 Rosa Estela García-Chanes1
Rosa Estela García-Chanes1 José Alberto Avila-Funes2,3
José Alberto Avila-Funes2,3 Miguel Germán Borda4
Miguel Germán Borda4 Mario Ulises Pérez-Zepeda1,5*
Mario Ulises Pérez-Zepeda1,5* Luis Miguel Gutiérrez-Robledo1,2
Luis Miguel Gutiérrez-Robledo1,2- 1Dirección de Investigación, Instituto Nacional de Geriatría, Mexico City, Mexico
- 2Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
- 3Bordeaux Population Health Research Center, INSERM-University of Bordeaux, UMR 1219, Bordeaux, France
- 4Centre for Age-Related Medicine (SESAM), Stavanger University Hospital, Stavanger, Norway
- 5Centro de Investigación en Ciencias de la Salud (CICSA), Facultad de Ciencias de la Salud, Universidad Anáhuac México Campus Norte, Huixquilucan de Degollado, Mexico
Background: Frailty has been recognized as a growing issue in older adults, with recent evidence showing that this condition heralds several health-related problems, including cognitive decline. The objective of this work is to determine if frailty is associated with cognitive decline among older adults from different countries.
Methods: We analyzed the baseline the Study on Global Ageing and Adult Health (SAGE), that includes six countries (Ghana, South Africa, Mexico, China, Russia, and India). A cross-section analysis was used to assess how Frailty was related with the Clinical Frailty Scale decision tree, while cognitive decline was evaluated using standardized scores of tests used in SAGE.
Results: A total of 30,674 participants aged 50 years or older were included. There was an association between frailty levels and cognitive performance. For example, women had an inverse relationship between frailty levels and cognitive scores, even when comparing robust category with frailty level 2 (RRR = 0.85; p = 0.41), although the relative risks decrease significantly at level 3 (RRR = 0.66; p = 0.03). When controlling for age, the relative risks between frailty levels 4 to 7 significantly decreased as cognitive performance increased (RRR = 0.46, RRR = 0.52, RRR = 0.44, RRR = 0.32; p < 0.001).
Conclusion: Our results show an association between frailty levels measured in a novel way, and cognitive decline across different cultural settings.
Introduction
Frailty is a common condition that mainly affects older adults and is characterized by the loss of an adequate response to common stressors that leads the individual to a worse health status (1). In fact, global aging has resulted in an increased frequency of conditions such as frailty, increasing the interest from health professionals and researchers in the field of aging and geriatric care (2). Evidence shows that assessing older adults leads to targeted interventions, improving health and especially when focusing this assessment on frailty (3). On the other hand, evidence shows that frailty is closely related to different conditions common to old age (4) and in particular the so-called ‘geriatric syndromes’ (5, 6).
In particular, frailty has been related to deteriorating mental health conditions, such as depression (7), anxiety (8), and cognitive impairment (9). In fact, evidence has grown in recent years, supporting the idea that mental and physical health converge at some point in time, leading to worse health-related outcomes (10, 11), whenever this happens. For example, Avila-Funes et al. showed that frailty is a better predictor of mortality whenever cognitive impairment is considered (12). As previously mentioned, understanding the underpinnings of this relationship has the potential of designing interventions that improve both frailty and cognitive performance in old age (13).
Finally, there is increasing data on how social determinants of health, impact the development and expression of frailty and dementia; those older adults who live in countries with high inequality have the most adverse outcomes (14–18). Taking advantage of the multi-country design of the Study on Global Ageing and Adult Health (SAGE) (includes six low- and middle-income countries) we aimed at understanding the association between frailty and cognitive performance in older adults from different sociocultural background.
Methods
Design and sample
A cross-sectional was used to baseline data of SAGE (2007–2010). This study was an initiative from the World Health Organization (WHO) to determine the factors that impact aging in six low- and middle-income countries (LMICs): Ghana, Mexico, India, South Africa, Russia, and China. It includes a set of harmonized questionnaires from different dominions (e.g., health, physical function, demographics, etc.), which was applied to a representative sample of adults aged 50 or older from the participant countries. Complete description of objectives and procedures is available elsewhere (19). For purposes of this report, only participants with complete baseline information from all the countries were included.
Ethical approval. The SAGE study was approved by the World Health Organization’s Ethical Review Board (reference number RPC149) and the Ethical and Protocol Review Committee of each country. Written informed consent was obtained from all study respondents.
Clinical Frailty Scale Decision Tree
Currently, numerous tools have been developed and used to categorize someone as frail (20). Among these instruments, the Clinical Frailty Scale, was developed to derive frailty levels after a geriatric assessment, resulting in scores from 1 (robust older adult) to 9 (end-stage frailty) (21). Using figurines and descriptive test for each level of frailty, the trained clinician can derive a category, that in turn may trigger interventions (22). Recently, a decision tree was developed to facilitate the application of the Clinical Frailty Scale (CFS) (21) for a wider range of professionals, not necessarily experts in the field (23). Since this is a very recent add-on to CFS, reports on its usage are still limited. However, a large study showed its ability to predict adverse health-related outcomes in older adults admitted in the intensive care unit (24), so its application in the community could be very useful.
As with the CFS, the decision tree results in frailty levels. The levels of the CFS decision tree were integrated according to instructions available in the original manuscript (23) and the website.1 The classification of frailty levels was built from the variables available in the SAGE survey including: activities of daily living (ADL)—bathing, getting dressed, eating, walking, getting up; instrumental ADL (IADL)—housework, participating in community activities, doing your day to day work, carrying things, using private or public transport, getting out of your home; chronic diseases—arthritis, stroke, angina, diabetes, chronic lung disease, asthma, depression, hypertension, cataract; self-rated health; fatigue—you have enough energy for everyday life; physical activity—any moderate-intensity sports, fitness or leisure activities causing a small increase in breathing or heart rate for at least 10 min at a time (See Supplementary Table A and Figure 1). Using the classification tree, frailty levels were defined from 1 to 7 according to the flow of conditions and characteristics reported by older persons. Levels 8 and 9 refer to individuals with terminal conditions, since SAGE does not include them, these levels were not considered.
Cognitive performance
The SAGE includes five cognitive tests to assess this dominion: immediate and delayed verbal recall (i.e., episodic memory), forward and backward digit span (i.e., working memory), and verbal fluency (i.e., semantic memory). For the immediate verbal recall test, interviewers first read a list of 10 words aloud and asked the participants to immediately recall as many words as they could in one minute (three trials), recording the best score. The delayed recall ability was assessed by asking participants to recall the list of words; and scored in a similar fashion as the previous test. Forward and backward digit span, scoring the number of correct series repeating in two trials (9 points-forward span and 8 points-backward span). Naming as many animals that come to one’s mind in one minute was used to test verbal fluency (spontaneous language production), with possible scores ranging from 0 to 70 (one point for each valid animal name). Z-scores were calculated to facilitate the comparison of the cognitive tests’ performance, between individuals and countries; a previously reported method (25). Furthermore, individual z-scores from each cognitive domain were added to obtain a global composite z-score for cognitive performance by countries.
Statistical analysis
Initially, all variables included were described by sex. Differences in the means for the composite cognitive z-score between CFS levels—also by sex—was done with one-way ANOVA, including post hoc estimation with Bonferroni’s test. The analysis of the CFC levels and the z scores of each one of the cognitive domains is also presented (see Supplementary Table B). The descriptive and ANOVA analyzes were also done for each country (see Supplementary Tables C, D). Finally, three multinomial models were fitted by sex to estimate the effects of age and education on cognition between CFS levels and their corresponding estimated probabilities were plotted. Additionally, adjusted models for country were performed (see Supplementary Table E). All statistical analyses were performed with STATA version 17.0.
Results
From the 35,330 participants aged 50 or older, 30,674 (86.8%) had complete data on the variables of interest. Our study sample was constituted by participants from China (39.5%), Ghana (13.1%), India (20.4%), México (6.8%), Russia (10.6%), and South Africa (9.6%) (See Supplementary Table C). When analyzing the total sample by sex, no differences in age were observed, but there was higher level of education in men.
Regarding CFS levels, higher levels of frailty were more frequent for women (26.5% in level 6 and 14.5% in level 7). These differences by sex were clear when observed in the number of chronic diseases (0 men vs. 1 women), in worse health perception (15.7% in men vs. 19.8% in women), physical activity (13.7% in men vs. 10.6% women) (see Table 1). An inverse relationship was found between the cognitive z-score and levels of frailty and sex, 1 ( men = 0.57,95%CI [0.35to0.79]; women = 0.61,95%CI[0.15to1.08]), level 2 ( men = 0.63,95%CI[0.58to0.69]); women = 0.46,95%CI[0.40to0.53]), level 3 men = 0.41,95%CI[0.38to 0.43]); women = 0.23,95%CI[0.20 to 0.26]), level 4 ( men = 0.08,95%CI[−0.01to 0.16]; women −.15,95%CI[−0.23to−0.62]), level 5 ( men = 0.13,95%CI[0.11to 0.16]; women = −0.10,95%CI[−0.13to−0.07]) level 6 men = −0.02,95%CI [−.05to0.02]); women = −0.28,95%CI[−0.31to−0.25]), level 7 men = −0.39,95%CI[−0.44to−0.34]); women = −0.65,95%CI[−0.68to−0.60]), (see Figure 1). When analyzing the differences for the composite cognitive z-score between levels of frailty, no significant differences were found for levels below 4. Moreover, there were no differences in the cognitive score between levels 4 and 5 in both men and women (see Table 2 and Figure 1).
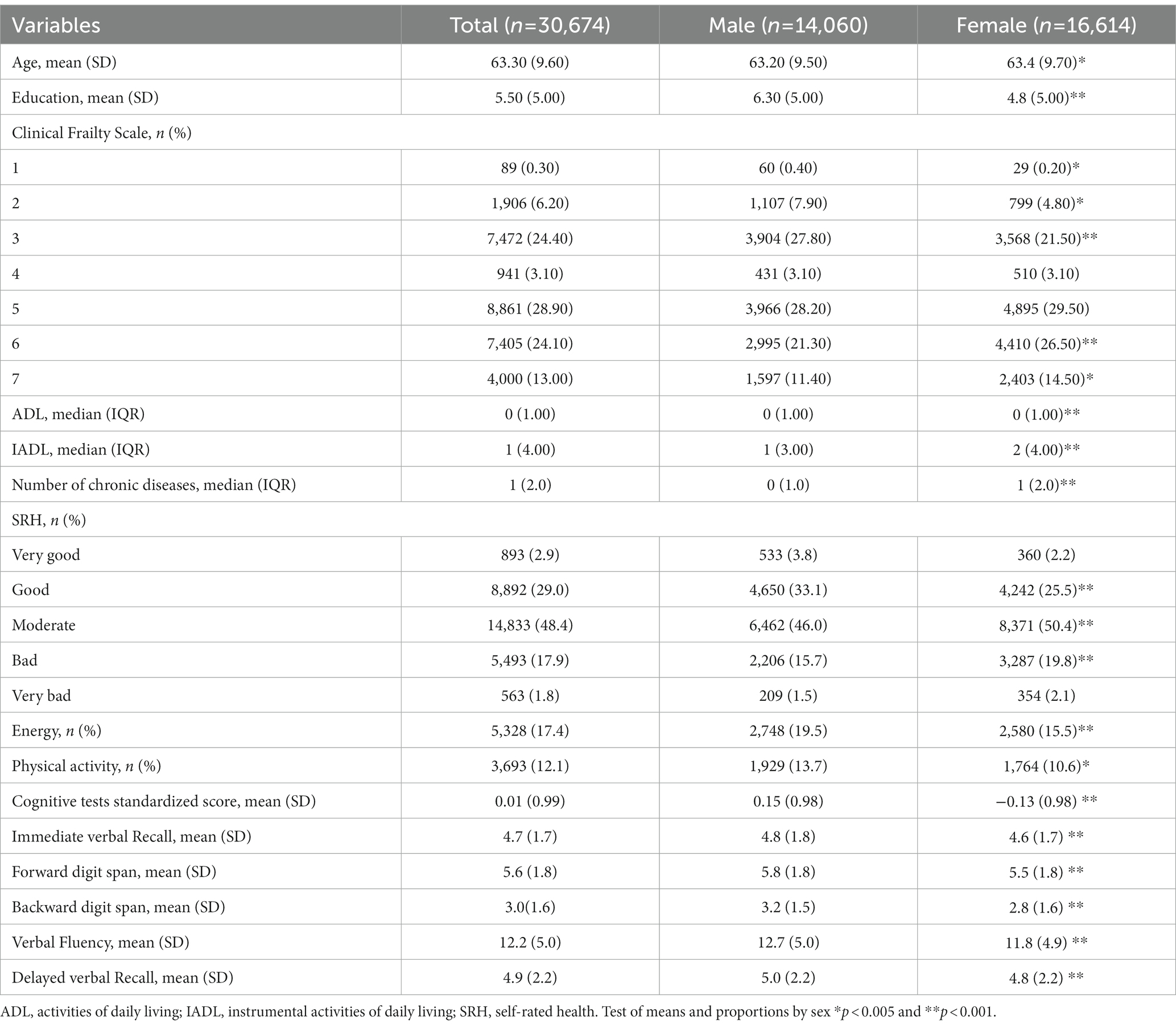
Table 1. Descriptive statistics stratified by sex.
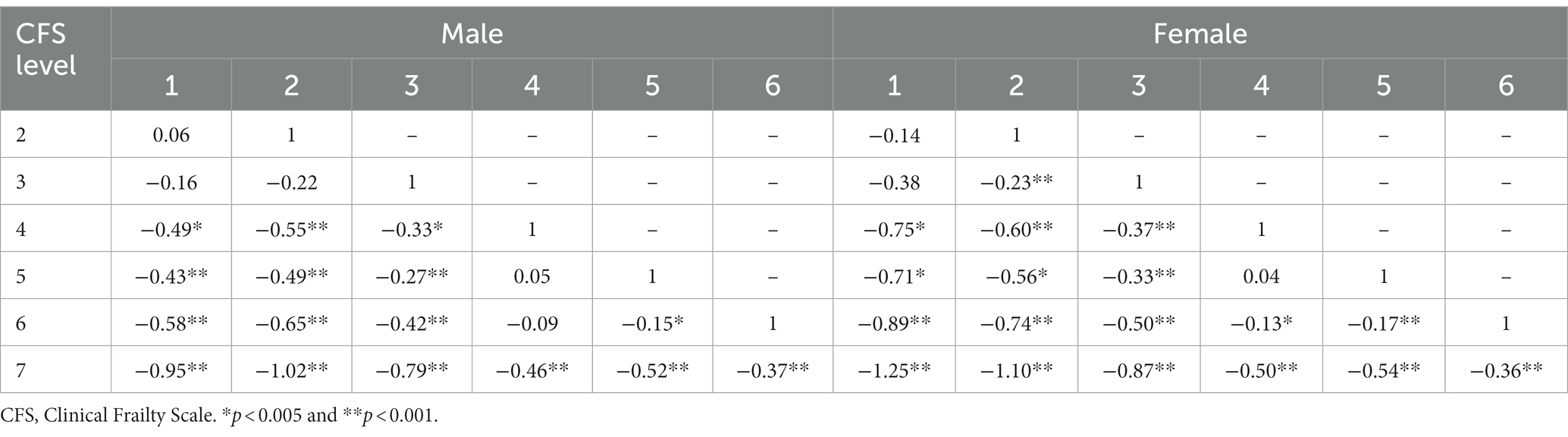
Table 2. Composite cognitive z-scores mean differences by Clinical Frailty Scale Level and stratified by sex, including post hoc Bonferroni’s test.

Figure 1. Comparison of the cognitive tests standardized scores between Clinical Frailty Scale levels by sex.
Table 3 shows the relative risk ratios (RRR) obtained from the unadjusted and adjusted multivariable multinomial logistic regression models that differentiated the cognitive score between frailty levels with level 1 (Very Fit) as the reference category. For men, the unadjusted model showed that for each additional unit of the cognitive score, the relative risks of being fit (level 2) (RRR = 1.08; p = 0.60) compared to being level 1 did not increase significantly. On the other hand, the risks related to having very mild (level 4), mild (level 5), moderate (level 6), and severe frailty (level 7) decreased significantly (RRR = 0.57, RRR = 0.61, RRR = 0.51, RRR = 0.34; p < 0.001) as cognitive scores increased. When controlling for age (model 2), this inverse association between cognition and frailty levels was maintained (RRR = 0.56, RRR = 0.66, RRR = 0.58, RRR = 0.41; p < 0.001). Furthermore, when adjusting for education and age, the differences between the cognitive score and the CFS levels were reduced; and when comparing level 5 to level 1 lost significance (RRR = 0.80; p = 0.13).
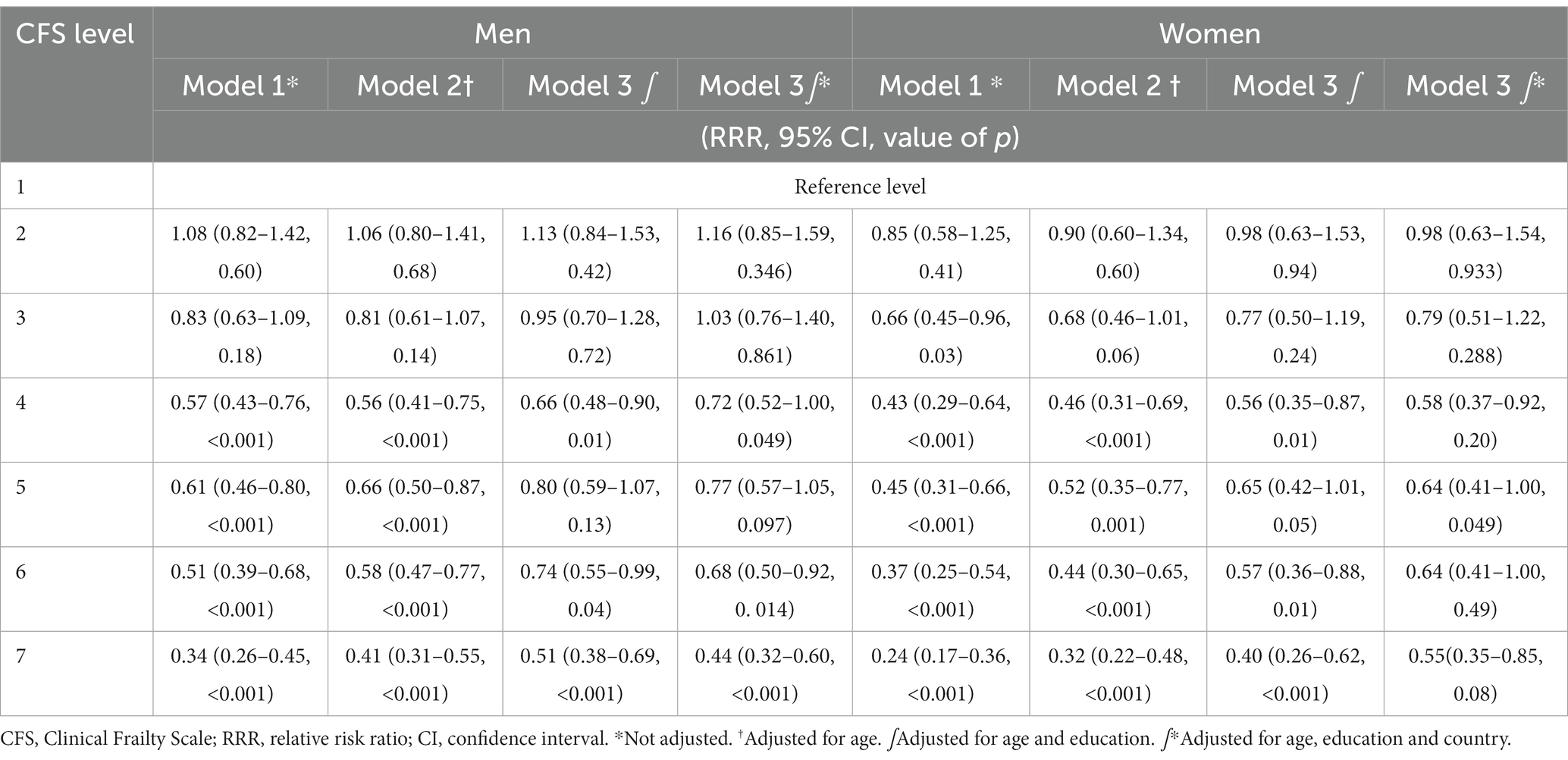
Table 3. Sex-stratified multinomial regression models for composite cognitive z-score and Clinical Frailty Scale level (level 1 as reference).
For women, the inverse relationship between frailty levels was maintained as the cognitive score increases even for level 2 (RRR = 0.85; p = 0.41), although the relative risks decreased significantly at level 3 (RRR = 0.66; p = 0.03). When controlling for age, the relative risks between levels 4 and 7 significantly decrease as cognitive performance increases (RRR = 0.46, RRR = 0.52, RRR = 0.44, RRR = 0.24; p < 0.001) (see Table 3).
Finally, regarding the sex-stratified predicted probabilities for cognitive performance by different levels of frailty (see Figure 2), the probability to experience higher levels of frailty (i.e., CFS 7) increases with lowering cognitive performance. Moreover, having lower frailty levels (i.e., CFS 2 or 3) decreases the probability of having cognitive impairment.
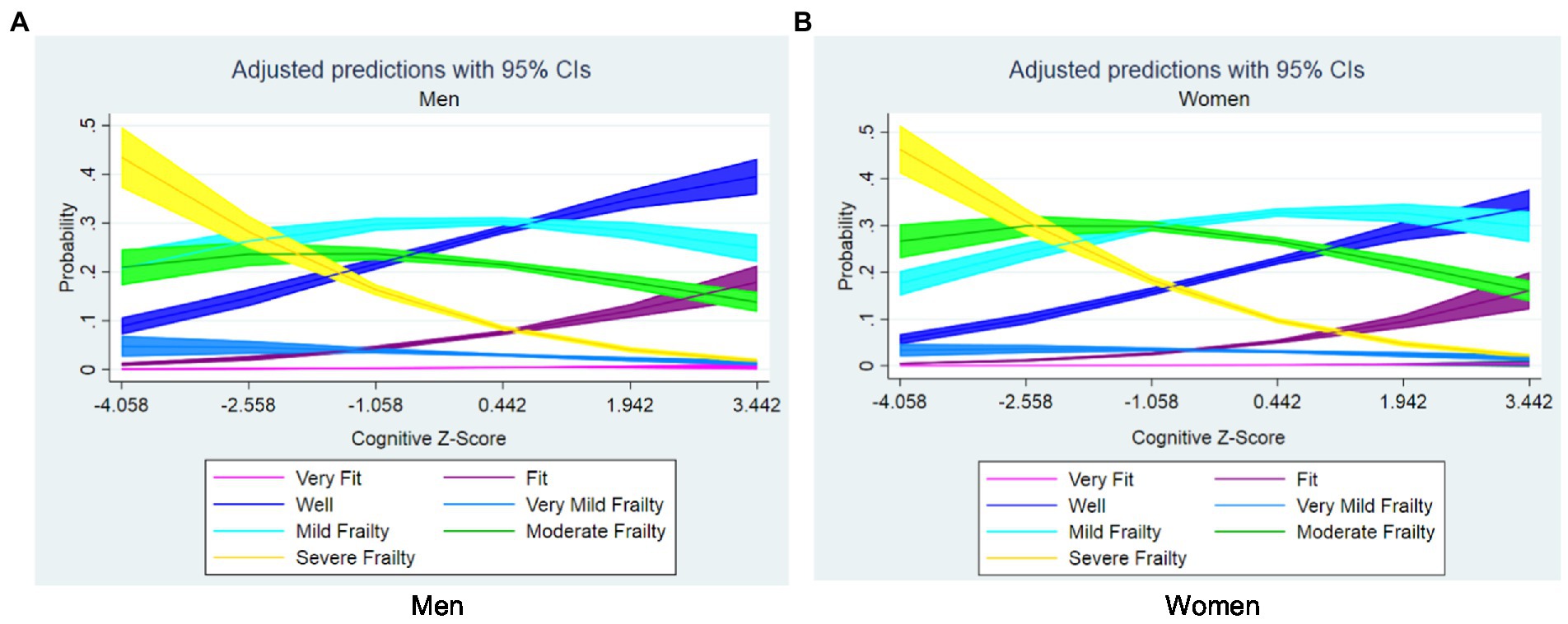
Figure 2. Sex-stratified estimated probabilities of frailty levels according to composite cognitive z-score, adjusted for age and education: (A) men and (B) women.
Discussion
To the best of our knowledge this is the first study to assess the association between cognitive performance tests and frailty measured using the CFS decision tree. Moreover, this adds to the current knowledge on how frailty relates to cognitive status in older adults, the higher the burden of frailty the lower the cognitive test scores. As shown in our results, those in charge of older adults should be careful to further examinate the cognitive status in those individuals with 3 or higher levels. Considering the CFS is a preliminary evaluation that leads to a more comprehensive assessment, the decision tree also showed that these levels are not limited to a progression in frailty, but alert that there might be a global decay in the older adult (i.e., mental and physical health), that merits further assessment (23, 26).
Previous evidence shows that frailty could precede dementia and other neurocognitive disorders, and even be related to neuropathological findings (27–29). On the other hand, there have been some interventions—mainly based in physical activity—that have shown to improve the overall health status of an older adult with frailty (30, 31), and this has the potential to stop the progression of both cognitive and physical decline. However, this relationship is still not fully understood, and merits further research.
Interestingly, our results were from a multi-national sample—the SAGE study—diming the effect of cross-cultural issues when assessing, since it utilizes a common tool and standardization with z-scores was used in this work, similar to what was used previously (25, 32). This points to the possible true nature of the association of mental and physical health, regardless of sociocultural differences. Assessment with the CFS decision tree allows to have a quick screening of an individual, as a screening of global health, and according to our results it could also alert about mental health. For instance, older adults with CFS level 3 or lower have the lowest probability of having low cognitive test scores and might not need further evaluation. In contrast, individuals with CFS levels ≥4 might benefit from a further evaluation, possibly focusing on cognition.
Although the tree is recommended only as an aid in assessing an older adult, it could be useful as a screen measure in an incremental approach to assessing older adults. Other studies have shown similar results, using other tools to measure frailty and other cognitive tests, whilst results seem consistent with that previously reported (12, 33–37). Moreover, one of the advantages that the CFS has is the ability to capture a continuum of frailty, rather than a limited ‘all or nothing’ grouping that almost all the other tools used for assessing frailty provide. This is helpful since interventions or different levels of care can be tailored to each of the levels. Moreover, a combination of CFS level with the presence or not of cognitive impairment is an add-on.
It is well-known that older population continues to grow, but that there are not enough resources to attend the needs of this age group. The CFS decision tree, could aid in identifying those at risk not only of increased risk of adverse health-related outcomes (23, 38, 39), but also of those that could be in the verge of presenting overt dementia, and benefit from early intervention for frailty that could impact cognitive health.
We need to acknowledge the limitations of our work. First, as a cross-sectional study, is difficult to address causality; though, longitudinal studies have shown that this might be the case. The SAGE has advantages, but there is no availability of follow-up (only for Mexico, currently), and some years have passed since the baseline data was released. Cognitive status was not assessed with the state-of-the-art evaluation, but similar approaches to testing cognition have been used in epidemiologic studies. Finally, we recognize that having a multi-country approach could be in one hand, an advantage, but in the other also a source of variability. Further research using these data (and hopefully follow-ups) should be aimed at unveiling the relationships of social, cultural, and economic characteristics of each country when it comes to the relationship between frailty and cognition.
Conclusion
The CFS decision tree used to assess frailty shows differences with lower scores for cognitive tests across different countries, adding to the existing knowledge an easy-to-use tool to assess frailty on how cognition and physical health are closely related.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation. The datasets are available in the WHO repository, http://apps.who.int/healthinfo/systems/surveydata/index.php/catalog/sage/about.
Author contributions
RG-C performed the statistical analysis and wrote the first draft. JA-F and MB reviewed and added additional ideas. MP-Z had the original idea and wrote the first draft and added additional ideas for the statistical analysis. LG-R supervised all the stages of the manuscript and added additional ideas. All authors contributed to the article and approved the submitted version.
Funding
The publication of this paper was supported by Instituto Nacional de Geriatría, México.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2023.1166365/full#supplementary-material
Footnotes
References
1. Rodríguez-Mañas, L, Féart, C, Mann, G, Viña, J, Chatterji, S, Chodzko-Zajko, W, et al. Searching for an operational definition of frailty: a Delphi method based consensus statement: the frailty operative definition-consensus conference project. J Gerontol A. (2013) 68:62–7. doi: 10.1093/gerona/gls119
2. Archibald, MM, Lawless, MT, Ambagtsheer, RC, and Kitson, AL. Understanding consumer perceptions of frailty screening to inform knowledge translation and health service improvements. Age Ageing. (2021) 50:227–32. doi: 10.1093/ageing/afaa187
3. van Kan, GA, Rolland, Y, Houles, M, Gillette-Guyonnet, S, Soto, M, and Vellas, B. The assessment of frailty in older adults. Clin Geriatr Med. (2010) 26:275–86. doi: 10.1016/j.cger.2010.02.002
4. Thillainadesan, J, Scott, IA, and Le Couteur, DG. Frailty, a multisystem ageing syndrome. Age Ageing. (2020) 49:758–63. doi: 10.1093/ageing/afaa112
5. Inouye, SK, Studenski, S, Tinetti, ME, and Kuchel, GA. Geriatric syndromes: clinical, research, and policy implications of a core geriatric concept. J Am Geriatr Soc. (2007) 55:780–91. doi: 10.1111/j.1532-5415.2007.01156.x
6. Tinetti, ME, Inouye, SK, Gill, TM, and Doucette, JT. Shared risk factors for falls, incontinence, and functional dependence. Unifying the approach to geriatric syndromes. JAMA. (1995) 273:1348–53. doi: 10.1001/jama.1995.03520410042024
7. Vasquez-Goñi, GAJ, Papuico-Romero, BM, Urrunaga-Pastor, D, Runzer-Colmenares, FM, and Parodi, JF. The depressed frail phenotype as a risk factor for mortality in older adults: a prospective cohort in Peru. Heliyon. (2022) 8:e08640. doi: 10.1016/j.heliyon.2021.e08640
8. Ellwood, A, Quinn, C, and Mountain, G. Psychological and social factors associated with coexisting frailty and cognitive impairment: a systematic review. Res Aging. (2021) 44:448–64. doi: 10.1177/01640275211045603
9. Pearson, E, Siskind, D, Hubbard, RE, Gordon, EH, Coulson, EJ, and Warren, N. Frailty and severe mental illness: a systematic review and narrative synthesis. J Psychiatr Res. (2022) 147:166–75. doi: 10.1016/j.jpsychires.2022.01.014
10. Pedersen, BK. Physical activity and muscle-brain crosstalk. Nat Rev Endocrinol. (2019) 15:383–92. doi: 10.1038/s41574-019-0174-x
11. Wallace, LMK, Theou, O, Darvesh, S, Bennett, DA, Buchman, AS, Andrew, MK, et al. Neuropathologic burden and the degree of frailty in relation to global cognition and dementia. Neurology. (2020) 95:e3269–79. doi: 10.1212/WNL.0000000000010944
12. Ávila-Funes, JA, Pina-Escudero, SD, Aguilar-Navarro, S, Gutierrez-Robledo, LM, Ruiz-Arregui, L, and Amieva, H. Cognitive impairment and low physical activity are the components of frailty more strongly associated with disability. J Nutr Health Aging. (2011) 15:683–9. doi: 10.1007/s12603-011-0111-8
13. Veninsek, G, and Gabrovec, B. Management of frailty at individual level—clinical management: systematic literature review. Zdr Varst. (2018) 57:106–15. doi: 10.2478/sjph-2018-0014
14. Hayajneh, AA, and Rababa, M. The association of frailty with poverty in older adults: a systematic review. Dement Geriatr Cogn Disord. (2021) 50:407–13. doi: 10.1159/000520486
15. Wang, J, and Hulme, C. Frailty and socioeconomic status: a systematic review. J Public Health Res. (2021) 10:2036. doi: 10.4081/jphr.2021.2036
16. Duppen, D, van der Elst, MCJ, Dury, S, Lambotte, D, and de Donder, L, D-SCOPE. The social Environment’s relationship with frailty: evidence from existing studies. J Appl Gerontol. (2019) 38:3–26. doi: 10.1177/0733464816688310
17. Llibre Rodriguez, JJ, Prina, AM, Acosta, D, Guerra, M, Huang, Y, Jacob, KS, et al. The prevalence and correlates of frailty in urban and rural populations in Latin America, China, and India: a 10/66 population-based survey. J Am Med Dir Assoc. (2018) 19:287–295.e4. doi: 10.1016/j.jamda.2017.09.026
18. Prince, M, Graham, N, Brodaty, H, Rimmer, E, Varghese, M, Chiu, H, et al. Alzheimer disease International’s 10/66 dementia research group—one model for action research in developing countries. Int J Geriatr Psychiatry. (2004) 19:178–81. doi: 10.1002/gps.1059
19. Kowal, P, Chatterji, S, Naidoo, N, Biritwum, R, Fan, W, Lopez Ridaura, R, et al. Data resource profile: the World Health Organization study on global AGEing and adult health (SAGE). Int J Epidemiol. (2012) 41:1639–49. doi: 10.1093/ije/dys210
20. Moloney, E, Sezgin, D, O’Donovan, M, Adja, KYC, McGrath, K, Liew, A, et al. The diagnostic accuracy and clinimetric properties of screening instruments to identify frail older adults attending emergency departments: a protocol for a mixed methods systematic review and meta-analysis. Int J Environ Res Public Health. (2022) 19:1380. doi: 10.3390/ijerph19031380
21. Rockwood, K, Song, X, MacKnight, C, Bergman, H, Hogan, DB, McDowell, I, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. (2005) 173:489–95. doi: 10.1503/cmaj.050051
22. Thandi, M, Wong, ST, Aponte-Hao, S, Grandy, M, Mangin, D, Singer, A, et al. Strategies for working across Canadian practice-based research and learning networks (PBRLNs) in primary care: focus on frailty. BMC Fam Pract. (2021) 22:220. doi: 10.1186/s12875-021-01573-y
23. Theou, O, Pérez-Zepeda, MU, van der Valk, AM, Searle, SD, Howlett, SE, and Rockwood, K. A classification tree to assist with routine scoring of the clinical frailty scale. Age Ageing. (2021) 50:1406–11. doi: 10.1093/ageing/afab006
24. Turcotte, LA, Zalucky, AA, Stall, NM, Downar, J, Rockwood, K, Theou, O, et al. Baseline frailty as a predictor of survival after critical care: a retrospective cohort study of older adults receiving home care in Ontario Canada. Chest. (2021) 160:2101–11. doi: 10.1016/j.chest.2021.06.009
25. Gildner, TE, Liebert, MA, Kowal, P, Chatterji, S, and Snodgrass, JJ. Associations between sleep duration, sleep quality, and cognitive test performance among older adults from six middle income countries: results from the study on global ageing and adult health (SAGE). J Clin Sleep Med. (2014) 10:613–21. doi: 10.5664/jcsm.3782
26. Church, S, Rogers, E, Rockwood, K, and Theou, O. A scoping review of the clinical frailty scale. BMC Geriatr. (2020) 20:393. doi: 10.1186/s12877-020-01801-7
27. Wallace, L, Hunter, S, Theou, O, Fleming, J, Rockwood, K, and Brayne, C. Frailty and neuropathology in relation to dementia status: the Cambridge City over-75s cohort study. Int Psychogeriatr. (2021) 33:1035–43. doi: 10.1017/S1041610220003932
28. Wallace, LMK, Theou, O, Godin, J, Andrew, MK, Bennett, DA, and Rockwood, K. Investigation of frailty as a moderator of the relationship between neuropathology and dementia in Alzheimer’s disease: a cross-sectional analysis of data from the rush memory and aging project. Lancet Neurol. (2019) 18:177–84. doi: 10.1016/S1474-4422(18)30371-5
29. Borda, MG, Pérez-Zepeda, MU, Jaramillo-Jimenez, A, Chaudhuri, KR, Tovar-Rios, DA, Wallace, L, et al. Frailty in Parkinson’s disease and its association with early dementia: a longitudinal study. Parkinsonism Relat Disord. (2022) 99:51–7. doi: 10.1016/j.parkreldis.2022.05.004
30. Travers, J, Romero-Ortuno, R, Bailey, J, and Cooney, MT. Delaying and reversing frailty: a systematic review of primary care interventions. Br J Gen Pract. (2019) 69:e61–9. doi: 10.3399/bjgp18X700241
31. Apóstolo, J, Cooke, R, Bobrowicz-Campos, E, Santana, S, Marcucci, M, Cano, A, et al. Effectiveness of interventions to prevent pre-frailty and frailty progression in older adults: a systematic review. JBI Database System Rev Implement Rep. (2018) 16:140–232. doi: 10.11124/JBISRIR-2017-003382
32. Gildner, TE, Liebert, MA, Kowal, P, Chatterji, S, and Josh Snodgrass, J. Sleep duration, sleep quality, and obesity risk among older adults from six middle-income countries: findings from the study on global AGEing and adult health (SAGE). Am J Hum Biol. (2014) 26:803–12. doi: 10.1002/ajhb.22603
33. Siejka, TP, Srikanth, VK, Hubbard, RE, Moran, C, Beare, R, Wood, AG, et al. Frailty is associated with cognitive decline independent of cerebral small vessel disease and brain atrophy. J Gerontol A. (2022) 77:1819–26. doi: 10.1093/gerona/glac078
34. Kusumastuti, S, Hoogendijk, EO, Gerds, TA, Lund, R, Mortensen, EL, Huisman, M, et al. Do changes in frailty, physical functioning, and cognitive functioning predict mortality in old age? Results from the longitudinal aging study Amsterdam. BMC Geriatr. (2022) 22:193. doi: 10.1186/s12877-022-02876-0
35. Lin, SM, Apolinário, D, Vieira Gomes, GC, Cassales Tosi, F, Magaldi, RM, Busse, AL, et al. Association of Cognitive Performance with frailty in older individuals with cognitive complaints. J Nutr Health Aging. (2022) 26:89–95. doi: 10.1007/s12603-021-1712-5
36. ÃVila-Funes, JéA, Amieva, Héè, Barberger-Gateau, P, le Goff, Mé, Raoux, N, Ritchie, K, et al. Cognitive impairment improves the predictive validity of the phenotype of frailty for adverse health outcomes: the three-city study. J Am Geriatr Soc. (2009) 57:453–61. doi: 10.1111/j.1532-5415.2008.02136.x
37. Samper-Ternent, R, al Snih, S, Raji, MA, Markides, KS, and Ottenbacher, KJ. Relationship between frailty and cognitive decline in older Mexican Americans. J Am Geriatr Soc. (2008) 56:1845–52. doi: 10.1111/j.1532-5415.2008.01947.x
38. Dicpinigaitis, AJ, Hanft, S, Cooper, JB, Gandhi, CD, Kazim, SF, Schmidt, MH, et al. Comparative associations of baseline frailty status and age with postoperative mortality and duration of hospital stay following metastatic brain tumor resection. Clin Exp Metastasis. (2022) 39:303–10. doi: 10.1007/s10585-021-10138-3
Keywords: frailty, geriatric epidemiology, cognitive impairment, SAGE, multi-country study
Citation: García-Chanes RE, Avila-Funes JA, Borda MG, Pérez-Zepeda MU and Gutiérrez-Robledo LM (2023) Higher frailty levels are associated with lower cognitive test scores in a multi-country study: evidence from the study on global ageing and adult health. Front. Med. 10:1166365. doi: 10.3389/fmed.2023.1166365
Edited by:
Kenneth L. Seldeen, University at Buffalo, United StatesReviewed by:
Roberta Zupo, University of Bari Aldo Moro, ItalyCarlo Custodero, University of Bari Medical School, Italy
Copyright © 2023 García-Chanes, Avila-Funes, Borda, Pérez-Zepeda and Gutiérrez-Robledo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mario Ulises Pérez-Zepeda, bXBlcmV6QGluZ2VyLmdvYi5teA==