 Julien Guiot1*
Julien Guiot1* Monique Henket1Marie Ernst2
Monique Henket1Marie Ernst2 Laurence Seidel2
Laurence Seidel2 Marie Winandy1
Marie Winandy1 Anna Denis1Anne-Noëlle Frix1Fanny Gester1Marie Thys3Laurie Giltay1Omaima Garah1
Anna Denis1Anne-Noëlle Frix1Fanny Gester1Marie Thys3Laurie Giltay1Omaima Garah1 Makon-Sébastien Njock1Perrine Canivet4Paul Meunier4Jean-Louis Corhay1
Makon-Sébastien Njock1Perrine Canivet4Paul Meunier4Jean-Louis Corhay1 Céline Regnier5
Céline Regnier5 Olivier Malaise5Michel Malaise5Renaud Louis1
Olivier Malaise5Michel Malaise5Renaud Louis1- 1Department of Respiratory Medicine, CHU Liège, Liège, Belgium
- 2Biostatistics and Research Method Center (B-STAT), CHU Liège, Liège, Belgium
- 3Department of Medico-Economic and Data, CHU Liège, Liège, Belgium
- 4Department of Radiology, CHU Liège, Liège, Belgium
- 5Department of Rheumatology, CHU Liège, Liège, Belgium
Objectives: In our study, we explored the specific subgroup of patients with rheumatoid arthritis (RA) suffering from obstructive lung disease (OLD) and its impact on morbi-mortality.
Methods: Our retrospective study included 309 patients suffering from RA with either obstructive (O-RA) or non-obstructive patterns (non-O-RA). OLD was defined based on the Tiffeneau index at the first available pulmonary functional test (PFT). Survival was then calculated and represented by a Kaplan–Meier curve. The comparison between the populations considered was performed by the Log-Rank test.
Results: Out of the 309 RA patients, 102 (33%) had airway obstruction. The overall survival time was significantly lower in the O-RA group than in the non-O-RA group (n = 207) (p < 0.001). The median survival time was 11.75 years in the O-RA group and higher than 16 years in the non-O-RA group. Multivariate analysis identified OLD as an independent risk factor for mortality (HR 2.20; 95% CI 1.21–4.00, p < 0.01).
Conclusion: Airway obstruction can be an independent risk factor of mortality in RA and should be considered as an early marker of poor prognosis. Further prospective longitudinal studies are required in order to determine the best clinical management for O-RA patients.
Introduction
Rheumatoid arthritis is a systemic inflammatory disorder that most commonly affects the joints, causing progressive destruction of the cartilage and the bone, which reduces mobility and can lead to severe functional disabilities. Apart from the musculoskeletal disease, one of the main manifestations driving its mortality is interstitial lung disease (ILD) widely known to be associated with a worse outcome in this context (1).
Patients suffering from RA typically have circulating antibodies, the most common being rheumatoid factor (RF) and anti-cyclic citrullinated peptide (CCP). Antibodies onset may precede the disease onset and may be associated with the development of RA-associated lung disease. Physiopathologically, there is growing evidence that RA begins in the lung with active citrullination of vimentin peptides induced by tobacco exposure (2, 3). Similarly, epidemiological data showed that in a global RA population, most of the patients were presenting a tobacco abuse history (former smokers or ex-smokers) (4).
Out of this context, chronic smoking abuse is widely recognized to induce chronic obstructive pulmonary disease (COPD) and emphysema. COPD is an obstructive lung disease (OLD) where airflow limitation is not fully reversible (5). Functional definition is based on spirometry and a post-bronchodilator FEV1/FVC ratio (Tiffeneau index) of less than 70%, which is the usually recommended cut-off (5). The origin of airflow obstruction is thought to be related to persistent bronchial inflammation due to noxious particles and gas.
The most frequently incriminated etiologic factor is tobacco smoking and environmental exposure. In opposition, RA is frequently associated with ILD and is clinically significant in up to 10% of the global RA population which leads to a restrictive syndrome defined as a reduced total lung capacity (TLC) (6–10). Some patients can experience an association of those two conditions that can modify the overall morbi-mortality of those patients (1, 6–8, 10). According to different studies, the percentages of RA patients with COPD vary from 3 to 10% (10), patients with bronchiectasis, from 2 to 58% (11, 12), and patients with ILD (either nonspecific interstitial pneumonia (NSIP) or usual interstitial pneumonia (UIP)) from 6 to 56% (9, 12).
Therefore, the evaluation of OLD associated with RA is a key question to determine its impact on patient mortality. It is important to note that patients suffering from RA can underestimate respiratory symptoms due to a significant reduction in their mobility induced by arthritis and inflammatory symptoms.
This descriptive and explorative study aimed to describe RA patients exhibiting OLD (O-RA) phenotype and their functional characteristics compared to those without obstruction.
Methods
Study population
A retrospective observational study was conducted. Patients were recruited from our ambulatory care policlinic at CHU from 01-08-2004 to 01-01-2020 based on a systematic evaluation of electronic hospital records using specific keywords (rheumatoid arthritis). We selected patients with available PFT suffering from RA according to ACR/EULAR 2010 classification criteria for RA (13) based on a specialized evaluation by a rheumatologist. We did not exclude patients based on clinical criteria or comorbidities.
Airway obstruction was defined by a Tiffeneau index (FEV1/FVC assessed after salbutamol 400 μg) < 70% (5). Progressive fibrosing ILD (PF-ILD) was defined as:
• a relative decline in FVC of at least 10% of the predicted value;
• or a relative decline in the FVC of 5% to less than 10% of the predicted value and worsening of respiratory symptoms;
• or an increased extent of fibrosis on high-resolution computed tomography (HRCT) of the chest;
• or worsening of respiratory symptoms and an increased extent of fibrosis on HRCT.
Asthma was evaluated as recommended by GINA guidelines (14), whereas specific documentation was manually obtained from the patient’s medical file.
Collected data
Information was collected on patients’ characteristics (age, gender, smoking status) and clinical characteristics (diagnosis, medical history, radiological patterns, lung function, biomarkers, and treatment). We were not able to collect cardiovascular comorbidities, known to be of interest in the RA population, nor common comorbidities such as diabetes, renal or hepatic failure, and arterial hypertension, from the patient’s medical files, because this study was retrospective, and we did not have a reliable and dedicated evaluation of these parameters.
Data on medications were collected throughout the study, including immunosuppressive agents. The survival status of the patients was confirmed based on a specific analysis of the national registry.
PFT values were the earliest available and the biological values [hemoglobin, white blood cell count, platelets, C-reactive protein (CRP), fibrinogen, lymphocytes, monocytes, neutrophils, anti-citrullinated peptide antibody (ACPA), and rheumatoid factor (RF)] were the values closest to the date of the first PFT (±1 month).
The protocol was approved by the ethics committee of the University Hospital of Liège (Belgian Number: B707201422832; ref.: 2022/52).
Patient and public involvement
Patients or the public were not involved in our research’s design, conduct, reporting, or dissemination plans.
Statistics
Results are presented as frequency tables for qualitative variables and as mean and standard deviation (SD) or as the median and interquartile range (IQR) for quantitative variables.
Comparisons between O-RA and non-O-RA groups were done by chi-square tests (or Fisher exact) for categorical variables, or by Student t-test for continuous variables (log-transformed data in case of skewness). Overall survival since the first available PFT was represented by a Kaplan–Meier curve. Cox regression models were used to analyze the overall survival concerning groups and other parameters (FVC, DLCO, FEV-1, Age, gender, RA-ILD, bronchiectasis, emphysema, asthma, neoplasia, and COPD). Results were considered significant at the 5% uncertainty level (p < 0.05). The calculations were performed using SAS version 9.4 and the graphs using R version 4.1.0.
Results
Subject demographics
Among our cohort of 1,497 retrospectively collected patients suffering from RA, 309 had at least one PFT available; 299 out of these 309 patients also had an HRCT. In this cohort, 102 patients were exhibiting the obstructive phenotype (33%). Patients were predominantly female, with 54 and 72% for O-RA and non-O-RA, respectively. The mean age was of 67 ± 10 years for the O-RA group. 69% of the non-O-RA and 76% of the O-RA group were active or former smokers. There was no significant difference between the two groups regarding smoking status.
Among patients treated with immunosuppressors, 70% were non-O-RA. Patients who suffered from O-RA were less likely to be affected by ILD. The obstructive phenotype of their disease was more often manifested by the presence of asthma, COPD, emphysema, or neoplasia. Patients with O-RA benefited more frequently from bronchodilator therapy and inhaled corticotherapy (Table 1).
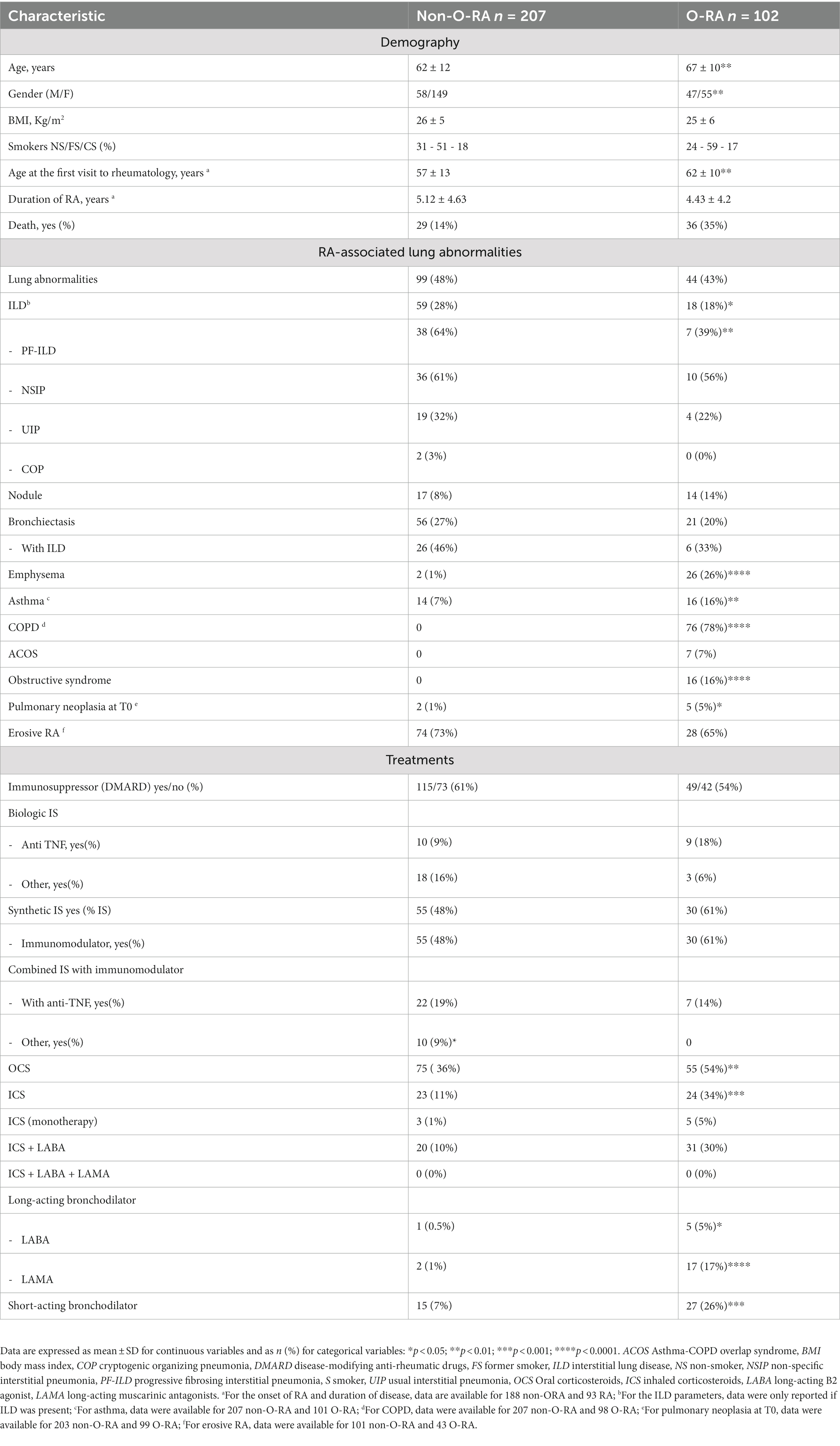
Table 1. Patient characteristics.
Pulmonary functional tests
Pulmonary functional tests are shown in Table 2. Spirometric values were significantly different between O-RA and non-O-RA patients. O-RA patients exhibited lower FEV1 (65% vs. 91% pred, p < 0.0001), FVC (86% vs. 93% pred, p < 0.01), which can be explained by hyperinflation linked to the obstruction, as well as DLCO (54% vs. 66% pred, p < 0.0001) but not KCO. By definition, all patients in the O-RA group were presenting a reduced Tiffeneau index (FEV1/FVC) under 70%, as commonly seen in COPD.
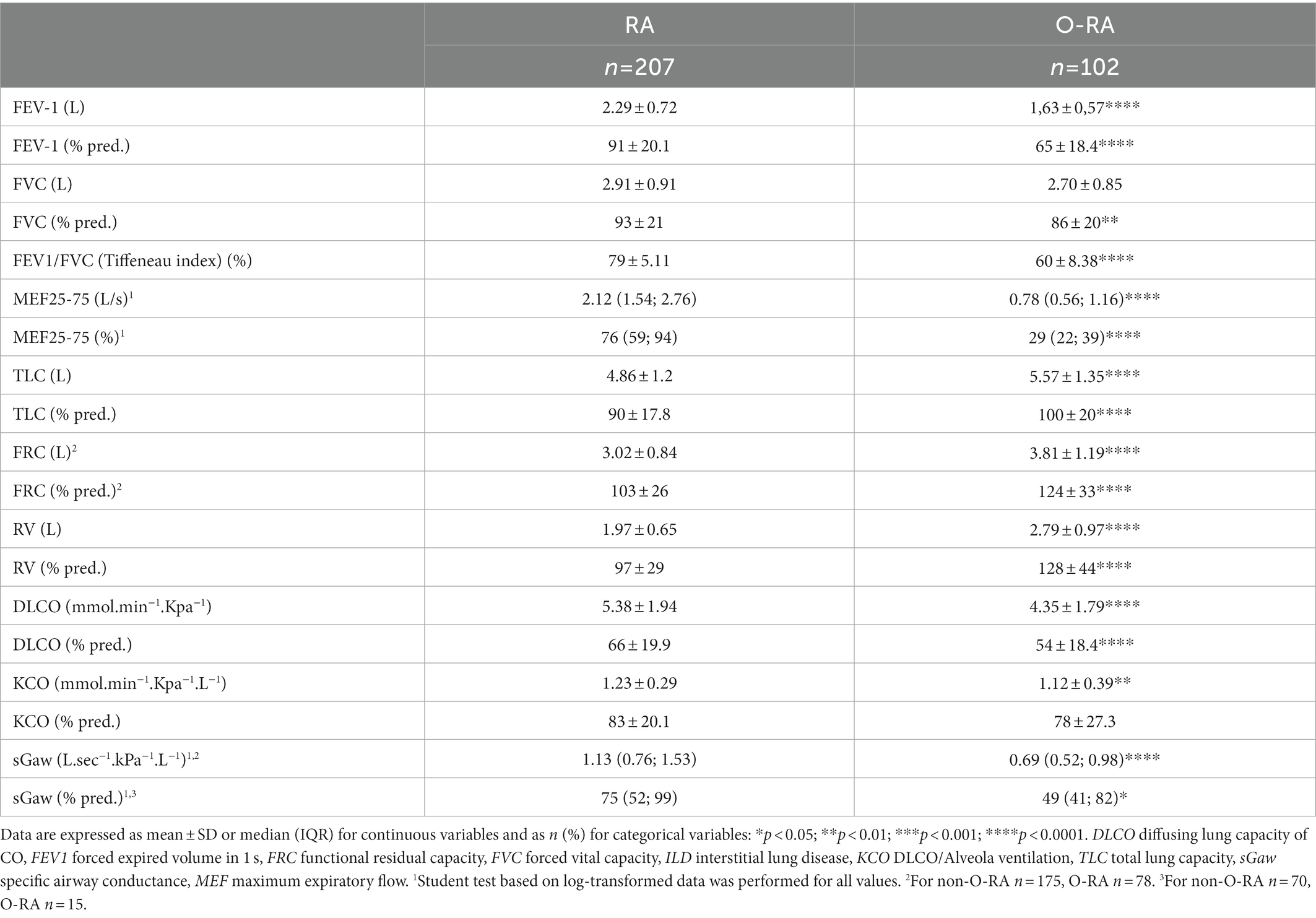
Table 2. Pulmonary function tests.
Inspiratory flow limitation related to dysfunction of the cricothyroid muscle of the larynx, which may be involved in RA patients, was not found in the medical record review (no dysphonia or inspiratory symptoms).
As usually identified in other obstructive airway diseases, O-RA patients had a significant reduction in their specific airway conductance as referred by the sGaw value compared to non-O-RA patients (0.69 and 1.13 l.sec−1.kPa−1.L−1, respectively, p < 0.0001), and small airway involvement assessed by maximum expiratory flow (MEF) 25/75 (29% vs. 76% pred, respectively, p < 0.0001). Supplementary Table S1 shows PFTs results according to each patient’s combination of pulmonary pathologies.
Blood analysis
In the O-RA subgroup, we identified a significant decrease in lymphocyte count (p < 0.05) whereas CRP, fibrinogen, and neutrophils count were significantly increased (p < 0.001, p < 0.01, p < 0.01, respectively). We did not identify significant differences concerning total IgE and total eosinophil count (Table 3). Missing values are listed in Supplementary Table S2.
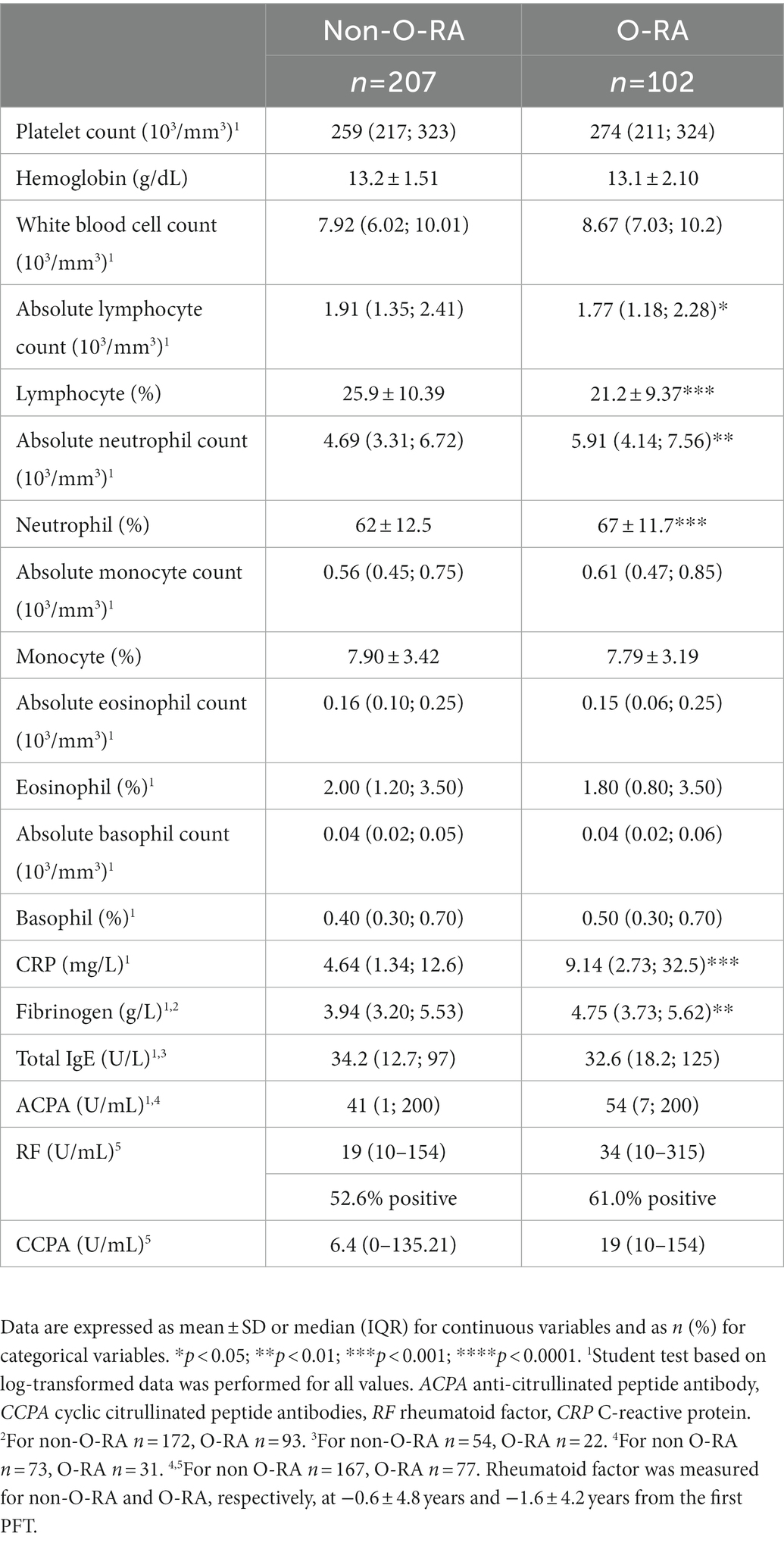
Table 3. Biological characteristics.
Survival analysis
The objective of this study was to predict the survival time for non-O-RA and O-RA patients. Therefore, time-dependent tools were required to evaluate these models. The predictive values of models have been evaluated using concordance statistics (Harrell’s C-statistics). The predictive accuracy of survival by O-RA is summarized in Supplementary Table S3 for both univariate and multivariate models.
An alternative is to compute the time-dependent ROC(t) curve and the associated AUC(t) for given survival thresholds t and to summarize it over time using the integrated AUC (iAUC). The AUC over time is represented in Supplementary Figure. Based on C-statistics or on iAUC, both multivariate models showed equivalent accuracy and they improved the accuracy from the univariate model.
In terms of survival analysis, we found that patients with O-RA had a significantly higher risk of death than those without obstruction (HR = 2.50; 95%CI 1.52–4.10, p < 0.001). The median survival time since the first PFT was 11.75 years in the O-RA group and was higher than 16 years in the non-O-RA group.
The survival probability at 8 years and 10 years was in the non-O-RA group at 87.1 and 84.5% and in the O-RA group at 68.0 and 58.8%, respectively (Figure 1).
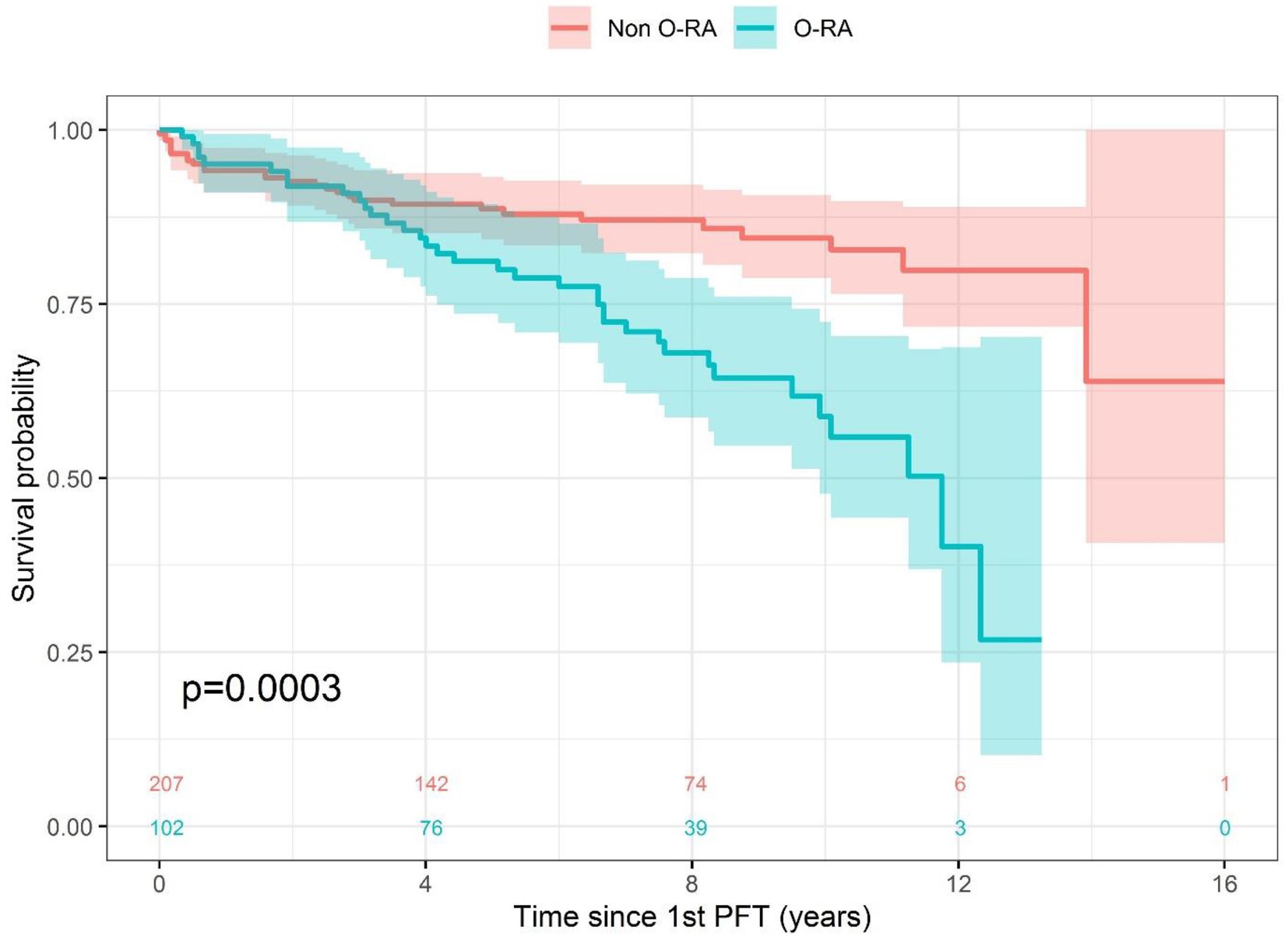
Figure 1. Survival analysis.
Multivariate survival analysis
In the univariate models, in addition to the obstructive character, all the parameters obtained from the fisrt PFT were significantly associated with an increased risk of death. This was also the case for age, ILD status, emphysema, COPD and active neoplasia at the beginning of the study.
The multivariate analysis performed on 301 patients, adjusting the model for the different comorbidities and demographic characteristics of the patients, confirmed that O-RA was an independent risk factor for mortality (HR 2.20; 95% CI 1.23–3.92, p < 0.01). ILD was also an independent risk factor for death (HR 1.86; 95% CI 1.06–3.27, p < 0.05), and age (HHR 1.04, 95% CI 1.01–10.7, p < 0.01). Active neoplasia was also an independent risk factor of increased mortality (HR 4.74, 95% CI 1.61–14.0, p < 0.01). Of note, we did not find any significantly increased mortality risk associated with bronchiectasis, or asthma (Table 4).
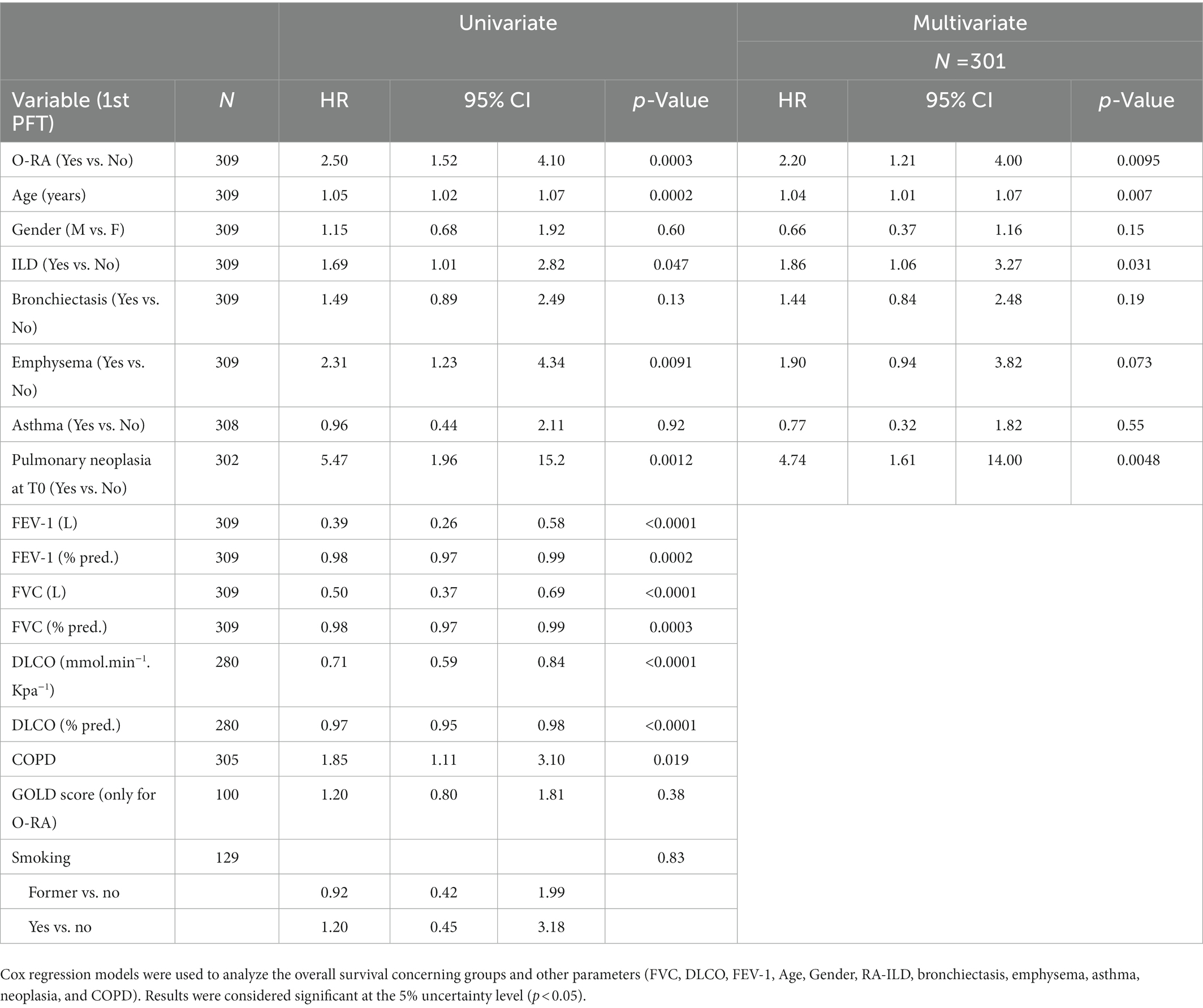
Table 4. Multivariate cox regression analysis.
Discussion
The current study provides a comprehensive analysis of a cohort of patients suffering from RA retrospectively analyzed to better qualify the specific subgroup of those suffering from obstructive lung disease (O-RA). We found that obstruction is an independent risk factor for increased mortality. Knowing that lung disease is recognized as one of the major comorbidities in RA, and even if smoking abuse is widely known to be associated with an increased risk of RA, we cannot exclude that COPD can act as an isolated factor contributing to RA-associated morbimortality (8, 15, 16) through neutrophilic inflammation associated with this condition. Whereas more than 70% of our O-RA population had a significant smoking history, RA can probably also independently lead to obstruction through autonomous bronchiolar inflammation.
In our study, approximately two-thirds of the O-RA population could be described as suffering from COPD. We identified that in a cohort of 309 RA patients that benefited from PFT during their clinical follow-up, 33% of them were suffering from OLD. Those O-RA patients were displaying a higher TLC with hyperinflation based on RV evaluation associated with per definition a reduced FEV1/FVC ratio (17). DLCO was also significantly lower in the O-RA cohort compared to the other patients. The O-RA patients were also presenting a reduced specific conductance (sGaw) with increased FRC. Focusing on the mortality, O-RA patients presenting an overall increased mortality with a median survival of 11.8 years (HR 2.50, 95% CI 1.52–4.10) confirmed by the multivariate analysis (HR 2.20; 95% CI 1.23–3.92).
Several studies have identified that COPD was an independent risk factor for developing RA. This observation suggests that mucosal airway inflammation may increase the risk of RA (18). Of interest, a case-control study previously showed that both RA and COPD were exhibiting similar morbidities (18, 19). In a meta-analysis evaluating previous studies, it has been described that RA patients have a significantly increased risk of suffering from COPD with a pooled RR of 1.82 (95% CI = 1.55 to 2.10, p < 0.001) (10). This meta-analysis showed a prevalence of COPD in RA of 6.2% (95% CI = 4.1 to 8.3%). Of note, few have compared the mortality of these patients longitudinally. Our prevalence is probably higher than in other studies due to the retrospective aspect of our study, considering that PFT has probably been performed in symptomatic patients only.
We have recently shown in a 1,500 RA patients cohort that patients with ILD had a higher mortality risk compared to non-ILD RA patients (9). This study confirms that ILD is an independent predictor of mortality also for patients with O-RA.
The association of RA with COPD may have affected the severity of the disease. Indeed, COPD causes high mortality and may play a decisive role in all patients with various chronic diseases, including RA. Currently, we are prospectively evaluating whether COPD may be an interfering factor in the control of RA in a systematic manner.
Interestingly, we identified that patients with O-RA were exhibiting increased levels of CRP. As it was previously described in other studies, increased CRP and fibrinogen levels are known to be associated with increased overall mortality in COPD (20, 21) as well as with the risk of cardiovascular events (22). There is evidence that the inflammatory process in COPD is relevant to the development of cardiovascular disease and lung cancer (23). Therefore, we cannot avoid that common physiopathological processes may be shared by both COPD and O-RA patients.
Whereas COPD is known to be the major cause of OLD, we cannot certify that in our cohort none of them was suffering from obliterans bronchiolitis (also previously referred to as constrictive bronchiolitis), which is clinically known to be more severe and often quickly fatal in RA.
The retrospective aspect of this study must be disclosed as a significant bias. Indeed, patients who have undergone PFT are thought to be more symptomatic than others or are suspected of suffering from an OLD. Therefore, the prevalence of O-RA might have been overestimated. We cannot avoid that some of them can also experience bronchiolitis associated with RA (15). This can overestimate the proportion of O-RA patients in a RA cohort. This bias was mitigated in our study as the non-O-RA cohort was similarly recruited.
Surprisingly, in our O-RA cohort, we found that only 41.4% of the population was treated with bronchodilators, which are the cornerstone of COPD treatment. Thus, COPD patients in this RA cohort were under-treated. However, the majority of O-RA patients aerosol-treated would have benefited in our study from those therapies based on the GOLD recommendation. COPD and RA have similar complications over time. Indeed, it appears that these two situations lead to progressive musculoskeletal degradation linked to a significant deterioration in the quality of life and a functional decline. In this context, both drug management and musculoskeletal rehabilitation remain imperative to minimize long-term complications.
One other limitation of this study out of its retrospective aspect is the lack of information concerning the occurrence of incidental respiratory infection favored by immunosuppressive therapies. COPD patients are at higher risk to develop lower respiratory tract infections. In this specific population, adding bronchodilator therapy is a key factor to reduce acute exacerbations. The multivariate analysis did not include immunosuppressive status since patients had benefited from multiple specific therapies that can modify the interpretability of those results. Moreover, we did not have information on the cardiovascular status of the patients, which is known to be also associated with an increased risk of mortality. We were not able to retrieve from the medical records frequent comorbidities such as diabetes, renal or hepatic insufficiency, and arterial hypertension, because this study was retrospective, and we did not have a reliable and dedicated evaluation of these parameters.
Many patients were referred to our center, which is a tertiary clinical center where the patients did not benefit from other examinations than rheumatologic ones, during which these points were not systematically identified as present or absent.
In conclusion, patients with combined obstructive lung disease and rheumatoid arthritis exhibit a characteristic functional profile with reduced FEV-1, small airway involvement, reduced sGaw, hyperinflation, and lower carbon monoxide diffusing capacity of the lung. Our study identified that patients with O-RA were at higher risk of death compared to other RA patients. OLD in RA seems to be an independent risk factor of mortality based on our data potentially associated with an underlying inflammatory process similar to what is seen in COPD.
Therefore, patients with RA have to be considered for specific and dedicated pulmonary evaluation to treat both ILD and OLD. Spirometry is a key indicator of RA-associated lung disease that can modify a patient’s outcome. Further prospective longitudinal studies will have to determine its implication in patients’ management and follow-up and particularly the need for an early diagnosis to propose appropriate bronchodilator therapy.
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available because these data are considered sensitive but are available from the corresponding author upon reasonable request.
Ethics statement
The studies involving human participants were reviewed and approved by Ethics Committee of the University Hospital of Liège (Belgian Number: B707201422832; ref.: 2022/52). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
JG, MM, and RL conceived the study. JG, ME, and LS developed the study methodology. MH and MT collected data and validated the data. AD, A-NF, FG, PC, CR, OM, LG, and OG acquired data. JG, M-SN, PM, and J-LC analyzed the data. MH, ME, and LS made the statistical analysis. JG, MH, ME, LS, and MW wrote the manuscript. MM and RL coordinated the research activity. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors wish to thank the study participants and the hospital staff for their participation in this study.
Conflict of interest
JG reports personal fees for the advisory board, work, and lectures from Boehringer Ingelheim, Janssens, GSK, Roche, AstraZeneca, and Chiesi, non-financial support for meeting attendance from AstraZeneca, Chiesi, Roche, Boehringer Ingelheim, and Janssens. He is in the permanent SAB of Radiomics (Oncoradiomics SA) for the SALMON trial without any specific consultancy fee for this work. He is a co-inventor of one issued patent on radiomics licensed to Radiomics (Oncoradiomics SA).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2023.1063012/full#supplementary-material
SUPPLEMENTARY FIGURE S1 | Comparison of time-dependent AUC(t) for univariate or multivariate models for survivval analysis.
References
1. Kadura, S, and Raghu, G. Rheumatoid arthritis-interstitial lung disease: manifestations and current concepts in pathogenesis and management. Eur Respir Rev Eur Respir Soc. (2021) 30:210011. doi: 10.1183/16000617.0011-2021
2. Saag, KG, Cerhan, JR, Kolluri, S, Ohashi, K, Hunninghake, GW, and Schwartz, DA. Cigarette smoking and rheumatoid arthritis severity. Ann Rheum Dis. (1997) 56:463–9. doi: 10.1136/ard.56.8.463
3. Bernstein, EJ, Barr, RG, Austin, JHM, Kawut, SM, Raghu, G, Sell, JL, et al. Rheumatoid arthritis-associated autoantibodies and subclinical interstitial lung disease: the multi-ethnic study of atherosclerosis. Thorax. (2016) 71:1082–90. doi: 10.1136/thoraxjnl-2016-208932
4. Roh, S. Smoking as a preventable risk factor for rheumatoid arthritis: rationale for smoking cessation treatment in patients with rheumatoid arthritis. J Rheumatic Dis. (2019) 26:12. doi: 10.4078/jrd.2019.26.1.12
5. Vogelmeier, CF, Criner, GJ, Martinez, FJ, Anzueto, A, Barnes, PJ, Bourbeau, J, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. Am J Respir Crit Care Med Am Thoracic Soc. (2017) 195:557–82. doi: 10.1164/rccm.201701-0218PP
6. Curtis, JR, Sarsour, K, Napalkov, P, Costa, LA, and Schulman, KL. Incidence and complications of interstitial lung disease in users of tocilizumab, rituximab, abatacept and anti-tumor necrosis factor α agents, a retrospective cohort study. Arthritis Res Ther. (2015) 17:319. doi: 10.1186/s13075-015-0835-7
7. Kim, EJ, Collard, HR, and King, TE. Rheumatoid arthritis-associated interstitial lung disease: the relevance of histopathologic and radiographic pattern. Chest. (2009) 136:1397–405. doi: 10.1378/chest.09-0444
8. Guiot, J, Henket, M, Frix, AN, Gester, F, Thys, M, Giltay, L, et al. Combined obstructive airflow limitation associated with interstitial lung diseases (O-ILD): the bad phenotype? Respir Res. (2022) 23. doi: 10.1186/s12931-022-02006-9
9. Denis, A, Henket, M, Ernst, M, Maes, N, Thys, M, Regnier, C, et al. Progressive fibrosing interstitial lung disease in rheumatoid arthritis: a retrospective study. Front Med. (2022) 9:1024298. doi: 10.3389/fmed.2022.1024298
10. Ma, Y, Tong, H, Zhang, X, Wang, M, Yang, J, Wu, M, et al. Chronic obstructive pulmonary disease in rheumatoid arthritis: a systematic review and meta-analysis. Respir Res. (2019) 20:144–8. doi: 10.1186/s12931-019-1123-x
11. Yunt, ZX, and Solomon, JJ. Lung disease in rheumatoid arthritis In:. Rheum Dis Clin North Am. (2015). 41: 225–36. doi: 10.1016/j.rdc.2014.12.004
12. Alunno, A, Gerli, R, Giacomelli, R, and Carubbi, F. Review article clinical, epidemiological, and histopathological features of respiratory involvement in rheumatoid arthritis. Biomed Res Int. (2017). doi: 10.1155/2017/7915340
13. Aletaha, D, Neogi, T, Silman, AJ, Funovits, J, Felson, DT, Bingham, CO, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheum. (2010) 62:2569–81. doi: 10.1002/art.27584
14. GINA-Main-Report-2022-FINAL-22-07-01-WMS. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2022. Available from: www.ginasthma.org
15. Olson, AL, Swigris, JJ, Sprunger, DB, Fischer, A, Fernandez-Perez, ER, Solomon, J, et al. Rheumatoid arthritis-interstitial lung disease-associated mortality. Am J Respir Crit Care Med. (2011) 183:372–8. doi: 10.1164/rccm.201004-0622OC
16. Perez, T, Remy-Jardin, M, and Cortet, B. Airways involvement in rheumatoid arthritis: clinical, functional, and HRCT findings. Am J Respir Crit Care Med. (1998) 157:1658–65. doi: 10.1164/ajrccm.157.5.9710018
17. O’Donnell, DE, and Laveneziana, P. Physiology and consequences of lung hyperinflation in COPD. Eur Respir Rev. (2006) 15:61–7. doi: 10.1183/09059180.00010002
18. Friedlander, HM, Ford, JA, Zaccardelli, A, Terrio, AV, Cho, MH, and Sparks, JA. Obstructive lung diseases and risk of rheumatoid arthritis. Expert Review of Clinical Immunology (2020). 16:37–50. doi: 10.1080/1744666X.2019.1698293
19. Othman, FM, Ismaeil, T, Alharbi, E, Alanazi, R, Alkharf, R, Alharbi, AA, et al. Risk of rheumatoid arthritis in patients with obstructive lung disease. Respir Care. (2021) 66(Suppl10):3603521
20. Sin, DD, Anthonisen, NR, Soriano, JB, and Agusti, AG. Mortality in COPD: role of comorbidities. Eur Respir J Eur Respir Soc. (2006) 28:1245–57. doi: 10.1183/09031936.00133805
21. Agustí, A, Edwards, LD, Rennard, SI, Macnee, W, Tal-Singer, R, and Miller, BE. et al., Persistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotype. PLoS One. (2012) 7:e37483. doi: 10.1371/journal.pone.0037483
22. Sin, DD, and Man, SFP. Systemic inflammation and mortality in chronic obstructive pulmonary disease. Can J Physiol Pharmacol. (2007) 85:141–7. doi: 10.1139/y06-093
23. King, PT. Inflammation in chronic obstructive pulmonary disease and its role in cardiovascular disease and lung cancer. Clin Transl Med. (2015) 4:26. doi: 10.1186/s40169-015-0068-z
Glossary
Keywords: rheumatoid arthritis, airway obstruction, chronic obstructive pulmonary disease, interstitial lung diseases, bronchiolitis
Citation: Guiot J, Henket M, Ernst M, Seidel L, Winandy M, Denis A, Frix A-N, Gester F, Thys M, Giltay L, Garah O, Njock M-S, Canivet P, Meunier P, Corhay J-L, Regnier C, Malaise O, Malaise M and Louis R (2023) Airflow obstruction as a marker of adverse prognosis in rheumatoid arthritis. Front. Med. 10:1063012. doi: 10.3389/fmed.2023.1063012
Edited by:
Chantal Raherison, Centre Hospitalier Universitaire Guadeloupe, FranceReviewed by:
Hung Yu Huang, Linkou Chang Gung Memorial Hospital, TaiwanMohammad Reza Aslani, Ardabil University of Medical Sciences, Iran
Copyright © 2023 Guiot, Henket, Ernst, Seidel, Winandy, Denis, Frix, Gester, Thys, Giltay, Garah, Njock, Canivet, Meunier, Corhay, Regnier, Malaise, Malaise and Louis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julien Guiot, Si5HdWlvdEBjaHVsaWVnZS5iZQ==