 Cancan Guo1†
Cancan Guo1† Mengtong Wan2†
Mengtong Wan2† Yue Wang3,4
Yue Wang3,4 Peijie Wang5Marissa Tousey-Pfarrer4Haoyang Liu1Liangming Yu1Lingqi Jian1Mengting Zhang1Ziqi Yang1Fenfen Ge3,4*‡
Peijie Wang5Marissa Tousey-Pfarrer4Haoyang Liu1Liangming Yu1Lingqi Jian1Mengting Zhang1Ziqi Yang1Fenfen Ge3,4*‡ Jun Zhang3*‡
Jun Zhang3*‡- 1West China School of Medicine, Sichuan University, Chengdu, China
- 2School of Medicine, Shanghai Jiao Tong University, Shanghai, China
- 3Mental Health Center, West China Hospital, Sichuan University, Chengdu, China
- 4Center of Public Health Sciences, Faculty of Medicine, University of Iceland, Reykjavík, Iceland
- 5School of Education, Tianjin University, Tianjin, China
Background: Intimate partner violence (IPV) has been associated with an elevated risk of multiple adverse birth outcomes, yet little is known about how specific IPV influences adverse birth outcomes. The aim of this study was to examine the association between IPV during pregnancy and adverse birth outcomes (i.e., preterm birth, low birth weight, and stillbirth).
Methods: Systematic searches were conducted using four databases: EMBASE, Web of Science, PubMed, and CINAHL for observational studies published from 1 January 2011 to 31 August 2021. Two reviewers independently carried out the literature search, study selection, data extraction, assessment of the study, and risk of bias assessment; disagreements were resolved by a third reviewer. A random-effect model was used to calculate the odds ratio (OR) with a 95% confidence interval (CI) for preterm birth, low birth weight, and stillbirth. I2 statistic accompanied by chi-square p-value was used to assess heterogeneity, and funnel plot and Peter's test were used to assess publication bias.
Results: In total, 23 studies met the inclusion criterion. IPV was associated with preterm birth (OR = 1.84; 95% CI: 1.37–2.49; I2 = 88%), low birth weight (OR = 2.73; 95% CI: 1.66–4.48; I2 = 95%), and stillbirth (OR = 1.74; 95% CI: 0.86–3.54; I2 = 64%). We attained comparable results among all specific IPV including physical, sexual, emotional, and mixed.
Conclusion: Intimate partner violence and specific IPV during pregnancy were significantly associated with adverse birth outcomes, especially for physical IPV. An urgent need for greater action to prevent or intervene in IPV during pregnancy is warranted.
Systematic review registration: CRD42021282936, https://www.crd.york.ac.uk/prospero/.
1. Introduction
Intimate partner violence (IPV) is a major and common public health problem in society globally (1). IPV refers to physical, sexual violence, and psychological aggression by a current or former intimate partner (2). A national prevalence estimate showed that approximately 33% of Americans have experienced IPV at some point in their lifetime (3). Specifically, an international survey conducted in 2005 by the World Health Organization (WHO) reported that the prevalence of IPV during pregnancy ranged from 4 to 12% (1). Whether IPV occurs during pregnancy or not, it could increase the risk of physical and mental disorders in both women and their children.
Previous studies have explored the associations between IPV and adverse birth outcomes including preterm birth, low birth weight, and stillbirth (4, 5). The relationship between IPV and adverse birth outcomes is complex. Although most researchers have found a positive association between IPV and adverse birth outcomes, some have not (6). For example, both Hill et al. (7) and Berhanie et al. (8) found an association between IPV and preterm birth, while Laelago et al. (6) did not. Pallitto et al. found no significant association between abuse and low birth weight after adjusting for confounding factors (9). Methodological limitations including search strategy, respondent selection, and mode effects may prevent drawing conclusions.
Various types of IPV have been associated with adverse birth outcomes, including physical and sexual IPV (10). Previous systematic reviews have been focused on this topic, with some defining violence as physical or sexual IPV, and found that IPV was strongly related to low birth weight as well as preterm birth, while intrauterine growth restriction was not significantly associated with IPV (7). There has been relatively better research attention on emotional or physiological IPV because of their less visible immediate impact. However, evidence is also emerging for the adverse birth outcomes of emotional or psychological-based IPV (11, 12).
We conducted a comprehensive and rigorous meta-analysis to explore the association between IPV and adverse birth outcomes. Our main aims were to: (1) evaluate the association between IPV during pregnancy and three adverse birth outcomes: preterm birth, low birth weight, and stillbirth, which were leading causes of neonatal morbidity and mortality; (2) explore the relation of specific types of IPV with adverse birth outcomes.
2. Inclusion criteria
The review included studies reported on IPV during pregnancy considering every pregnant woman as a population. The exposure to IPV was defined as experiencing any physical, sexual, or emotional abuse perpetrated by a current or former partner. We defined women who experienced more than one type of IPV at the same time as mixed IPV in the present study. Women who reported not experiencing IPV were considered as a control in this review. The outcome of the review included preterm birth, low birth weight, and stillbirth. Preterm birth refers to a baby born before 37 weeks of gestation, whereas a low birth weight is referring to a baby born with a weight of < 2,500 grams. A stillbirth is defined as a baby dying after 28 weeks of pregnancy but before or during delivery.
In this review, all quantitative observational studies reported on the relationship between IPV during pregnancy and the outcomes of interest were included. Meanwhile, the articles included in the present study had to meet the following criteria: (1) English language; (2) published in/after 1 January 2011; (3) raw data included. However, observational studies that did not report on original research (i.e., conference abstract, comment, editorial or letter, review) or just qualitative studies were excluded.
3. Methods
3.1. Search strategy
We searched four databases including EMBASE, Web of Science, PubMed, and CINAHL from 1 January 2011 to 31 August 2021. We planned to summarize contemporary literature through this review, thus, the included studies were limited to the past 10 years, considering that the birth outcomes may be influenced by environmental, behavioral, and sociodemographic factors (13–15). In addition, eligible articles were also attained by reviewing references. We used a combination of keywords and medical subject headings (MeSH) to search: intimate partner violence, partner abuse, spouse abuse, domestic abuse, battered women, preterm/premature birth/labor/delivery, low birth weight, and stillbirth. The detailed information is described in Supplementary Table 1.
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (16). We have registered this study in the International Prospective Register of Systematic Reviews (PROSPERO) system (Registration No.: CRD42021282936), and no similar reviews were listed in the PROSPERO database before registration.
3.2. Data extraction
Two independent reviewers (Guo and Wan) searched for articles that met the inclusion criteria, obtained potentially relevant articles through a preliminary screening of the titles and abstracts, and then read the full text of the literature and determined its eligibility through the exclusion criteria. For any discrepancies, a third reviewer (Ge) was consulted, and we would reach a consensus. Then, two reviewers (Guo and Wan) independently extracted the data from the eligible studies using a pre-prepared form. Extracted data were reviewed and verified by the reviewer (Ge). The form mainly included study characteristics (authors, year of publication, study design, sample size, and study location), type of IPV (physical, sexual, and emotional) and the abuse assessment tool, and the adverse birth outcomes (i.e., preterm birth, low birth weight, and stillbirth).
3.3. Assessment of study quality
We critically appraised all included studies using the Joanna Briggs Institute (JBI) checklist for cross-sectional studies, the JBI checklist for cohort studies, and the JBI checklist for case–control studies (17). Briefly, the checklist for cross-sectional study, cohort study, and case–control study includes a total of eight, 11, and 10 items, respectively. Each item is divided into three grades: 1 = Yes, 2 = No, 3 = Not applicable, with lower scores reflecting higher quality (ranging from 8 to 24 for cross-sectional studies, 11 to 33 for cohort studies, and 10 to 30 for case–control studies). Guo and Wan conducted quality assessments independently when extracting the data for meta-analysis. Any discrepancies were discussed and reached a consensus among the different reviewers.
3.4. Data synthesis and statistical analysis
We calculated the odds ratio (OR) with a corresponding 95% confidence interval (CI) for preterm birth, low birth weight, and stillbirth using a random-effect model, which is suitable where there is heterogeneity between included studies. Heterogeneity across studies was assessed using an I2 statistic accompanied by a chi-square p-value. Heterogeneity was assigned adjectives of low, moderate, and high to I2 values of 25, 50, and 75% (18). Publication bias was assessed using a funnel plot and Peter's test (19). We used leave-one-out sensitivity analysis to explore the influence of small sample size studies or low-quality studies. Meta-regression and subgroup analysis were performed to explore the source of heterogeneity (I2 ≥ 50%). The aforementioned analyses were based on the year of publication (as a continuous variable), development level (developed countries and developing countries), study quality (continuous), and measurement of IPV (self-report questionnaires and face-to-face interviews). All analyses were conducted in RStudio-4.0 using the meta package.
4. Results
4.1. Study and sample characteristics
A total of 1,403 articles were identified through the four databases. After removing the duplicates and preliminary screening titles and abstracts, 73 studies were selected and read in full text to assess the eligibility along with five studies identified from the references lists. Ultimately, 23 studies were included, meeting the aforementioned inclusion and exclusion criteria, and providing the raw data that needed to be included in the meta-analysis (Figure 1).
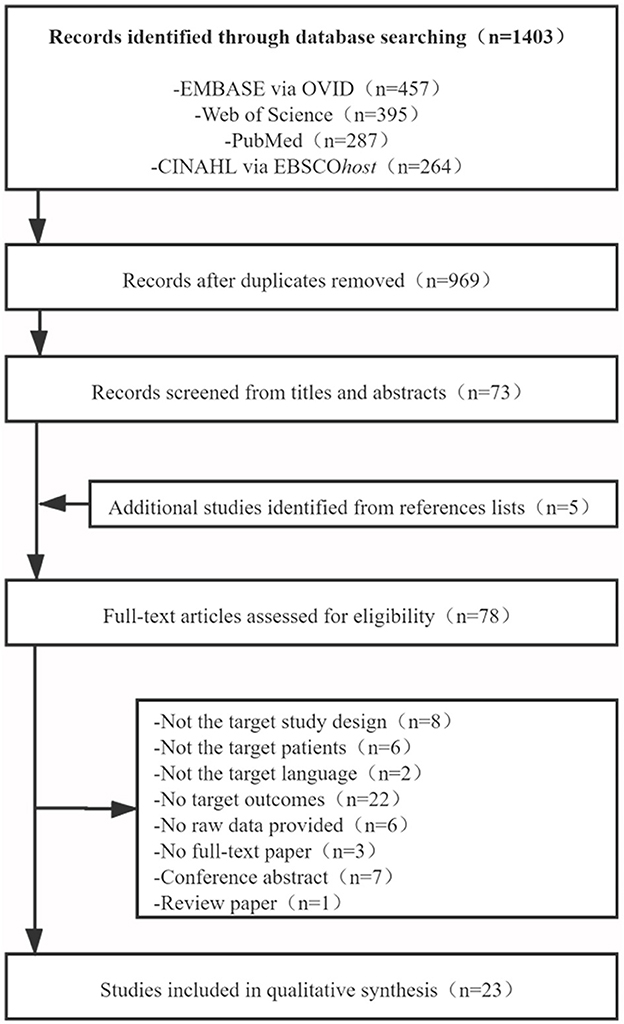
Figure 1. Flow diagram of study selection.
Table 1 demonstrates the study design and sample characteristics of included studies. In total, 23 studies included a total of 42,089 middle-aged (ranging from 25 to 35) adult females. A total of 11 studies were conducted in Asia, eight studies were conducted in Africa, two studies were conducted in North America, one study was conducted in South America, and the last study was conducted in Europe. All eligible research articles are observational studies. Among the included studies, cross-sectional and cohort studies were each represented by 11 articles, while the remaining article was a case–control study. IPV was measured by self-report questionnaires in 18 studies (the most used was the modified WHO Domestic Violence Questionnaire, eight studies), and five studies were obtained through face-to-face interviews with doctors or nurses in hospitals. The majority of studies focused on physical IPV and single birth outcomes, mostly preterm as a birth outcome.
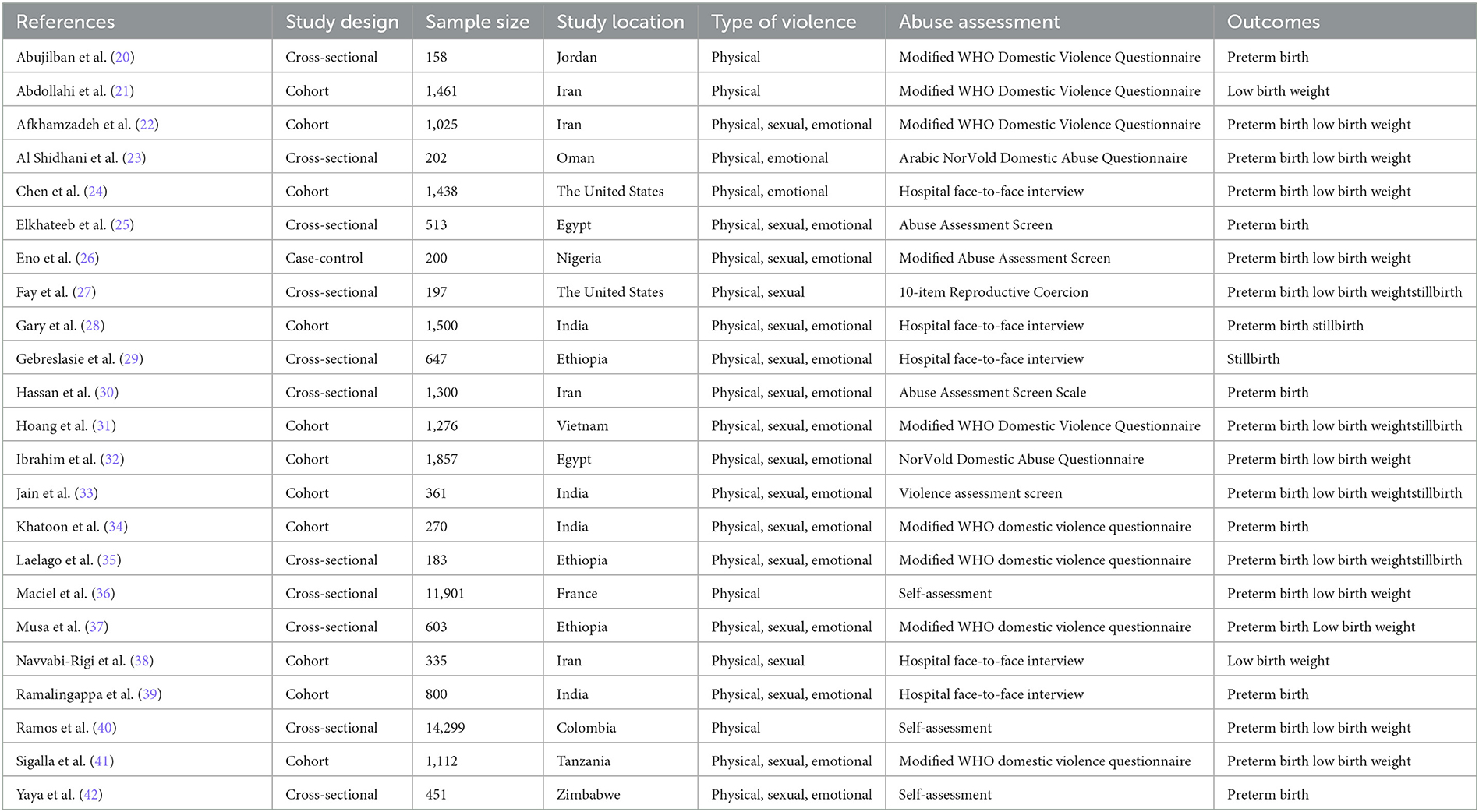
Table 1. Characteristics of studies included in the meta-analysis of IPV and birth outcomes.
4.2. Risk of bias in individual studies
As demonstrated in Figure 2A, all included cross-sectional studies indicated the criteria for inclusion of the sample in a clear way; the study subjects and settings were described in detail; the exposure was measured in a valid and reliable way; objective and standard criteria were used for the measurement of the condition; confounding factors were identified and dealt with appropriate strategies; and appropriate statistical analysis was used. As shown in Figure 2B, the included cohort studies indicated that the two groups were similar and recruited from the same population; the exposures were measured similarly to assign people to both exposed and unexposed groups; the outcomes were measured in a valid and reliable way; the follow-up time was reported and sufficient for outcomes to occur; and appropriate statistical analysis was used. Meanwhile, six of 11 studies accounted for all important confounding factors and dealt with them. Most of the included studies described the reasons to lose follow-up and utilized strategies to address incomplete follow-up. As can be seen from Figure 2C, Eno's study indicated the groups were comparable other than the presence of disease in cases or the absence of disease in controls; cases and controls were matched appropriately, and the same criteria were used for the identification of cases and controls; both exposure and outcome were measured in a standard, valid, and reliable way; the exposure period was long enough, and appropriate statistical analysis was used. This study did not indicate the confounding factors. Overall, the summary quality of all included studies was assessed as moderate to high.
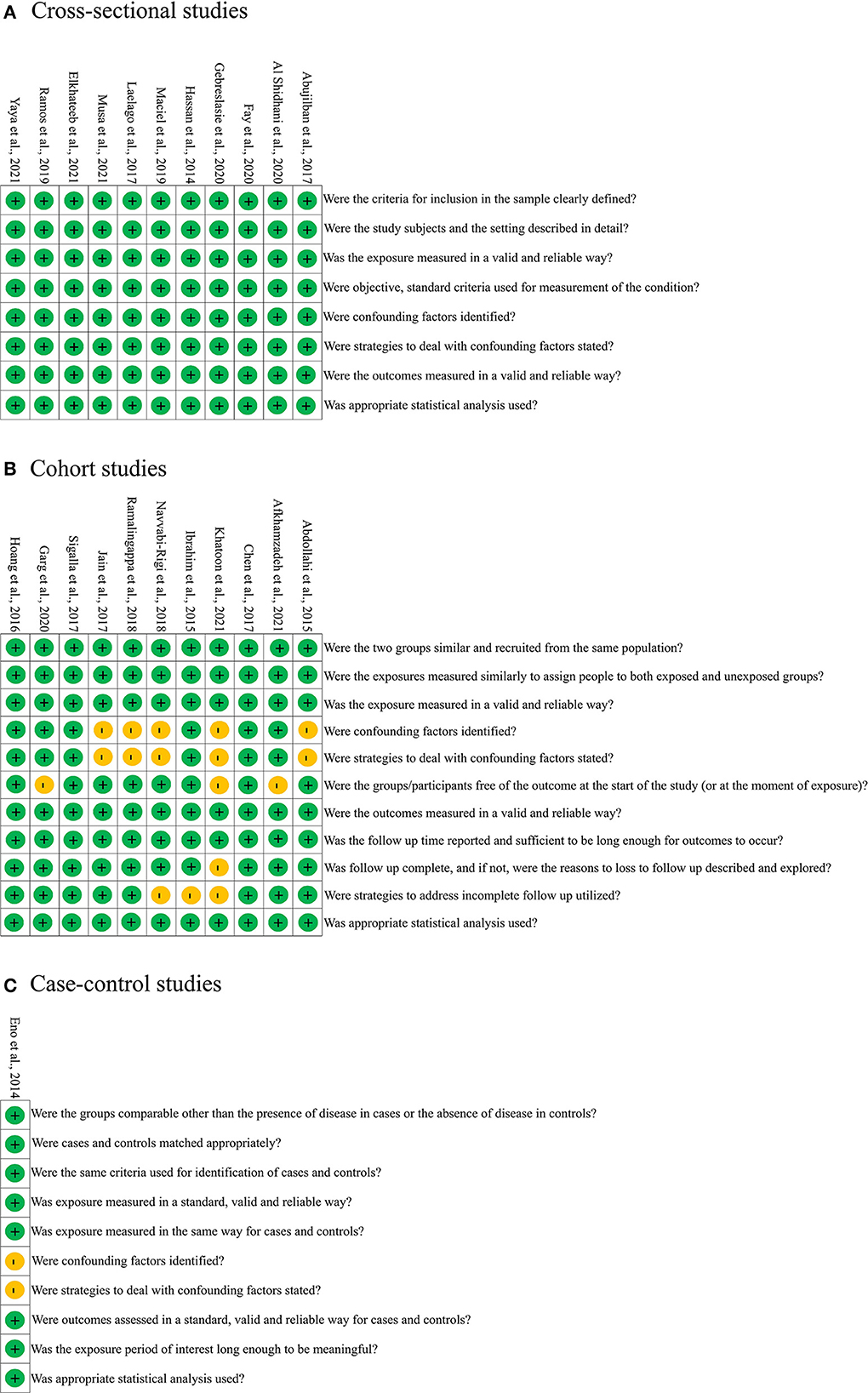
Figure 2. Risk of bias for the included cross-sectional (A), cohort (B), and case-control (C) studies.
4.3. Associations between IPV and risk of birth outcomes
As shown in Figure 3A, the association between IPV during pregnancy and preterm birth has been reported in 18 studies. Compared with women who did not experience IPV, victims of IPV during pregnancy were nearly twice as likely to give birth to a premature infant (OR = 1.84; 95% CI: 1.37–2.49), with high heterogeneity (I2 = 88%, p < 0.01). Based on 13 studies, the pooled OR for IPV associated with low birth weight was 2.73 (95% CI: 1.66–4.48) and heterogeneity is 95% (p < 0.01) (Figure 3B). As for stillbirth, six of the included studies showed that women who experienced IPV during pregnancy were more likely to experience it (OR = 1.74; 95% CI: 0.86–3.54; I2 = 64%) (Figure 3C).
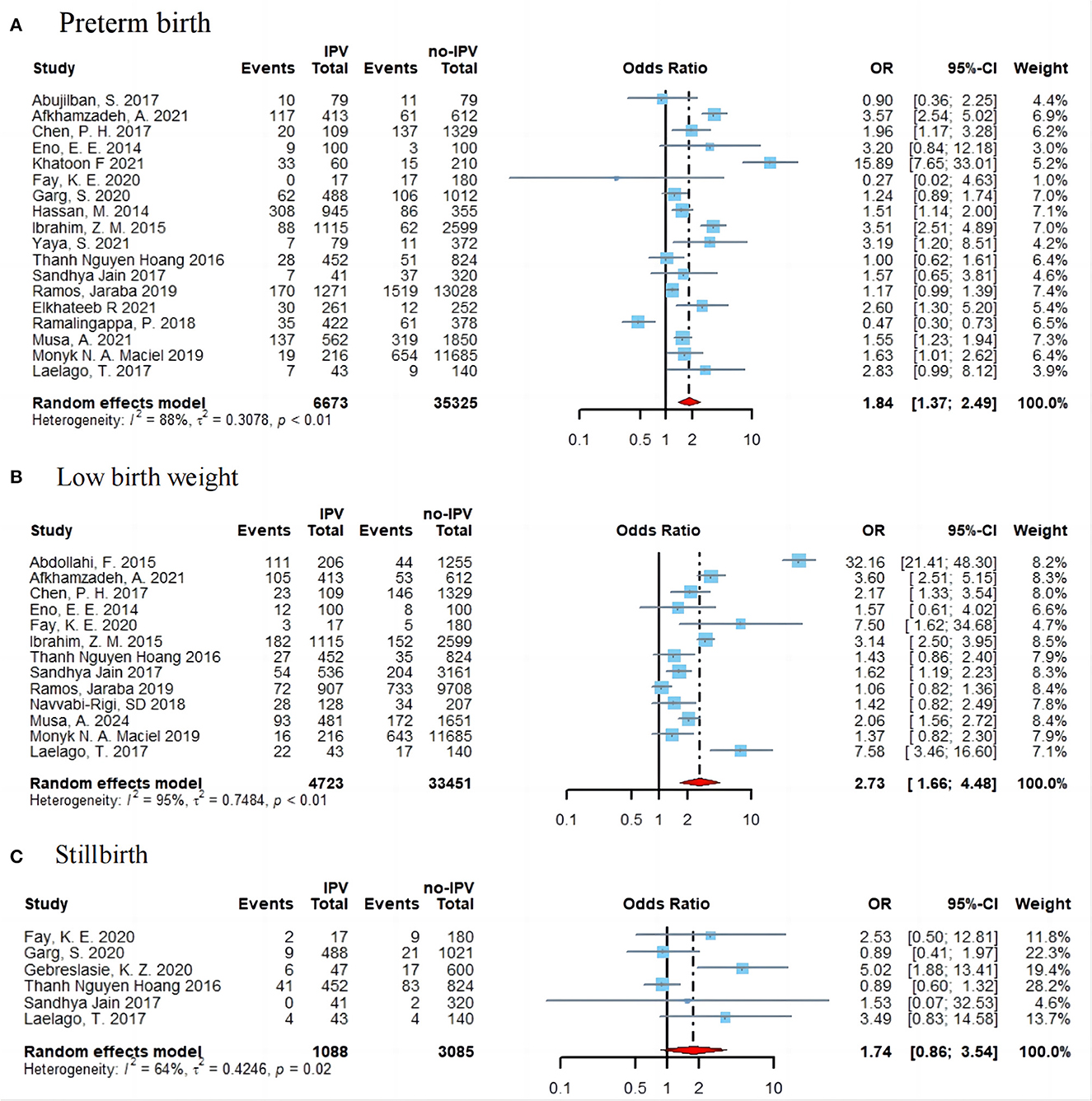
Figure 3. Forest plot of effect estimates for IPV in pregnancy and preterm birth (A), low birth weight (B), and stillbirth (C).
4.4. Associations between specific IPV and risk of birth outcomes
As shown in Figure 4, the association between preterm birth and low birth weight was still significant by specific IPV types. We did not explore the association between specific IPV types and stillbirth due to a small number of available studies. For the preterm birth (Figure 4A), significant associations were found in physical IPV (OR = 2.11; 95% CI: 1.17–3.80; I2 = 97%), sexual IPV (OR = 2.64; 95% CI: 1.44–4.82; I2 = 67%), emotional IPV (OR = 2.12; 95% CI 1.08–4.16; I2 = 80%), and mixed IPV (OR = 1.90; 95% CI: 1.29–2.80; I2 = 85%). For the low birth weight, the ORs for the association of the specific IPV (physical, sexual, emotional, and mixed IPV) were, respectively, 3.69 (95% CI: 1.51–9.02), 2.64 (95% CI: 1.44–4.82), 2.12 (95% CI: 1.08–4.15), and 2.11 (95% CI: 1.54–2.90) (Figure 4B).
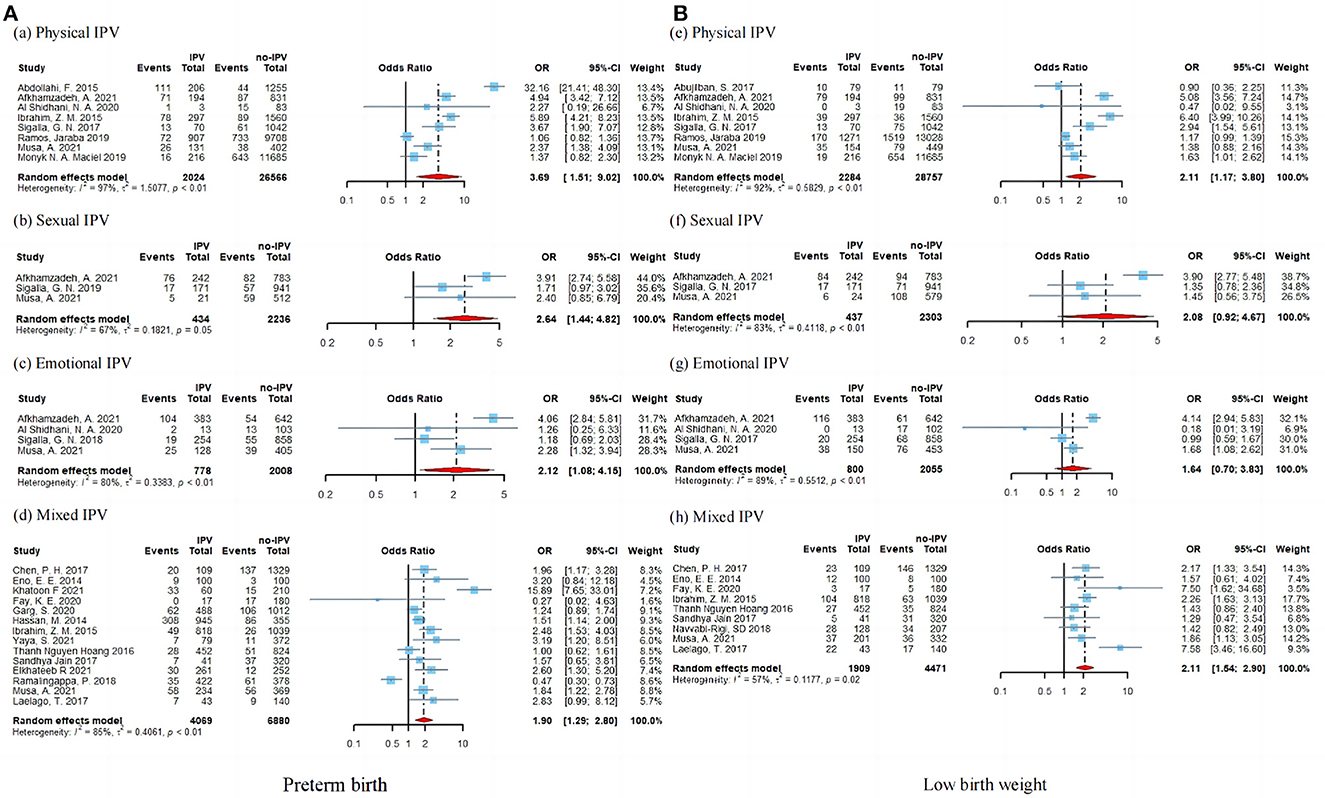
Figure 4. Subgroup analysis of preterm birth (A) and low birth weight (B) according to IPV type.
4.5. Publication bias, meta-regression, and subgroup analyses
Visual inspection of the funnel plots for preterm birth, low birth weight, and stillbirth showed little publication bias (Supplementary Figure 1). Peter's test is 0.33 and 0.30 for preterm birth and low birth weight outcomes, respectively. Due to the small number of studies (< 10 studies), we were unable to conduct Peter's test for stillbirth outcomes. We did not significantly alter the pooled OR for preterm birth, low birth weight, and stillbirth in the leave-one-out sensitivity analysis (Supplementary Figure 2). We performed univariate meta-regression models and subgroup analyses to detect the possible sources of heterogeneity according to the year of publication, level of development, study quality, and measurement of IPV, but none of the above variables were found to be statistically significant (p-value > 0.05). The details are shown in Supplementary Figure 3.
5. Discussion
The aim of the present study is to synthesize the recent studies involving the association between IPV during pregnancy and adverse birth outcomes. At the global scale, all subtypes of IPV were associated with an increased risk of adverse birth outcomes, especially for physical IPV. To evaluate the robustness of our findings, we calculated the association in different subgroups, including the development level, study quality, and measurement of IPV.
Consistent with previous studies, we found that IPV is a risk factor that can lead to severe birth outcomes involving preterm birth, low birth weight, and stillbirth (43, 44). Donovan et al. (43) found that women exposed to IPV during pregnancy were more likely to deliver a premature or low birth weight infant than women who did not experience IPV. In addition, there is also a positive association between IPV during pregnancy and stillbirth (44). Although the mechanism of the associations between IPV and adverse birth outcomes was unclear, previous studies explored it from the following aspects. First, physical IPV can directly affect fetal growth through trauma (45), which may explain the stronger association between physical IPV and adverse birth outcomes in the subgroup analysis. One possible reason is that violence may lead to pregnancy complications, such as placental damage, uterine contractions, and premature rupture of membranes (45, 46) and then followed by preterm birth and low birth weight. Second, sexual violence can increase the risk of sexually transmitted diseases and genitourinary infections (47). Third, maltreatment can lead to anxiety and depression in pregnant women, on the one hand (48, 49), and increased behavioral risk factors associated with adverse birth outcomes, on the other hand, such as maternal smoking, alcohol abuse, or less weight gain during pregnancy (50, 51). Premature rupture of membranes, depression, smoking, drinking, and other factors mentioned above are all risk factors for adverse birth outcomes (13–15), especially for preterm birth and low birth weight. We obtained comparable results across different subgroups (e.g., development level or study quality) and meta-regression analyses, which suggested that the observed associations could not be modified by study-level characteristics.
This study evaluated the association between IPV during pregnancy and preterm birth, low birth weight, and stillbirth and showed that IPV during pregnancy can not only harm the pregnant woman herself but also adversely affect the birth outcomes, which can more intuitively present the severity of IPV during pregnancy, so as to alert the health decision-makers and healthcare providers to its attention. The proportion of eligible birth outcomes is also an indicator of a country's socioeconomic development. Therefore, based on the results of this study and reality, we are likely to put forward a proposal; women who experience IPV during pregnancy should be identified as early as possible and given care and support to avoid more serious physical and emotional damage and worse birth outcomes. Prenatal care can be an important entry point for identifying violence among pregnant women, as under normal circumstances most people receive at least one or more prenatal care visits. Paradoxically, prenatal care and health services specifically for IPV during pregnancy are not available in almost all countries. IPV raises many ethical and legal issues, and to prevent and intervene in IPV during pregnancy, we must collaborate between healthcare, political, and social justice systems.
This meta-analysis has several strengths including considering stillbirth as an adverse birth outcome in our study. Although prior meta-analyses existed, none included stillbirth as an interesting outcome (7, 43, 44, 52, 53). Second, having a large sample size and detailed reported subtypes of IPV enabled us to assess the association between specific IPV (i.e., physical IPV, sexual IPV, emotional IPV, and mixed IPV) and adverse birth outcomes. Furthermore, we did some subgroup analysis (e.g., publication year, study location, and study quality) to avoid a spurious association. Our study has some limitations. First, the heterogeneity was high in our meta-analysis. This may be attributed to the cultural differences across countries. In some low-income countries (e.g., Ethiopia, Iran, and Tanzania), 81% of female victims reported that IPV is justified (54, 55); however, in some countries, the victims do not think so, such as Israel (56). Second, birth outcomes may be influenced by some behavior (e.g., smoking), maternal (e.g., overweight and obesity), and environmental (e.g., high temperature) factors (57–59). However, existing studies were not able to provide some detailed behavioral, maternal, and environmental information. Thus, it is difficult for us to control these potential confounders in our study.
6. Conclusion
This meta-analysis summarized all literature on the association between IPV during pregnancy and adverse birth outcomes in the last decade. Women who experienced IPV during pregnancy had a higher risk of adverse birth outcomes when compared to women who have not been exposed to IPV during pregnancy. All specific IPV, including physical, sexual, emotional, and mixed, were associated with adverse birth outcomes. In the future, more research on IPV during pregnancy is warranted and there is also an urgent need for greater action to prevent or intervene in IPV during pregnancy.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
FG and JZ were responsible for the study's concept and design. CG and MW independently extracted the data. FG reviewed and verified extracted data. CG, MW, PW, and FG cleaned the data and performed the analyses. CG, MW, YW, MT-P, and FG drafted the article. All authors contributed to the interpretation of data. All authors read and approved the final manuscript.
Funding
This study was financially supported by the project Key Research Project, Science and Technology Department of Sichuan Province (No. 2020YFS0232, JZ).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2023.1140787/full#supplementary-material
References
1. Organization WH. WHO multi-country study on women's health and domestic violence against women: initial results on prevalence, health outcomes and women's responses. Geneva: World Health Organization (2005).
2. Breiding M, Basile KC, Smith SG, Black MC, Mahendra RR. Intimate Partner Violence Surveillance Uniform Definitions and Recommended Data Elements. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention (1999).
3. Smith SG, Basile KC, Gilbert LK, Merrick MT, Patel N, Walling M, et al. National intimate partner and sexual violence survey (NISVS): 2010-2012 state report. (2017).
4. Alhusen JL, Ray E, Sharps P, Bullock L. Intimate partner violence during pregnancy: maternal and neonatal outcomes. J Women's Health. (2015) 24:100–06. doi: 10.1089/jwh.2014.4872
5. Dhar D, McDougal L, Hay K, Atmavilas Y, Silverman J, Triplett D, et al. Associations between intimate partner violence and reproductive and maternal health outcomes in Bihar, India: a cross-sectional study. Reprod Health. (2018) 15:1–14. doi: 10.1186/s12978-018-0551-2
6. Laelago T, Belachew T, Tamrat M. Effect of intimate partner violence on birth outcomes. Afr Health Sci. (2017) 17:681–9. doi: 10.4314/ahs.v17i3.10
7. Hill A, Pallitto C, McCleary-Sills J, Garcia-Moreno C. A systematic review and meta-analysis of intimate partner violence during pregnancy and selected birth outcomes. Int J Gynecol Obstetr. (2016) 133:269–76. doi: 10.1016/j.ijgo.2015.10.023
8. Berhanie E, Gebregziabher D, Berihu H, Gerezgiher A, Kidane G. Intimate partner violence during pregnancy and adverse birth outcomes: a case-control study. Reprod Health. (2019) 16:1–9. doi: 10.1186/s12978-019-0670-4
9. Pallitto CC, Campbell JC, O'Campo P. Is intimate partner violence associated with unintended pregnancy? A review of the literature. Trauma, Violence, Abuse. (2005) 6:217–35. doi: 10.1177/1524838005277441
10. Silverman JG, Gupta J, Decker MR, Kapur N, Raj A. Intimate partner violence and unwanted pregnancy, miscarriage, induced abortion, and stillbirth among a national sample of Bangladeshi women. BJOG. (2007) 114:1246–52. doi: 10.1111/j.1471-0528.2007.01481.x
11. Martin-de-Las-Heras S, Velasco C, Luna-Del-Castillo J, Khan KS. Maternal outcomes associated to psychological and physical intimate partner violence during pregnancy: A cohort study and multivariate analysis. PLoS ONE. (2019) 14:e0218255. doi: 10.1371/journal.pone.0218255
12. Yu H, Jiang X, Bao W, Xu G, Yang R, Shen M. Association of intimate partner violence during pregnancy, prenatal depression, and adverse birth outcomes in Wuhan, China. BMC Pregn Childbirth. (2018) 18:1–7. doi: 10.1186/s12884-018-2113-6
13. Shen ZZ, Wang YW, Ma S, Zhan YL, Wu SS, Feng YH, et al. Risk factors for preterm birth, low birth weight and small for gestational age: a prospective cohort study. Zhonghua liu xing bing xue za zhi. (2019) 40:1125–9. doi: 10.3760.cma.j.issn/0254-6450.2019.09.020
14. Li X, Gao R, Dai X, Liu H, Zhang J, Liu X, et al. The association between symptoms of depression during pregnancy and low birth weight: a prospective study. BMC Pregn Childbirth. (2020) 20:1–7. doi: 10.1186/s12884-020-2842-1
15. Tamura N, Hanaoka T, Ito K, Araki A, Miyashita C, Ito S, et al. Different risk factors for very low birth weight, term-small-for-gestational-age, or preterm birth in Japan. Int J Environ Res Public Health. (2018) 15:369. doi: 10.3390/ijerph15020369
16. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
17. Ma LL, Wang YY, Yang ZH, Huang D, Weng H, Zeng XT. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: what are they and which is better? Milit Med Res. (2020) 7:7. doi: 10.1186/s40779-020-00238-8
18. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
19. Peters JL, Sutton AJ, Jones DR, Abrams KR, Rushton L. Comparison of two methods to detect publication bias in meta-analysis. Jama. (2006) 295:676–80. doi: 10.1001/jama.295.6.676
20. Abujilban S, Mrayan L, Al-Modallal H, Isaa E. Effects of intimate partner physical violence on newborns' birth outcomes among jordanian birthing women. J Interpers Violence. (2017) 32:3822–38. doi: 10.1177/0886260515603975
21. Abdollahi F, Abhari FR, Delavar MA, Charati JY. Physical violence against pregnant women by an intimate partner, and adverse pregnancy outcomes in Mazandaran Province, Iran. J Family Community Med. (2015) 22:13–8. doi: 10.4103/2230-8229.149577
22. Afkhamzadeh A, Rahmani K, Yaghubi R, Ghadrdan M, Faraji O. Adverse perinatal outcomes of intimate partner violence during pregnancy. Int J Human Rights Healthcare. (2021) 14:465–76. doi: 10.1108/IJHRH-08-2019-0067
23. Al Shidhani NA, Al Kendi AA, Al Kiyumi MH. Prevalence, risk factors and effects of domestic violence before and during pregnancy on birth outcomes: An observational study of literate omani women. Int J Womens Health. (2020) 12:911–25. doi: 10.2147/IJWH.S272419
24. Chen PH, Rovi S, Vega ML, Barrett T, Pan KY, Johnson MS. Birth outcomes in relation to intimate partner violence. J Natl Med Assoc. (2017) 109:238–45. doi: 10.1016/j.jnma.2017.06.017
25. Elkhateeb R, Abdelmeged A, Ahmad S, Mahran A, Abdelzahar WY, Welson NN, et al. Impact of domestic violence against pregnant women in Minia governorate, Egypt: a cross sectional study. BMC Preg Childbirth. (2021) 21:535. doi: 10.1186/s12884-021-03953-9
26. Eno EE, Fawole AA, Aboyeji AP, Adesina KT, Adeniran AS. Domestic violence and obstetric outcome among pregnant women in Ilorin, north central Nigeria. Int J Gynaecol Obstet. (2014) 125:170–1. doi: 10.1016/j.ijgo.2013.11.007
27. Fay KE, Yee LM. Birth outcomes among women affected by reproductive coercion. J Midwifery Womens Health. (2020) 65:627–33. doi: 10.1111/jmwh.13107
28. Garg S, Rustagi R, Singh MM, Engtipi K. Effect of intimate partner violence on maternal and birth outcomes of pregnancy among antenatal clinic attendees in Delhi: A prospective observational study. Indian J Community Med. (2020) 45:501–5. doi: 10.4103/ijcm.IJCM_538_19
29. Gebreslasie KZ, Weldemariam S, Gebre G, Mehari MA. Intimate partner violence during pregnancy and risk of still birth in hospitals of Tigray region Ethiopia. Ital J Pediatr. (2020) 46:107. doi: 10.1186/s13052-020-00857-w
30. Hassan M, Kashanian M, Hassan M, Roohi M, Yousefi H. Maternal outcomes of intimate partner violence during pregnancy: study in Iran. Public Health. (2014) 128:410–5. doi: 10.1016/j.puhe.2013.11.007
31. Hoang TN, Van TN, Gammeltoft T, Meyrowitsch D, Nguyen Thi Thuy H, Rasch V. Association between intimate partner violence during pregnancy and adverse pregnancy outcomes in Vietnam: A prospective cohort study. PLoS ONE. (2016) 11:e0162844. doi: 10.1371/journal.pone.0162844
32. Ibrahim ZM, Sayed Ahmed WA, El-Hamid SA, Hagras AM. Intimate partner violence among Egyptian pregnant women: incidence, risk factors, and adverse maternal and fetal outcomes. Clin Exp Obstet Gynecol. (2015) 42:212–9
33. Jain S, Varshney K, Vaid NB, Guleria K, Vaid K, Sharma N. A hospital-based study of intimate partner violence during pregnancy. Int J Gynaecol Obstet. (2017) 137:8–13. doi: 10.1002/ijgo.12086
34. Khatoon F, Fatima M, Zaidi Z, Nishad S, Ahmad A. Domestic violence during pregnancy: evaluating the impact on maternal and perinatal health-a pilot study in Uttar Pradesh. J Obstet Gynaecol India. (2021) 71:386–92. doi: 10.1007/s13224-021-01463-4
35. Laelago T, Belachew T, Tamrat M. Effect of intimate partner violence on birth outcomes. Afr Health Sci. (2017) 17:681–9. doi: 10.4314/ahs.v17i3
36. Maciel MNA, Blondel B, Saurel-Cubizolles MJ. Physical violence during pregnancy in france: frequency and impact on the health of expectant mothers and new-borns. Matern Child Health J. (2019) 23:1108–16. doi: 10.1007/s10995-019-02747-y
37. Musa A, Chojenta C, Loxton D. The association between intimate partner violence and low birth weight and preterm delivery in eastern Ethiopia: Findings from a facility-based study. Midwifery. (2021) 92:102869. doi: 10.1016/j.midw.2020.102869
38. Navvabi-Rigi S, Moudi Z, Sheikhi Z, Moudi F. The association between Intimate Partner Violence (IPV) during pregnancy and birth weight. Prensa Medica Argentina. (2018).
39. Ramalingappa AP, Anjali R, Sowmya K. Domestic violence in pregnancy and its adverse maternal and perinatal outcome: A prospective cohort study. Religion. (2018) 401:94–9
40. Jaraba SMR, Garcés-Palacio IC. Association between violence during pregnancy and preterm birth and low birth weight in Colombia: Analysis of the demographic and health survey. Health Care Women Int. (2019) 40:1149–69. doi: 10.1080/07399332.2019.1566331
41. Sigalla GN, Mushi D, Meyrowitsch DW, Manongi R, Rogathi JJ, Gammeltoft T, et al. Intimate partner violence during pregnancy and its association with preterm birth and low birth weight in Tanzania: A prospective cohort study. PLoS ONE. (2017) 12:e0172540. doi: 10.1371/journal.pone.0172540
42. Yaya S, Odusina EK, Adjei NK, Uthman OA. Association between intimate partner violence during pregnancy and risk of preterm birth. BMC Public Health. (2021) 21:1610. doi: 10.1186/s12889-021-11625-8
43. Donovan BM, Spracklen CN, Schweizer ML, Ryckman KK, Saftlas AF. Intimate partner violence during pregnancy and the risk for adverse infant outcomes: a systematic review and meta-analysis. BJOG. (20161) 23:1289–99. doi: 10.1111/1471-0528.13928
44. Han A, Stewart DE. Maternal and fetal outcomes of intimate partner violence associated with pregnancy in the Latin American and Caribbean region. Int J Gynecol Obstetr. (2014) 124:6–11. doi: 10.1016/j.ijgo.2013.06.037
45. Heaman MI. Relationships between physical abuse during pregnancy and risk factors for preterm birth among women in Manitoba. J Obstetr Gynecol Neonatal Nurs. (2005) 34:721–31. doi: 10.1177/0884217505281906
46. Curry MA, Harvey SM. Stress related to domestic violence during pregnancy and infant birth weight. Empowering survivors of abuse: Health care for battered women and their children. London: Sage Publications, Inc. (1998) 98–108.
47. Campbell JC. Health consequences of intimate partner violence. Lancet. (2002) 359:1331–6. doi: 10.1016/S0140-6736(02)08336-8
48. Mahenge B, Likindikoki S, Stöckl H, Mbwambo J. Intimate partner violence during pregnancy and associated mental health symptoms among pregnant women in T anzania: a cross-sectional study. BJOG. (2013) 120:940–7. doi: 10.1111/1471-0528.12185
49. Taylor CA, Guterman NB, Lee SJ, Rathouz PJ. Intimate partner violence, maternal stress, nativity, and risk for maternal maltreatment of young children. Am J Public Health. (2009) 99:175–83. doi: 10.2105/AJPH.2007.126722
50. Sanchez SE, Alva AV, Diez Chang G, Qiu C, Yanez D, Gelaye B, et al. Risk of spontaneous preterm birth in relation to maternal exposure to intimate partner violence during pregnancy in Peru. Matern Child Health J. (2013) 17:485–92. doi: 10.1007/s10995-012-1012-0
51. Cokkinides VE, Coker AL, Sanderson M, Addy C, Bethea L. Physical violence during pregnancy: maternal complications and birth outcomes. Obstetr Gynecol. (1999) 93:661–6. doi: 10.1097/00006250-199905000-00006
52. Pastor-Moreno G, Ruiz-Perez I, Henares-Montiel J, Petrova D. Intimate partner violence during pregnancy and risk of fetal and neonatal death: a meta-analysis with socioeconomic context indicators. Am J Obstet Gynecol. (2020) 222:123–33. doi: 10.1016/j.ajog.2019.07.045
53. Hall M, Chappell LC, Parnell BL, Seed PT, Bewley S. Associations between intimate partner violence and termination of pregnancy: a systematic review and meta-analysis. PLoS Med. (2014) 11:e1001581. doi: 10.1371/journal.pmed.1001581
54. Gossaye Y, Deyessa N, Berhane Y, Ellsberg M, Emmelin M, Ashenafi M, et al. Women's health and life events study in rural Ethiopia. Ethiop J Health Dev. (2003) 17:1–47. doi: 10.4314/ejhd.v17i5.9856
55. Yigzaw T, Yibric A, Kebede Y. Domestic violence around Gondar in northwest Ethiopia. Ethiopian J Health Develop. (2004) 18:133–9. doi: 10.4314/ejhd.v18i3.9846
56. Wallach HS, Weingram Z, Avitan O. Attitudes toward domestic violence: A cultural perspective. J Interp Viol. (2010) 25:1284–97. doi: 10.1177/0886260509340540
57. Gray R, Bonellie SR, Chalmers J, Greer I, Jarvis S, Kurinczuk JJ, et al. Contribution of smoking during pregnancy to inequalities in stillbirth and infant death in Scotland 1994-2003: retrospective population based study using hospital maternity records. BMJ. (2009) 339:b3754. doi: 10.1136/bmj.b3754
58. Flenady V, Koopmans L, Middleton P, Frøen JF, Smith GC, Gibbons K, et al. Major risk factors for stillbirth in high-income countries: a systematic review and meta-analysis. Lancet. (2011) 377:1331–40. doi: 10.1016/S0140-6736(10)62233-7
Keywords: intimate partner violence, preterm birth, low birth weight, stillbirth, meta-analysis
Citation: Guo C, Wan M, Wang Y, Wang P, Tousey-Pfarrer M, Liu H, Yu L, Jian L, Zhang M, Yang Z, Ge F and Zhang J (2023) Associations between intimate partner violence and adverse birth outcomes during pregnancy: a systematic review and meta-analysis. Front. Med. 10:1140787. doi: 10.3389/fmed.2023.1140787
Received: 10 January 2023; Accepted: 19 April 2023;
Published: 17 May 2023.
Edited by:
Abdulbasit Musa Seid, Murdoch Childrens Research Institute, AustraliaReviewed by:
Marleen Temmerman, Aga Khan University Hospital, Nairobi, KenyaSonia Minooee, James Cook University, Australia
Copyright © 2023 Guo, Wan, Wang, Wang, Tousey-Pfarrer, Liu, Yu, Jian, Zhang, Yang, Ge and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jun Zhang, emgyMDAwanVuMjAwMEAxNjMuY29t; Fenfen Ge, ZmVuZmVuZ2VAaGkuaXM=
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work