
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 29 June 2023
Sec. Infectious Diseases: Pathogenesis and Therapy
Volume 10 - 2023 | https://doi.org/10.3389/fmed.2023.1211265
 Taniya Kaewarpai1
Taniya Kaewarpai1 Shelton W. Wright2
Shelton W. Wright2 Thatcha Yimthin1
Thatcha Yimthin1 Rungnapa Phunpang3Adul Dulsuk3Lara Lovelace-Macon4Guilhem F. Rerolle4
Rungnapa Phunpang3Adul Dulsuk3Lara Lovelace-Macon4Guilhem F. Rerolle4 Denisse B. Dow4
Denisse B. Dow4 Viriya Hantrakun3Nicholas P. J. Day3,5
Viriya Hantrakun3Nicholas P. J. Day3,5 Ganjana Lertmemongkolchai6,7
Ganjana Lertmemongkolchai6,7 Direk Limmathurotsakul3,8
Direk Limmathurotsakul3,8 T. Eoin West4†
T. Eoin West4† Narisara Chantratita1,3*†
Narisara Chantratita1,3*†Introduction: Melioidosis is an often-fatal tropical infectious disease caused by the Gram-negative bacillus Burkholderia pseudomallei, but few studies have identified promising biomarker candidates to predict outcome.
Methods: In 78 prospectively enrolled patients hospitalized with melioidosis, six candidate protein biomarkers, identified from the literature, were measured in plasma at enrollment. A multi-biomarker model was developed using least absolute shrinkage and selection operator (LASSO) regression, and mortality discrimination was compared to a clinical variable model by receiver operating characteristic curve analysis. Mortality prediction was confirmed in an external validation set of 191 prospectively enrolled patients hospitalized with melioidosis.
Results: LASSO regression selected IL-1R2 and soluble triggering receptor on myeloid cells 1 (sTREM-1) for inclusion in the candidate biomarker model. The areas under the receiver operating characteristic curve (AUC) for mortality discrimination for the IL-1R2 + sTREM-1 model (AUC 0.81, 95% CI 0.72–0.91) as well as for an IL-1R2-only model (AUC 0.78, 95% CI 0.68–0.88) were higher than for a model based on a modified Sequential Organ Failure Assessment (SOFA) score (AUC 0.69, 95% CI 0.56–0.81, p < 0.01, p = 0.03, respectively). In the external validation set, the IL-1R2 + sTREM-1 model (AUC 0.86, 95% CI 0.81–0.92) had superior 28-day mortality discrimination compared to a modified SOFA model (AUC 0.80, 95% CI 0.74–0.86, p < 0.01) and was similar to a model containing IL-1R2 alone (AUC 0.82, 95% CI 0.76–0.88, p = 0.33).
Conclusion: Biomarker models containing IL-1R2 had improved 28-day mortality prediction compared to clinical variable models in melioidosis and may be targets for future, rapid test development.
Melioidosis is a severe infectious disease caused by the environmental saprophyte Burkholderia pseudomallei. Melioidosis is endemic to parts of Southeast Asia, South Asia, Northern Australia with sporadic cases reported in the Americas (1). The clinical manifestations of melioidosis are often variable but commonly include pneumonia, bacteremia, abscesses, and sepsis. The clinical course of melioidosis is also unpredictable, though patients frequently develop multi-organ dysfunction leading to death (2). Despite appropriate antibiotic treatment, the mortality rate from melioidosis can exceed 40% in Southeast Asia (3).
Identifying patients at highest risk of poor outcomes can help in guiding clinical management and resource allocation. Clinical severity illness scores–such as the Sequential Organ Failure Assessment (SOFA) and the Acute Physiology and Chronic Health Evaluation (APACHE) III score–reasonably predict mortality in patients with sepsis in Southeast Asia; however, these approaches require extensive clinical and laboratory data, limiting their utility in low- and middle-income countries (LMIC) where many melioidosis cases may occur (4–6). Many critically ill patients in LMIC are treated outside of intensive care settings, further limiting the utility of these scoring systems (7). Biomarkers, when integrated into clinical laboratory or point-of-care tests, are potential tools for rapid patient management and triage decisions, critical in LMIC where resources or information about baseline co-morbidities may be limited. We recently reported that the inclusion of IL-6 and IL-8 plasma concentrations augments a model comprised of clinical variables in predicting mortality in melioidosis (8). Elevated concentrations of other inflammatory biomarkers, including calprotectin (a heterodimer containing S100A9), C-reactive protein (CRP), procalcitonin (PCT) and soluble triggering receptor on myeloid cells 1 (sTREM-1) have been associated with worse outcome or lack of response to therapy in melioidosis (9–11). However, in patients suspected of melioidosis there is still a critical need for biomarkers which can reliably predict severe outcomes but do not require additional clinical variables and that can potentially be used to develop future point-of-care tests for use in resource-limited settings.
In the last several years, commercially-available tests have been developed for the rapid, bedside diagnosis of melioidosis (12). Additionally, we recently reported that melioidosis non-survivors have increased expression of gene associated with interleukin 1 receptor, type 2 (IL-1R2) in peripheral blood leukocytes compared to melioidosis survivors (13). Therefore, we sought to extend this bedside diagnostic approach to include prediction in patients already diagnosed with, or suspected of, melioidosis. We hypothesized that plasma concentrations of IL-1R2 protein could predict outcome similar to a model of clinical variables in patients with melioidosis. Additionally, we hypothesized that a multivariable model combining IL-1R2 and other non-correlated inflammatory protein biomarkers could surpass clinical prediction models in patients with melioidosis. We therefore performed an extensive literature review and identified five additional inflammatory biomarkers representing alternative inflammatory pathways which might provide complimentary outcome prediction to, or even surpass, IL-1R2. In this study, we then developed and tested these biomarker models to predict melioidosis-related mortality. We subsequently validated the strongest prediction models in an external cohort of patients with melioidosis.
Subjects aged 15 years or older admitted to Udon Thani Hospital, Udon Thani, Thailand from 2015 to 2018 were prospectively enrolled within 24 h of B. pseudomallei culture positivity. This cohort has previously been described in part (8, 13). Plasma samples were drawn at enrollment. Clinical information was abstracted from the medical records or determined by the study team and reported in a case report form. Mortality at 28 days from the time of enrollment was obtained from medical records or patient interviews by telephone. Ninety patients with available plasma were selected for plasma biomarker measurement, and 78 subjects with complete biomarker data and an enrollment time of less than 7 days after admission were included in the final analysis.
Subjects aged 18 years or older who were admitted from 2013 to 2017 to Sunpasittiprasong Hospital, Ubon Ratchathani, Thailand with suspected infection were prospectively enrolled. Enrollment occurred within 24 h of admission to the hospital. This cohort as well as subsets have been previously reported (7, 14). Plasma samples were obtained at enrollment, and clinical data and 28-day mortality were obtained from medical records and patient interviews. One hundred and ninety-one enrolled patients had a specimen that was culture-positive for B. pseudomallei and so were included in the external validation cohort.
In the derivation cohort, six biomarkers were measured by ELISA: IL-1R2, CRP, PCT, sTREM-1, calprotectin (Abcam) as well as S100A9 (Biolegend). In the external validation cohort, plasma concentrations of IL-1R2 (Abcam) and sTREM-1 (R&D Systems) were measured by ELISA. Samples were tested and analyzed per the manufacturers’ instructions.
The SOFA score was originally designed as a sequential scoring system using clinical and laboratory data as markers of organ dysfunction and/or failure, including respiratory, coagulation, hepatic, cardiovascular and renal components (4). In the derivation cohort, an organ failure score was generated using clinical data from within the first 24 h of admission by modifying a SOFA score. These modifications were necessary because clinical data obtained at enrollment lacked a mental status assessment, arterial blood gas measurements, or vasoactive drug doses necessary to calculate a complete SOFA score. The organ failure score was calculated using the respiratory, cardiovascular, liver, renal, and coagulation measurements from a SOFA score. For the respiratory component of the score, 2 points were given to patients requiring mechanical ventilation when no arterial blood gas was available. For the cardiovascular component of the score, 2 points were given to patients requiring dobutamine or dopamine and 3 points were given to patients requiring norepinephrine or epinephrine.
In the external validation cohort, a modified SOFA score including the Glasgow Coma Scale (GCS) was calculated by adding the highest component score from the time of presentation to the time of study enrollment, which was within 24 h of admission. Because arterial blood gases are not frequently used at the study hospital and dosages of vasoactive medications were not recorded, the cardiovascular and respiratory components of the SOFA score were modified as described above and as previously reported (14).
Novel candidate models of mortality prediction were developed according to Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD) recommendations (15). To develop a potentially multibiomarker-based prediction model, as recommended by TRIPOD guidelines, to reduce bias and to develop the simplest multivariable prediction model, we employed a least absolute shrinkage and selection operator (LASSO) approach to select the biomarkers to include in a final multivariable model (16). LASSO minimizes bias in multivariable model selection by employing shrinkage penalties on each included variable coefficient and then sequentially eliminating variables, including those with high correlation to other variables. Therefore, all measured biomarkers, regardless of their association with mortality, were included in the LASSO selection. Lambda was selected by Bayesian Information Criterion, and the selected biomarkers were confirmed when using the largest lambda within one standard error of the minimal mean squared prediction error based on 10-fold internal cross-validation analysis (17). Biomarkers chosen by LASSO were then included in a candidate multivariable prediction model. Twenty-eight-day mortality prediction of LASSO-selected biomarkers was evaluated using logistic regression models. Models were assessed for calibration by Hosmer-Lemeshow goodness-of-fit chi-square analysis and bias by internal validation of 1,000 replication sets by bootstrapping (18, 19). Mortality discrimination was determined by generating receiver operating characteristic curves and calculating the area under the curve. To assess the improvement of model performance after the addition of individual biomarkers, the likelihood ratio test and integrated improvement analysis (IDI) were used (20, 21). To assess clinical utility, the net benefit of selected models across a range of risk thresholds was compared using decision curve analysis (22). For the final model, an optimal cut-off value representing the optimal discrimination was determined using a Youden’s index (23). Subsequently, the sensitivity, specificity, negative and positive predictive likelihood ratios with corresponding 95% confidence intervals were calculated.
Variables were reported as median and interquartile range (IQR) for non-normally distributed data. Differences in biomarker concentrations were evaluated by the Mann–Whitney U test. Biomarkers were log10-transformed prior to regression analysis and the association of selected biomarkers with 28-day mortality was determined by logistic regression.
Correlations between biomarkers were assessed using a Spearman’s rank-order correlation. Mortality prediction models of clinical variables were generated using the cohort-specific organ failure score or modified SOFA score. Analyzes were performed using Stata SE version 14.2 (StataCorp, College Station, TX, United States).
Plasma samples were obtained at study enrollment from patients with culture-proven melioidosis in the derivation cohort. The study flow diagram is shown in Supplementary Figure S1, and the characteristics of this cohort are shown in Table 1. The median age was 58 years (IQR, 47–67 years) and 77% were male. The median Charlson Comorbidity Index was 3 (IQR 1–4) and 72% of patients had diabetes. The median time to enrollment in this cohort was 4 days and 37% of the patients died within 28 days.
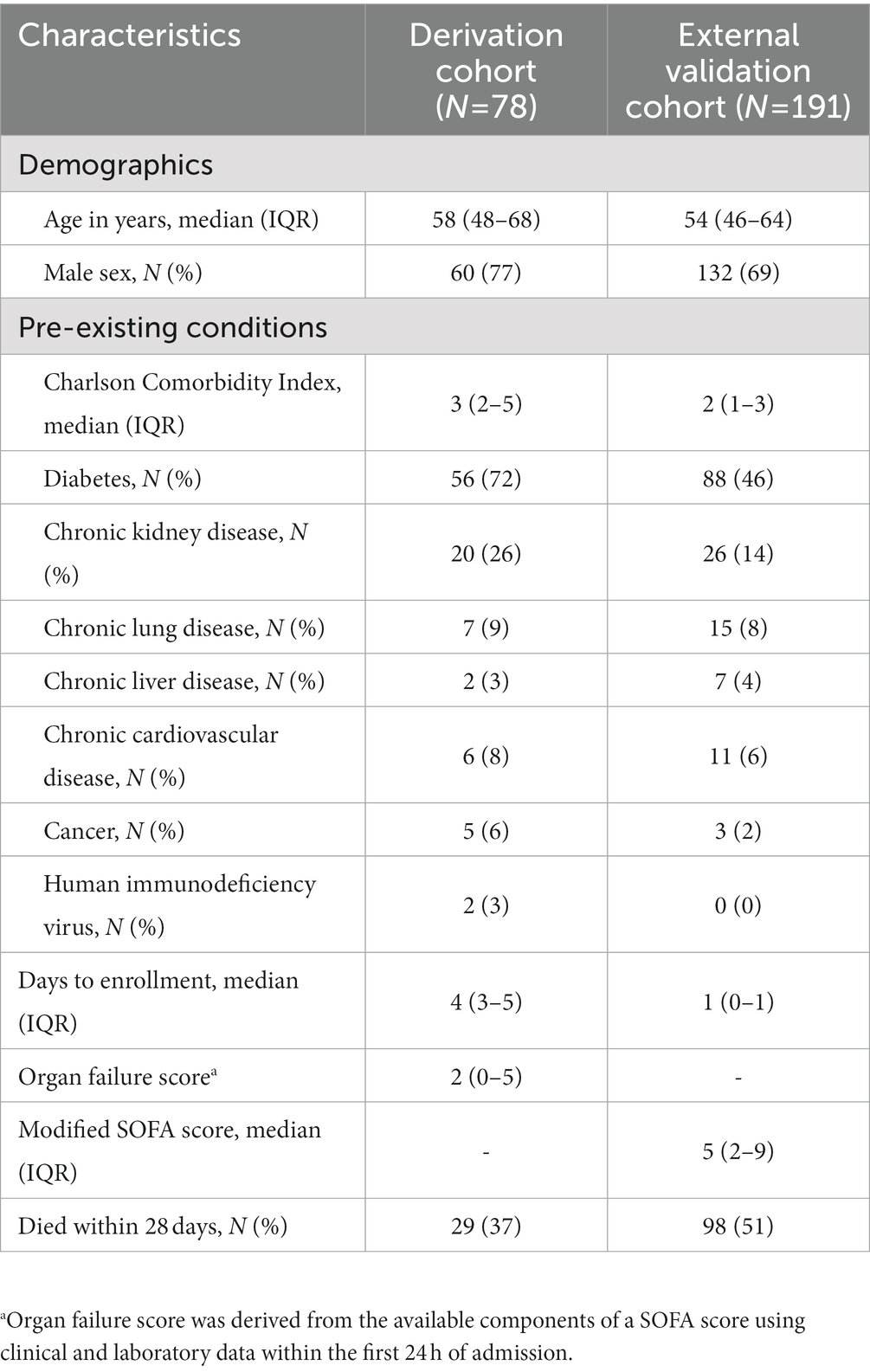
Table 1. Clinical characteristics of melioidosis patients.
Plasma concentrations of IL-1R2, CRP, PCT, sTREM-1, S100A9 and calprotectin were measured at the time of study enrollment and were compared between survivors and non-survivors at 28-days. Concentrations of IL-1R2 and PCT were significantly higher in non-survivors compared to survivors (both p < 0.01; Table 2). We tested the association of each of the six log10-transformed biomarkers with 28-day mortality. IL-1R2 was the only measured biomarker significantly associated with 28-day mortality when adjusting for baseline risk factors including age, sex and Charlson Comorbidity Index plus organ failure score (OR 210.8, 95% CI 13.4–3,381, p < 0.001; Table 3).
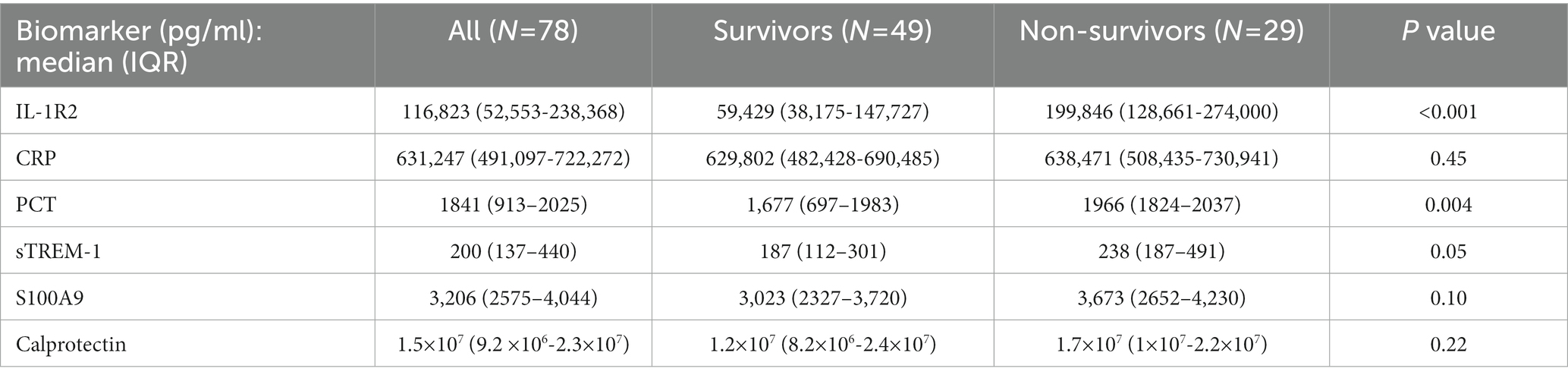
Table 2. Biomarkers by 28-day survival status of melioidosis patients.
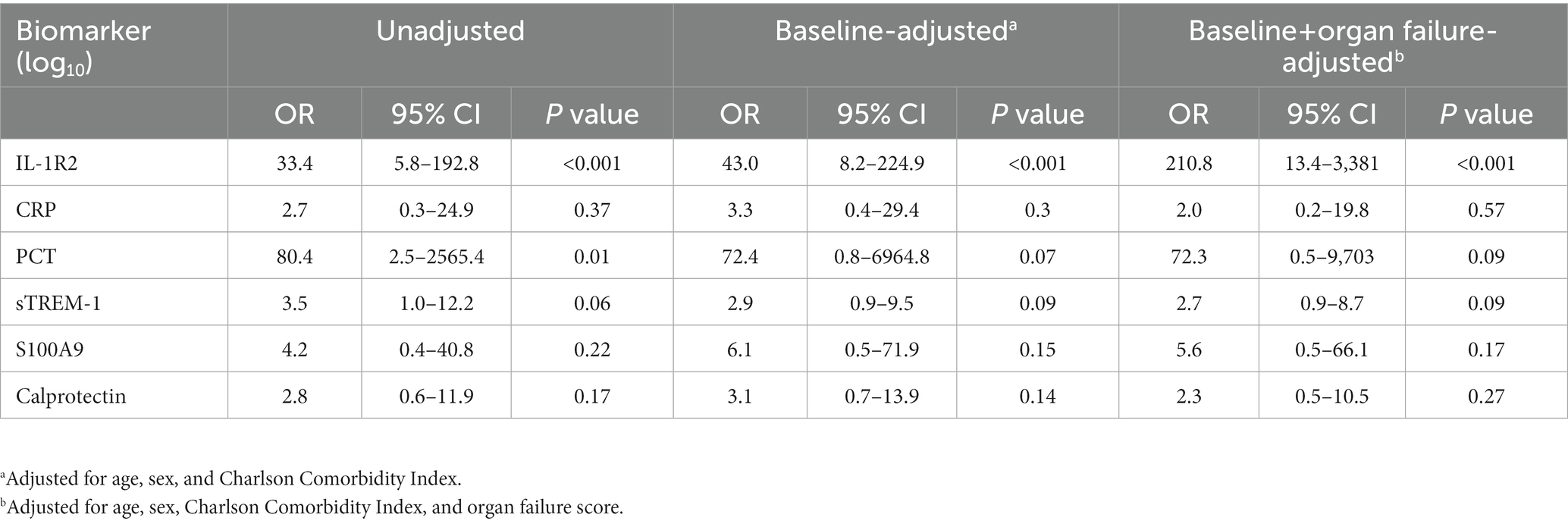
Table 3. Association of biomarkers with 28-day mortality in the derivation cohort.
To develop the simplest yet unbiased mortality prediction model, we performed LASSO regression on all six measured biomarkers from the derivation cohort, regardless of association with 28-day mortality. LASSO regression selected IL-1R2 and sTREM-1 for the final model. IL-1R2 and sTREM-1 were not significantly correlated (rho = 0.07, p = 0.53) and so both biomarkers were carried forward for further evaluation.
We next compared mortality discrimination of the two-biomarker model in comparison to a model comprised of the organ failure score using receiver operating characteristic curve analysis. The area under the receiver operating characteristic curve (AUC) was calculated for both models as well as single biomarker models containing IL-1R2 and sTREM-1 (Table 4; Figure 1A). The two-biomarker model had significantly higher mortality discrimination (AUC 0.81, 95% CI 0.72–0.91) compared to the organ failure score model (AUC 0.69, 95% CI 0.56–0.81; p < 0.01). Additionally, the IL-1R2 model had significantly higher mortality discrimination compared to the organ failure score model (AUC 0.78, 95% CI 0.68–0.88; p = 0.03) and similar discrimination compared to the two-biomarker model (p = 0.21). All models maintained their mortality discrimination after optimism-adjustment by bootstrapping and were assessed for calibration by goodness-of-fit testing (Supplementary Table S1).
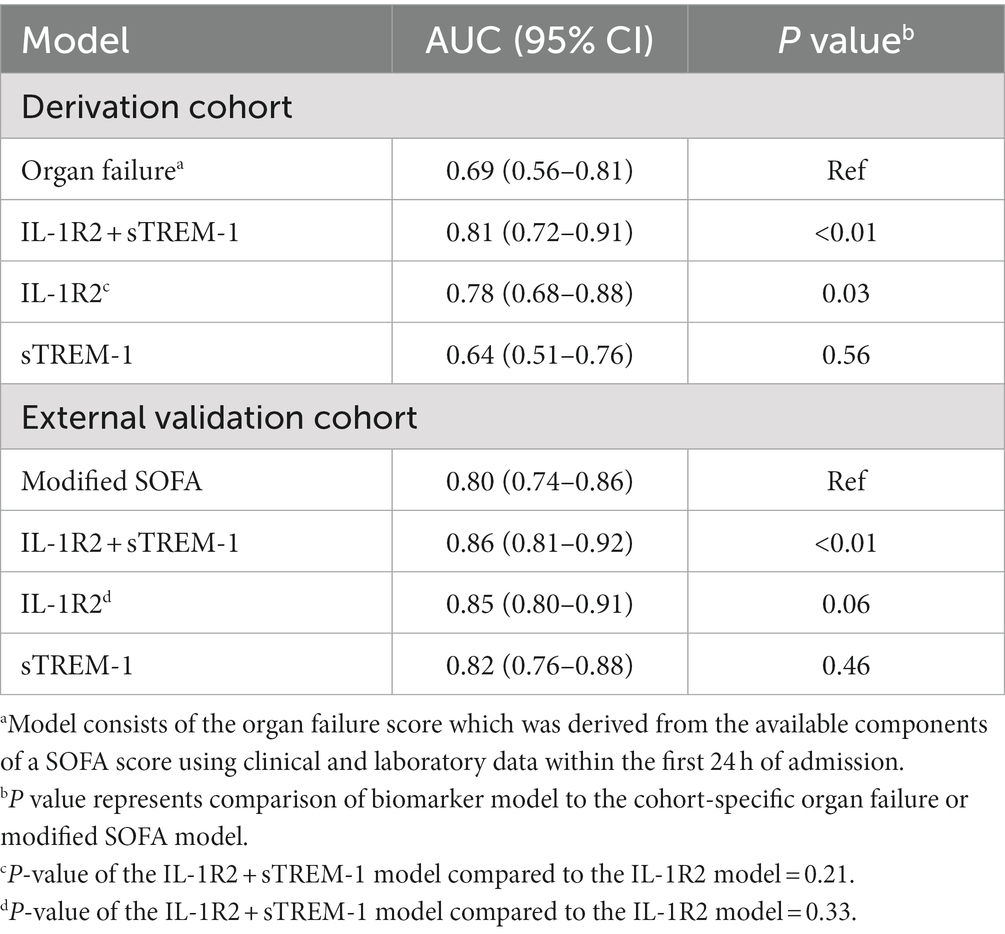
Table 4. Mortality discrimination in the derivation and external validation cohorts.
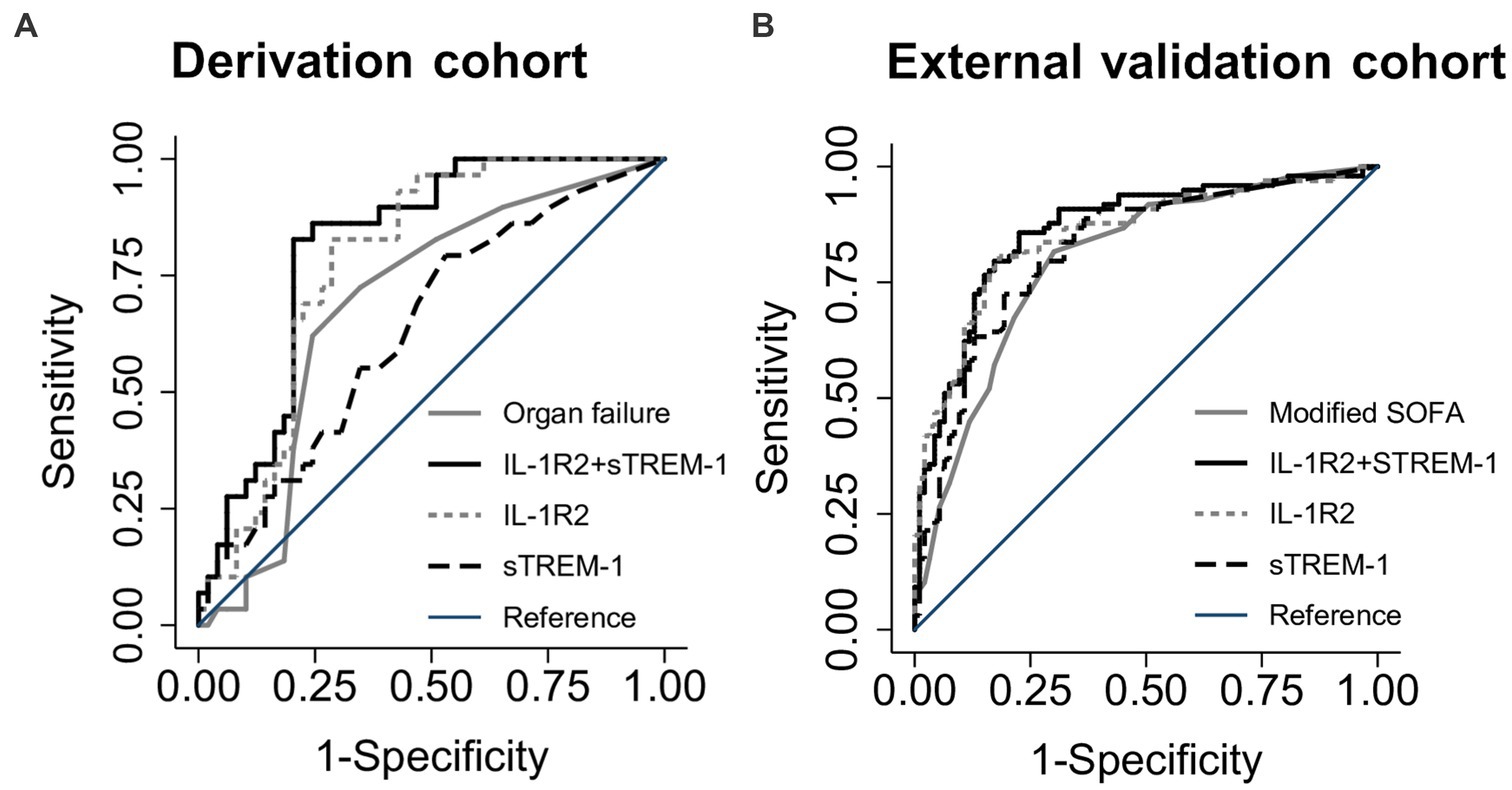
Figure 1. Receiver operating characteristic curves for discrimination of death at 28 days. Area under the receiver operating characteristic curves (AUC) for the two-biomarker model (IL-1R2 + sTREM-1) compared to IL-1R2 and sTREM-1 single biomarker models and an organ failure or modified SOFA score in either the derivation (A) or external validation (B) cohorts.
Given the similar mortality discrimination of the two-biomarker model and the IL-1R2 model, we next tested whether the IL-1R2 model had improved performance after the addition of sTREM-1. The addition of sTREM-1 did significantly improve the IL-1R2 model (likelihood ratio (LR) p = 0.02; Supplementary Table S2) though discrimination was only borderline improved (IDI = 0.06, p = 0.05). Given these findings, both models were brought forward for validation in an external cohort.
We next sought to validate the IL-1R2 + sTREM-1 and IL-1R2 models in an external cohort of melioidosis patients (Table 1). This cohort was larger than the derivation cohort, enrolled subjects less than 24 h after study hospital presentation and captured sufficient data to calculate a modified SOFA score including GCS. In this cohort, concentrations of both IL-1R2 and sTREM-1 were significantly higher in non-survivors compared to survivors (both p < 0.001; Supplementary Table S3). IL-1R2 and sTREM-1 were also significantly associated with 28-day mortality in models adjusted for baseline factors including age, sex, Charlson Comorbidity Index, with and without modified SOFA score (all p < 0.001; Table 5). The two-biomarker model significantly improved mortality discrimination compared to a modified SOFA score model (AUC 0.86, 95% CI 0.81–0.92 vs. AUC 0.80, 95% CI 0.74–0.86, p < 0.01; Figure 1B; Table 4). The IL-1R2 model trended toward significantly higher discrimination compared to the modified SOFA model (AUC 0.85, 95% CI 0.80–0.91, p = 0.06) and was similar to the two-biomarker model (p = 0.33). Both models had unchanged discrimination after bias-adjustment and appropriate goodness-of-fit (Supplementary Table S1).

Table 5. Association of biomarkers with 28-day mortality in the external validation cohort.
As the two-biomarker model had similar mortality discrimination to the IL-1R2 model, we next sought to determine if there was any clinical benefit of using the two-biomarker model compared to the IL-1R2 model by decision curve analysis. The IL-1R2 + sTREM-1 model had a higher clinical benefit for a cohort mortality of 10% to 50% (Supplementary Figure S2; Supplementary Table S4). However, the increase in correct identification of patients who would die in 28-days using the two-biomarker model was modest, ranging between 1 to 2.3 patients per 100.
As a one-biomarker model may have simplistic advantages and since the IL-1R2 model was nearly identical to the two-biomarker model in terms of mortality discrimination and clinical benefit, we next sought to calculate a reasonable prognostic cut-off value for IL-1R2. An optimal cut-off value of 173,911 pg/mL yielded a sensitivity for death of 72% (95% CI 63–81%) and specificity of 85% (95% CI 76–92%; Supplementary Table S5).
In this study, we report the development and validation of a plasma biomarker model to predict mortality in melioidosis. A model comprised of plasma concentrations of IL-1R2 and sTREM-1 performed better than an organ failure model in both our derivation and external validation cohorts in predicting mortality in melioidosis. Additionally, a simple model composed only of IL-1R2 performed nearly as well as the two-biomarker model and may be a reasonable substitute. Implemented for clinical use, these biomarker profiles may have value for melioidosis outcome prognostication in regions where the infection is endemic and may complement emerging rapid diagnostic tests (12).
We have previously reported that IL-6 and IL-8 concentrations augment the melioidosis mortality prediction of a clinical model (24). However, whether a biomarker model may be able to replace a clinical prediction model in melioidosis for prognostication has not been established. Clinical scores such as SOFA require multiple laboratory and clinical data, including the availability of mechanical ventilation and circulatory support. In our study, IL-1R2-containing models, which do not include any clinical variables, had superior performance compared to a comprehensive clinical variable model.
During systemic infection, IL-1R2 may serve as a decoy receptor for capturing and reducing the bioavailability of the pro-inflammatory cytokine IL-1 (25). Notably, some in vivo melioidosis models suggest IL-1 signaling may be detrimental. IL-1R1 knockout mice display increased resistance to B. pseudomallei infection but with decreased lung neutrophil recruitment and lower associated lung pathology (26). Similarly, anti-IL-1β treatment of B. pseudomallei-infected mice decreased bacterial replication and was associated with reduced mortality (27). In humans, up-regulated transcription of the IL1R2-associated gene has been described in critically ill patients with sepsis (28). Our novel finding that IL-1R2 plasma concentration is associated with mortality in melioidosis supports our recent report that blood leukocyte IL1R2 upregulation is likewise associated with melioidosis mortality (13). Triggering receptor expressed on myeloid cells 1 (TREM-1) is a transmembrane receptor which is commonly found on innate immune cells, including neutrophils (29). Additionally, sTREM-1 plasma concentrations have strong mortality prediction in sepsis in Southeast Asia and are elevated in melioidosis (11, 30).
In our study an optimized cutoff of IL-1R2 assessed within 24 h of admission yielded both a reasonable sensitivity and specificity for 28-day mortality. While IL-1R2 protein measurements may not be widely available assays in clinical laboratories, our findings suggest that IL-1R2 alone or in combination with sTREM-1 could be adapted as a rapid point-of-care assay. Such tests, deployed to the bedside, could be used by a variety of personnel with varying levels of medical training, and may supplant the need for detailed clinical efforts to ascertain prognostic information.
Our study has a variety of strengths. This is one of the few reported studies to include prospectively enrolled patients with melioidosis in independent cohorts from different sites. All included subjects had culture-proven B. pseudomallei infection, the gold standard for melioidosis diagnosis. Both cohort studies had minimal missing data or loss to follow-up and thorough sample processing. Our model development and validation methodology was rigorous, followed TRIPOD guidelines, and also minimized bias effects and model overfitting. Finally, both cohorts utilized 28-day mortality (rather than hospital mortality) as the primary outcome, important in areas such as northeast Thailand where many critically ill patients are discharged at their request to die at home.
Our study also has several limitations. Both cohorts were drawn from referral healthcare centers in northeast Thailand and may not be representative outside those settings. In our derivation cohort, subjects were enrolled at the time of diagnosis, typically about 4 days after admission, whereas in our external validation cohort, subjects were enrolled within 24 h of hospital admission. These timing differences may account for the higher discrimination of IL-1R2 and sTREM-1 in our external validation cohort. Furthermore, we did not have a GCS score available in our derivation cohort, limiting complete assessments of clinical severity. Similarly, in both cohorts, the paucity of arterial blood gas and other data prevented complete SOFA calculations. Our plasma biomarker quantification of IL-1R2 utilized the same ELISA for both cohorts. However, our assessment of sTREM-1 used different ELISAs in each cohort, allowing for a possible difference in sensitivity and may explain the lower concentrations in the derivation cohort. ELISA methodology may also have lower sensitivity than other methods including bead-based multiplex and electrochemiluminescence assays. Furthermore, our analysis plan was designed a priori to select the simplest biomarker model while minimizing bias. However, other biomarkers such as CRP and PCT, which were not carried forward in our selection process, may furnish similar mortality discrimination to those analyzed. Finally, outside a randomized controlled trial, assessing the clinical utility of a biomarker model is challenging (31). Therefore, additional studies are required to better determine how our biomarkers might be adapted to a clinical context, including use in a point-of-care format.
In summary, we have developed and validated novel biomarker models with IL-1R2 protein for predicting 28-day mortality in patients with melioidosis. These models are a viable substitute for outcome prediction based on multiple clinical variables. If implemented in the future at the point-of-care in melioidosis-endemic areas, detection of IL-1R2 may be able to identify patients at highest risk of deterioration early in their course and inform clinical decision making.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the studies were approved by the ethics committee of Faculty of Tropical Medicine, Mahidol University (approval no. MUTM 2015-002-04, MUTM 2011-007-03, MUTM 2012-024-01, and MUTM 2018-047), Udon Thani Hospital Ethics Committee (00.32.102/318), Sunpasitthiprasong Hospital Ethics Committee (039/2556), the University of Washington Institutional Review Board (42988) and the Oxford University Tropical Research Ethics Committee (OXTREC172-12). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
TK, NC, SW, and TW were involved in the design of the study. TK, TY, SW, LL-M, GR, DD, and AD collected samples and performed experiments. RP, VH, and GL recruited patients and collected data. TW, SW, and TK performed the statistical analysis. ND, NC, DL, and GL provided facilities. NC and TW were responsible for supervision of the study. All authors were involved in writing the paper and have approved the final version.
This work was supported by the United States National Institutes of Health [grant numbers T32GM086270, K12HD047349, K08HL157562, R01HL113382, R01AI137111, and U01AI115520] and the Wellcome Trust [090219/Z/09/Z; 101103/Z/13/Z; 220211]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Wellcome Trust. For the purpose of Open Access, the authors have applied a CC BY public copyright license to any author accepted manuscript version arising from this submission.
The authors are grateful for the support of the staff at Udon Thani Hospital, Sunpasitthiprasong Hospital, Mahidol-Oxford Tropical Medicine Research Unit (MORU) and Department of Microbiology and Immunology, Faculty of Tropical Medicine, Mahidol University for their assistance.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2023.1211265/full#supplementary-material
1. Wiersinga, WJ, Virk, HS, Torres, AG, Currie, BJ, Peacock, SJ, Dance, DAB, et al. Melioidosis. Nat Rev Dis Primers. (2018) 4:17107. doi: 10.1038/nrdp.2017.107
2. Wiersinga, WJ, Currie, BJ, and Peacock, SJ. Melioidosis. N Engl J Med. (2012) 367:1035–44. doi: 10.1056/NEJMra1204699
3. Limmathurotsakul, D, Golding, N, Dance, DA, Messina, JP, Pigott, DM, Moyes, CL, et al. Predicted global distribution of Burkholderia pseudomallei and burden of melioidosis. Nat Microbiol. (2016) 1:15008. doi: 10.1038/nmicrobiol.2015.8
4. Vincent, JL, Moreno, R, Takala, J, Willatts, S, de Mendonça, A, Bruining, H, et al. The SOFA (Sepsis-related organ failure assessment) score to describe organ dysfunction/failure. On behalf of the working group on Sepsis-related problems of the European Society of Intensive Care Medicine. Intensive Care Med. (1996) 22:707–10. doi: 10.1007/BF01709751
5. Knaus, WA, Wagner, DP, Draper, EA, Zimmerman, JE, Bergner, M, Bastos, PG, et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest. (1991) 100:1619–36. doi: 10.1378/chest.100.6.1619
6. Lie, KC, Lau, CY, Van Vinh, CN, and West, TE. Limmathurotsakul D for Southeast Asia infectious disease clinical research network. Utility of SOFA score, management and outcomes of sepsis in Southeast Asia: a multinational multicenter prospective observational study. J Intensive Care. (2018) 6:9. doi: 10.1186/s40560-018-0279-7
7. Rudd, KE, Seymour, CW, Aluisio, AR, Augustin, ME, Bagenda, DS, Beane, A, et al. Association of the Quick Sequential (Sepsis-related) organ failure assessment (qSOFA) score with excess hospital mortality in adults with suspected infection in low- and middle-income countries. JAMA. (2018) 319:2202–11. doi: 10.1001/jama.2018.6229
8. Kaewarpai, T, Ekchariyawat, P, Phunpang, R, Wright, SW, Dulsuk, A, Moonmueangsan, B, et al. Longitudinal profiling of plasma cytokines in melioidosis and their association with mortality: a prospective cohort study. Clin Microbiol Infect. (2020) 26:783.e1–8. doi: 10.1016/j.cmi.2019.10.032
9. Natesan, M, Corea, E, Krishnananthasivam, S, Sathkumara, HD, Dankmeyer, JL, Dyas, BK, et al. Calprotectin as a biomarker for Melioidosis disease progression and management. J Clin Microbiol. (2017) 55:1205–10. doi: 10.1128/JCM.02284-16
10. Smith, MD, Suputtamongkol, Y, Chaowagul, W, Assicot, M, Bohuon, C, Petitjean, S, et al. Elevated serum procalcitonin levels in patients with melioidosis. Clin Infect Dis. (1995) 20:641–5. doi: 10.1093/clinids/20.3.641
11. Wiersinga, WJ, Veer, C, Wieland, CW, Gibot, S, Hooibrink, B, Day, NP, et al. Expression profile and function of triggering receptor expressed on myeloid cells-1 during melioidosis. J Infect Dis. (2007) 196:1707–16. doi: 10.1086/522141
12. Noparatvarakorn, C, Sengyee, S, Yarasai, A, Phunpang, R, Dulsuk, A, Ottiwet, O, et al. Prospective analysis of antibody diagnostic tests and TTS1 real-time PCR for diagnosis of Melioidosis in areas where it is endemic. J Clin Microbiol. (2023) 61:e0160522. doi: 10.1128/jcm.01605-22
13. Yimthin, T, Cliff, JM, Phunpang, R, Ekchariyawat, P, Kaewarpai, T, Lee, JS, et al. Blood transcriptomics to characterize key biological pathways and identify biomarkers for predicting mortality in melioidosis. Emerg Microbes Infect. (2021) 10:8–18. doi: 10.1080/22221751.2020.1858176
14. Hantrakun, V, Somayaji, R, Teparrukkul, P, Boonsri, C, Rudd, K, Day, NPJ, et al. Clinical epidemiology and outcomes of community acquired infection and sepsis among hospitalized patients in a resource limited setting in Northeast Thailand: a prospective observational study (Ubon-sepsis). PLoS One. (2018) 13:e0204509. doi: 10.1371/journal.pone.0204509
15. Moons, KG, Altman, DG, Reitsma, JB, Ioannidis, JP, Macaskill, P, Steyerberg, EW, et al. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): explanation and elaboration. Ann Intern Med. (2015) 162:W1–W73. doi: 10.7326/M14-0698
16. Tibshirani, R. Regression shrinkage and selection via the lasso. J R Stat Soc Ser B. (1996) 58:267–88. doi: 10.1111/j.2517-6161.1996.tb02080.x
17. Pavlou, M, Ambler, G, Seaman, S, De Iorio, M, and Omar, RZ. Review and evaluation of penalised regression methods for risk prediction in low-dimensional data with few events. Stat Med. (2016) 35:1159–77. doi: 10.1002/sim.6782
18. Hosmer, DW, Hosmer, T, Le Cessie, S, and Lemeshow, S. A comparison of goodness-of-fit tests for the logistic regression model. Stat Med. (1997) 16:965–80. doi: 10.1002/(sici)1097-0258(19970515)16:9<965::aid-sim509>3.0.co;2-o
19. Harrell, FE Jr, Lee, KL, and Mark, DB. Multivariable prognostic models: issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat Med. (1996) 15:361–87. doi: 10.1002/(SICI)1097-0258(19960229)15:4<361::AID-SIM168>3.0.CO;2-4
20. Pencina, MJ, D'Agostino, RB, D'Agostino, RB, and Vasan, RS. Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat Med. (2008) 27:157–72. doi: 10.1002/sim.2929
21. Steyerberg, EW, Vickers, AJ, Cook, NR, Gerds, T, Gonen, M, Obuchowski, N, et al. Assessing the performance of prediction models: a framework for traditional and novel measures. Epidemiology. (2010) 21:128–38. doi: 10.1097/EDE.0b013e3181c30fb2
22. Vickers, AJ, Cronin, AM, Elkin, EB, and Gonen, M. Extensions to decision curve analysis, a novel method for evaluating diagnostic tests, prediction models and molecular markers. BMC Med Inform Decis Mak. (2008) 8:53. doi: 10.1186/1472-6947-8-53
23. Youden, WJ. Index for rating diagnostic tests. Cancer. (1950) 3:32–5. doi: 10.1002/1097-0142(1950)3:1<32::aid-cncr2820030106>3.0.co;2-3
24. Wright, SW, Kaewarpai, T, Lovelace-Macon, L, Ducken, D, Hantrakun, V, Rudd, KE, et al. A 2-biomarker model augments clinical prediction of mortality in Melioidosis. Clin Infect Dis. (2021) 72:821–8. doi: 10.1093/cid/ciaa126
25. Peters, VA, Joesting, JJ, and Freund, GG. IL-1 receptor 2 (IL-1R2) and its role in immune regulation. Brain Behav Immun. (2013) 32:1–8. doi: 10.1016/j.bbi.2012.11.006
26. Ceballos-Olvera, I, Sahoo, M, Miller, MA, Del Barrio, L, and Re, F. Inflammasome-dependent pyroptosis and IL-18 protect against Burkholderia pseudomallei lung infection while IL-1beta is deleterious. PLoS Pathog. (2011) 7:e1002452. doi: 10.1371/journal.ppat.1002452
27. Weehuizen, TA, Lankelma, JM, de Jong, HK, de Boer, OJ, Roelofs, JJ, Day, NP, et al. Therapeutic administration of a monoclonal anti-Il-1β antibody protects against experimental Melioidosis. Shock. (2016) 46:566–74. doi: 10.1097/SHK.0000000000000625
28. Schaack, D, Siegler, BH, Tamulyte, S, Weigand, MA, and Uhle, F. The immunosuppressive face of sepsis early on intensive care unit-a large-scale microarray meta-analysis. PLoS One. (2018) 13:e0198555. doi: 10.1371/journal.pone.0198555
29. Bouchon, A, Dietrich, J, and Colonna, M. Cutting edge: inflammatory responses can be triggered by TREM-1, a novel receptor expressed on neutrophils and monocytes. J Immunol. (2000) 164:4991–5. doi: 10.4049/jimmunol.164.10.4991
30. Wright, SW, Lovelace-Macon, L, Hantrakun, V, Rudd, KE, Teparrukkul, P, Kosamo, S, et al. sTREM-1 predicts mortality in hospitalized patients with infection in a tropical, middle-income country. BMC Med. (2020) 18:159. doi: 10.1186/s12916-020-01627-5
Keywords: biomarkers, melioidosis, IL-1R2, sTREM-1, mortality
Citation: Kaewarpai T, Wright SW, Yimthin T, Phunpang R, Dulsuk A, Lovelace-Macon L, Rerolle GF, Dow DB, Hantrakun V, Day NPJ, Lertmemongkolchai G, Limmathurotsakul D, West TE and Chantratita N (2023) IL-1R2-based biomarker models predict melioidosis mortality independent of clinical data. Front. Med. 10:1211265. doi: 10.3389/fmed.2023.1211265
Edited by:
Sam Donta, Falmouth Hospital, United StatesReviewed by:
Thomas Robert Laws, Defence Science and Technology Laboratory, United KingdomCopyright © 2023 Kaewarpai, Wright, Yimthin, Phunpang, Dulsuk, Lovelace-Macon, Rerolle, Dow, Hantrakun, Day, Lertmemongkolchai, Limmathurotsakul, West and Chantratita. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Narisara Chantratita, bmFyaXNhcmFAdHJvcG1lZHJlcy5hYw==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.