 Kladoum Nassarmadji
Kladoum Nassarmadji Anthony Vanjak
Anthony Vanjak Venceslas BourdinKarine ChampionRuxandra BurlacuStéphane MoulyDamien Sène
Venceslas BourdinKarine ChampionRuxandra BurlacuStéphane MoulyDamien Sène Cloé Comarmond*
Cloé Comarmond*- Department of Internal Medicine and Clinical Immunology, Lariboisière Hospital, Université Paris Cité, Paris, France
Diagnosis, prognostic assessment, and monitoring disease activity in patients with large vessel vasculitis (LVV) can be challenging. Early recognition of LVV and treatment adaptation is essential because vascular complications (aneurysm, dilatations, ischemic complications) or treatment related side effects can occur frequently in these patients. 18-fluorodeoxyglucose positron emission tomography/computed tomography (2-[18F]FDG-PET/CT) is increasingly used to diagnose, follow, and evaluate treatment response in LVV. In this review, we aimed to summarize the current evidence on the value of 2-[18F]FDG-PET/CT for diagnosis, follow, and treatment monitoring in LVV.
Introduction
Giant cell arteritis (GCA) and Takayasu arteritis (TA) are two vasculitis predominantly affecting large vessels: aorta and its major branches (1). They differ by their clinical presentation, prognosis, and treatment. Imaging modalities such as ultrasound (US), computed tomography (CT) and 18-Fluorodeoxyglucose positron emission tomography (2-[18F]FDG-PET/CT) are more frequently used, have replaced angiography and have modified management of these diseases (2).
18-Fluorodeoxyglucose positron emission tomography/computed tomography is a functional imaging modality of fundamental utility in oncology that has progressively been used in rheumatic diseases. Indeed, 2-[18F]FDG-PET/CT has shown in preclinical models the ability to detect glucose intake in inflammatory and endothelial cells (3, 4). In this review, we aim to illustrate the usefulness of 2-[18F]FDG-PET/CT in management of LVV.
2-[18F]FDG-PET/CT and giant cell arteritis
2-[18F]FDG-PET/CT in GCA diagnosis
Giant cell arteritis is the most frequent large vessel vasculitis affecting patients older than 50 years with a prevalence of 9/100,000 in a prospective study of a German population and up to 25/100,000 in patients older than 50 years (5). Diagnosis of GCA is based on the presence of clinical signs of vasculitis, proof of vessel inflammation, eliminating alternate diagnosis and dramatic response to steroids in patients older than 50 years.
Giant cell arteritis encompass cranial and extracranial manifestations. Constitutional symptoms and elevated inflammatory markers are present in >90% of cases and patients may present with fever of unknown origin as the initial symptom in 15% of cases (6, 7). Cranial manifestations such as headaches may present in two third of patients (8). The most severe acute complication, visual loss, is described in around 20% of cases but this has been reduced with early recognition of disease and usage of temporal artery ultrasound (9, 10). Pseudomyalgia rheumatica (PMR) is the most common extra cranial manifestation in GCA and occur in 45–50% of GCA patients (11). Clinical manifestations of large vessel involvement (limb claudication, thoracic pain) may develop in one fifth of GCA patients (12).
Temporal artery biopsy (TAB) was initially recommended in every case of suspected GCA and was considered the gold standard (13). However, results are delayed and biopsy may be negative in up to 42% of patients with predominantly large vessel GCA (LV GCA) (12). Temporal artery ultrasound has shown very good performance with a pooled sensitivity of 77% and a pooled specificity of 96% as compared with the clinical diagnosis of GCA (2). It is also cost effective compared to TAB but remains limited for the exploration of aorta and visceral arteries (14). Thus, it is the first line recommended imaging technique for suspected predominantly cranial GCA (2). Nevertheless, TAB remains strongly recommended over imaging in ACR 2021 guidelines (15). Recently, the 2022 American College of Rheumatology/EULAR GCA classification criteria emphasized the use of 2-[18F]FDG-PET/CT, as well as other investigative methods: Ultrasound, MRI, for use in clinical practice (16). PET, MRI, and CT are equally proposed to detect large vessel inflammation in GCA in recommendations from different scientific societies: ACR, EULAR, the British Society for Rheumatology and the French study Group for Large Vessel Vasculitis (2, 15, 17, 18).
18-Fluorodeoxyglucose positron emission tomography/computed tomography has overall good performance for the diagnosis of GCA. Specific patterns of PET/CT uptake show that patients with GCA and positive 2-[18F]FDG-PET/CT are more likely to have a diffuse disease with thoracic and abdominal aorta, bilateral subclavian and axillary arteries involvement (19). Ascending aorta is the most affected zone (72%) followed by the brachiocephalic trunk (62%), aortic arch (60%), and descending aorta (60%) (20).
Blockmans et al. (21) have compared PET versus TAB performance and found a sensitivity of 77% and a specificity of 66%. Subsequently, three meta-analysis including studies of GCA patients comparing PET alone or with CT vs. different gold standard (clinical diagnosis or TAB) found sensitivity of 80–89% and specificity of 89–98% (22–24). The main limitations of these meta-analysis are the inclusion of predominantly retrospective studies and the usage of different reference standard between included studies. More recently, a longitudinal prospective study comparing 2-[18F]FDG-PET/CT with clinical diagnosis at 6 months found a sensitivity of 67%, a specificity of 100%, a negative predictive value of 64% and a positive predictive value of 100% (25).
18-Fluorodeoxyglucose positron emission tomography/computed tomography is also a useful imaging technique to assess large vessel involvement in patients with suspected GCA and negative TAB. In a retrospective study of 63 patients with suspected GCA and negative TAB, large vessel involvement with 2-[18F]FDG-PET/CT was observed in 14 patients (22%). The final diagnosis of GCA was based on the presence of clinical symptoms, laboratory results, imaging data compatible with GCA, and good response to corticosteroid therapy (26).
Moreover, new generations of 2-[18F]FDG-PET/CT provide improved image resolution and can detect arteritis in smaller cranial arteries (temporal, maxillary, vertebral and occipital arteries) (Figure 1). Diagnosis of cranial artery inflammation with head, neck and chest PET/CT before or within 72 h after glucocorticoids intake showed a sensitivity of 82–92% and a specificity of 85–100% for diagnosis of GCA (27–29).
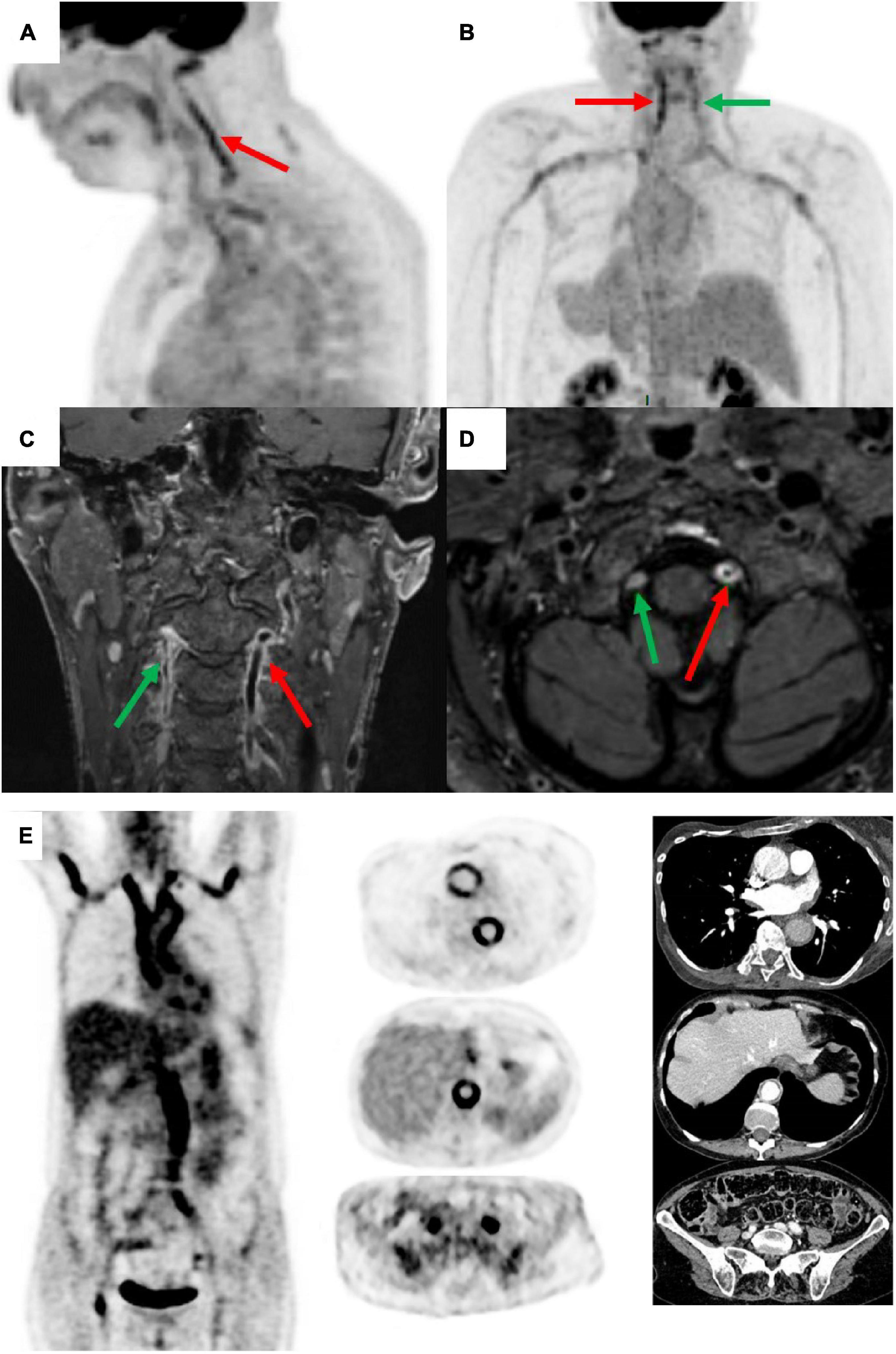
Figure 1. Positron emission tomography (PET) and magnetic resonance angiography (MRA) in a patient with giant cell arteritis (GCA) (man of 73 years old, CRP 17 mg/L, TAB positive). PET shows an inflammatory pattern with clear uptake (>liver uptake, grade 3) in vertebral arteries (left = red arrow and right = green arrow), sub-clavicular arteries, aortic arch, and thoracic aorta [panels (A,B) posterior image]. MRA shows vertebral arterial wall thickening, occlusion, and parietal enhancement [panels (C,D)]. PET and compute tomography angiography (CTA) illustrating aortitis at diagnosis in GCA patient, woman of 64 years old, CRP 84 mg/L, TAB negative [panel (E)].
Finally, 2-[18F]FDG-PET/CT can be helpful in patients presenting with extracranial manifestation of GCA. In patients presenting with fever of unknown origin (FUO), abnormal 2-[18F]FDG-PET/CT increase the diagnosis rate to 83% among whom one-third have inflammatory diseases, such as vasculitis (30). In patients with suspicion of PMR, prospective studies using 2-[18F]FDG-PET/CT revealed the presence of LVV involvement in 31–60% of patients (31, 32).
The main differential diagnosis of FDG vessel uptake in vasculitis is atherosclerosis. Based on qualitative and quantitative vascular 18 FDG uptake, vascular site involved and disappearance upon steroid treatment, some differences can be noted (33): In atherosclerotic disease, uptake is usually low to moderate (Grade 0–1), has a patchy pattern and is predominantly located on iliofemoral sites and aortic bifurcations. In vasculitis however, FDG uptake is usually intense: a grade 3 uptake is found in aortitis only and semi quantitative analysis of FDG uptake are significantly higher in aortitis compared to atherosclerotic disease (mean SUVm 4.6 vs. 2.7) (34). Furthermore, FDG uptake in aortitis has a concentric, smooth linear pattern and may affect whole aorta. Also, CT images show non-concentric calcifications in atherosclerotic disease versus circumferential aortic wall thickness of more than 2–3 mm in vasculitis (35; Table 1).
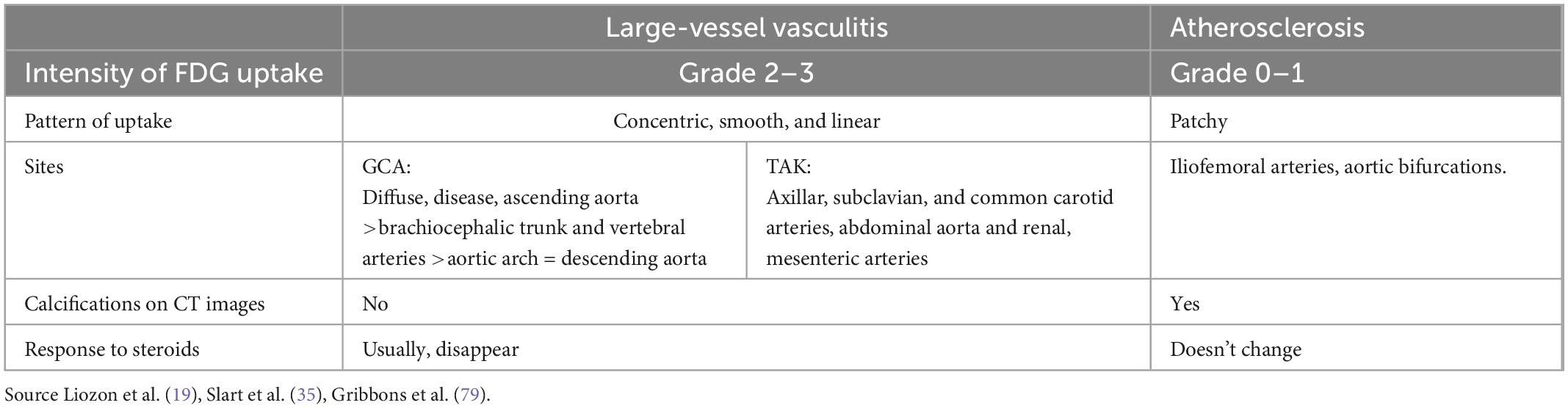
Table 1. Differences in the pattern of fluorodeoxyglucose (FDG) uptake between vasculitis and atherosclerosis.
2-[18F]FDG-PET/CT in GCA prognosis
The prognosis in GCA is dominated by irreversible vision during short term course and vascular complications (dilatation, dissection, aneurysm, atherosclerosis) during long term follow-up (36).
Positron emission tomography/computed tomography is not adequate to evaluate the risk of vision loss because if ocular involvement is suspected, glucocorticoids must be started immediately and no imaging should delay the treatment (2). Moreover, ciliary arteries and central retinal arteries which are involved in ocular retinal damages are too small to be evaluated by PET/CT. Patients with GCA have a 2-fold increased risk of aortic aneurysm than control in a large UK cohort (37). Approximatively 20% of patients with GCA may develop aortic structural damage (aneurysm, dissection) (38, 39), mainly after 5 years from diagnosis (40).
Some risk factors for aortic damage in GCA have been identified and include male sex, smoking, hypertension and diabetes (37).
In two prospective studies by Blockmans et al. (31) and Galli et al. (41) assessing FDG uptake at diagnosis and during follow up, respectively up to 6 months and with a mean 97 months, vascular uptake at diagnosis did not predict subsequent relapse. However, an increased FDG uptake in the aorta at the diagnosis of GCA was associated with development of thoracic aorta dilatation (42) and in a prospective study including both GCA and TAK, future clinical relapses were more frequent in patients with a high PETVAS (≥20) than in patients with a low PETVAS (55 vs. 11%; P = 0.03) over a median follow-up of 15 months (43). More recently, the presence of FDG-PET activity at baseline in arterial territories of patients with LVV (TA or GCA) preceded angiographic progression and change (44). An arterial territory with baseline PET activity had 20 times increased odds for angiographic change compared to a paired arterial territory without PET activity. Concomitant edema and wall thickness further increased risk for angiographic change (44).
2-[18F]FDG-PET/CT in monitoring GCA activity
Therapeutic options for GCA comprise glucocorticoids (GC), tocilizumab (TCZ) and methotrexate (MTX). The optimal length of therapy is not well-known but treatment is usually maintained at least 2 years (15, 45). Indeed, relapses have been reported in around 30% of cases in prospective studies, mainly during the first 2 years following diagnosis (46, 47).
18-Fluorodeoxyglucose positron emission tomography/computed tomography in GCA can detect active aortitis and localize inflammation for extra-cranial arterial territories and peripheral arthritis (bilateral shoulder/hip pain and morning stiffness compatible with polymyalgia rheumatica–PMR) (2, 7). An activity score has been proposed to compare uptake evolution and is based on the sum of visual scores in different arterial regions: the Total Vascular Score (TVS). This visual score uses a standardized 0–3 grading system: 0 = no uptake (≤mediastinum); 1 = low-grade uptake (<liver); 2 = intermediate-grade uptake (=liver), 3 = high-grade uptake (>liver). Grade 2 is considered possibly indicative and grade 3 is considered positive for active LVV. The total score can be determined at seven different vascular regions (thoracic aorta, abdominal aorta, subclavian arteries, axillary arteries, carotid arteries, iliac arteries, and femoral arteries) and ranges from 0 to 21 (35). An increased number of vascular region can be chosen in a similar score: PET vascular activity score (PETVAS) by including four segments of the aorta (ascending, arch, descending thoracic, and abdominal) and five branch arteries (carotids, brachiocephalic trunk, subclavian/axillary arteries) with a maximum score of 27 (43).
In a prospective study of 29 patients with biopsy proven GCA and initially positive 2-[18F]FDG-PET/CT, TVS decreased from baseline to 3 months after treatment but remained unchanged at 6 months (31). Furthermore, there was no significant correlation between PET activity and clinical score (BVAS) or biological markers of activity (CRP, ESR) in patients with vascular complications or persistent inflammatory markers despite treatment (48). The persistence of FDG uptake despite clinical and biological remission is poorly understood (vascular remodeling vs. persistent mural inflammation) and its role in further vessel damage is unknown and is among the future research agenda (2).
The role of 2-[18F]FDG-PET/CT for treatment monitoring in LVV has been recently reviewed by van der Geest et al. (49). Longitudinal studies showed a decrease of baseline arterial FDG uptake after treatment induced remission. Investigation of early changes upon glucocorticoid treatment showed the persistence of FDG uptake after 3 days but its disappearance in 64% of cases after 10 days (50). The meta-analysis of four cross-sectional showed a moderate diagnostic accuracy for detecting active disease with a pooled sensitivity of 77% (95% CI 57–90%) and specificity of 71% [95% CI (47–87%)] (49). In a subsequent study comparing treatment effect on vascular inflammation, MTX and TCZ were associated with a higher decreased PETVAS than corticosteroids alone (51). The PET vascular activity score is useful to differentiate active and inactive disease and to predict relapse. However, PET/CT seems less accurate to evaluate clinically active disease in GCA compared to TAK probably explained by a younger age and less atherosclerosis in TAK, and a spectrum of cranial and articular clinical manifestations less frequently the expression of the LVV inflammation in GCA population.
There are no studies available using 2-[18F]FDG-PET/CT alone to guide treatment adaptation. 2-[18F]FDG-PET/CT provides information about vascular inflammation that is complementary from clinical assessment in LVV. A prospective imaging study in patients with GCA treated with tocilizumab shows that 2-[18F]FDG-PET/CT activity is significantly reduced in response to treatment with tocilizumab and repeat 2-[18F]FDG-PET/CT after tocilizumab discontinuation reveal worsening vascular PET activity in most patients (52). Therefore, treatment adaptation is guided by multimodal assessment with clinical, biological and imaging parameters. The 2-[18F]FDG-PET/CT place remains to be specified but 2-[18F]FDG-PET/CT persistent uptake despite clinical remission could be associated with future clinical relapse.
2-[18F]FDG-PET/CT versus other imaging
Comparison of extended vascular US and 2-[18F]FDG-PET/CT showed comparable diagnostic accuracy in a cohort of suspected GCA (53). However, US was more sensible for temporal arteries vasculitis and popliteal vasculitis and 2-[18F]FDG-PET/CT was more performant for thoracic and abdominal aorta vasculitis. Thus, these two imaging modalities may be complementary. The advantages of US over 2-[18F]FDG-PET/CT are its availability, the absence of irradiation and a lower-cost imaging. However, it is operator dependent and does not detect alternate diagnosis such as neoplasia.
Multiple studies have shown comparable diagnostic accuracy between CT angiography (CTA) and PET/CT (25, 54–56). A higher correlation of PET with inflammatory markers was found (25, 55). The main advantages of CT over PET alone were the better evaluation of parietal damage and its availability. However, combination of PET with CT allows better evaluation of parietal damage even if reconstructed slice thickness remains superior to CT alone (∼3.5 mm vs. ∼2 mm) (Figure 1E).
In a prospective study comparing early diagnosis performance of MRI and 2-[18F]FDG-PET/CT, their diagnosis accuracy were comparable, however, 2-[18F]FDG-PET/CT detected more vascular regions involved than MRI (57). It should be noted that both are poorly correlate with clinical disease activity in patients with preexisting immunosuppressive therapy (48, 58). We summarize diagnostic performances of different imaging modalities for baseline evaluation in Table 2.
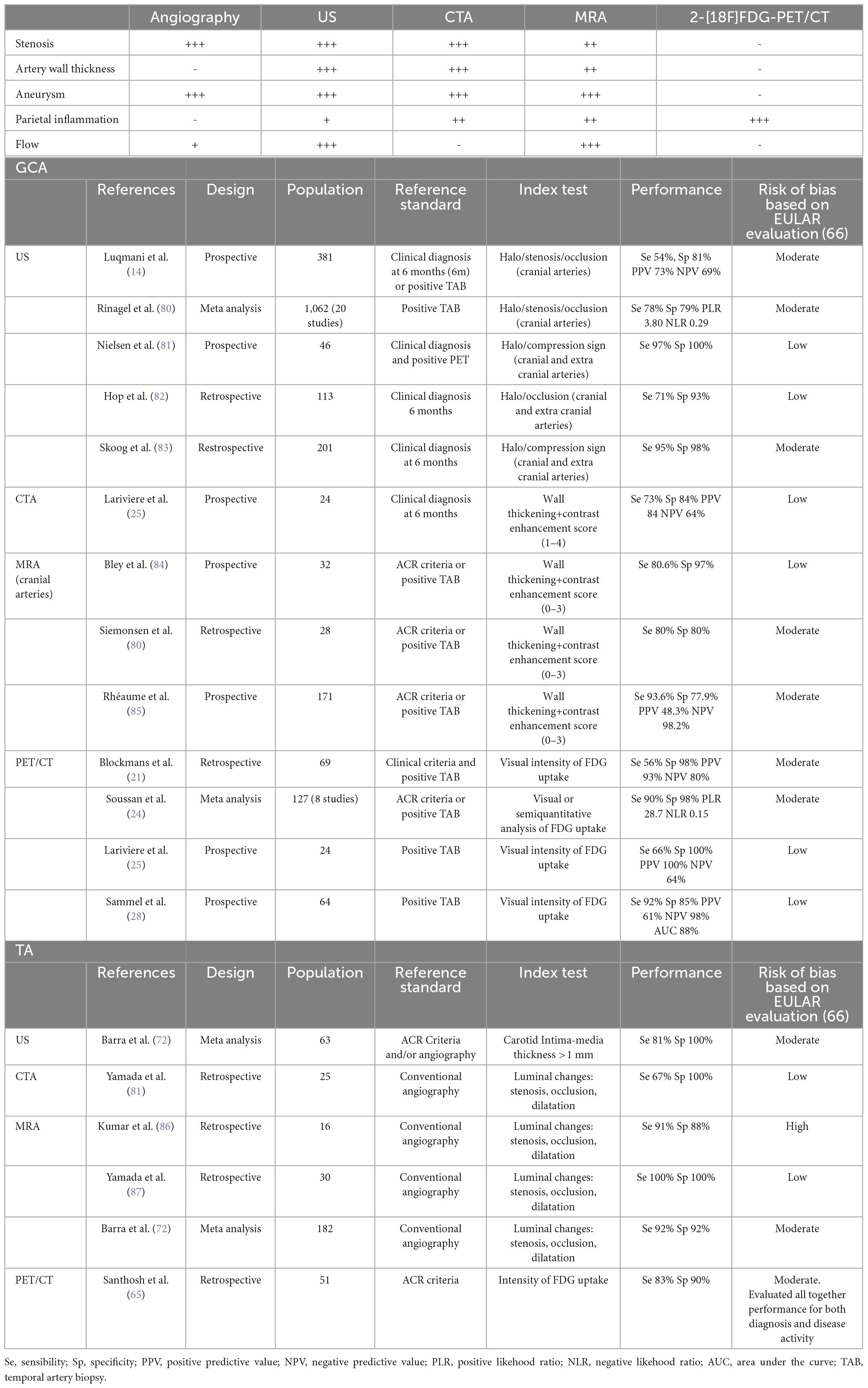
Table 2. Study characteristics and main findings on the diagnostic accuracy by angiography, ultrasound, CTA, magnetic resonance angiography (MRA) and 18-fluorodeoxyglucose positron emission tomography/computed tomography (2-[18F]FDG-PET/CT) at baseline in giant cell arteritis (GCA) and Takayasu arteritis.
Conclusion 2-[18F]FDG-PET/CT and GCA
To sum up, 2-[18F]FDG-PET/CT is a useful diagnosis to assess diagnosis and prognosis of GCA.
It can be used in two situations: first, GCA is confirmed or highly probable, for example a high pretest probability and positive US or TAB. In this clinical situation the role of 2-[18F]FDG-PET/CT is to early detect large vessel involvement and to predict vessel damage, particularly thoracic aortitis which is associated with an increased risk of developing thoracic aorta dilatation (42, 44).
Secondly, GCA is suspected but uncertain. For example in patients presenting with constitutional symptoms, FUO, suspected LV involvement or signs of PMR with an intermediate or low pretest probability. In this clinical situation, 2-[18F]FDG-PET/CT is useful to detect signs of vasculitis and search for an alternate diagnosis: signs of PMR, neoplasia, other inflammatory diseases (sarcoidosis) or infection.
Its role in the follow-up of patients with GCA is not well-established. We propose to use 2-[18F]FDG-PET/CT during follow-up of GCA patients depending on clinical and biological parameters evolution to aid in therapeutic decisions: If patient present with clinical symptoms (extracephalic) but without inflammatory markers, a negative TEP may help in deciding to stop or not restart treatment. Also, in a patient with increased biological markers without clinical signs, a positive TEP may detect preclinical lesions and help in deciding to restart or increase anti-inflammatory treatment.
2-[18F]FDG-PET/CT and takayasu arteritis
Takayasu arteritis (TA) is the second primitive vasculitis affecting predominantly large vessels (1). It is ubiquitous but the highest incidence is found in Asia (59). Contrary to GCA it affects mainly patients under 40 years, has a higher F/M sex ratio and differs by clinical presentation and disease course (60).
2-[18F]FDG-PET/CT and TA diagnosis
There is no gold standard for diagnosis of TA and artery biopsy is not routinely available. Diagnosis is mainly based on the presence of characteristic imaging of large arteries in young patients under 50 years with clinical signs and/or elevated inflammatory markers (61).
Patients with TA may present with vascular symptoms attributable to arteritis but also systemic symptoms or “non-vascular” symptoms. Systemic symptoms may precede the vascular phase and are non-specific. They encompass fever, skin manifestations, arthralgia, episcleritis. Also, TA may be associated with other inflammatory diseases, such as sarcoidosis, spondylarthritis, or Crohn disease (62).
TA predominantly affect subclavian and common carotid arteries but aorta and all its branches may be involved (60). The disease is often diagnosed during the vascular phase which results from vascular complications: stenosis in >90% of cases, aneurysm in 20% of cases (63).
Appropriate imaging is the mainstay for the diagnosis of TA (Table 2). Based on its performance to investigate mural inflammation and/or luminal changes and the young age of the patients, European guidelines recommend angio-MRI as the first line imaging option replacing angiography (2). Moreover, to assess peripheral artery disease, French guidelines propose vascular doppler ultrasound to evaluate vessel wall morphology and blood flow (61).
We did not find study evaluating the accuracy of 2-[18F]FDG-PET/CT as a diagnostic tool only in TA. However, based on current clinical practice, recent 2022 ACR/EULAR classification criteria for Takayasu arteritis fully integrate evidence of vasculitis in the aorta or branch arteries confirmed by vascular imaging: CT/catheter-based/magnetic resonance angiography (MRA), ultrasound and PET (58, 64). One study by Santhosh et al. (65) studied 2-[18F]FDG-PET/CT as diagnostic tool but also included activity evaluation. Other studies or meta-analysis focused on 2-[18F]FDG-PET/CT as a measurement of the disease activity or included both GCA and TA. Similarly, there was no study on 2-[18F]FDG-PET/CT as diagnostic tool in TA included in the meta-analysis informing the EULAR guidelines on imaging (66).
2-[18F]FDG-PET/CT and TA prognosis
In a multicentric retrospective study of TA patients, relapse were observed in 43% of patients and vascular complications occurred in 38% of patients after a median follow up of 6.1 years (67). Main vascular complications in TA are: neurovascular disease (stroke, transitory ischemic attack), ischemic retinopathy, cardiovascular complications ranging from aortic regurgitation to pulmonary hypertension including coronaropathy and microvascular ischemia, renovascular disease, and peripheral artery disease. Risk factors for relapse were male sex, high CRP and carotidynia at diagnosis. Progressive disease, thoracic aorta involvement and retinopathy were associated with vascular complications (67).
One retrospective study evaluated the predictive value of 2-[18F]FDG-PET/CT in 32 patients with baseline 2-[18F]FDG-PET/CT and a median follow up of 83.5 months. Maximal standardized uptake value (SUVmax) in arteries ≥1.3 seemed to be associated with disease relapse [Odds ratio (OR): 5.667; 95% confidence interval (95 CI): (1.067–30.085)] and the need to change therapy [OR: 7.933; 95 CI: (1.478–42.581)]. Interpretation of these results must be cautious because of potential bias due to study design and very large 95% confidence interval of ORs. Also, there was no association between SUVmax intensity at baseline and the development of ischemic events, new angiographic lesions or sustained remission (68). In a recent prospective cohort to assess whether vascular 2-[18F]FDG-PET/CT activity is associated with angiographic change in LVV including 38 TA patients, lack of 2-[18F]FDG-PET/CT activity was strongly associated with stable angiographic disease, P < 0.01 (44). An arterial territory with baseline 2-[18F]FDG-PET/CT activity had 20 times increased odds for angiographic change compared to a paired arterial territory without PET activity. Angiographic progression with arterial damage was preceded by the presence of 2-[18F]FDG-PET/CT activity (44).
2-[18F]FDG-PET/CT and monitoring TA activity
Treatment of TA is based on glucocorticoids often associated with methotrexate or anti-TNFα in severe disease or in case of steroids dependence (15, 45, 61). There are no consensual criteria for assessing TA activity. Inflammatory markers are poorly correlated with angiographic progression and may remain negative in 30% of patients with clinically active disease (69). Two tools are commonly used : First the NIH criteria and more recently, the ITAS2010 criteria which is increasingly being used (70, 71).
A meta-analysis including 131 patients with TA evaluated 2-[18F]FDG-PET/CT performance for assessing activity of disease based on NIH and showed a sensitivity and specificity of 84% (24). All four included studies had a retrospective design. These results were confirmed in a second meta-analysis including 57 studies, mainly cross-sectional and of low methodological quality. The pooled sensitivity was 81% and specificity 74% (72). A recent longitudinal study included 126 patients with LVV (GCA = 50; TAK = 76) with 2-[18F]FDG-PET/CT at enrollment and follow up. Global arterial FDG uptake was quantified with PETVAS. After a median follow up of 2.6 years, there was no significant decrease in PETVAS in TA patients. Also, there was no direct correlation between PETVAS during follow up and clinical and biological activity (73).
One case report suggested that 2-[18F]FDG-PET/CT may not detect pulmonary artery (PA) involvement in TA) (74). This was infirmed in a study Gao et al. (75) which compared performance of 2-[18F]FDG-PET/CT versus CTPA or AMR in TA patients with PA involvement. 2-[18F]FDG-PET/CT was as sensible as radiological imaging (71.4 vs. 92.9%, P = 0.250) and seemed to have higher specificity (91.7 vs. 37.5%, P = 0.001).
Finally, a multimodal assessment of TA activity was proposed by amalgamating the sum of mean SUV, ESR and soluble interleukin-2 receptor (IL-2Rs) which seemed concordant with NIH and ITAS2010 criteria (76). However, the population included had different disease course and treatment. This model needs further validation using prospective studies and homogenous population.
Conclusion PET/CT and TA
The place of 2-[18F]FDG-PET/CT in TA management remains poorly defined. Diagnosis and disease activity assessment in TA can be challenging as patients may not have overt clinical symptoms or elevated CRP at diagnosis or during periods of active disease. Combination of non-invasive vascular imaging such as doppler ultrasound, MRA, CTA, and 2-[18F]FDG-PET/CT remains the first line modality for diagnosis of TA and is essential to monitor vascular disease in patients with TA. During follow up, new areas of arterial damage can develop despite apparent clinical and biological remission in TA. 2-[18F]FDG-PET/CT cannot be systematically recommended for follow up but incorporate the use of 2-[18F]FDG-PET/CT with non-invasive vascular imaging may complete multimodal imaging assessment of disease activity and risk of vascular damage.
Prospects
Novel PET imaging techniques are progressively used or under research.
Positron emission tomography/MRI has been evaluated in large vessel vasculitis and allow analysis of different pattern: fibrous vs. inflammatory pattern (77). Its place in LVV, TA particularly, remains to be specified.
Van der Geest et al. (49) recently reviewed novel PET imaging techniques using novel cell targets and novel tracers. These techniques could improve imaging accuracy by using a more specific cell uptake of FDG with less background activity. Also, it could enhance activity evaluation after treatment (78). Some of these novel targets are: T cells targeted radio tracers (IL2-R, CD4, CD8), macrophages [Translocator protein (TSPO), mannose receptor (CD206), folate receptor and others], B cells, activated fibroblasts (Fibroblast activation protein alpha pathway), endothelial cells (VCAM-1).
Some drawbacks have been underlined by Van der Geest et al. (49): the risk of high irradiation dose, the complexity and cost of radiotracers development and the need of clinical study to confirm their utility.
Conclusion
This review illustrates that 2-[18F]FDG-PET/CT is a powerful metabolic imaging tool that may help improving early diagnosis, current classification, and prognostic assessment in LVV. In patients with a clinical suspicion for LVV, 2-[18F]FDG-PET/CT can help to diagnose LVV especially at the early onset of disease or in case of non-specific signs. Early recognition of LVV is essential because irreversible ischemic complication (e.g., stroke, vision loss, myocardial infarction) almost always occur early, prior to steroids therapy. Moreover, the presence of vascular 2-[18F]FDG-PET/CT activity can precede angiographic change and progression in LVV. Conversely, the disappearance of 2-[18F]FDG-PET/CT uptake after effective therapy is possible. Thus, 2-[18F]FDG-PET/CT may be useful to evaluate treatment efficiency as well as for detection of LVV relapse and vascular complication at an early stage. Persistent activity however, is difficult to interpret, and its impact on disease treatment modifications is not well-known yet and needs further research. 2-[18F]FDG-PET/CT may help clinician to determine patients with more active, diffuse, and severe LVV requiring a more intensive treatment and close monitoring.
Author contributions
KN and CC collected the data and wrote the manuscript. AV, VB, KC, RB, SM, and DS made imaging analysis. KN and CC were responsible for verification of all the underlying data and took full responsibility for the integrity of the work. All authors critically reviewed and approved the final version of the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Jennette J, Falk R, Bacon P, Basu N, Cid M, Ferrario F, et al. 2012 Revised international chapel hill consensus conference nomenclature of vasculitides. Arthritis Rheum. (2013) 65:1–11. doi: 10.1002/art.37715
2. Dejaco C, Ramiro S, Duftner C, Besson F, Bley T, Blockmans D, et al. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice. Ann Rheum Dis. (2018) 77:636–43. doi: 10.1136/annrheumdis-2017-212649
3. Kubota R, Yamada S, Kubota K, Ishiwata K, Tamahashi N, Ido T. Intratumoral distribution of fluorine-18-fluorodeoxyglucose in vivo: high accumulation in macrophages and granulation tissues studied by microautoradiography. J Nucl Med. (1992) 33:1972–80.
4. Yamada S, Kubota K, Kubota R, Ido T, Tamahashi N. High accumulation of fluorine-18-fluorodeoxyglucose in turpentine-induced inflammatory tissue. J Nucl Med. (1995) 36:1301–6.
5. Reinhold-Keller E, Zeidler A, Gutfleisch J, Peter H, Raspe H, Gross W. Giant cell arteritis is more prevalent in urban than in rural populations: results of an epidemiological study of primary systemic vasculitides in Germany. Rheumatol Oxf Engl. (2000) 39:1396–402. doi: 10.1093/rheumatology/39.12.1396
6. Calamia K, Hunder G. Giant cell arteritis (Temporal Arteritis) presenting as fever of undetermined origin. Arthritis Rheum. (1981) 24:1414–8.
7. Buttgereit F, Dejaco C, Matteson E, Dasgupta B. Polymyalgia rheumatica and giant cell arteritis: A systematic review. JAMA. (2016) 315:2442–58.
8. Salvarani C, Macchioni P, Tartoni P, Rossi F, Baricchi R, Castri C, et al. Polymyalgia rheumatica and giant cell arteritis: a 5-year epidemiologic and clinical study in Reggio Emilia. Italy. Clin Exp Rheumatol. (1987) 5:205–15.
9. Patil P, Williams M, Maw W, Achilleos K, Elsideeg S, Dejaco C, et al. Fast track pathway reduces sight loss in giant cell arteritis: results of a longitudinal observational cohort study. Clin Exp Rheumatol. (2015) 33(2 Suppl 89):103–6.
10. Diamantopoulos A, Haugeberg G, Lindland A, Myklebust G. The fast-track ultrasound clinic for early diagnosis of giant cell arteritis significantly reduces permanent visual impairment: towards a more effective strategy to improve clinical outcome in giant cell arteritis? Rheumatol Oxf Engl. (2016) 55:66–70. doi: 10.1093/rheumatology/kev289
11. Schmidt W, Seifert A, Gromnica-Ihle E, Krause A, Natusch A. Ultrasound of proximal upper extremity arteries to increase the diagnostic yield in large-vessel giant cell arteritis. Rheumatol Oxf Engl. (2008) 47:96–101. doi: 10.1093/rheumatology/kem322
12. Brack A, Martinez-Taboada V, Stanson A, Goronzy J, Weyand C. Disease pattern in cranial and large-vessel giant cell arteritis. Arthritis Rheum. (1999) 42:311–7.
13. Mukhtyar C, Guillevin L, Cid M, Dasgupta B, Groot de K, Gross W, et al. EULAR recommendations for the management of large vessel vasculitis. Ann Rheum Dis. (2009) 68:318–23. doi: 10.1136/ard.2008.088351
14. Luqmani R, Lee E, Singh S, Gillett M, Schmidt W, Bradburn M, et al. The Role of Ultrasound Compared to Biopsy of Temporal Arteries in the Diagnosis and Treatment of Giant Cell Arteritis (TABUL): a diagnostic accuracy and cost-effectiveness study. Health Technol Assess Winch Engl. (2016) 20:1–238. doi: 10.3310/hta20900
15. Maz M, Chung S, Abril A, Langford C, Gorelik M, Guyatt G, et al. 2021 American college of rheumatology/vasculitis foundation guideline for the management of giant cell arteritis and takayasu arteritis. Arthritis Rheumatol. (2021) 73:1349–65.
16. Ponte C, Grayson P, Robson J, Suppiah R, Gribbons K, Judge A, et al. 2022 American College of Rheumatology/EULAR classification criteria for giant cell arteritis. Ann Rheum Dis. (2022) 81:1647–53.
17. Bienvenu B, Ly K, Lambert M, Agard C, André M, Benhamou Y, et al. Management of giant cell arteritis: Recommendations of the French Study Group for Large Vessel Vasculitis (GEFA). Rev Med Interne. (2016) 37:154–65. doi: 10.1016/j.revmed.2015.12.015
18. Mackie S, Dejaco C, Appenzeller S, Camellino D, Duftner C, Gonzalez-Chiappe S, et al. British Society for Rheumatology guideline on diagnosis and treatment of giant cell arteritis: executive summary. Rheumatology. (2020) 59:487–94. doi: 10.1093/rheumatology/kez664
19. Gribbons K, Ponte C, Carette S, Craven A, Cuthbertson D, Hoffman G, et al. Patterns of arterial disease in takayasu’s arteritis and giant cell arteritis. Arthritis Care Res. (2020) 72:1615–24. doi: 10.1002/acr.24055
20. Malich L, Gühne F, Hoffmann T, Malich A, Weise T, Oelzner P, et al. Distribution patterns of arterial affection and the influence of glucocorticoids on 18F-fluorodeoxyglucose positron emission tomography/CT in patients with giant cell arteritis. RMD Open. (2022) 8:e002464. doi: 10.1136/rmdopen-2022-002464
21. Blockmans D, Stroobants S, Maes A, Mortelmans L. Positron emission tomography in giant cell arteritis and polymyalgia rheumatica: evidence for inflammation of the aortic arch. Am J Med. (2000) 108:246–9. doi: 10.1016/s0002-9343(99)00424-6
22. Besson F, Parienti J, Bienvenu B, Prior J, Costo S, Bouvard G, et al. Diagnostic performance of 18F-fluorodeoxyglucose positron emission tomography in giant cell arteritis: a systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. (2011) 38:1764–72. doi: 10.1007/s00259-011-1830-0
23. Lee Y, Choi S, Ji J, Song G. Diagnostic accuracy of 18F-FDG PET or PET/CT for large vessel vasculitis: A meta-analysis. Z Rheumatol. (2016) 75:924–31.
24. Soussan M, Nicolas P, Schramm C, Katsahian S, Pop G, Fain O, et al. Management of large-vessel vasculitis with FDG-PET: A systematic literature review and meta-analysis. Medicine (Baltimore). (2015) 94:e622. doi: 10.1097/MD.0000000000000622
25. Lariviere D, Benali K, Coustet B, Pasi N, Hyafil F, Klein I, et al. Positron emission tomography and computed tomography angiography for the diagnosis of giant cell arteritis: A real-life prospective study. Medicine (Baltimore). (2016) 95:e4146. doi: 10.1097/MD.0000000000004146
26. Hay B, Mariano-Goulart D, Bourdon A, Benkiran M, Vauchot F, De Verbizier D, et al. Diagnostic performance of 18F-FDG PET-CT for large vessel involvement assessment in patients with suspected giant cell arteritis and negative temporal artery biopsy. Ann Nucl Med. (2019) 33:512–20. doi: 10.1007/s12149-019-01358-5
27. Nielsen B, Hansen I, Kramer S, Haraldsen A, Hjorthaug K, Bogsrud T, et al. Simple dichotomous assessment of cranial artery inflammation by conventional 18F-FDG PET/CT shows high accuracy for the diagnosis of giant cell arteritis: a case-control study. Eur J Nucl Med Mol Imaging. (2019) 46:184–93. doi: 10.1007/s00259-018-4106-0
28. Sammel A, Hsiao E, Schembri G, Nguyen K, Brewer J, Schrieber L, et al. Diagnostic accuracy of positron emission tomography/computed tomography of the head, neck, and chest for giant cell arteritis: A prospective, double-blind, cross-sectional study. Arthritis Rheumatol. (2019) 71:1319–28. doi: 10.1002/art.40864
29. Nienhuis P, Sandovici M, Glaudemans A, Slart R, Brouwer E. Visual and semiquantitative assessment of cranial artery inflammation with FDG-PET/CT in giant cell arteritis. Semin Arthritis Rheum. (2020) 50:616–23. doi: 10.1016/j.semarthrit.2020.04.002
30. Besson F, Chaumet-Riffaud P, Playe M, Noel N, Lambotte O, Goujard C, et al. Contribution of (18)F-FDG PET in the diagnostic assessment of fever of unknown origin (FUO): a stratification-based meta-analysis. Eur J Nucl Med Mol Imaging. (2016) 43:1887–95. doi: 10.1007/s00259-016-3377-6
31. Blockmans D, De Ceuninck L, Vanderschueren S, Knockaert D, Mortelmans L, Bobbaers H. Repetitive 18-fluorodeoxyglucose positron emission tomography in isolated polymyalgia rheumatica: a prospective study in 35 patients. Rheumatol Oxf Engl. (2007) 46:672–7. doi: 10.1093/rheumatology/kel376
32. Lavado-Pérez C, Martínez-Rodríguez I, Martínez-Amador N, Banzo I, Quirce R, Jiménez-Bonilla J, et al. (18)F-FDG PET/CT for the detection of large vessel vasculitis in patients with polymyalgia rheumatica. Rev Esp Med Nucl Imagen Mol. (2015) 34:275–81.
33. Belhocine T, Blockmans D, Hustinx R, Vandevivere J, Mortelmans L. Imaging of large vessel vasculitis with (18)FDG PET: illusion or reality? A critical review of the literature data. Eur J Nucl Med Mol Imaging. (2003) 30:1305–13.
34. Espitia O, Schanus J, Agard C, Kraeber-Bodéré F, Hersant J, Serfaty J, et al. Specific features to differentiate Giant cell arteritis aortitis from aortic atheroma using FDG-PET/CT. Sci Rep. (2021) 11:17389. doi: 10.1038/s41598-021-96923-2
35. Slart R. FDG-PET/CT(A) imaging in large vessel vasculitis and polymyalgia rheumatica: joint procedural recommendation of the EANM, SNMMI, and the PET Interest Group (PIG), and endorsed by the ASNC. Eur J Nucl Med Mol Imaging. (2018) 45:1250–69. doi: 10.1007/s00259-018-3973-8
36. Pugh D, Karabayas M, Basu N, Cid M, Goel R, Goodyear C, et al. Large-vessel vasculitis. Nat Rev Dis Primer. (2022) 7:1–23. doi: 10.1038/s41572-021-00327-5
37. Robson J, Kiran A, Maskell J, Hutchings A, Arden N, Dasgupta B, et al. The relative risk of aortic aneurysm in patients with giant cell arteritis compared with the general population of the UK. Ann Rheum Dis. (2015) 74:129–35. doi: 10.1136/annrheumdis-2013-204113
38. Nuenninghoff D, Hunder G, Christianson T, McClelland R, Matteson E. Incidence and predictors of large-artery complication (aortic aneurysm, aortic dissection, and/or large-artery stenosis) in patients with giant cell arteritis: a population-based study over 50 years. Arthritis Rheum. (2003) 48:3522–31. doi: 10.1002/art.11353
39. García-Martínez A, Hernández-Rodríguez J, Arguis P, Paredes P, Segarra M, Lozano E, et al. Development of aortic aneurysm/dilatation during the followup of patients with giant cell arteritis: a cross-sectional screening of fifty-four prospectively followed patients. Arthritis Rheum. (2008) 59:422–30. doi: 10.1002/art.23315
40. Kermani T, Warrington K, Crowson C, Ytterberg S, Hunder G, Gabriel S, et al. Large-vessel involvement in giant cell arteritis: a population-based cohort study of the incidence-trends and prognosis. Ann Rheum Dis. (2013) 72:1989–94. doi: 10.1136/annrheumdis-2012-202408
41. Galli E, Muratore F, Mancuso P, Boiardi L, Marvisi C, Besutti G, et al. The role of PET/CT in disease activity assessment in patients with large vessel vasculitis. Rheumatol Oxf Engl. (2022) 8:keac125. doi: 10.1093/rheumatology/keac125
42. Blockmans D, Coudyzer W, Vanderschueren S, Stroobants S, Loeckx D, Heye S, et al. Relationship between fluorodeoxyglucose uptake in the large vessels and late aortic diameter in giant cell arteritis. Rheumatol Oxf Engl. (2008) 47:1179–84. doi: 10.1093/rheumatology/ken119
43. Grayson P, Alehashemi S, Bagheri A, Civelek A, Cupps T, Kaplan M, et al. 18 F-Fluorodeoxyglucose-Positron emission tomography as an imaging biomarker in a prospective, longitudinal cohort of patients with large vessel vasculitis. Arthritis Rheumatol. (2018) 70:439–49. doi: 10.1002/art.40379
44. Quinn K, Ahlman M, Alessi H, LaValley M, Neogi T, Marko J, et al. Association of 18F-fluorodeoxyglucose positron emission tomography and angiographic progression of disease in large-vessel vasculitis. Arthritis Rheumatol. (2022) 75:98–107. doi: 10.1002/art.42290
45. Hellmich B, Agueda A, Monti S, Buttgereit F, de Boysson H, Brouwer E, et al. 2018 Update of the EULAR recommendations for the management of large vessel vasculitis. Ann Rheum Dis. (2020) 79:19–30. doi: 10.1136/annrheumdis-2019-215672
46. Alba M, García-Martínez A, Prieto-González S, Tavera-Bahillo I, Corbera-Bellalta M, Planas-Rigol E, et al. Relapses in patients with giant cell arteritis: prevalence, characteristics, and associated clinical findings in a longitudinally followed cohort of 106 patients. Medicine (Baltimore). (2014) 93:194–201. doi: 10.1097/MD.0000000000000033
47. Kermani T, Warrington K, Cuthbertson D, Carette S, Hoffman G, Khalidi N, et al. Disease relapses among patients with giant cell arteritis: A prospective, longitudinal cohort study. J Rheumatol. (2015) 42:1213–7. doi: 10.3899/jrheum.141347
48. Both M, Ahmadi-Simab K, Reuter M, Dourvos O, Fritzer E, Ullrich S, et al. MRI and FDG-PET in the assessment of inflammatory aortic arch syndrome in complicated courses of giant cell arteritis. Ann Rheum Dis. (2008) 67:1030–3. doi: 10.1136/ard.2007.082123
49. van der Geest K, Treglia G, Glaudemans A, Brouwer E, Sandovici M, Jamar F, et al. Diagnostic value of [18F]FDG-PET/CT for treatment monitoring in large vessel vasculitis: a systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. (2021) 48:3886–902. doi: 10.1007/s00259-021-05362-8
50. Nielsen B, Gormsen L, Hansen I, Keller K, Therkildsen P, Hauge E. Three days of high-dose glucocorticoid treatment attenuates large-vessel 18F-FDG uptake in large-vessel giant cell arteritis but with a limited impact on diagnostic accuracy. Eur J Nucl Med Mol Imaging. (2018) 45:1119–28. doi: 10.1007/s00259-018-4021-4
51. Schönau V, Roth J, Tascilar K, Corte G, Manger B, Rech J, et al. Resolution of vascular inflammation in patients with new-onset giant cell arteritis: data from the RIGA study. Rheumatol Oxf Engl. (2021) 60:3851–61. doi: 10.1093/rheumatology/keab332
52. Quinn K, Dashora H, Novakovich E, Ahlman M, Grayson P. Use of 18F-fluorodeoxyglucose positron emission tomography to monitor tocilizumab effect on vascular inflammation in giant cell arteritis. Rheumatol Oxf Engl. (2021) 60:4384–9. doi: 10.1093/rheumatology/keaa894
53. Imfeld S, Aschwanden M, Rottenburger C, Schegk E, Berger C, Staub D, et al. [18F]FDG positron emission tomography and ultrasound in the diagnosis of giant cell arteritis: congruent or complementary imaging methods? Rheumatol Oxf Engl. (2020) 59:772–8. doi: 10.1093/rheumatology/kez362
54. de Boysson H, Dumont A, Liozon E, Lambert M, Boutemy J, Maigné G, et al. Giant-cell arteritis: concordance study between aortic CT angiography and FDG-PET/CT in detection of large-vessel involvement. Eur J Nucl Med Mol Imaging. (2017) 44:2274–9. doi: 10.1007/s00259-017-3774-5
55. Olthof S, Krumm P, Henes J, Nikolaou K, la Fougère C, Pfannenberg C, et al. Imaging giant cell arteritis and Aortitis in contrast enhanced 18F-FDG PET/CT: Which imaging score correlates best with laboratory inflammation markers? Eur J Radiol. (2018) 99:94–102. doi: 10.1016/j.ejrad.2017.12.021
56. Vaidyanathan S, Chattopadhyay A, Mackie S, Scarsbrook A. Comparative effectiveness of 18F-FDG PET-CT and contrast-enhanced CT in the diagnosis of suspected large-vessel vasculitis. Br J Radiol. (2018) 91:20180247. doi: 10.1259/bjr.20180247
57. Meller J, Strutz F, Siefker U, Scheel A, Sahlmann C, Lehmann K, et al. Early diagnosis and follow-up of aortitis with [(18)F]FDG PET and MRI. Eur J Nucl Med Mol Imaging. (2003) 30:730–6.
58. Quinn K, Ahlman M, Malayeri A, Marko J, Civelek A, Rosenblum J, et al. Comparison of magnetic resonance angiography and 18F-fluorodeoxyglucose positron emission tomography in large-vessel vasculitis. Ann Rheum Dis. (2018) 77:1165–71. doi: 10.1136/annrheumdis-2018-213102
59. Toshihiko N. Current status of large and small vessel vasculitis in Japan. Int J Cardiol. (1996) 54 Suppl:S91–8. doi: 10.1016/s0167-5273(96)88777-8
60. Watanabe Y, Miyata T, Tanemoto K. Current clinical features of new patients with takayasu arteritis observed from cross-country research in japan: Age and sex specificity. Circulation. (2015) 132:1701–9. doi: 10.1161/CIRCULATIONAHA.114.012547
61. Saadoun D, Bura-Riviere A, Comarmond C, Lambert M, Redheuil A, Mirault T, et al. French recommendations for the management of Takayasu’s arteritis. Orphanet J Rare Dis. (2021) 16(Suppl 3):311. doi: 10.1186/s13023-021-01922-1
62. Saadoun D, Vautier M, Cacoub P. Medium- and large-vessel vasculitis. Circulation. (2021) 143:267–82. doi: 10.1161/CIRCULATIONAHA.120.046657
63. Mason J. Takayasu arteritis–advances in diagnosis and management. Nat Rev Rheumatol. (2010) 6:406–15. doi: 10.1038/nrrheum.2010.82
64. Grayson P, Ponte C, Suppiah R, Robson J, Gribbons K, Judge A, et al. 2022 American College of Rheumatology/EULAR classification criteria for Takayasu arteritis. Ann Rheum Dis. (2022) 81:1654–60.
65. Santhosh S, Mittal B, Gayana S, Bhattacharya A, Sharma A, Jain S. F-18 FDG PET/CT in the evaluation of Takayasu arteritis: an experience from the tropics. J Nucl Cardiol. (2014) 21:993–1000. doi: 10.1007/s12350-014-9910-8
66. Duftner C, Dejaco C, Sepriano A, Falzon L, Schmidt W, Ramiro S. Imaging in diagnosis, outcome prediction and monitoring of large vessel vasculitis: a systematic literature review and meta-analysis informing the EULAR recommendations. RMD Open. (2018) 4:e000612. doi: 10.1136/rmdopen-2017-000612
67. Comarmond C, Biard L, Lambert M, Mekinian A, Ferfar Y, Kahn J, et al. Long-Term outcomes and prognostic factors of complications in takayasu arteritis. Circulation. (2017) 136:1114–22.
68. Janes A, Castro M, Arraes A, Savioli B, Sato E, de Souza A. A retrospective cohort study to assess PET-CT findings and clinical outcomes in Takayasu arteritis: does 18F-fluorodeoxyglucose uptake in arteries predict relapses? Rheumatol Int. (2020) 40:1123–31. doi: 10.1007/s00296-020-04551-2
69. Ishihara T, Haraguchi G, Tezuka D, Kamiishi T, Inagaki H, Isobe M. Diagnosis and assessment of Takayasu arteritis by multiple biomarkers. Circ J. (2013) 77:477–83.
70. Kerr G, Hallahan C, Giordano J, Leavitt R, Fauci A, Rottem M, et al. Takayasu arteritis. Ann Intern Med. (1994) 120:919–29.
71. Misra R, Danda D, Rajappa S, Ghosh A, Gupta R, Mahendranath K, et al. Development and initial validation of the Indian Takayasu Clinical Activity Score (ITAS2010). Rheumatology. (2013) 52:1795–801. doi: 10.1093/rheumatology/ket128
72. Barra L, Kanji T, Malette J, Pagnoux C, CanVasc. Imaging modalities for the diagnosis and disease activity assessment of Takayasu’s arteritis: A systematic review and meta-analysis. Autoimmun Rev. (2018) 17:175–87. doi: 10.1016/j.autrev.2017.11.021
73. Alessi H, Quinn K, Ahlman M, Novakovich E, Saboury B, Luo Y, et al. Longitudinal characterization of vascular inflammation and disease activity in takayasu’s arteritis and giant cell arteritis: A single-center prospective study. Arthritis Care Res. (2022) 1–9. doi: 10.1002/acr.24976
74. Addimanda O, Spaggiari L, Pipitone N, Versari A, Pattacini P, Salvarani C. Pulmonary artery involvement in Takayasu arteritis. PET/CT versus CT angiography. Clin Exp Rheumatol. (2013) 31(1 Suppl 75):S3–4.
75. Gao W, Gong J, Guo X, Wu J, Xi X, Ma Z, et al. Value of 18F-fluorodeoxyglucose positron emission tomography/computed tomography in the evaluation of pulmonary artery activity in patients with Takayasu’s arteritis. Eur Heart J Cardiovasc Imaging. (2021) 22:541–50. doi: 10.1093/ehjci/jeaa229
76. Ma L, Wu B, Jin X, Sun Y, Kong X, Ji Z, et al. A novel model to assess disease activity in Takayasu arteritis based on 18F-FDG-PET/CT: a Chinese cohort study. Rheumatol Oxf Engl. (2022) 61(SI):SI14–22.
77. Laurent C, Ricard L, Fain O, Buvat I, Adedjouma A, Soussan M, et al. PET/MRI in large-vessel vasculitis: clinical value for diagnosis and assessment of disease activity. Sci Rep. (2019) 9:12388.
78. van der Geest K, Sandovici M, Nienhuis P, Slart R, Heeringa P, Brouwer E, et al. Novel PET imaging of inflammatory targets and cells for the diagnosis and monitoring of giant cell arteritis and polymyalgia rheumatica. Front Med. (2022) 9:902155. doi: 10.3389/fmed.2022.902155
79. Liozon E. Place actuelle de l’imagerie non invasive des artères de gros calibre dans l’artérite à cellules géantes: du diagnostic au suivi. Rev Méd Interne. (2020) 41:756–68. doi: 10.1016/j.revmed.2020.06.004
80. Rinagel M, Chatelus E, Jousse-Joulin S, Sibilia J, Gottenberg J, Chasset F, et al. Diagnostic performance of temporal artery ultrasound for the diagnosis of giant cell arteritis: a systematic review and meta-analysis of the literature. Autoimmun Rev. (2019) 18:56–61.
81. Nielsen B, Hansen I, Keller K, Therkildsen P, Gormsen L, Hauge E. Diagnostic accuracy of ultrasound for detecting large-vessel giant cell arteritis using FDG PET/CT as the reference. Rheumatol Oxf Engl. (2020) 59:2062–73. doi: 10.1093/rheumatology/kez568
82. Hop H, Mulder D, Sandovici M, Glaudemans A, van Roon A, Slart R, et al. Diagnostic value of axillary artery ultrasound in patients with suspected giant cell arteritis. Rheumatology. (2020) 59:3676–84.
83. Skoog J, Svensson C, Eriksson P, Sjöwall C, Zachrisson H. The diagnostic performance of an extended ultrasound protocol in patients with clinically suspected giant cell arteritis. Front Med. (2021) 8:807996. doi: 10.3389/fmed.2021.807996
84. Bley T, Uhl M, Carew J, Markl M, Schmidt D, Peter H, et al. Diagnostic value of high-resolution MR imaging in giant cell arteritis. AJNR Am J Neuroradiol. (2007) 28:1722–7. doi: 10.3174/ajnr.A0638
85. Rhéaume M, Rebello R, Pagnoux C, Carette S, Clements-Baker M, Cohen-Hallaleh V, et al. High-Resolution magnetic resonance imaging of scalp arteries for the diagnosis of giant cell arteritis: Results of a prospective cohort study. Arthritis Rheumatol Hoboken NJ. (2017) 69:161–8. doi: 10.1002/art.39824
86. Kumar S, Radhakrishnan S, Phadke R, Gupta R, Gujral R. Takayasu’s arteritis: evaluation with three-dimensional time-of-flight MR angiography. Eur Radiol. (1997) 7:44–50. doi: 10.1007/s003300050107
Keywords: 2-[18F]FDG-PET/CT, giant cell arteritis, takayasu arteritis, large vessel vasculitis, large vessel arteritis
Citation: Nassarmadji K, Vanjak A, Bourdin V, Champion K, Burlacu R, Mouly S, Sène D and Comarmond C (2023) 18-Fluorodeoxyglucose positron emission tomography/computed tomography for large vessel vasculitis in clinical practice. Front. Med. 10:1103752. doi: 10.3389/fmed.2023.1103752
Received: 20 November 2022; Accepted: 04 January 2023;
Published: 19 January 2023.
Edited by:
Clément Bailly, Centre Hospitalier Universitaire (CHU) de Nantes, FranceReviewed by:
Bastien Jamet, Centre Hospitalier Universitaire (CHU) de Nantes, FranceCopyright © 2023 Nassarmadji, Vanjak, Bourdin, Champion, Burlacu, Mouly, Sène and Comarmond. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cloé Comarmond,  Y2hsb2UuY29tYXJtb25kb3J0b2xpQGFwaHAuZnI=
Y2hsb2UuY29tYXJtb25kb3J0b2xpQGFwaHAuZnI=