 Timothy S. Fitzsimmons1*†
Timothy S. Fitzsimmons1*† Niharika Singh1*†
Niharika Singh1*† Thomas D. J. Walker2
Thomas D. J. Walker2 Claire Newton3
Claire Newton3 Dafydd G. R. Evans4
Dafydd G. R. Evans4 Emma J. Crosbie2*
Emma J. Crosbie2* Neil A. J. Ryan5,6*
Neil A. J. Ryan5,6*- 1Clinical Medical School, University of Bristol, Bristol, United Kingdom
- 2Division of Cancer Sciences, St Mary’s Hospital, Faculty of Biology, Medicine and Health, University of Manchester, Manchester, United Kingdom
- 3Department of Obstetrics and Gynaecology, St Michaels Hospital, Bristol, United Kingdom
- 4Division of Evolution and Genomic Medicine, St Mary’s Hospital, University of Manchester, Manchester, United Kingdom
- 5The College of Medicine and Veterinary Medicine, University of Edinburgh, Edinburgh, United Kingdom
- 6Department of Gynaecology Oncology, Royal Infirmary of Edinburgh, Edinburgh, United Kingdom
Background: Immune checkpoint inhibitors (ICPI) are a tumor agnostic treatment. However, trials of their use have been site specific. Here we summarize the trial data and explore the utility of programmed death-ligand 1 (PD-L1) expression as a biomarker to direct their pan-cancer use.
Method: A systematic review of literature, following PRISMA guidelines, was performed. Medline, Embase, Cochrane CENTRAL, NHS Health and Technology, and Web of Science were searched from their conception to June 2022 limited to the English language. The search terms and method were devised by a specialist medical librarian. Studies were limited to adults with solid cancers (excluding melanomas) treated with ICPIs. Only phase III randomized control trials (RCT) were included. The primary outcome was overall survival and secondary outcomes were progression free survival, PD-L1 expression, quality of life outcomes and adverse event data. Where present in eligible clinical trials, hazard ratios (HR), risk ratios (RR), standard error (SE) and 95% confidence intervals (CI) were extracted or calculated. Heterogeneity across studies was described with the use of an I2 score (Low: 25, 50%: moderate, 75% low heterogeneity). HR pools inverse variance methods were adopted by Random Effects (RE). Means were standardized across any heterogenous scale limits.
Results: In total 46,510 participants were included in the meta-analysis. Overall, meta-analysis favored the use of ICPIs with an overall survival (OS) HR of 0.74 (95% CI 0.71 to 0.78). Lung cancers showed the most benefit in OS [HR 0.72 (95% 0.66–0.78)] followed by head and neck cancers [HR 0.75 (95% CI 0.66–0.84)] and gastroesophageal junction cancers [HR 0.75 (95% CI 0.61–0.92)]. ICPIs seem to be efficacious at both primary presentation and recurrence [OS HR 0.73 (95% CI 0.68–0.77)] vs. [OS HR 0.79 (95% CI 0.72 to 0.87)] respectively. Interestingly, subgroup analysis comparing studies in which most cancers demonstrated PD-L1 expression vs. those studies in which a minority of cancer demonstrated PD-L1 expression reported similar effect of ICPI use on OS; oddly the data favored ICPI use in studies with a minority of PD-L1 expression. Specifically, studies with minority PD-L1 expression had an HR 0.73 (95% CI 0.68–0.78) vs. studies with majority PD-L1 expression HR 0.76 (95% CI 0.70–0.84). This was maintained even when studies exploring the same cancer site were directly compared. Subgroup analysis was performed comparing the impact on OS subdivided by the specific ICPI used. Where meta-analysis was performed, Nivolumab led to the greatest impact [HR 0.70 (95% CI 0.64–0.77)] with Avelumab failing to reach significance [HR 0.93 (95% CI 0.80–1.06)]. However, overall heterogenicity was high (I2 = 95%). Finally, the use of ICPIs led to an improved side effect profile when compared with standard chemotherapy [RR 0.85 (95% CI 0.73–0.98)].
Conclusion: ICPIs improve survival outcomes in all cancer types. These effects are seen in the primary, recurrent, chemotherapy sensitive, chemotherapy resistant disease. These data support their use as a tumor agnostic therapy. Furthermore, they are well tolerated. However, PD-L1 as a biomarker for the targeting of ICPI use seems problematic. Other biomarkers such as mismatch repair or tumor mutational burden should be explored in randomized trials. In addition, there are still limited trials looking at ICPI use outside of lung cancer.
Background
Cancer is the second leading cause of death in the world; only behind cardiovascular disease (1). Despite advancements in treatments, the mortality rate for many cancers remains high (2). For patients with advanced cancer, chemotherapy and radiotherapy are the primary treatment options. However, due to the systemic nature of chemotherapy, there have been issues with toxic side effects as well as drug resistance. Targeted therapies are therefore of intrinsic value as they seek to reduce treatment toxicity and resistance (3). One such targeted therapy are immune checkpoint inhibitors (ICPIs).
Immune checkpoint inhibitors are a class of treatment that exploit a common mechanism of cancer immune escape: the programmed death-1/programmed death ligand (PD-1/PD-L1) ligand/receptor interaction (4). Indeed, cancers that arise due to a defective mismatch repair system commonly exploit the PD-1/PD-L1 pathway (5). Cancers which overexpress PD-L1 inhibit cytotoxic T cells (6). These deactivated T cells remain in the tumor microenvironment as they are continuously recruited through the production of cancer related neo-antigens (7). ICPIs are monoclonal antibodies that act to block the PD-1/PD-L1 axis and reverse the induced T cell exhaustion to prevent cancer immune escape (8). They lead to a re-activation of the recruited tumor associated lymphocytes and tumor containment or eradication.
ICPIs have been trialed in numerous cancer sites with generally encouraging results (9). They were the first class of drug to receive approval from the Federal Drug Agency (FDA) based on a molecular characteristic within the tumor (microsatellite instability (MSI) or high mutational burden (HMB)) as opposed to the anatomical cancer site (10, 11). This approval was based on pooled data of single arm cohorts from trials as no meta-analysis existed (12). However to date, most trials have used PD-L1 as a biomarker for ICPI use and not MSI or HMB (13).
The use of PD-L1 as a biomarker for ICPI is based on its use in the initial trials done in melanomas (14). This is despite the original study that explored ICPI use in melanoma reporting that PD-L1 did not predict those in whom ICPI would lead to significant improved survival (15). There remains limited data synthesis as to the utility of PD-L1 as a biomarker of ICPIs effectiveness across all cancer sites. These data are important given the clinical application of ICPIs is not based on cancer site but tumoral biomarkers. This analysis is also prudent given the increasing use of ICPIs across multiple cancer sites, despite a relatively limited evidence base for their use in that specific cancer site (16). If pan-cancer analysis supported their application based on the expression of a biomarker, clinicians could be more confident in trialing ICPIs in these lesser studied cancer types based on the molecular profile of the cancer. In addition, if PD-L1 expression proved to be an accurate predictor of ICPIs treatment efficacy across multiple cancer sites, its sustained use as such a biomarker in trials would become clinically meaningful.
The aim of this study was to perform a systematic review and meta-analysis to synthesis the existing trial data evaluating the ICPIs use in all solid cancer types. Our hope was to provide evidence as to their cross-cancer utility and help inform their current application based on molecular characteristics as opposed to anatomical cancer site. In addition, we will explore the utility of PD-L1 as a biomarker of ICPI treatment efficacy.
Method
Search strategy and study identification
A systematic review of literature, following PRISMA guidelines, was performed (17). Medline, Embase, Cochrane CENTRAL, NHS Health and Technology, and Web of Science were searched from their conception to May 2022. The search terms and method were devised by a specialist medical librarian. In addition, we searched for non-published trial data via www.controlled-trials.com/rct and www.cancer.gov/clinicaltrials. Initial search results were supplemented by citation searching. Non-electronic and grey literature were excluded. The search methods are detailed in Supplementary material section 1.
Selection criteria
The protocol for this systematic review was preregistered with the PROSPERO database registration (ref: CRD420202219410). Only studies published in English were included. Studies were limited to adults with solid cancers (excluding melanomas) treated with ICPIs. Melanoma was excluded due to its exceptionally high expression of PD-L1 and the extensive evidence indicating ICPI therapeutic efficacy along with standardized PD-L1 immunohistochemistry protocols (18). These factors make it a distinct clinical entity that would be problematic to include in a pan-cancer meta-analysis. Only phase III randomized control trials were included. The primary outcome was overall survival with secondary outcomes being progression free survival, PD-L1 expression, quality of life outcomes and adverse event data. Full selection criteria are detailed in Supplementary material section 1.
Data extraction
Titles and abstracts were collated and screened using the Rayyan software1. Screening was done independently by two authors (TF and NS), with any discrepancies reviewed by a third party (NAJR). Studies that were identified as meeting the inclusion criteria underwent full paper review which was conducted by two authors (TF and NS), with issues resolved through discussion and consensus with a senior author (NAJR) who made the final decision. A bespoke data collection tool was designed to ensure complete capture of all primary and secondary outcome data points (available on request). Demographic, tumor characteristics, therapeutic and outcome data were collected independently by two authors (TF and NS) and crosschecked (NAJR). The key outcomes are detailed in Supplementary Table S2. In studies in which there were multiple treatment arms, data was only extracted from the relevant arm in which an ICPI has been directly compared to a standard therapy or placebo.
Assessment of bias
Risk of bias was assessed using the International Cochrane Collaborations guidelines. This tool uses a 3-point scale to assess the following: selection, performance, detection, attrition, and reporting (19). Using scores from each of these 6 domains, an overall risk of bias for each trial was calculated. Definition of overall bias was calculated: ‘low’ if 4 or more domains were scored as low; ‘high’ if 3 or more domains were scored as high; ‘medium’ if neither of the above.
PD-L1 status
Studies were grouped into two groups; namely those in which the majority of tumors demonstrated high PD-L1 expression and those in which minority of tumors demonstrated high PD-L1 expression. The definition of high PD-L1 expression was taken from the authors’ definition. A majority was defined as >50% of the study population treated with ICPIs had tumors with high PD-L1 expression. In addition, the effect of significant PD-L1 expression (again as defined by the authors) was explored in different subgroup analysis.
Statistical analysis
A Priori power analyses were conducted for Random-Effects (RE) models with a conservative OR of 0.85 and between-study heterogeneity gradings at “low,” “medium,” and “high” with study size n-1 the predicted dataset.
Where present in eligible clinical trials, hazard ratios (HR), risk ratios (RR), standard error (SE) and 95% confidence intervals (CI) were extracted or calculated from source data. Means were standardized across any heterogenous scale limits. See Supplementary material for more detail.
All analysis was performed using R version 4.1.02 with the following libraries: tidyverse, meta version 5.0, metafor, and dmetar (20–22).
Results
Search results
Our search of the medical databases yielded 3,567 articles. In addition, searching the trials registry resulted in 695 additional studies. Therefore, after the removal of duplicates (n = 258), 4,004 studies underwent initial abstract screening. Four further studies were identified through citation searching. In total 81 papers underwent full manuscript review of which 44 were excluded (see Supplementary Table S4). Therefore 37 studies (23–59) were included in this systematic review and meta-analysis. This process is summarized in Figure 1.

Figure 1. Prisma flow diagram.
Study characteristics
In total 46,510 participants were included in the meta-analysis. Four studies (31, 53, 54, 56) were found to have no risk of bias (see Supplementary Figure S1). Included studies were conducted in North America (n = 25), China (n = 5), Europe (n = 4), and Japan (n = 3). These studied lung (n = 18), gastro-esophageal junction (n = 6), head and neck (n = 3), breast (n = 3), uroepithelial (n = 2), ovarian (n = 2), liver (n = 1), mesothelioma (n = 1), and renal cell (n = 1) cancers. Studies were either in the primary (n = 15) or relapsed (n = 22) setting. The majority (n = 27) reported the number of tumors with PD1/PD-L1 expression. A range of ICPIs were used: Pembrolizumab (n = 16), Nivolumab (n = 11), Atezolizumab (n = 6) or Avelumab (n = 3) Durvalumab (n = 1). Most controls were non-ICPI agents, however five studies had a sole placebo control arm. These data are summarized in Table 1. Results detailing analysis power, small study effects, and influential studies can be found in the Supplementary material section 1.4.
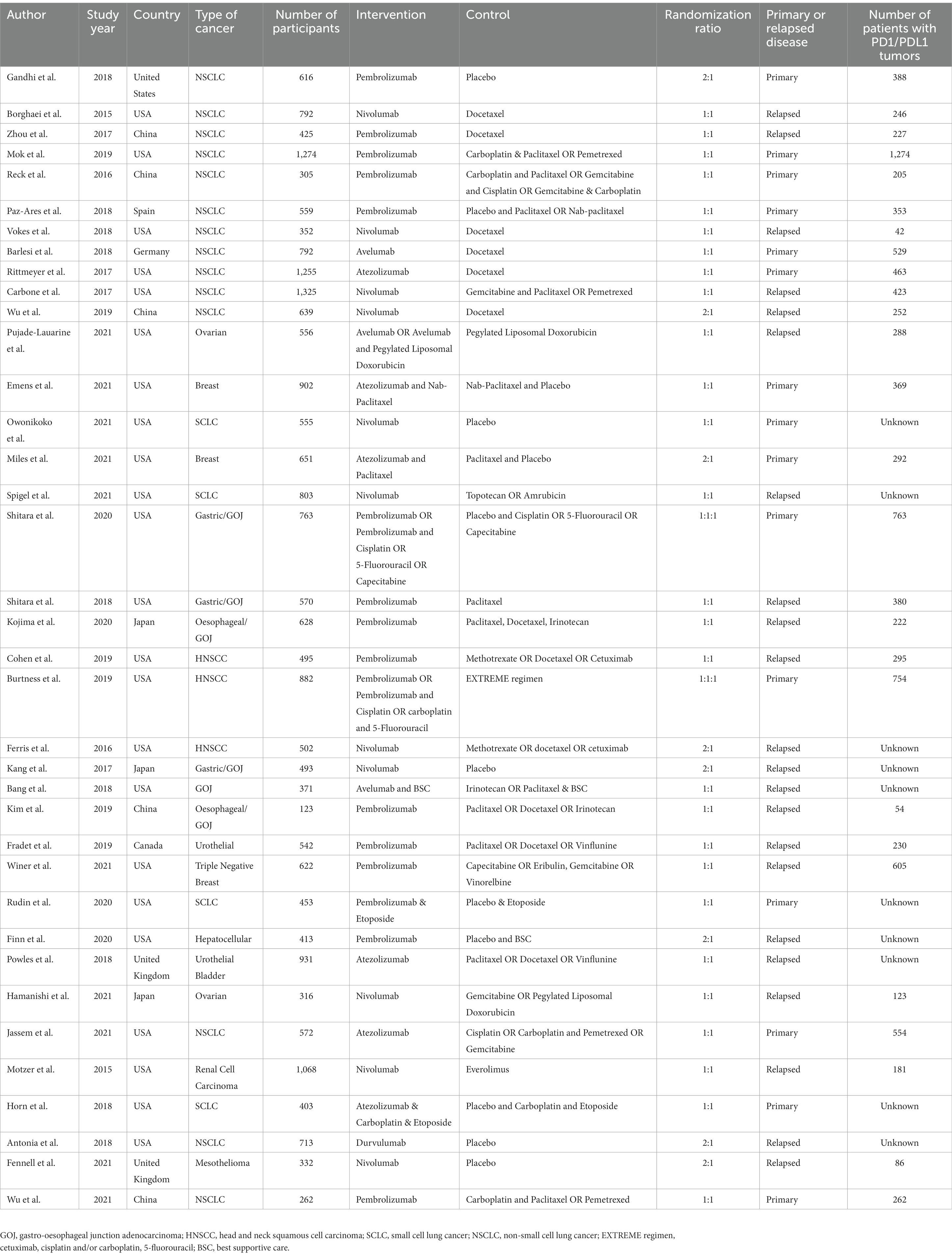
Table 1. Included studies characteristics.
Overall survival
All cancers
In total, 34 studies informed the pan-cancer overall survival (OS) meta-analysis, with four studies (26, 40, 44, 47) contributing data from more than one arm. Overall, meta-analysis favored the use of ICPIs with a HR of 0.74 (95% CI 0.71–0.78). Heterogeneity was high [I2 95% (95% CI 94–96)]. These data are summarized in Figure 2.
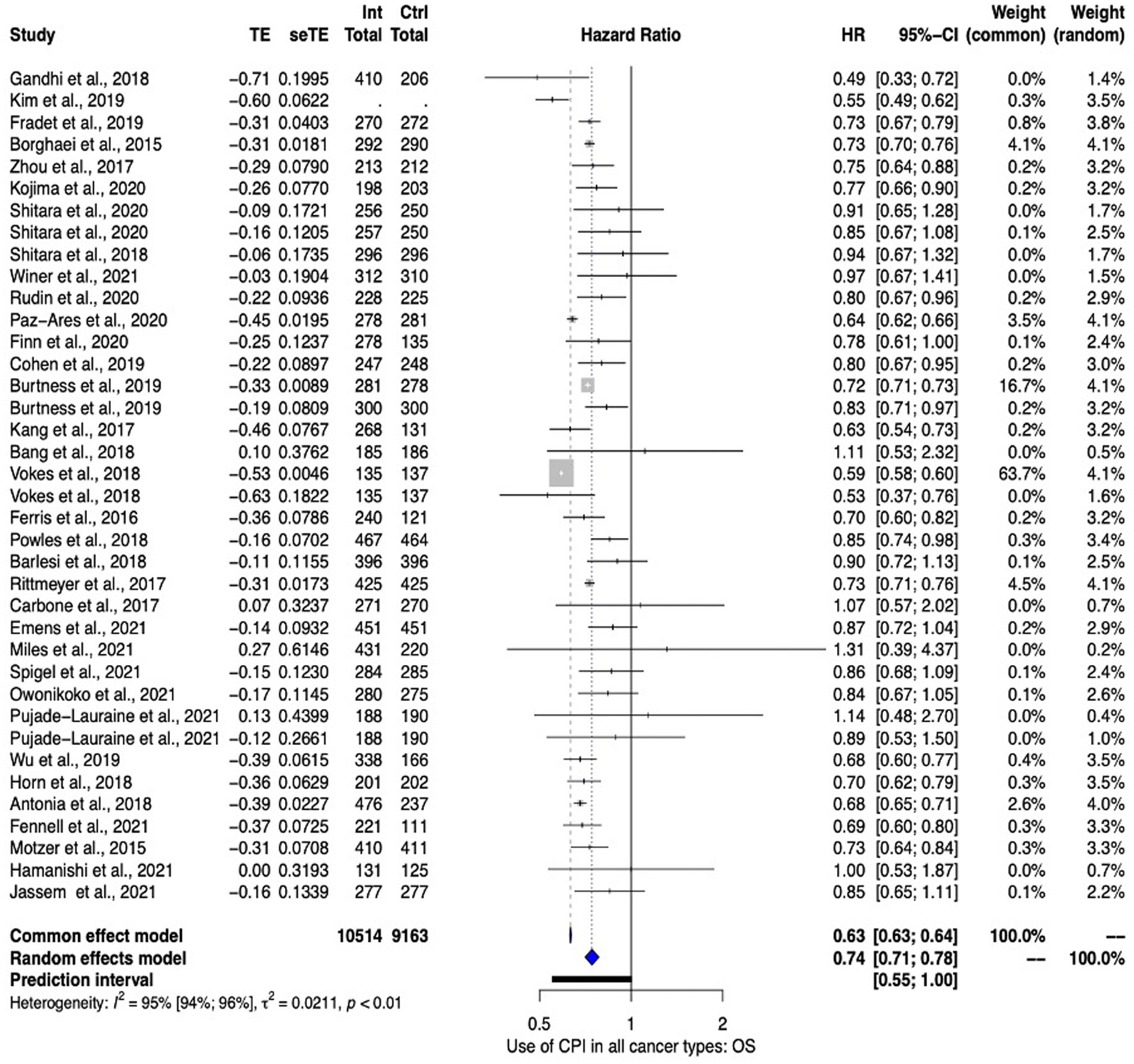
Figure 2. Pan cancer overall survival analysis ICPIs vs Control.
Cancer site
Subgroup analysis was performed by cancer site as to explore its effect on OS. The subgroup analysis included studies investigating lung (n = 15), gastro-esophageal junction (n = 6), breast (n = 3), head and neck (n = 3), ovarian (n = 2), urothelial cancers (n = 2), liver (n = 1), renal (n = 1), and mesothelioma (n = 1). Overall, all cancer sites favored the use of ICPIs [HR 0.78 (95% CI 0.74–0.81)]. However, only lung, head and neck, liver, mesothelioma, renal and gastro-esophageal junction cancers demonstrated a significant benefit in their subgroup analysis. Mesothelioma demonstrated the most significant effect [HR 0.69 (95% 0.60–0.80)] however this was based on one study. Where meta-analysis was possible, lung cancers showed the most benefit [HR 0.72 (95% CI 0.66–0.78)] followed by head and neck cancers [HR 0.75 (95% CI 0.66–0.84)] and gastro-esophageal junction cancers [HR 0.75 (95% CI 0.61 to 0.92)]. These data are summarized in Figure 3.
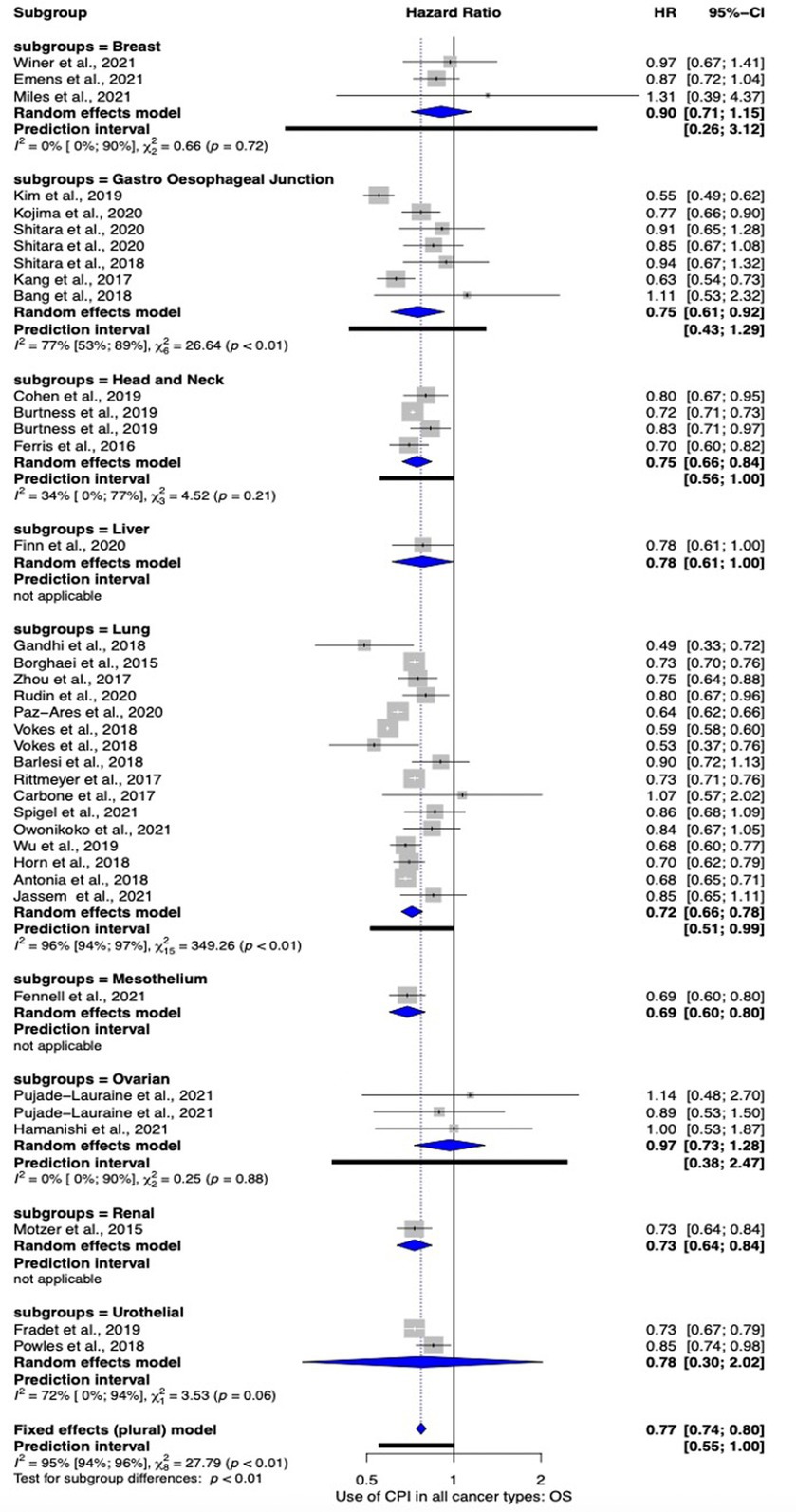
Figure 3. Subgroup meta-analysis comparing the efficacy of ICPI use on OS by cancer site.
Looking to lung cancer in more detail, a subgroup analysis was performed comparing the effect of ICPIs in both small cell and non-small disease. This was due to the higher levels of tumor mutational burden (TMB) in small cell cancers versus non-small cancers (11). Both histotypes demonstrated a significant benefit favoring the use of ICPIs [HR 0.73 (CI 95% 0.68–0.78)] however the effect was more pronounced in non-small cell cancers vs. small cell cancers (HR 0.69 vs. 0.77 respectively). These data are summarized in Supplementary Figure S2.
Disease specific characteristics
Immune checkpoint inhibitors seem to be efficacious at both primary presentation and recurrence {[HR 0.73 (95% CI 0.68 to 0.77)] vs. [HR 0.79 (95% CI 0.72 to 0.87)] respectively}. In advanced and metastatic cancers, the use of ICPIs led to an improved OS [HR 0.73 (95% CI 0.68–0.79)]. This was less pronounced in the recurrence setting [HR 0.80 (95% CI 0.72–0.89)] however fewer studies informed this sub meta-analysis when compared to the primary presentation. These data are presented in Supplementary Figure S3. See 1.4 in Supplementary material.
Treatment characteristics
Subgroup analysis was performed comparing the impact on OS subdivided by the specific ICPI used. Where meta-analysis was performed, Nivolumab lead to the greatest impact [HR 0.70 (95% CI 0.64 to 0.77)] with Avelumab failing to reach significance [HR 0.93 (95% CI 0.80 to 1.06)]. However, overall heterogenicity was high (I2 = 95%). These data are presented in Figure 4. Furthermore, we explored the impact on OS in studies whereby a single ICPI was used vs. studies in which more than one ICPI was used. The impact was similar in both scenarios [single agent HR: 0.68 (95% CI 0.62–0.75) vs. multiple agent HR: 0.68 (95% CI 0.57–0.81)]. These data are shown in Supplementary Figure S6.
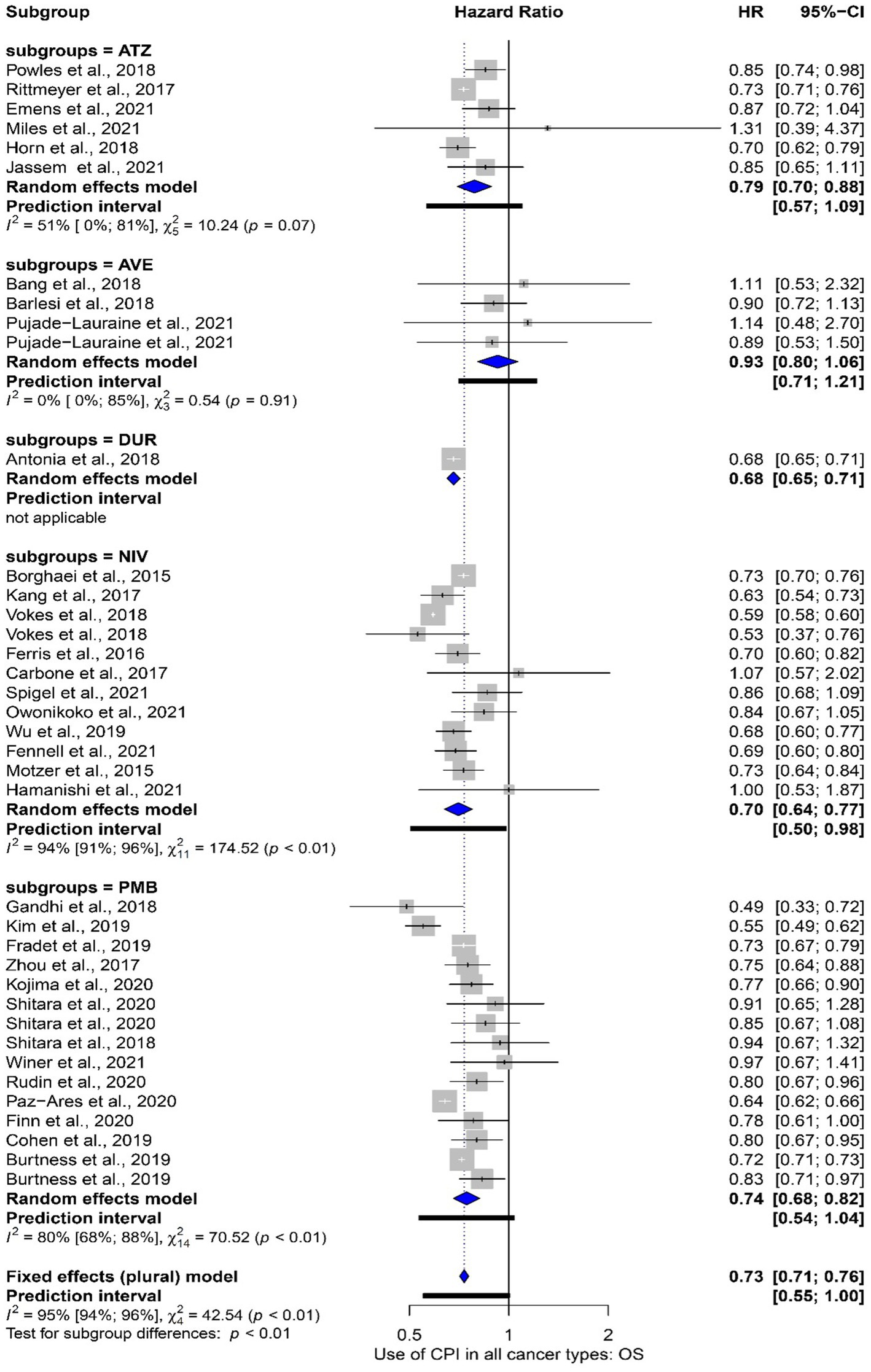
Figure 4. Subgroup meta-analysis comparting the overall survival grouped by studies that used different ICPI agents. Abbreviations: ATZ: Atezolizumab; AVE: Avelumab; NIV: Nivolumab; PMB: Pembrolizumab.
Study characteristics
The impact on OS was compared in studies deemed to be low bias vs. those studies deemed to have a high bias. There was limited impact on OS [low bias HR 0.72 (95% CI 0.66–0.78) vs. high bias HR 0.76 (95% CI 0.71–0.81)]. However, the low bias subgroup had a lower degree of heterogeneity (I2 77% vs. 94%). These data are presented in Supplementary Figure S7. Furthermore, we explored the impact of a placebo arm. When compared to a placebo or other treatment, ICPI performed well leading to significant improvement in OS HR 0.74 (95% CI 0.71–0.78). This was, as expected, more pronounced in the placebo arm with an of HR 0.67 (95% CI 0.56–0.82) vs. HR 0.75 (95% CI 0.71–0.80). Only a limited number of studies that included a placebo arm (n = 5); these data are summarized in Supplementary Figure S8.
Progression free survival
All cancers
In total 32 studies informed the pan-cancer progression free survival (PFS) analysis. Once more, four studies contributed data from more than one study arm (26, 40, 44, 47). The use of ICPIs did improve PFS across all cancer sites [HR 0.80 (95% CI 0.74–0.87)]. Heterogeneity across studies was high (I2 98%). These data are presented in Figure 5.
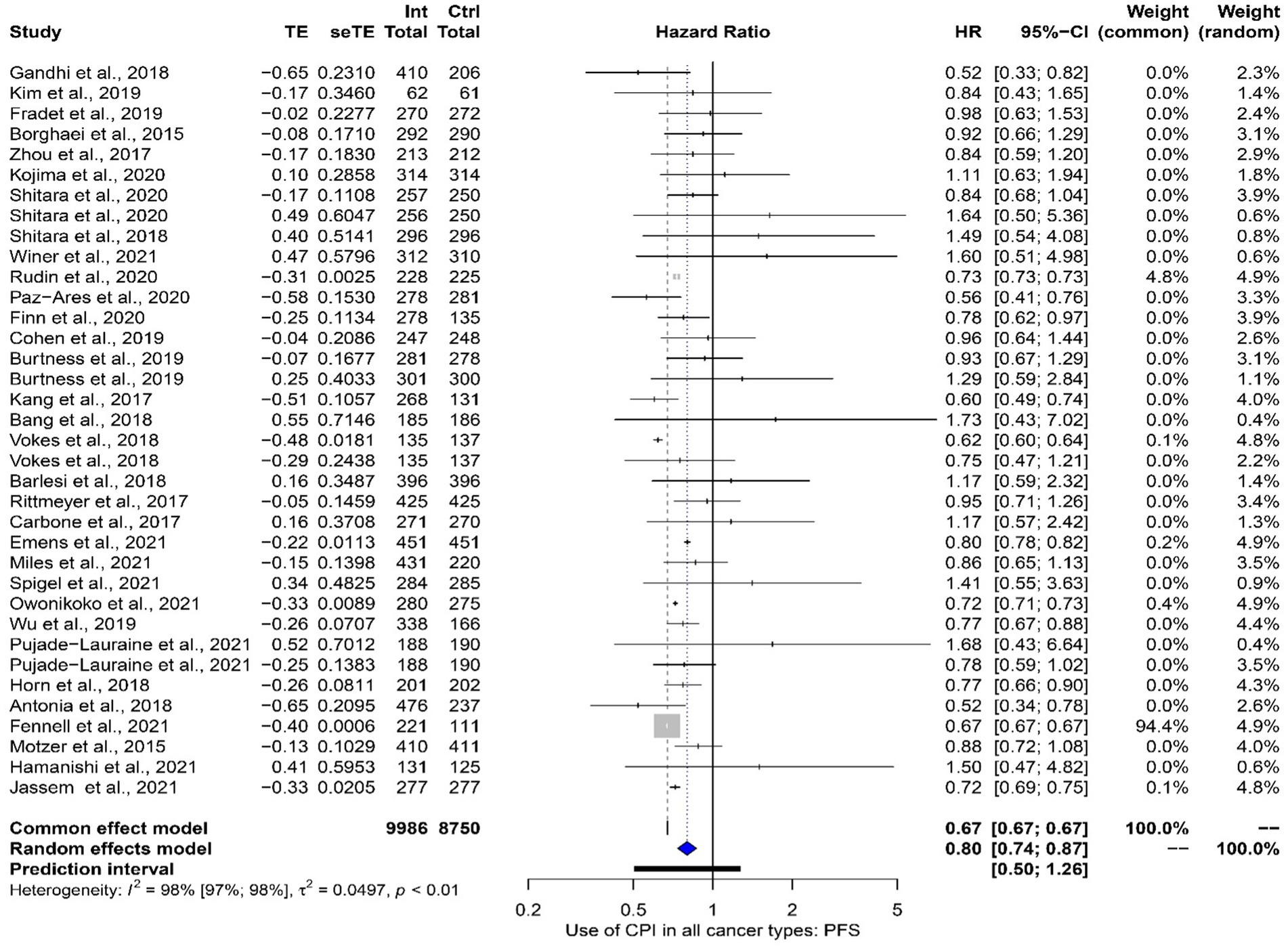
Figure 5. A meta-analysis exploring the impact of ICPIs on progression free survival across all cancer sites.
Cancer site
Studies examining the impact of ICPIs on the PFS of the lung (n = 15), gastro-esophageal junction (n = 6), breast (n = 3), head and neck (n = 2), ovarian (n = 2), liver (n = 1), renal (n = 1), mesothelium (n = 1), and urothelial (n = 1) cancers underwent subgroup analysis to explore the bearing of cancer site on the impact of ICPIs on PFS. Of those in which a meta-analysis was possible, only lung cancers showed a significant improvement in PFS. Looking at lung cancer in more detail, non-small cell studies (n = 11) reported a significant improvement [HR 0.73 (95% CI 0.63–0.85)] in PFS with ICPI use. Studies reporting small cell lung cancers (n = 4) also reached significance [HR 0.76 (95% CI 0.59–0.97)]. These data are shown in Supplementary Figures S9, S10.
Disease specific characteristics
Progression free survival was significantly improved using ICPIs in the primary presentation setting [HR 0.78 (95% CI 0.71–0.86)] however, although there was a trend to improvement in the recurrence setting it did not reach significance [HR 0.85 (95% CI 0.71–1.02)]. These data are outlined in Supplementary Figure S11. PFS was improved with the use of ICPIs in both studies reporting participants who had and had not responded to primary routine treatment {[HR 0.78 (95% CI 0.67–0.89)] and [HR 0.81 (95% CI 0.73–0.91)] respectively – see Supplementary Figure S12}. As seen in OS, the degree of PD-L1 expression did not greatly impact on PFS {[majority PD-L1 HR 0.83 (95% CI 0.71–0.97) vs. minority PD-L1 HR 0.78 (95% CI 0.71 to 0.87)] – see Figure S13}. This is explored in more detail in Supplementary material section 1.5.
Treatment characteristics
Regarding specific ICPI use, the PFS mirrored OS with Nivolumab demonstrating the greatest impact [HR 0.75 (95% CI 0.65–0.87)] and Avelumab failing to reach significance [HR 0.97 (95% CI 0.57–1.67)] as shown in Supplementary Figure S14. PFS only showed a significant improvement in the meta-analysis single agent studies [HR 0.78 (95% CI 0.71–0.86)]. In combination ICPI therapy there was a trend toward improved PFS, however this failed to reach significance [HR 0.86 (95% 0.70–1.06)]. Single agent studies had a higher heterogenicity (I2 98%) compared with studies with that explored multiple agent use (I2 45%). These data are shown in Supplementary Figure S15.
Study characteristics
Subgroup analysis demonstrated that overall PFS was improved by ICPI use in studies judged to be high and low bias [HR 0.80 (95% CI 0.74–0.86)]. However, low bias studies demonstrated a greater effect (HR 0.73 vs. 0.85) but with a higher heterogenicity (I2 99% vs. 77%). These data are summarized in Supplementary Figure S16. Studies that compared ICPIs with placebo found a significant improvement in PFS [HR 0.65 (95% CI 0.56–0.76)]. In the meta-analysis of ICPIs compared to standard treatment, a significant but less pronounced improvement was seen [HR 0.83 (95% CI 0.77–0.90)]. Five studies made up the placebo meta-analysis (32, 33, 37, 47, 54). These data are shown in Supplementary Figure S17.
Side effect profile
Overall, a significantly improved side effect profile with ICPI use however was demonstrated [RR 0.80 (95% CI 0.68–0.95)]. A summary meta-analysis is shown in Figure 6 and described in more detail in Supplementary material section 1.4. It should be noted the former side effects were only reported by a few studies.

Figure 6. Summary forest plot showing the meta-analysis of reported side effects when comparing ICPI use vs standard treatment/placebo in all cancers.
Quality of life outcomes
Too few studies reported quality of life outcomes for a meta-analysis or an informative narrative analysis. Only Pujade-Lauraine et al. made specific reference to quality-of-life outcomes, stating that “treatment related symptom burden was generally similar across all groups” (40).
Discussion
Immune checkpoint inhibitors are considered tumor-agnostic therapies (60). However, to date, their efficacy has only been studied in RCTs in single tumor sites with limited attempts to describe their therapeutic effect across multiple cancer sites. Furthermore, PD-L1 has been accepted as the biomarker of choice for directing IPCI therapy without any pan-cancer level analysis. To the authors’ knowledge, here we present the most comprehensive review of ICPI use as a tumor-agnostic treatment. We found the use of ICPIs lead to improved survival outcomes across numerous tumor sites with limited toxicity. This was most pronounced in lung, head and neck and gastro-esophageal junction cancers. Our data would suggest the use of ICPI is most effective in the primary treatment setting however it was still beneficial in recurrent disease. Furthermore, ICPI are of benefit in those who have, and have not responded to first line treatment. These findings do not seem to be influenced by the number of ICPIs or the specific ICPI that is used. Finally, PD-L1 as a biomarker of ICPI treatment efficacy would seem problematic.
The variation in ICPI efficacy by cancer site that is seen within our data can be explained mechanistically. ICPIs prevents tumor escape through the PD1/PD-L1 axis which is commonly utilized by cancers with a high mutational burden, as these malignancies express high levels of neoantigens that stimulate a cytotoxic immune response (7, 61) We observed an improved ICPI efficacy in lung, head and neck and gastro-esophageal junction cancers which all have a relatively high mutational burden (62). The improved immunotherapeutic effect in non-small cell lung cancer is well documented (63) and was seen in our data; these cancers also have a hypermutated phenotype (62). Furthermore, we noted primary metastatic cancers had a better response ICPIs; again, metastatic disease is known to have a high mutational burden (64).
Not all studies reported a favorable outcome. Bang et al. (23), Carbone et al. (27), and Miles et al. (35) reported no significant improvement in survival. These outliers can be explained by methodological issues within the studies. Bang et al. stained for PD-L1 with several different antibodies. Of note, subgroup analysis found those cases in which 22C3 antibodies were used for defining PD-L1 expression had better survival outcomes (65); this could speak to a methodological issue rather than a true negative result. Carbone et al. suffered from significant treatment cross over with over 60% of their control group receiving an ICPI. Mature survival data from Miles et al. did find that ICPI use was associated with an improved survival (66).
The use of biomarkers to direct treatment is a tenant of personalized therapy. We explored the effect of using PD-L1 as a biomarker for ICPI use. In studies in which the authors had preselected their treatment cohort based on positive PD-L1 expression, an improved OS HR was noted. However, in head-to-head comparison between studies in which most cancers had a high PD-L1 expression vs. those with a minority where PD-L1 positive, our analysis would indicate that using PD-L1 as a ICPI treatment biomarker was of deleterious effect, although this did not reach significance. Given these data are not consistent it may suggest PD-L1 may not be as reliable a predictor of ICPI effectiveness as commonly held. The immunohistochemistry for PD-L1 is known to be difficult and often open to high levels of result inconsistency (67–69). Issues with fixation, antibody binding, clonal expression, and interpretation are established issues (70, 71) The included studies within this meta-analysis used a range of immunohistochemical platforms, antibodies, scoring methods, thresholds and number of pathologists involved in forming a consensus opinion. This therefore reflects the real word situation in which PD-L1 testing and scoring is heterogeneous (72). The authors therefore recommend that PD-L1 is not preferentially used as to direct ICPI treatment as it does not seem to improve survival outcomes. Other biomarkers, with higher levels of test consistency, such as TMB and or MMRd either via immunohistochemistry or MSI testing should be explored as potential biomarkers. Meta-analysis exploring the utility of TMB as a biomarker of ICPI treatment concluded it led to a significant improvement in survival outcomes, however this analysis relied on retrospective trial data (73). Tumor mutational analysis has been used to direct ICPI treatment in trials and has been shown to predict significantly improved survival outcomes (73). We were unable to do this in this meta-analysis due to a lack of study data; only one RCT used tumor mutational burden prospectively in our analysis (39).
To put our work in context, Sun et al. published a systematic review and meta-analysis on ICPI use in advanced and metastatic cancers including 35 studies in adult and non-adult populations (13). They too found potential issues with PD-L1 as a biomarker for directing ICPI use, however they were unable to draw clear conclusions do to methodological issues. Studies included in this analysis included trials with ICPIs and other biological treatments which makes conclusions on ICPI effect difficult. Subgroup analyses within this work relied on small numbers. In addition, this meta-analysis included a large proportion of melanomas (8%); these cancers are known to demonstrate consistently high PD-L1 expression and therefore could impact on the conclusions of PD-L1 as a biomarker of ICPI efficacy in other cancer sites (74). Overall response rate was included in their analysis, and as noted by the authors, such a measure is thought unhelpful in immunotherapy as cancers often demonstrate a pseudo-progression on ICPI as they increase in size secondary to immune infiltrate (75). Finally, the inclusion of phase II trials is problematic as these studies tend to be underpowered to explore survival outcomes and present immature data which add to the heterogeneity of analysis and make summary statistics more problematic (76). Therefore, our work does add to the current knowledgebase given it applies a more robust inclusion/exclusion criteria and more mature survival data.
A strength of our work is it followed PRISMA guidance throughout (17). Our thorough search and screening lead to the inclusion of 37 phase III randomized control trials for our meta-analysis. This has enabled a comprehensive summary of the current evidence and enabled robust conclusions as to the clinical efficacy of ICPIs across numerous tumor sites and populations. Furthermore, we limited subgroup analysis to remain within our published protocol. These subgroups were comprised of large cohorts of study subjects giving reliability to the analysis. In addition, throughout the meta-analysis, multiple sensitivity studies were conducted to ensure the robustness of results.
Our work is not without its limitations. We used study level data as our attempts to contact authors to collect individual level data were unsuccessful. Furthermore, most studies included in this analysis were not free from methodological bias. We recognize the studies included in this meta-analysis are heterogeneous; the effects of this were mitigated by the use random effects modeling. However, meaningful comparisons in heterogeneous data can be difficult. Of note, because of the available studies, there is a predominance of lung cancers, the use of Pembrolizumab and North American populations which could impact on the generalizability of this meta-analysis and its conclusions. In addition, we were unable to include studies without an English translation which introduces selection bias within our study. In addition, there are several studies that have or are due to publish exploring ICPI use in novel cancer sites that had not published at the time of our search; these are therefore not included in this analysis. These factors, individually and combined, decrease the reliability of this analysis. However, even with these limitations, our work remains the most comprehensive meta-analysis of ICPI use in solid cancers published to date.
We did not include melanomas in this study. This was to reduce the confounding effect of their inclusion on this analysis; melanomas have an excellent response to ICPIs which is well established (18). In addition, the staining for PD-L1 has been extensively explored in this cancer meaning that PD-L1 interpretation benefits from established protocols (77, 78). PD-L1 is often expressed at high levels in melanoma which also aids in the interpretation of this biomarker in a way that is not so in other cancer sites (77–79). Therefore, through the exclusion of melanomas, our meta-analysis can better explore the impact of ICPIs in non-melanoma solid cancers which we believe have distinct clinical characteristics. However, we recognize it does mean the findings of this study cannot be applied to melanomas.
Conclusion
In conclusion, herein we present the most comprehensive review of ICPIs as a tumor agnostic therapy. These data confirm that their use improves survival outcomes across a range of tumor sites and are well tolerated. This benefit is seen regardless of specific ICPI used, whether in primary or recurrent disease and where there had and had not been a good response to primary treatment. Of note, the use of PD-L1 immunohistochemistry to direct ICPI use would seem potentially problematic and other biomarkers such as TMB or mismatch repair status should be explored in more depth. In addition, trials should be conducted in cancers that have been so far under investigated.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
TF, NS, TW and NR contributed to the data acquisition, data interpretation and data analysis. NR drafted the manuscript. All authors contributed to the literature search, study concept and design, and critical revision to the manuscript.
Funding
EC was supported by the NIHR Manchester Biomedical Research Centre (IS-BRC-1215-2007) and an NIHR advanced fellowship (NIHR300650). DE is an NIHR Senior Investigator (NF-SI-0513-10076).
Acknowledgments
We would like to thank the medical library at the University of Bristol for their support with this work.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2023.1192762/full#supplementary-material
Abbreviations
CI, confidence Interval; FDA, Federal Drug Administration; HMB, high mutational burden; HR, hazard ratio; ICPI, immune checkpoint inhibitors; MSI, microsatellite instability; OS, overall survival; PD-1, programmed death 1; PD-L1, programmed death-ligand 1; PFS, progression free survival; PRISMA, preferred reporting items for systematic reviews and meta-analyses; RCT, randomized control trial; RE, random effects; RR, risk ratio; SE, standard error.
Footnotes
References
1. GBD 2017 Causes of Death Collaborators. Global, regional, And national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1736–88. doi: 10.1016/s0140-6736(18)32203-7
2. Nagai, H, and Kim, YH. Cancer prevention from the perspective of global cancer burden patterns. J Thorac Dis. (2017) 9:448–51. doi: 10.21037/jtd.2017.02.75
3. Gerber, DE. Targeted therapies: a new generation of cancer treatments. Am Fam Physician. (2008) 77:311–9. Available at: https://pubmed.ncbi.nlm.nih.gov/18297955/
4. Pardoll, DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. (2012) 12:252–64. doi: 10.1038/nrc3239
5. le, DT, Uram, JN, Wang, H, Bartlett, BR, Kemberling, H, Eyring, AD, et al. PD-1 blockade in tumors with mismatch-repair deficiency. N Engl J Med. (2015) 372:2509–20. doi: 10.1056/nejmoa1500596
6. Keir, ME, Butte, MJ, Freeman, GJ, and Sharpe, AH. PD-1 and its ligands in tolerance and immunity. Annu Rev Immunol. (2008) 26:677–704. doi: 10.1146/annurev.immunol.26.021607.090331
7. Ramchander, NC, Ryan, NAJ, Walker, TDJ, Harries, L, Bolton, J, Bosse, T, et al. Distinct immunological landscapes characterize inherited and sporadic mismatch repair deficient endometrial Cancer. Front Immunol. (2020) 10:3023. doi: 10.3389/fimmu.2019.03023
8. Nair, VS, and Elkord, E. Immune checkpoint inhibitors in cancer therapy: a focus on T-regulatory cells. Immunol Cell Biol. (2017) 96:21–33. doi: 10.1111/imcb.1003
9. Thallinger, C, Füreder, T, Preusser, M, Heller, G, Müllauer, L, Höller, C, et al. Review of cancer treatment with immune checkpoint inhibitors. Wien Klin Wochenschr. (2018) 130:85–91. doi: 10.1007/s00508-017-1285-9
10. Marcus, L, Lemery, SJ, Keegan, P, and Pazdur, R. FDA approval summary: Pembrolizumab for the treatment of microsatellite instability-high solid tumors. Clin Cancer Res Official J Am Assoc Cancer Res. (2019) 25:3753–8. doi: 10.1158/1078-0432.ccr-18-4070
11. Sha, D, Jin, Z, Budczies, J, Kluck, K, Stenzinger, A, and Sinicrope, FA. Tumor mutational burden as a predictive biomarker in solid tumors. Cancer Discov. (2020) 10:1808–25. doi: 10.1158/2159-8290.cd-20-0522
12. Twomey, JD, and Zhang, B. Cancer immunotherapy update: FDA-approved checkpoint inhibitors and companion diagnostics. AAPS J. (2021) 23:39. doi: 10.1208/s12248-021-00574-0
13. Sun, L, Zhang, L, Yu, J, Zhang, Y, Pang, X, Ma, C, et al. Clinical efficacy and safety of anti-PD-1/PD-L1 inhibitors for the treatment of advanced or metastatic cancer: a systematic review and meta-analysis. Sci Rep. (2020) 10:2083. doi: 10.1038/s41598-020-58674-4
14. Robert, C. A decade of immune-checkpoint inhibitors in cancer therapy. Nat Commun. (2020) 11:3801. doi: 10.1038/s41467-020-17670-y
15. Larkin, J, Chiarion-Sileni, V, Gonzalez, R, Grob, JJ, Rutkowski, P, Lao, CD, et al. Five-year survival with combined Nivolumab and Ipilimumab in advanced melanoma. New Engl J Med. (2019) 381:1535–46. doi: 10.1056/nejmoa1910836
16. Haslam, A, and Prasad, V. Estimation of the percentage of US patients with Cancer who are eligible for and respond to checkpoint inhibitor immunotherapy drugs. JAMA Netw Open. (2019) 2:e192535. doi: 10.1001/jamanetworkopen.2019.2535
17. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
18. Huang, AC, and Zappasodi, R. A decade of checkpoint blockade immunotherapy in melanoma: understanding the molecular basis for immune sensitivity and resistance. Nat Immunol. (2022) 23:660–70. doi: 10.1038/s41590-022-01141-1
19. Shemilt, I, Aluko, P, Graybill, E, Craig, D, Henderson, C, Drummond, M, et al. Cochrane handbook for systematic reviews of interventions. The Cochrane Collaboration and John Wiley & Sons Ltd. (2019) 507–523
20. Balduzzi, S, Rücker, G, and Schwarzer, G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Heal. (2019) 22:153–60. doi: 10.1136/ebmental-2019-300117
21. Wickham, H, Averick, M, Bryan, J, Chang, W, McGowan, L, François, R, et al. Welcome to the Tidyverse. J Open Source Softw. (2019) 4:1686. doi: 10.21105/joss.01686
22. Viechtbauer, W. Conducting Meta-analyses in R with the metafor package. J Stat Softw. (2010) 36:1–42. doi: 10.18637/jss.v036.i03
23. Bang, YJ, Ruiz, EY, van Cutsem, E, Lee, KW, Wyrwicz, L, Schenker, M, et al. Phase III, randomised trial of avelumab versus physician’s choice of chemotherapy as third-line treatment of patients with advanced gastric or gastro-oesophageal junction cancer: primary analysis of JAVELIN gastric 300. Ann Oncol. (2018) 29:2052–60. doi: 10.1093/annonc/mdy264
24. Barlesi, F, Vansteenkiste, J, Spigel, D, Ishii, H, Garassino, M, de Marinis, F, et al. Avelumab versus docetaxel in patients with platinum-treated advanced non-small-cell lung cancer (JAVELIN lung 200): an open-label, randomised, phase 3 study. Lancet Oncol. (2018) 19:1468–79. doi: 10.1016/s1470-2045(18)30673-9
25. Borghaei, H, Paz-Ares, L, Horn, L, Spigel, DR, Steins, M, Ready, NE, et al. Nivolumab versus docetaxel in advanced nonsquamous non–small-cell lung Cancer. New Engl J Med. (2015) 373:1627–39. doi: 10.1056/nejmoa1507643
26. Burtness, B, Harrington, KJ, Greil, R, Soulières, D, Tahara, M, de Castro, G Jr, et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet. (2019) 394:1915–28. doi: 10.1016/s0140-6736(19)32591-7
27. Carbone, DP, Reck, M, Paz-Ares, L, Creelan, B, Horn, L, Steins, M, et al. First-line Nivolumab in stage IV or recurrent non-small-cell lung Cancer. New Engl J Medicine. (2017) 376:2415–26. doi: 10.1056/nejmoa1613493
28. Cohen, EEW, Soulières, D, le Tourneau, C, Dinis, J, Licitra, L, Ahn, MJ, et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): a randomised, open-label, phase 3 study. Lancet. (2019) 393:156–67. doi: 10.1016/s0140-6736(18)31999-8
29. Emens, LA, Adams, S, Barrios, CH, Diéras, V, Iwata, H, Loi, S, et al. First-line atezolizumab plus nab-paclitaxel for unresectable, locally advanced, or metastatic triple-negative breast cancer: IMpassion130 final overall survival analysis. Ann Oncol. (2021) 32:983–93. doi: 10.1016/j.annonc.2021.05.355
30. Ferris, RL, Blumenschein, G, Fayette, J, Guigay, J, Colevas, AD, Licitra, L, et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med. (2016) 375:1856–67. doi: 10.1056/nejmoa1602252
31. Finn, RS, Ryoo, BY, Merle, P, Kudo, M, Bouattour, M, Lim, HY, et al. Pembrolizumab As second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: a randomized, double-blind, phase III trial. J Clin Oncol Official J Am Soc Clin Oncol. (2019) 38:193–202. doi: 10.1200/jco.19.01307
32. Gandhi, L, Rodríguez-Abreu, D, Gadgeel, S, Esteban, E, Felip, E, de Angelis, F, et al. Pembrolizumab plus chemotherapy in metastatic non–small-cell lung Cancer. New Engl J Med. (2018) 378:2078–92. doi: 10.1056/nejmoa1801005
33. Kang, YK, Boku, N, Satoh, T, Ryu, MH, Chao, Y, Kato, K, et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. (2017) 390:2461–71. doi: 10.1016/s0140-6736(17)31827-5
34. Kojima, T, Shah, MA, Muro, K, Francois, E, Adenis, A, Hsu, CH, et al. Randomized phase III KEYNOTE-181 study of Pembrolizumab versus chemotherapy in advanced esophageal Cancer. J Clin Oncol Official J Am Soc Clin Oncol. (2020) 38:4138–48. doi: 10.1200/jco.20.01888
35. Miles, D, Gligorov, J, André, F, Cameron, D, Schneeweiss, A, Barrios, C, et al. Primary results from IMpassion131, a double-blind, placebo-controlled, randomised phase III trial of first-line paclitaxel with or without atezolizumab for unresectable locally advanced/metastatic triple-negative breast cancer. Ann Oncol. (2021) 32:994–1004. doi: 10.1016/j.annonc.2021.05.801
36. Mok, TSK, Wu, YL, Kudaba, I, Kowalski, DM, Cho, BC, Turna, HZ, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet Lond Engl. (2019) 393:1819–30. doi: 10.1016/s0140-6736(18)32409-7
37. Owonikoko, TK, Park, K, Govindan, R, Ready, N, Reck, M, Peters, S, et al. Nivolumab and Ipilimumab as maintenance therapy in extensive-disease small-cell lung Cancer: CheckMate 451. J Clin Oncol. (2021) 39:1349–59. doi: 10.1200/jco.20.02212
38. Paz-Ares, L, Luft, A, Vicente, D, Tafreshi, A, Gümüş, M, Mazières, J, et al. Pembrolizumab plus chemotherapy for squamous non–small-cell lung Cancer. New Engl J Med. (2018) 379:2040–51. doi: 10.1056/nejmoa1810865
39. Powles, T, Durán, I, van der, HMS, van der Heijden, MS, Loriot, Y, Vogelzang, NJ, et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): a multicentre, open-label, phase 3 randomised controlled trial. Lancet. (2018) 391:748–57. doi: 10.1016/s0140-6736(17)33297-x
40. Pujade-Lauraine, E, Fujiwara, K, Ledermann, JA, Oza, AM, Kristeleit, R, Ray-Coquard, IL, et al. Avelumab alone or in combination with chemotherapy versus chemotherapy alone in platinum-resistant or platinum-refractory ovarian cancer (JAVELIN ovarian 200): an open-label, three-arm, randomised, phase 3 study. Lancet Oncol. (2021) 22:1034–46. doi: 10.1016/s1470-2045(21)00216-3
41. Reck, M, Rodríguez-Abreu, D, Robinson, AG, Hui, R, Csőszi, T, Fülöp, A, et al. Pembrolizumab versus chemotherapy for PD-L1–positive non–small-cell lung Cancer. N Engl J Med. (2016) 375:1823–33. doi: 10.1056/nejmoa1606774
42. Rittmeyer, A, Barlesi, F, Waterkamp, D, Park, K, Ciardiello, F, von Pawel, J, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet. (2017) 389:255–65. doi: 10.1016/s0140-6736(16)32517-x
43. Rudin, CM, Awad, MM, Navarro, A, Gottfried, M, Peters, S, Csőszi, T, et al. Pembrolizumab or placebo plus etoposide and platinum as first-line therapy for extensive-stage small-cell lung Cancer: randomized, double-blind, phase III KEYNOTE-604 study. J Clin Oncol. (2020) 38:2369–79. doi: 10.1200/jco.20.00793
44. Shitara, K, van Cutsem, E, Bang, YJ, Fuchs, C, Wyrwicz, L, Lee, KW, et al. Efficacy and safety of Pembrolizumab or Pembrolizumab plus chemotherapy vs chemotherapy alone for patients with first-line, advanced gastric Cancer. JAMA Oncol. (2020) 6:1571–80. doi: 10.1001/jamaoncol.2020.3370
45. Shitara, K, Özgüroğlu, M, Bang, YJ, di Bartolomeo, M, Mandalà, M, Ryu, MH, et al. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): a randomised, open-label, controlled, phase 3 trial. Lancet. (2018) 392:123–33. doi: 10.1016/s0140-6736(18)31257-1
46. Spigel, DR, Vicente, D, Ciuleanu, TE, Gettinger, S, Peters, S, Horn, L, et al. Second-line nivolumab in relapsed small-cell lung cancer: check mate 331. Ann Oncol Official J European Soc Medical Oncol. (2021) 32:631–41. doi: 10.1016/j.annonc.2021.01.071
47. Vokes, EE, Ready, N, Felip, E, Horn, L, Burgio, MA, Antonia, SJ, et al. Nivolumab versus docetaxel in previously treated advanced non-small-cell lung cancer (check mate 017 and check mate 057): 3-year update and outcomes in patients with liver metastases. Ann Oncol. (2018) 29:959–65. doi: 10.1093/annonc/mdy041
48. Winer, EP, Lipatov, O, Im, SA, Goncalves, A, Muñoz-Couselo, E, Lee, KS, et al. Pembrolizumab versus investigator-choice chemotherapy for metastatic triple-negative breast cancer (KEYNOTE-119): a randomised, open-label, phase 3 trial. Lancet Oncol. (2021) 22:499–511. doi: 10.1016/s1470-2045(20)30754-3
49. Wu, YL, Lu, S, Cheng, Y, Zhou, C, Wang, J, Mok, T, et al. Nivolumab versus docetaxel in a predominantly Chinese patient population with previously treated advanced NSCLC: CheckMate 078 randomized phase III clinical trial. J Thorac Oncol. (2019) 14:867–75. doi: 10.1016/j.jtho.2019.01.006
50. NCT02864394. Study of pembrolizumab versus docetaxel in participants previously treated for non-small cell lung Cancer (MK-3475-033/KEYNOTE-033) (2022). Available at: https://clinicaltrials.gov/ct2/show/NCT02864394 (Accessed December 17, 2021).
51. NCT03933449. Study of pembrolizumab (MK-3475) versus investigator’s choice of chemotherapy for participants with advanced esophageal/esophagogastric junction carcinoma that progressed after first-line therapy (MK-3475-181/KEYNOTE-181)-China extension study. (2019). Available at: https://clinicaltrials.gov/ct2/show/NCT03933449 (Accessed December 17, 2021)
52. Fradet, Y, Bellmunt, J, Vaughn, DJ, Lee, JL, Fong, L, Vogelzang, NJ, et al. Randomized phase III KEYNOTE-045 trial of pembrolizumab versus paclitaxel, docetaxel, or vinflunine in recurrent advanced urothelial cancer: results of > 2 years of follow-up. Ann Oncol. (2019) 30:970–6. doi: 10.1093/annonc/mdz127
53. Antonia, SJ, Villegas, A, Daniel, D, Vicente, D, Murakami, S, Hui, R, et al. Overall survival with Durvalumab after Chemoradiotherapy in stage III NSCLC. New Engl J Med. (2018) 379:2342–50. doi: 10.1056/nejmoa1809697
54. Fennell, DA, Ewings, S, Ottensmeier, C, Califano, R, Hanna, GG, Hill, K, et al. Nivolumab versus placebo in patients with relapsed malignant mesothelioma (CONFIRM): a multicentre, double-blind, randomised, phase 3 trial. Lancet Oncol. (2021) 22:1530–40. doi: 10.1016/s1470-2045(21)00471-x
55. Hamanishi, J, Takeshima, N, Katsumata, N, Ushijima, K, Kimura, T, Takeuchi, S, et al. Nivolumab versus gemcitabine or Pegylated liposomal doxorubicin for patients with platinum-resistant ovarian Cancer: open-label, randomized trial in Japan (NINJA). J Clin Oncol. (2021) 39:3671–81. doi: 10.1200/jco.21.00334
56. Horn, L, Mansfield, AS, Szczęsna, A, Havel, L, Krzakowski, M, Hochmair, MJ, et al. First-line Atezolizumab plus chemotherapy in extensive-stage small-cell lung Cancer. New Engl J Medicine. (2018) 379:2220–9. doi: 10.1056/nejmoa1809064
57. Jassem, J, de Marinis, F, Giaccone, G, Vergnenegre, A, Barrios, CH, Morise, M, et al. Updated overall survival analysis from IMpower110: Atezolizumab versus platinum-based chemotherapy in treatment-naive programmed death-ligand 1–selected NSCLC. J Thorac Oncol. (2021) 16:1872–82. doi: 10.1016/j.jtho.2021.06.019
58. Motzer, RJ, Rini, BI, McDermott, DF, Redman, BG, Kuzel, TM, Harrison, MR, et al. Nivolumab for metastatic renal cell carcinoma: results of a randomized phase II trial. JCO. (2015) 33:1430–7. doi: 10.1200/jco.2014.59.0703
59. Wu, YL, Zhang, L, Fan, Y, Zhou, J, Zhang, L, Zhou, Q, et al. Randomized clinical trial of pembrolizumab vs chemotherapy for previously untreated Chinese patients with PD-L1-positive locally advanced or metastatic non-small-cell lung cancer: KEYNOTE-042 China study. Int J Cancer. (2020) 148:2313–20. doi: 10.1002/ijc.33399
60. Looney, AM, Nawaz, K, and Webster, RM. Tumour-agnostic therapies. Nat Rev Drug Discov. (2020) 19:383–4. doi: 10.1038/d41573-020-00015-1
61. Rousseau, B, Foote, MB, Maron, SB, Diplas, BH, Lu, S, Argilés, G, et al. The Spectrum of benefit from checkpoint blockade in Hypermutated tumors. N Engl J Med. (2021) 384:1168–70. doi: 10.1056/nejmc2031965
62. Alexandrov, LB, Kim, J, Haradhvala, NJ, Huang, MN, Tian Ng, AW, Wu, Y, et al. The repertoire of mutational signatures in human cancer. Nature. (2020) 578:94–101. doi: 10.1038/s41586-020-1943-3
63. Thai, AA, Solomon, BJ, Sequist, LV, Gainor, JF, and Heist, RS. Lung cancer. Lancet. (2021) 398:535–54. doi: 10.1016/s0140-6736(21)00312-3
64. Schnidrig, D, Turajlic, S, and Litchfield, K. Tumour mutational burden: primary versus metastatic tissue creates systematic bias. Immuno Oncol Technol. (2019) 4:8–14. doi: 10.1016/j.iotech.2019.11.003
65. Moehler, M, Dvorkin, M, Boku, N, Özgüroğlu, M, Ryu, MH, Muntean, AS, et al. Phase III trial of Avelumab maintenance after first-line induction chemotherapy versus continuation of chemotherapy in patients with gastric cancers: results from JAVELIN gastric 100. J Clin Oncol. (2021) 39:966–77. doi: 10.1200/jco.20.00892
66. Emens, LA, Adams, S, Barrios, CH, Dieras, VC, Iwata, H, Loi, S, et al. IMpassion130: final OS analysis from the pivotal phase III study of atezolizumab + nab-paclitaxel vs placebo + nab-paclitaxel in previously untreated locally advanced or metastatic triple-negative breast cancer. Ann Oncol. (2020) 31:S1148. doi: 10.1016/j.annonc.2020.08.2244
67. Ruiter, EJde, Mulder, FJ, Koomen, BM, Speel, EJ, van den Hout, MFCM, de Roest, RH, et al. Comparison of three PD-L1 immunohistochemical assays in head and neck squamous cell carcinoma (HNSCC). Mod Pathol Official J United States Can Acad Pathology Inc (2020) 34: 1125–1132. doi: 10.1038/s41379-020-0644-7
68. Hutarew, G. PD-L1 testing, fit for routine evaluation? From a pathologist’s point of view. Memo-Mag European Medical Oncol. (2016) 9:201–6. doi: 10.1007/s12254-016-0292-2
69. Lou, SK, Ko, HM, Kinoshita, T, MacDonald, S, Weiss, J, Czarnecka-Kujawa, K, et al. Implementation of PD-L1 22C3 IHC pharmDx<sup>TM</sup> in cell block preparations of lung Cancer: concordance with surgical resections and technical validation of CytoLyt® Prefixation. Acta Cytol. (2020) 64:577–87. doi: 10.1159/000508628
70. Jöhrens, K, and Rüschoff, J. The challenge to the pathologist of PD-L1 expression in tumor cells of non-small-cell lung Cancer—an overview. Curr Oncol. (2021) 28:5227–39. doi: 10.3390/curroncol28060437
71. Akhtar, M, Rashid, S, and Al-Bozom, IA. PD-L1 immunostaining: what pathologists need to know. Diagn Pathol. (2021) 16:94. doi: 10.1186/s13000-021-01151-x
72. McLaughlin, J, Han, G, Schalper, KA, Carvajal-Hausdorf, D, Pelekanou, V, Rehman, J, et al. Quantitative assessment of the heterogeneity of PD-L1 expression in non-small-cell lung Cancer. JAMA Oncol. (2016) 2:46–54. doi: 10.1001/jamaoncol.2015.3638
73. Kim, JY, Kronbichler, A, Eisenhut, M, Hong, SH, van der Vliet, HJ, Kang, J, et al. Tumor mutational burden and efficacy of immune checkpoint inhibitors: a systematic review and Meta-analysis. Cancers. (2019) 11:1798. doi: 10.3390/cancers11111798
74. Kuryk, L, Bertinato, L, Staniszewska, M, Pancer, K, Wieczorek, M, Salmaso, S, et al. From conventional therapies to immunotherapy: melanoma treatment in review. Cancers. (2020) 12:3057. doi: 10.3390/cancers12103057
75. Ozaki, Y, Shindoh, J, Miura, Y, Nakajima, H, Oki, R, Uchiyama, M, et al. Serial pseudoprogression of metastatic malignant melanoma in a patient treated with nivolumab: a case report. BMC Cancer. (2017) 17:778. doi: 10.1186/s12885-017-3785-4
76. Korn, EL, Liu, PY, Lee, SJ, Chapman, JAW, Niedzwiecki, D, Suman, VJ, et al. Meta-analysis of phase II cooperative group trials in metastatic stage IV melanoma to determine progression-free and overall survival benchmarks for future phase II trials. J Clin Oncol. (2008) 26:527–34. doi: 10.1200/jco.2007.12.7837
77. Madore, J, Vilain, RE, Menzies, AM, Kakavand, H, Wilmott, JS, Hyman, J, et al. PD-L1 expression in melanoma shows marked heterogeneity within and between patients: implications for anti-PD-1/PD-L1 clinical trials. Pigm Cell Melanoma R. (2014) 28:245–53. doi: 10.1111/pcmr.12340
78. O'Malley, DP, Yang, Y, Boisot, S, Sudarsanam, S, Wang, JF, Chizhevsky, V, et al. Immunohistochemical detection of PD-L1 among diverse human neoplasms in a reference laboratory: observations based upon 62,896 cases. Mod Pathol. (2019) 32:929–42. doi: 10.1038/s41379-019-0210-3
Keywords: pan-cancer therapy, checkpoint immune blockade antibodies, PDL1, mismatch repair, oncology, immunotherapy
Citation: Fitzsimmons TS, Singh N, Walker TDJ, Newton C, Evans DGR, Crosbie EJ and Ryan NAJ (2023) Immune checkpoint inhibitors efficacy across solid cancers and the utility of PD-L1 as a biomarker of response: a systematic review and meta-analysis. Front. Med. 10:1192762. doi: 10.3389/fmed.2023.1192762
Edited by:
Heping Yang, Cedars-Sinai Medical Center, United StatesReviewed by:
Man Jiang, The Affiliated Hospital of Qingdao University, ChinaBing Yang, Cedars-Sinai Medical Center, United States
Copyright © 2023 Fitzsimmons, Singh, Walker, Newton, Evans, Crosbie and Ryan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Timothy S. Fitzsimmons, dGltZml0enNpbW1vbnMyMTAxQGljbG91ZC5jb20=; Niharika Singh, bmloYXJpa2FzaW5naHVrQGxpdmUuY28udWs=; Neil A. J. Ryan, bmVpbC5yeWFuQGVkLmFjLnVr; Emma J. Crosbie, RW1tYS5jcm9zYmllQG1hbmNoZXN0ZXIuYWMudWs=
†These authors share first authorship