
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 21 June 2023
Sec. Infectious Diseases: Pathogenesis and Therapy
Volume 10 - 2023 | https://doi.org/10.3389/fmed.2023.1182359
This article is part of the Research Topic New Frontiers in HIV Antiretroviral Treatment: From the Management of Metabolic Complications and Chronic Inflammation to New Long-Acting Regimens View all 5 articles
 Raquel Martín-Iguacel1,2*†
Raquel Martín-Iguacel1,2*† Mari Carmen Vazquez-Friol3†Joaquin Burgos4Andreu Bruguera1,5,6Juliana Reyes-Urueña1Sergio Moreno-Fornés1,5Jordi Aceitón1Yesika Díaz1
Mari Carmen Vazquez-Friol3†Joaquin Burgos4Andreu Bruguera1,5,6Juliana Reyes-Urueña1Sergio Moreno-Fornés1,5Jordi Aceitón1Yesika Díaz1 Pere Domingo7Maria Saumoy8Hernando Knobel9David Dalmau10Beatriz Borjabad11
Pere Domingo7Maria Saumoy8Hernando Knobel9David Dalmau10Beatriz Borjabad11 Isik Somuncu Johansen2Jose M. Miro12,13Jordi Casabona1,5,6,14Josep M. Llibre15,16* on behalf of the PISCIS study group
Isik Somuncu Johansen2Jose M. Miro12,13Jordi Casabona1,5,6,14Josep M. Llibre15,16* on behalf of the PISCIS study groupObjectives: People with HIV (PWH) have a higher cardiovascular risk than the general population. It remains unclear, however, whether the risk of cardiovascular disease (CVD) is higher in late HIV presenters (LP; CD4 ≤ 350 cells/μL at HIV diagnosis) compared to PWH diagnosed early. We aimed to assess the rates of incident cardiovascular events (CVEs) following ART initiation among LP compared to non-LP.
Methods: From the prospective, multicentre PISCIS cohort, we included all adult people with HIV (PWH) initiating antiretroviral therapy (ART) between 2005 and 2019 without prior CVE. Additional data were extracted from public health registries. The primary outcome was the incidence of first CVE (ischemic heart disease, congestive heart failure, cerebrovascular, or peripheral vascular disease). The secondary outcome was all-cause mortality after the first CVE. We used Poisson regression.
Results: We included 3,317 PWH [26 589.1 person/years (PY)]: 1761 LP and 1556 non-LP. Overall, 163 (4.9%) experienced a CVE [IR 6.1/1000PY (95%CI: 5.3–7.1)]: 105 (6.0%) LP vs. 58 (3.7%) non-LP. No differences were observed in the multivariate analysis adjusting for age, transmission mode, comorbidities, and calendar time, regardless of CD4 at ART initiation [aIRR 0.92 (0.62–1.36) and 0.84 (0.56–1.26) in LP with CD4 count <200 and 200– ≤ 350 cells/μL, respectively, compared to non-LP]. Overall mortality was 8.5% in LP versus 2.3% in non-LP (p < 0.001). Mortality after the CVE was 31/163 (19.0%), with no differences between groups [aMRR 1.24 (0.45–3.44)]. Women vs. MSM and individuals with chronic lung and liver disease experienced particularly high mortality after the CVE [aMRR 5.89 (1.35–25.60), 5.06 (1.61–15.91), and 3.49 (1.08–11.26), respectively]. Sensitivity analyses including only PWH surviving the first 2 years yielded similar results.
Conclusion: CVD remains a common cause of morbidity and mortality among PWH. LP without prior CVD did not exhibit an increased long-term risk of CVE compared with non-LP. Identifying traditional cardiovascular risk factors is essential for CVD risk reduction in this population.
Despite absolute rates of cardiovascular disease (CVD) declining significantly over time, people with HIV (PWH) continue to have an ~50% higher relative risk compared with HIV-negative individuals (1). The American Heart Association recommends adjusting the calculated risk estimate upward by 1.5–2 times for PWH on the basis that most risk calculators tend to underestimate their cardiovascular risk (2).
Late HIV diagnosis, defined as CD4 count < 350 cells/μL or AIDS at diagnosis regardless of CD4 count, still represents an unmet need, with half of PWH being diagnosed late. Individuals not belonging to the traditional HIV risk groups, such as heterosexual men, females, older individuals, and migrants, are at a higher risk of late HIV diagnosis (3). Older people are at increased risk of both late HIV diagnosis and CVD, and their proportional rates among PWH are increasing (4).
Late HIV diagnosis has been associated with increased risks of death, AIDS, and non-AIDS comorbidities (5, 6). The risk for AIDS and death is highest in the first year, mainly due to AIDS-related conditions, often present at baseline (3). Factors such as unremitting inflammation potentially related to higher HIV reservoirs and persistent immune activation due to late ART initiation (7), have been associated with premature aging and may predispose to non-AIDS comorbidities (8). However, their link with CVD in this scenario has not been proven, and the understanding of the subsequent CV risk in late presenters (LPs) is incomplete. Furthermore, additional factors other than low CD4 cell count and chronic inflammation may also contribute to the disparity in long-term morbidity and mortality in LP such as differences in access and adherence to care (9, 10), behavioral factors such as smoking (11), the burden of comorbidities, and socio-economic factors. In addition, lower CD4 count led to more conservative surgical approaches to CV complications (12).
While some studies have not found a greater risk of CVD in LP (13–15), others have reported that CD4 count depletion along the course of the HIV disease is associated with a higher risk of CVD. The latter, however, has been mainly described in immunological non-responders after the initiation of ART or in individuals with unsuppressed viremia (16–20).
It is thus uncertain whether the long-term cardiovascular risk in LP who initiate effective ART is higher than in those individuals who were diagnosed early. We aimed to assess the rates of incident CV events following ART initiation among LP in a prospective cohort.
This is a cohort study conducted in Catalonia, Spain. On January 2021, Catalonia had a population of 7.7 million citizens and an estimated adult prevalence of HIV infection of 0.4%. The Catalan healthcare system provides universal, tax-funded healthcare, and ART to all citizens.
Data were retrieved from the PISCIS cohort (Catalonian and Balearic Islands HIV cohort) and PADRIS (Public Data Analysis for Health Research and Innovation Program). Briefly, PISCIS is an ongoing, prospective, multicentre, population-based cohort that includes all PWH aged ≥16 years followed in one of the 16 collaborating hospitals, representing 84% of all PWH in Catalonia, from 1998 to 2022 (21). Data are updated yearly and include demographics, date of HIV diagnosis, AIDS-defining events, ART, and measurement of CD4 count and plasma HIV-RNA over time. PADRIS is a central research-oriented database that gathers and cross-matches real-world health data generated by the different public health systems (SISCAT), provided by the Catalan Agency for Health Quality and Evaluation (AQuAS). The database includes comorbidity data from hospital discharge diagnoses and primary healthcare from 2005 according to the International Classification of Disease 10th revision (ICD-10) (22). We used ICD-10 codes to define comorbidities according to the Swedish National Study of Aging and Care in Kungsholmen (SNAC-K) cohort (www.snac-k.se). Mortality data were obtained by cross-matching the information from PISCIS, PADRIS, and the national mortality registry.
The study complies with the STROBE reporting guidelines.
The PISCIS cohort has received ethical approval from Germans Trias i Pujol University Hospital's Clinical Research Ethics Committee, reference number EO-11-108, and patient data extraction is allowed by the 203/2015 Decree from the Catalan Health Department. All data are pseudo-anonymized in accordance with Regulation 2016/679 of the European Parliament.
We included all treatment naïve PWH aged ≥18 years, who initiated ART between 1 January 2005 and 30 June 2019. PWH with prior CV events were excluded from the analysis.
Individuals were classified according to their CD4 count at ART initiation into LP (i.e., CD4 count < 200 and 200–350 cells/μ) and non-LP (i.e., CD4 count >350 cells/μL). Non-LP contributed as the reference population.
The primary outcome was the first CV event after ART initiation, defined as the first event of ischemic heart disease, congestive heart failure, cerebrovascular disease, or peripheral vascular disease during the study period.
The secondary outcome was all-cause mortality among PWH experiencing a CV event.
Continuous variables were described as the median and interquartile range (IQR), whereas categorical variables were presented as the frequency and percentage over available data. We used Pearson's chi-squared test, t-test, and Mann–Whitney U-test to compare these variables between LP and non-LP. For polychotomous categorical variables with a statistically significant chi-square test of homogeneity, we further provided a significance test of the difference between proportions across categories of the variable between LP and non-LP.
Individuals were followed from ART initiation to the first CV event, loss-to-follow-up, death, or end of the observation period (30 June 2021), whichever occurred first. The cumulative incidence of the first CV event in LP vs. non-LP was compared using the log-rank test. We used Poisson regression to assess the association between CD4 count at ART initiation (< 200, 200–350, and >350 cells/μL) and the risk of a subsequent CV event. We adjusted for the following potential confounders at baseline: age (time-updated), gender, mode of HIV transmission, region of birth, time-updated calendar period [2005–2009, 2010–2014, 2015–2019, according to pre-integrase strand transfer inhibitor (INSTI)-available period, INSTI-available period, and universal ART implementation, respectively] (23), HIV-1 viral load, AIDS-defining disease, comorbidities (diabetes mellitus, arterial hypertension, dyslipidemia, chronic kidney, lung, or liver disease, malignancy, or depression), and educational level. We provide incidence rates (IRs) and IR ratios (IRRs) and their corresponding 95% confidence interval (CI).
For mortality after the first CV event, individuals were followed from the CV event to death, loss-to-follow-up, or 30 June 2021, whichever came first. The cumulative mortality was compared using the log-rank test. We used a Poisson regression analysis to assess the risk of late HIV presentation and mortality adjusting for the above-mentioned potential confounders. We provide mortality rates (MRs) and MR ratios (MRRs) and a 95%CI.
We conducted a sensitivity analysis including only PWH who initiated ART and survived 2 years, in order to remove the bias of the increased risk of severe AIDS-related comorbidities and complications in the initial period and to assess the effect of early immune recovery on CVD (3, 24). PWH were stratified according to their 2-year CD4 count (< 200, 200–500, and >500 cells/μL in LP and ≤ 500 cells/μL and >500 cells/μL in non-LP).
All analyses were conducted with STATA software (v.16; Stata Corp, College Station, TX, USA).
We identified 4036 adult PWH who initiated ART between 2005 and 2019. Of them, 3317 met the inclusion criteria, 1556 (46.9%) non-LP, and 1,761 (53.1%) LP (Figure 1). The median follow-up was 8.0 years (IQR: 5.0–11.2), giving rise to 26 589.1 persons/years (PY) at risk.
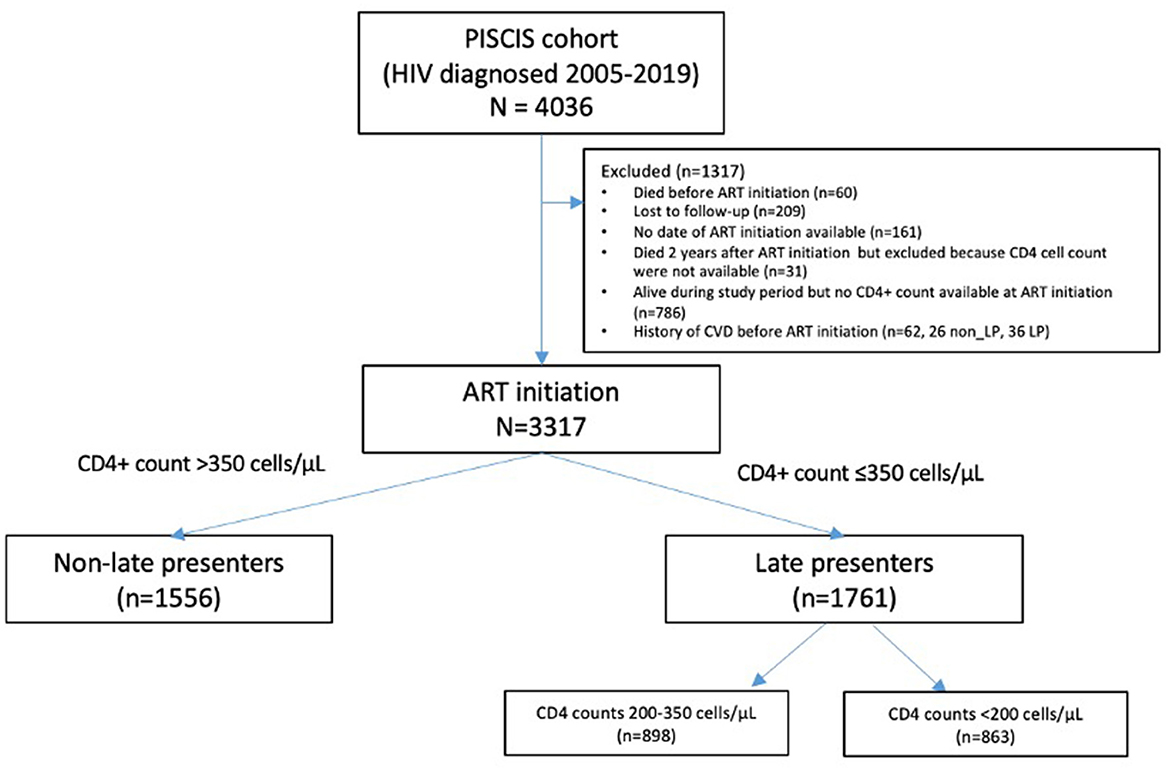
Figure 1. Flowchart of cohort construction.
Table 1 summarizes baseline characteristics. LP were more likely heterosexual men, women, IDU, older, treated with protease inhibitors or non-nucleoside reverse transcriptase inhibitors, having higher plasma HIV-RNA, and having lower educational levels. LP had higher rates of AIDS-defining events, liver disease, dementia, and less arterial hypertension.
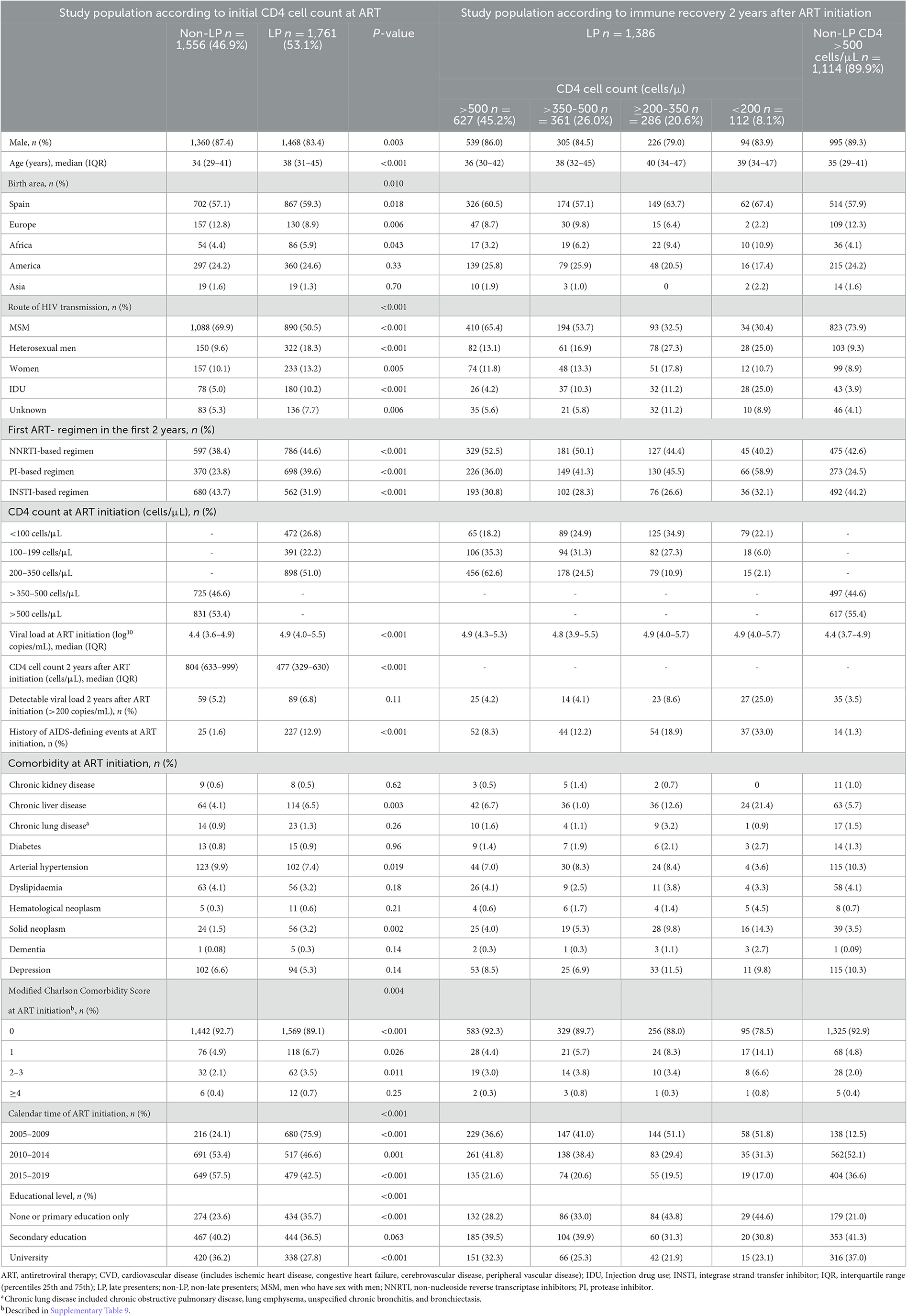
Table 1. Baseline characteristics of the study participants.
At 2 years, 112 (8.1%) LP remained with a CD4 count of < 200 cells/μL, 286 (20.6%) had 200–350 cells/μL, 661 (26.0%) had 351–500 cells/μL, and 627 (45.2%) had >500 cells/μL. LP with a 2-year CD4 count of < 200 cells/μL after ART initiation had higher rates of detectable HIV-RNA (p < 0.0001) (Table 1).
Overall, 163 (4.9%) PWH experienced a first CV event during the study period [IR 6.1/1000 PY (95%CI: 5.3–7.1)]: 105 (6.0%) LP vs. 58 (3.7%) non-LP (p = 0.003). Forty-eight (29.4%) experienced a heart failure event, 42 (25.8%) experienced an ischemic heart event, 53 (32.5%) experienced a cerebrovascular event, and 20 (12.3%) experienced a peripheral artery event (Supplementary Table 3). Most PWH experienced 1 CV event (n = 136, 83.4%), 24 (14.7%) experienced 2 CV events, and 3 (1.8%) experienced 3 different events. The rates of CV events did not change along the calendar time analyzed (Table 2).
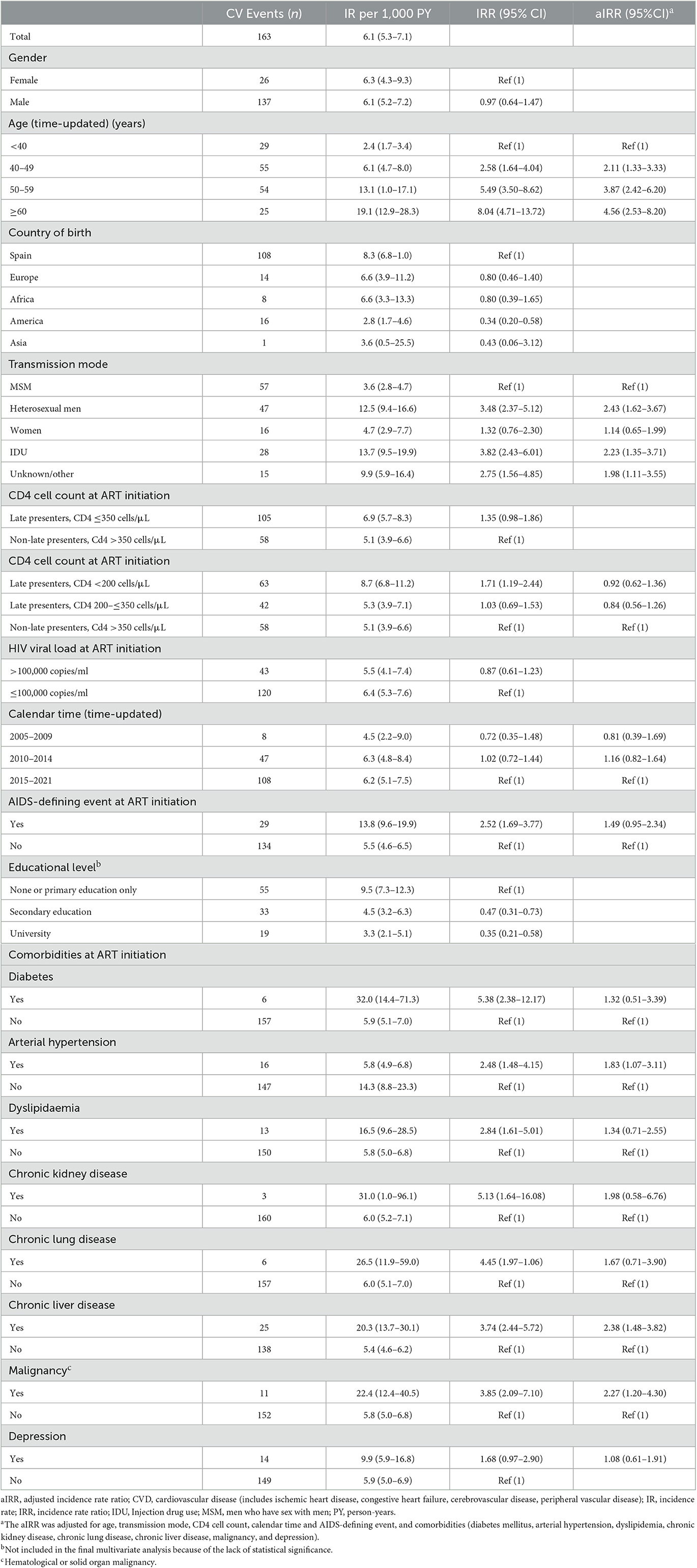
Table 2. Incidence rate of a first CV event in the overall cohort, including all LP and non-LP.
Kaplan–Meier curves for incident CV events stratified by CD4 count at ART initiation (LP vs. non-LP) or by their 2-year CD4 recovery (non-LP with CD4 count >500 cells/μL vs. LP with CD4 count >500, >350–500, 200–350, and < 200 cells/μL) showed no significant differences between groups (log-rank test, p = 0.07 and p = 0.22, respectively) (Figures 2A, B).
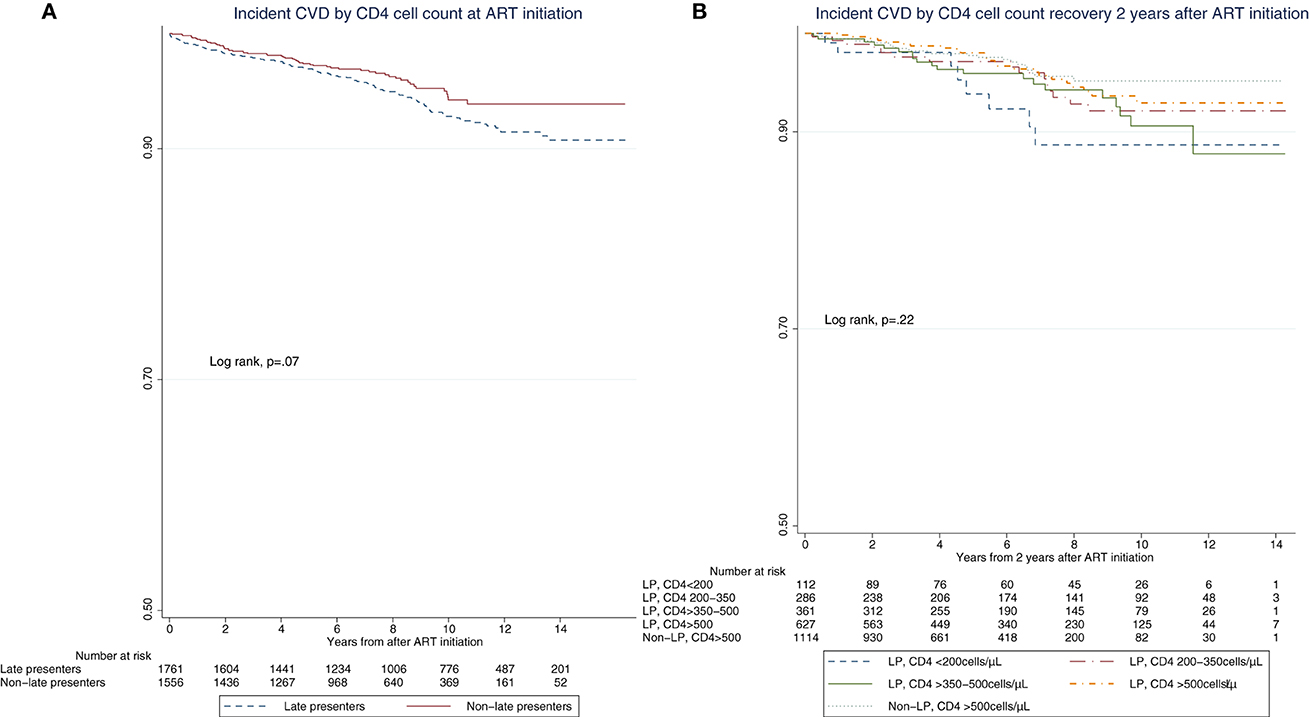
Figure 2. Kaplan–Meier curves of time to cardiovascular events. (A) Incident cardiovascular events by CD4 cell count at ART initiation. (B) Incident cardiovascular events by CD4 cell count 2 years after ART initiation.
In the univariate regression analysis, only LP with a baseline CD4 count of < 200 cells/μL had an increased risk of CV events compared to non-LP [IRR 1.71 (95%CI: 1.19–2.44)]. However, this association was no longer shown in the multivariate analysis adjusted for age, HIV transmission mode, calendar time, and comorbidities [aIRR 0.92 (95%CI: 0.62–1.36) and 0.84 (95%CI: 0.56–1.26) for LP with baseline CD4 count < 200 and 200–350 cells/μL, respectively] (Table 2). The risk of CV events increased significantly paralleling the age of PWH with no evidence of effect modification for LP (Supplementary Table 4). Other variables associated with increased risk were heterosexual males compared to MSM [aIRR 2.43 (95%CI: 1.62–3.67)], chronic liver disease [aIRR 2.38 (1.48–3.82)], and malignancy [aIRR 2.27 (1.20–4.30)]. Diabetes, arterial hypertension, dyslipidemia, chronic kidney or lung disease, and depression were not associated with an increased risk for CV events in the multivariate analysis.
Overall, 185 (5.6%) patients died during the study period (Supplementary Tables 5, 6). Among the 163 PWH experiencing a CV event, 31 died [26 LP and 5 non-LP, MR 40.4/1000PY (95%CI: 28.4–57.4)]. One-third of these deaths (n = 12, 38.7%) occurred within 3 months and 18 (58%) within the first year (Supplementary Figure 2). LP exhibited higher cumulative mortality (log-rank, P = 0.038) (Supplementary Figure 2); however, mortality was no longer higher in the multivariate analysis after adjusting for age, HIV transmission mode, and comorbidities [aMRR 1.24 (95%CI: 0.45–3.44)], although the absolute numbers were small. Women and individuals with chronic lung and/or liver disease had an increased mortality after a CV event [aMRR 5.89 (95%CI:1.35–25.60), 5.06 (95%CI:1.61–15.91) and 3.49 (95%CI:1.08–11.26), respectively] (Table 3).

Table 3. All-cause mortality in 163 people with HIV developing a first CV event.
Given the known high morbidity and mortality due to AIDS-related conditions in LP during the first 2 years, we specifically analyzed the subset surviving the first 2 years after ART initiation (n = 2625 PWH) (Supplementary Figure 1). In this analysis, with 103 persons experiencing a CV event, we found similar results with no increased risk of CV events in LP compared to non-LP with 2-year CD4 count >500 cells/μL (reference population) after adjusting for age (time-updated), calendar time (time-updated), HIV transmission mode, and comorbidities, regardless of the 2-year CD4 count [aIRR 0.99 (0.43–2.26) and 0.82 (0.48–1.39), in LP with a 2-year CD4 count of < 200 cells/μL and 200–500 cells/μL, respectively] (Supplementary Tables 7, 8; Supplementary Figure 3).
In this multicenter, population-based, prospective cohort analysis, we observed that LP with no previous CV events at ART initiation did not have an increased long-term risk of CV events compared to non-LP. The definition included a composite endpoint of congestive heart failure, ischemic heart disease, cerebrovascular, and peripheral vascular disease. Mortality rates after CV events were high with ~40% of them occurring within the first 3 months after the event. Women and individuals with chronic lung and liver disease experienced particularly elevated mortality rates after CV events. Additional adjusted analyses including only PWH surviving the first 2 years after ART initiation yielded similar results, regardless of 2-year CD4 cell recovery, reinforcing the main findings of the study.
Several studies have shown that unremitting immune activation, persistent inflammation, and vascular dysfunction could be common in PWH and potentially associated with earlier atherosclerosis and premature CVD (25). LP have increased chronic inflammation due to persistent immune damage established before ART initiation (7), and higher levels of immune activation could theoretically play an additional role in the development of early CVD in this subpopulation. However, our results do not confirm an increased risk of CV events in LP compared to the rest of PWH. Although no differences were observed in the adjusted analysis, PWH with a CD4 count of < 200 cells/μL at ART initiation or after 2 years had an approximately unadjusted 2-fold increased risk of CV events compared to non-LP. This association is likely due to the confounding effect of age, calendar time, and various comorbidities, which themselves are independent risk factors for CVD. Not unexpectedly, an increased risk for CV events was seen in older PWH. Older people are at increased risk of both LP and CVD and in fact, the proportion of PWH older than 50 years is increasing, and about half of them have delayed presentation (4). On the other side, multimorbidity is common in LP, and a recent cross-sectional Italian study showed that multimorbidity was more common in LP compared to non-LP across all age distributions (26). All this suggests that data suggesting increased rates of CV events in LP could be biased by unadjusted confounders.
Calendar time could theoretically play a role as well, with lower CV risk in recent years, paralleling with improved cardiovascular risk management in PWH and increased safety and efficacy of ART, although this trend was not confirmed in our cohort. Recent investigations on the risk of CVD using INSTI-based regimens, the currently recommended first-line choices, have yielded inconsistent results. A study from the RESPOND cohort consortium, which included 29340 individuals, 14000 of whom were given an INSTI, have reported an increased risk of CVD in the first 2 years after INSTI initiation compared to initiating other regimens (27). However, another recent study in the Swiss HIV Cohort, which included 5362 individuals initiating ART after May 2008, 1837 individuals initiated an INSTI-based regimen, found no such risk (28). In the following years, it will be important to determine whether the link between INSTI usage and CVD is due to INSTI use or to unmeasured confounding. On the other side, the use of INSTI has been recently been associated with several studies with a more favorable immune recovery (29, 30).
Our results are in concordance with the results from the Spanish CoRIS cohort including patients initiating ART between 2004 and 2018, where they found no evidence of an increment of CV events in LP compared to non-LP. However, the analysis was not adjusted for previous comorbidities that could play a major role in the development of CVD (14). Similarly, in a study from the Veterans Aging Cohort including individuals from 1996 to 2012, no increased risk of CVD was seen with individuals initiating ART with a CD4 count of < 200 cells/μL compared to those ≥200 cells/μL (15). In a Dutch Athena Cohort study including patients between 1998 and 2009, no association was found between LP with a 2-year CD4 count of < 200 cells/μL and risk of CVD in the adjusted analysis, although individuals with previous CVD were not excluded (13).
In contrast, other studies have described an association between CD4 cell count below 200 cells/μL and a higher risk of CVD. Two cohort studies from the US (Veterans Aging Cohort and North American AIDS Cohort Collaboration on Research and Design [NA-ACCORD]) and two metanalyses, all including participants before the year 2013, have shown that CD4 counts < 200 cells/μL were associated with increased CV risk, including incident myocardial infarction (aHR 2.02; 95% CI, 1.42–2.88), ischemic stroke (aHR 1.66; 95% CI, 1.30–2.12), and peripheral artery disease (HR, 1.91; 95% CI, 1.71–2.13) (16–20). However, most of these studies included immunological non-responders, who fail to reconstitute their CD4 cell count despite virological suppression on ART, who are known to have increased long-term morbidity and mortality risk (31). Furthermore, a significant proportion of individuals in these studies had unsuppressed viremia at the moment of the event, either because they were not on ART at the time or because they belonged to an HIV subpopulation that was heavily treated or had poor treatment adherence. HIV unsuppressed viremia is strongly correlated with chronic inflammation, ongoing immune activation, and accelerated atherosclerosis and could have confounded the finding. Our study included very few immunological non-responders with a 2-year CD4 count of < 200 cells/μL and CV events to draw reliable conclusions in this subpopulation. These patients had higher rates of detectable viremia, comorbidities (AIDS-defining events, chronic liver disease, and malignancies), and lower educational levels, which could also influence their CV risk. However, in the whole cohort, only 6.4% of LP had detectable viremia 2 years after ART initiation.
We also identified an increased risk of CV events in patients with chronic liver disease and malignancies. This association must be interpreted with caution given that other risk factors, such as tobacco and alcohol abuse, could be possible underlying confounders in these groups. A higher frequency of smoking, alcohol, and recreational drug abuse has been, indeed, associated with higher rates of CVD (32).
Mortality after a CV event was very high. However, we did not observe mortality differences between LP and non-LP. Nevertheless, the absolute numbers were low and do not allow for an in-depth analysis to establish robust conclusions.
To our knowledge, this is the first assessment of CV event rates in LP starting ART in a more recent calendar period (2005–2019), including integrase inhibitor use, with information on important comorbidities related to CVD enabling the performance of an accurate adjusted analysis. We adjusted for calendar time because both the management and prognosis of CVD and ART initiation guidelines have varied over time. Other strengths of this study include the prospective, population-based, multicenter HIV-cohort design, including 84% of all PWH followed in Catalonia and the long observation period. We had access to high-quality, real-world health data generated by the public health system of Catalonia, including all hospital and primary care diagnoses, thus including accurate information on CV events, comorbidities, and mortality. We assessed the risk of CVD in PWH initiating ART and in PWH surviving the first 2 years, to avoid the vulnerable first 2-year period after HIV diagnosis with high risk for severe comorbidities and complications.
In terms of limitations, we did not have access to causes of death, neither overall nor in CV event-related deaths, and a low prevalence of the latter limits a more thorough interpretation. Furthermore, the percentage of subjects with a CD4 count of < 200 cells/μL after 2 years of ART initiation was low (only 8%) and it is therefore not possible to draw definitive conclusions to establish a relationship between immunological non-response and CVD. We had no information on current smoking, alcohol consumption, or substance abuse other than injectable drug usage, all of which are known independent risk factors for CVD. We included chronic lung and liver disease in the model, which could be interpreted as a surrogate marker, especially for the first two risk factors. Finally, the number of events was low, and type II errors in this analysis cannot be ruled out.
In conclusion, CVD remains a common cause of morbidity and mortality among PWH. LP with no prior CV events at ART initiation did not have an increased long-term risk of CV events compared with non-LP. Our results call for risk stratification and identification of PWH at increased risk of future CVD based on traditional risk factors and comorbidities linked to increased CV risk, to focus risk-reducing strategies in these subjects. When initiating successful ART, late HIV presentation does not increase by itself the risk for CVD.
The data analyzed in this study is subject to the following licenses/restrictions: The data collected for this study are available from the Centre for Epidemiological Studies of Sexually Transmitted Diseases and HIV/AIDS in Catalonia (CEEISCAT), the coordinating center of the PISCIS Cohort Study and from each of the collaborating hospitals upon request. Requests can be made via https://pisciscohort.org/contacte/. The study protocol, the statistical codebook and codes for the analysis can be requested from RM-I (cmFxdWVsQGJpc2F1cmluLm9yZw==).
The studies involving human participants were reviewed and approved by Germans Trias i Pujol University Hospital's Clinical Research Ethics Committee, Reference Number EO-11-108. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
RM-I conducted the research and analyzed the data. RM-I, MV-F, and JL wrote the first draft of the manuscript. All authors contributed to the interpretation of the results and revision of the manuscript and gave their final approval to the manuscript.
The PISCIS study group includes: Jordi Casabona, A. Esteve, Andreu Bruguera, Sergio Moreno-Fornés (CEEISCAT), Jose M. Miró, J. Mallolas, E. Martínez, JL Blanco, M. Laguno, M. Martínez-Rebollar, B. Torres, A. Gonzalez-Cordon (Hospital Clínic-Idibaps, Universitat de Barcelona), Elisa De Lazzari (Hospital Clínic-Idibaps), Arkaitz Imaz (Unitat de VIH i ITS, Servei de Malalties Infeccioses, Hospital Universitari de Bellvitge, IDIBELL), Pere Domingo (Unitat de VIH/SIDA Hospital de la Santa Creu i Sant Pau), Josep María Llibre (Fundació Lluita contra la Sida-Hospital Universitari Germans Trias i Pujol-Universitat Autònoma de Barcelona), Francisco Fanjul (Servei Medicina Interna, Hospital Universitari Son Espases), Gemma Navarro (Unitat de VIH/SIDA, Parc Tauli Hospital Universitari-Universitat Autònoma de Barcelona), Vicenç Falcó Ferrer [Servei de Malalties Infeccioses, Hospital Universitari Vall d'Hebron, Vall d'Hebron Research Institute (VHIR)], and Hernando Knobel (Servei de Malalties Infeccioses, Hospital del Mar).
This work was supported by scholarships from the University of Southern Denmark, the Danish AIDS-foundation, and Public Regional Funds. JM received a personal 80:20 research grant from Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain, during 2017–23. The study was investigator-driven and thus independent of any pharmaceutical company. The funding sources were not involved in study design, data collection, analyses, report writing, or the decision to submit the paper.
The authors are grateful to the patients who participated in this cohort and our colleagues in the clinical departments for their continued contribution and dedication. The authors are grateful to PADRIS and the Programme for the Prevention, Control, and Care for HIV, Sexually Transmitted Diseases and Viral Hepatitis of the Ministry of Health of the Government of Catalonia for their support and the Danish AIDS Foundation, the University of Southern Denmark, the Region of Southern Denmark, Odense University Hospital, and Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS) for financial support.
JM has received consulting honoraria and/or research grants from AbbVie, Angelini, Contrafect, Cubist, Genentech, Gilead Sciences, Jansen, Lysovant, Medtronic, MSD, Novartis, Pfizer, and ViiV Healthcare, outside the submitted study. JL has received honoraria and/or research grants from ViiV Healthcare, Gilead Sciences, and Janssen-Cilag.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2023.1182359/full#supplementary-material
1. Gooden TE, Gardner M, Wang J, Jolly K, Lane DA, Benjamin LA, et al. Incidence of cardiometabolic diseases in people with and without human immunodeficiency virus in the United Kingdom: a population-based matched cohort study. J Infect Dis. (2022) 225:1348–56. doi: 10.1093/infdis/jiab420
2. So-Armah K, Benjamin LA, Bloomfield GS, Feinstein MJ, Hsue P, Njuguna B, et al. HIV and cardiovascular disease. Lancet HIV. (2020) 7:e279–93. doi: 10.1016/S2352-3018(20)30036-9
3. Mocroft A, Lundgren JD, Sabin ML, Monforte A d'Arminio, Brockmeyer N, et al. Risk factors and outcomes for late presentation for HIV-positive persons in Europe: results from the Collaboration of Observational HIV Epidemiological Research Europe Study (COHERE). PLoS MED. (2013) 10:e1001510. doi: 10.1371/journal.pmed.1001510
4. Justice AC, Goetz MB, Stewart CN, Hogan BC, Humes E, Luz PM, et al. Delayed presentation of HIV among older individuals: a growing problem. Lancet HIV. (2022) 9:e269–80. doi: 10.1016/S2352-3018(22)00003-0
5. May M, Gompels M, Delpech V, Porter K, Post F, Johnson M, et al. Impact of late diagnosis and treatment on life expectancy in people with HIV-1: UK Collaborative HIV Cohort (UK CHIC) Study. BMJ. (2011) 343:d6016. doi: 10.1136/bmj.d6016
6. Gueler A, Moser A, Calmy A, Günthard HF, Bernasconi E, Furrer H, et al. Life expectancy in HIV-positive persons in Switzerland: matched comparison with general population. Aids. (2017) 31:427–36. doi: 10.1097/QAD.0000000000001335
7. Nou, Eric; LO, Janet; Gripspoon SK. Inflammation, immune activation, and cardiovascular disease in HIV. AIDS. (2016) 176:139–48. doi: 10.1097/QAD.0000000000001109
8. Deeks SG, HIV. Infection, inflammation, immunosenescence, and aging. Annu Rev Med. (2011) 62:141–55. doi: 10.1146/annurev-med-042909-093756
9. Manner IW, Trøseid M, Oektedalen O, Baekken M, Os I. Low Nadir CD4 cell count predicts sustained hypertension in HIV-infected individuals. J Clin Hypertens. (2013) 15:101–6. doi: 10.1111/jch.12029
10. Samad F, Harris M, Puskas CM, Ye M, Chia J, Chacko S, et al. Incidence of diabetes mellitus and factors associated with its development in HIV-positive patients over the age of 50. BMJ Open Diabetes Res Care. (2017) 5:1–9. doi: 10.1136/bmjdrc-2017-000457
11. Hile SJ, Feldman MB, Alexy ER, Irvine MK. Recent tobacco smoking is associated with poor HIV medical outcomes among HIV-infected individuals in New York. AIDS Behav. (2016) 20:1722–9. doi: 10.1007/s10461-015-1273-x
12. Crane HM, Paramsothy P, Drozd DR, Nance RM, Delaney JAC, Heckbert SR, et al. Types of myocardial infarction among human immunodeficiency virus–infected individuals in the United States. JAMA Cardiol. (2017) 2:260–7. doi: 10.1001/jamacardio.2016.5139
13. Van Lelyveld SFL, Gras L, Kesselring A, Zhang S, De Wolf F, Wensing AMJ, et al. Long-term complications in patients with poor immunological recovery despite virological successful HAART in Dutch ATHENA cohort. Aids. (2012) 26:465–74. doi: 10.1097/QAD.0b013e32834f32f8
14. Rava M, Domínguez-Domínguez L, Bisbal O, López-Cortés LF, Busca C, Antela A, et al. Late presentation for HIV remains a major health issue in Spain: results from a multicenter cohort study, 2004–2018. PLoS One. (2021) 16:2004–18. doi: 10.1371/journal.pone.0249864
15. Salinas JL, Rentsch C, Marconi VC, Tate J, Budoff M, Butt AA, et al. Baseline, time-updated, and cumulative HIV care metrics for predicting acute myocardial infarction and all-cause mortality. Clin Infect Dis. (2016) 63:1423–30. doi: 10.1093/cid/ciw564
16. Althoff K, Gebo K, Moore R, Boyd C, Justice A, Wong C. The contributions of traditional and HIV-related risk factors on non-AIDS-defining cancer, myocardial infarction, and end-stage liver and renal diseases in adults with HIV in the US and Canada: A collaboration of cohort studies Keri. Lancet HIV. (2019) 6:e93–104. doi: 10.1016/S2352-3018(18)30295-9
17. Beckman JA, Duncan MS, Alcorn CW, So-Armah K, Butt AA, Goetz MB, et al. Association of HIV infection and risk of peripheral artery disease. Circulation. (2018) 138:255–65. doi: 10.1161/CIRCULATIONAHA.117.032647
18. Sico JJ, Chang C-CH, So-Armah K, Justice AC, Hylek E, Skanderson M, et al. HIV status and the risk of ischemic stroke among men. Neurology. (2015) 84:1933–40. doi: 10.1212/WNL.0000000000001560
19. D'Ascenzo F, Quadri G, Cerrato E, Calcagno A, Omedè P, Grosso Marra W, et al. A meta-analysis investigating incidence and features of stroke in HIV-infected patients in the highly active antiretroviral therapy era. J Cardiovasc Med. (2014) 1:1. doi: 10.2459/JCM.0b013e328365ca31
20. Eyawo O, Brockman G, Goldsmith CH, Hull MW, Lear SA, Bennett M, et al. Risk of myocardial infarction among people living with HIV: An updated systematic review and meta-analysis. BMJ Open. (2019) 9:5–9. doi: 10.1136/bmjopen-2018-025874
21. Jaén Á, Casabona J, Esteve A, Miró JM, Tural C, Ferrer E, et al. Características clinicoepidemiológicas y tendencias en el tratamiento antirretroviral de una cohorte de pacientes con infección por el virus de la inmunodeficiencia humana. Cohorte PISCIS Med Clin (Barc). (2005) 124:525–31. doi: 10.1157/13073938
22. Goverment of Catalonia. Public Program of Data Analysis for Health Research and Innovation in Catalonia. PADRIS.
23. Lundgren J, Babiker AG, Fred G, Sean E, Grund B, Sharma S, et al. Initiation of antiretroviral therapy in early asymptomatic HIV infections. The INSIGHT START Study Group. N Engl J Med. (2015) 373:795–807. doi: 10.1056/NEJMoa1506816
24. Martin-Iguacel R, Reyes-Urueña J, Bruguera A, Aceitón J, Díaz Y, Moreno-Fornés S, et al. Determinants of long-term survival in late HIV presenters: The prospective PISCIS cohort study. eClinicalMedicine. (2022) 52:101600. doi: 10.1016/j.eclinm.2022.101600
25. Hsue PY, Hunt PW, Schnell A, Kalapus SC, Hoh R, Ganz P, et al. Role of viral replication, antiretroviral therapy, and immunodeficiency in HIV-associated atherosclerosis. AIDS. (2009) 23:1059–67. doi: 10.1097/QAD.0b013e32832b514b
26. Guaraldi G, Zona S, Menozzi M, Brothers TD, Carli F, Stentarelli C, et al. Late presentation increases risk and costs of non-infectious comorbidities in people with HIV: An Italian cost impact study. AIDS Res Ther. (2017) 14:1–7. doi: 10.1186/s12981-016-0129-4
27. Neesgaard B, Greenberg L, Miró JM, Grabmeier-Pfistershammer K, Wandeler G, Smith C, et al. Associations between integrase strand-transfer inhibitors and cardiovascular disease in people living with HIV: a multicentre prospective study from the RESPOND cohort consortium. Lancet HIV. (2022) 9:e474–85. doi: 10.1016/S2352-3018(22)00094-7
28. Surial B, Chammartin F, Damas J, Calmy A, Haerry D, Stöckle M, et al. Impact of integrase inhibitors on cardiovascular disease events in people with HIV starting antiretroviral therapy. Clin Infect Dis. (2023). ciad286. doi: 10.1093/cid/ciad286
29. Neesgaard B, Mocroft A, Zangerle R, Wit F, Lampe F, Günthard HF, et al. Virologic and immunologic outcomes of treatment with integrase inhibitors in a real-world setting: The RESPOND cohort consortium. PLoS ONE. (2020) 15:1–19. doi: 10.1371/journal.pone.0243625
30. Martin-Iguacel R, Negredo E, Peck R, Friis-Møller N. Hypertension is a key feature of the metabolic syndrome in subjects aging with HIV. Curr Hypertens Rep. (2016) 26:1–14. doi: 10.1007/s11906-016-0656-3
31. Engsig FN, Gerstoft J, Kronborg G, Larsen CS, Pedersen G, Røge B, et al. Long-term mortality in hiv patients virally suppressed for more than three years with incomplete cd4 recovery: a cohort study. BMC Infect Dis. (2010) 10:318. doi: 10.1186/1471-2334-10-318
Keywords: late HIV presentation, cardiovascular disease, myocardial infarction, cerebrovascular disease, HIV
Citation: Martín-Iguacel R, Vazquez-Friol MC, Burgos J, Bruguera A, Reyes-Urueña J, Moreno-Fornés S, Aceitón J, Díaz Y, Domingo P, Saumoy M, Knobel H, Dalmau D, Borjabad B, Johansen IS, Miro JM, Casabona J and Llibre JM (2023) Cardiovascular events in delayed presentation of HIV: the prospective PISCIS cohort study. Front. Med. 10:1182359. doi: 10.3389/fmed.2023.1182359
Received: 08 March 2023; Accepted: 22 May 2023;
Published: 21 June 2023.
Edited by:
Guido Poli, Vita-Salute San Raffaele University, ItalyReviewed by:
Lishomwa (Lish) Ndhlovu, Cornell University, United StatesCopyright © 2023 Martín-Iguacel, Vazquez-Friol, Burgos, Bruguera, Reyes-Urueña, Moreno-Fornés, Aceitón, Díaz, Domingo, Saumoy, Knobel, Dalmau, Borjabad, Johansen, Miro, Casabona and Llibre. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raquel Martín-Iguacel, cmFxdWVsQGJpc2F1cmluLm9yZw==; Josep M. Llibre, am1sbGlicmVAZmxzaWRhLm9yZw==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.