 Alicia Lorenzo1*
Alicia Lorenzo1* Patricia Beroiz2,3Salvador Ortiz4Jorge del Toro5
Patricia Beroiz2,3Salvador Ortiz4Jorge del Toro5 Lucia Mazzolai6Alessandra Bura-Riviere7
Lucia Mazzolai6Alessandra Bura-Riviere7 Adriana Visonà8
Adriana Visonà8 Peter Verhamme9
Peter Verhamme9 Pierpaolo Di Micco10Giuseppe Camporese11Teresa Sancho Bueso1Manuel Monreal12,13 and the RIETE Investigators†
Pierpaolo Di Micco10Giuseppe Camporese11Teresa Sancho Bueso1Manuel Monreal12,13 and the RIETE Investigators†- 1Department of Internal Medicine, Hospital Universitario La Paz, Madrid, Spain
- 2Department of Geriatrics, Hospital Germans Trias i Pujol, Badalona, Barcelona, Spain
- 3Department of Medicine, Universidad Autónoma de Barcelona, Barcelona, Spain
- 4Department of Applied Economics, Universidad Autónoma Madrid, S&H Medical Science Service Advisor, Madrid, Spain
- 5Department of Internal Medicine, Hospital General Universitario Gregorio Marañón, Madrid, Spain
- 6Department of Angiology, Centre Hospitalier Universitaire Vaudois (CHUV), Lausanne, Switzerland
- 7Department of Vascular Medicine, Hôpital de Rangueil, Toulouse, France
- 8Department of Vascular Medicine, Ospedale Castelfranco Veneto, Castelfranco Veneto, Italy
- 9Vascular Medicine and Haemostasis, University of Leuven, Leuven, Belgium
- 10Department of Internal Medicine and Emergency Room, Ospedale Buon Consiglio Fatebenefratelli, Naples, Italy
- 11Angiology Unit, Department of Cardiac, Thoracic and Vascular Sciences, Padua University Hospital, Padua, Italy
- 12Department of Internal Medicine, Hospital Germans Trias i Pujol, Badalona, Barcelona, Spain
- 13Chair for the Study of Thromboembolic Disease, Faculty of Health Sciences, UCAM—Universidad Católica San Antonio de Murcia, Murcia, Spain
Background: Current guidelines recommend the use of direct oral anticoagulants (DOACs) for patients with venous thromboembolism (VTE). However little is known about the use of DOACs in daily practice.
Methods: We used the RIETE registry to identify predictors of use of DOACs for initial and/or long-term therapy of VTE based on patient-related factors, institution-related factors or over time.
Results: Among 41,678 patients from March 2013 to September 2021, 12,286 (29%) used DOACs: for initial therapy 6,456; for long-term therapy 12,046. On multivariable analysis, independent predictors were: age < 65 years (odds ratio [OR]: 1.30; 95% CI: 1.23–1.38), body weight <50 kg (OR: 0.54; 95% CI: 0.45–0.65) or >120 kg (OR: 0.64; 95% CI: 0.53–0.77), initial VTE presentation as pulmonary embolism (OR: 1.18; 95% CI: 1.13–1.25), recent bleeding (OR: 0.53; 95% CI: 0.45–0.63), renal insufficiency (OR: 0.44; 95% CI: 0.38–0.51), liver cirrhosis (OR: 0.32; 95% CI: 0.20–0.52), thrombocytopenia (OR: 0.40; 95% CI: 0.34–0.49), atrial fibrillation (OR: 1.58; 95% CI: 1.42–1.75) and prior VTE (OR: 1.14; 95% CI: 1.06–1.22). The DOACs were more likely used in other European countries (OR: 8.97; 95% CI: 8.49–9.49), America (OR: 6.35; 95% CI: 5.67–7.11) or in other countries of the world (OR: 2.99; 95% CI: 2.70–3.31) than in Spain, and progressively increased from 2013–2015 to 2016–2018 (OR: 2.78; 95% CI: 2.62–2.95) and 2019–2021 (OR: 6.36; 95% CI: 5.95–6.80).
Conclusion: In this large multinational VTE registry, variations were observed in the use of DOACs according to patient or country factors, and over time. The safety, costs, and influence of the DOACs on VTE-related outcomes in daily practice warrant further investigation.
Introduction
Current guidelines of anticoagulant therapy recommend the use of direct oral anticoagulants (DOACs) for initial and long-term therapy of patients with venous thromboembolism (VTE) (1, 2). The risk reduction of recurrent VTE with DOACs is similar to the risk reduction with low-molecular-weight heparin (LMWH) and vitamin K antagonists (VKAs), while the risk of bleeding is less with DOACs than with standard therapy (3). However, the use of DOACs has not completely replaced the use of standard therapy. There are patient-related factors, and also institutional or logistical reasons that may limit the use of DOACs in daily practice. Patient-related factors include older age, extreme body weights (where there may be doubts about the optimal dose) or concomitant diseases (where there may be concern about the risk of bleeding) (4–12). In addition, resource availability may also drive the choice of therapies. A better knowledge of the reasons why physicians prescribe the use of DOACs for the initial and/or long-term therapy of VTE could lead to design randomized trials for subgroups of patients where its use is lower than expected (to reassure on the efficacy and safety of DOACs) or higher than expected (to avoid undesirable outcomes).
The RIETE (Registro Informatizado Enfermedad TromboEmbólica) registry is an international, ongoing registry of consecutive patients with symptomatic, objectively confirmed, acute VTE (ClinicalTrials.gov identifier: NCT02832245). Since its inception in 2001, data from this registry have been used to evaluate outcomes after acute VTE, such as the frequency of recurrent VTE, bleeding and mortality, and risk factors for these outcomes (13). In the current study, we aimed to determine the potential variations in the use of DOACs in patients with confirmed VTE, based on patient-related factors, institution-related factors, and over time.
Patients and methods
Inclusion criteria
Consecutive patients with acute deep vein thrombosis (DVT) or pulmonary embolism (PE) confirmed by objective tests (compression ultrasonography for suspected DVT; helical CT-scan, ventilation-perfusion lung scintigraphy or conventional angiography for suspected PE) were enrolled in RIETE. Patients were excluded if they were currently participating in a therapeutic clinical trial with a blinded therapy. All patients (or their legal power of attorney) provided written or oral consent for participation in the registry, in accordance with local ethics committee requirements.
Study design
Data were collected from March 2013 (corresponding to the time when the prescription of DOACs was allowed) to July 2021. The primary goal of this study was to determine the potential variations in the use of DOACs in patients with symptomatic, objectively confirmed VTE, based on patient-related factors, or institution-related factors. As such, the main outcome was the proportion of patients using DOACs vs. those using other anticoagulant drugs. Secondary outcomes were the proportion of patients using each DOAC (vs. the other DOACs), and the proportion of patients using lower-than recommended doses of DOACs. Recommended dosing was defined as dosing consistent with FDA-labeled dosing for treatment of VTE as of September 2021.
Patient-related factors explored in this study included demographics (sex, age, body weight), initial VTE presentation (PE with or without concomitant DVT vs. isolated DVT), concomitant diseases that could contraindicate the use of DOACs [including recent (<30 days before) major bleeding, biopsy-proven liver cirrhosis, creatinine clearance (CrCl) levels <30 mL/min and platelet count <100,000/μLat baseline], and concomitant disorders that could lead to prolong the duration of anticoagulant therapy (prior VTE and atrial fibrillation). We also evaluated the proportion of fragile patients that used DOACs (fragile patients defined as those aged ≥75 years, with CrCl levels ≤50 mL/min or body weight ≤50 kg) (14). Institutional factors assessed in the current study included the country of enrolment. Further, we explored the trends in the use of DOACs over the study years.
Treatment
Patients were managed according to the clinical practice of each participating hospital (i.e., there was no standardization of treatment). The decision on the type and duration of therapy was left to the attending physicians. Patients were followed-up for at least 3 months in the outpatient clinic or physician’s office.
Statistical analysis
Categorical variables were compared using the chi-square test (two-sided) and Fisher’s Exact Test (two-sided). Continuous variables were compared using Student t test. To identify predictors of prescription of drugs we used logistic regression analyses. All the analyses were adjusted for sex, age (65 years; 65–79; >79 years), body weight (<50 kg; 50–120; >120 kg), initial VTE presentation (symptomatic PE; isolated DVT), recent major bleeding, liver cirrhosis, CrCl levels at baseline <30 mL/min, platelet count <100,000/μL, atrial fibrillation, prior VTE, the country where the VTE was diagnosed (Spain; other European countries; America; rest of the world) and years of VTE diagnosis (2013–2015; 2016–2018; 2019–2021). Odds ratios (OR) and corresponding 95% confidence intervals (CI) were calculated, and a p value < 0.05 was considered to be statistically significant. Statistical analyses were conducted with SPSS for Windows Release 25.0 (SPSS, Inc.).
Role of the funding source
The sponsors of the RIETE registry (Sanofi, Leo Pharma and Rovi) had no role in study design, data collection, data analysis, data interpretation or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Results
Among 41,678 patients with VTE recruited from January 2013 to September 2021 in RIETE, 12,286 (29%) used DOACs: 6,456 for initial therapy and 12,046 for long-term therapy. Among the 41,678 patients, 20,896 (50%) were men; mean age was 65 ± 17 years; 23,458 (56%) initially presented with PE; 970 (2.3%) had recent major bleeding; CrCl levels <30 mL/min 2,097 (5.0%); liver cirrhosis 209 (0.5%); platelet count < 100,000/μL 1,055 (2.5%); atrial fibrillation 2,361 (5.7%) and prior VTE 5,818 (14%). In total, 16,767 patients (40%) were fragile.
Most patients (65%) were attended in Spanish centers, 25% in other European countries, 3.7% in America and 6.0% in the rest of the world (Table 1). For initial therapy, 5,141 patients (12%) used rivaroxaban and 1,315 (3.2%) apixaban. For long-term therapy, 6,631 patients (16%) used rivaroxaban, apixaban 3,548 (8.5%), edoxaban 1,473 (3.5%), and dabigatran 394 (0.9%). The proportion of patients using DOACs progressively increased over time (Figure 1).
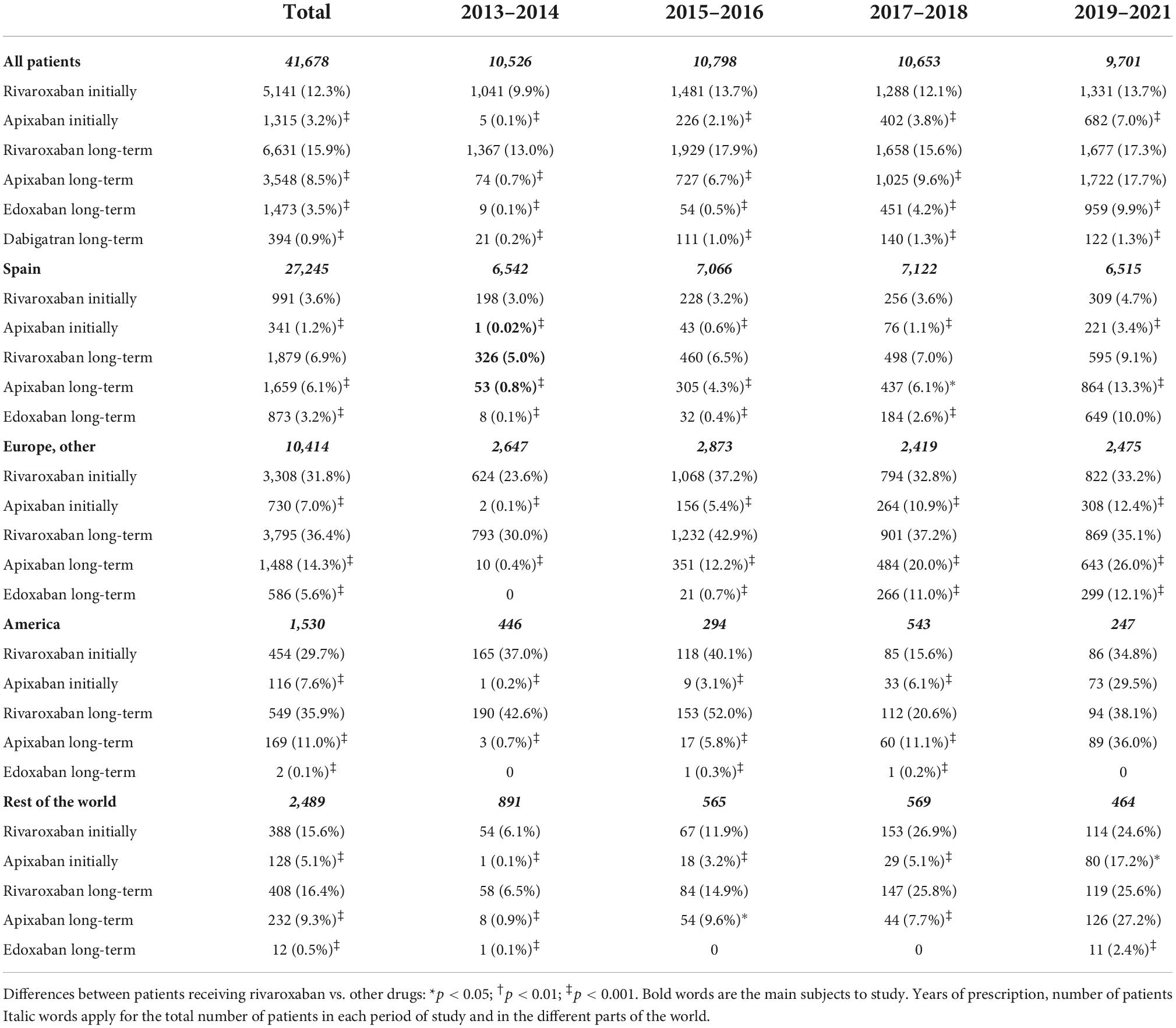
Table 1. Prescription of DOACs over time in different countries.
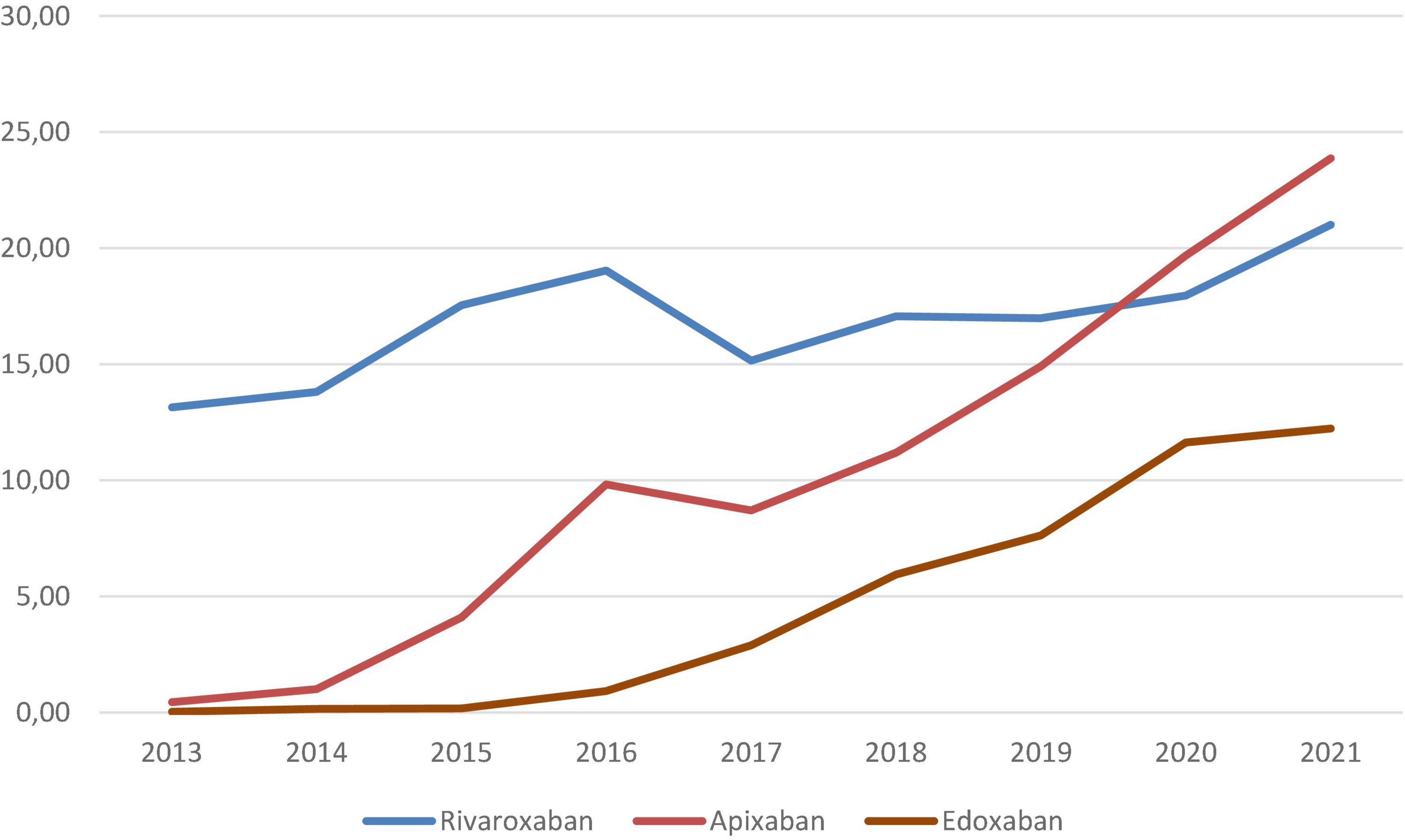
Figure 1. Cumulative rates of patients receiving DOACs for initial and/or long-term therapy of VTE over time.
Predictors of use of direct oral anticoagulants vs. other drugs
Overall, 12,286 patients (29%) used DOACs for initial and/or for the long-term therapy of VTE. The proportion of patients using DOACs was highest among those aged <65 years (33%), with atrial fibrillation (33%) or prior VTE (34%), and lowest in patients with CrCl levels < 30 mL/min (15%), liver cirrhosis (11%) or thrombocytopenia (16%) (Table 2) The use of DOACs was lowest in Spain (17%) and highest in other European countries (59%) or America (50%), and progressively increased over time: from 17% in 2013–2015 to 47% in 2019–2021. Among 12,286 patients using DOACs, 2,154 (18%) used lower-than recommended doses. The subgroups of patients that were more likely to use lower-than recommended doses of DOACs were: patients aged >79 years (30%), with CrCl levels <30 mL/min (44%) or with atrial fibrillation (30%). Only 4,105 of the 17,767 fragile patients with VTE (24%) used DOACs: 25% at lower than recommended doses.
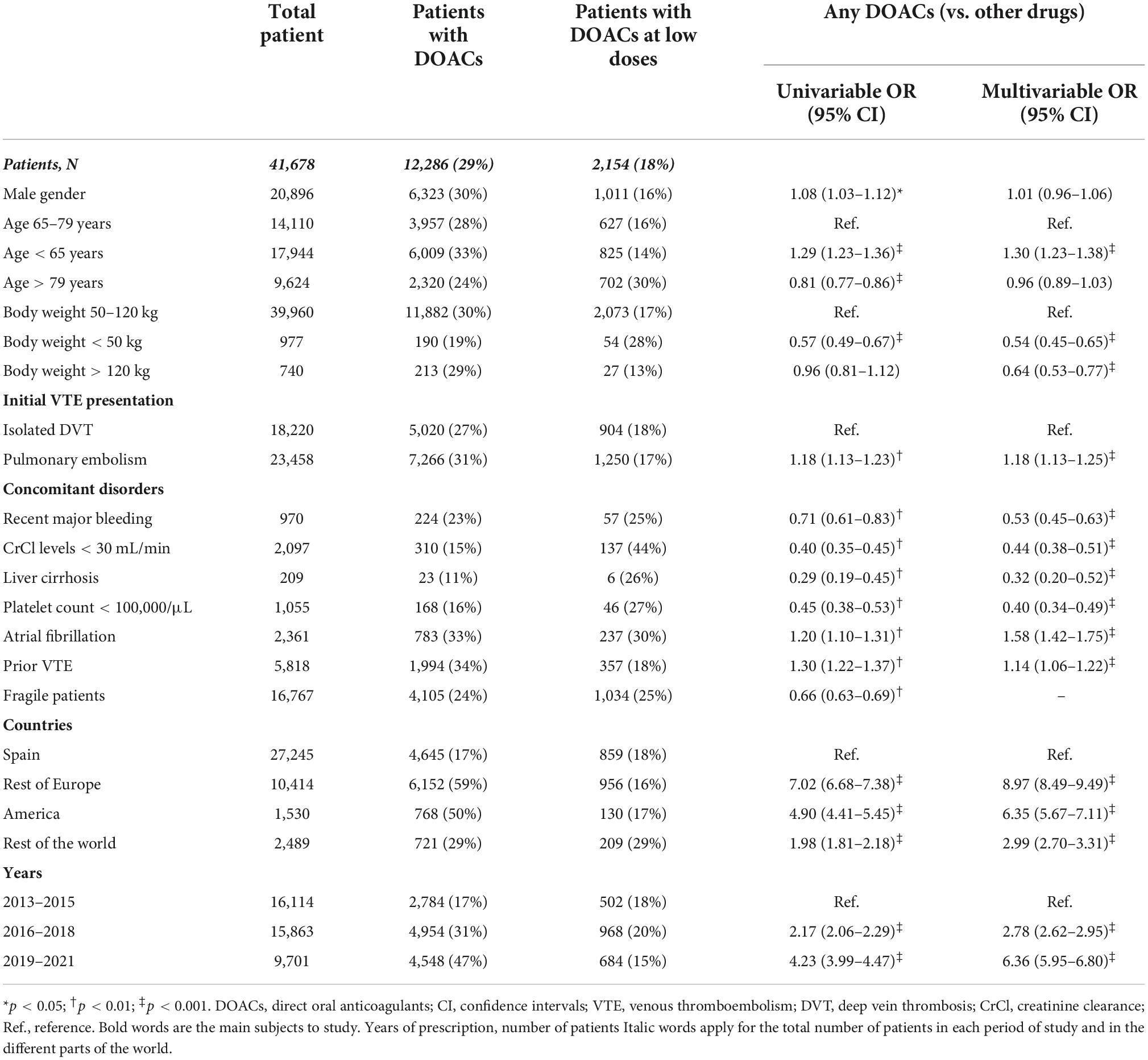
Table 2. Univariable and multivariable analyses for predictors of use of DOACs vs. other drugs.
On multivariable analysis, independent predictors for the use of DOACs (vs. other anticoagulants) were: age <65 years (OR: 1.30; 95% CI: 1.23–1.38) body weight <50 kg (OR: 0.54; 95% CI: 0.45–0.65) or > 120 kg (OR: 0.64; 95% CI: 0.53–0.77) initial VTE presentation as PE (OR: 1.18; 95% CI: 1.13–1.25) recent bleeding (OR: 0.53; 95% CI: 0.45–0.63) CrCl levels <30 mL/min (OR: 0.44; 95% CI: 0.38–0.51) liver cirrhosis (OR: 0.32; 95% CI: 0.20–0.52) platelet count <100,000/μL (OR: 0.40; 95% CI: 0.34–0.49) atrial fibrillation (OR: 1.58; 95% CI: 1.42–1.75) and prior VTE (OR: 1.14; 95% CI: 1.06–1.22) (Table 3) The use of DOACs was more likely in other European countries (OR: 8.97; 95% CI: 8.49–9.49) America (OR: 6.35; 95% CI: 5.67–7.11) or in the rest of the world (OR: 2.99; 95% CI: 2.70–3.31) than in Spain, and progressively increased from 2013–2015 to 2016–2018 (OR: 2.78; 95% CI: 2.62–2.95) and 2019–2021 (OR: 6.36; 95% CI: 5.95–6.80).
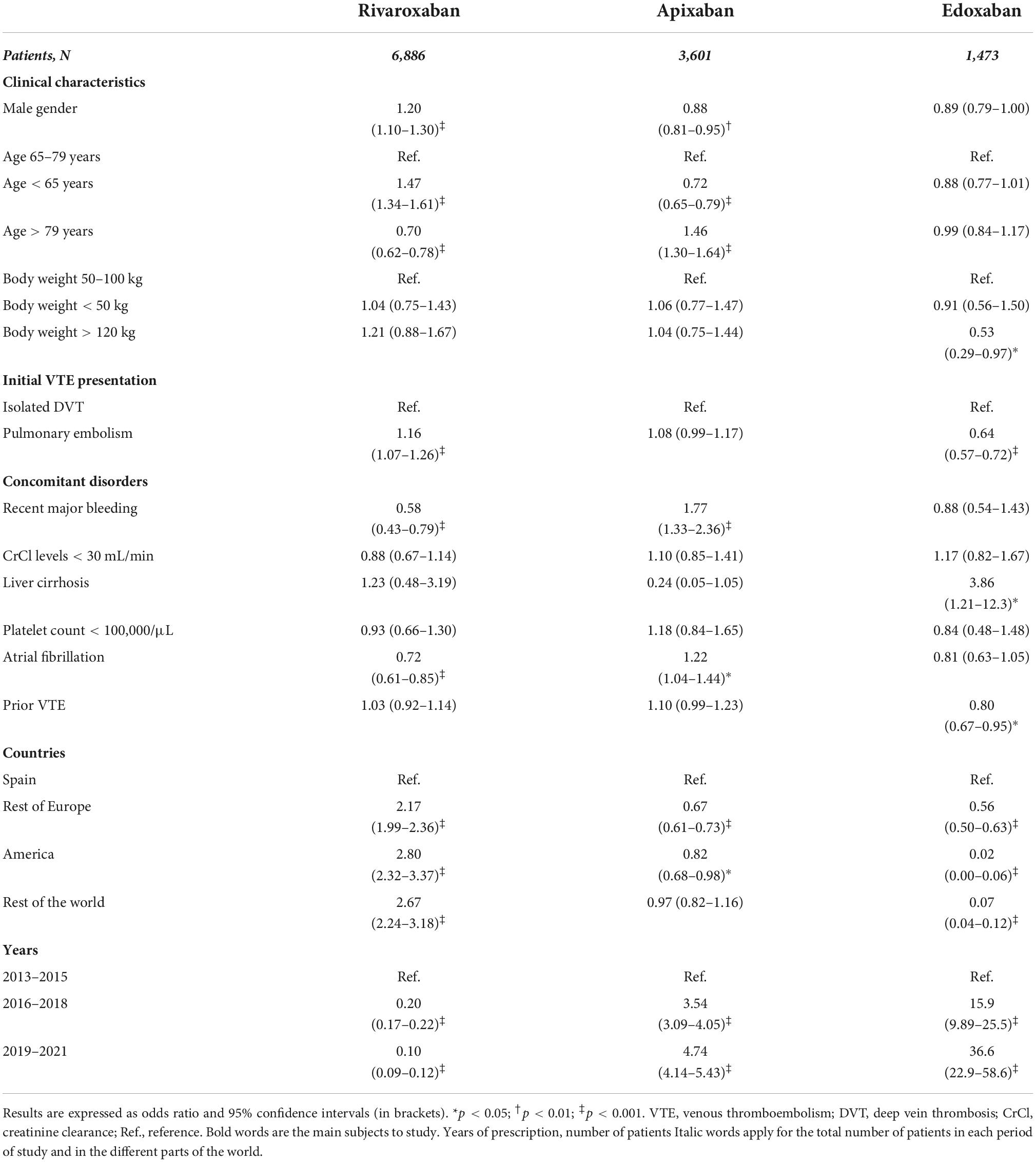
Table 3. Multivariable analyses for predictors of use of every DOAC (vs. the rest of DOACs).
Predictors of use of one direct oral anticoagulant vs. the rest of direct oral anticoagulants
Among patients using DOACs, rivaroxaban was more likely used in men (OR: 1.26; 95% CI: 1.18–1.36) in patients aged <65 years (OR: 1.51; 95% CI: 1.39–1.63) weighing > 120 kg (OR: 1.61; 95% CI: 1.21–2.15) or with prior VTE (OR: 1.23; 95% CI: 1.12–1.36) (Table 4). Apixaban was the preferred DOAC among patients >79 years (OR: 1.59; 95% CI: 1.43–1.76) in those initially presenting with PE (OR: 1.17; 95% CI: 1.08–1.27) with recent bleeding (OR: 1.80; 95% CI: 1.37–2.35) renal insufficiency (OR: 1.89; 95% CI: 1.51–2.38) atrial fibrillation (OR: 1.62; 95% CI: 1.39–1.88) or in fragile patients (OR: 1.79; 95% CI: 1.65–1.94) Edoxaban was much more likely used in Spain than in other countries.
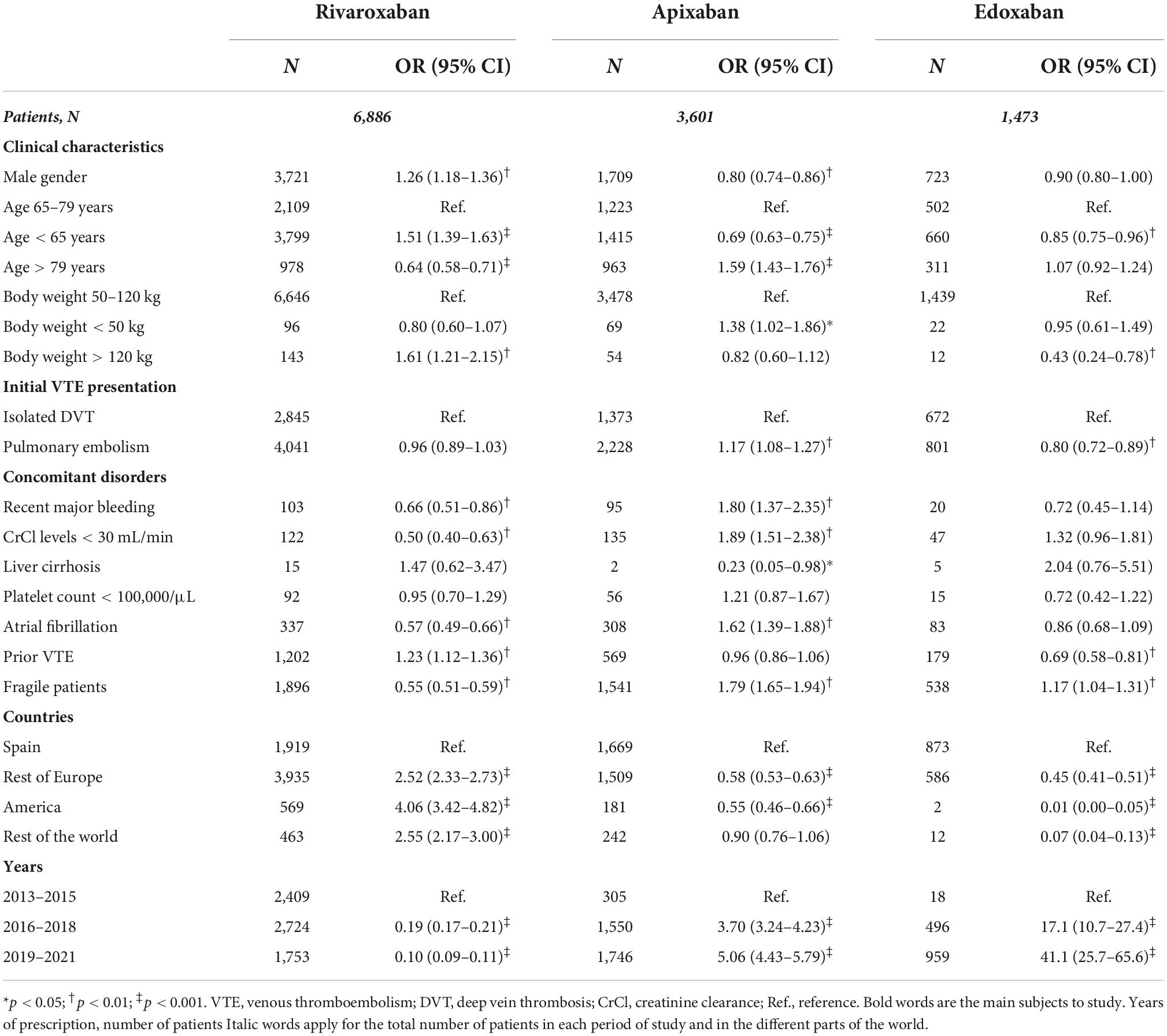
Table 4. Univariable analyses for predictors of use of each DOAC vs. the rest of DOACs.
Independent predictors for the use of rivaroxaban (vs. other DOACs) were: male gender (OR: 1.20; 95% CI: 1.10–1.30), age <65 years (OR: 1.47; 95% CI: 1.34–1.61) initial presentation as PE (OR: 1.16; 95% CI: 1.07–1.26) and VTE diagnosis in non-Spanish European countries (OR: 2.17; 95% CI: 1.99–2.36) America (OR: 2.80; 95% CI: 2.32–3.37) or in other countries (OR: 2.67; 95% CI: 2.24–3.18) Rivaroxaban was less prescribed for >79 years (OR: 0.70; 95% CI: 0.62–0.78) recent bleeding (OR: 0.58; 95% CI: 0.43–0.79) and atrial fibrillation (OR: 0.72; 95% CI: 0.61–0.85) (Table 4) Independent predictors for the use of apixaban were: male gender (OR: 0.88; 95% CI: 0.81–0.95) >79 years (OR: 1.46; 95% CI: 1.30–1.64) recent major bleeding (OR: 1.77; 95% CI: 1.33–2.36) atrial fibrillation (OR: 1.22; 95% CI: 1.04–1.44) Apixaban was less used in age <65 years (OR: 0.72; 95% CI: 0.65–0.79) and VTE diagnosis in non-Spanish European countries (OR: 0.67; 95% CI: 0.61–0.73) or in America (OR: 0.82; 95% CI: 0.68–0.98) Independent predictors for the use of edoxaban were: body weight >120 kg (OR: 0.53; 95% CI: 0.29–0.97) initial VTE presentation as PE (OR: 0.64; 95% CI: 0.57–0.72) liver cirrhosis (OR: 3.86; 95% CI: 1.21–12.3) prior VTE (OR: 0.80; 95% CI: 0.67–0.95) and being diagnosed in Spain. Interestingly, the use of rivaroxaban (comparatively with the other two DOACs) progressively decreased over time.
Discussion
Our findings, obtained from a large cohort of patients with acute VTE in up to 30 countries over the world, reveal large variations in the use of DOACs according to patient factors, institutional factors and also over time. As it could have been expected, the DOACs were more likely used in young patients, those with normal body weight and with no exclusion criteria to be enrolled in the pivotal trials where their indication was based (i.e., recent bleeding, renal insufficiency, liver cirrhosis or thrombocytopenia) Studies about patients preferences usually report more satisfied patients with DOAC than VKA drugs (15, 16) but it seems it is not a reason from prescription in some countries as Spain. Also, its use was much lower in Spain (where the DOACs are not reimbursed) and progressively increased over time. However, there were surprising findings in some subgroups of patients. For example, while the use of DOACs was lower than expected in the subgroups of patients where they had demonstrated to be superior to standard therapy, they were not infrequently used in patients with contraindications to their use.
Subgroup analyses from randomized trials revealed that the DOACs had advantages over standard anticoagulation in fragile patients with VTE. In the EINSTEIN trials, the risk for major bleeding in fragile patients using rivaroxaban was significantly lower than in those on standard therapy (17–19). This difference was not found in non-fragile patients. In the HOKUSAI trial, fragile patients using edoxaban had a significantly higher efficacy than those on VKAs (19). The superiority of the DOACs over standard therapy in fragile patients with VTE was subsequently confirmed in real-life conditions (20, 21). However, only 24% of the 17,767 fragile patients in our cohort used DOACs. We hypothesize that a higher use of DOACs in fragile patients with VTE (40% of the whole series) might have been associated with improved outcomes.
On the other hand, the use of DOACs is contraindicated in patients with severe liver or renal insufficiency, in pregnant or breast-feeding women, and in patients perceived to be at high risk for bleeding (4). Because most of these patients with were excluded from the clinical trials, data regarding their effectiveness and safety are only available through non-randomized studies of which statistical type I/type II errors could play a role (6, 22). Despite this knowledge gap, 23% of patients with recent major bleeding, 15% with CrCl levels <30 mL/min, 11% with cirrhosis, and 16% with thrombocytopenia in our cohort used DOACs. There are few data about resuming anticoagulation after major bleeding with DOAC. In the study from Little (23), reassumption of DOAC in extracranial non-gastrointestinal bleeding was accompanied by reduction in thrombosis. We haven’t studied DOAC in pregnancy in RIETE as opposite to GARFIELD study (24). Data of DOAC used in patient with recently bleeding are an interesting finding since the lack of a monitoring assays say and reversal agents (25) have been important safety concerns for clinicians. A substantial proportion of these patients (25, 44, 26, and 27%, respectively) received lower than recommended doses. This is also of concern, since under-dosing of DOACs has been associated with decreased efficacy and no benefit in safety (26–29). Apixaban was seen to be the most frequent DOAC with dose modification. It could be argued that attending physician has used the same adjustment for dose that has to be made in atrial fibrillation, as it’s supposed in the study from, about changing pattern of type of anticoagulant use and in off-label use a cohort from Switzerland (30). Also low doses are used in atrial fibrillation (31, 32).
Finally, because patients at extremes of body weight were underrepresented in DOAC clinical trials and randomized trials for these patient subgroups are currently unavailable, the International Society of Thrombosis and Hemostasis Scientific and Standardization Committee recently suggested that rivaroxaban and apixaban can be adequate for VTE therapy regardless of body weight, and suggested not using dabigatran, edoxaban or betrixaban in patients weighing >120 kg (12). In our cohort, 12 patients weighing >120 kg used edoxaban (5.6% of the obese patients using DOACs).
Among patients receiving DOACs in our cohort, there was some preference for apixaban over rivaroxaban or edoxaban in the elderly (33) and in patients with recent major bleeding or atrial fibrillation. On the other hand, rivaroxaban was preferred in the young, and edoxaban in those with liver cirrhosis. However, in the absence of clinical trials comparing the DOACs each other, there is no evidence to support that one specific DOAC is superior to any other in terms of efficacy or safety in any clinical scenario.
The main strength of this study is the large size of the RIETE registry, which enabled us to explore the variations across multiple settings, including across patient-related factors, across geographic regions as well over time. As such, the data related to temporal, institutional, and particularly patient-level variations per clinical subgroups provide real-world evidence about contemporary practice and could be helpful for practice management, policy making, and designing future research studies. However, a number of limitations of this study must be acknowledged. First, we did not evaluate the role of patient income and sociodemographic variables as they relate to patient’s willingness to pay for DOACs. Second, factors related to DOACs therapy choice may change over time as prescribers and patients gain more familiarity and experience with the newer DOACs, and additional research will be needed to identify predictors of treatment and changes in DOAC treatment patterns in the future. Third, some countries had fewer participating centers or enrolled only a few patients. As such, although findings from this multicenter, multinational study demonstrate regional variations in diagnostic practices, accurate comparisons for point estimates are not feasible for some countries. Finally, future research needs to consider the impact of patient preferences in DOAC therapy decisions.
This is the first of a series of studies to explore the use of DOACs in patients with VTE and their potential consequences. The focus of the current study was on the assessment and description of potential variations in the choice of drugs for VTE therapy. Future studies are required to explore the reasons behind the variations, the accuracy of each approach, and to assess the impact of these variations on VTE-related and non- VTE-related outcomes in adjusted analyses.
In conclusion, in a large multicenter, multinational registry of patients with VTE, we observed noticeable variations in the choice of DOACs according to the underlying patient factors and institutional factors.
Data availability statement
The original contributions presented in this study are included in the article further inquiries can be directed to the corresponding author.
Author contributions
PB, SO, JT, TS, LM, and AB-R: review of draft. All authors contributed to the article, approved the submitted version, and contributed to the patients’ enrollment.
Acknowledgments
We express our gratitude to Sanofi Spain, LEO PHARMA and ROVI for supporting this Registry with an unrestricted educational grant. We also thank the RIETE Registry Coordinating Center, S&H Medical Science Service, for their quality control data, logistic and administrative support and Prof. Salvador Ortiz, Universidad Autónoma Madrid and Silvia Galindo, both Statistical Advisors in S&H Medical Science Service for the statistical analysis of the data presented in this paper.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
DOACs, direct oral anticoagulants; VTE, venous thromboembolism; OR, odds ratio; CI, confidence intervals; LMWH, low-molecular-weight heparin; VKAs, vitamin K antagonists; PE, pulmonary embolism; DVT, deep vein thrombosis; CT-scan, computed tomography scan; CrCl, creatinine clearance.
References
1. Ortel TL, Neumann I, Ageno W, Beyth R, Clark NP, Cuker A, et al. American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism. Blood Adv. (2020) 4:4693–738. doi: 10.1182/bloodadvances.2020001830
2. Stevens SM, Woller SC, Baumann-Kreuziger L, Bounameaux H, Doerschug K, Geersing G, et al. Antithrombotic therapy for VTE disease: second update of the CHEST guideline and expert panel report. Chest. (2021) 160:e545–608. doi: 10.1016/j.chest.2021.07.055
3. Van Es N, Coppens M, Schulman S, Middeldorp S, Büller H. Direct oral anticoagulants compared with vitamin K antagonists for acute venous thromboembolism: evidence from phase 3 trials. Blood. (2014) 124:1968–75. doi: 10.1182/blood-2014-04-571232
4. Burnett AE, Mahan CE, Vazquez SR, Oertel LB, Garcia DA, Ansell J. Guidance for the practical management of the direct oral anticoagulants (DOACs) in VTE treatment. J Thromb Thrombolys. (2016) 41:206–32. doi: 10.1007/s11239-015-1310-7
5. Toorop MMA, Lijfering WM, Scheres LJJ. The relationship between DOAC levels and clinical outcomes: the measures tell the tale. J Thromb Haemost. (2020) 18:3163–8. doi: 10.1111/jth.15104
6. Weber J, Olyaei A, Shatzel J. The efficacy and safety of direct oral anticoagulants in patients with kidney disease. Eur J Haematol. (2019) 102:312–8. doi: 10.1111/ejh.13208
7. Cheung CYS, Parikh J, Farrell A, Lefebvre M, Summa-Sorgini C, Battistella M. Direct oral anticoagulant use in chronic kidney disease and dialysis patients with venous thromboembolism: a systematic review of thrombosis and bleeding outcomes. Ann Pharmacother. (2021) 55:711–22. doi: 10.1177/1060028020967635
8. Ting C, Rhoten M, Dempsey J, Nichols H, Fanikos J, Ruff CT. Evaluation of direct oral anticoagulant prescribing in patients with moderate to severe renal impairment. Clin Appl Thromb Hemost. (2021) 27:1076029620987900. doi: 10.1177/1076029620987900
9. Elhosseiny S, Al Moussawi H, Chalhoub JM, Lafferty J, Deeb L. Direct oral anticoagulants in cirrhotic patients: current evidence and clinical observations. Can J Gastroenterol Hepatol. (2019) 2019:4383269. doi: 10.1155/2019/4383269
10. Speed V, Green B, Roberts LN, Woolcombe S, Bartoli-Abdou J, Barsam S, et al. Fixed dose rivaroxaban can be used in extremes of body weight: a population pharmacokinetic analysis. J Thromb Haemost. (2020) 18:2296–307. doi: 10.1111/jth.14948
11. Katel A, Aryal M, Neupane A, Gosain R, Pathak R, Bhandari Y, et al. Efficacy and safety of direct oral anticoagulants in venous thromboembolism compared to traditional anticoagulants in morbidly obese patients: a systematic review and meta-analysis. Cureus. (2021) 13:e14572. doi: 10.7759/cureus.14572
12. Martin KA, Beyer-Westendorf J, Davidson BL, Huisman MV, Sandset PM, Moll S. Use of direct oral anticoagulants in patients with obesity for treatment and prevention of venous thromboembolism: updated communication from the ISTH SSC subcommittee on control of anticoagulation. J Thromb Haemost. (2021) 19:1874–82. doi: 10.1111/jth.15358
13. Bikdeli B, Jiménez D, Hawkins M, Ortíz S, Prandoni P, Brenner B, et al. Rationale, design and methodology of the computerized registry of patients with venous thromboembolism (RIETE). Thromb Haemost. (2018) 118:214–24. doi: 10.1160/TH17-07-0511
14. Einstein-Pe Investigators, Büller HR, Prins MH, Lensin AW, Decousus H, Jacobson BF, et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. (2010) 363:2499–510.
15. Afzal SK, Hasan SS, Babar ZU. A systematic review of patient-reported outcomes associated with the use of direct-acting oral anticoagulants. Br J Clin Pharmacol. (2019) 85:2652–67. doi: 10.1111/bcp.13985
16. Keita I, Aubin-Auger I, Lalanne C, Aubdert JR, Chassany O, Durancisky M, et al. Assessment of quality of life, satisfaction with anticoagulation therapy, and adherence to treatment in patients receiving long-course vitamin K antagonists or direct oral anticoagulants for venous thromboembolism. Patient Prefer Adherence. (2017) 11:1625–34. doi: 10.2147/PPA.S131157
17. Einstein Investigators, Bauersachs R, Berkowitz SD, Brenner B, Buller HR, Decousus H, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. (2012) 366:1287–97. doi: 10.1056/NEJMoa1113572
18. Prins MH, Lensing A, Bauersachs R, van Bellen B, Bounameaux H, Brighton TA, et al. Oral rivaroxaban versus standard therapy for the treatment of symptomatic venous thromboembolism: a pooled analysis of the EINSTEIN-DVT an PE randomized studies. Thromb J. (2013) 11:21–31. doi: 10.1186/1477-9560-11-21
19. Hokusai-Vte Investigators, Büller HR, Décousus H, Grosso MA, Mercuri M, Middeldorp S, et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med. (2013) 369:1406–15. doi: 10.1056/NEJMoa1306638
20. López-Núñez JJ, Pérez-Andrés R, Di Micco P, Schellong S, Gómez Cuervo C, Sahuquillo JC. Direct oral anticoagulants or standard anticoagulant therapy in fragile patients with venous thromboembolism. TH Open. (2019) 3:e67–76. doi: 10.1055/s-0039-1683970
21. Trujillo-Santos J, Beroiz P, Alonso A, Morejón E, López-Reyes R, Casado I, et al. Rivaroxaban or apixaban in fragile patients with acute venous thrombo-embolism. Thromb Res. (2020) 193:160–5. doi: 10.1016/j.thromres.2020.06.035
22. Derebail VK, Rheault MN, Kerlin BA. Role of direct oral anticoagulants in patients with kidney disease. Kidney Int. (2020) 97:664–75. doi: 10.1016/j.kint.2019.11.027
23. Little DHW, Sutradhar R, Cerasuolo JO, Perez R, Douketis J, Holbrook A, et al. Rates of rebleeding, thrombosis and mortality associated with resumption of anticoagulant therapy after anticoagulant-related bleeding. CMAJ. (2021) 193:E304–9. doi: 10.1503/cmaj.201433
24. Jerjes-Sánchez C, Rodriguez D, Farjat AE, Kayani G, MacCallum P, Lopes RD, et al. Pregnancy-associated venous thromboembolism: insights from GARFIELD-VTE. TH Open. (2021) 5:e24–34. doi: 10.1055/s-0040-1722611
25. Shih AW, Crowther MA. Reversal of direct oral anticoagulants: a practical approach. Hematology Am Soc Hematol Educ Program. (2016) 2016:2012–9. doi: 10.1182/asheducation-2016.1.612
26. Trujillo-Santos J, Di Micco P, Dentali F, Douketis J, Díaz-Peromingo JA, Núñez MJ, et al. Real-life treatment of venous thromboembolism with direct oral anticoagulants: the influence of recommended dosing and regimens. Thromb Haemost. (2017) 117:382–9. doi: 10.1160/TH16-07-0494
27. Dentali F, Fantoni C. Is it reasonable to use a lower DOAC dose in some patients with VTE? No. Intern Emerg Med. (2017) 12:565–7. doi: 10.1007/s11739-017-1695-8
28. Chopard R, Serzian G, Humbert S, Falvo N, Morel-Aleton M, Bonnet B, et al. Non-recommended dosing of direct oral anticoagulants in the treatment of acute pulmonary embolism is related to an increased rate of adverse events. J Thromb Thrombolysis. (2018) 46:283–91. doi: 10.1007/s11239-018-1690-6
29. Deitelzweig S, Keshishian A, Li X, Kang A, Dhamane AD, Luo X, et al. Comparisons between oral anticoagulants among older nonvalvular atrial fibrillation patients. J Am Geriatr Soc. (2019) 67: 1662–71. doi: 10.1111/jgs.15956
30. Eschler C, Antelo A, Funk GC, Exadaktylos AK, Lindner G. High fluctuation between anticoagulants, frequent off-label dosing, and no difference concerning outcomes: results of a real-life cohort study. Am J Med. (2021) 134:e165–70. doi: 10.1016/j.amjmed.2020.09.018
31. Navarro-Almenzara B, Cerezo-Manchado JJ, Caro-Martinez C, García-Candela C, Flores Blanco PJ, Elvira Ruiz G, et al. Real-life behaviour of direct oral anticoagulants in a Spanish cohort with non-valvular atrial fibrillation: refase registry. Curr Med Res Opin. (2019) 35:2035–41. doi: 10.1080/03007995.2019.1647735
32. Ruiz Orti M, Muñiz J, Raña Míguez P, Roldán I, Marín F, Esteve-Pastor A, et al. Inappropriate doses of direct oral anticoagulants in real-world clinical practice: prevalence and associated factors. A subanalysis of the FANTASIIA registry. Europace. (2018) 20:1577–83. doi: 10.1093/europace/eux316
33. Geldhof V, Vandenbriele C, Verhamme P, Vanassche T. Venous thromboembolism in the elderly: efficacy and safety of non-VKA oral anticoagulants. Thromb Jour. (2014) 12:21. doi: 10.1186/1477-9560-12-21
Appendix
Members of the RIETE Group
SPAIN: Adarraga MD, Agudo P, Aibar J, Aibar MA, Amado C, Arcelus JI, Ballaz A, Barba R, Barbagelata C, Barrón M, Barrón-Andrés B, Bascuñana J, Blanco-Molina A, Beddar Chaib F, Botella E, Camón AM, Castro J, Chasco L, Criado J, de Ancos C, de Miguel J, del Toro J, Demelo-Rodríguez P, Díaz-Brasero AM, Díaz-Pedroche MC, Díaz-Peromingo JA, Díaz-Simón R, Domínguez IM, Dubois-Silva A, Escribano JC, Espósito F, Farfán-Sedano AI, Fernández-Capitán C, Fernández-Reyes JL, Fidalgo MA, Font C, Francisco I, Gabara C, Galeano-Valle F, García MA, García-Bragado F, García de Herreros M, García de la Garza R, García-Díaz C, García-Mullor MM, Gil-Díaz A, Gómez-Cuervo C, Gómez-Mosquera AM, González-Martínez J, Grau E, Guirado L, Gutiérrez J, Hernández-Blasco L, Jara-Palomares L, Jaras MJ, Jiménez D, Jiménez R, Jiménez-Alfaro C, Jou I, Joya MD, Lainez-Justo S, Latorre-Díez A, Lalueza A, Lecumberri R, Lobo JL, López-Brull H, López-De la Fuente M, López-Jiménez L, López-Miguel P, López-Núñez JJ, López-Reyes R, López-Sáez JB, Lorenzo A, Lumbierres M, Madridano O, Maestre A, Marchena PJ, Marcos M, Martín-Martos F, Martínez-Urbistondo D, Mella C, Mellado M, Mercado MI, Monreal M, Muñoz-Blanco A, Muñoz-Gamito G, Morales MV, Nieto JA, Núñez-Fernández MJ, Olid-Velilla M, Otalora S, Otero R, Parra P, Parra V, Pedrajas JM, Pellejero G, Peris ML, Porras JA, Portillo J, Rivera A, Roca M, Rosa V, Ruiz-Artacho P, Ruiz-Giménez N, Ruiz-Ruiz J, Ruiz-Sada P, Salgueiro G, Sánchez-Muñoz-Torrero JF, Sancho T, Sigüenza P, Soler S, Suriñach JM, Torres MI, Trujillo-Santos J, Uresandi F, Usandizaga E, Valle R, Varona JF, Vela L, Vela JR, Villalobos A, Villares P, Zamora C, AUSTRIA: Ay C, Nopp S, Pabinger I, BELGIUM: Engelen MM, Vanassche T, Verhamme P, COLOMBIA: Esguerra G, Montenegro AC, Roa J, CZECH REPUBLIC: Hirmerova J, Malý R, FRANCE: Accassat S, Bertoletti L, Bura-Riviere A, Catella J, Chopard R, Couturaud F, Espitia O, El Harake S, Helfer H, Le Mao R, Mahé I, Moustafa F, Poenou G, Sarlon-Bartoli G, Suchon P, GERMANY: Schellong S, ISRAEL: Braester A, Brenner B, Kenet G, Tzoran I, ITALY: Basaglia M, Bilora F, Bortoluzzi C, Brandolin B, Ciammaichella M, Colaizzo D, De Angelis A, Di Micco P, Grandone E, Imbalzano E, Mastroiacovo D, Merla S, Pesavento R, Prandoni P, Siniscalchi C, Tufano A, Visonà A, Vo Hong N, Zalunardo B, LATVIA: Kalejs RV, Rusa E, Skride A, PORTUGAL: Fonseca S, Manuel M, Meireles J, REPUBLIC OF MACEDONIA: Bosevski M, Krstevski G, SWITZERLAND: Bounameaux H, Mazzolai L, USA: Caprini JA, Weinberg I, VIETNAM: Bui HM.
Coordinator of the RIETE Registry: Manuel Monreal.
RIETE Steering Committee Members: Paolo Prandoni, Benjamin Brenner, and Dominique Farge-Bancel.
RIETE National Coordinators: Raquel Barba (Spain), Pierpaolo Di Micco (Italy), Laurent Bertoletti (France), Sebastian Schellong (Germany), Inna Tzoran (Israel), Abilio Reis (Portugal), Marijan Bosevski (R. Macedonia), Henri Bounameaux (Switzerland), Radovan Malý (Czech Republic), Peter Verhamme (Belgium), Joseph A. Caprini (USA), Hanh My Bui (Vietnam).
RIETE Registry Coordinating Center: S&H Medical Science Service.
Keywords: venous thromboembolism, direct oral anticoagulants, anticoagulant therapy, predictors, RIETE, different countries
Citation: Lorenzo A, Beroiz P, Ortiz S, del Toro J, Mazzolai L, Bura-Riviere A, Visonà A, Verhamme P, Di Micco P, Camporese G, Sancho Bueso T, Monreal M and The RIETE Investigators (2022) Predictors of use of direct oral anticoagulants in patients with venous thromboembolism: Findings from the Registro Informatizado Enfermedad Tromboembólica registry. Front. Med. 9:991376. doi: 10.3389/fmed.2022.991376
Received: 11 July 2022; Accepted: 05 October 2022;
Published: 25 November 2022.
Edited by:
Alejandro Lazo-Langner, Western University, CanadaReviewed by:
Andreina Carbone, University of Campania Luigi Vanvitelli, ItalyGianluca Di Micco, Ospedale Buon Consiglio Fatebenefratelli, Italy
Copyright © 2022 Lorenzo, Beroiz, Ortiz, del Toro, Mazzolai, Bura-Riviere, Visonà, Verhamme, Di Micco, Camporese, Sancho Bueso, Monreal and the RIETE Investigators. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alicia Lorenzo, YWxpY2lhLmxvaGVyQGdtYWlsLmNvbQ==
†A full list of RIETE investigators is given in Appendix