 2. Frequencies of Clostridioides difficile and toxigenic C. difficile carriers by hospital and by ward.
Risk factors for toxigenic C. difficile asymptomatic carriage in patients >3 years old were investigated by uni- and multivariate analysis: 61 toxigenic C. difficile asymptomatic carriage patients were compared with 1724 asymptomatic non-carriers of C. difficile (Table 3).
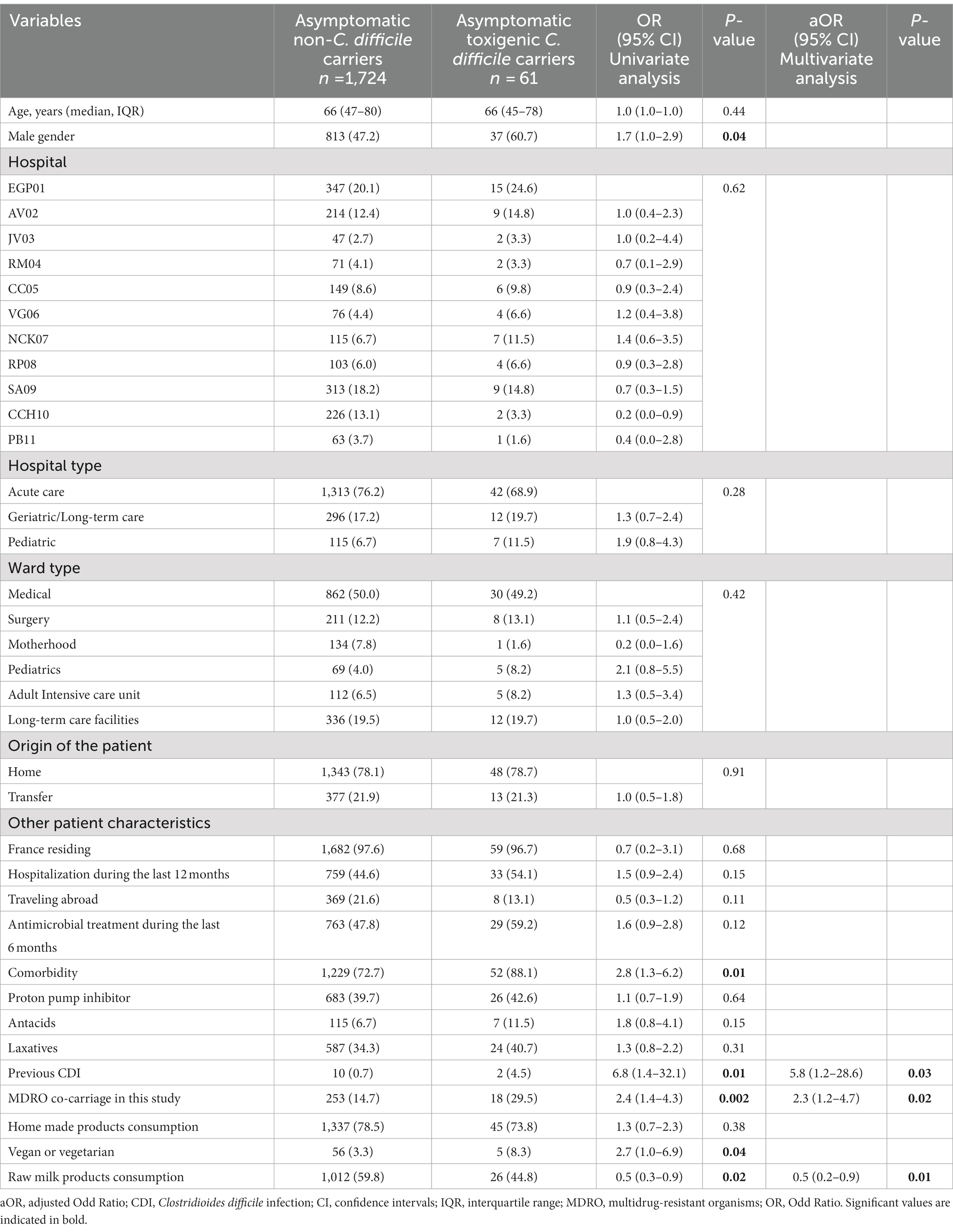
Table 3. Univariate and multi-variate logistic regression analyses of factors associated with toxigenic Clostridioides difficile asymptomatic carriers aged >3 years.
In univariate analysis, six factors were significantly associated with toxigenic C. difficile asymptomatic carriage: male gender, comorbidity, previous CDI, MDRO co-carriage, vegan or vegetarian and consumption of raw milk products. Other factors, e.g., previous antimicrobial treatment, use of proton-pump inhibitor, laxatives or anti acids or hospitalization during the last 12 months were more frequently found in C. difficile carriers than controls but the difference was not significant.
In multivariate analysis, only two factors remained significantly associated with toxigenic C. difficile asymptomatic carriage: MDRO co-carriage (aOR 2.3, CI95% 1.2–4.7, p = 0.02) and previous CDI (aOR 5.8, CI95% 1.2–28.6, p = 0.03). Conversely, consumption of raw milk products were associated with reduced risk of toxigenic C. difficile colonization (aOR 0.5, CI95% 0.2–0.9, p = 0.01).
In this large French multicenter point-prevalence study, a low prevalence of toxigenic C. difficile carriage was observed among hospitalized patients (3.9%). These results provide valuable epidemiological insight into the understanding of CDI, a frequent and severe condition in hospitalized patients. Asymptomatic carriers of C. difficile have been shown to play a role in the transmission of CDI (11, 19) and can contaminate the hospital environment by spores. Moreover, asymptomatic carriers after discharge from hospital could also be a source of community-associated CDI cases (20, 21).
Our results are in the lower range of asymptomatic carriage previously reported in hospitalized patients (6–18%) and also lower than the prevalence of 5.8% found in another recent French multicenter study (4–8). This result may reflect differences in studied populations, or local epidemiology such as hospital outbreaks. It can also be explained by different microbiological techniques used to isolate C. difficile. We used rectal swabbing and direct culture whereas others used stool samples and enriched culture (4).
Children ≤3 years old were frequently found positive for C. difficile (22.4%) including with toxigenic C. difficile (7.0%) but the presence of C. difficile in this population has often been considered as non-pathogenic (22). Our results are in agreement with previous studies where a high colonization rate in children less than 2 years old was observed, ranging from 17 to 70% and mainly due to nontoxigenic strains (22–26). In contrast, prevalence was the lowest in parturient (0.7%), reflecting asymptomatic carriage in the community (27).
We identified two factors positively associated with toxigenic C. difficile carriage in subjects >3 years old. A previous CDI episode was already known as a risk factor (28, 29), and had the highest impact in our study (aOR 5.7, CI95% 1.2–28.1, p = 0.03). The other associated factor was MDRO co-carriage. This risk factor may be a marker of a prolonged hospitalization and antibiotic exposure. It may also reflect the high level of healthcare worker contacts linked to inter-individual transmission of pathogens.
In contrast, consumption of raw milk products reduced risk of toxigenic C. difficile carriage, probably due to the barrier effect of milk-associated bacteria. A meta-analysis suggested that probiotic prophylaxis may be a useful and safe CDI prevention strategy (30).
Another striking finding of this study was the lack of significant association between C. difficile colonization and antimicrobials or proton-pump inhibitor therapy. Use of antibiotics and proton-pump inhibitors, by disrupting the intestinal microbiota, were previously associated with C. difficile colonization and infection (31, 32). However, in a recent meta-analysis including 1,588 asymptomatic patients colonized with C. difficile, antibiotics in the previous 3 months was not associated with significant effects on risk of colonization (9).
The results of the strain typing analysis indicated a large diversity of strains and the distribution of RT was consistent with previous investigations. For several years, RTs 014 and 020 have been predominant in epidemiological studies in France or in Europe. They represented 18.7 and 21.9% of C. difficile strains in France in 2009 (33) and in 2024–2015 (34), respectively. They were also the most common RTs in the ECDC-coordinated surveillance of healthcare-associated CDI in 2016–2017 (35) and RT 014 was the third most frequent in a recent European study including 119 sites in 12 countries (36). In a recent French multicenter study, RT 014/020 was the most common toxigenic strain in C. difficile carriers (4). RT 106 is an emerging RT: between 2012 and 2017, its prevalence in France increased from <1 to 4.65% (3). The predominance of RT 106 in our study could be linked to a potential outbreak in one of the included healthcare facilities. However, epidemiological data to support this hypothesis are lacking. The absence of any RT 027 in our study should be noted. This hypervirulent strain was responsible for several outbreaks in France in the 2000s (37). Since then, control measures were implemented to prevent its spreading in Europe. In France, the frequency of RT 027 decreased from 21.7 to 9.56% between 2012 and 2017 (3). Our results support the successful control of the RT 027 spread in France.
This study has some limitations. First, the cross-sectional survey design did not allow us to investigate the dynamics of C. difficile colonization (acquisition, persistence and clearance of carriage). Second, generalizing our results is difficult because only 55.7% of eligible patients were included and screened. Third, the screening method for carriage was not the most sensitive since we used rectal swabbing rather than stool specimens and there was no broth enrichment step during culture.
A strength of our study was the inclusion of a large number of hospitalized patients from 11 facilities, without selecting patients at hospital admission or from high-risk units, thus reducing the impact of center effect. We also explored many risk factors including food consumption in the context of one health.
In conclusion, the prevalence of C. difficile toxigenic carriage was low in patients >3 years old (3.5%), but higher in ≤3 years old (7.0%) and in patients hospitalized >3 days (4.6%). These patients and may therefore represent a potential reservoir for CDIs.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the AP-HP project CODBAHRE no. 180561; IDRCB no. 2019-A01226-51. Written informed consent to participate in this study was provided by the participants or their legal guardian/next of kin.
PG, NK-C, and IP: initial idea and writing of the grant proposal. FB, PF, PG, NK-C, ChL, VM, IP, and J-RZ: study design. FB, PB, AC, PF, ChL, VM, and J-RZ: local hospital management. CB: regulatory management. AB: data management. SJ, PG, and AV: data analysis and statistics. ClL, SP, and LS: technical investigations. JC and FB: microbiological result validation. SJ and JC: writing—original draft. SJ, JC, FB, PF, PG, NK-C, ChL, IP, AV, and J-RZ: writing—review and editing. All authors have read and agreed to the published version of the manuscript.
This study was funded by a grant from Programme Hospitalier de Recherche Clinique—PHRC 2018 (Ministère de la Santé No. AOR 18062). This sponsor was Assistance Publique—Hôpitaux de Paris (Direction de la Recherche Clinique et de l’Innovation).
The authors gratefully acknowledge Rabab Syed-Zaidi for her technical assistance.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2023.1221363/full#supplementary-material
1. Suetens, C, Latour, K, Kärki, T, Ricchizzi, E, Kinross, P, Moro, ML, et al. Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: results from two European point prevalence surveys, 2016 to 2017. Euro Surveill. (2018) 23:1800516. doi: 10.2807/1560-7917.ES.2018.23.46.1800516
2. Le Monnier, A, Duburcq, A, Zahar, J-R, Corvec, S, Guillard, T, Cattoir, V, et al. Hospital cost of Clostridium difficile infection including the contribution of recurrences in French acute-care hospitals. J Hosp Infect. (2015) 91:117–22. doi: 10.1016/j.jhin.2015.06.017
3. Colomb-Cotinat, M, Assouvie, L, Durand, J, Daniau, C, Leon, L, Maugat, S, et al. Epidemiology of Clostridioides difficile infections, France, 2010 to 2017. Euro Surveill. (2019) 24:1800638. doi: 10.2807/1560-7917.ES.2019.24.35.1800638
4. Le Monnier, A, Candela, T, Mizrahi, A, Bille, E, Bourgeois-Nicolaos, N, Cattoir, V, et al. One-day prevalence of asymptomatic carriage of toxigenic and non-toxigenic Clostridioides difficile in 10 French hospitals. J Hosp Infect. (2022) 129:65–74. doi: 10.1016/j.jhin.2022.05.011
5. Ziakas, PD, Zacharioudakis, IM, Zervou, FN, Grigoras, C, Pliakos, EE, and Mylonakis, E. Colonization with toxinogenic C. difficile upon hospital admission, and risk of infection: a systematic review and meta-analysis. Am J Gastroenterol. (2015) 110:381–90; quiz 391. doi: 10.1038/ajg.2015.22
6. Alasmari, F, Seiler, SM, Hink, T, Burnham, C-AD, and Dubberke, ER. Prevalence and risk factors for asymptomatic Clostridium difficile carriage. Clin Infect Dis. (2014) 59:216–22. doi: 10.1093/CID/CIU258
7. Guerrero, DM, Becker, JC, Eckstein, EC, Kundrapu, S, Deshpande, A, Sethi, AK, et al. Asymptomatic carriage of toxigenic Clostridium difficile by hospitalized patients. J Hosp Infect. (2013) 85:155–8. doi: 10.1016/J.JHIN.2013.07.002
8. Koo, HL, Van, JN, Zhao, M, Ye, X, Revell, PA, Jiang, Z-D, et al. Real-time polymerase chain reaction detection of asymptomatic Clostridium difficile colonization and rising C. difficile-associated disease rates. Infect Control Hosp Epidemiol. (2014) 35:667–73. doi: 10.1086/676433
9. Anjewierden, S, Han, Z, Brown, AM, Donskey, CJ, and Deshpande, A. Risk factors for Clostridioides difficile colonization among hospitalized adults: a meta-analysis and systematic review. Infect Control Hosp Epidemiol. (2021) 42:565–72. doi: 10.1017/ice.2020.1236
10. Ziakas, PD, Zacharioudakis, IM, Zervou, FN, Grigoras, C, Pliakos, EE, and Mylonakis, E. Asymptomatic carriers of toxigenic C. difficile in long-term care facilities: a meta-analysis of prevalence and risk factors. PLoS One. (2015) 10:e0117195. doi: 10.1371/journal.pone.0117195
11. Worley, J, Delaney, ML, Cummins, CK, DuBois, A, Klompas, M, and Bry, L. Genomic determination of relative risks for Clostridioides difficile infection from asymptomatic carriage in intensive care unit patients. Clin Infect Dis. (2021) 73:e1727–36. doi: 10.1093/cid/ciaa894
12. Mawer, DPC, Eyre, DW, Griffiths, D, Fawley, WN, Martin, JSH, Quan, TP, et al. Contribution to Clostridium Difficile transmission of symptomatic patients with toxigenic strains who are fecal toxin negative. Clin Infect Dis. (2017) 64:1163–70. doi: 10.1093/cid/cix079
13. Gilboa, M, Houri-Levi, E, Cohen, C, Tal, I, Rubin, C, Feld-Simon, O, et al. Environmental shedding of toxigenic Clostridioides difficile by asymptomatic carriers: a prospective observational study. Clin Microbiol Infect. (2020) 26:1052–7. doi: 10.1016/j.cmi.2019.12.011
14. Longtin, Y, Paquet-Bolduc, B, Gilca, R, Garenc, C, Fortin, E, Longtin, J, et al. Effect of detecting and isolating Clostridium difficile carriers at hospital admission on the incidence of C. difficile infections: a quasi-experimental controlled study. JAMA Intern Med. (2016) 176:796–804. doi: 10.1001/jamainternmed.2016.0177
15. Tschudin-Sutter, S, Kuijper, EJ, Durovic, A, Vehreschild, MJGT, Barbut, F, Eckert, C, et al. Guidance document for prevention of Clostridium difficile infection in acute healthcare settings. Clin Microbiol Infect. (2018) 24:1051–4. doi: 10.1016/j.cmi.2018.02.020
16. Grohs, P, Vilfaillot, A, Zahar, JR, Barbut, F, Frange, P, Casetta, A, et al. Faecal carriage of multidrug-resistant bacteria and associated risk factors: results from a point prevalence study. J Antimicrob Chemother. (2022) 77:2667–78. doi: 10.1093/jac/dkac289
17. Barbut, F, Day, N, Bouée, S, Youssouf, A, Grandvoinnet, L, Lalande, V, et al. Toxigenic Clostridium difficile carriage in general practice: results of a laboratory-based cohort study. Clin Microbiol Infect. (2019) 25:588–94. doi: 10.1016/j.cmi.2018.12.024
18. Bidet, P, Barbut, F, Lalande, V, Burghoffer, B, and Petit, JC. Development of a new PCR-ribotyping method for Clostridium difficile based on ribosomal RNA gene sequencing. FEMS Microbiol Lett. (1999) 175:261–6. doi: 10.1111/j.1574-6968.1999.tb13629.x
19. Halstead, FD, Ravi, A, Thomson, N, Nuur, M, Hughes, K, Brailey, M, et al. Whole genome sequencing of toxigenic Clostridium difficile in asymptomatic carriers: insights into possible role in transmission. J Hosp Infect. (2019) 102:125–34. doi: 10.1016/j.jhin.2018.10.012
20. Miller, AC, Arakkal, AT, Sewell, DK, Segre, AM, Pemmaraju, SV, Polgreen, PM, et al. Risk for asymptomatic household transmission of Clostridioides difficile infection associated with recently hospitalized family members. Emerg Infect Dis. (2022) 28:932–9. doi: 10.3201/EID2805.212023
21. Rousseau, C, Poilane, I, De Pontual, L, Maherault, A-C, Le Monnier, A, and Collignon, A. Clostridium difficile carriage in healthy infants in the community: a potential reservoir for pathogenic strains. Clin Infect Dis. (2012) 55:1209–15. doi: 10.1093/cid/cis637
22. Enoch, DA, Butler, MJ, Pai, S, Aliyu, SH, and Karas, JA. Clostridium difficile in children: colonisation and disease. J Infect. (2011) 63:105–13. doi: 10.1016/j.jinf.2011.05.016
23. Schutze, GE, and Willoughby, RE. Committee on infectious diseases, American Academy of Pediatrics. Clostridium difficile infection in infants and children. Pediatrics. (2013) 131:196–200. doi: 10.1542/peds.2012-2992
24. Jangi, S, and Lamont, JT. Asymptomatic colonization by Clostridium difficile in infants: implications for disease in later life. J Pediatr Gastroenterol Nutr. (2010) 51:2–7. doi: 10.1097/MPG.0b013e3181d29767
25. Rousseau, C, Lemée, L, Le Monnier, A, Poilane, I, Pons, J-L, and Collignon, A. Prevalence and diversity of Clostridium difficile strains in infants. J Med Microbiol. (2011) 60:1112–8. doi: 10.1099/jmm.0.029736-0
26. Stoesser, N, Eyre, DW, Quan, TP, Godwin, H, Pill, G, Mbuvi, E, et al. Epidemiology of Clostridium difficile in infants in Oxfordshire, UK: risk factors for colonization and carriage, and genetic overlap with regional C. difficile infection strains. PLoS One. (2017) 12:e0182307. doi: 10.1371/journal.pone.0182307
27. Manzoor, SE, McNulty, CAM, Nakiboneka-Ssenabulya, D, Lecky, DM, Hardy, KJ, and Hawkey, PM. Investigation of community carriage rates of Clostridium difficile and Hungatella hathewayi in healthy volunteers from four regions of England. J Hosp Infect. (2017) 97:153–5. doi: 10.1016/j.jhin.2017.05.014
28. Mallia, G, Van, TJ, Rousseau, J, Jacob, L, Boerlin, P, Greer, A, et al. Examining the epidemiology and microbiology of Clostridium difficile carriage in elderly patients and residents of a healthcare facility in southern Ontario, Canada. J Hosp Infect. (2018) 99:461–8. doi: 10.1016/J.JHIN.2018.01.020
29. Nissle, K, Kopf, D, and Rösler, A. Asymptomatic and yet C. difficile-toxin positive? Prevalence and risk factors of carriers of toxigenic Clostridium difficile among geriatric in-patients. BMC Geriatr. (2016) 16:185. doi: 10.1186/s12877-016-0358-3
30. Johnston, BC, Lytvyn, L, Lo, CK-F, Allen, SJ, Wang, D, Szajewska, H, et al. Microbial preparations (probiotics) for the prevention of Clostridium difficile infection in adults and children: an individual patient data meta-analysis of 6,851 participants. Infect Control Hosp Epidemiol. (2018) 39:771–81. doi: 10.1017/ice.2018.84
31. Loo, VG, Bourgault, A-M, Poirier, L, Lamothe, F, Michaud, S, Turgeon, N, et al. Host and pathogen factors for Clostridium difficile infection and colonization. N Engl J Med. (2011) 365:1693–703. doi: 10.1056/NEJMoa1012413
32. Vincent, C, Stephens, DA, Loo, VG, Edens, TJ, Behr, MA, Dewar, K, et al. Reductions in intestinal Clostridiales precede the development of nosocomial Clostridium difficile infection. Microbiome. (2013) 1:18. doi: 10.1186/2049-2618-1-18
33. Eckert, C, Coignard, B, Hebert, M, Tarnaud, C, Tessier, C, Lemire, A, et al. Clinical and microbiological features of Clostridium difficile infections in France: the ICD-RAISIN 2009 national survey. Med Mal Infect. (2013) 43:67–74. doi: 10.1016/j.medmal.2013.01.004
34. Davies, KA, Ashwin, H, Longshaw, CM, Burns, DA, Davis, GL, Wilcox, MH, et al. Diversity of Clostridium difficile PCR ribotypes in Europe: results from the European, multicentre, prospective, biannual, point-prevalence study of Clostridium difficile infection in hospitalised patients with diarrhoea (EUCLID), 2012 and 2013. Euro Surveill. (2016) 21:pii=30294. doi: 10.2807/1560-7917.ES.2016.21.29.30294
35. European Centre for Disease Prevention and Control. Costridioides (Clostridium) difficile infections. Annual epidemiological report for 2016–2017. Stockholm (2022). Available at: https://www.ecdc.europa.eu/en/publications-data/clostridiodes-difficile-infections-annual-epidemiological-report-2016-2017 (Accessed March 14, 2023).
36. Viprey, VF, Granata, G, Vendrik, KEW, Davis, GL, Petrosillo, N, Kuijper, EJ, et al. European survey on the current surveillance practices, management guidelines, treatment pathways and heterogeneity of testing of Clostridioides difficile, 2018-2019: results from the combatting bacterial resistance in Europe CDI (COMBACTE-CDI). J Hosp Infect. (2023) 131:213–20. doi: 10.1016/j.jhin.2022.11.011
37. Kuijper, EJ, Coignard, B, and Tüll, P, ESCMID Study Group for Clostridium difficile, EU Member States, European Centre for Disease Prevention and Control. Emergence of Clostridium difficile-associated disease in North America and Europe. Clin Microbiol Infect. (2006) 12:2–18. doi: 10.1111/j.1469-0691.2006.01580.x
Keywords: Clostridioides difficile, colonization, asymptomatic, prevalence, risk factors
Citation: Jolivet S, Couturier J, Grohs P, Vilfaillot A, Zahar J-R, Frange P, Casetta A, Moulin V, Lawrence C, Baune P, Bourgeois C, Bouffier A, Laussucq C, Sienzonit L, Picard S, Podglajen I, Kassis-Chikhani N and Barbut F (2023) Prevalence and risk factors of toxigenic Clostridioides difficile asymptomatic carriage in 11 French hospitals. Front. Med. 10:1221363. doi: 10.3389/fmed.2023.1221363
Edited by:
Sam Donta, Falmouth Hospital, United StatesReviewed by:
Wen-Qiang He, The University of Sydney, AustraliaCopyright © 2023 Jolivet, Couturier, Grohs, Vilfaillot, Zahar, Frange, Casetta, Moulin, Lawrence, Baune, Bourgeois, Bouffier, Laussucq, Sienzonit, Picard, Podglajen, Kassis-Chikhani and Barbut. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sarah Jolivet, c2FyYWguam9saXZldEBhcGhwLmZy
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.