 Désirée Tampe
Désirée Tampe Eva Baier
Eva Baier Samy Hakroush
Samy Hakroush Björn Tampe
Björn Tampe
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Med. , 20 July 2023
Sec. Nephrology
Volume 10 - 2023 | https://doi.org/10.3389/fmed.2023.1020691
This article is part of the Research Topic Nephrotoxicity of Immune Checkpoint Inhibitors View all 6 articles
Background: Immune checkpoint inhibitors (ICIs) are novel drugs targeting programmed cell death protein 1-ligand 1 (PD-L1) or its receptor (PD-1). Enhancing the immune system has also been associated with a wide range of immune-related adverse events (irAE). Among them, acute interstitial nephritis (AIN) is a rare but deleterious irAE in the kidney. However, determinants of recovery and long-term kidney function after ICI withdrawal and steroid therapy thereafter remain elusive. Therefore, we here aimed to identify parameters associated with recovery of kidney function in this previous established cohort of AIN in the context of ICI therapy.
Methods: We here monitored kidney function over a mean follow-up time of 812 days in comparison with clinical, histopathological and laboratory parameters associated with recovery of kidney function after AIN related to ICI nephrotoxicity.
Results: Abundance of intrarenal PD-L1/PD-1 did not correlate with recovery of kidney function. Furthermore, cumulative steroid dose that was initiated for treatment of AIN related to ICI nephrotoxicity was also not associated with improvement of kidney function. Finally, chronic lesions in the kidney including glomerular sclerosis and interstitial fibrosis/tubular atrophy (IF/TA) did not correlate with eGFR change during the follow-up time. However, we here identified that lower levels of serum sodium at time of kidney biopsy were the strongest independent predictor of renal recovery in ICI-related nephrotoxicity.
Conclusion: Because low serum sodium levels associated with better improvement of kidney function, these observations might contribute to novel approaches to enhance recovery after AIN related to ICI nephrotoxicity.
Immune checkpoint inhibitors (ICIs) are novel drugs targeting programmed cell death protein 1-ligand 1 (PD-L1, synonym CD274, B7 homolog 1) or its receptor (PD-1, synonym CD 279), and are increasingly used in cancer therapy (1). Allowing T cells to remain an activated state by blocking negative co-stimulatory pathways, ICIs enhance the anti-tumoral immune response. However, enhancing the immune system has also been associated with a wide range of immune-related adverse events (irAE) (2). Among them, acute interstitial nephritis (AIN) is a rare but severe irAE in the kidney and the most common biopsy-proven diagnosis in ICI-related nephrotoxicity (3, 4). We have recently characterized abundance of PD-L1 and its receptor PD-1 in a cohort of biopsy-proven AIN related to nephrotoxicity of ICI therapy presenting with acute kidney injury (AKI) (5). While glomerular PD-L1 correlated with kidney function and interstitial cell PD-1 positivity specifically with severity of kidney injury, determinants of long-term kidney function after ICI withdrawal and steroid therapy thereafter remain elusive (5). Therefore, we here aimed to identify parameters associated with recovery of kidney function in this previous established cohort of AIN in the context of ICI therapy by monitoring of long-term kidney function (5).
A total number of 6 cases with biopsy-proven AIN related to nephrotoxicity of ICI therapy with a long-term follow-up were retrospectively included between 2015 to 2020 at the University Medical Center Göttingen, Germany (Table 1). The patient cohort has previously been described (5, 6). The studies involving human participants were reviewed and approved by the Institutional Review Board of the University Medical Center Göttingen, Germany (no. 22/2/14). The patients/participants provided their written informed consent for the use of routinely collected data for research purposes as part of their regular medical care in the contract of the University Medical Center Göttingen. Medical records were used to obtain data on age, sex, medication, date of biopsy, laboratory results and urinary analysis. At the time of kidney biopsy, 3/6 (50%) of patients received a proton pump inhibitor (PPI), and none a non-steroidal anti-inflammatory drug (NSAR) or antibiotic (Table 1). For assessment of kidney function recovery, difference between worst estimated glomerular filtration rate (eGFR) at time of kidney biopsy and last documented eGFR during follow-up was calculated. The mean follow-up time was 812 days, and 5/6 (83.3%) of patients showed improvement of kidney function (Table 1).
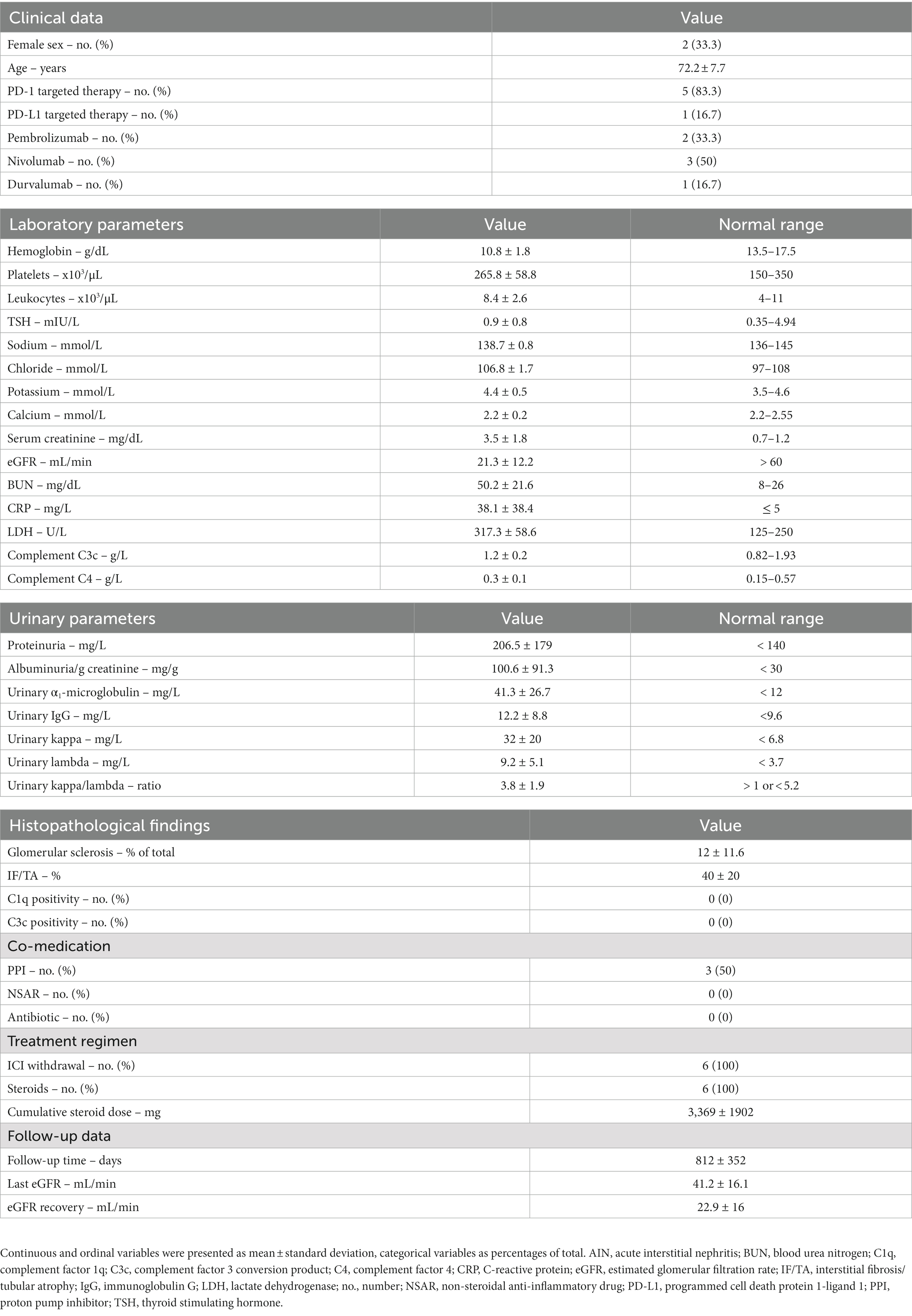
Table 1. Clinical, laboratory, and histopathological parameters of the total cohort.
A renal pathologist evaluated the kidney biopsies and was blinded to clinical data. After deparaffinization in xylene and rehydration in ethanol containing distilled water, formalin-fixed, paraffin-embedded kidney sections were stained using primary antibodies against PD-L1 (1:100, ab205921, Abcam, Cambridge, UK), PD-1 (1:500, ab52587, Abcam, Cambridge, UK), C1q (1:30,000, A0136, Agilent Dako, Santa Clara, USA), and C3c (1:10,000, A0062, Agilent Dako, Santa Clara, USA), labeling was performed using Novolink™ Polymer Detection System (Leica Biosystems, Wetzlar, Germany) according to the manufacturer’s protocol. Nuclear counterstain was performed by using Mayer’s Hematoxylin Solution (Sigma, St. Louis, USA). As previously described, the intensity of PD-L1 staining was evaluated at 400x magnification and scored semiquantitatively (0: no staining, 1: weak and segmental staining, 2: moderate staining, 3: strong staining). Interstitial cells positive for PD-1 were evaluated by using mean values of 10 randomly selected cortical visual fields at 400x magnification and scored semiquantitative (0, no cell per visual field, 1: 1–3 cells per visual field, 2: 3–6 cells per visual field, 3: >6 cells per visual field) (5).
Plasma concentrations of human complement components C3c (9D9621, Abbott, Chicago, USA) and C4 (9D9721, Abbott, Chicago, USA) were determined by turbidimetric measurements on the ARCHITECT-C module.
Variables were tested for normal distribution using the Shapiro–Wilk test. Statistical comparisons were not formally powered or prespecified. Continuous and ordinal variables were presented as mean ± standard deviation, categorical variables as percentages of total. Spearman’s correlation was performed to assess correlations and heatmaps reflect the mean values of Spearman’s ρ. A Spearman’s ρ more than ±0.9 in the correlation matrix was defined as relevant indicated by rectangle boxes, and independent statistical evaluation of these parameters was performed by multiple linear regression. A probability (p) value of <0.05 was considered statistically significant. Data analyses were performed with GraphPad Prism (version 8.4.3 for MacOS, GraphPad Software, San Diego, California, USA), regression analyses were performed using IBM SPSS Statistics (version 27 for MacOS, IBM Corporation, Armonk, NY, USA).
We included a total number of 6 kidney specimens with ICI-related nephrotoxicity (5 cases with ICI therapy targeting PD-1 and 1 targeting PD-L1, Table 1). In all cases, ICI treatment was discontinued, and steroids were initiated (Table 1). The mean follow-up time was 812 days, and 5/6 (83.3%) of patients showed improvement of kidney function (Figure 1A). Based on our previous observations that intrarenal PD-L1 and PD-1 positivity was associated with kidney injury, we first analyzed its association with renal recovery in this cohort (5). Abundance of intrarenal PD-L1/PD-1 did not correlate with recovery of kidney function (Figure 1B). Furthermore, cumulative steroid dose that was initiated for treatment of AIN related to ICI nephrotoxicity was also not associated with improvement of kidney function (Figure 1B). Finally, chronic lesions in the kidney including glomerular sclerosis and interstitial fibrosis/tubular atrophy (IF/TA) did not correlate with eGFR change during the follow-up time (Figure 1B). We next analyzed recovery of kidney function in association with clinical and laboratory parameters at time of kidney biopsy. Platelet counts were positively associated with eGFR recovery (Spearman’s ρ = 0.9276), and sodium levels negatively with recovery of kidney function (Spearman’s ρ = −0.9258, Figure 2A). These observations were confirmed by simple linear regression analysis for platelet counts (p = 0.0082) and serum sodium levels (p = 0.0056, Figure 2B). As confirmed by multiple regression analysis comparing the association between eGFR recovery and identified parameters, lower levels of serum sodium at time of kidney biopsy were the strongest independent predictor of renal recovery in ICI-related nephrotoxicity (Table 2). In summary, lower serum sodium levels correlated with recovery of kidney function after AIN related to ICI nephrotoxicity independent of histopathological lesions or cumulative steroid dose.
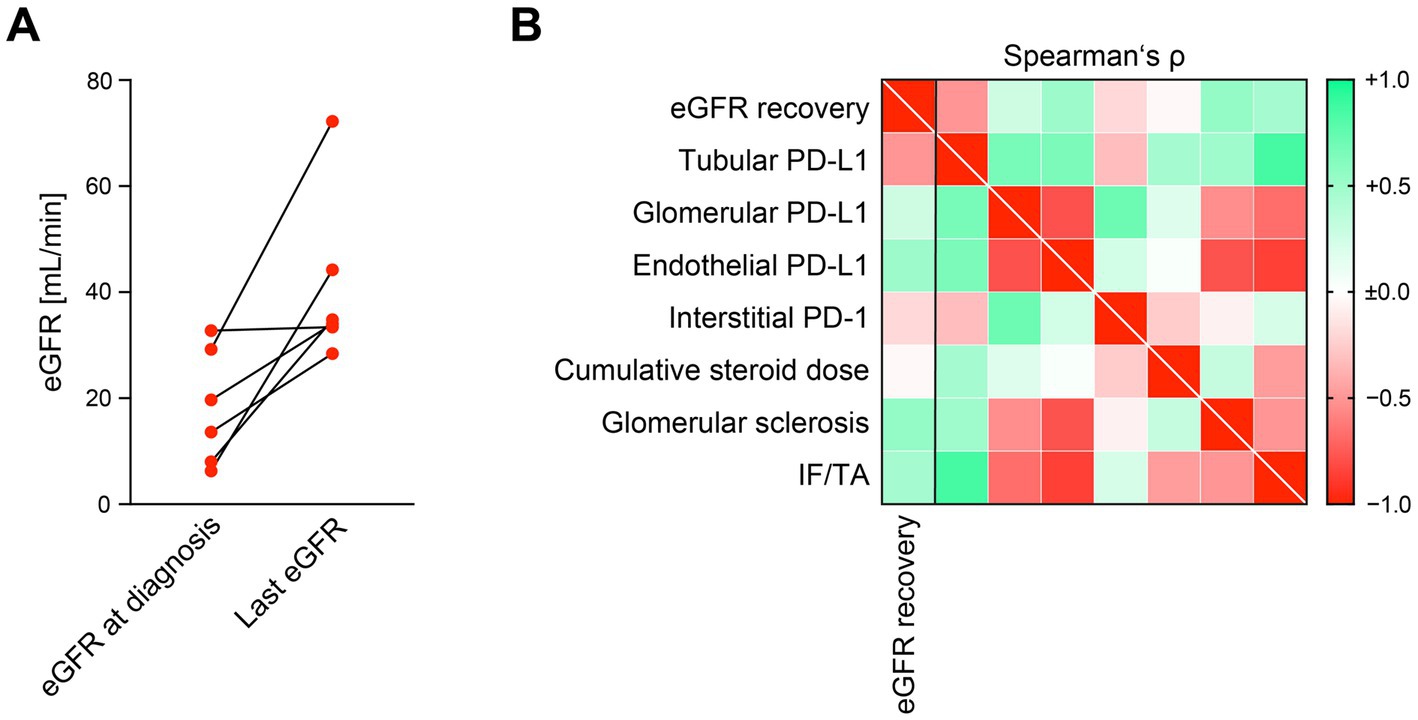
Figure 1. Histopathological lesions or cumulative steroid dose do not affect renal recovery after AIN related to ICI nephrotoxicity. (A) Difference between worst eGFR at time of diagnosis and last documented eGFR during follow-up in the patient cohort are shown. (B) Intensity of PD-L1/PD-1 positivity within different renal compartments, cumulative steroid dose and histopathological findings in association with eGFR recovery in AIN related to ICI nephrotoxicity are shown by heatmap reflecting mean values of Spearman’s ρ. AIN, acute interstitial nephritis; eGFR, estimated glomerular filtration rate (CKD-EPI); ICI, immune checkpoint inhibitor; IF/TA, interstitial fibrosis/tubular atrophy; PD-1, programmed cell death protein 1; PD-L1, programmed cell death protein 1-ligand 1.
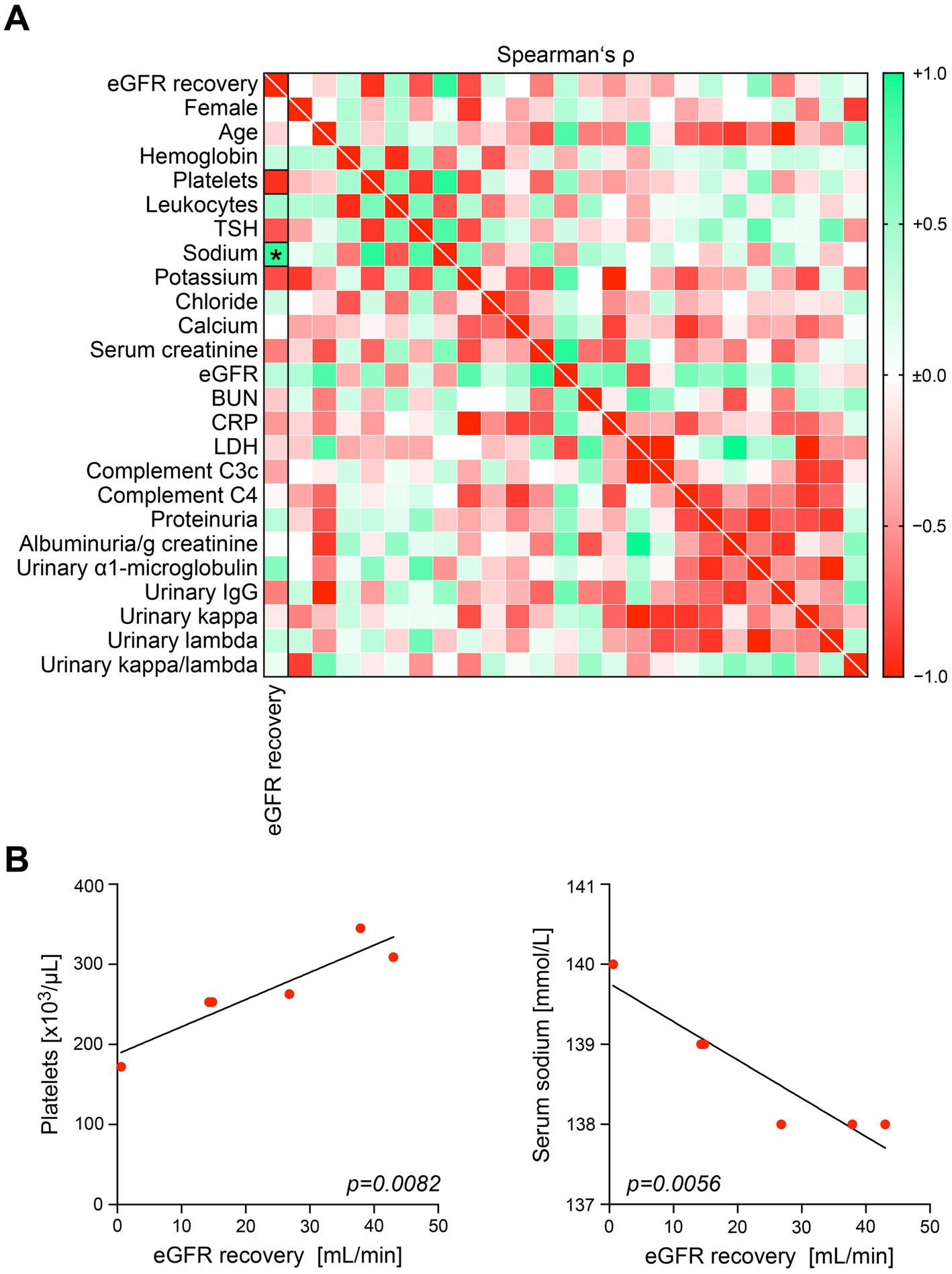
Figure 2. Lower serum sodium levels correlate with recovery of kidney function after AIN related to ICI nephrotoxicity. (A) Recovery of eGFR during follow-up in association with clinical and laboratory parameters are shown by heatmap reflecting mean values of Spearman’s ρ. Rectangle boxes indicate a Spearman’s ρ more than ±0.9, the asterisk a significant correlation in the stepwise linear regression analysis (p < 0.05). (B) Simple linear regression analysis for platelet counts and serum sodium levels in association with eGFR recovery in the patient cohort. AIN, acute interstitial nephritis; BUN, blood urea nitrogen; C3c, complement factor 3 conversion product; C4, complement factor 4; CRP, C-reactive protein; eGFR, estimated glomerular filtration rate; ICI, immune checkpoint inhibitor; IgG, immunoglobulin G; LDH, lactate dehydrogenase; TSH, thyroid stimulating hormone.

Table 2. Multiple linear regression analyses correlating with eGFR recovery.
We have recently characterized abundance of PD-L1 and its receptor PD-1 in a cohort of biopsy-proven AIN related to nephrotoxicity of ICI therapy presenting with acute kidney injury (AKI) (5). While glomerular PD-L1 correlated with kidney function and interstitial cell PD-1 positivity specifically with severity of kidney injury, determinants of long-term kidney function after ICI withdrawal and steroid therapy thereafter remain elusive (5). Therefore, we here monitored kidney function over a mean follow-up time of 812 days and identified higher platelet counts and low serum sodium levels to be associated with improved renal recovery after AIN related to ICI nephrotoxicity. An inverse correlation between platelet counts and serum sodium levels has already been described, and we here confirm that serum sodium at time of kidney biopsy was the strongest independent predictor of renal recovery in ICI-related nephrotoxicity (7). Higher dietary salt consumption in populations with chronic kidney disease (CKD) has already been associated with proteinuria as independent risk factors for CKD progression (8). While it has been proposed that small increases in serum sodium levels are of importance, the mechanisms underlying these adverse effects of sodium are incompletely understood (9, 10). Besides effects attributed to altered blood pressure affected by serum sodium, there is in vitro evidence that small increases in sodium concentrations directly impact endothelial cell homeostasis by damage to the glycocalyx layer and inhibition of nitric oxide release (11, 12). Furthermore, increased sodium concentrations have also been shown to enhance transcription induction of pro-fibrotic mediators including transforming growth factor-beta 1 (TGF-β1), associated with progressive CKD (13). Interestingly, it has recently been shown that a 5 mmol/L increase in baseline serum sodium was associated with an eGFR loss of 7.4 mL/min over 6 years in a population with established CKD (14). These findings support that serum sodium levels within the normal range are a risk factor for CKD progression. Consistent to that, we here identified low levels of serum sodium within the normal range associated with renal recovery after AIN related to ICI nephrotoxicity. These observations require further confirmation in independent cohorts, and restriction of salt consumption to lower serum sodium levels after AIN related to ICI nephrotoxicity would be an attractive therapeutical intervention as it has also been shown in multiple trials including CKD patients (15–21).
This study has several limitations due to the small patient number, its retrospective design, and no independent validation. Moreover, urinary sodium levels were not measured but would be of interest regarding urinary sodium excretion. However, nephrotoxicity related to ICI therapy is a rare event with only a limited number of kidney biopsies (22–24). Our observations that low serum sodium levels to be associated with better improvement of kidney function might contribute to novel approaches to enhance recovery after AIN related to ICI nephrotoxicity.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by the Ethics Committee of the University Medical Center Göttingen. The patients/participants provided their written informed consent to participate in this study.
BT conceived the study, collected and analyzed data, and wrote the first draft. DT and EB collected and analyzed data. SH evaluated all kidney biopsies. All authors contributed to the article and approved the submitted version.
BT was supported by the Research program, University Medical Center Göttingen (1403720). EB was funded by the Else-Kröner research program entitled “molecular therapy and prediction of gastrointestinal malignancies” (7-67-1840876). The authors also acknowledge support by the Open Access Publication Funds of the Göttingen University. The funding sources were not involved in the design, collection, analysis, interpretation, writing or decision to submit the article.
The authors thank Katrin Schwarze, Ulrike Ehbrecht, Charlotta Tegeler and Sabrina Becker for technical assistance.
Author SH was employed by company SYNLAB Holding Germany.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Gill, J, and Prasad, V. A reality check of the accelerated approval of immune-checkpoint inhibitors. Nat Rev Clin Oncol. (2019) 16:656–8. doi: 10.1038/s41571-019-0260-y
2. Postow, MA, Sidlow, R, and Hellmann, MD. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med. (2018) 378:158–68. doi: 10.1056/NEJMra1703481
3. Hu, F, Zhai, Y, Yuan, L, Liang, J, Xu, J, Guo, X, et al. Renal toxicities in immune checkpoint inhibitors with or without chemotherapy: an observational, retrospective, pharmacovigilance study leveraging US FARES database. Cancer Med. (2021) 10:8754–62. doi: 10.1002/cam4.4343
4. Cassol, C, Satoskar, A, Lozanski, G, Rovin, B, Hebert, L, Nadasdy, T, et al. Anti-PD-1 immunotherapy may induce interstitial nephritis with increased tubular epithelial expression of PD-L1. Kidney Int Rep. (2019) 4:1152–60. doi: 10.1016/j.ekir.2019.06.001
5. Tampe, D, Kopp, SB, Baier, E, Hakroush, S, and Tampe, B. Compartmentalization of intrarenal programmed cell death protein 1-ligand 1 and its receptor in kidney injury related to immune checkpoint inhibitor nephrotoxicity. Front Med (Lausanne). (2022) 9:902256. doi: 10.3389/fmed.2022.902256
6. Hakroush, S, Kopp, SB, Tampe, D, Gersmann, AK, Korsten, P, Zeisberg, M, et al. Variable expression of programmed cell death protein 1-ligand 1 in kidneys independent of immune checkpoint inhibition. Front Immunol. (2020) 11:624547. doi: 10.3389/fimmu.2020.624547
7. Kjeldsen, SE, Westheim, A, Lande, K, Gjesdal, K, Leren, P, Enger, E, et al. Sodium depletion increases platelet and plasma catecholamines in hypertensive men. Hypertension. (1988) 11:477–82. doi: 10.1161/01.HYP.11.5.477
8. McMahon, EJ, Campbell, KL, Bauer, JD, Mudge, DW, and Kelly, JT. Altered dietary salt intake for people with chronic kidney disease. Cochrane Database Syst Rev. (2021) 2021:CD010070. doi: 10.1002/14651858.CD010070.pub3
9. de Wardener, HE, He, FJ, and MacGregor, GA. Plasma sodium and hypertension. Kidney Int. (2004) 66:2454–66. doi: 10.1111/j.1523-1755.2004.66018.x
10. He, FJ, Markandu, ND, Sagnella, GA, de Wardener, HE, and MacGregor, GA. Plasma sodium: ignored and underestimated. Hypertension. (2005) 45:98–102. doi: 10.1161/01.HYP.0000149431.79450.a2
11. Oberleithner, H, Riethmuller, C, Schillers, H, MacGregor, GA, de Wardener, HE, and Hausberg, M. Plasma sodium stiffens vascular endothelium and reduces nitric oxide release. Proc Natl Acad Sci U S A. (2007) 104:16281–6. doi: 10.1073/pnas.0707791104
12. Oberleithner, H, Peters, W, Kusche-Vihrog, K, Korte, S, Schillers, H, Kliche, K, et al. Salt overload damages the glycocalyx sodium barrier of vascular endothelium. Pflugers Arch. (2011) 462:519–28. doi: 10.1007/s00424-011-0999-1
13. August, P, and Suthanthiran, M. Transforming growth factor beta and progression of renal disease. Kidney Int Suppl. (2003) 64:S99–S104. doi: 10.1046/j.1523-1755.64.s87.15.x
14. Cole, NI, Suckling, RJ, Desilva, V, He, FJ, MacGregor, GA, and Swift, PA. Serum sodium concentration and the progression of established chronic kidney disease. J Nephrol. (2019) 32:259–64. doi: 10.1007/s40620-018-0541-z
15. He, J, Mills, KT, Appel, LJ, Yang, W, Chen, J, Lee, BT, et al. Urinary sodium and potassium excretion and CKD progression. J Am Soc Nephrol. (2016) 27:1202–12. doi: 10.1681/ASN.2015010022
16. Vegter, S, Perna, A, Postma, MJ, Navis, G, Remuzzi, G, and Ruggenenti, P. Sodium intake, ACE inhibition, and progression to ESRD. J Am Soc Nephrol. (2012) 23:165–73. doi: 10.1681/ASN.2011040430
17. Fan, L, Tighiouart, H, Levey, AS, Beck, GJ, and Sarnak, MJ. Urinary sodium excretion and kidney failure in nondiabetic chronic kidney disease. Kidney Int. (2014) 86:582–8. doi: 10.1038/ki.2014.59
18. Smyth, A, Dunkler, D, Gao, P, Teo, KK, Yusuf, S, O'Donnell, MJ, et al. The relationship between estimated sodium and potassium excretion and subsequent renal outcomes. Kidney Int. (2014) 86:1205–12. doi: 10.1038/ki.2014.214
19. Lambers Heerspink, HJ, Holtkamp, FA, Parving, HH, Navis, GJ, Lewis, JB, Ritz, E, et al. Moderation of dietary sodium potentiates the renal and cardiovascular protective effects of angiotensin receptor blockers. Kidney Int. (2012) 82:330–7. doi: 10.1038/ki.2012.74
20. Thomas, MC, Moran, J, Forsblom, C, Harjutsalo, V, Thorn, L, Ahola, A, et al. The association between dietary sodium intake, ESRD, and all-cause mortality in patients with type 1 diabetes. Diabetes Care. (2011) 34:861–6. doi: 10.2337/dc10-1722
21. Torres, VE, Abebe, KZ, Schrier, RW, Perrone, RD, Chapman, AB, Yu, AS, et al. Dietary salt restriction is beneficial to the management of autosomal dominant polycystic kidney disease. Kidney Int. (2017) 91:493–500. doi: 10.1016/j.kint.2016.10.018
22. Manohar, S, Kompotiatis, P, Thongprayoon, C, Cheungpasitporn, W, Herrmann, J, and Herrmann, SM. Programmed cell death protein 1 inhibitor treatment is associated with acute kidney injury and hypocalcemia: meta-analysis. Nephrol Dial Transplant. (2019) 34:108–17. doi: 10.1093/ndt/gfy105
23. Seethapathy, H, Zhao, S, Strohbehn, IA, Lee, M, Chute, DF, Bates, H, et al. Incidence and clinical features of immune-related acute kidney injury in patients receiving programmed cell death Ligand-1 inhibitors. Kidney Int Rep. (2020) 5:1700–5. doi: 10.1016/j.ekir.2020.07.011
Keywords: PD-L1, PD-1, checkpoint inhibition, kidney injury, kidney function recovery, serum sodium
Citation: Tampe D, Baier E, Hakroush S and Tampe B (2023) Serum sodium levels associate with recovery of kidney function in immune checkpoint inhibitor nephrotoxicity. Front. Med. 10:1020691. doi: 10.3389/fmed.2023.1020691
Edited by:
Alain Le Moine, Université libre de Bruxelles, BelgiumCopyright © 2023 Tampe, Baier, Hakroush and Tampe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Björn Tampe, YmpvZXJuLnRhbXBlQG1lZC51bmktZ29ldHRpbmdlbi5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.