
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Med. , 09 February 2023
Sec. Family Medicine and Primary Care
Volume 10 - 2023 | https://doi.org/10.3389/fmed.2023.1021255
This article is part of the Research Topic Acupuncture for Pain Management View all 20 articles
 Jae-Hong Kim1,2*†
Jae-Hong Kim1,2*† Changsop Yang3†
Changsop Yang3† Jaehee Yoo1,2Gwang-Cheon Park2
Jaehee Yoo1,2Gwang-Cheon Park2 Byoung-Kab Kang3
Byoung-Kab Kang3 Ae-Ran Kim4Jihye Kim5Dongwoo Nam6Yejin Hong7
Ae-Ran Kim4Jihye Kim5Dongwoo Nam6Yejin Hong7Background: We aim to obtain clinical trial data regarding the safety, efficacy, and usefulness of invasive laser acupuncture (ILA) for non-specific chronic low back pain (NSCLBP) through a randomized placebo-controlled trial.
Methods: Our clinical trial will be an assessor- and patient-blinded, prospective, parallel-arm, multi-center, randomized placebo-controlled clinical trial. One hundred and six participants with NSCLBP will be allocated evenly to the 650 ILA or control group. All participants will receive education on exercise and self-management. The 650 ILA group will undergo 650 nm ILA for 10 min, and the control group will undergo sham ILA for 10 min per visit, twice a week for 4 weeks, at bilateral GB30, BL23, BL24, and BL25. The primary outcome will be the proportion of responders (≥30% reduction in pain visual analogue scale [VAS] without increased use of painkillers) at 3 days after the intervention ends. The secondary outcomes will include changes in the scores of the VAS, European Quality of Life Five Dimension Five Level scale, and Korean version of the Oswestry Disability Index at 3 days after the intervention ends and 8 weeks after the intervention ends.
Discussions: The results of our study will provide clinical evidence concerning the safety and efficacy of 650 nm ILA for the management of NSCLBP.
Clinical trial registration: https://cris.nih.go.kr/cris/search/detailSearch.do?search_lang=E&focus=reset_12&search_page=M&pageSize=10&page=undefined&seq=21591&status=5&seq_group=21591, identifier KCT0007167.
Low back pain (LBP), defined as discomfort and pain, localized below the costal margin and above the inferior gluteal folds with or without referred lower extremity pain, is a symptom rather than a specific disease (1, 2). It is a major cause of disability in daily living. Functional restrictions and consequent disabilities pose a huge economic burden for individuals and the society (3). Most LBPs are non-specific (commonly cited as 90–95%) (4), and non-specific chronic LBP (NSCLBP) is defined as that which cannot be attributed to a known specific pathology (e.g., structural deformity, tumor, osteoporosis, infection, radicular syndrome, fracture, cauda equina syndrome, or ankylosing spondylitis) and persists for >3 months (1, 2, 5–7).
Treatment guidelines for patients with NSCLBP recommend the use of exercise therapy, antidepressants, psychosocial interventions, and non-steroidal anti-inflammatory drugs (2, 5, 6). Non-pharmacological treatments, such as exercise and self-management, are preferred to pharmacological interventions in the management of NSCLBP (2, 7–9). Physical modalities such as transcutaneous electrical nerve stimulation and low level laser therapy (LLLT) have a low quality evidence (6, 8) and acupuncture has mixed support and received conflicting recommendations (2, 5, 8).
Low level laser therapy is a light source intervention that creates no vibration, heat, or sound and stimulates photochemical or non-thermal cellular processes (10). LLLT is currently used to treat musculoskeletal disorders, such as back pain (11). The possible underlying mechanisms for the pain reduction effects of LLLT include its inhibition of neural function, anti-inflammatory effect, and connective tissue repair ability which have been demonstrated by a number of experiments (12–14). Laser acupuncture (LA) is the irradiation of a low-intensity laser at the acupoints using laser pointer devices (15). Whether LLLT, including LA, is effective for LBP when compared with sham laser remains controversial. A Cochrane systematic review of LLLT on non-specific LBP in 2008 decried the lack of sufficient data to either refute or support the efficacy of LLLT for the management of LBP (16). In contrast, a meta-analysis suggested that LLLT was an effective treatment for reducing pain in patients with NSCLBP (17, 18). Glazov et al. reported that LLLT alone or in combination with other therapies might effectively reduce pain for up to 3 months in NSCLBP without adverse effects (19).
While LA is a non-invasive therapy that uses laser-emitting devices, invasive LA (ILA) is conducted concurrently with invasive acupuncture and focused laser irradiation utilizing an acupuncture needle attached to a laser instrument (20). Our previous pilot randomized controlled trial (RCT) revealed that 650 nm ILA with the same ILA parameters (650 nm wavelength, 20 mW power, and 50 Hz frequency), treatment acupoint, and treatment schedule as in this study significantly improved pain and pain-related functional limitations in patients with NSCLBP at the end of the intervention (21). These potential effects of 650 nm ILA on NSCLBP requires validation using a rigorous RCT with a large sample size. Therefore, we aim to obtain clinical evidence on the safety and efficacy of 650 nm ILA for the management of NSCLBP. In a situation where is no high-quality evidence supporting the efficacy of LLLT and acupuncture, the results of this study will provide clinical evidence of the use of ILA for NSCLBP and thus promote the use of ILA in the treatment of NSCLBP.
1) We will investigate the clinically persistent pain-reduction effect of 650 nm ILA for NSCLBP at 3 days after the end of intervention.
2) We will investigate the pain reduction, functional limitation improvement, and quality of life improvement effects of 650 nm ILA for NSCLBP.
3) We will investigate the safety of 650 nm ILA in patients with NSCLBP.
1) The 650 ILA group will have a significantly higher proportion of responders than the control group at 3 days after the end of intervention.
2) The 650 nm ILA will show improvements in pain intensity, quality of life, and functional limitation in patients with NSCLBP.
3) The 650 nm ILA would be a safe treatment for patients with NSCLBP.
Our study was approved by the Ministry of Food and Drug Safety (Medical Device Approval No. 1322) and was registered with the Clinical Research Information Service (registration No. KCT0007167). Our study complies with the Korean Good Clinical Practice guidelines and the principles of the Declaration of Helsinki. We have written the manuscript in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) reporting checklist (22).
This clinical trial will be an assessor and patient–blinded, prospective, parallel-arm, multi-center, randomized placebo-controlled clinical trial. In total, 106 eligible participants will be randomized evenly into the 650 ILA or control group (n = 53 in each group). All participants will receive education on exercise and self-management. Participants in the 650 ILA group will undergo real 650 nm ILA for 10 min, while those in the control group will undergo sham ILA for 10 min. The treatment will be administered once per visit, twice a week for 4 weeks, at bilateral Gallbladder 30 (GB30; Huantiao), Bladder 23 (BL23; Shenshu), Bladder 24 (BL24; Qihaishu), and Bladder 25 (BL25; Dachangshu).
The primary outcome will be the proportion of responders (≥30% reduction in pain visual analogue scale [VAS] without increased use of painkillers) at 3 days after the intervention ends. The secondary outcome will be changes in the scores of the VAS, European Quality of Life Five Dimension Five Level scale (EQ-5D-5L), and Korean version of the Oswestry Disability Index (ODI) at 3 days after the intervention ends and 8 weeks after the intervention ends.
The clinical trial design is shown in Table 1.
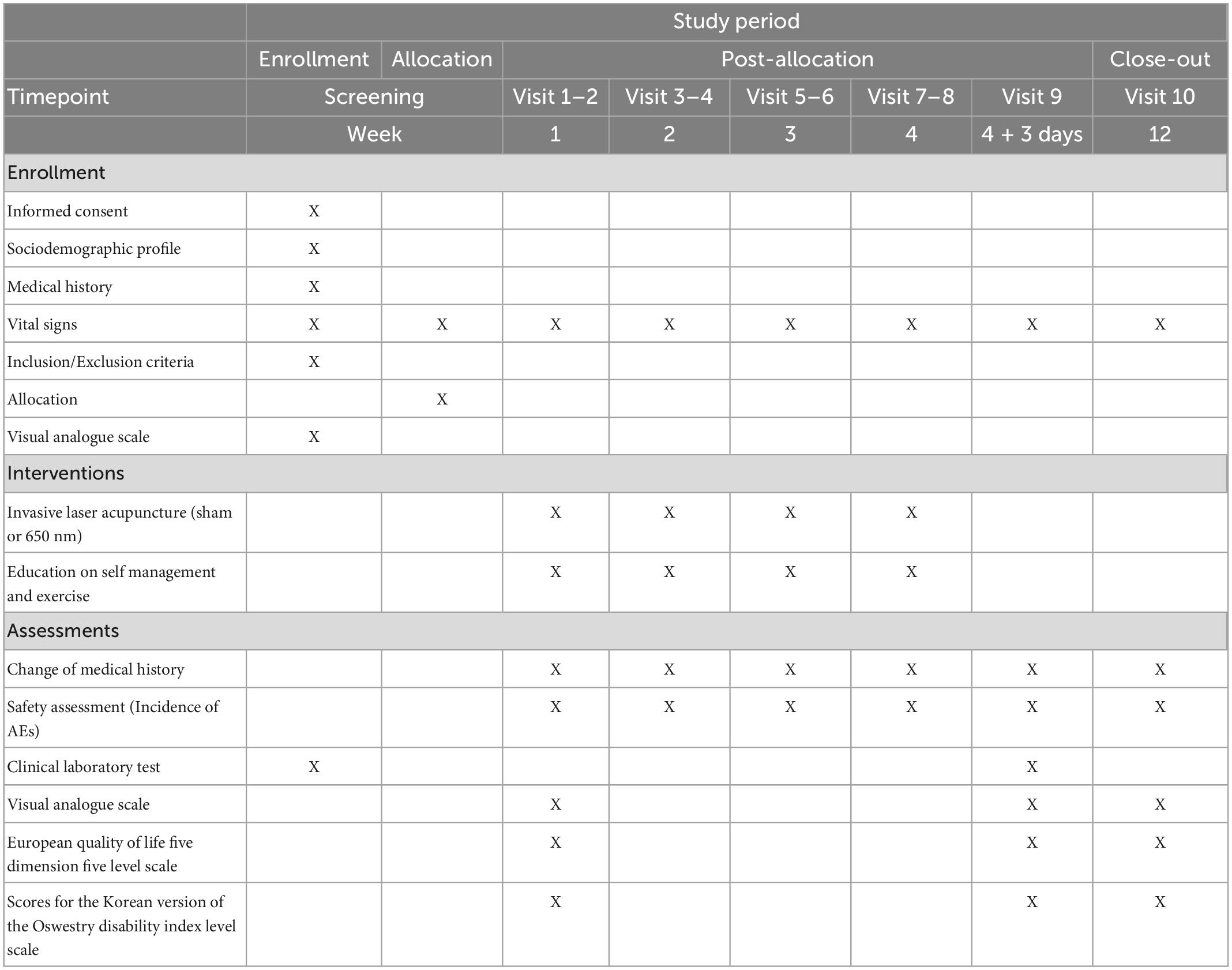
Table 1. SPIRIT statement showing the enrollment, interventions, and data collection.
We will recruit participants at the Kyung Hee University Korean Medicine Hospital and Dongshin University Gwangju Korean Medicine Hospital in the Republic of Korea via the use of posters, local newspapers, and the internet in hospitals and communities. Interested people will receive an explanation of this study from the clinical research coordinator (CRC) upon visiting the hospital and will provide written informed consent prior to participation.
At each visit, the CRC will explain the following visit schedule and will adjust the visit schedules for each participant to facilitate participation.
(1) Adults aged between 19 and 70 years; (2) has NSCLBP lasting for at least the preceding 3 months, and LBP that occurred more than 14 days a month; (3) has no change in history of medications for 4 weeks before screening. For participants with medications prescribed and used for NSCLBP, usage shall be at a stable dose in the 4 weeks prior to the baseline visit; (4) moderate pain (100 mm VAS scores for pain had a range of 35–74) (23) at screening; and (5) has sufficient fluency in Korean to perform valid assessments.
(1) Participants has progressive neurological deficits or radicular pain; (2) has a serious disease (diabetic neuropathy or cancer, severe kidney, liver, cerebrovascular, or cardiovascular disease); (3) has a serious spinal pathology (cauda equina syndrome, cancer, inflammatory spondylitis, recent vertebral fracture, or spinal infection); (4) has a LBP caused by rheumatoid arthritis, ankylosing spondylitis, gout, trauma, or fibromyalgia; (5) has a history of treatment for mental illness (depression, dementia, schizophrenia, or epilepsy) or drug/alcohol dependency in the 6 months preceding screening; (6) has moderate or severe depression (scored ≥ 23 points on a Korean version of Beck depression inventory-II) (24) at screening; (7) has contraindications for ILA, such as presence of electronic medical devices, severe skin disease in the lumbar region, blood clotting abnormalities, or presence of metallic devices in the lumbar vertebrae; (8) has a history of lumbar spinal surgery within 1 year or scheduled procedures during the trial; (9) participation for the purpose of social insurance or compensation; (10) concurrent participation in another trial; (11) Pregnant or having a plan for pregnancy; and (12) not suitable for ILA and our rescue regimen.
The dropout criteria are as follows: (1) incomplete data that can affect the results of the trial; (2) decision to discontinue participation in this trial by the institutional review board (IRB) or principal investigator (PI) owing to the inability of the participant to participate in this study or the occurrence of a side effects requiring long-term treatment; (3) withdrawal of consent; or (4) occurrence of a serious adverse event (SAE) causing requirement of hospitalization or surgery, serious disability, or death. Participants who meet the dropout criteria will be discontinued from participating in our clinical trial.
The violation criteria are as follows: (1) participating in less than six of the eight treatment sessions (<75% compliance with the intervention protocol); and (2) serious deviation in implementation or critical errors in the protocol.
The participants who meet the violation and dropout criteria will be excluded from the per protocol set (PPS) analysis.
This protocol (version. 1.0) was approved by the Ministry of Food and Drug Safety (date: March 16, 2022; Medical Device Approval # 1322). It was approved by the IRB of Kyung Hee University Korean Medicine Hospital (date: April 22, 2022; approval No.: KOMCIRB 2022-03-004-001) and Dongshin University Gwangju Korean Medicine Hospital (date: March 22, 2022; approval No.: DSGOH-2022-002). Participants and their companions will be informed of the study purpose and risks. All participants will provide written informed consent prior to participation.
The investigator will carry out a screening interview, and then the assessor will conduct baseline assessment. The 106 enrolled participants will be randomly allocated evenly to the 650 ILA or control group (n = 53 per group). The serial numbers will be generated by stratified block randomization using SAS® version 9.4 (SAS Institute Inc., Cary, NC, USA). The serial numbers will be packed in opaque envelopes and stored in a cabinet with two locks.
The investigator managing the serial numbers will open the envelopes and assign participants to the investigator who will conduct the intervention.
The investigator managing the serial numbers will generate the randomization sequence and distribute participants to the groups. The CRC will enroll the participants.
The practitioner will insert the acupuncture needles into GB30, BL23, BL24, and BL25 and then operate the laser emitting device according to the treatment method of each group (650 ILA group, 20 mW power for 10 min; control group, 0 mW power for 10 min). Therefore, the practitioner who will conduct the intervention would know the group assignment of participant. Owing to the practitioner unblinding, we will adopt an assessor and patient-blinded design using sham ILA. During the course of the study, all investigators except those who will perform the intervention and manage the serial number codes will be blinded. However, if necessary, such as in the event of SAE, unblinding will be permitted under the IRB approval. This study will only include individuals without predetermined positions or competing interests.
Trained Korean medical doctors will administer the treatment. The investigators who will carry out the interventions will undergo joint training to ensure adherence to our protocol. ILA treatment will be conducted using a laser emitting device (Ellise; Wontech Co. Ltd., Daejeon, Republic of Korea) comprising an optical fiber-coupled laser diode (InGaAIP), a sterile acupuncture needle with optical fibers inserted therein, and a laser output device (Figure 1).

Figure 1. Invasive laser acupuncture (ILA) therapy.
The acupuncture needles will be vertically inserted into GB30, BL23, BL24, and BL25 and then the laser (650 ILA group, 20 mW power for 10 min; control group, 0 mW power for 10 min) will be turned on. The ILA parameters will be 50 Hz frequency, 20 mW power, 63.69 W/cm2 power density, 12 J/point energy dose, 38216.56 J/cm2 energy density, and pulse type wave. Participants will receive treatment for 10 min per visit, twice a week for 4 weeks. Based on previous RCTs investigating the efficacy of LLLT for NSCLBP (25, 26), the control group will receive the same procedure as the 650 ILA group. No significant differences in sound, feeling, or observation will be expected between the two groups. Hence, all participants will be blinded. The ILA treatment methods have been described in more details in our previous pilot study (20).
All participants will receive education on exercise and self-management during the treatment period (Visit 1–Visit 8). We will provide all participants with acetaminophen (500 mg), which can be taken when the pain is severe as a rescue regimen.
At each visit, the medical condition of the participants will be monitored to ensure that they adhere to the trial procedure. All participants will be expected to comply with the intervention protocol. However, the assessment and treatment schedule may be changed upon the request of the participant or in accordance with the judgment of the PI.
During the study period, all participants will not be permitted to receive other treatments (complementary and alternative therapies, physical therapy, or pharmacological treatments not allowed in our trial) for improving NSCLBP symptoms. However, they will be allowed to use pharmacological and non-pharmacological treatments for improving other symptoms.
The primary outcome will be the between-group differences of the proportions of responders at 3 days after the intervention ends. A responder is defined as a participant who responds with more than 30% decrease in baseline VAS score without an increase in baseline use of painkillers (27, 28).
The secondary outcomes will include the between-group differences of changes in VAS, EQ-5D-5L, and ODI at 3 days after the treatment ends and 8 weeks after the treatment ends.
The VAS is a self-reported scale, usually a 100-mm-long straight line marked 0 for no pain and 100 for pain as intense as it could be (29). It is widely used to assess pain severity in LBP trials (30).
The EQ-5D is a generic assessment tool for measuring health-related quality of life (31). The EQ-5D-5L is a new version of the EQ-5D that extends the level of each dimension from three to five (32).
The ODI includes nine questions about interference with several physical activities and one question about pain intensity (33). We used the Korean version of the ODI, which excluded sexual life from the original ODI and has been validated (34).
Adverse events (AEs) are unintentional and undesirable symptoms, signs, or diseases that appear during or after treatment in a clinical trial. In our pilot study, no AEs and SAEs were associated with laser irradiation (21). AEs that could occur in our trial include bleeding, pallor, local hematoma, skin irritation, objective worsening of pain, and dizziness or fainting. All the AEs and SAEs would be recorded in detail, including the potential causalities between the intervention and AE, degree of severity, time of occurrence, and any measures taken to improve AE by the CRC. They will be reported to the IRB. The occurrence rate of SAEs and AEs will be compared between the two groups in the safety assessment. Participants who will experience AEs and SAEs related to our intervention will be compensated according to the relevant regulations.
Our protocol has been developed and revised severally by experts in LA, NSCLBP, and statistics. Before the study, all investigators will be trained severally to fully understand the standard operating procedures (SOPs) of this trial and the protocol. An independent clinical research associate will monitor our study and check all the trial documents. Any revision of this protocol will be reviewed and approved by the Ministry of Food and Drug Safety and the IRB of Kyung Hee University Korean Medicine Hospital and Dongshin University Gwangju Korean Medicine Hospital.
In our previous pilot study (21), the difference in proportion of responders between 650 ILA (93% [14/15]) and control groups (40% [6/15]) was 53%. To obtain sufficient clinical data, we determined the sample size assuming an expected responder proportion of 30% in the control group and 60% in the 650 ILA group, a two-sided alpha level of 0.05, and a statistical power of 0.8. Under these assumptions, a total of 84 (42 per group) participants will be required. Estimating a maximum dropout rate of 20%, 106 participants (53 in each group) will be required in our trial.
The final data will be analyzed by a biostatistician not involved in the execution of our trial. The primary analysis population for assessing the efficacy of the intervention will be a full analysis set (FAS), while the supplementary analysis population will be a PPS. The results of the FAS and PPS analyses will be compared and reflected in the efficacy evaluation. “Multiple Imputation” method will be used to obtain the missing value. All analyses will be performed at the 5% (two-sided) significance level using SAS® version 9.4 (SAS institute. Inc., Cary, NC, USA) software. We will not perform interim analyses.
Baseline characteristics and variables will be compared between the two groups. Categorical data will be compared using the Fisher’s exact test or chi-square test, while continuous data will be compared using the Wilcoxon’s rank sum test or independent t-test.
The difference in responder proportions will be tested using the chi-square test or Fisher’s exact test. The degrees of changes in the VAS, EQ-5D-5L, and ODI scores at 3 days after the treatment ends and 8 weeks after the intervention ends, relative to the baseline score, between the groups will be evaluated using analysis of covariance with baseline scores as covariates. Within each group, changes in VAS, EQ-5D-5L, and ODI scores at each time will be analyzed using one-way analysis of variance and a paired t-test or Wilcoxon signed rank test. Sub-analyses will be performed according to each institution.
A safety assessment will be conducted for all SAEs and AEs that will occur during the trial period. The incidences of SAEs and AEs will be compared between the two groups using chi-square test or Fisher’s exact test. A comparative analysis will be carried out between the groups for participants who will be out of normal range for a clinical laboratory test.
All documents will be classified and logged with identification codes, but the names will remain concealed.
All identification records will be kept confidential and will not be accessible without IRB approval. All data will be recorded in the electronic case report forms (eCRFs) by the CRC and checked by a investigator, who will not be involved in the execution of this trial. Electronic data will be securely stored in the eCRFs using the myTrial data management system (NIKOM, Republic of Korea). Data access will be protected by user name and password. The data manager will have online access to the all data, whereas institutions will have access only to data related to their own institution. The data manager and the statistician will have online access to the entire database. The data coordinating center in the Korea Institute of Oriental Medicine will be unaffiliated with the sponsor and devoid of competing interests. No access to the data will be granted to anyone not approved by the IRB. In addition, raw data will be stored for 3 years after the completion of the trial. Participants will voluntarily offer informed written consent for the dissemination of their personal information.
The efficacy of LA for musculoskeletal pain is majorly determined by the energy dosage applied (35). Energy penetration through the skin is affected by the scatter, reflection, and absorption of energy by skin structures. As the acupoints are thought to be located in the myofascial layer, the low energy transmission of non-invasive LA may not be fully effective in stimulating acupoints (15). However, the 650 nm wavelength ILA used in this study is safe and can compensate for the scatter, reflection, and absorption of light by the skin and enhance energy transmission, because the laser is emitted at the acupuncture needle’s tip after being placed beneath the skin. The design of this study, including the ILA intervention (i.e., treatment acupoint and laser wavelength), treatment schedules, outcome measurements, and sample size, is based on that of our previous pilot study (21). In our previous pilot clinical trial (21), 650 nm ILA at bilateral GB30, BL23, BL24, and BL25 showed significant improvement in the VAS and ODI scores at the intervention endpoint and ODI score at 4 weeks after the intervention ends, compared with sham laser in patients with NSCLBP. Therefore, BL23, BL24, BL25, and GB30 were selected for treatment acupoints and 650 nm for laser wavelength in this study.
The clinical assessments used in LBP trials are often highly subjective and correlate poorly with symptoms. The responder index could be sensitive to clinically meaningful treatment effects and could mitigate the placebo effect (27). The preliminary developed responder index for chronic low back pain was at least 30% improvement in pain, with an improvement of at least 30% in patient global assessment and no worsening in function (27). We adopted responder proportions (≥30% relief on the VAS without analgesics increase) used in a recent chronic LBP clinical trial as a primary outcome (28). Four core outcome domains for LBP trial are pain intensity, number of deaths, health-related quality of life, and physical functioning (36, 37). We used change in VAS scores to measure the pain intensity, ODI scores to measure the physical functioning, and EQ-5D-5L scores to evaluate the health-related quality of life.
Considering the results of this study, 650 nm ILA is expected to show safety, clinically significant improvement, pain reduction, and improvement of functional limitation and quality of life in patients with NSCLBP. This is important for the clinical use of 650 nm ILA and development of optimal laser parameters for the treatment of NSCLBP.
This protocol has certain limitations. First, we will not use different treatment methods of LA for NSCLBP treatment. The factors that influence the efficacy of LA are selected acupoints, wavelength, and energy dose. Various treatment methods of LA differ according to wavelength, energy dose, and acupoints for treating NSCLBP (16–19, 38). Since 650 nm ILA parameters, including the wavelength, power, energy dose, and acupoints, used in our pilot study show significant pain reduction at the intervention endpoint, we adopted only the 650 nm ILA parameters used in our pilot study in this study. Thus, further studies should be conducted to investigate the optimal parameters. Second, since most participants in our pilot study had moderate pain at the baseline and the high dropout rate owing to pain increase during the study period in the case of patients with severe pain was concerning, our study will include only patients with moderate NSCLBP, not those with severe NSCLBP. Third, since the practitioner will operate the laser emitting device according to the treatment method of each group (650 ILA group, 20 mW power for 10 min; control group, 0 mW power for 10 min), we cannot adopt practitioner blinding. Therefore, we will adopt an assessor- and patient-blinded study design.
Nevertheless, the findings of this study would suggest clinical evidence concerning the safety and efficacy of 650 nm ILA for the management of NSCLBP, thereby establishing the basis for further investigation. It would contribute to increasing the availability of laser and promoting the development of optimal laser treatment method in the management of LBP.
This protocol (version. 1.0) was approved by the Ministry of Food and Drug Safety (date: March 16, 2022; Medical Device Approval # 1322). It was approved by the IRB of Kyung Hee University Korean Medicine Hospital (date: April 22, 2022; approval No.: KOMCIRB 2022-03-004-001) and Dongshin University Gwangju Korean Medicine Hospital (date: March 22, 2022; approval No.: DSGOH-2022-002). Participants and their companions will be informed of the study purpose and risks. All participants will provide written informed consent prior to participation.
J-HK and CY were responsible for designing and conceiving the trial, preparing the manuscript, supervising the entire clinical trial process, and writing and revising the final manuscript. J-HK, JY, G-CP, A-RK, JK, DN, and YH participated in the data collection and were in charge of the recruitment, treatment, and evaluation of the patients. B-KK was responsible for planning the data analysis and analyzing final data from the trial. All authors reviewed and approved the final manuscript.
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (grant number: HF21C0044). The sponsor had no role in the data collection, analysis, or interpretation, writing of the report, or the decision to submit the resulting report for publication.
We thank our staff and colleagues at the Dongshin University Gwangju Korean Medicine Hospital, Kyung Hee University Korean Medicine Hospital, and Korea Institute of Oriental Medicine for their support. We also thank Mapi Research Trust (contact information and permission to use: Mapi Research Trust, Lyon, France, http://eprovide.mapi-trust.org) and EuroQol Research Foundation (EuroQol request registration number: 48780) for permitting us to use ODI and EQ-5D-5L.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
AE, adverse event; CRC, clinical research coordinator; eCRF, electronic case report form; EQ-5D-5L, European quality of life five dimension five level scale; FAS, full analysis set; ILA, invasive laser acupuncture; IRB, institutional review board; LA, laser acupuncture; LBP, low back pain; LLLT, low-level laser therapy; NSCLBP, non-specific chronic low back pain; ODI, Oswestry disability index; PI, principal investigator; PPS, per-protocol set; RCTs, randomized controlled trials; SAE, serious adverse event; SOPs, standard operating procedures; SPIRIT, standard protocol items: recommendations for interventional trials; VAS, visual analogue scale.
1. Airaksinen O, Brox J, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, et al. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. (2006) 15(Suppl 2):S192–300. doi: 10.1007/s00586-006-1072-1
2. Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. (2017) 389:736–47. doi: 10.1016/S0140-6736(16)30970-9
3. Hoy D, March L, Brooks P, Blyth F, Woolf A, Bain C, et al. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. (2014) 73:968–74. doi: 10.1136/annrheumdis-2013-204428
4. Bardin L, King P, Maher C. Diagnostic triage for low back pain: a practical approach for primary care. Med J Aust. (2017) 206:268–73. doi: 10.5694/mja16.00828
5. Oliveira C, Maher C, Pinto R, Traeger A, Lin C, Chenot J, et al. Clinical practice guidelines for the management of non-specific low back pain in primary care: an updated overview. Eur Spine J. (2018) 27:2791–803. doi: 10.1007/s00586-018-5673-2
6. Qaseem A, Wilt T, McLean R, Forciea M. Clinical Guidelines Committee of the American College of Physicians, Denberg TD, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. (2017) 166:514–30. doi: 10.7326/M16-2367
7. Krenn C, Horvath K, Jeitler K, Zipp C, Siebenhofer-Kroitzsch A, Semlitsch T. Management of non-specific low back pain in primary care – a systematic overview of recommendations from international evidence-based guidelines. Prim Health Care Res Dev. (2020) 21:e64. doi: 10.1017/S1463423620000626
8. Meroni R, Piscitelli D, Ravasio C, Vanti C, Bertozzi L, De Vito G, et al. Evidence for managing chronic low back pain in primary care: a review of recommendations from high-quality clinical practice guidelines. Disabil Rehabil. (2021) 43:1029–43. doi: 10.1080/09638288.2019.1645888
9. Foster N, Anema J, Cherkin D, Chou R, Cohen S, Gross D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet. (2018) 391:2368–83. doi: 10.1016/S0140-6736(18)30489-6
10. Basford J. Low-energy laser therapy: controversies and new research findings. Lasers Surg Med. (1989) 9:1–5. doi: 10.1002/lsm.1900090103
11. Clijsen R, Brunner A, Barbero M, Clarys P, Taeymans J. Effects of low-level laser therapy on pain in patients with musculoskeletal disorders: a systematic review and meta-analysis. Eur J Phys Rehabil Med. (2017) 53:603–10. doi: 10.23736/S1973-9087.17.04432-X
12. Sakurai Y, Yamaguchi M, Abiko Y. Inhibitory effect of low-level laser irradiation on LPS-stimulated prostaglandin E2 production and cyclooxygenase-2 in human gingival fibroblasts. Eur J Oral Sci. (2000) 108:29–34. doi: 10.1034/j.1600-0722.2000.00783.x
13. Skinner S, Gage J, Wilce P, Shaw RM. A preliminary study of the effects of laser radiation on collagen metabolism in cell culture. Aust Dent J. (1996) 41:188–92. doi: 10.1111/j.1834-7819.1996.tb04854.x
14. Chow R, Armati P. Photobiomodulation: implications for anesthesia and pain relief. Photomed Laser Surg. (2016) 34:599–609. doi: 10.1089/pho.2015.4048
15. Chon T, Mallory M, Yang J, Bublitz S, Do A, Dorsher P. Laser acupuncture: a concise review. Med Acupunct. (2019) 31:164–8. doi: 10.1089/acu.2019.1343
16. Yousefi-Nooraie R, Schonstein E, Heidari K, Rashidian A, Pennick V, Akbari-Kamrani M, et al. Low level laser therapy for nonspecific low-back pain. Cochrane Database Syst Rev. (2008) 2:CD005107. doi: 10.1002/14651858.CD005107.pub4
17. Huang Z, Ma J, Chen J, Shen B, Pei F, Kraus V. The effectiveness of low-level laser therapy for nonspecific chronic low back pain: a systematic review and meta-analysis. Arthritis Res Ther. (2015) 17:360. doi: 10.1186/s13075-015-0882-0
18. Yeum H, Hong Y, Nam D. Low-level laser therapy including laser acupuncture for non-specific chronic low back pain: systematic review and meta-analysis. J Acupunct Res. (2021) 38:8–19. doi: 10.13045/jar.2020.00283
19. Glazov G, Yelland M, Emery J. Low-level laser therapy for chronic non-specific low back pain: a meta-analysis of randomised controlled trials. Acupunct Med. (2016) 34:328–41. doi: 10.1136/acupmed-2015-011036
20. Kim J, Na C, Park G, Lee J. Effects of different wavelengths of invasive laser acupuncture on chronic non-specific low back pain: a study protocol for a pilot randomized controlled trial. Trials. (2021) 22:118. doi: 10.1186/s13063-021-05038-6
21. Kim J, Na C, Cho M, Park G, Lee J. Efficacy of invasive laser acupuncture in treating chronic non-specific low back pain: a randomized controlled trial. PLoS One. (2022) 17:e0269282. doi: 10.1371/journal.pone.0269282
22. Chan A, Tetzlaff J, Altman D, Laupacis A, Gøtzsche P, Krleža-Jerić K, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. (2013) 158:200–7. doi: 10.7326/0003-4819-158-3-201302050-00583
23. Boonstra A, Schiphorst Preuper H, Balk G, Stewart R. Cut-off points for mild, moderate, and severe pain on the visual analogue scale for pain in patients with chronic musculoskeletal pain. Pain. (2014) 155:2545–50. doi: 10.1016/j.pain.2014.09.014
24. Park K, Jaekal E, Yoon S, Lee S, Choi K. Diagnostic utility and psychometric properties of the Beck Depression Inventory – II Among Korean adults. Front Psychol. (2019) 10:2934. doi: 10.3389/fpsyg.2019.02934
25. Glazov G, Yelland M, Emery J. Low-dose laser acupuncture for non-specific chronic low back pain: a double-blind randomised controlled trial. Acupunct Med. (2014) 32:116–23. doi: 10.1136/acupmed-2013-010456
26. Shin J, Ku B, Kim J, Lee Y, Kang J, Heo H, et al. Short-term effect of laser acupuncture on lower back pain: a randomized, placebo-controlled, double-blind trial. Evid Based Complement Alternat Med. (2015) 2015:808425. doi: 10.1155/2015/808425
27. Simon L, Evans C, Katz N, Bombardier C, West C, Robbins J, et al. Preliminary development of a responder index for chronic low back pain. J Rheumatol. (2007) 34:1386–91.
28. Gilligan C, Volschenk W, Russo M, Green M, Gilmore C, Mehta V, et al. An implantable restorative-neurostimulator for refractory mechanical chronic low back pain: a randomized sham-controlled clinical trial. Pain. (2021) 162:2486–98. doi: 10.1097/j.pain.0000000000002258
29. Huskisson E. Measurement of pain. J Rheumatol. (1982) 9:768–9. doi: 10.1016/S0140-6736(74)90884-8
30. Chiarotto A, Maxwell L, Ostelo R, Boers M, Tugwell P, Terwee C. Measurement properties of visual analogue scale, numeric rating scale, and pain severity subscale of the brief pain inventory in patients with low back pain: a systematic review. J Pain. (2019) 20:245–63. doi: 10.1016/j.jpain.2018.07.009
31. Kim M, Cho Y, Uhm W, Kim S, Bae S. Cross-cultural adaptation and validation of the Korean version of the EQ-5D in patients with rheumatic diseases. Qual Life Res. (2005) 14:1401–6. doi: 10.1007/s11136-004-5681-z
32. Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. (2011) 20:1727–36. doi: 10.1007/s11136-011-9903-x
33. Fairbank J, Pynsent P. The Oswestry disability index. Spine. (2000) 25:2940–52. doi: 10.1097/00007632-200011150-00017
34. Jeon C, Kim D, Kim S, Kim D, Lee H, Park H. Validation in the cross-cultural adaptation of the Korean version of the Oswestry Disability Index. J Korean Med Sci. (2006) 21:1092–7. doi: 10.3346/jkms.2006.21.6.1092
35. Law D, McDonough S, Bleakley C, Baxter G, Tumilty S. Laser acupuncture for treating musculoskeletal pain: a systematic review with meta-analysis. J Acupunct Meridian Stud. (2015) 8:2–16. doi: 10.1016/j.jams.2014.06.015
36. Froud R, Patel S, Rajendran D, Bright P, Bjørkli T, Buchbinder R, et al. A systematic review of outcome measures use, analytical approaches, reporting methods, and publication volume by year in low back pain trials published between 1980 and 2012: respice, adspice, et prospice. PLoS One. (2016) 11:e0164573. doi: 10.1371/journal.pone.0164573
37. Chiarotto A, Deyo R, Terwee C, Boers M, Buchbinder R, Corbin T, et al. Core outcome domains for clinical trials in non-specific low back pain. Eur Spine J. (2015) 24:1127–42. doi: 10.1007/s00586-015-3892-3
Keywords: safety, efficacy, non-specific chronic low back pain, study protocol, randomized controlled trial, laser acupuncture
Citation: Kim J-H, Yang C, Yoo J, Park G-C, Kang B-K, Kim A-R, Kim J, Nam D and Hong Y (2023) Safety and efficacy of 650 nm invasive laser acupuncture on non-specific chronic low back pain: A protocol for a multicenter randomized placebo-controlled trial. Front. Med. 10:1021255. doi: 10.3389/fmed.2023.1021255
Received: 17 August 2022; Accepted: 27 January 2023;
Published: 09 February 2023.
Edited by:
Jian Kong, Massachusetts General Hospital and Harvard Medical School, United StatesReviewed by:
Shuxing Wang, Foshan University, ChinaCopyright © 2023 Kim, Yang, Yoo, Park, Kang, Kim, Kim, Nam and Hong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jae-Hong Kim,  bmFob25nYUBoYW5tYWlsLm5ldA==
bmFob25nYUBoYW5tYWlsLm5ldA==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.