 David A. De Luca1*
David A. De Luca1* Cristian Papara1,2
Cristian Papara1,2 Artem Vorobyev1,2
Artem Vorobyev1,2 Hernán Staiger3
Hernán Staiger3 Katja Bieber1
Katja Bieber1 Diamant Thaçi4
Diamant Thaçi4 Ralf J. Ludwig1,2
Ralf J. Ludwig1,2- 1Lübeck Institute of Experimental Dermatology, University of Lübeck, Lübeck, Germany
- 2Department of Dermatology, University Medical Center Schleswig-Holstein, Lübeck, Germany
- 3Department of Dermatology, Hospital Italiano de Buenos Aires, Buenos Aires, Argentina
- 4Institute and Comprehensive Center Inflammation Medicine, University of Lübeck, Lübeck, Germany
Lichen sclerosus (LS) is an underdiagnosed inflammatory mucocutaneous condition affecting the anogenital areas. Postmenopausal women are predominantly affected and, to a lesser extent, men, prepubertal children, and adolescents. The etiology of LS is still unknown. Hormonal status, frequent trauma and autoimmune diseases are well-known associations for LS, yet infections do not seem to be clear risk factors. LS pathogenesis involves factors such as a genetic predisposition and an immune-mediated Th1-specific IFNγ-induced phenotype. Furthermore, there is a distinct expression of tissue remodeling associated genes as well as microRNAs. Oxidative stress with lipid and DNA peroxidation provides an enabling microenvironment to autoimmunity and carcinogenesis. Circulating IgG autoantibodies against the extracellular matrix protein 1 and hemidesmosome may contribute to the progression of LS or simply represent an epiphenomenon. The typical clinical picture includes chronic whitish atrophic patches along with itching and soreness in the vulvar, perianal and penile regions. In addition to genital scarring, and sexual and urinary dysfunction, LS may also lead to squamous cell carcinoma. Disseminated extragenital LS and oral LS are also reported. The diagnosis is usually clinical; however, a skin biopsy should be performed in case of an unclear clinical picture, treatment failure or suspicion of a neoplasm. The gold-standard therapy is the long-term application of ultrapotent or potent topical corticosteroids and, alternatively, topical calcineurin inhibitors such as pimecrolimus or tacrolimus. Collectively, LS is a common dermatological disease with a so far incompletely understood pathogenesis and only limited treatment options. To foster translational research in LS, we provide here an update on its clinical features, pathogenesis, diagnosis and (emerging) treatment options.
1. Introduction
Lichen sclerosus (LS) is a chronic mucocutaneous immune-mediated disease which typically involves genital skin. The term was first coined by Hallopeau in 1887 and it received multiple names such as kraurosis vulvae, balanitis xerotica obliterans, white spot disease, leukoplakia and lichen sclerosus et atrophicus. The final term “lichen sclerosus” was accepted in 1976 by the International Society of the Study of Vulvovaginal Disease (1, 2).
The etiology and pathogenesis of LS are still not fully elucidated. There is a genetic and familial predisposition in LS, whereas frequent trauma, hormonal status and certain drugs could also play a role in the pathogenesis. LS is a type 1 T helper (Th1) mediated and miR-155 dependent immune-mediated disease. Although autoantibodies against extracellular matrix protein 1 and BP180 have been described, it is still unclear if they represent an accurate piece of LS pathogenesis. There is also a particular expression of tissue remodeling associated genes and an exacerbated oxidative stress that may lead to scarring and malignancy (3).
A bimodal peak incidence of LS in premenarchal girls and in menopausal women has been outlined. However, premenopausal women could experience LS with mild symptoms, delaying the diagnosis for several years and underestimating the real incidence in this age group. Men and adolescents are also, to a lesser extent, affected by the disease (4, 5).
The clinical picture of anogenital LS (gLS) includes ivory-white patches, atrophy and severe pruritus, altering the quality of life (QoL). Extragenital LS (eLS) comprises areas such as neck, shoulders, upper trunk, thighs and oral cavity (6, 7). The lesions could evolve to scarring of the vaginal introitus, phimosis and functional impairment (8). Furthermore, it has been described as an intrinsic risk factor for malignancy in untreated patients, but there is no evidence of increased neoplasm development after long-term treatments (9, 10).
The established diagnosis of LS based on the clinical features is usually sufficient, and a skin biopsy should only be performed in case of clinical doubts, differential diagnosis or suspected malignancy. The first-line therapy is ultrapotent or potent topical glucocorticoids (TC) and in case of anatomical changes due to scarring, surgical procedures should be performed (3, 11). In order to prevent complications, aside from an early diagnosis and a correct treatment, a long-term follow-up is imperative (9). The objective of this review is to deliver a thorough update of LS focusing on its pathogenesis, clinical features, diagnosis and treatment options.
2. Epidemiology
LS can occur at any age and it affects both sexes. However, women are most commonly affected, with a female-to-male ratio between 3:1 and 10:1 (9). A family history of LS has been described in 8.7% of women affected by this condition (12). There is a well-known historically bimodal presentation of vulvar LS (VLS) with a first peak in prepubertal girls (average: 7.6 years) and a second one during the peri- and postmenopause (average age: 52.6 years) (13). This specific distribution in females has been linked to a low estrogen status, leading to a humoral over T-cell mediated response, as well as to a Köbner phenomenon due to the lack of proper lubrication (9). However, VLS can affect women of any age and the proportion in fertile women could be higher than expected. In a survey of women of reproductive age with histological confirmation of VLS, the mean age of diagnosis was 32 years, with symptom onset at 27 years (14). Furthermore, up to 40% of the surveyees described symptoms prior to menopause or they were diagnosed with asymptomatic VLS during the gynecologic examination (11, 15). On the contrary, the onset of male genital LS (MGLS) in men is relatively stable with a first postpubertal peak during the third decade and a second one after 60 years (16). The mean age of onset in adult men was 36.2 years and a delay to seek medical advice of 1.6 years (17).
The exact prevalence and incidence of LS are underestimated. On the one hand, one third of the cases are asymptomatic, while, on the other hand, LS is frequently misdiagnosed or unrecognized (4). The estimated incidence of LS in both sexes is 0.1 to 0.3% (8). In regard to VLS, the prevalence in general gynecology private practice reached 1.7% (15). The Research Institute of the Health Insurance AOK in Germany exhibited a prevalence of 0.29% in women over 80 years old, whereas the prevalence in nursing home women over 80 years old escalated to 3%, probably influenced by incontinence and immobilization (18, 19). According to the Brooke Army Medical Center, the incidence of LS in men reached 0.07%, while the Department of Defense in the USA reported an incidence of 0.0014% (16, 20).
The incidence of pediatric LS is estimated at 0.04 to 0.06%, with a female-to-male ratio of 1:1.7 (21, 22). In a systematic review, the age-onset in children was 6.5 years in females and 8.6 years in males, with a mean diagnostic delay of 18 and 12.5 months, respectively (22). Premenarchal VLS presents with nonspecific symptoms and can occur in 1:900 girls. These symptoms usually withdraw after the menarche, underestimating further the frequency of LS (23). In a prospective observational study, histologically diagnosed preputial LS was found in 32% of male children with phimosis. Boys with phimosis due to LS were older than those without the disease (mean 8.4 versus 4.7 years old) (24). In Germany, LS in prepubertal boys was estimated to have a much higher prevalence of up to 0.4% of, as the majority are not commonly circumcised after birth (25).
Other forms of LS are rare. It is estimated that eLS comprises only 15–20% of LS patients. It usually occurs simultaneously with gLS, but in 6% of the cases, eLS is present as an isolated entity without any genital lesions. Most cases of eLS are diagnosed in middle-aged adults (26, 27). Nevertheless, the prevalence of eLS may be underestimated,as it is also frequently asymptomatic (28).
3. Pathogenesis
A summary of the pathogenesis and histological changes in LS is depicted in Figure 1.
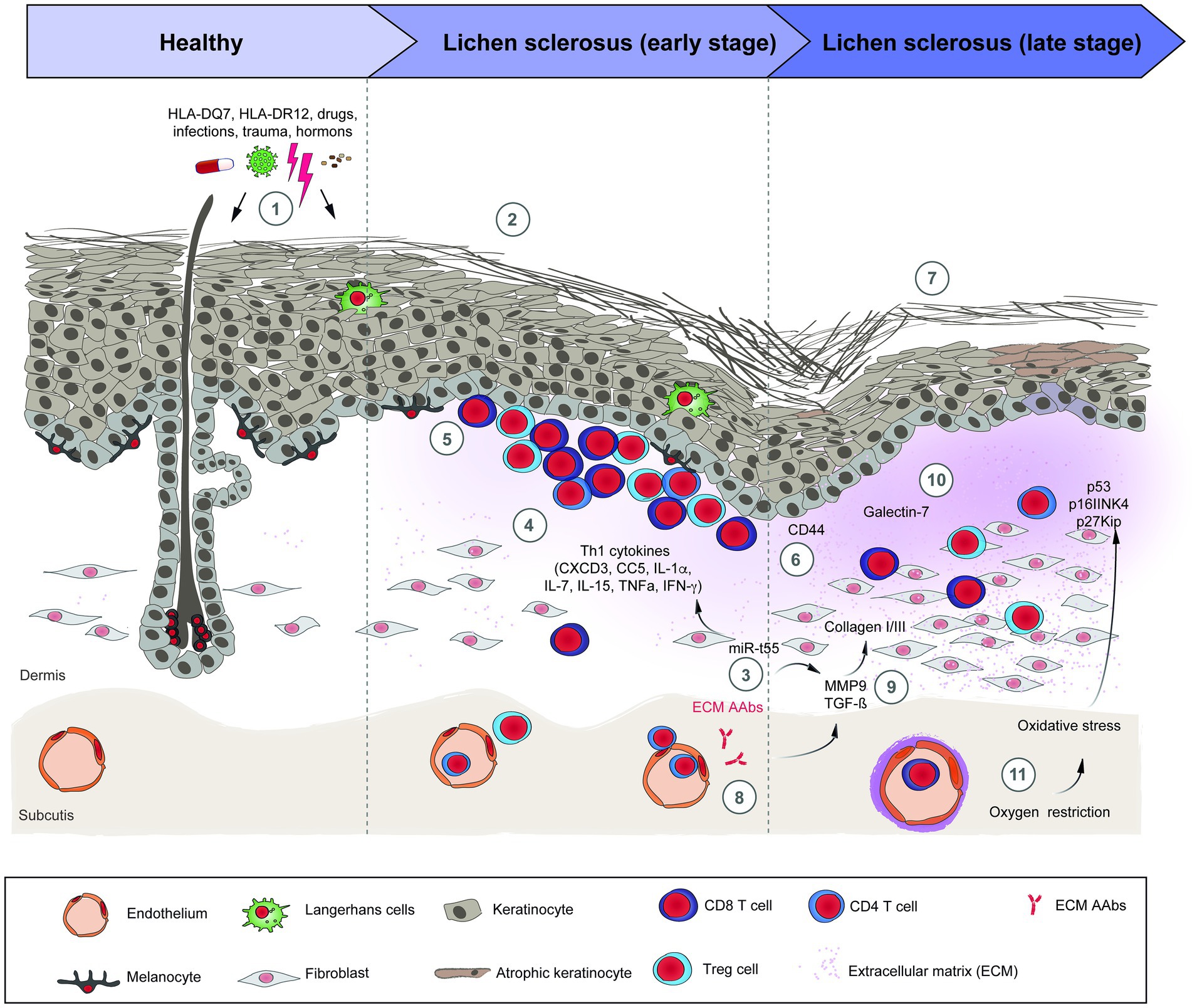
Figure 1. Schematic overview of lichen sclerosus pathogenesis. (1) Risk factors for LS; (2) The inflammatory early stage of LS is unspecific and shows a dermoepidermal interface band of mostly T-cells. (3) miR-155 is overexpressed in LS, stimulates the Th1 profile and the dermal sclerosis. (4) Th1 cytokines implicated in the pathogenesis of LS. (5) Lichenoid infiltrate of TCD4+, TCD8+, and Tregs cells in the upper dermis. (6) Abnormal expression of CD44 in the epidermis and lichenoid infiltrate. (7) The sclerotic late stage of LS presents an atrophic epidermis, with comedo-like plugs and a cleft in the stratum corneum, dermal sclerosis, reduction and dilation of dermal vessels and the appendages disappear. (8) The autoantibodies against EMC1 may activate MMP9, which subsequently activates TGF-β. (9) TGF-β and BMP2 induce the synthesis of collagen I and III in fibroblasts. (10) Galectin-7 induces the synthesis of collagen I and III. (11) Along with inflammation, the vessel sclerosis contributes to the oxidative stress in LS, leading to downregulation of tumor suppressors genes and overexpression of p53 in the skin, factors related with the development of skin carcinomas. The precise sequence of events and their interactions are only incompletely understood. References: BMP2: bone morphogenetic protein 2; EMC1: extracellular matrix protein 1; LS: lichen sclerosus; MMP9: metalloproteinase 9; TGF-β: tumor growth factor beta. TNF-α: Tumor necrosis factor alpha.
3.1. Genetics
Immune-mediated diseases have an immunogenetic scenario. A positive family history of LS in first-degree female relatives can be found in 12% of patients (29). HLA-DR and DQ are supposed to be involved in the susceptibility and protection from LS (30). In children with VLS, HLA-DQ7 was present in 66% of the cases, in comparison to 31% in controls. Although these children showed a low association with autoimmunity, up to 56% of their relatives presented another autoimmune disease (31). In both adult male and female patients, HLA-DQ7 has been observed to occur more frequently in LS (32, 33). A study of UK women with VLS demonstrated an increased frequency of HLA-DR12 (DRB1*12) and a lower frequency of HLA-DR17 (DRB1*0301/04) compared to controls. Furthermore, HLA-DR and DQ could not be associated with the time of onset of VLS, anatomical changes and localization of the skin lesions, and the response to topical glucocorticoids (34). In a cohort of Han Chinese women, the HLA-A*11, HLA-B*13, HLA-B*15, and HLA-DRB1*12 genotypes have been linked to a higher risk of VLS. Moreover, the women carrying HLA-A*11, HLA-B*15, HLA-B*35, and HLA-DRB1*12 genotypes were more susceptible to developing vulvar malignancy (35).
3.2. Epigenetic
Epigenetic changes in LS may potentially induce malignant transformation. At the beginning of the disease, LS lacks p53 and CDKN2A mutations, suggesting that the cell-cycle regulation is not appreciably altered (36). However, VLS is associated with altered isocitrate dehydrogenase, an enzyme responsible for DNA 5-hydroxymethylation patterns. As a consequence, the global methylation levels in the epidermis are diminished in VLS, and the UVA1 treatment could lead to a normalization of these levels (37). Nevertheless, the contribution of the epigenetics LS is enigmatic. It was described that a hypermethylation in p16INKa gene promoters could lead to an epigenetic silencing and, therefore, to an abnormal cell growth. This could be an early event in tandem with subsequent p53 somatic mutations, associated with tumor development and progression (38). Furthermore, the p16INKa hypermethylation was linked to vulvar carcinoma arising from LS, rather than to those not associated (39).
3.3. Immunology
In LS, there is an important T-cell infiltration limited to the dermis, composed mostly of CD8+ and Treg T-cells, and to a lesser extent, CD4+ T-cells (40). The involved cells express the chemokine receptors CXCR3 and CCR5 and lack CCR3 and CCR4, suggesting a Th1 profile. Th1 response intensifies through the production of interferon γ and the attraction of more Th1 cells. Other proinflammatory cytokines such as IL-1α, IL-7, IL-15, and TNF-α are upregulated in LS, whereas antiinflammatory cytokines (e.g., IL-10) are downregulated (39, 41). However, IL-4 levels are high in LS with congenital phimosis, a cytokine typically considered a marker of T helper 2 profile (42).
The small endogenous noncoding miR-155 plays a primordial role in regulating the homeostasis of the immune system and the sclerotic tissue formation. Activated immune cells in LS express miR-155 and, as a result, miR-155 enhances the Th1 differentiation. The high expression of miR-155 in CD4+ T cells reduces the Treg-cells-mediated suppression. As a consequence of miR-155 levels, the increased numbers of Treg cells in the dermis may not fully affect CD4+ T cells. Furthermore, the expression of Foxp3, a transcription factor of Treg cells, were significantly lower in the skin of VLS, compared to healthy vulvar skin. These results may lead to an impairment of the immune tolerance and, as a result, autoreactive CD4+ effector T cells may trigger an immune response against self-antigens (40, 41, 43).
The extracellular matrix protein 1 (EMC1) is a glycoprotein that binds different molecules of the basement membrane zone (BMZ) and dermis, being responsible for the structural organization and integrity in human skin. Autoantibodies against ECM1 and other antigens of the BMZ, i.e., BP180 and BP230, were found in gLS. The significance of the autoantibodies is unclear and, except for anti-EMC1 antibodies, they may only represent an epiphenomenon rather than a key-component of the LS pathogenesis (44, 45).
CD44 is a cell surface glycoprotein involved in cell adhesion and migration; it also acts as a hyaluronate receptor. The role of CD44 in keratinocytes is unclear. It was shown that the levels of CD44 are decreased in all layers of the epidermis in LS. The lack of CD44 may result in an abnormal dermal accumulation of hyaluronate in gLS and eLS (46, 47). On the other hand, other authors confirmed the high expression of pan CD44 around keratinocytes and in areas of inflammation in the dermis, but not in areas of sclerosis (48).
3.4. Fibroblast proliferation
Another characteristic of LS is the augmented collagen synthesis in the dermis, in particular, collagen I and III. The sclerotic tissue formation depends also on the increased expression of miR-155. As a consequence, the tumor suppressor genes FOXO3 and CDKN1B are downregulated, leading to fibroblast proliferation as well as persistence (49). Furthermore, in congenital phimosis due to LS, cytokines of the TGF-β superfamily are overexpressed. Among them, TGFβ-2 and BMP2 and their correspondent receptors play a central role in fibrosis control and tissue turnover (42).
ECM1 autoantibodies release the regulatory inhibition of metalloproteinase 9 (MMP9), thus enhancing the collagenase activity and, as a result, disrupting the BMZ (50). Nevertheless, the hyperactivity of MMP9 may cleave and activate TGF-β, hence the increased collagen synthesis (39). Apart from the increased levels of collagen I and III, an abnormal deposition of collagen V, a reduction of elastic fiber in the upper dermis as well as a low expression of ECM1 in the blood vessels of hyalinized tissue, were also observed (51).
The fibroblast activity may also be stimulated by galectin-7, a pro-apoptotic protein. In VLS, the epidermal levels of galectin-7 are increased, inhibiting keratinocyte viability and, thus, inducing epidermal atrophy (52). Galectin-7 could also act as paracrine in the fibroblast, enhancing the transcription of type I and III collagen and downregulating the cell growth rate (53).
3.5. Oxidative stress
Oxidative stress may be responsible for the pathogenesis, maintenance and progression of chronic inflammatory disease, including LS (54). Lipid peroxidation in keratinocytes, oxidative DNA damage and protein oxidation in areas of LS were associated with low concentrations of antioxidant enzymes, such as superoxide dismutase (55). The oxidative DNA damage in LS downregulates the expression of two cyclin-dependent kinase inhibitors p16IINK4 and p27Kip1. As a consequence, the inhibition of these two tumor suppressors releases the cell-cycle, thus contributing to the malignancy in LS (56).
Oxidative stress and inflammation may induce the overexpression of wild-type p53 in basal keratinocytes, independent from the LS subtype. Additionally, due to the development of sclerotic vessels and the poor oxygenation, the restriction of oxygen flow induces ischemic stress, intensifying the p53 overexpression (57). In contrast to vulvar carcinoma, chromosome 17p-linked loss of heterozygosity and p53 mutations are not characteristic in LS (58).
4. Risk factors
4.1. Trauma and chronic irritation
Chronic irritation and trauma play an important part in the development of LS. For instance, occlusion, scratching, friction and surgical procedures act as a Koebner phenomenon, resulting in the appearance of LS lesions (19). Urinary incontinence, multiparous status, scarce genital washing frequency and high BMI are associated with VLS in elderly women (59). In men, chronic irritative penile microincontinence, anatomical abnormalities (hypospadias), and interventions, e.g., cysto- and urethroscopies, radical prostatectomy, bladder surgery or penile prosthesis implantation are linked to MGLS (60, 61). LS affects uncircumcised men or boys with preputiolysis, but seldom circumcised males at birth (62).
There are also reports about koebnerization of eLS after insulin injections, influenza vaccination and intramuscular drug administration (63–65). Periostomal LS around urostomies are described as uncommon complications, possibly due to local trauma, occlusion and urine irritation (66). There are reports of LS after intimate body piercing (67, 68). Postirradiation eLS was described in patients treated for breast neoplasm, and VLS after vaginal cancer radiotherapy (69–71).
4.2. Hormones
The role of the hormones in LS is controversial. In the past, hypoestrogenism was considered a risk factor of VLS, due to its typical presentation during pre-puberty and postmenopause. However, this theory could not be proved (72). The expression of estrogen receptor (ER) isoforms in epidermis and dermis of VLS are comparable to those of healthy women. The isoform alpha of ER was absent in the fibromuscular layers, while the isoform beta was highly upregulated in VLS, as opposed to the absent expression of isoform beta in normal tissue. These variations in the ER isoforms may suggest that VLS is refractory to estrogen therapy (73).
Other studies speculated that a decreased 5 alpha-reductase activity could contribute to the pathogenesis of VLS by leading to low serum levels of dihydrotestosterone, free testosterone, and androstenedione (74). Furthermore, a low density of androgen receptors, both in gLS and eLS, could also induce a disease progression (75). Supporting this theory, it was observed that the use of oral contraceptives with anti-androgenic properties might trigger an early onset of VLS in susceptible young women (76). Nevertheless, the widespread topical treatment with testosterone became obsolete, as a consequence of the androgenic side effects and the therapy’s lack of effectiveness (9).
Contraception methods based on progesterone alone were, however, protective for VLS development, while this preventive benefit seemed to be lost when the contraceptive was combined with estrogens (12). Additionally, the topical treatment with progesterone 8% induced remission in 60% of premenopausal VLS but, in spite of that, ultrapotent TC are still superior in matters of therapeutic efficacy. (77).
4.3. Infections
There are no triggering infections associated with LS. However, there are many reports of the presence of HPV16 in the prepuce of not only adult men, but also in boys before having sexual intercourse (78, 79). In a case series of 329 patients, no correlation between MGLS and HPV infection was shown (61). Furthermore, in HPV16-associated MGLS cases, the role of the virus may be rather accidental than pathogenic, as also non-specific HPV-associated gene expression patterns have been found (80, 81).
Borrelia burgdorferi has also been postulated as a possible risk factor of LS and morphea, but this association remains obscure, as many studies showed no evidence for bacterial DNA in serological studies and skin biopsies specimens (82).
Many reports have suggested that hepatitis C virus (HCV) could also play a role in gLS and eLS (83, 84). In a lipidomic and metabolomic analysis, VLS correlated with an abnormal antivirus response due to the presence of HCV poly U/UC sequences (85). Nevertheless, the HCV serology screening in MGLS showed no seropositivity for the virus, thus assuming that it would unlikely play a pathogenic part in MGLS (86).
Circular RNA were shown to be closely related to the pathogenesis of different diseases and neoplasms. A recent study that aimed to investigate the differential expression profile of circular RNA in VLS observed an enrichment of the human T-cell leukemia virus (HTLV-1) signaling pathway, a retrovirus related to adult T-cell lymphoma/leukemia and chronic inflammatory diseases. The authors concluded that the HTLV-1 signaling pathway could be related to the occurrence and development of VLS (87).
4.4. Medications
The association of LS and medications is occasional. There are reports of blistering variants of LS, gLS and eLS with imatinib mesylate in patients treated for chronic myelogenous leukemia and gastrointestinal stromal tumor (88, 89). Carbamazepin has also been implicated in a case of generalized LS after 6 months duration of treatment (90).
There is a well-known association of autoimmune-induced diseases in cancer patients treated with immunotherapy and check-point inhibitors. In concrete, gLS was also reported in adult patients with malignancy, treated with pembrolizumab, nivolumab, or ipilimumab (91, 92). The reports indicated that the development of gLS usually occurred after 3 to 5 months of the beginning of therapy (91, 93).
There is an inverse relationship between VLS, ACE inhibitors and beta-blockers. While ACE inhibitors reduce the inflammatory cell infiltrate in the skin, beta-blockers reduce AMPc levels, induce keratinocyte proliferation and lymphocyte motility, which could impact on the clinical picture of VLS (94).
5. Clinics
LS lesions are flat, ivory-coloured, wax-textured spots, which may coalesce into crinkly thin or hyperkeratotic patches. Adjacent erythema and the Koebner phenomenon may also be observed. Other typical signs of LS are ecchymosis, excoriations and fissures. (3) LS can affect any part of skin or mucosa, however, in 85% of cases, the genital mucosa is involved, and extragenital lesions are seen only in around 15–20% of cases (23). Extragenital lesions often appear simultaneously with genital lesions, but in 6% of cases only extragenital forms have been reported (27).
5.1. Female lichen sclerosus
Initial manifestations in the anogenital area in females can be nonspecific and include itch, burning sensation, as well as slight redness and swelling in the periclitoral area. Later on, affected skin becomes fragile and atrophic lesions, fissures and erosions may occur (Figure 2A). Fissures are often localized between clitoris and urethra and in the interlabial sulci, leading to dysuria (95). Due to intense pruritus, hyperkeratotic lesions and ecchymoses in the involved regions can be observed. Mostly, clitoral hood, labia minora, inner part of labia majora, perineum and perianal region is affected (Figure 2B), sometimes resembling “figure of eight,” also termed “keyhole” or “hourglass,” with involvement of vulvar and perianal regions. Progression of disease can lead to scarring, which is observed in 80% of adult female patients and 30% of girls (11). Scarring often results in fusion or even complete resorption of labia minora and loss of clitoral hood. In addition, narrowing of vaginal introitus can occasionally lead to dyspareunia, strongly affecting sexual life of the patients (5).

Figure 2. Clinical, dermoscopic and histological hallmarks of lichen sclerosus (LS). (A) Ivory-white wax-textured atrophic patches in the vulva. Agglutination, labial resorption, clitoral hood scarring. Fissures and erosions due to the narrowing of the vaginal introitus. (B) Erythema and anogenital scarring. Loss of the normal vulvar architecture with resorption of labia majora and minora. Ivory-white perineal spots perianal and scarring. (C) Hypopigmented macules, erythema and adhesions between glans and preputium. (D) Extensive scarring and atrophy of glans and partial loss of the balanopreputial sulcus. Ecchymotic and hypopigmented penile shaft. (E) Hemorrhagic variant of lichen sclerosus in glans penis over whitish scars, erosions and crusts. (F) Dermoscopy of LS in glans penis with structureless whitish and yellowish patches (red arrow), glomerular and dotted vessels (blue arrow). (G) Dermoscopy of LS in glans penis with penile intraepithelial neoplasia transformation. Glomerular vessels grouped over a pink and yellow surface, compatible with lichen sclerosus (green arrow). Structureless infiltrated whitish areas (red arrow) with glomerular and dotted vessels (yellow arrow), with histopathological confirmation of differentiated penile intraepithelial neoplasia. (H) Scapular ivory-white polygonal coalescing papules with adjacent erythema and comedo-like openings. (I) Whitish extensive macules, surrounded by hyperpigmentation, erythema and areas of ecchymosis on the groin. (J) Mammary and submammary ivory-white wax-textured atrophic coalescing spots with perilesional erythema and hyperpigmentation. (K) Small monomorph ivory-white wax-textured spots in extragenital lichen sclerosus. (L) The histopathology from a skin biopsy showing an atrophic epidermis with compact orthohyperkeratosis, hypergranulosis, degeneration of basal keratinocytes, and exocytosis. Under the thick basement membrane, there is a scarcely cellular zone of sclerosis. In the upper dermis, a superficial lichenoid inflammatory band and vasodilation with perivascular infiltrate are shown (H&E 40x).
In prepubertal girls, the clinical symptoms are similar to that of adult females, which often present itch, soreness and sometimes dysuria. Typical clinical manifestations, such as fissures, erosions, vulvar and perianal bruising can be mistaken for sexual abuse (96). Perianal involvement and constipation, caused by painful anal fissures are frequently observed in girls. Importantly, the extent of the genital involvement does not directly correlate with the intensity of clinical symptoms, so not relevant lesions can cause significant complaints (72).
5.2. Male lichen sclerosus
Clinical manifestations of LS in boys and adult men are usually localized to glans penis and foreskin, whereas involvement of perianal area is rare. Typical symptoms include pruritus and soreness, sometimes accompanied by dysuria. Clinically, porcelain-like whitish sclerotic scarring on the distal portion of prepuce is usually observed (25). This scarring leads to phimosis in previously retractable foreskin, or adhesions of the foreskin to glans penis (Figure 2C) (3). In addition to preputial lesions, involvement of perifrenular region of glans is often seen, causing sclerotic frenulum breve (Figure 2D). In some cases, erosions, ulcers and even bullous lesions may be present. In around 17% of patients, external meatus urethrae can also be involved, which is often accompanied by dysuria and poor urinary stream. Sometimes meatal stenosis can appear years after the initial manifestation of LS, without any signs of persistent or recurrent LS (25, 97).
5.3. Extragenital lichen sclerosus
Extragenital manifestations are rare and found mostly in females, with female to male ratio ranging from 6:1 to 10:1 (27). Extent of the extragenital involvement vary from small well-defined area to widespread eruption, mostly localized to submammary area, neck, shoulders, inner thighs, wrists, upper back (Figures 2E–H) (98). Clinical lesions usually appear as asymptomatic or slightly pruritic ivory-white polygonal coalescing papules. Comedo-like plugs or evenly spaced dells, corresponding to appendageal ostia on the surface of the plaques are characteristic for extragenital LS. These dells and plugs may disappear with time, leaving smooth porcelain-white plaques (99). In some cases, the typical LS lesions are accompanied by telangiectasias, and hemorrhagic- or non-hemorrhagic bullae. Bullous lesions may lead to ulcerations or erosions that turn into white sclerotic plaques (100–102). The Koebner phenomenon is often observed, with extragenital manifestations of LS arising at pressure points, sites of surgical scars or traumas (19).
In rare cases, involvement of oral mucosa has been described, mostly affecting labial mucosa, followed by the buccal mucosa, and lip. Oral manifestations are asymptomatic well-demarcated macules with a whitish, ivory- or porcelain-white color. Pain, pruritus, and tightness when opening the mouth were described in a minority of the patients (103, 104).
6. Histology
Typical histological features of LS include orthohyperkeratosis, epidermal atrophy, degeneration of basal keratinocytes, homogenized collagen in upper dermis, and band-like and perivascular inflammatory infiltrate in the dermis (Figure 2I) (105, 106). However, the histological features in early stages are often difficult to distinguish among other lichenoid disorders (95). In early lesions, the initial dermoepidermal interface band of inflammation shifts gradually downwards into the dermis. As a result in later stages, the appendages disappear, due to the deposition of an altered extracellular matrix in the dermis. The destruction of the papillary capillaries starts early in LS, along with the thickening of the perivascular basement membrane. In the late stage, the capillaries are dilated and in resolved lesions, there is a complete absence of normal vessels (107). Some authors demonstrated an increased density of capillaries during the sclerotic stage of LS, in comparison with healthy controls (108). The BMZ demonstrates an alteration of the antigen expression, augmented collagen IV and VII, and loss of expression of hemidesmosomal and anchoring filament components. As a result of these changes, the BMZ is disrupted or some areas of BMZ are completely absent (109).
The immunohistochemistry approach shows a dense infiltrate of CD4+ and CD8+ T-cells, localized in the subepidermal inflammatory band. In certain cases, the T-cells also infiltrate the dermoepidermal junction, lower epidermis and dermis. CD68+ macrophages are present in the inflammatory band and also scattered throughout sclerotic regions. HLA-DR is also expressed, in variable percentages, in the inflammatory infiltrates and keratinocytes (48).
7. Associations
Autoimmune diseases are associated with LS in more than a quarter of the patients (110). In a large retrospective study, autoimmune thyroid diseases such as Hashimoto’s thyroiditis and Graves’ disease, antithyroid antibodies and elevated autoantibodies were more commonly associated with female LS (18.9%) than male patients (5.1%) (111). In a case–control study of 765 cases of VLS, it was found a 2.88-, 2.34-, and 2.05-fold increase in odds of having autoimmune thyroiditis, hypothyroidism, and hyperthyroidism, respectively. This study provides further evidence that screening for thyroid disorders in LS patients should be considered (112).
There are also reports from vitiligo, alopecia areata, rheumatoid arthritis, pernicious anemia, systemic lupus erythematosus, Sjögren syndrome, and multiple sclerosis (110, 111, 113–116). In 5.7% of patients, morphea coexists with LS, especially the circumscribed and generalized types (117). While in men morphea associates typically with eLS, in women the frequent relation with VLS obliges the inspection of the anogenital area (27).
Atopic dermatitis was found in 25% of boys who underwent circumcision due to gLS. The authors hypothesized that the disturbed atopic skin barrier could be more susceptible to LS triggering agents (118). In the case of psoriasis, the prevalence in the general population is 2%, while it rises to 7.5% in women suffering from VLS. Moreover, a total of 26.3% of the female psoriasis patients also had concomitantly LS (119).
Female patients with LS had an increased risk of developing metabolic syndrome in comparison to the healthy controls. They were also more likely to suffer from arterial hypertension, diabetes type 2, coronary artery and peripheral vascular diseases as well as to be prescribed statins. There were no differences in the body mass index, triglycerides or HDL levels, probably because of the statin prescription. The authors hypothesize that this relation could be due to an increased systemic inflammation and a decreased overall daily activity level (120).
8. Diagnosis
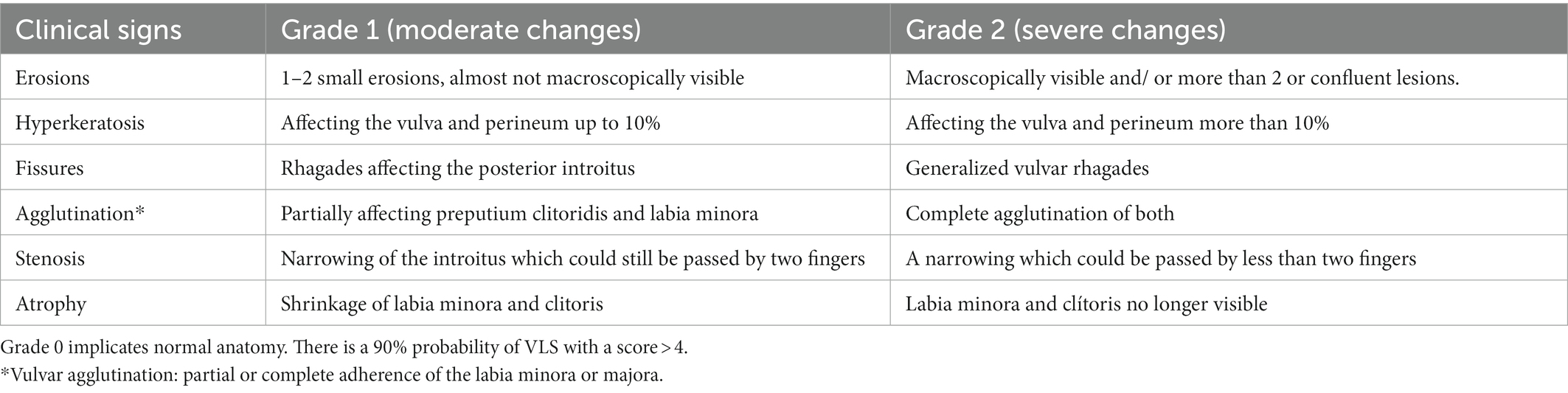
The diagnosis of LS in adults and children is typically clinical, involving a thorough medical history and physical examination. Photographic records are also recommendable to monitor therapy efficacy or disease progression (121). The clinical scoring system in VLS is a validated useful tool to ease the diagnosis and to evaluate related symptoms and the therapy response (Table 1) (122, 123). An autoimmune disease assessment should be conducted, especially in case of positive clinical features for thyroid autoimmune diseases, type 1 diabetes mellitus, rheumatoid arthritis or scleroderma (13, 124).
Histopathological assessment is mostly not necessary, as the clinical picture can be enough for the diagnosis. Nevertheless, there are many situations where an histological examination should always be considered (Table 2) (124). The biopsy should be performed from active sclerotic skin areas and erosions that do not improve after the therapy (13). Early, ulcerative or erythematous lesions are inadequate biopsy areas, as they present mostly an unspecified histological picture (105). Preceding treatment with topical corticosteroids can also erase typical histopathological changes (5).
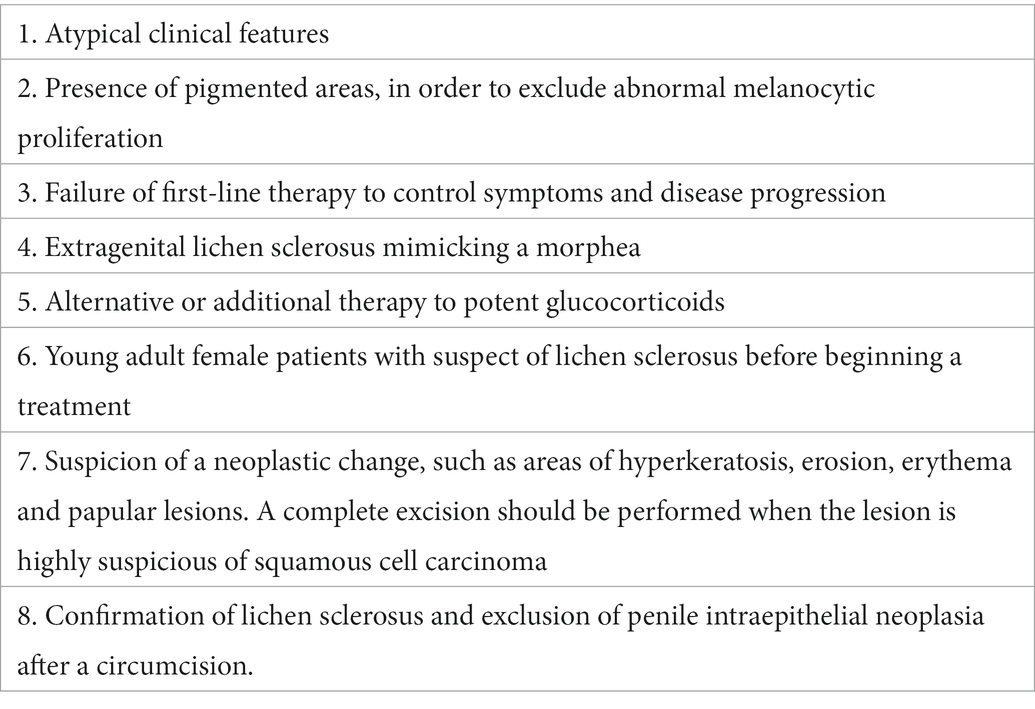
Table 2. Recommendations for histological examination in lichen sclerosus (124).
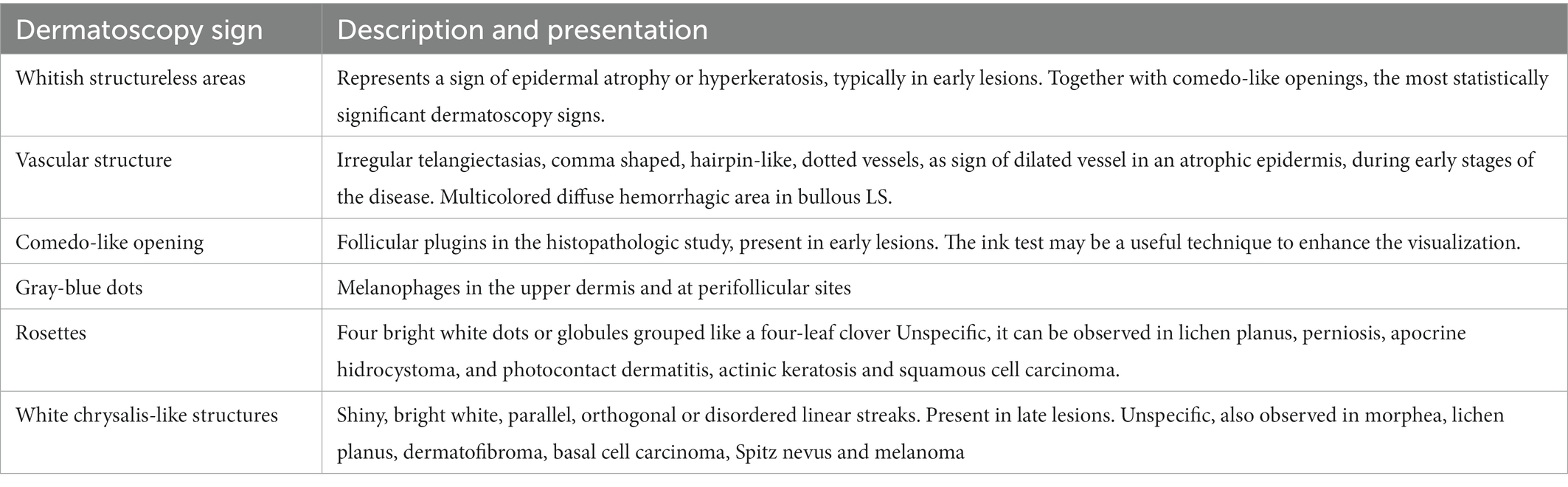
Dermoscopy is a useful tool to support the non-invasive diagnosis of LS as well as to optimize the biopsy site (125). In VLS, the most prevalent feature is the presence of the structureless whitish or white-yellowish patches placed over a white atrophic background. These dermoscopic changes represent signs of dermal sclerosis and hyalinization. Another hallmark is the reduction of the vascular density compared to normal vulvar skin. The dermoscopy of VLS reveals irregular linear vessels in over 97% and dotted vessels in almost 45% of early stages VLS. In later stages, most vessels disappear as dermal fibrosis may exceed the vascular changes. Other dermoscopy signs include the scattered gray-blue dots, the comedo-like openings and the scales (125). In eLS, the most common dermoscopy hallmarks are the whitish structureless areas, comedo-like openings and telangiectasias and dotted vessels in the early stages. White chrysalis-like structures are not specific for eLS, but they have been documented in later stages (126). Rosettes or four-dot signs were also described in LS, however, they lack specificity (127). The dermoscopic clues of LS are further explained in Table 3 (125–130).
The reflectance confocal microscopy is another non-invasive technique for imaging skin in vivo. In MGLS, prominent fiber-like structures representing hyaline sclerosis can be observed in almost half of the patients, and an atypical honeycomb pattern could be related to penile intraepithelial neoplasia (131).
The impact of LS in the quality of life (QoL) as a whole, but also in relation to sexuality, should be assessed with validated tests. The dermatology life quality index (DLQI) measures the impact of the skin disease on different social areas and also covers symptomatology and response to the treatment. The female sexual functioning index (FSFI) is a self-reporting measure of sexual function in women with sexual arousal disorders and vulvodynia. The World Health Organization Five-Item Well-being Index is a short and generic global rating scale for subjective well being (132–135).
9. Differential diagnosis
9.1. Clinical differential diagnosis
A summary of differential diagnosis for gLS, eLS, and oral LS are listed in Table 4 (13). Anogenital lesions in women could be easily misdiagnosed for lichen planus, Candida vulvitis, postmenopausal atrophy and vitiligo, therefore, an extensive list of differential diagnoses should be considered. The most common form of lichen planus in the genital area is the erosive type, which may involve the vagina with symptomatic erythematous and friable lesions, inflammatory vaginal discharge, synechiae and obliteration. Candida vulvitis with or without vagina discharge can coexist with VLS and it might be treated repetitively before establishing the diagnosis of VLS. Even so, candida vulvitis can cause flares of VLS symptoms. Postmenopausal atrophy presents vaginal dryness, decreased lubrication, dyspareunia, discharge and urinary symptoms, with loss of vulvar tissue’ elasticity and fat. The clinical findings of vitiligo are asymptomatic demarcated chalk-white or milky macules that lack clinical signs of inflammation. Other differential diagnoses in VLS are lichen simplex chronicus, contact dermatitis, psoriasis, morphea, leukoplakia, extramammary Paget diseases, mucous membrane pemphigoid and vulvar intraepithelial neoplasia. In children, ecchymotic and bleeding could be a suspicion of sexual abuse (13, 136). Beside inflammatory and autoimmune diseases, in MGLS following diseases should be additionally considered as differential diagnosis: infectious and plasma cell balanitis, balanitis circinata, fixed drug eruption, penile neoplasms and in boys, physiologic phimosis (137, 138).
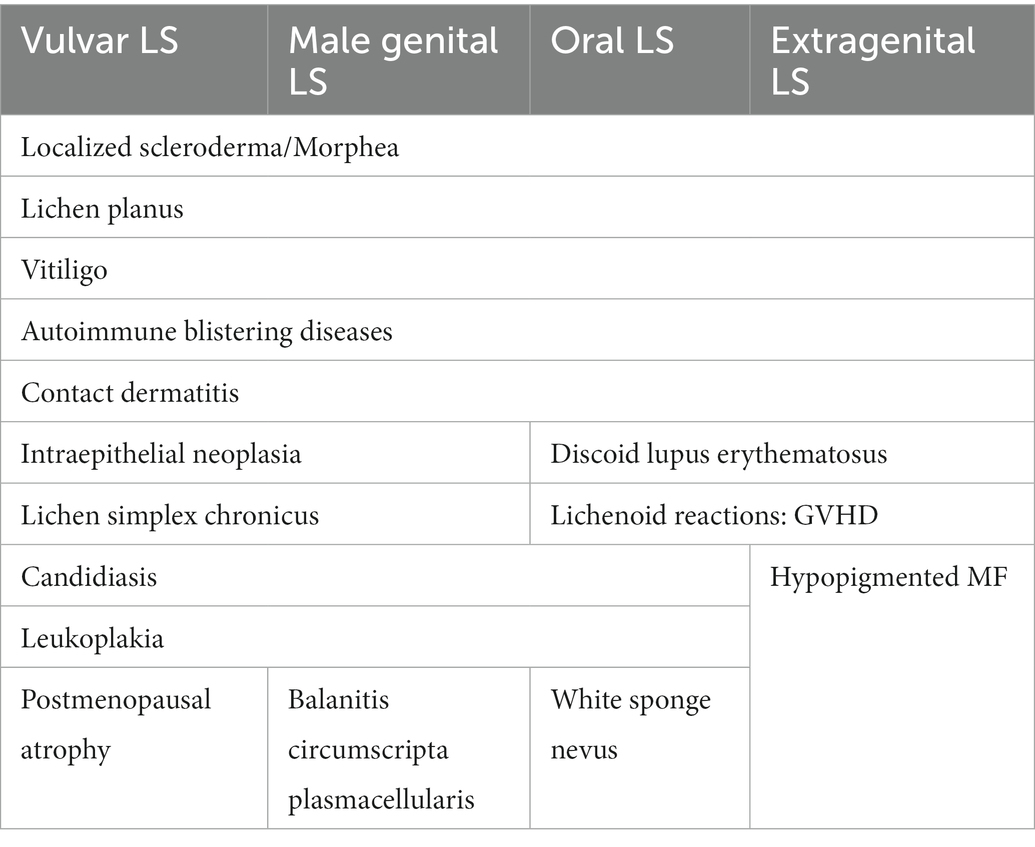
Table 4. Summary of clinical differential diagnoses in lichen sclerosus (LS) (13).
The differential diagnoses of eLS depend on the extent and morphology of the lesions. For the early indurated eLS lesions, discoid lupus erythematosus and morphea plaque type are clinically resemblant. While discoid lupus erythematosus presents scales, pigmentation and scarring on photoexposed skin, morphea has initially a violaceous halo. The late hypopigmented lesions should be differentiated from vitiligo, hypopigmented mycosis fungoides and atrophic lichen planus. The diagnosis of hypopigmented mycosis fungoides could be clinically challenging and it requires an histopathological confirmation. Beside vitiligo and morphea, generalized eLS may be confused for graft-vs-host disease. Bullous LS may pose a diagnostic challenge in bullous lichen planus, autoimmune blistering diseases, bullous scleroderma, bullous lupus erythematosus and bullous insect bite reactions (27, 139).
Oral LS could be mistaken for many other mucous lesions. Oral lichen planus presents white reticular plaques, usually with a bilateral and symmetrical distribution. Lichenoid reactions show a reticular, atrophic or ulcerative lesions, often asymmetrical, with a history of an implicated medication, dental restorative material, or graft-versus-host disease. Leukoplakia are white plaques that cannot be categorized as any other disease, and premalignant lesions usually emerge as a proliferative verrucous leukoplakia. Candida infection presents with white patches or pseudomembranes that can be removed, revealing underneath an erythematous mucosa. Other differential diagnoses include vitiligo, localized scleroderma, fibrous scar, submucous fibrosis, white sponge nevus and discoid lupus erythematosus (7).
9.2. Dermoscopic differential diagnosis
Morphea is one of the most challenging differential diagnoses of LS by dermoscopy. While in LS white-yellowish patches are the most common dermoscopy feature, morphea presents white fibrotic beams. Both structures are similar, however, the white fibrotic beams tend to be smaller, more opaque with less defined margins, compared to the white-yellowish patches in LS. Vascular components such as linear-irregular or dotted vessels are to be found in both pathologies. LS often displays follicular plugging, which may correlate with the rosettes. Morphea lacks comedo-like openings, scaling and hemorrhagic areas. The presence of structureless or reticular brownish areas is more common in morphea, while pigmented dots may be found in both. The rosette sign, along with whitish plaque and comedo-like openings, may lead to an earlier diagnosis of LS. Dermoscopy differential diagnoses in gLS and eLS are listed in Table 5 (140–145).
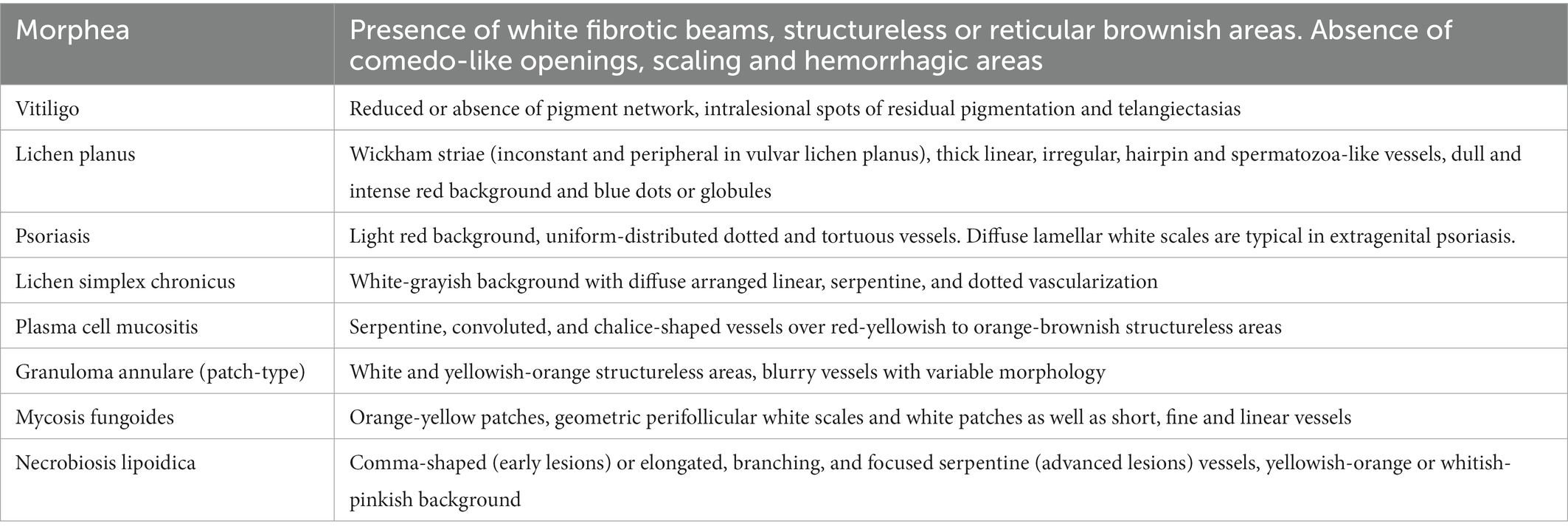
Table 5. Summary of dermoscopy differential diagnoses of genital and extragenital lichen sclerosus (140–145).
10. Management
Every case of gLS should be treated, in order to preserve QoL and to prevent scarring, anatomical, sexual and urinary dysfunction (9, 124). The therapeutic strategy should be discussed with the patient, as there are many options that have been explored to achieve clinical remission and prevent progression. A list of non-pharmacological recommendations as well as the proposed schema with TC in LS are enumerated in Table 6 (9, 124). A list of the ongoing clinical trials is tabulated in Table 7.
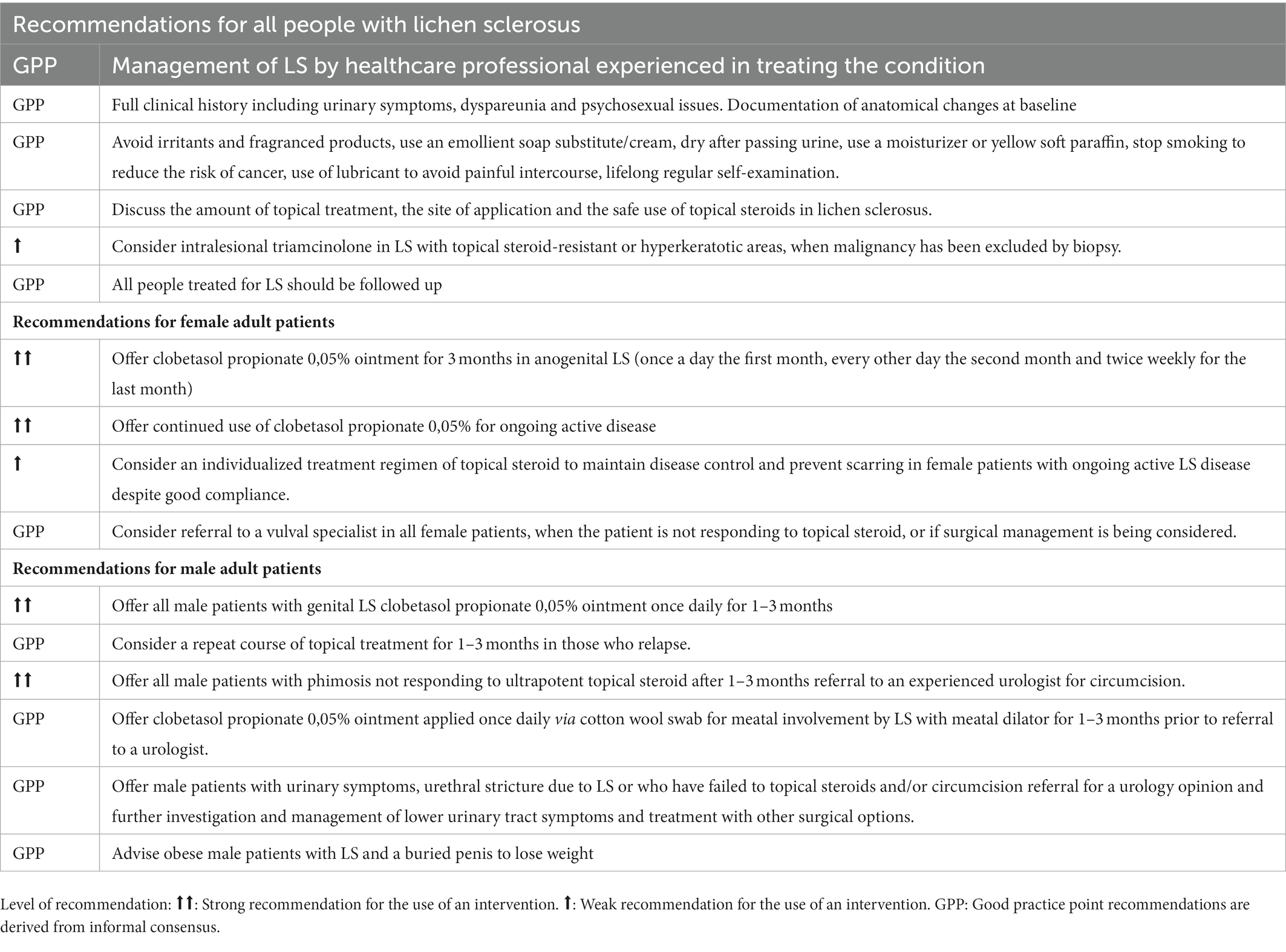
Table 6. Summary of recommendations for adults with lichen sclerosus (LS; Modified from the British Association of Dermatologists guidelines, 2018) (124).
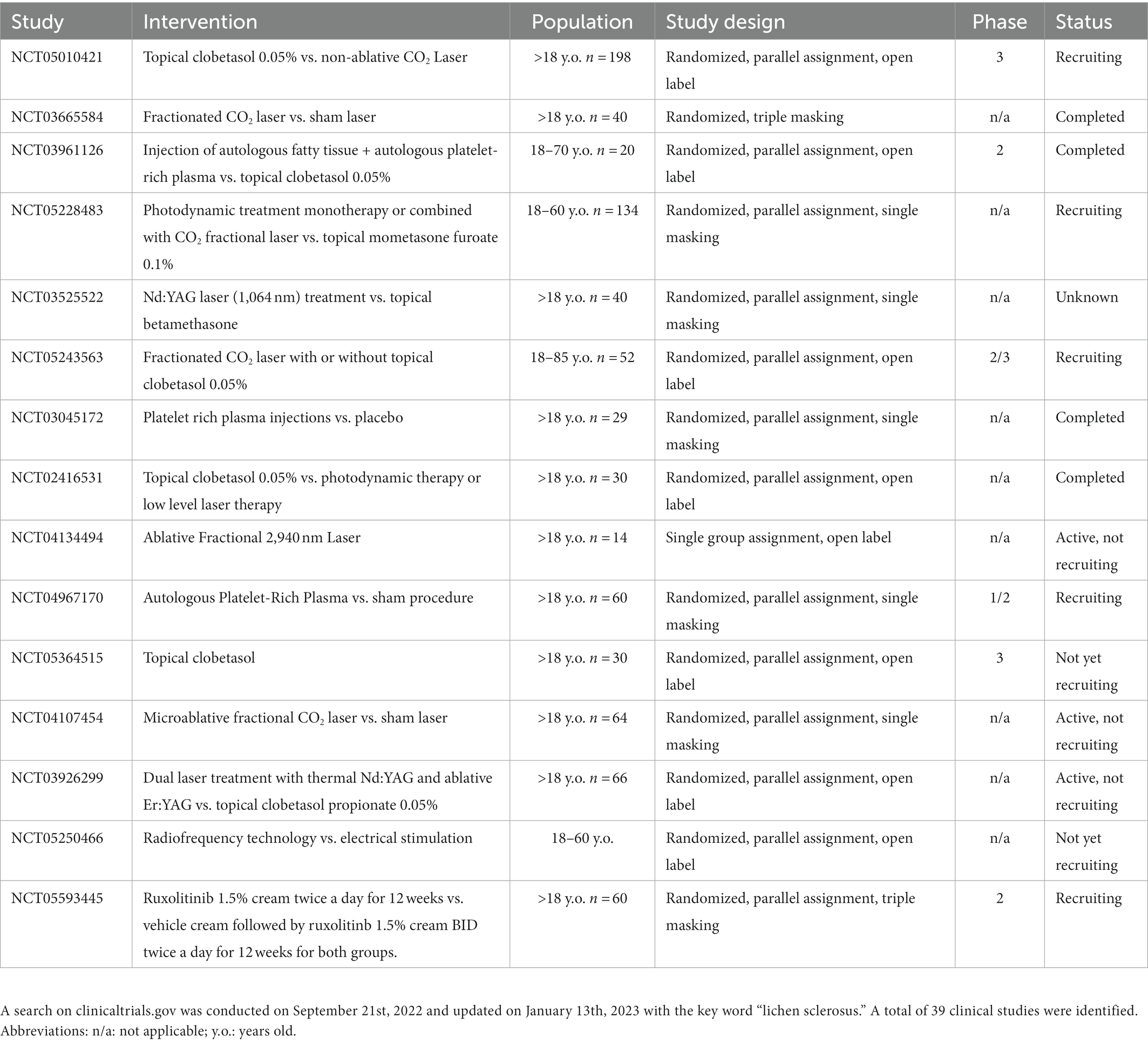
Table 7. Selected interventional clinical trials in female anogenital lichen sclerosus.
10.1. Topical treatment
A summary of topical and intralesional therapies in LS with recommendation grade and evidence level is described in Table 8.
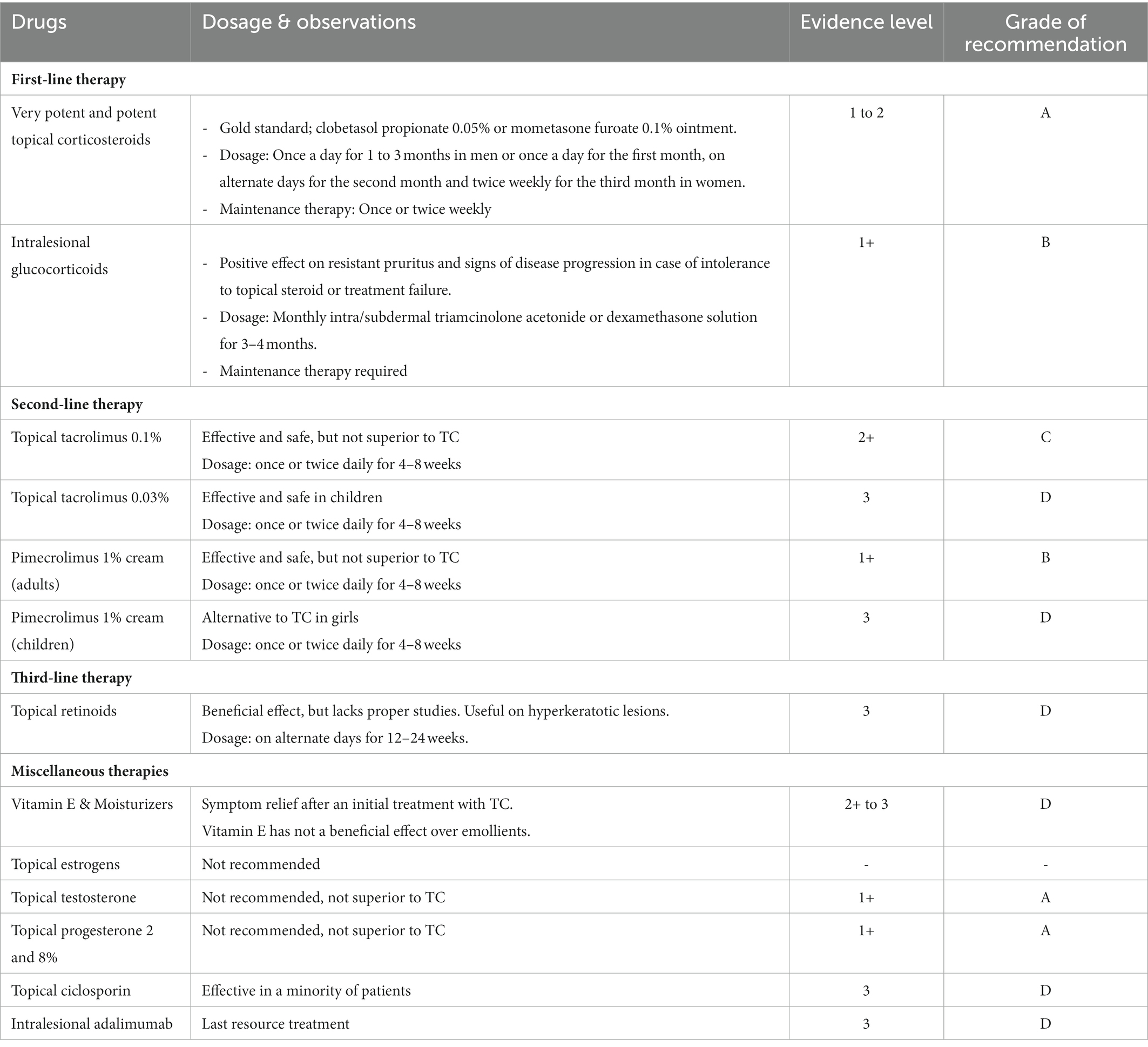
10.1.1. Glucocorticoids
Topical glucocorticosteroids are the first-line therapy in gLS (9). Most studies recommend clobetasol propionate 0.05% ointment (CP) daily, as it improves symptoms and signs in three quarters of VLS (146). A dose of 0.5 grams daily during 1 to 3 months applied to the affected area should be sufficient. The risk of adverse effects is low and some authors described no predisposition to infections, contact dermatitis and worsening of the skin atrophy (147). In a randomized trial in VLS, mometasone furoate 0.1% ointment (MF) showed a comparable efficacy and tolerability to CP (148). In a retrospective study of MGLS, topical CP during 3 months in decreasing application frequency was successful in almost 60% of MGLS, avoiding the subsequent necessity of circumcision (61).
In girls, CP 0.05% applied 3 months is also the most effective treatment to induce remission and manage the symptoms. Despite the good response, recurrences were reported in two-thirds of the girls within 1 year, requiring a new cycle of CP for 3 months and/or intermittent maintenance (149). In boys, the use of TC such as MF or betamethasone cream prevents circumcision in up to 35% of the cases (150, 151). The preputioplasty combined with intralesional corticosteroid is an effective alternative in boys, however, with a higher rate of relapse compared to circumcision (152).
Long-term treatment with ultrapotent or potent TC appears to be safe and effective and improves the QoL. Maintenance treatment has shown a greater effectiveness and it is usually more often required in VLS than in MGLS (9). A proactive maintenance treatment should be recommended after achieving remission, in order to prevent recurrence and malignity (3). In a cohort of 327 VLS patients, it was observed a symptom relief in 96% treated with ultrapotent TC, 66% became symptom free, while only 23% had completely reversed skin signs (11).
10.1.2. Calcineurin inhibitors
Calcineurin inhibitors, namely tacrolimus 0.1% ointment or pimecrolimus 1% cream once or twice a day for 1–2 months, can be considered as an off-label alternative in case of failure or intolerance to CP (3). Both in adults and children, topical calcineurin inhibitors are effective and safe alternatives to TC, nevertheless, CP seems to be more effective and should remain as the first-line therapy (153, 154). A relationship between calcineurin inhibitors and malignancy in LS has not yet been established (9).
10.2. UV light treatment
10.2.1. Phototherapy
UVA1 phototherapy is a potential first-line therapy for eLS, with an evidence level 1+ and recommendation grade B (9, 155). There are also reports of VLS treated successfully with narrowband UVB, UVA1 and topical PUVA phototherapy (156–158). However, phototherapy for VLS should be only indicated in case of failure to standard therapies, as it is not superior to TC regarding symptom relief, QoL and practicability (159). Furthermore, the well-known development of skin malignancy after phototherapy could be inconvenient in genital areas, as the risk of cancer per se in LS is increased (9).
10.2.2. Photodynamic therapy
Photodynamic therapy (PDT) with topical 5-aminolevulinic acid is a valid option to treat incoercible pruritus in VLS, when other therapies have failed (9). However, clinical and histological improvements are controversial (160). Objectively, some cases reported healing of superficial erosions and improvement of the clinical signs, whereas others demonstrated no clinical changes after PDT (161–164). Moreover, no improvement was revealed in the histopathological findings, while other authors described an augmented apoptosis and resolution of the chronic inflammation (165–167). Regarding adverse effects, burning sensation during PDT and lubrication disorders following the therapy were reported (165, 168). Recurrence of the VLS was observed by many authors after 3 to 9 months of therapeutic response (164, 169).
10.3. Systemic treatment
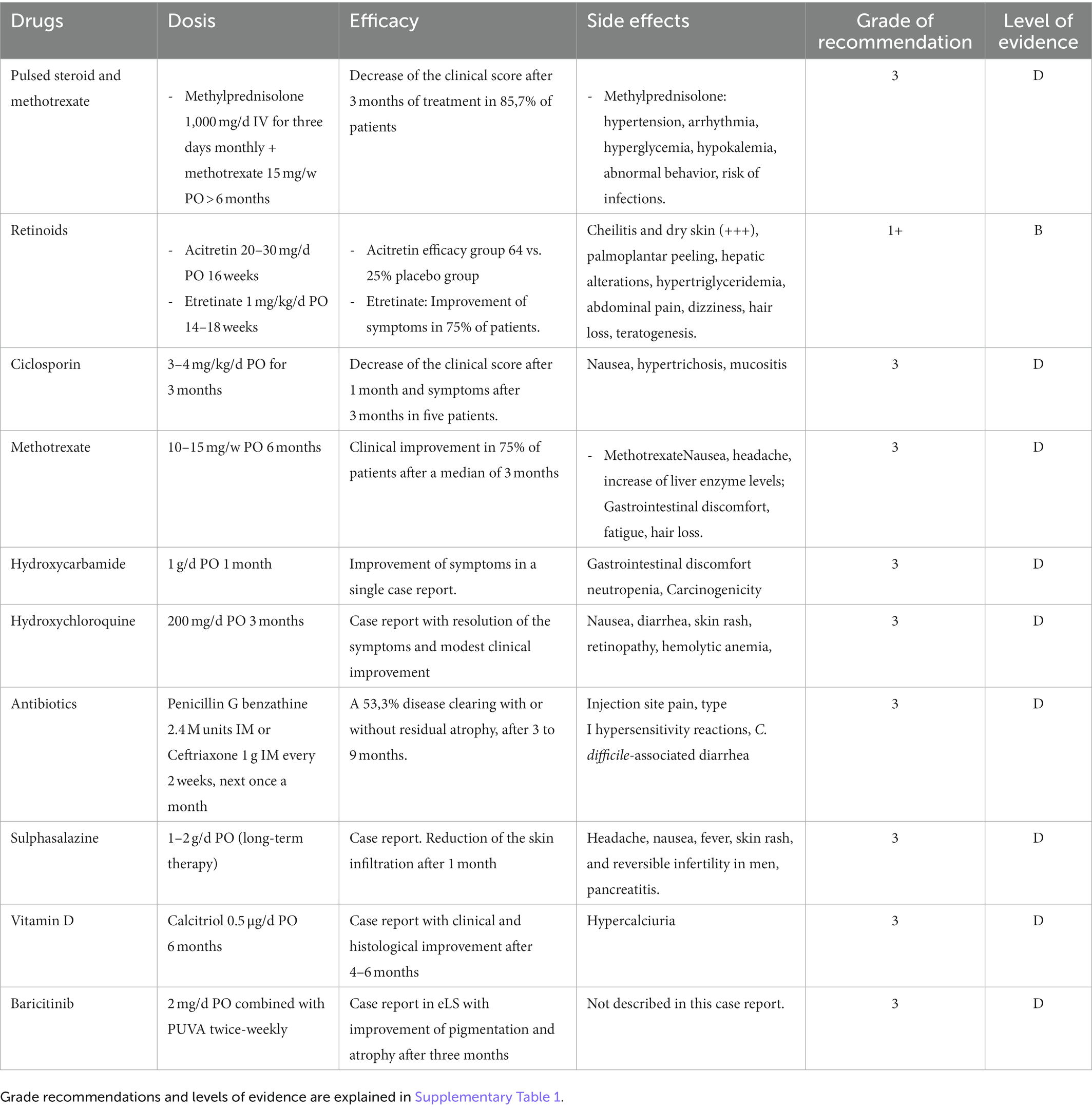
Systemic therapy is sporadically indicated and only recommended in widespread eLS or LS refractory to the standard topical treatment. In a retrospective study, pulsed high-dose corticosteroids combined with low-dose methotrexate therapy improved the clinical condition in refractory generalized eLS (170). Systemic retinoids such as etretinate and acitretin were effective in eLS, severe gLS or when other therapies failed to control the disease (171, 172). A list of systemic treatments with the recommended doses are enumerated in Table 9 (170–181).
10.4. Surgical treatment
There is no surgical first-line therapy for adult MGLS and recommendations are based on expert opinion or non-analytical studies (9, 182). Therefore, the initial treatment should include an ultrapotent TC for mild cases, and if the patient remains symptomatic after a sufficient conservative treatment, they should be offered a surgical option (9). Some of the proposed surgical techniques are circumcision, dilating or surgically correcting meatal stenosis, urethroplasty techniques and glans resurfacing with CO2 laser (Table 10) (183). An early complete circumcision in boys improves the prognosis of MGLS restricted to foreskin and glans, and it could also resolve the disease completely without any additional postoperative antiinflammatory treatment (184, 185). Recurrences are seldom after a complete foreskin removal, but the residual foreskin in partial circumcisions showed a recurrent disease in 50% of the patients (25). Glans and meatus involvement are negative prognostic factors for meatal stenosis and proximal urethral strictures (9, 186). Periodic dilations of strictures are a surgical option unlikely to be a permanent solution for MGLS. An indication for meatotomy is the meatal stenosis with uroflowmetry with a plateau phase under 10 ml/min (25, 187). Strictures longer than 2 cm, recurrent or penile urethral strictures could benefit from primary urethroplasty (188).
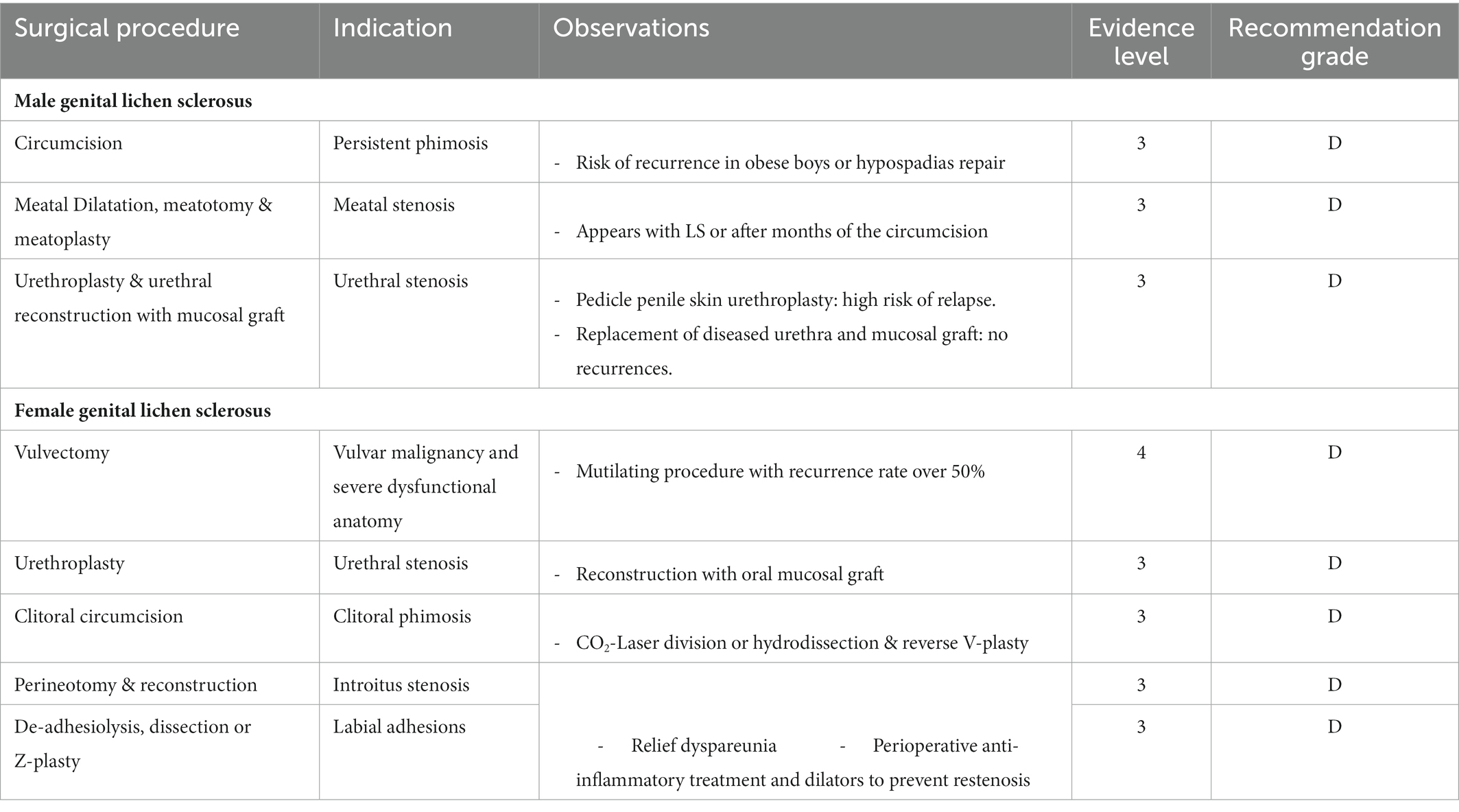
Surgery in VLS patients should be indicated in selected cases (Table 10) (9). Labial agglutination and clitoral hood scarring refractory to conservative treatments should be surgically corrected, in order to avoid obstructive urinary symptoms and for cosmetic reasons (189). Female sexual dysfunction due to severe clitoral phimosis can be treated with clitoral circumcision (190). Median perineotomy and perineoplasty are reserved for severe cases of introital stenosis, thus achieving an improvement in QoL (191, 192). Vulvectomy in LS is an invasive procedure with poor outcome and recurrence rate of up to 40–50% (193, 194). Hence, vulvectomy should only be performed in case of vulvar malignancy (9).
10.5. Miscellaneous treatments
10.5.1. Laser therapy
Laser therapy is an emerging therapeutic in gLS, despite the poor evidence and the lack of long-term data to support it (9, 195). Carbon-dioxide laser ablation may improve symptoms, signs and QoL in gLS and eLS. Long term remission of up to 14 years was described after CO2 therapy in a single arm trial, but only symptomatic patients were invited to a clinical examination to confirm the presence of LS (196). Nevertheless, some authors conclude that CO2 laser is not only superior to high-potent TC, but also not effective enough as monotherapy for VLS and it should be performed only as adjuvant therapy, in addition to TC (195, 197).
10.5.2. Focused ultrasound
High focused ultrasound (HIFU) has been demonstrated to be an effective treatment for VLS in pediatric and adolescent patients. HIFU is a nonsurgical treatment that relieves pruritus and stimulates cell proliferation and revascularization in order to repair damaged tissue (198). The common adverse effects are blistering and ulcers due to possible skin burns. After a follow-up of 5 years, the total response rate was 75%, and the recurrence rate was 12.5% (199). HIFU could be considered as an alternative if the standard treatment fails (9).
10.5.3. Regenerative therapies
The regenerative therapies could be considered as a therapeutic option for complications such as atrophy and scarring, when the first-line therapy is unresponsive. For instance, platelet rich plasma (PRP) seeks to repair damaged tissue and restore the skin function. PRP promotes angiogenesis, cell proliferation and differentiation and regulates the inflammatory cascades in LS (200). PRP improves QoL and the objective parameters in gLS (201, 202). However, the reports on PRP have a poor level of evidence due to a lack of standardization for PRP preparation and application (203).
11. Complications
11.1. Scarring
Lichen sclerosus in women leads to skin fragility, bleeding, chronic fissuring scars and secondary infections. It may evolve to a fusion of the labias, complete loss of the vulvar architecture, and narrowing of the vaginal introitus, preventing normal sexual intercourse. Furthermore, chronic anterior scarring can trap the clitoris within the clitoral hood, leading to phimosis and painful clitoral engorgement during arousal (clitoral pseudocyst) (13, 204, 205). After a long-term severe scarring may occur urinary retention, anal stenosis, obstruction and constipation (13).
In MGLS, preputial scarring leads to a frenulum contracture and a progressive fibrous phimosis with trans- and subcoronal adhesions. Frenulum scarring alters significantly QoL in men and a frenuloplasty in the context of complete circumcision should be recommended (124). Urethral involvement and urinary microincontinence is also reported in MGLS (9, 183, 206). To prevent further scarring after surgery, ultrapotent TC should be regularly applied, particularly around the coronal sulcus, if LS is still active (124).
11.2. Malignancy
LS in genital areas has a risk of neoplastic transformation to squamous cell carcinoma (SCC) (207, 208). Vulvar SCC was observed in 3.5 to 7% of women with VLS, while up to 65% of vulvar carcinomas arise on a background of VLS (209). Hence, early detection of premalignant lesions and a lifelong follow-up are required (13, 210). In a retrospective study, the neoplasia incidence rate in 976 women with VLS was 8.1 per 1,000 person-years, and the cumulative probability of progression to vulvar cancer escalates from 1.2% at 2 years to 36.8% at 25 years (211). In another cohort, VLS predisposed women under 70 years of age for vulvar SCC, with a attributable risk of 98% (209). Penile SCC was estimated in 4 to 13.4% of MGLS cases (210, 212, 213). Twelve percent of all penile SCC are entirely due to MGLS, whilst it was found that 29.4% of them arose in combination with histologically confirmed HPV (214).
The pathomechanism of malignancy in LS is unknown, but it is presumed that chronic inflammation, oxidative stress and single base substitution mutations at C742T and G818C in p53 could play an important role (215). Most cases of LS associated with SCC are not related to HPV infection and when detected, it may be a non-oncogenic type (216). Moreover, HPV-negative SCC associated with MGLS expresses p53 and lacks p16ink4a overexpression (217). While some authors mentioned that ultrapotent TC could act as risk for cancer due to local immunosuppression, one study shows a statistically significant lesser likelihood to develop malignancies when TC were regularly used as a prophylactic measure in asymptomatic VLS (9, 209, 218, 219).
There are also sporadic reports of concomitant melanoma, basal cell and Merkel carcinoma with LS, without any increased frequency (13). Other gynecologic malignancies have been reported in VLS. In a retrospective survey, the association between LS and endometrial and ovarian carcinoma was statistically significant, whereas colon cancer was not related to VLS. Furthermore, all patients with ovarian cancer had a history of LS. The association with breast cancer is controversial, as one work group found a higher frequency in LS, while another could not replicate this link (220, 221). When gynecologic cancers precedes VLS, the increased level of circulating extracellular matrix protein 1, estrogen status and radiotherapy could play a part in the development of VLS (220).
11.3. Psychosexual impact
LS negatively impacts on the psychosexual health of both women and men (9, 61). The late diagnosis of LS leads to frustration and delays in starting an adequate treatment (222). Both sexes experience a reduction in QoL in LS, but they might experience the symptomatology differently (223). Through DLQI assessment, VLS diminishes QoL and correlates with sexual functioning impairment, mostly attributed to the physical symptoms of LS and the feelings of embarrassment, anxiety, and stigma around open discussion of genital conditions (222, 223). More than a half of male and female LS patients experienced pain during sexual intercourse, but complaints about LS were higher in women (223, 224). The QoL in men after circumcision improved remarkably; however and despite adequate treatments, psychosexual issues may still persist in women, particularly in those with a higher degree of disease severity (225, 226).
11.4. Sensory abnormality
Vulvodynia, burning sensation around the glans and urethral meatus may occur after inflammatory diseases. The symptoms remain usually long after the disease has remitted. Neuropathic pain does not improve with TC and other approaches should be considered (124).
12. Follow-up
The follow-up visits in LS enables the assessment of the response to treatment and gives the opportunity to educate the patient as well as to rule out complications. The efficacy of the therapy should be evaluated by the improvement of the symptoms and clinical manifestations with photographic documentation, performed with every visit. For both uncomplicated VLS and MGLS, the first follow-up visit after 3 months, assesses the response and the proper use of CT, while a second follow-up visit 6 months later, gives the chance to discuss remaining problems. Patients with active ongoing disease require a long-term follow-up. Even after many years of resolved gLS, patients should seek referral to specialists in case of signs of recurrent disease (3, 124).
Men with persistent disease and phimosis, who do not respond to high potent TC after 3 months of treatment, should be reviewed for surgery. Histopathological studies should be performed in case of suspicious lesions. Patients with urinary and sexual symptoms should be referred to a urology specialist to measure flow rate and postvoid residual volume in order to identify and treat urethral stricture or meatal stenosis (227).
A long-term follow-up by secondary-care specialists should be proposed in VLS, when the patients had an atypical clinical course, uncontrolled symptoms with TC or previous cancer. Persistent erythematous lesions, erosions, ulcerations and hyperkeratotic plaques should be biopsied. Female patients who underwent surgery due to anatomical changes need a postoperative follow-up and TC in order to prevent recurrences (228).
13. Outlook
LS is an under-recognized and misdiagnosed dermatosis with a not-fully understood pathogenesis. The late recognition of LS may alter the QoL, lead to disfiguring anatomical changes and increase the risk of genital cancer. Although laser-based, regenerative therapies and more innovative approaches with topical JAK inhibitors are promising, ultrapotent topical corticosteroids are still the most commonly used first-line treatment. Periodic controls are necessary for the early detection of characteristic complications. Hopefully, with the emergence of new treatment options and proper high-quality studies, the pathogenetic and therapeutic landscape of LS will improve in the near future.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
Funding sources from Cluster of Excellence Precision Medicine in Chronic Inflammation (EXC 2167) and the Research Training Group Autoimmune Pre-Disease (GRK 2633), all from the Deutsche Forschungsgemeinschaft; and the Schleswig-Holstein Excellence-Chair Program from the State of Schleswig Holstein.
Conflict of interest
DT: Honoraria for participation on advisory boards, as a speaker and for consultancy from AbbVie, Almirall, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, Galapagos, Janssen, LEO Pharma, Morphosis, Novartis, Pfizer, Regeneron, Samsung, Sandoz, Sanofi Genzyme, and UCB Pharma; research grants received from LEO Pharma, and Novartis.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2023.1106318/full#supplementary-material
References
1. Hallopeau, H. Leçons cliniques sur les maladies cutanées et syphilitiques. Union Med Can. (1887) 43:472.
2. Kaufman, RH, DiPaola, GR, Friedrich, EG Jr, Hewitt, J, and Woodruff, JD. New nomenclature for vulvar disease. J Cutan Pathol. (1976) 3:159–61. doi: 10.1111/j.1600-0560.1976.tb01105.x
3. Papini, M, Russo, A, Simonetti, O, Borghi, A, Corazza, M, Piaserico, S, et al. Mucous membrane disorders research group of SIDeMaST. Diagnosis and management of cutaneous and anogenital lichen sclerosus: recommendations from the Italian Society of Dermatology (SIDeMaST). Ital J Dermatol Venerol. (2021) 156:519–33. doi: 10.23736/S2784-8671.21.06764-X
4. Schlosser, BJ, and Mirowski, GW. Lichen sclerosus and lichen planus in women and girls. Clin Obstet Gynecol. (2015) 58:125–42. doi: 10.1097/GRF.0000000000000090
5. Krapf, JM, Mitchell, L, Holton, MA, and Goldstein, AT. Vulvar lichen Sclerosus: current perspectives. Int J Women's Health. (2020) 12:11–20. doi: 10.2147/IJWH.S191200
6. Ganesan, L, Parmar, H, Das, JK, and Gangopadhyay, A. Extragenital lichen Sclerosus et Atrophicus. Indian J Dermatol. (2015) 60:420. doi: 10.4103/0019-5154.160516
7. Matela, AM, Hagström, J, and Ruokonen, H. Lichen sclerosus of the oral mucosa: clinical and histopathological findings. Review of the literature and a case report. Acta Odontol Scand. (2018) 76:364–3. doi: 10.1080/00016357.2018.1463452
9. Kirtschig, G, Becker, K, Günthert, A, Jasaitiene, D, Cooper, S, Chi, CC, et al. Evidence-based (S3) guideline on (anogenital) lichen sclerosus. J Eur Acad Dermatol Venereol. (2015) 29:e1–e43. doi: 10.1111/jdv.13136
10. Halonen, P, Jakobsson, M, Heikinheimo, O, Riska, A, Gissler, M, and Pukkala, E. Lichen sclerosus and risk of cancer. Int J Cancer. (2017) 140:1998–2002. doi: 10.1002/ijc.30621
11. Cooper, SM, Gao, XH, Powell, JJ, and Wojnarowska, F. Does treatment of vulvar lichen sclerosus influence its prognosis? Arch Dermatol. (2004) 140:702–6. doi: 10.1001/archderm.140.6.702
12. Higgins, CA, and Cruickshank, ME. A population-based case-control study of aetiological factors associated with vulval lichen sclerosus. J Obstet Gynaecol. (2012) 32:271–5. doi: 10.3109/01443615.2011.649320
13. Singh, N, and Ghatage, P. Etiology, clinical features, and diagnosis of vulvar lichen sclerosus: a scoping review. Obstet Gynecol Int. (2020) 2020:1–8. doi: 10.1155/2020/7480754
14. Krapf, JM, Smith, AB, Cigna, ST, and Goldstein, AT. Presenting symptoms and diagnosis of vulvar lichen sclerosus in premenopausal women: a cross-sectional study. J Low Genit Tract Dis. (2022) 26:271–5. doi: 10.1097/LGT.0000000000000679
15. Goldstein, AT, Marinoff, SC, Christopher, K, and Srodon, M. Prevalence of vulvar lichen sclerosus in a general gynecology practice. J Reprod Med. (2005) 50:477–80.
16. Kizer, WS, Prarie, T, and Morey, AF. Balanitis xerotica obliterans: epidemiologic distribution in an equal access health care system. South Med J. (2003) 96:9–11. doi: 10.1097/00007611-200301000-00004
17. Kantere, D, Löwhagen, GB, Alvengren, G, Månesköld, A, Gillstedt, M, and Tunbäck, P. The clinical spectrum of lichen sclerosus in male patients - a retrospective study. Acta Derm Venereol. (2014) 94:542–6. doi: 10.2340/00015555-1797
18. Leibovitz, A, Kaplun, VV, Saposhnicov, N, and Habot, B. Vulvovaginal examinations in elderly nursing home women residents. Arch Gerontol Geriatr. (2000) 31:1–4. doi: 10.1016/s0167-4943(00)00059-5
19. Kirtschig, G. Lichen Sclerosus-presentation, diagnosis and management. Dtsch Arztebl Int. (2016) 113:337–43. doi: 10.3238/arztebl.2016.0337
20. Nelson, DM, and Peterson, AC. Lichen sclerosus: epidemiological distribution in an equal access health care system. J Urol. (2011) 185:522–5. doi: 10.1016/j.juro.2010.09.107
21. Kyriakis, KP, Emmanuelides, S, Terzoudi, S, Palamaras, I, Damoulaki, E, and Evangelou, G. Gender and age prevalence distributions of morphea en plaque and anogenital lichen sclerosus. J Eur Acad Dermatol Venereol. (2007) 21:825–6. doi: 10.1111/j.1468-3083.2006.01954.x
22. Balakirski, G, Grothaus, J, Altengarten, J, and Ott, H. Paediatric lichen sclerosus: a systematic review of 4516 cases. Br J Dermatol. (2020) 182:231–3. doi: 10.1111/bjd.18267
23. Powell, J, and Wojnarowska, F. Childhood vulvar lichen sclerosus: an increasingly common problem. J Am Acad Dermatol. (2001) 44:803–6. doi: 10.1155/2020/7480754
24. Aziz Filho, AM, de Azevedo, LMS, Rochael, MC, and de Jesus, LE. Frequency of lichen sclerosus in children presenting with phimosis: a systematic histological study. J Pediatr Urol. (2022) 18:529.e1–6. doi: 10.1016/j.jpurol.2022.06.030
25. Becker, K. Lichen sclerosus in boys. Dtsch Arztebl Int. (2011) 108:53–8. doi: 10.3238/arztebl.2011.053
26. Fistarol, SK, and Itin, PH. Diagnosis and treatment of lichen sclerosus: an update. Am J Clin Dermatol. (2013) 14:27–47. doi: 10.1007/s40257-012-0006-4
27. Arif, T, Fatima, R, and Sami, M. Extragenital lichen sclerosus: a comprehensive review. Australas J Dermatol. (2022) 63:452–62. doi: 10.1111/ajd.13890. [Epub ahead of print]
28. Diwan, NG, and Nair, PA. Extragenital lichen sclerosus et atrophicus along the lines of Blaschko. Indian Dermatol Online J. (2015) 6:342–4. doi: 10.4103/2229-5178.164486
29. Sherman, V, McPherson, T, Baldo, M, Salim, A, Gao, XH, and Wojnarowska, F. The high rate of familial lichen sclerosus suggests a genetic contribution: an observational cohort study. J Eur Acad Dermatol Venereol. (2010) 24:1031–4. doi: 10.1111/j.1468-3083.2010.03572.x
30. Khan Mohammad Beigi, P. The immunogenetics of morphea and lichen sclerosus. Adv Exp Med Biol. (2022) 1367:155–72. doi: 10.1007/978-3-030-92616-8_7
31. Powell, J, Wojnarowska, F, Winsey, S, Marren, P, and Welsh, K. Lichen sclerosus premenarche: autoimmunity and immunogenetics. Br J Dermatol. (2000) 142:481–4. doi: 10.1046/j.1365-2133.2000.03360.x
32. Azurdia, RM, Luzzi, GA, Byren, I, Welsh, K, Wojnarowska, F, Marren, P, et al. Lichen sclerosus in adult men: a study of HLA associations and susceptibility to autoimmune disease. Br J Dermatol. (1999) 140:79–83. doi: 10.1046/j.1365-2133.1999.02611.x
33. Marren, P, Yell, J, Charnock, FM, Bunce, M, Welsh, K, and Wojnarowska, F. The association between lichen sclerosus and antigens of the HLA system. Br J Dermatol. (1995) 132:197–203. doi: 10.1111/j.1365-2133.1995.tb05013.x
34. Gao, XH, Barnardo, MC, Winsey, S, Ahmad, T, Cook, J, Agudelo, JD, et al. The association between HLA DR, DQ antigens, and vulval lichen sclerosus in the UK: HLA DRB112 and its associated DRB112/DQB10301/04/09/010 haplotype confers susceptibility to vulval lichen sclerosus, and HLA DRB10301/04 and its associated DRB10301/04/DQB10201/02/03 haplotype protects from vulval lichen sclerosus. J Invest Dermatol. (2005) 125:895–9. doi: 10.1111/j.0022-202X.2005.23905.x
35. Liu, GL, Cao, FL, Zhao, MY, Shi, J, and Liu, SH. Associations between HLA-A\B\DRB1 polymorphisms and risks of vulvar lichen sclerosus or squamous cell hyperplasia of the vulva. Genet Mol Res. (2015) 14:15962–71. doi: 10.4238/2015.December.7.8
36. Soufir, N, Queille, S, Liboutet, M, Thibaudeau, O, Bachelier, F, Delestaing, G, et al. Inactivation of the CDKN2A and the p53 tumour suppressor genes in external genital carcinomas and their precursors. Br J Dermatol. (2007) 156:448–53. doi: 10.1111/j.1365-2133.2006.07604.x
37. Gambichler, T, Terras, S, Kreuter, A, and Skrygan, M. Altered global methylation and hydroxymethylation status in vulvar lichen sclerosus: further support for epigenetic mechanisms. Br J Dermatol. (2014) 170:687–93. doi: 10.1111/bjd.12702
38. Dumitrescu, RG. Epigenetic markers of early tumor development. Methods Mol Biol. (2012) 863:3–14. doi: 10.1007/978-1-61779-612-8_1
39. Tran, DA, Tan, X, Macri, CJ, Goldstein, AT, and Fu, SW. Lichen sclerosus: an autoimmunopathogenic and genomic enigma with emerging genetic and immune targets. Int J Biol Sci. (2019) 15:1429–39. doi: 10.7150/ijbs.34613
40. Terlou, A, Santegoets, LA, van der Meijden, WI, Heijmans-Antonissen, C, Swagemakers, SM, van der Spek, PJ, et al. An autoimmune phenotype in vulvar lichen sclerosus and lichen planus: a Th1 response and high levels of microRNA-155. J Invest Dermatol. (2012) 132:658–66. doi: 10.1038/jid.2011.369
41. Farrell, AM, Dean, D, Millard, PR, Charnock, FM, and Wojnarowska, F. Cytokine alterations in lichen sclerosus: an immunohistochemical study. Br J Dermatol. (2006) 155:931–40. doi: 10.1111/j.1365-2133.2006.07414.x
42. Pilatz, A, Altinkilic, B, Schormann, E, Maegel, L, Izykowski, N, Becker, J, et al. Congenital phimosis in patients with and without lichen sclerosus: distinct expression patterns of tissue remodeling associated genes. J Urol. (2013) 189:268–74. doi: 10.1016/j.juro.2012.09.010
43. Wang, L, Yi, JL, Chen, HY, Wang, PL, and Shen, YL. Level of Foxp3, DNMTs, methylation of Foxp3 promoter region, and CD4 + CD25 + CD127low regulatory T cells in vulvar lichen sclerosus. Kaohsiung J Med Sci. (2021) 37:520–7. doi: 10.1002/kjm2.12356
44. Edmonds, EV, Oyama, N, Chan, I, Francis, N, McGrath, JA, and Bunker, CB. Extracellular matrix protein 1 autoantibodies in male genital lichen sclerosus. Br J Dermatol. (2011) 165:218–9. doi: 10.1111/j.1365-2133.2011.10326.x
45. Howard, A, Dean, D, Cooper, S, Kirtshig, G, and Wojnarowska, F. Circulating basement membrane zone antibodies are found in lichen sclerosus of the vulva. Australas J Dermatol. (2004) 45:12–5. doi: 10.1111/j.1440-0960.2004.00026.x
46. Kaya, G, Augsburger, E, Stamenkovic, I, and Saurat, JH. Decrease in epidermal CD44 expression as a potential mechanism for abnormal hyaluronate accumulation in superficial dermis in lichen sclerosus et atrophicus. J Invest Dermatol. (2000) 115:1054–8. doi: 10.1046/j.1523-1747.2000.00194.x
47. Kaya, G, and Saurat, JH. Restored epidermal CD44 expression in lichen sclerosus et atrophicus and clinical improvement with topical application of retinaldehyde. Br J Dermatol. (2005) 152:570–2. doi: 10.1111/j.1365-2133.2005.06396.x
48. Farrell, AM, Marren, P, Dean, D, and Wojnarowska, F. Lichen sclerosus: evidence that immunological changes occur at all levels of the skin. Br J Dermatol. (1999) 140:1087–92. doi: 10.1046/j.1365-2133.1999.02909.x
49. Ren, L, Zhao, Y, Huo, X, and Wu, X. MiR-155-5p promotes fibroblast cell proliferation and inhibits FOXO signaling pathway in vulvar lichen sclerosis by targeting FOXO3 and CDKN1B. Gene. (2018) 653:43–50. doi: 10.1016/j.gene.2018.01.049
50. Fujimoto, N, Terlizzi, J, Aho, S, Brittingham, R, Fertala, A, Oyama, N, et al. Extracellular matrix protein 1 inhibits the activity of matrix metalloproteinase 9 through high-affinity protein/protein interactions. Exp Dermatol. (2006) 15:300–7. doi: 10.1111/j.0906-6705.2006.00409.x
51. Godoy, CA, Teodoro, WR, Velosa, AP, Garippo, AL, Eher, EM, Parra, ER, et al. Unusual remodeling of the hyalinization band in vulval lichen sclerosus by type V collagen and ECM 1 protein. Clinics (Sao Paulo). (2015) 70:356–62. doi: 10.6061/clinics/2015(05)09
52. Lee, JS, Ys, L, Jeon, B, Yj, J, Yoo, H, and Kim, TY. EC-SOD induces apoptosis through COX-2 and galectin-7 in the epidermis. J Dermatol Sci. (2012) 65:126–33. doi: 10.1016/j.jdermsci.2011.12.013
53. Zhao, Y, Zhao, S, Li, H, Qin, X, and Wu, X. Expression of galectin-7 in vulvar lichen sclerosus and its effect on dermal fibroblasts. Oncol Lett. (2018) 16:2559–64. doi: 10.3892/ol.2018.8897
54. Paulis, G, and Berardesca, E. Lichen sclerosus: the role of oxidative stress in the pathogenesis of the disease and its possible transformation into carcinoma. Res Rep Urol. (2019) 11:223–32. doi: 10.2147/RRU.S205184
55. Sander, CS, Ali, I, Dean, D, Thiele, JJ, and Wojnarowska, F. Oxidative stress is implicated in the pathogenesis of lichen sclerosus. Br J Dermatol. (2004) 151:627–35. doi: 10.1111/j.1365-2133.2004.06142.x
56. Zannoni, GF, Faraglia, B, Tarquini, E, Camerini, A, Vrijens, K, Migaldi, M, et al. Expression of the CDK inhibitor p27kip1 and oxidative DNA damage in non-neoplastic and neoplastic vulvar epithelial lesions. Mod Pathol. (2006) 19:504–13. doi: 10.1038/modpathol.3800532
57. Liegl, B, and Regauer, S. p53 immunostaining in lichen sclerosus is related to ischaemic stress and is not a marker of differentiated vulvar intraepithelial neoplasia (d-VIN). Histopathology. (2006) 48:268–74. doi: 10.1111/j.1365-2559.2005.02321.x
58. Vanin, K, Scurry, J, Thorne, H, Yuen, K, and Ramsay, RG. Overexpression of wild-type p53 in lichen sclerosus adjacent to human papillomavirus-negative vulvar cancer. J Invest Dermatol. (2002) 119:1027–33. doi: 10.1046/j.1523-1747.2002.19513.x
59. Kirby, L, Gran, S, Orekoya, F, Owen, C, and Simpson, R. Is urinary incontinence associated with vulval lichen sclerosus in women? A cross‐sectional study. Br J Dermatol Syph. (2021) 185:1063–5. doi: 10.1111/bjd.20583
60. Panou, E, Panagou, E, Foley, C, Kravvas, G, Watchorn, R, Alnajjar, H, et al. Male genital lichen sclerosus associated with urological interventions and microincontinence: a case series of 21 patients. Clin Exp Dermatol. (2022) 47:107–9. doi: 10.1111/ced.14869
61. Edmonds, EV, Hunt, S, Hawkins, D, Dinneen, M, Francis, N, and Bunker, CB. Clinical parameters in male genital lichen sclerosus: a case series of 329 patients. J Eur Acad Dermatol Venereol. (2012) 26:730–7. doi: 10.1111/j.1468-3083.2011.04155.x
62. Bunker, CB. Occlusion, urine and genital lichen sclerosus. Indian J Dermatol Venereol Leprol. (2012) 78:367–8. doi: 10.4103/0378-6323.95461
63. Vishwanath, T, Ghate, S, Shinde, G, Lahoria, V, Binny, B, and Sonwane, A. Koebnerization of lichen sclerosus et atrophicus at insulin injection sites - a rare case with dermoscopic features. Indian J Dermatol. (2021) 66:224. doi: 10.4103/ijd.IJD_634_18
64. Requena López, S, Hidalgo García, Y, Gómez Díez, S, and Vivanco, AB. Morphea and extragenital lichen sclerosus et atrophicus after influenza vaccination. Actas Dermosifiliogr (Engl Ed). (2018) 109:86–8. doi: 10.1016/j.ad.2017.05.016
65. Arif, T, Adil, M, Amin, SS, and Mahtab, A. Concomitant morphea and lichen sclerosus et atrophicus in the same plaque at the site of intramuscular drug injection: an interesting case presentation. Acta Dermatovenerol Alp Pannonica Adriat. (2018) 27:111–3. doi: 10.15570/actaapa.2018.23
66. Al-Niaimi, F, and Lyon, C. Peristomal lichen sclerosus: the role of occlusion and urine exposure? Br J Dermatol. (2013) 168:643–6. doi: 10.1111/bjd.12014
67. De Giorgi, V, Scarfì, F, Silvestri, F, Maida, P, Venturi, F, Trane, L, et al. Genital piercing: a warning for the risk of vulvar lichen sclerosus. Dermatol Ther. (2021) 34:e14703. doi: 10.1111/dth.14703
68. Chan, S, Watchorn, RE, Muneer, A, and Bunker, CB. Lichen sclerosus following genital piercing. Int J STD AIDS. (2022) 33:095646242210790–4. doi: 10.1177/09564624221079068
69. Bonfill-Ortí, M, Martínez-Molina, L, Penín, RM, and Marcoval, J. Extragenital lichen Sclerosus induced by radiotherapy. Actas Dermosifiliogr (Engl Ed). (2019) 110:69–71. doi: 10.1016/j.ad.2017.09.024
70. Nemer, KM, and Anadkat, MJ. Postirradiation lichen sclerosus et atrophicus. JAMA Dermatol. (2017) 153:1067–9. doi: 10.1001/jamadermatol.2017.0823
71. Edwards, LR, Privette, ED, Patterson, JW, Tchernev, G, Chokoeva, AA, Wollina, U, et al. Radiation-induced lichen sclerosus of the vulva: first report in the medical literature. Wien Med Wochenschr. (2017) 167:74–7. doi: 10.1007/s10354-016-0525-3
72. Orszulak, D, Dulska, A, Niziński, K, Skowronek, K, Bodziony, J, Stojko, R, et al. Pediatric vulvar lichen sclerosus-a review of the literature. Int J Environ Res Public Health. (2021) 18:7153. doi: 10.3390/ijerph18137153. doi: 10.1111/j.1365-2133.2007.08371.x
73. Taylor, AH, Guzail, M, and Al-Azzawi, F. Differential expression of oestrogen receptor isoforms and androgen receptor in the normal vulva and vagina compared with vulval lichen sclerosus and chronic vaginitis. Br J Dermatol. (2008) 158:319–28. doi: 10.1111/j.1365-2133.2007.08371.x
74. Friedrich, EG Jr, and Kalra, PS. Serum levels of sex hormones in vulvar lichen sclerosus, and the effect of topical testosterone. N Engl J Med. (1984) 310:488–91. doi: 10.1056/NEJM198402233100803
75. Clifton, MM, Garner, IB, Kohler, S, and Smoller, BR. Immunohistochemical evaluation of androgen receptors in genital and extragenital lichen sclerosus: evidence for loss of androgen receptors in lesional epidermis. J Am Acad Dermatol. (1999) 41:43–6. doi: 10.1016/s0190-9622(99)70404-4
76. Günthert, AR, Faber, M, Knappe, G, Hellriegel, S, and Emons, G. Early onset vulvar lichen Sclerosus in premenopausal women and oral contraceptives. Eur J Obstet Gynecol Reprod Biol. (2008) 137:56–60. doi: 10.1016/j.ejogrb.2007.10.005
77. Günthert, AR, Limacher, A, Beltraminelli, H, Krause, E, Mueller, MD, Trelle, S, et al. Efficacy of topical progesterone versus topical clobetasol propionate in patients with vulvar lichen sclerosus - a double-blind randomized phase II pilot study. Eur J Obstet Gynecol Reprod Biol. (2022) 272:88–95. doi: 10.1016/j.ejogrb.2022.03.020
78. Prowse, DM, Ktori, EN, Chandrasekaran, D, Prapa, A, and Baithun, S. Human papillomavirus-associated increase in p16INK4A expression in penile lichen sclerosus and squamous cell carcinoma. Br J Dermatol. (2008) 158:261–5. doi: 10.1111/j.1365-2133.2007.08305.x
79. de Martino, M, Haitel, A, Wrba, F, Schatzl, G, Klatte, T, and Waldert, M. High-risk human papilloma virus infection of the foreskin in asymptomatic boys. Urology. (2013) 81:869–72. doi: 10.1016/j.urology.2012.12.011
80. Edmonds, E, Barton, G, Buisson, S, Francis, N, Gotch, F, Game, L, et al. Gene expression profiling in male genital lichen sclerosus. Int J Exp Pathol. (2011) 92:320–5. doi: 10.1111/j.1365-2613.2011.00779.x
81. Shim, TN, Harwood, CA, Marsh, SG, Gotch, FM, Quint, W, de Koning, MN, et al. Immunogenetics and human papillomavirus (HPV) in male genital lichen sclerosus (MGLSc). Int J STD AIDS. (2020) 31:1334–9. doi: 10.1177/0956462420949395
82. Alonso-Llamazares, J, Persing, DH, Anda, P, Gibson, LE, Rutledge, BJ, and Iglesias, L. No evidence for Borrelia burgdorferi infection in lesions of morphea and lichen sclerosus et atrophicus in Spain. A prospective study and literature review. Acta Derm Venereol. (1997) 77:299–304. doi: 10.2340/0001555577299304
83. Ena, P, Lorrai, P, Pintus, A, Marras, V, and Dessy, LA. Development of multifocal squamous cell carcinoma in lichen sclerosus et atrophicus of the penis associated to HCV hepatitis. Andrologia. (2004) 36:38–40. doi: 10.1046/j.1439-0272.2003.00600.x
84. Boulinguez, S, Bernard, P, Lacour, JP, Nicot, T, Bedane, C, Ortonne, JP, et al. Bullous lichen sclerosus with chronic hepatitis C virus infection. Br J Dermatol. (1997) 137:474–6. doi: 10.1111/j.1365-2133.1997.tb03767.x
85. Cong, Q, Guo, X, Zhang, S, Wang, J, Zhu, Y, Wang, L, et al. HCV poly U/UC sequence-induced inflammation leads to metabolic disorders in vulvar lichen sclerosis. Life Sci Alliance. (2021) 4:e202000906. doi: 10.26508/lsa.202000906
86. Shim, TN, and Bunker, CB. Male genital lichen sclerosus and hepatitis C. Br J Dermatol. (2012) 167:1398–9. doi: 10.1111/j.1365-2133.2012.11065.x
87. Yang, M, Sun, K, and Chang, J. Screening differential circular RNAs expression profiles in vulvar lichen Sclerosus. Biomed Eng Online. (2022) 21:51. doi: 10.1186/s12938-022-01013-7
88. Mühl, S, Ehrchen, J, and Metze, D. Blistering and skin fragility due to imatinib therapy: loss of laminin and collagen IV as a possible cause of cutaneous basement membrane instability. Am J Dermatopathol. (2018) 40:371–4. doi: 10.1097/DAD.0000000000001063
89. Skupsky, H, Abuav, R, High, W, Pass, C, and Goldenberg, G. Development of lichen sclerosus et atrophicus while receiving a therapeutic dose of imatinib mesylate for chronic myelogenous leukemia. J Cutan Pathol. (2010) 37:877–80. doi: 10.1111/j.1600-0560.2009.01398.x
90. Pranteda, G, Muscianese, M, Grimaldi, M, Fidanza, L, Pranteda, G, Narcisi, A, et al. Lichen sclerosus et atrophicus induced by carbamazepine: a case report. Int J Immunopathol Pharmacol. (2013) 26:791–4. doi: 10.1177/039463201302600326
91. Conteduca, V, Medri, M, Mazzoni, L, De Giorgi, U, and Stanganelli, I. Anogenital lichen sclerosus et atrophicus lesions in a case series of cancer patients on immunotherapy. Cancer Immunol Immunother. (2022) 71:1545–8. doi: 10.1007/s00262-021-03094-0
92. Seyed Jafari, SM, Feldmeyer, L, and Hunger, RE. Development of extragenital lichen sclerosus in malignant melanoma patients treated with Ipilimumab in combination with nivolumab. Front Oncol. (2020) 10:573527. doi: 10.3389/fonc.2020.573527
93. Miraglia, E, Soda, G, and Giustini, S. Genital lichen sclerosus after nivolumab. Dermatol Online J. (2020) 26:13030. doi: 10.5070/D32611047516
94. Baldo, M, Ali, I, and Wojnarowska, F. The contribution of drugs to lichen sclerosus. Clin Exp Dermatol. (2014) 39:234. doi: 10.1111/ced.12264
95. Gautam, MM, Singh, V, Nadkarni, NJ, and Patil, SP. Anogenital lichen sclerosus. Indian J Sex Transm Dis AIDS. (2020) 41:1–9. doi: 10.4103/ijstd.IJSTD_49_17
96. Navarro-Crummenauer, B, Pickhardt, CP, and Urban, R. Lichen sclerosus mistaken for sexual abuse--prevention of victimization. Klin Padiatr. (2015) 227:239–42. doi: 10.1055/s-0034-1395616
97. Promm, M, Rösch, WH, and Kirtschig, G. Lichen sclerosus im kindesalter [Lichen sclerosus in children]. Urologe A. (2020) 59:271–7. doi: 10.1007/s00120-020-01140-w
98. Powell, JJ, and Wojnarowska, F. Lichen sclerosus. Lancet. (1999) 353:1777–83. doi: 10.1016/s0140-6736(98)08228-2
99. Meffert, JJ, Davis, BM, and Grimwood, RE. Lichen sclerosus. J Am Acad Dermatol. (1995) 32:393–416; quiz 417-8. doi: 10.1016/0190-9622(95)90060-8
100. Khatib, J, Wargo, JJ, Krishnamurthy, S, and Travers, JB. Hemorrhagic bullous lichen sclerosus: a case report. Am J Case Rep. (2020) 21:e919353. doi: 10.12659/AJCR.919353
101. Sauder, MB, Linzon-Smith, J, and Beecker, J. Extragenital bullous lichen sclerosus. J Am Acad Dermatol. (2014) 71:981–4. doi: 10.1016/j.jaad.2014.06.037
102. Burshtein, A, Burshtein, J, and Rekhtman, S. Extragenital lichen sclerosus: a comprehensive review of clinical features and treatment. Arch Dermatol Res. (2022). doi: 10.1007/s00403-022-02397-1. [Epub ahead of print]
103. Bevans, SL, Keeley, JM, and Sami, N. Oral lichen sclerosus-a review of clinical presentation, treatment, and clinical outcomes. Oral Surg Oral Med Oral Pathol Oral Radiol. (2017) 124:e243–8. doi: 10.1016/j.oooo.2017.07.005
104. Kakko, T, Salo, T, and Siponen, MK. Oral lichen sclerosus: a systematic review of reported cases and two new cases. Int J Dermatol. (2018) 57:521–8. doi: 10.1111/ijd.13870
105. Niamh, L, Naveen, S, and Hazel, B. Diagnosis of vulval inflammatory dermatoses: a pathological study with clinical correlation. Int J Gynecol Pathol. (2009) 28:554–8. doi: 10.1097/PGP.0b013e3181cff7d5
106. Morrel, B, Ewing-Graham, PC, van der Avoort, IAM, Pasmans, SGMA, and Damman, J. Structured analysis of histopathological characteristics of vulvar lichen sclerosus in a juvenile population. Hum Pathol. (2020) 106:23–31. doi: 10.1016/j.humpath.2020.09.003
107. Attili, VR, and Attili, SK. Clinical and histopathological spectrum of genital lichen sclerosus in 133 cases: focus on the diagnosis of pre-sclerotic disease. Indian J Dermatol Venereol Leprol. (2022) 88:774–80. doi: 10.25259/IJDVL_640_20
108. Hussein, MRA. Immunohistological analysis of CD34-positive dermal dendritic cells and microvessel density in the genital and extragenital lichen sclerosus. Actas Dermosifiliogr (Engl Ed). (2021) S0001-7310:00114–9. doi: 10.1016/j.ad.2021.02.009
109. Marren, P, Dean, D, Charnock, M, and Wojnarowska, F. The basement membrane zone in lichen sclerosus: an immunohistochemical study. Br J Dermatol. (1997) 136:508–14. doi: 10.1046/j.1365-2133.1997.6061582.x
110. Cooper, SM, Ali, I, Baldo, M, and Wojnarowska, F. The association of lichen sclerosus and erosive lichen planus of the vulva with autoimmune disease: a case-control study. Arch Dermatol. (2008) 144:1432–5. doi: 10.1001/archderm.144.11.1432
111. Kreuter, A, Kryvosheyeva, Y, Terras, S, Moritz, R, Möllenhoff, K, Altmeyer, P, et al. Association of autoimmune diseases with lichen sclerosus in 532 male and female patients. Acta Derm Venereol. (2013) 93:238–41. doi: 10.2340/00015555-1512
112. Fan, R, Leasure, AC, Maisha, FI, Cohen, JM, and Little, AJ. Thyroid disorders associated with lichen sclerosus: a case-control study in the all of us research program. Br J Dermatol. (2022) 187:797–9. doi: 10.1111/bjd.21702. [Epub ahead of print]
113. Arousse, A, Boussofara, L, Mokni, S, Gammoudi, R, Saidi, W, Aounallah, A, et al. Alopecia areata in Tunisia: epidemio-clinical aspects and comorbid conditions. A prospective study of 204 cases. Int J Dermatol. (2019) 58:811–5. doi: 10.1111/ijd.14381
114. Miraglia, E, Calvieri, S, and Giustini, S. Lichen sclerosus and sjögren's syndrome. Ital J Dermatol Venerol. (2021) 156:63–4. doi: 10.23736/S2784-8671.19.06362-4
115. Stagi, S, Gasperini, S, Manoni, C, Greco, A, Funghini, S, and Donati, A. Autoimmune thyroiditis, pernicious anaemia, vitiligo and scleroatrophic lichen in a boy with short-chain acylCoA dehydrogenase deficiency. Horm Res Paediatr. (2010) 73:409–13. doi: 10.1159/000308176
116. McGrath, EJ, and Davies, MG. Lichen sclerosus arising from a chronic wound and coexistent with multiple sclerosis. J Eur Acad Dermatol Venereol. (2005) 19:139–41. doi: 10.1111/j.1468-3083.2004.01082.x
117. Kreuter, A, Wischnewski, J, Terras, S, Altmeyer, P, Stücker, M, and Gambichler, T. Coexistence of lichen sclerosus and morphea: a retrospective analysis of 472 patients with localized scleroderma from a German tertiary referral center. J Am Acad Dermatol. (2012) 67:1157–62. doi: 10.1016/j.jaad.2012.04.003
118. Becker, K, Meissner, V, Farwick, W, Bauer, R, and Gaiser, MR. Lichen sclerosus and atopy in boys: coincidence or correlation? Br J Dermatol. (2013) 168:362–6. doi: 10.1111/j.1365-2133.2012.11201.x
119. Eberz, B, and Regauer, S. Assoziation von anogenitalem Lichen sclerosus und Psoriasis bei erwachsenen Frauen. Geburtshilfe Frauenheilkd. (2008) 68:32. doi: 10.1055/s-2008-1078319
120. Ranum, A, Freese, R, Ramesh, V, and Pearson, DR. Lichen sclerosus in female patients is associated with an increased risk of metabolic syndrome and cardiovascular comorbidities: a retrospective cohort review. Br J Dermatol. (2022) 187:1030–2. doi: 10.1111/bjd.21811. [Epub ahead of print]
121. Yeon, J, Oakley, A, Olsson, A, Drummond, C, Veysey, E, Marshman, G, et al. Vulval lichen sclerosus: an Australasian management consensus. Australas J Dermatol. (2021) 62:292–9. doi: 10.1111/ajd.13594
122. Günthert, AR, Duclos, K, Jahns, BG, Krause, E, Amann, E, Limacher, A, et al. Clinical scoring system for vulvar lichen sclerosus. J Sex Med. (2012) 9:2342–50. doi: 10.1111/j.1743-6109.2012.02814.x
123. Naswa, S, and Marfatia, YS. Physician-administered clinical score of vulvar lichen sclerosus: a study of 36 cases. Indian J Sex Transm Dis AIDS. (2015) 36:174–7. doi: 10.4103/0253-7184.167169
124. Lewis, FM, Tatnall, FM, Velangi, SS, Bunker, CB, Kumar, A, Brackenbury, F, et al. British Association of Dermatologists guidelines for the management of lichen sclerosus, 2018. Br J Dermatol. (2018) 178:839–53. doi: 10.1111/bjd.16241
125. Borghi, A, Corazza, M, Minghetti, S, Bianchini, E, and Virgili, A. Dermoscopic features of vulvar lichen sclerosus in the setting of a prospective cohort of patients: new observations. Dermatology. (2016) 232:71–7. doi: 10.1159/000439198
126. Ankad, BS, and Beergouder, SL. Dermoscopic patterns in lichen sclerosus: a report of three cases. Indian Dermatol Online J. (2015) 6:237–40. doi: 10.4103/2229-5178.156450
127. Jindal, R, Chauhan, P, and Shirazi, N. Rosette or four dot signs in dermoscopy: a non-specific observation. Dermatol Pract Concept. (2022) 12:e2022069. doi: 10.5826/dpc.1202a69
128. Ramos-Rodríguez, D, Arteaga-Henríquez, M, Lukoviek, V, and Markthaler, M. Ink test: a useful technique to enhance extragenital lichen sclerosus diagnosis. Pediatr Dermatol. (2022) 39:648–9. doi: 10.1111/pde.14960
129. Mani, S, and Oberoi, B. Dermoscopic keys in extragenital bullous hemorrhagic lichen sclerosus. Dermatol Pract Concept. (2022) 12:e2022063. doi: 10.5826/dpc.1202a63
130. Shim, WH, Jwa, SW, Song, M, Kim, HS, Ko, HC, Kim, MB, et al. Diagnostic usefulness of dermatoscopy in differentiating lichen sclerous et atrophicus from morphea. J Am Acad Dermatol. (2012) 66:690–1. doi: 10.1016/j.jaad.2011.06.042
131. Kantere, D, Neittaanmäki, N, Maltese, K, Wennberg Larkö, AM, and Tunbäck, P. Exploring reflectance confocal microscopy as a non-invasive diagnostic tool for genital lichen sclerosus. Exp Ther Med. (2022) 23:410. doi: 10.3892/etm.2022.11337
132. Vittrup, G, Mørup, L, Heilesen, T, Jensen, D, Westmark, S, and Melgaard, D. Quality of life and sexuality in women with lichen sclerosus: a cross-sectional study. Clin Exp Dermatol. (2022) 47:343–50. doi: 10.1111/ced.14893
133. Rosen, R, Brown, C, Heiman, J, Leiblum, S, Meston, C, Shabsigh, R, et al. The female sexual function index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. (2000) 26:191–208. doi: 10.1080/009262300278597
134. Finlay, AY, and Khan, GK. Dermatology life quality index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol. (1994) 19:210–6. doi: 10.1111/j.1365-2230.1994.tb01167.x
135. Topp, CW, Østergaard, SD, Søndergaard, S, and Bech, P. The WHO-5 well-being index: a systematic review of the literature. Psychother Psychosom. (2015) 84:167–76. doi: 10.1159/000376585
136. Vyas, A. Genital lichen sclerosus and its mimics. Obstet Gynecol Clin N Am. (2017) 44:389–406. doi: 10.1016/j.ogc.2017.05.004
137. Kirtschig, G. Lichen sclerosus: symptomatik, diagnostik, therapeutisches procedere. Hautarzt. (2018) 69:127–33. doi: 10.1007/s00105-017-4121-2
138. Nguyen, ATM, and Holland, AJA. Balanitis xerotica obliterans: an update for clinicians. Eur J Pediatr. (2020) 179:9–16. doi: 10.1007/s00431-019-03516-3
139. Arnold, N, Manway, M, Stephenson, S, and Lipkin, H. Extragenital bullous lichen sclerosus on the anterior lower extremities: report of a case and literature review. Dermatol Online J. (2017) 23: 13030/qt8dn3p7kv
140. Errichetti, E, Lallas, A, Apalla, Z, Di Stefani, A, and Stinco, G. Dermoscopy of morphea and cutaneous lichen sclerosus: clinicopathological correlation study and comparative analysis. Dermatology. (2017) 233:462–70. doi: 10.1159/000484947
141. Veronesi, G, Virdi, A, Leuzzi, M, Gurioli, C, Chessa, MA, Guglielmo, A, et al. Vulvar vitiligo and lichen sclerosus in children: a clinical challenge. Pediatr Dermatol. (2021) 38:1012–9. doi: 10.1111/pde.14771
142. Mahajan, SA, and Dave, JS. Dermoscopic evaluation of extragenital lichen sclerosus et atrophicus. Dermatol Pract Concept. (2022) 12:e2022125. doi: 10.5826/dpc.1203a125
143. Ozturk, MK, Zindancı, I, and Zemheri, E. Dermoscopy of stage llA mycosis fungoides. North Clin Istanb. (2019) 7:174–9. doi: 10.14744/nci.2019.02439
144. Errichetti, E, Lallas, A, Apalla, Z, Di Stefani, A, and Stinco, G. Dermoscopy of granuloma annulare: a clinical and histological correlation study. Dermatology. (2017) 233:74–9. doi: 10.1159/000454857
145. Lallas, A, Zaballos, P, Zalaudek, I, Apalla, Z, Gourhant, JY, Longo, C, et al. Dermoscopic patterns of granuloma annulare and necrobiosis lipoidica. Clin Exp Dermatol. (2013) 38:425–7. doi: 10.1111/ced.12126
146. Smith, YR, and Quint, EH. Clobetasol propionate in the treatment of premenarchal vulvar lichen sclerosus. Obstet Gynecol. (2001) 98:588–91. doi: 10.1016/s0029-7844(01)01496-x
147. Bradford, J, and Fischer, G. Long-term management of vulval lichen sclerosus in adult women. Aust N Z J Obstet Gynaecol. (2010) 50:148–52. doi: 10.1111/j.1479-828X.2010.01142.x
148. Virgili, A, Borghi, A, Toni, G, Minghetti, S, and Corazza, M. First randomized trial on clobetasol propionate and mometasone furoate in the treatment of vulvar lichen sclerosus: results of efficacy and tolerability. Br J Dermatol. (2014) 171:388–96. doi: 10.1111/bjd.12910
149. Mashayekhi, S, Flohr, C, and Lewis, FM. The treatment of vulval lichen sclerosus in prepubertal girls: a critically appraised topic. Br J Dermatol. (2017) 176:307–16. doi: 10.1111/bjd.15202
150. Folaranmi, SE, Corbett, HJ, and Losty, PD. Does application of topical steroids for lichen sclerosus (balanitis xerotica obliterans) affect the rate of circumcision? A systematic review. J Pediatr Surg. (2018) 53:2225–7. doi: 10.1016/j.jpedsurg.2017.12.021
151. Kumar, KS, Morrel, B, van Hees, CLM, van der Toorn, F, van Dorp, W, and Mendels, EJ. Comparison of lichen sclerosus in boys and girls: a systematic literature review of epidemiology, symptoms, genetic background, risk factors, treatment, and prognosis. Pediatr Dermatol. (2022) 39:400–8. doi: 10.1111/pde.14967
152. Wilkinson, DJ, Lansdale, N, Everitt, LH, Marven, SS, Walker, J, Shawis, RN, et al. Foreskin preputioplasty and intralesional triamcinolone: a valid alternative to circumcision for balanitis xerotica obliterans. J Pediatr Surg. (2012) 47:756–9. doi: 10.1016/j.jpedsurg.2011.10.059
153. Sotiriou, E, Apalla, Z, Patsatsi, A, and Panagiotidou, D. Topical tacrolimus for recalcitrant vulvar lichen sclerosus. Eur J Dermatol. (2009) 19:515–6. doi: 10.1684/ejd.2009.0733
154. Goldstein, AT, Thaçi, D, and Luger, T. Topical calcineurin inhibitors for the treatment of vulvar dermatoses. Eur J Obstet Gynecol Reprod Biol. (2009) 146:22–9. doi: 10.1016/j.ejogrb.2009.05.026
155. Beattie, PE, Dawe, RS, Ferguson, J, and Ibbotson, SH. UVA1 phototherapy for genital lichen sclerosus. Clin Exp Dermatol. (2006) 31:343–7. doi: 10.1111/j.1365-2230.2006.02082.x
156. Garrido-Colmenero, C, Martínez-Peinado, CM, Galán-Gutiérrez, M, Barranco-Millán, V, and Ruiz-Villaverde, R. Successful response of vulvar lichen sclerosus with NB-UVB. Dermatol Ther. (2021) 34:e14801. doi: 10.1111/dth.14801
157. Reichrath, J, Reinhold, U, and Tilgen, W. Treatment of genito-anal lesions in inflammatory skin diseases with PUVA cream photochemotherapy: an open pilot study in 12 patients. Dermatology. (2002) 205:245–8. doi: 10.1159/000065858
158. Rombold, S, Lobisch, K, Katzer, K, Grazziotin, TC, Ring, J, and Eberlein, B. Efficacy of UVA1 phototherapy in 230 patients with various skin diseases. Photodermatol Photoimmunol Photomed. (2008) 24:19–23. doi: 10.1111/j.1600-0781.2008.00328.x
159. Terras, S, Gambichler, T, Moritz, RK, Stücker, M, and Kreuter, A. UV-A1 phototherapy vs clobetasol propionate, 0.05%, in the treatment of vulvar lichen sclerosus: a randomized clinical trial. JAMA Dermatol. (2014) 150:621–7. doi: 10.1001/jamadermatol.2013.7733
160. Gerkowicz, A, Szczepanik-Kułak, P, and Krasowska, D. Photodynamic therapy in the treatment of vulvar lichen sclerosus: a systematic review of the literature. J Clin Med. (2021) 10:5491. doi: 10.3390/jcm10235491
161. Romero, A, Hernández-Núñez, A, Córdoba-Guijarro, S, Arias-Palomo, D, and Borbujo-Martínez, J. Treatment of recalcitrant erosive vulvar lichen sclerosus with photodynamic therapy. J Am Acad Dermatol. (2007) 57:S46–7. doi: 10.1016/j.jaad.2006.04.005
162. Li, Z, Wang, Y, Wang, J, Li, S, Xiao, Z, Feng, Y, et al. Evaluation of the efficacy of 5-aminolevulinic acid photodynamic therapy for the treatment of vulvar lichen sclerosus. Photodiagn Photodyn Ther. (2020) 29:101596. doi: 10.1016/j.pdpdt.2019.101596
163. Sotiriou, E, Panagiotidou, D, and Ioannidis, D. An open trial of 5-aminolevulinic acid photodynamic therapy for vulvar lichen sclerosus. Eur J Obstet Gynecol Reprod Biol. (2008) 141:187–8. doi: 10.1016/j.ejogrb.2008.07.027
164. Imbernón-Moya, A, Martínez-Pérez, M, Churruca-Grijelmo, M, Lobato-Berezo, A, Vargas-Laguna, E, Fernández-Cogolludo, E, et al. Photodynamic therapy as a therapeutic alternative in vulvar lichen sclerosus: series of 8 cases. Photodermatol Photoimmunol Photomed. (2016) 32:307–10. doi: 10.1111/phpp.12242
165. Sotiriou, E, Apalla, Z, Patsatsi, A, and Panagiotidou, D. Recalcitrant vulvar lichen sclerosis treated with aminolevulinic acid-photodynamic therapy: a report of five cases. J Eur Acad Dermatol Venereol. (2008) 22:1398–9. doi: 10.1111/j.1468-3083.2008.02661.x
166. Zawislak, AA, McCluggage, WG, Donnelly, RF, Maxwell, P, Price, JH, Dobbs, SP, et al. Response of vulval lichen sclerosus and squamous hyperplasia to photodynamic treatment using sustained topical delivery of aminolevulinic acid from a novel bioadhesive patch system. Photodermatol Photoimmunol Photomed. (2009) 25:111–3. doi: 10.1111/j.1600-0781.2009.00410.x
167. Zhang, F, Li, D, Shi, L, Gu, Y, Xu, Y, and Wu, C. Efficacy of 5-Aminolevulinic acid (ALA)-photodynamic therapy (PDT) in refractory vulvar lichen sclerosus: preliminary results. Med Sci Monit. (2021) 27:e927406. doi: 10.12659/MSM.927406
168. Skrzypulec, V, Olejek, A, Drosdzol, A, Nowosielski, K, Kozak-Darmas, I, and Wloch, S. Sexual functions and depressive symptoms after photodynamic therapy for vulvar lichen sclerosus in postmenopausal women from the upper Silesian region of Poland. J Sex Med. (2009) 6:3395–400. doi: 10.1111/j.1743-6109.2009.01505.x
169. Osiecka, BJ, Jurczyszyn, K, Nockowski, P, Murawski, M, and Ziółkowski, P. Photodynamic therapy with green light for the treatment of vulvar lichen sclerosus - preliminary results. Photodiagn Photodyn Ther. (2017) 17:185–7. doi: 10.1016/j.pdpdt.2016.11.015
170. Kreuter, A, Tigges, C, Gaifullina, R, Kirschke, J, Altmeyer, P, and Gambichler, T. Pulsed high-dose corticosteroids combined with low-dose methotrexate treatment in patients with refractory generalized extragenital lichen sclerosus. Arch Dermatol. (2009) 145:1303–8. doi: 10.1001/archdermatol.2009.235
171. Bousema, MT, Romppanen, U, Geiger, JM, Baudin, M, Vähä-Eskeli, K, Vartiainen, J, et al. Acitretin in the treatment of severe lichen sclerosus et atrophicus of the vulva: a double-blind, placebo-controlled study. J Am Acad Dermatol. (1994) 30:225–31. doi: 10.1016/s0190-9622(94)70021-4
172. Mørk, NJ, Jensen, P, and Hoel, PS. Vulval lichen sclerosus et atrophicus treated with etretinate (Tigason). Acta Derm Venereol. (1986) 66:363–5.
173. Bulbul Baskan, E, Turan, H, Tunali, S, Toker, SC, and Saricaoglu, H. Open-label trial of cyclosporine for vulvar lichen sclerosus. J Am Acad Dermatol. (2007) 57:276–8. doi: 10.1016/j.jaad.2007.03.006
174. Cuellar-Barboza, A, Bashyam, AM, Ghamrawi, RI, Aickara, D, Feldman, SR, and Pichardo, RO. Methotrexate for the treatment of recalcitrant genital and extragenital lichen sclerosus: a retrospective series. Dermatol Ther. (2020) 33:e13473. doi: 10.1111/dth.13473
175. Tomson, N, and Sterling, JC. Hydroxycarbamide: a treatment for lichen sclerosus? Br J Dermatol. (2007) 157:622. doi: 10.1111/j.1365-2133.2007.07991.x
176. Wakelin, SH, and James, MP. Extensive lichen sclerosus et atrophicus with bullae and ulceration--improvement with hydroxychloroquine. Clin Exp Dermatol. (1994) 19:332–4. doi: 10.1111/j.1365-2230.1994.tb01208.x
177. Shelley, WB, Shelley, ED, Grunenwald, MA, Anders, TJ, and Ramnath, A. Long-term antibiotic therapy for balanitis xerotica obliterans. J Am Acad Dermatol. (1999) 40:69–72. doi: 10.1016/s0190-9622(99)70529-3
178. Shelley, WB, Shelley, ED, and Amurao, CV. Treatment of lichen sclerosus with antibiotics. Int J Dermatol. (2006) 45:1104–6. doi: 10.1111/j.1365-4632.2006.02978.x
179. Taveira, M, Selores, M, Costa, V, and Massa, A. Generalized morphea and lichen sclerosus et atrophicus successfully treated with sulphasalazine. J Eur Acad Dermatol Venereol. (1999) 12:283–4. doi: 10.1111/j.1468-3083.1999.tb01053.x
180. Ronger, S, Viallard, AM, Meunier-Mure, F, Chouvet, B, Balme, B, and Thomas, L. Oral calcitriol: a new therapeutic agent in cutaneous lichen sclerosis. J Drugs Dermatol. (2003) 2:23–8.
181. Li, J, Zheng, W, Tang, J, and Yang, B. Lichen sclerosus successfully treated with baricitinib plus psoralen and ultraviolet A. Dermatol Ther. (2021) 34:e14896. doi: 10.1111/dth.14896
182. Stewart, L, McCammon, K, Metro, M, and Virasoro, R. SIU/ICUD consultation on urethral strictures: anterior urethra-lichen sclerosus. Urology. (2014) 83:S27–30. doi: 10.1016/j.urology.2013.09.013
183. Depasquale, I, Park, AJ, and Bracka, A. The treatment of balanitis xerotica obliterans. BJU Int. (2000) 86:459–65. doi: 10.1046/j.1464-410x.2000.00772.x
184. Kulkarni, S, Barbagli, G, Kirpekar, D, Mirri, F, and Lazzeri, M. Lichen sclerosus of the male genitalia and urethra: surgical options and results in a multicenter international experience with 215 patients. Eur Urol. (2009) 55:945–56. doi: 10.1016/j.eururo.2008.07.046
185. Kiss, A, Király, L, Kutasy, B, and Merksz, M. High incidence of balanitis xerotica obliterans in boys with phimosis: prospective 10-year study. Pediatr Dermatol. (2005) 22:305–8. doi: 10.1111/j.1525-1470.2005.22404.x
186. Gargollo, PC, Kozakewich, HP, Bauer, SB, Borer, JG, Peters, CA, Retik, AB, et al. Balanitis xerotica obliterans in boys. J Urol. (2005) 174:1409–12. doi: 10.1097/01.ju.0000173126.63094.b3
187. Barbagli, G, Palminteri, E, Balò, S, Vallasciani, S, Mearini, E, Costantini, E, et al. Lichen sclerosus of the male genitalia and urethral stricture diseases. Urol Int. (2004) 73:1–5. doi: 10.1159/000078794
188. Chung, ASJ, and Suarez, OA. Current treatment of lichen sclerosus and stricture. World J Urol. (2020) 38:3061–7. doi: 10.1007/s00345-019-03030-z
189. Singh, N, Mishra, N, and Ghatage, P. Treatment options in vulvar lichen sclerosus: a scoping review. Cureus. (2021) 13:e13527. doi: 10.7759/cureus.13527
190. Chmel, R, Nováčková, M, Fait, T, Zámečník, L, Krejčová, L, and Pastor, Z. Clitoral phimosis: effects on female sexual function and surgical treatment outcomes. J Sex Med. (2019) 16:257–66. doi: 10.1016/j.jsxm.2018.12.012
191. Rouzier, R, Haddad, B, Deyrolle, C, Pelisse, M, Moyal-Barracco, M, and Paniel, BJ. Perineoplasty for the treatment of introital stenosis related to vulvar lichen sclerosus. Am J Obstet Gynecol. (2002) 186:49–52. doi: 10.1067/mob.2002.119186
192. Gurumurthy, M, Morah, N, Gioffre, G, and Cruickshank, ME. The surgical management of complications of vulval lichen sclerosus. Eur J Obstet Gynecol Reprod Biol. (2012) 162:79–82. doi: 10.1016/j.ejogrb.2012.01.016
193. Rojavin, Y, Salgado, CJ, Hsu, PW, Liu, J, and Aikins, JK. The surgical management of vulvar lichen sclerosus refractory to medical management. J Plast Reconstr Aesthet Surg. (2008) 61:848–9. doi: 10.1016/j.bjps.2007.10.076
194. Abramov, Y, Elchalal, U, Abramov, D, Goldfarb, A, and Schenker, JG. Surgical treatment of vulvar lichen sclerosus: a review. Obstet Gynecol Surv. (1996) 51:193–9. doi: 10.1097/00006254-199603000-00023
195. Tasker, F, Kirby, L, Grindlay, DJC, Lewis, F, and Simpson, RC. Laser therapy for genital lichen sclerosus: a systematic review of the current evidence base. Skin Health Dis. (2021) 1:e52. doi: 10.1002/ski2.52
196. Windahl, T. Is carbon dioxide laser treatment of lichen sclerosus effective in the long run? Scand J Urol Nephrol. (2006) 40:208–11. doi: 10.1080/00365590600589666
197. Mitchell, L, Goldstein, AT, Heller, D, Mautz, T, Thorne, C, Joyce Kong, SY, et al. Fractionated carbon dioxide laser for the treatment of vulvar lichen sclerosus: a randomized controlled trial. Obstet Gynecol. (2021) 137:979–87. doi: 10.1097/AOG.0000000000004409
198. Wu, C, Zou, M, Xiong, Y, Wang, L, Chen, H, Fan, Y, et al. Short- and long-term efficacy of focused ultrasound therapy for non-neoplastic epithelial disorders of the vulva. BJOG. (2017) 124:87–92. doi: 10.1111/1471-0528.14747
199. He, S, and Jiang, J. High-intensity focused ultrasound therapy for pediatric and adolescent vulvar lichen sclerosus. Int J Hyperth. (2022) 39:579–83. doi: 10.1080/02656736.2022.2060528
200. Jain, NK, and Gulati, M. Platelet-rich plasma: a healing virtuoso. Blood Res. (2016) 51:3–5. doi: 10.5045/br.2016.51.1.3
201. Eshtiaghi, P, and Sadownik, LA. Fact or fiction? Adipose-derived stem cells and platelet-rich plasma for the treatment of vulvar lichen sclerosus. J Low Genit Tract Dis. (2019) 23:65–70. doi: 10.1097/LGT.0000000000000440
202. Tedesco, M, Pranteda, G, Chichierchia, G, Paolino, G, Latini, A, Orsini, D, et al. The use of PRP (platelet-rich plasma) in patients affected by genital lichen sclerosus: clinical analysis and results. J Eur Acad Dermatol Venereol. (2019) 33:e58–9. doi: 10.1111/jdv.15190
203. Villalpando, BK, Wyles, SP, Schaefer, LA, Bodiford, KJ, and Bruce, AJ. Platelet-rich plasma for the treatment of lichen sclerosus. Plast Aesthet Res. (2021) 8:63. doi: 10.20517/2347-9264.2021.86
204. Flynn, AN, King, M, Rieff, M, Krapf, J, and Goldstein, AT. Patient satisfaction of surgical treatment of clitoral phimosis and labial adhesions caused by lichen sclerosus. Sex Med. (2015) 3:251–5. doi: 10.1002/sm2.90
205. Chamli, A, and Souissi, A. Lichen Sclerosus. Treasure Island (FL): StatPearls Publishing (2022). 9 p.
206. Kravvas, G, Muneer, A, Watchorn, RE, Castiglione, F, Haider, A, Freeman, A, et al. Male genital lichen sclerosus, microincontinence and occlusion: mapping the disease across the prepuce. Clin Exp Dermatol. (2022) 47:1124–30. doi: 10.1111/ced.15127
207. Carli, P, Cattaneo, A, De Magnis, A, Biggeri, A, Taddei, G, and Giannotti, B. Squamous cell carcinoma arising in vulval lichen sclerosus: a longitudinal cohort study. Eur J Cancer Prev. (1995) 4:491–6. doi: 10.1097/00008469-199512000-00008
208. Corazza, M, Borghi, A, Gafà, R, Ghirardi, C, and Ferretti, S. Risk of vulvar carcinoma in women affected with lichen sclerosus: results of a cohort study. J Dtsch Dermatol Ges. (2019) 17:1069–71. doi: 10.1111/ddg.13961
209. Corazza, M, Schettini, N, Zedde, P, and Borghi, A. Vulvar lichen sclerosus from pathophysiology to therapeutic approaches: evidence and prospects. Biomedicine. (2021) 9:950. doi: 10.3390/biomedicines9080950
211. Micheletti, L, Preti, M, Radici, G, Boveri, S, Di Pumpo, O, Privitera, SS, et al. Vulvar lichen sclerosus and neoplastic transformation: a retrospective study of 976 cases. J Low Genit Tract Dis. (2016) 20:180–3. doi: 10.1097/LGT.0000000000000186
212. Barbagli, G, Palminteri, E, Mirri, F, Guazzoni, G, Turini, D, and Lazzeri, M. Penile carcinoma in patients with genital lichen sclerosus: a multicenter survey. J Urol. (2006) 175:1359–63. doi: 10.1016/S0022-5347(05)00735-4
213. Kravvas, G, Shim, TN, Doiron, PR, Freeman, A, Jameson, C, Minhas, S, et al. The diagnosis and management of male genital lichen sclerosus: a retrospective review of 301 patients. J Eur Acad Dermatol Venereol. (2018) 32:91–5. doi: 10.1111/jdv.14488
214. Kravvas, G, Ge, L, Ng, J, Shim, TN, Doiron, PR, Watchorn, R, et al. The management of penile intraepithelial neoplasia (PeIN): clinical and histological features and treatment of 345 patients and a review of the literature. J Dermatolog Treat. (2022) 33:1047–62. doi: 10.1080/09546634.2020.1800574
215. Tapp, RA, Feng, J, Jones, JW, Carlson, JA, and Wilson, VL. Single base instability is promoted in vulvar lichen sclerosus. J Invest Dermatol. (2007) 127:2563–76. doi: 10.1038/sj.jid.5700889
216. Paolino, G, Panetta, C, Cota, C, Muscardin, L, Donati, P, and Di Carlo, A. Lichen sclerosus and the risk of malignant progression: a case series of 159 patients. G Ital Dermatol Venereol. (2013) 148:673–8.
217. Mannweiler, S, Sygulla, S, Winter, E, and Regauer, S. Two major pathways of penile carcinogenesis: HPV-induced penile cancers overexpress p16ink4a, HPV-negative cancers associated with dermatoses express p53, but lack p16ink4a overexpression. J Am Acad Dermatol. (2013) 69:73–81. doi: 10.1016/j.jaad.2012.12.973
218. Lee, A, Bradford, J, and Fischer, G. Long-term Management of Adult Vulvar lichen sclerosus: a prospective cohort study of 507 women. JAMA Dermatol. (2015) 151:1061–7. doi: 10.1001/jamadermatol.2015.0643
219. Renaud-Vilmer, C, Cavelier-Balloy, B, Porcher, R, and Dubertret, L. Vulvar lichen sclerosus: effect of long-term topical application of a potent steroid on the course of the disease. Arch Dermatol. (2004) 140:709–12. doi: 10.1001/archderm.140.6.709
220. Ganesan, AK, Taylor, TH, and Kraus, CN. Association of vulvar lichen sclerosus with endometrial and ovarian cancer. JAAD Int. (2022) 9:26–7. doi: 10.1016/j.jdin.2022.07.003
221. Moreno-Vílchez, C, Llobera-Ris, C, Torrecilla-Vall-Llossera, C, Notario, J, and Figueras-Nart, I. Lichen sclerosus and its association with cancer: a retrospective cohort study. Int J Dermatol. (2022) 62:e84–5. doi: 10.1111/ijd.16218. [Epub ahead of print]
222. Sivalingam, V, and Tamber, K. Understanding the impact of life with vulval lichen sclerosus. Br J Dermatol. (2022) 187:840. doi: 10.1111/bjd.21846. [Epub ahead of print]
223. Ranum, A, and Pearson, DR. The impact of genital lichen sclerosus and lichen planus on quality of life: a review. Int J Womens Dermatol. (2022) 8:e042. doi: 10.1097/JW9.0000000000000042
224. Hagedorn, M, Buxmeyer, B, Schmitt, Y, and Bauknecht, T. Survey of genital lichen sclerosus in women and men. Arch Gynecol Obstet. (2002) 266:86–91. doi: 10.1007/s004040100209
225. Burrows, LJ, Creasey, A, and Goldstein, AT. The treatment of vulvar lichen sclerosus and female sexual dysfunction. J Sex Med. (2011) 8:219–22. doi: 10.1111/j.1743-6109.2010.02077.x
226. van Cranenburgh, OD, Nijland, SBW, Lindeboom, R, de Korte, J, de Rie, MA, Ter Stege, JA, et al. Patients with lichen sclerosus experience moderate satisfaction with treatment and impairment of quality of life: results of a cross-sectional study. Br J Dermatol. (2017) 176:1508–15. doi: 10.1111/bjd.15125
227. Mangera, A, Osman, N, and Chapple, C. Recent advances in understanding urethral lichen sclerosus. F1000Res. (2016) 5:96. doi: 10.12688/f1000research.7120.1
Keywords: lichen sclerosus, kraurosis vulvae, white spot disease, balanitis xerotica obliterans, autoimmunity
Citation: De Luca DA, Papara C, Vorobyev A, Staiger H, Bieber K, Thaçi D and Ludwig RJ (2023) Lichen sclerosus: The 2023 update. Front. Med. 10:1106318. doi: 10.3389/fmed.2023.1106318
Edited by:
Aikaterini Patsatsi, Aristotle University of Thessaloniki, GreeceReviewed by:
Gianpaolo Tessari, Integrated University Hospital Verona, ItalyAnca Chiriac, Apollonia University, Romania
Copyright © 2023 De Luca, Papara, Vorobyev, Staiger, Bieber, Thaçi and Ludwig. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David A. De Luca, ✉ ZGF2aWRkZWx1Y2FAZ21haWwuY29t