 Diana Morales-Jadán1,2Alexander Paolo Vallejo-Janeta1,2Vanessa Bastidas2Maria Belen Paredes-Espinosa2Byron Freire-Paspuel2Ismar Rivera-Olivero1Esteban Ortiz-Prado1,3Aquiles Rodrigo Henriquez-Trujillo1Tannya Lozada2 the UDLA COVID-19 Team
Diana Morales-Jadán1,2Alexander Paolo Vallejo-Janeta1,2Vanessa Bastidas2Maria Belen Paredes-Espinosa2Byron Freire-Paspuel2Ismar Rivera-Olivero1Esteban Ortiz-Prado1,3Aquiles Rodrigo Henriquez-Trujillo1Tannya Lozada2 the UDLA COVID-19 Team Miguel Angel Garcia-Bereguiain1,3*
Miguel Angel Garcia-Bereguiain1,3*- 1One Health Research Group, Universidad de las Américas, Quito, Ecuador
- 2“UDLA COVID-19 Team, ” Universidad de Las Américas, Quito, Ecuador
- 3Universidad Latina de Costa Rica, San José, Costa Rica
Background: Neglected indigenous groups and underserved rural populations in Latin America are highly vulnerable to COVID-19 due to poor health infrastructure and limited access to SARS-CoV-2 diagnosis. The Andean region in Ecuador includes a large number of isolated rural mestizo and indigenous communities living under poverty conditions.
Objective: We herein present a retrospective analysis of the surveillance SARS-CoV-2 testing in community-dwelling populations from four provinces in the Ecuadorian Andes, carried out during the first weeks after the national lockdown was lifted in June 2020.
Results: A total number of 1,021 people were tested for SARS-CoV-2 by RT-qPCR, resulting in an overall high infection rate of 26.2% (268/1,021, 95% CI: 23.6–29%), which was over 50% in several communities. Interestingly, community-dwelling super spreaders with viral loads over 108 copies/mL represented 7.46% (20/268, 95% CI: 4.8–11.1%) of the SARS-CoV-2 infected population.
Conclusion: These results support that COVID-19 community transmission in rural communities from the Andean region was happening at the early stages of the COVID-19 pandemic in Ecuador and point out the weakness of the COVID-19 control program. Community-dwelling individuals in neglected rural and indigenous communities should be considered for a successful control and surveillance program in future pandemics in low- and middle-income countries.
Introduction
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was first reported in China in December 2019 and spread worldwide, causing the COVID-19 pandemic (1). A few weeks after the initial outbreaks, the first COVID-19 cases were reported in Latin America that has since then been deeply affected. For instance, the first case of COVID-19 was confirmed on 29 February 2020 in Ecuador (2), and during the first year of the COVID-19 pandemic, more than 400,000 COVID-19 cases and 20,000 COVID-19-related deaths have been reported by Ecuadorian public health authorities (3).
Vulnerable groups infected with COVID-19 include not only the elderly and individuals with comorbidities but also historically neglected indigenous populations (4–9). There are more than 476 million indigenous people in the world, highly represented and traditionally neglected in Latin America (10, 11). In Ecuador, indigenous people represent more than 7% of the total population and are mainly associated with underserved rural communities (10–13). Those communities are usually isolated or poorly communicated and have poor access to health services. In many cases, such health services have little capacity and limited coverage, which may delay seeking medical attention, complicating early management, and therefore leading to greater risks of complications and mortality under a scenario such as the COVID-19 pandemic (7–9, 13).
From the early stages of the COVID-19 pandemic, there was a call for action to protect indigenous people from the Americas (7–9). In Ecuador, The National Council for the Equality of Peoples and Nationalities has demanded the protection of indigenous people, reporting COVID-19 outbreaks among their communities and claiming support from public health authorities to contain the pandemic in their communities (8, 11). Moreover, several reports have already shown dramatic SARS-CoV-2 outbreaks leading to community transmission in rural and indigenous populations from the Amazonian and Coastal regions of Ecuador (7, 8, 14–19). Under this scenario, following the request from community leaders, we carried out a SARS-CoV-2 surveillance testing among community-dwelling indigenous and mestizo people in the Ecuadorian Andes few weeks after the population lockdown was lifted in June 2020.
This study aimed to carry out a retrospective analysis of the results of our SARS-CoV-2 testing surveillance in mestizo and indigenous communities from the Ecuadorian Andes to show that COVID-19 community transmission had been happening since the early stages of the pandemic.
Materials and methods
Study design and setting
We carried out a retrospective analysis of the data collected from this cross-sectional surveillance to describe the attack rates of SARS-CoV-2 infection among rural indigenous and mestizo communities from the Andean region of Ecuador from June to August 2020. The communities were selected by local public health authorities and community leaders at convenience, using the inclusion criteria of an individual for each household. No random selection of individuals was carried out, so potential bias associated with the sampling cannot be ruled out.
A total of 1,021 community-dwelling individuals were recruited. The communities included in this study belong to the provinces of Chimborazo (communities Lizarzaburu, San Juan, and San Luis at canton Riobamba; community Columbe at canton Colta; and community Penipe at canton Penipe), Tungurahua (communities Benitez, Huambaló, Pelileo, and Salasaca at canton Pelileo), Bolivar (communities Facundo Vela, San Luis, Simiatug, Guaranda, and Veintimilla at canton Guaranda), and Napo (community Oyacachi at canton El Chaco); although Napo is included in the Amazonian provinces of Ecuador, the communities included in this study belong to the highlands area of this province.
In addition, the sociodemographic information was obtained from the official epidemiological record that is mandatory to submit to the local health authority and the Minister of Public Health (MoH) for each sample collected.
Sample collection, RNA extraction, and RT-qPCR for SARS-CoV-2 diagnosis using the CDC protocol
The samples were processed in the BSL2-certified molecular biology laboratory at Universidad de Las Americas. Nasopharyngeal swabs were collected on a 0.5-mL TE pH 8 buffer for SARS-CoV-2 diagnosis by RT-qPCR, following an adapted version of the CDC protocol as it has been previously described by our laboratory. In brief, the CDC RT-qPCR protocol is based on N1 and N2 probes to detect SARS-CoV-2 and RNase P as an RNA extraction quality control (20–28). In addition, negative controls (TE pH 8 buffer) were included as a control for carryover contamination, one for each set of RNA extractions, to guarantee that only true positives were reported. For viral loads calculation, the 2019-nCoV N positive control (IDT, USA) was used, provided at 200.000 genome equivalents/μL, and a factor of 200 was applied to convert the viral loads to genome equivalents/mL and then converted to a logarithmic scale.
Statistical analysis
For the statistical analysis of data, infection rates were calculated for each community and province, and also for sex and age group. To assess differences in the infection rates among communities, provinces, sex, or age group, a chi-square test for comparison of proportions was applied. All statistical analyses were carried out using SPSS Statistics 28 software.
Results
SARS-CoV-2 infection rates
A total of 1,021 indigenous and mestizo individuals from 15 rural communities distributed along four different provinces of the Ecuadorian Andes were tested for SARS-CoV-2 infection (Figure 1A). For Bolivar province, 334 individuals were recruited, distributed in five locations: Facundo Vela, San Luis, Simiatug, Guaranda, and Veintimilla. For Chimborazo province, 322 individuals were recruited, distributed in five locations: Lizarzaburu, San Juan, San Luis, Columbe, and Penipe. For Tungurahua province, 213 individuals were recruited, distributed in four locations: Benitez, Huambaló, Pelileo, and Salasaca. For Napo province, 152 individuals were recruited from the Oyacachi community. The distribution according to sex was 52.1% (532/1,021) male and 47.9% (489/1,021) female participants. The age distribution for the study population is presented in Figure 1B.
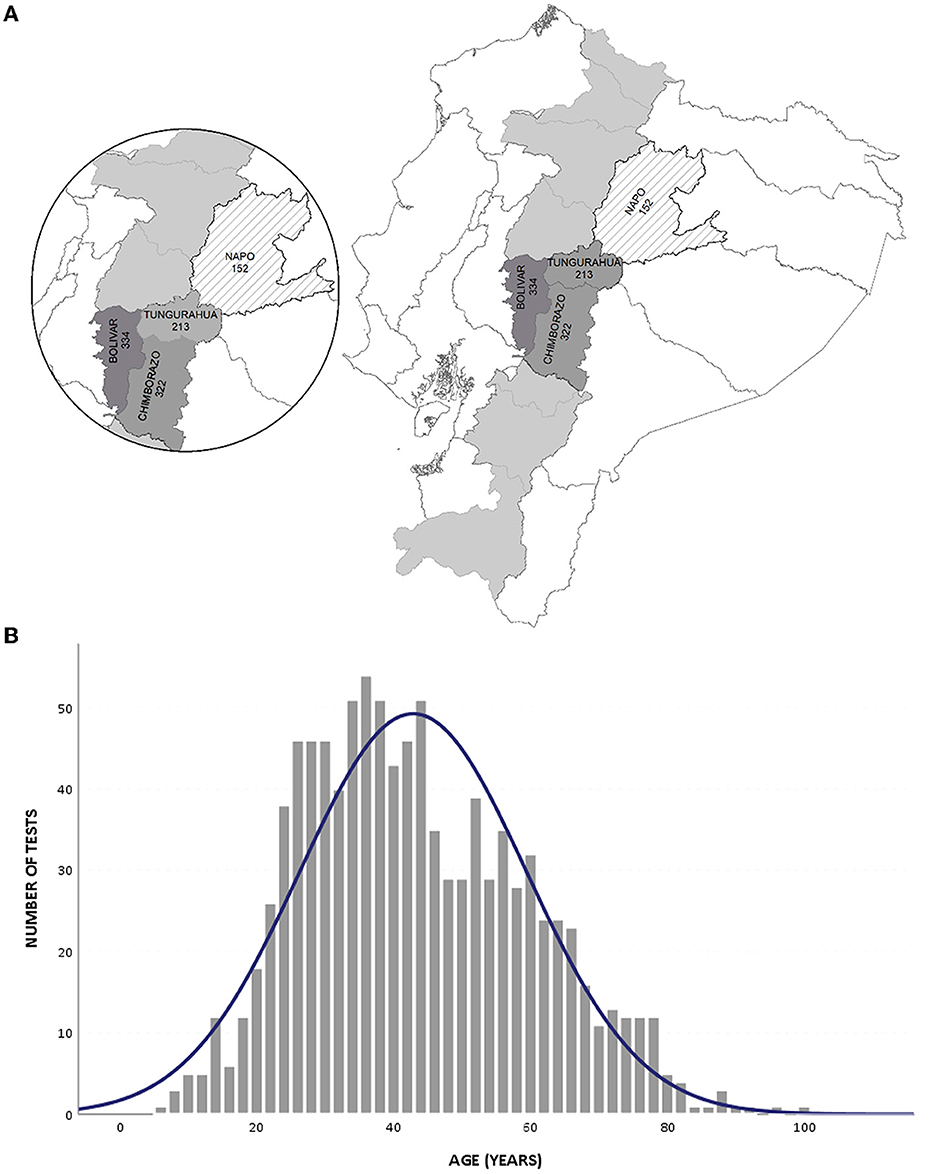
Figure 1. Study population. (A) Location of the provinces; the gray area indicates the Ecuadorian Andean region. (B) Distribution of tests according to the age of participants.
The overall SARS-CoV-2 infection rate was 26.2% (268/1,021, 95% CI: 23.6–29%), with 268 out of 1,021 participants testing positive. The distribution according to sex and age for the individuals infected with SARS-CoV-2 is presented in Table 1. There are no significant differences in the average SARS-CoV-2 infection rate between male and female participants (p > 0.05). However, there are significant differences between age groups (p < 0.05).
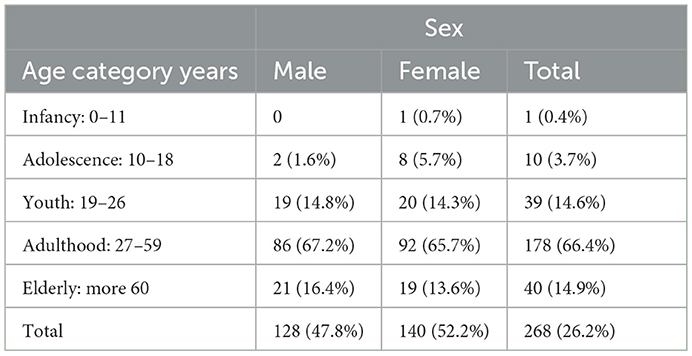
Table 1. SARS-CoV-2 infection rates (%) distribution according to sex and age.
The SARS-CoV-2 infection rates for each province, canton, and community are presented in Table 2. Tungurahua had the highest infection rate value of 139/213, 65.3% (95% IC 58.7–71.4%); followed by Napo with 58/152, 38.2% (95% IC: 30.7–46%); Chimborazo with 54/322, 16.77% (95% IC: 12–21.6%); and Bolivar with 17/334, 5.1% (95% IC: 3.1–7.8%). The SARS-CoV-2 infection rates for cantons comprised Guaranda 5.09% (17/334), Colta 12% (4/33), Penipe 20.6% (13/63), Riobamba 16.4% (37/226), El Chaco 38.2% (58/152), and Pelileo 65.3% (139/213). The SARS-CoV-2 infection rates for communities comprised Simiatug 7.9% (3/38), Veintimilla 7.4% (5/68), Guaranda 4.6% (8/175), San Luis 3.7% (1/27), Facundo 0% (0/26), Columbe 12% (4/33), Penipe 21% (13/63), San Juan 19 % (26/136), San Luis 13% (9/68), Lizarzaburu 9% (2/22), Oyacachi 38% (58/152), Huambaló 74% (58/78), Salasaca 68% (46/68), Benitez 64% (18/28), and Pelileo 44% (17/39). Significant differences were found between those values (p < 0.01).

Table 2. SARS-CoV-2 infection rates for each province, canton, and community included in this study.
SARS-CoV-2 viral loads
The distribution of SARS-CoV-2 viral loads according to sex and age is presented in Figure 2. No significant differences were found (p > 0.05). In addition, 20 individuals had viral SARS-CoV-2 load values of above 108 copies/mL belonging to the cantons of Penipe (3), Riobamba (5), El Chaco (7), and Pelileo (5). Those individuals represented 7.46% (20/268, 95% CI: 4.8–11.1%) of the individuals infected with SARS-CoV-2.
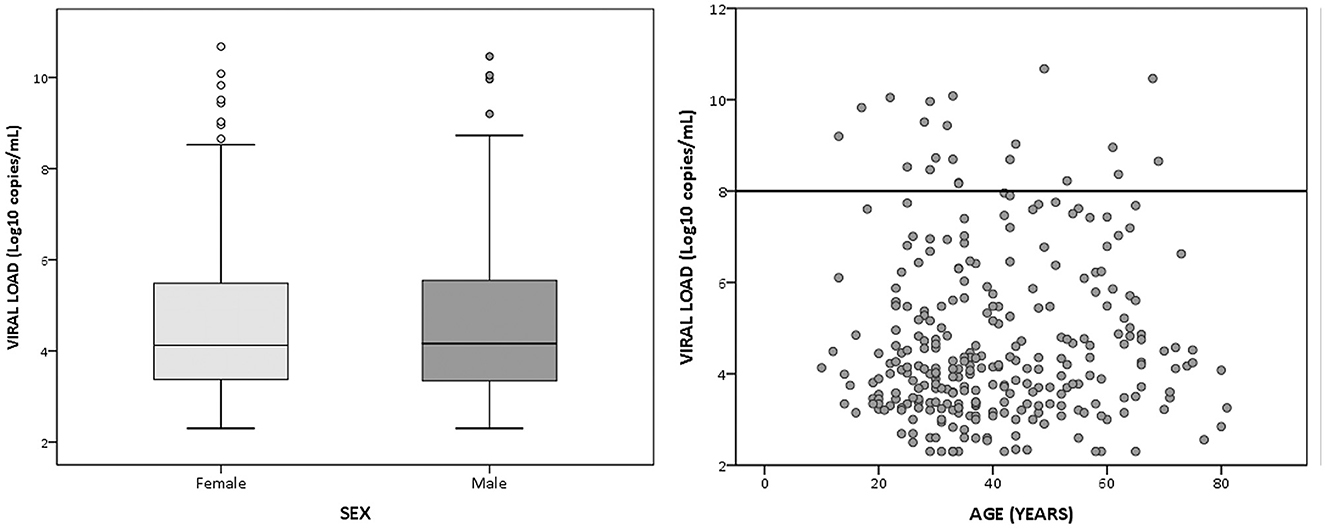
Figure 2. Distribution of SARS-CoV-2 viral loads according to sex and age in the study population. Viral load is represented in a log scale.
Discussion
Due to the retrospective nature of this study, there was not a randomized sample collection to include a statistically representative population sampling for these provinces in the Andean region. This is a strong limitation in our study, as the bias on sample collection could mean that the results obtained were not truly representative of the COVID-19 epidemiological context in this region but were limited to the communities selected. However, as the average SARS-CoV-2 infection rate was over 26% (peaking over 50% in several communities) and outbreaks were found at 14 out of 15 communities visited, our results would suggest that non-control COVID-19 community transmission had been happening among rural indigenous communities in the Andes just a few weeks since the national lockdown was lifted. It has been reported that the current health crisis caused by COVID-19 has further aggravated the conditions of vulnerability and social exclusion of indigenous populations in Latin America, and the Andean region would not be an exception (29–33). Similarly, severe COVID-19 outbreaks have been described for Amazonian indigenous people in Brazil and Ecuador (7–9) despite the supposed isolation of those ethnic groups, pointing out the high vulnerability to COVID-19 of those traditionally neglected communities (29–36). In addition, rural communities from the Coastal Region of Ecuador in the provinces of Esmeraldas, Manabí, and Santa Elena were deeply affected by COVID-19 outbreaks during the first wave of the pandemic (14–16, 19). Although widespread, the COVID-19 pandemic has burdened neglected rural and indigenous populations more than others due to limited access to water, poor sanitation of households, lack of information in indigenous languages, and limited access to the healthcare system (32–36).
Interestingly, this study included only community-dwelling non-hospitalized individuals, so either no symptoms or mild symptoms were reported among the individuals infected with SARS-CoV-2. Moreover, 20 individuals from four different cantons had viral loads over 108 viral copies/mL and could be considered SARS-CoV-2 super spreaders, representing a 7.46% of the infected population (37). Although there are limitations associated with the calculated viral load based on Ct values representing all the viral genomic material on the sample, and infection of cell cultures is used for sample infectivity confirmation, it is a clear association between low Ct values (that indicates high viral loads based on genomic material quantification) and infectivity (37). As the COVID-19 control and surveillance program in Ecuador was mainly limited to hospitalized individuals, our results clearly endorsed that the strategy was not sufficient to control COVID-19 outbreaks (14–19). Nevertheless, the SARS-CoV-2 testing capacity for the public health system in Ecuador was very limited for a 17-million population (38–40). In addition, no resources were allocated to most of the rural provinces of the country, and the SARS-CoV-2 diagnosis was centralized in the three laboratories from the “Instituto Nacional de Salud Publica e Investigación” located in the three main cities of Ecuador (18). Together with studies carried out in Afro-Ecuadorian communities (19), rural villages from the Manabi province (14, 15), Amazonian indigenous communities (7, 8), women victims of gender-based violence (41), food riders, or funeral home workers (42, 43) from Ecuador, those results highlight the need for active COVID-19 monitoring in community-dwelling individuals from vulnerable groups and neglected communities.
In conclusion, our findings support that COVID-19 community transmission and super-spreading events were happening among rural mestizo and indigenous communities from the Andean region in Ecuador during the first wave of the COVID-19 pandemic. For the still ongoing COVID-19 pandemic and future ones, our results endorse that control and prevention strategies have to focus not only on hospitalized and symptomatic individuals but also on community-dwelling individuals at locations where outbreaks are suspected.
Author's note
In this study, we described COVID-19 outbreaks in rural indigenous population from the Andean Region of Ecuador. Although several studies regarding COVID-19 and indigenous people have been published from Latin America, this is the first one addressing the situation in the Andean region during the early stages of the pandemics. With a sample over 1,000 community dwelling individuals, high infection rates were found endorsing community transmission during the first wave of COVID-19 pandemic in these neglected population in Ecuador.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The paired samples used for the homogenization protocol were the leftover of the samples collected for routine SARS-CoV-2 diagnosis. Nevertheless, this work is included in a study that was approved by the IRB from the Dirección Nacional de Inteligencia de la Salud (Ministerio de Salud Publica, Ecuador) under the code 008-2020.
UDLA COVID-19 team
Tatiana Jaramillo, Daniela Santander Gordon, Gabriel Alfredo Iturralde, Julio Alejandro Teran, Karen Marcela Vasquez, Jonathan Dario Rondal, Genoveva Granda, Ana Cecilia Santamaria, Cynthia Lorena Pino, Oscar Lenin Espinosa, Angie Buitron, David Sanchez Grisales, Karina Beatriz Jimenez, Heberson Galvis, Barbara Coronel, Dayana Marcela Aguilar, Ines Maria Paredes, Christian David Bilvao, Sebastian Rodriguez Pazmiño, Juan Carlos Laglaguano, Henry Herrera, Pablo Marcelo Espinosa, Edison Andrés Galarraga, Marlon Steven Zambrano-Mila, Ana María Tito, and Nelson David Zapata.
Author contributions
DM-J and MG-B wrote the manuscript. All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This study was funded by the Universidad de Las Américas and by Fundación CRISFE (Fondo Sumar juntos).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. (2020) 395:470–3. doi: 10.1016/S0140-6736(20)30185-9
2. Secretaría General de Comunicación. Available online at: https://www.comunicacion.gob.ec/se-registra-el-primer-caso-de-coronavirus-en-ecuador/ (accessed July 20, 2022).
4. Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo Q, et al. Prevalence of comorbidities and its effects in coronavirus disease 2019 patients: a systematic review and meta-analysis. Int J Infect Dis. (2020) 94:91–5. doi: 10.1016/j.ijid.2020.03.017
5. CDC. Coronavirus Disease 2019 (COVID-19). Available online at: https://www.cdc.gov/coronavirus/2019-ncov/index.html (accessed July 20, 2022).
6. Park M, Cook AR, Lim JT, Sun Y, Dickens BL. A systematic review of COVID-19 epidemiology based on current evidence. J Clin Med. (2020) 9:967. doi: 10.3390/jcm9040967
7. Ortiz-Prado E, Rivera-Olivero IA, Freire-Paspuel B, Lowe R, Lozada T, Henriquez-Trujillo AR, et al. Testing for SARS-CoV-2 at the core of voluntary collective isolation: lessons from the indigenous populations living in the Amazon region in Ecuador. Int J Infect Dis. (2021) 105:234–5. doi: 10.1016/j.ijid.2021.02.039
8. Henriquez-Trujillo AR, Ortiz-Prado E, Rivera-Olivero IA, Nenquimo N, Tapia A, Anderson M, et al. COVID-19 outbreaks among isolated Amazonian indigenous people, Ecuador. Bull World Health Organ. (2021) 99:478A. doi: 10.2471/BLT.20.283028
9. Sansone NM, Boschiero MN, Ortega MM, Ribeiro IA, Peixoto AO, Mendes RT, et al. Severe acute respiratory syndrome by SARS-CoV-2 infection or other etiologic agents among Brazilian indigenous population: an observational study from the first year of coronavirus disease (COVID)-19 pandemic. Lancet Reg Health Am. (2022) 8:100177. doi: 10.1016/j.lana.2021.100177
10. El Mundo Indígena PO-T. 2020: Ecuador—IWGIA—International Work Group for Indigenous Affairs. Available online at: https://www.iwgia.org/es/ecuador/3741-mi-2020-ecuador.html (accessed March 2, 2021).
11. Consejo Nacional para la igualdad de pueblos y Nacionalidades. Nacionalidades y Pueblos Indígenas Frente al Coronavirus (COVID-19). Consejo Nacional para la Igualdad de Pueblos y Nacionalidades. Available online at: http://www.pueblosynacionalidades.gob.ec/nacionalidades-y-pueblos-indigenas-del-ecuador-frente-al-coronavirus-covid-19/ (accessed March 4, 2021).
12. Instituto Nacional de Estadísticas y Censos Ecuador. VII Censo de Población y VI de Vivienda Galápagos—Variable—V426. (2010). Available online at: https://anda.inec.gob.ec/anda/index.php/catalog/659/datafile/F10/V427 (accessed March 3, 2021).
13. Cupertino GA, do Carmo Cupertino M, Gomes AP, Braga LM, Siqueira-Batista R. COVID-19 and Brazilian indigenous populations. Am J Trop Med Hyg. (2020) 103:609–12. doi: 10.4269/ajtmh.20-0563
14. Ortiz-Prado E, Henriquez-Trujillo AR, Rivera-Olivero IA, Freire-Paspuel B, Vallejo-Janeta AP, Lozada T, et al. Massive SARS-CoV-2 RT-PCR testing on rural communities in Manabi province (Ecuador) reveals severe COVID-19 outbreaks. Am J Trop Med Hyg. (2021) 104:1493–4. doi: 10.4269/ajtmh.20-1208
15. Rodriguez-Paredes MB, Vallejo-Janeta PA, Morales-Jadan D, Freire-Paspuel B, Ortiz-Prado E, Henriquez-Trujillo AR, et al. COVID-19 community transmission and super spreaders in rural villages from Manabi province in the coastal region of Ecuador assessed by massive testing of community-dwelling population. Am J Trop Med Hyg. (2022) 106:121–6. doi: 10.4269/ajtmh.21-0582
16. Del Brutto OH, Costa AF, Mera RM, Recalde BY, Bustos JA, García HH. Household clustering of SARS-CoV-2 in community settings: a study from rural Ecuador. Am J Trop Med Hyg. (2020) 103:1207–10. doi: 10.4269/ajtmh.20-0688
17. Freire-Paspuel B, Vega-Mariño P, Velez A, Castillo P, Masaquiza C, Cedeño-Vega R, et al. “One health” inspired SARS-CoV-2 surveillance: the Galapagos islands experience. One Health. (2020) 11:100185. doi: 10.1016/j.onehlt.2020.100185
18. Santander-Gordon D, Iturralde GA, Freire-Paspuel B, Zambrano-Mila MS, Morales DC, Vallejo-Janeta PA. The crucial contribution of the universities on the SARS-CoV-2 surveillance in Ecuador: lessons for developing countries. One Health. (2021) 13:100267. doi: 10.1016/j.onehlt.2021.100267
19. Vallejo-Janeta AP, Morales-Jadan D, Paredes-Espinosa MB, Coronel B, Galvis H, Bone-Guano HR, et al. Sustained COVID-19 community transmission and potential super spreading events at neglected Afro-Ecuadorian communities assessed by massive RT-qPCR and serological testing of community dwelling population. Front Med. (2022) 9:933260. doi: 10.3389/fmed.2022.933260
20. CDC. Interim Guidelines for Clinical Specimens for COVID-19. CDC. Available online at: https://www.cdc.gov/coronavirus/2019-ncov/lab/guidelines-clinical-specimens.html (accessed March 2, 2021).
21. Freire-Paspuel B, Bruno A, Orlando A, Garcia-Bereguiain MA. Clinical performance and analytical sensitivity of three SARS-CoV-2 nucleic acid diagnostic tests. Am J Trop Med Hyg. (2021) 104:1516–8. doi: 10.4269/ajtmh.20-1484
22. Freire-Paspuel B, Garcia-Bereguiain MA. Clinical performance and analytical sensitivity of two SARS-CoV-2 nucleic acid diagnostic tests used in Ecuador. Am J Trop Med Hyg. (2021) 104:1672–5. doi: 10.4269/ajtmh.20-1439
23. Freire-Paspuel B, Garcia-Bereguiain MA. Analytical and clinical evaluation of “AccuPower SARS-CoV-2 multiplex RT-PCR kit (Bioneer, South Korea)” and “Allplex 2019-nCoV assay (Seegene, South Korea)” for SARS-CoV2 RT-PCR diagnosis: Korean CDC EUA as a quality control proxy for developing countries. Front Cell Infect Microbiol. (2021) 11:630552. doi: 10.3389/fcimb.2021.630552
24. Freire-Paspuel B, Garcia-Bereguiain MA. Poor sensitivity of “AccuPower SARS-CoV-2 real time RT-PCR kit (Bioneer, South Korea).” Virol J. (2020) 17:178. doi: 10.1186/s12985-020-01445-4
25. Freire-Paspuel B, Garcia-Bereguiain MA. Analytical sensitivity and clinical performance of “COVID-19 RT-PCR Real TM FAST (CY5) (ATGen, Uruguay) and “ECUGEN SARS-CoV-2 RT-qPCR” (UDLA-Starnewcorp, Ecuador)”: high quality-low cost local SARS-CoV-2 tests for South America. PLOS Negl Trop Dis. (2022) 16:e0010082. doi: 10.1371/journal.pntd.0010082
26. Morales-Jadán D, Viteri-Dávila C, Castro-Rodriguez B, Vallejo-Janeta AP, Rivera-Olivero IA, Perez F, et al. Clinical performance of three commercial SARS-CoV-2 rapid antigen tests for community dwelling individuals in a tropical setting. Front Cell Infect Microbiol. (2022) 12:832235. doi: 10.3389/fcimb.2022.832235
27. Figueroa S, Freire-Paspuel B, Vega-Mariño P, Velez A, Cruz M, Cardenas WB, et al. High sensitivity-low cost detection of SARS-CoV-2 by two steps end point RT-PCR with agarose gel electrophoresis visualization. Sci Rep. (2021) 11:21658. doi: 10.1038/s41598-021-00900-8
28. Bruno A, de Mora D, Freire-Paspuel B, Rodriguez AS, Paredes-Espinosa MB, Olmedo M, et al. Analytical and clinical evaluation of a heat shock SARS-CoV-2 detection method without RNA extraction for N and E genes RT-qPCR. Int J Infect Dis. (2021) 109:315–20. doi: 10.1016/j.ijid.2021.06.038
29. Ferrante L, Fearnside PM. Protect indigenous peoples from COVID-19. Science. (2020) 368:251. doi: 10.1126/science.abc0073
30. Kopel J, Perisetti A, Roghani A, Aziz M, Gajendran M, Goyal H. Racial and gender-based differences in COVID-19. Front Public Health. (2020) 8:418. doi: 10.3389/fpubh.2020.00418
31. Laurencin CT, McClinton A. The COVID-19 pandemic: a call to action to identify and address racial and ethnic disparities. J Racial Ethn Health Disparities. (2020) 7:398–402. doi: 10.1007/s40615-020-00756-0
32. Chiquete E, Alegre-Díaz J, Ochoa-Guzmán A, Toapanta-Yanchapaxi LN, González-Carballo C, Garcilazo-Ávila A, et al. Ethnicity and other COVID-19 death risk factors in Mexico. Arch Med Sci. (2020) 18:711–8. doi: 10.5114/aoms.2020.101443
33. Meneses-Navarro S, Freyermuth-Enciso MG, Pelcastre-Villafuerte BE, Campos-Navarro R, Meléndez-Navarro DM, Gómez-Flores-Ramos L. The challenges facing indigenous communities in Latin America as they confront the COVID-19 pandemic. Int J Equity Health. (2020) 19:19–21. doi: 10.1186/s12939-020-01178-4
34. Kaplan HS, Trumble BC, Stieglitz J, Mamany RM, Cayuba MG, Moye LM, et al. Voluntary collective isolation as a best response to COVID-19 for indigenous populations? A case study and protocol from the Bolivian amazon. Lancet. (2020) 395:1727–34. doi: 10.1016/S0140-6736(20)31104-1
35. Díaz de León-Martínez L, de la Sierra-de la Vega L, Palacios-Ramírez A, Rodriguez-Aguilar M, Flores-Ramírez R. Critical review of social, environmental and health risk factors in the Mexican indigenous population and their capacity to respond to the COVID-19. Sci Total Environ. (2020) 733:139357. doi: 10.1016/j.scitotenv.2020.139357
36. Palamim CVC, Ortega MM, Marson FAL. COVID-19 in the indigenous population of Brazil. J Racial Ethnic Health Disparities. (2020) 7:1053–1058. doi: 10.1007/s40615-020-00885-6
37. Yang Q, Saldi TK, Gonzales PK, Lasda E, Decker CJ, Tat KL, et al. Just 2% of SARS-CoV-2–positive individuals carry 90% of the virus circulating in communities. Proc Natl Acad Sci USA. (2021) 118:e2104547118. doi: 10.1073/pnas.2104547118
38. Herrera D, Altamirano CT, Gaus D. COVID-19 in Ecuador: imported control strategies without context in a challenged healthcare system. Am J Trop Med Hyg. (2021) 104:414–5. doi: 10.4269/ajtmh.20-1347
39. Torres I, Sacoto F. Localising an asset-based COVID-19 response in Ecuador. Lancet. (2020) 395:1339. doi: 10.1016/S0140-6736(20)30851-5
40. Ortiz-Prado E, Simbaña-Rivera K, Barreno LG, Diaz AM, Barreto A, Moyano C, et al. Epidemiological, socio-demographic and clinical features of the early phase of the COVID-19 epidemic in Ecuador. PLoS Negl Trop Dis. (2021) 15:e0008958. doi: 10.1371/journal.pntd.0008958
41. Vallejo-Janeta AP, Morales-Jadan D, Freire-Paspuel B, Lozada T, Cherrez-Bohorquez C, Garcia-Bereguiain MA, et al. COVID-19 outbreaks at shelters for women who are victims of gender-based violence from Ecuador. Int J Infect Dis. (2021) 108:531–6. doi: 10.1016/j.ijid.2021.06.012
42. Ortiz-Prado E, Henriquez-Trujillo AR, Rivera-Olivero IA, Lozada T, Garcia-Bereguiain MA. High prevalence of SARS-CoV-2 infection among food delivery riders. A case study from Quito, Ecuador. Sci Total Environ. (2021) 770:145225. doi: 10.1016/j.scitotenv.2021.145225
Keywords: SARS-CoV-2, indigenous people, COVID-19, Ecuador, Andean region
Citation: Morales-Jadán D, Vallejo-Janeta AP, Bastidas V, Paredes-Espinosa MB, Freire-Paspuel B, Rivera-Olivero I, Ortiz-Prado E, Henriquez-Trujillo AR, Lozada T, the UDLA COVID-19 Team and Garcia-Bereguiain MA (2023) High SARS-CoV-2 infection rates and viral loads in community-dwelling individuals from rural indigenous and mestizo communities from the Andes during the first wave of the COVID-19 pandemic in Ecuador. Front. Med. 10:1001679. doi: 10.3389/fmed.2023.1001679
Received: 23 July 2022; Accepted: 12 January 2023;
Published: 09 February 2023.
Edited by:
Bin Luo, Lanzhou University, ChinaReviewed by:
Alberto Orlando, National Institute of Public Health and Research, EcuadorYanjun Wang, Hunan University of Science and Technology, China
Copyright © 2023 Morales-Jadán, Vallejo-Janeta, Bastidas, Paredes-Espinosa, Freire-Paspuel, Rivera-Olivero, Ortiz-Prado, Henriquez-Trujillo, Lozada, the UDLA COVID-19 Team and Garcia-Bereguiain. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Miguel Angel Garcia-Bereguiain,  bWFnYmVyZWd1aWFpbkBnbWFpbC5jb20=
bWFnYmVyZWd1aWFpbkBnbWFpbC5jb20=