 Christopher Neuhaus
Christopher Neuhaus Petra Grawe2
Petra Grawe2- 1Department of Anesthesiology, Heidelberg University Hospital, Heidelberg, Germany
- 2Department of Anesthesiology, University Hospital Erlangen, Erlangen, Germany
- 3Division of Risk Management and Societal Safety, Lund University, Lund, Sweden
Background: Patient safety gained public notoriety following the 1999 report of the Institute of Medicine: To Err is Human – Building a Safer Health System which summarized a culminated decades' worth of research that had so far been largely ignored. The aim of this study was to analyze the report's impact on patient safety research in anesthesiology.
Methods: A bibliometric analysis was performed on all anesthesiologic publications from 2000 to 2019 that referenced To Err Is Human. In bibliometric literature, references are understood to represent an author's conscious decision to express a relationship between his own manuscript and the cited document.
Results: The anesthesiologic data base contained 1.036 publications. The journal with the most references to the IOM report is Anesthesia & Analgesia. By analyzing author keywords and patterns of collaboration, changes in the patient safety debate and its core themes in anesthesiology over time could be visualized. The generic notion of “error,” while initially a central topic in the scientific discourse, was subsequently replaced by terms representing a more granular, team-oriented, and educational approach. Patient safety research in anesthesia, while profiting from a certain intellectual and conceptual head start, showed a discursive shift toward more managerial, quality-management related topics as observed in the health care system as a whole.
Conclusions: Over the last 20 years, the research context expanded from the initial focus set forth by the IOM report, which ultimately led to an underrepresentation of research on critical incident reporting and systemic approaches to safety. Important collaborations with safety researchers from outside of health care dating back to the 1990's were gradually reduced, while previous research within anesthesiology was aligned with a broader, more managerial patient safety agenda.
Introduction
Anesthesiology is generally acknowledged to have achieved order of magnitude improvements in safety in the comparatively short time span of a few decades. While much of that success is commonly attributed to technological innovation, a more complex story fortifies its role as vanguard of the modern patient safety movement (1) beginning with the seminal 1978 study by Cooper et al. (2).
In the wake of the 1979 nuclear disaster of the Three Mile Island reactor in Pennsylvania (and various other highly visible accidents) the multidisciplinary research tradition of safety science gained momentum, generating a plethora of concepts about work in complex sociotechnical systems and a new understanding of “human error” (3). While generally unrecognized, anesthesiology was likely the first healthcare specialty to tap into this rich body of knowledge generated through research methodology foreign to medicine. Ultimately, this resulted in practice innovation and substantial progress in anesthetic patient safety that by far exceeded the benefits of technology alone (4).
On a broader scale, patient safety gained public notoriety following the 1999 report of the Institute of Medicine (IOM): To Err is Human – Building a Safer Health System (5) which summarized a culminated decades' worth of research that had so far been largely ignored. The comprehensively researched information, in combination with alarming “body counts” (6) and interpretations by the IOM shocked the public, elevated the occurrence of patient harm to the level of an epidemic health crisis, spawned research on patient safety, and initiated a discursive change in the patient safety debate.
On the occasion of the IOM report's 20th anniversary, we previously analyzed the academic impact the report had on global efforts in patient safety research (7). As anesthesiology initially sought the cooperation with human factor specialists, it is conceivable that the report created an academic momentum in this particular specialty different to the rest of the medical field. The aim of this study was to gain a comprehensive and systematic understanding of the academic impact and momentum the IOM report created within anesthesiology by applying bibliometric methods. This assumes that any publication referencing To Err Is Human is most likely conceptually or discursively influenced by the IOM report.
Materials and methods
Bibliographical methods
Methodologically, it is possible to assess and measure scientific impact by applying bibliometrics to scientific publications stored or indexed in big bibliographic databases (8). Bibliometrics provides robust analyses of large amounts of published research by applying mathematical and statistical methods in the study of the use of documents and publication patterns. The two main methods commonly applied in bibliometric studies are performance analysis and science mapping (8, 9): Performance analysis (10) aims to evaluate the research and publication performance of scientific actors (i.e., individuals, institutions, countries) by analyzing bibliographic coupling (11) and co-citation patterns (12).
Science mapping uses bibliometric methods to assess the social, intellectual, and conceptual structure of a research field and describe its knowledge base. This is done by analyzing the publications' meta data about authors, institutions, and countries (13, 14), the co-citation networks among publications (12) and by means of co-words analysis (15). We described the bibliometric methods applied to this study in great detail in a previous publication (7). Based on the study design, the study was exempted from approval by the University of Heidelberg Ethics Review Board.
Data collection and analysis
The data for this study were retrieved from Scopus (www.scopus.com, Elsevier B.V., Amsterdam, NL) on July 7th, 2020. By using the “references” filter and the query “to err is human” in the Scopus database, all documents bibliographically coupled to the IOM report from 1999–2019 were retrieved. The search results returned all essential bibliographic information (e.g., title, author's names and affiliations, abstracts, keywords, references) and were exported and stored in two different formats: BibTeX –files (*.bib) for import into the bibliometric application Biblioshiny (Bibliometric analysis program “Bibliometrix,” designed by Aria M. and Cuccurullo C. 2017) and *.ris-files for import into the citation management software Endnote X8 (Clarivate Analytics). Publications from the field of anesthesiology were identified in Endnote X8 using the query „anesthe*” and „anaesthe*”. As Biblioshiny cannot preprocess imported data, the publications from the field of anesthesiology identified in Endnote served as basis for further manual selection within the BibTeX–files. For this purpose, the *.bib-files were imported into the unicode editor Texmaker (https://www.xm1math.net/texmaker/), which allowed to manually delete files not belonging to the database.
Analyses were carried out using the open-source R-based tool bibliometrix (16) and its web user interface biblioshiny (17). Due to a large variety in reference notation (e.g., the IOM report Crossing the Quality Chasm (2001) is referenced with 2.322 (!) different entries), biblioshiny's query results for the most locally cited references had to be completed manually. For that purpose, the data base was searched for the exact title of biblioshiny's suggested top results and additional references were identified. References pointing toward the most relevant safety scientists were found by searching the data base for their family names and by manually identifying documents with the correct surname.
The workflow adheres to the applicable EQUATOR guidelines (Standards for Reporting Qualitative Research SRQR) and is illustrated in Figure 1.
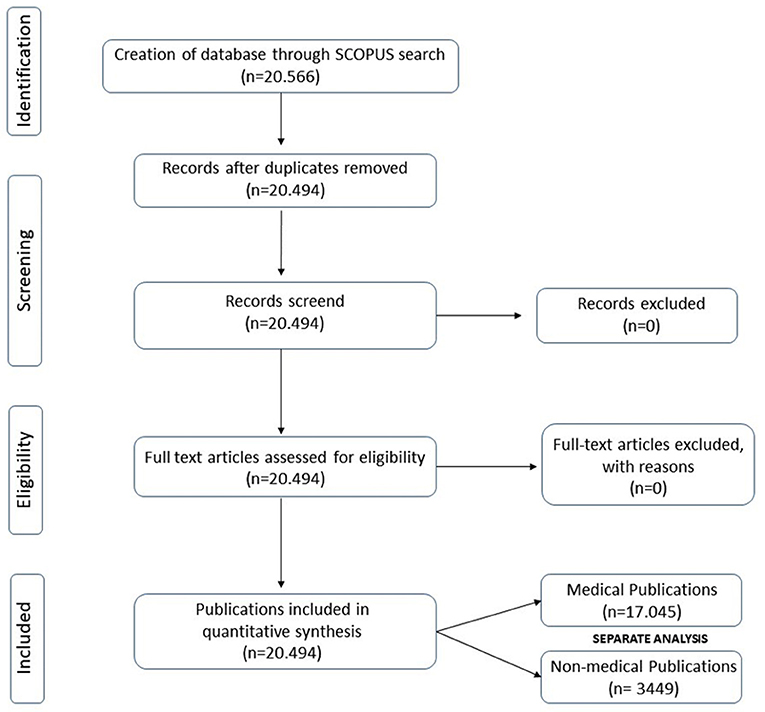
Figure 1. SRQR flow diagram of the identification, screening and inclusion of source documents. Publications were subsequently separated in to medical and non-medical documents for further analysis.
Results
The Scopus database search resulted in 20.566 matching documents. The anesthesiologic data base contained 1.036 publications (Table 1). Our analysis covers the scientific production period of 2000–2019. The number of publications citing the IOM report increased steadily from 2000 to 2012. After 2012, we observed a declining trend (Figure 2).
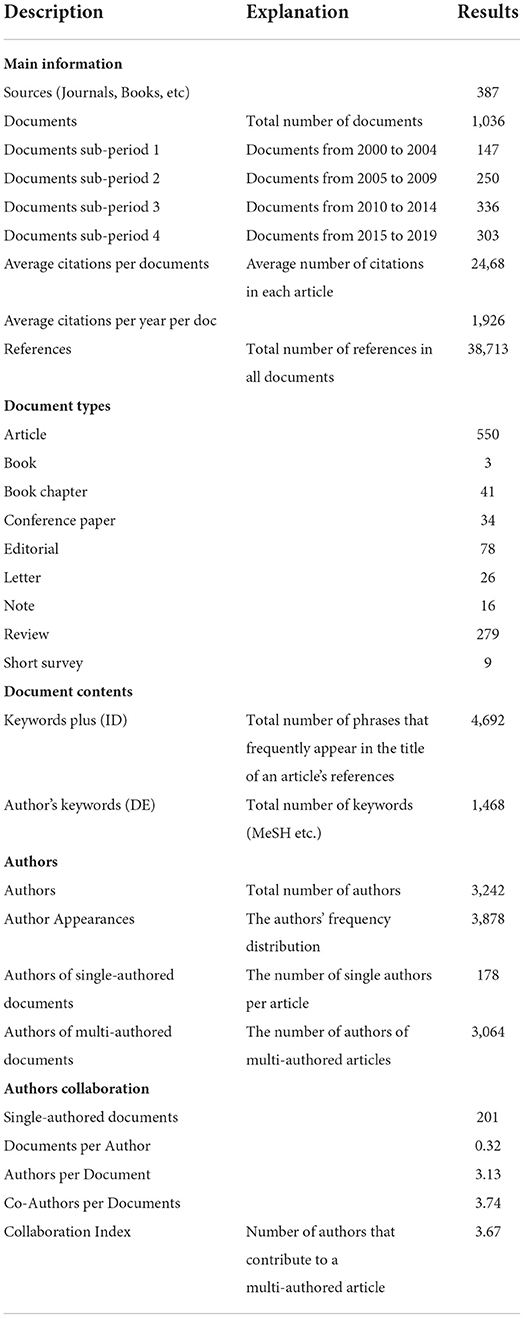
Table 1. Main bibliographical information.
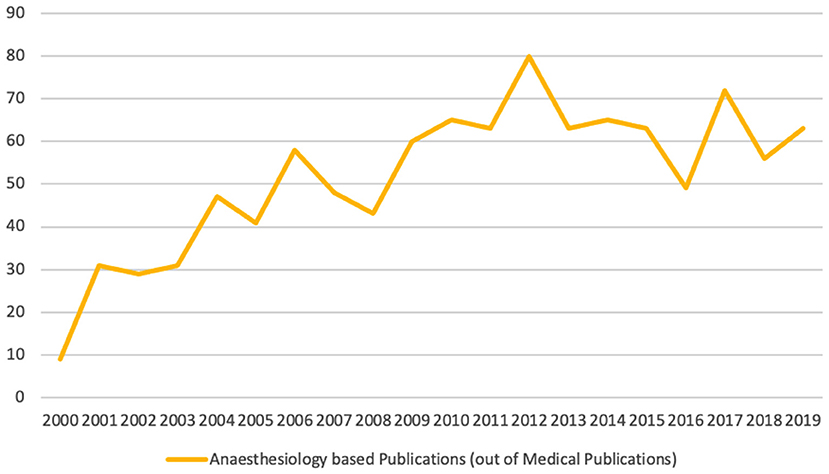
Figure 2. Number of anesthetic publications per year citing To Err Is Human.
Highly influential authors and papers
Table 2 lists the twenty most influential authors, sorted both in terms of total number of publications they authored or co-authored and in terms of number of citations authors received within our database (i.e., locally cited authors). Only three authors published more than 10 articles, while 87% (n = 2.877) published only one article. The author with the biggest academic impact (22 articles, h-index 12, g-index 21) is Merry AF.
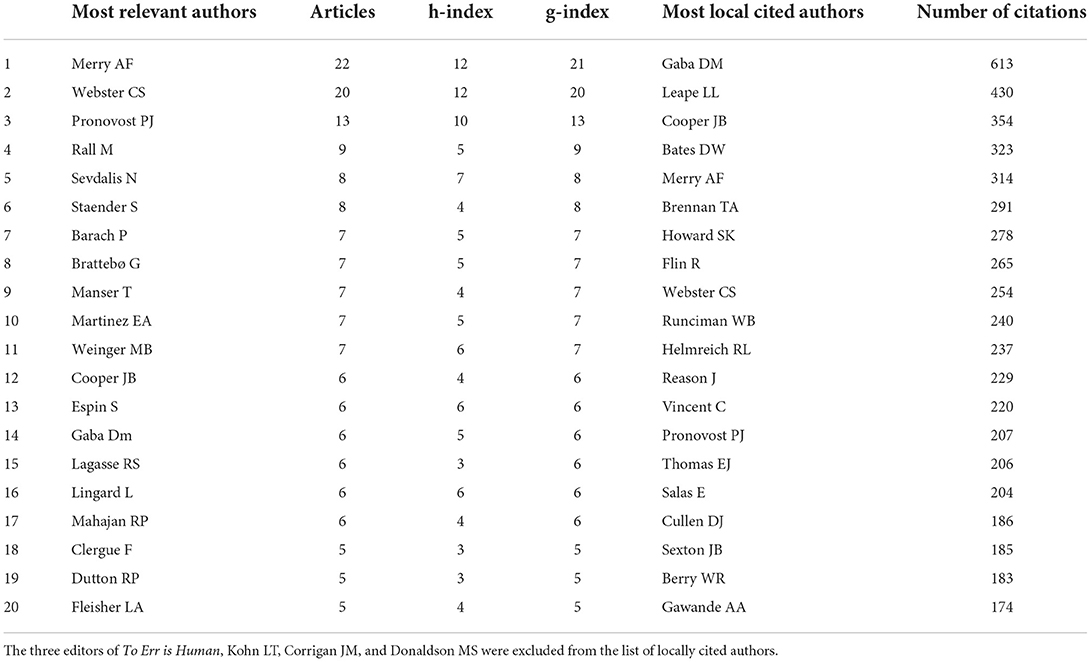
Table 2. The 20 most relevant authors with the number of articles citing To Err is Human and the 20 most locally cited authors from 2000 to 2019.
Six of the 20 most influential authors are among the most locally cited authors (within the dataset). Some authors, while often cited, published less documents referencing To Err is Human (e.g., Gaba DM, who is #1 of locally cited authors but only #14 of the most relevant authors in the database). Other authors are cited most likely for their theoretical framework that help understand patient safety (e.g., Vincent C or Reason J). Both authors, Merry AF und Webster CS, showed near constant annual publications, while Pronovost PJ was active in anesthesiology from 2000 to 2012, with a highly cited article in 2006 (Figure 3).
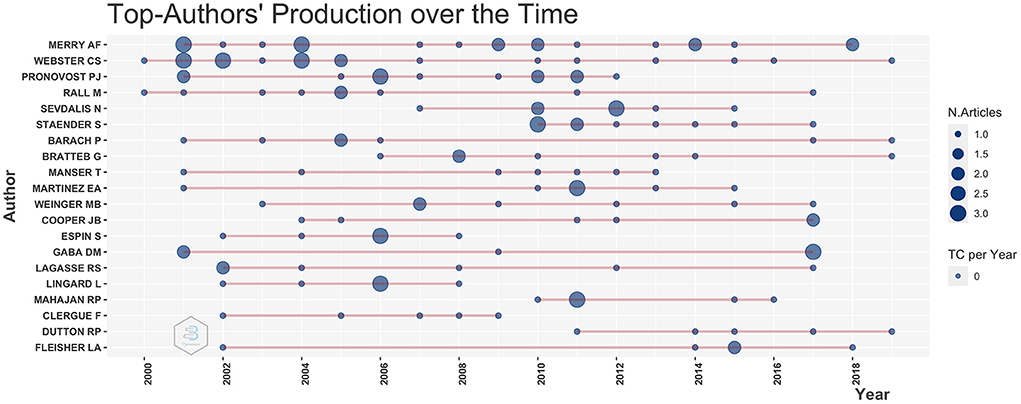
Figure 3. The 20 top-author's production over time. The line represents an author's timeline. The bubble size is proportional to the number of documents published, and the color intensity is proportional to the total citations per year the documents collected.
Publications citing the IOM report
The 1.036 documents included in the bibliographic collection were published in 387 sources (Table 2). The majority of these were published as peer reviewed articles (53%), followed by reviews (27%), books and book chapters (4%). The remaining documents included conference papers, short surveys and editorials. The most references to the IOM report were found in the journal Anesthesia & Analgesia. The most impactful journal was Anesthesiology with a total of 1.893 citations received (Table 3). The dynamics of publications over time for journals is shown in Figure 4. It visualizes the growing relevance of Anesthesia & Analgesia between 2009 and 2015. Starting in 2017, three other journals surpassed Anesthesia & Analgesia in terms of publications linked to the IOM report.
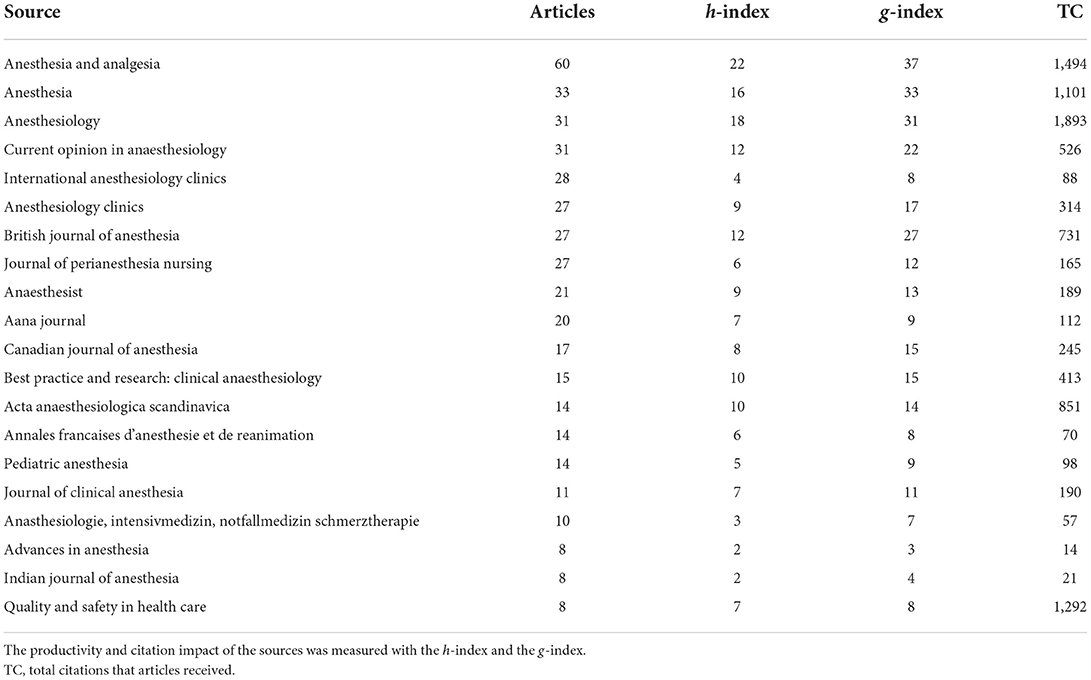
Table 3. The top 10 journals in which To Err is Human was cited.

Figure 4. Annual occurrences of publications in the most relevant sources. To enhance legibility of the plot, the number of source dynamics was restricted to the 10 most relevant journals.
Global distribution and cooperation
The origin of 867 documents (83.7%) could be linked to 49 different countries, while 16.3% of documents were devoid of geographical information. Institutions from 3 countries (USA, Germany, UK) were responsible for most of the scientific output (68%), while most countries contributed with only one to five articles (Table 4).

Table 4. Table, corresponding author's country, publication activity and frequency of international collaboration (2000–2019).
Most documents were published by a single academic center (SCP), while multi-center publications (MCP) made up only a small fraction of publications. The US features both: the highest publication activity and the lowest international collaboration rate (MCP-ratio of 0.05). As visualized in Figure 5, most collaboration existed between North America, Europe, and Australia. Less contribution could be identified for authors from Latin America, Africa, Asia, and India.
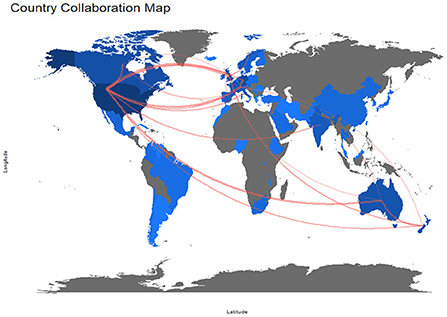
Figure 5. Map of international collaborations between 2000 and 2019. Every line represents a collaboration between institutions in two different countries. To better illustrate the pattern, only national collaborations with more than 10 joint publications in both decades are shown. The color intensity of blue is proportional to the number of publications of the country. Countries in gray did not publish any article that references To Err Is Human.
Regarding the institutional affiliations, the leading academic institutions were mostly located in North America, the most influential being Harvard Medical School (Table 5).
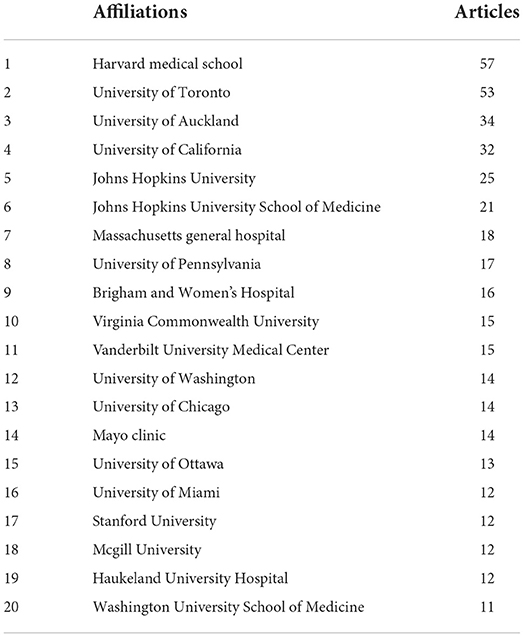
Table 5. The top 20 leading institutions regarding publications and citations liked to the IOM report.
Relevance and citation analysis
The analysis of citation and co-citation patterns of documents is of interest because a significant contribution to a scientific field can be assumed for frequently quoted papers. Also, papers that are more often cited together by other publications are more likely to relate to a shared subject area (8). Consequently, a change over time in the most locally cited references may be indicative of a shift in the thematic priority of patient safety. Table 6 lists the 20 most locally cited references between 2000 to 2019. To add granularity and better interpret thematic developments over time, Table 7 shows the 20 most local cited references in 5-year increments.
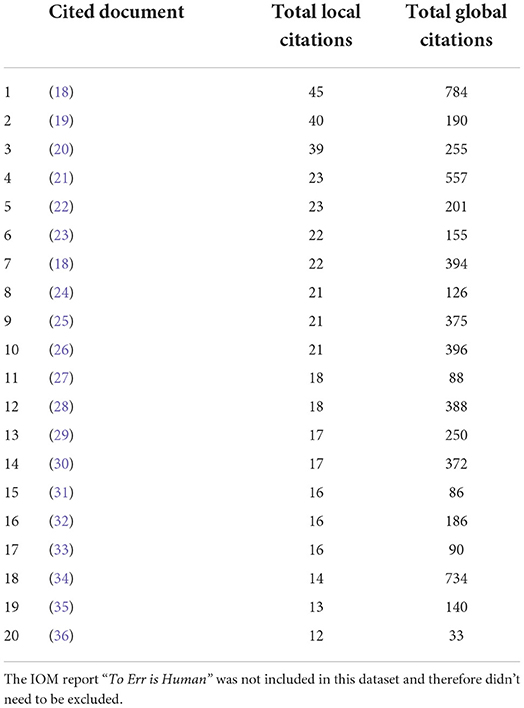
Table 6. The 20 most locally cited references within the anesthesiologic dataset between 2000 and 2019.
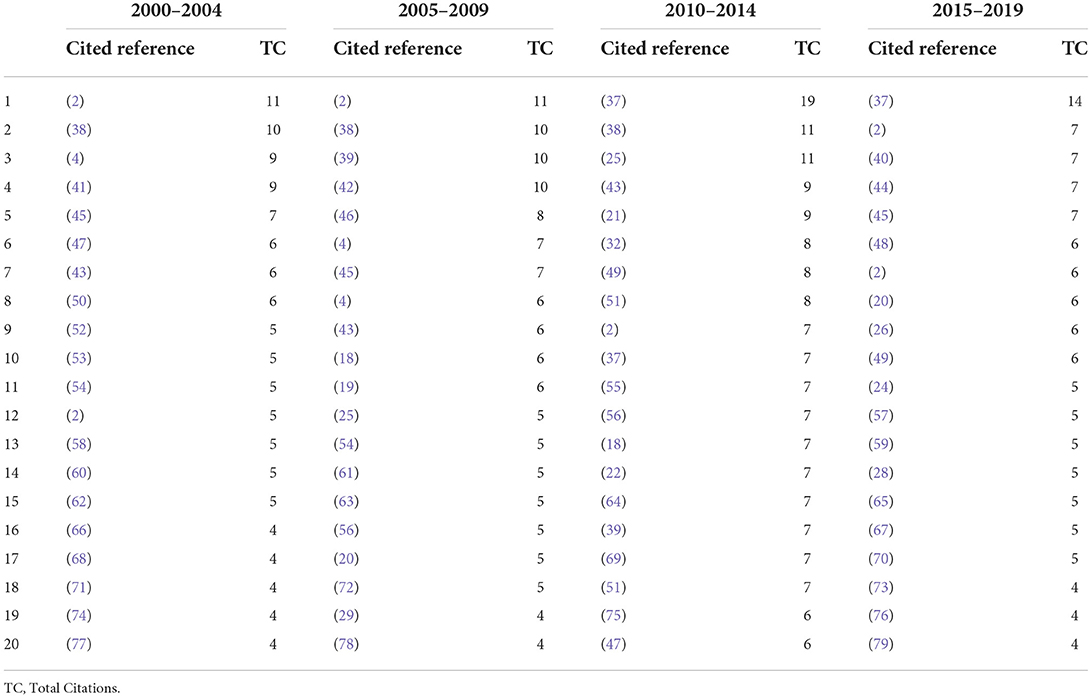
Table 7. The 20 most locally cited references within the anesthesiologic dataset between 2000 – 2019, sorted in 5-year increments for higher granularity.
While published long before the IOM-report, “An analysis of major errors and equipment failures in anesthesia management: considerations for prevention and detection” by Cooper et al. (38) remained the most (2000–2009) or second-most (2010–2019) cited article in the anesthesiologic dataset. A discursive shift toward increasing interest in checklists is manifested by the Safe-Surgery-Saves-Lives-Study-Group paper “A surgical safety checklist to reduce morbidity and mortality in a global population” (37), showing the most local citations in the 2010–2019 period. When examining the 20 most relevant authors, David Gaba is by far the most influential contributor with 613 local citations (Table 8). The perceived predominance of certain theoretical frameworks in anesthesia, such as the “Swiss Cheese” metaphor for system failure and “Non-technical skills/CRM” are underscored by the high ranking of authors like James Reason and Rhona Flin.
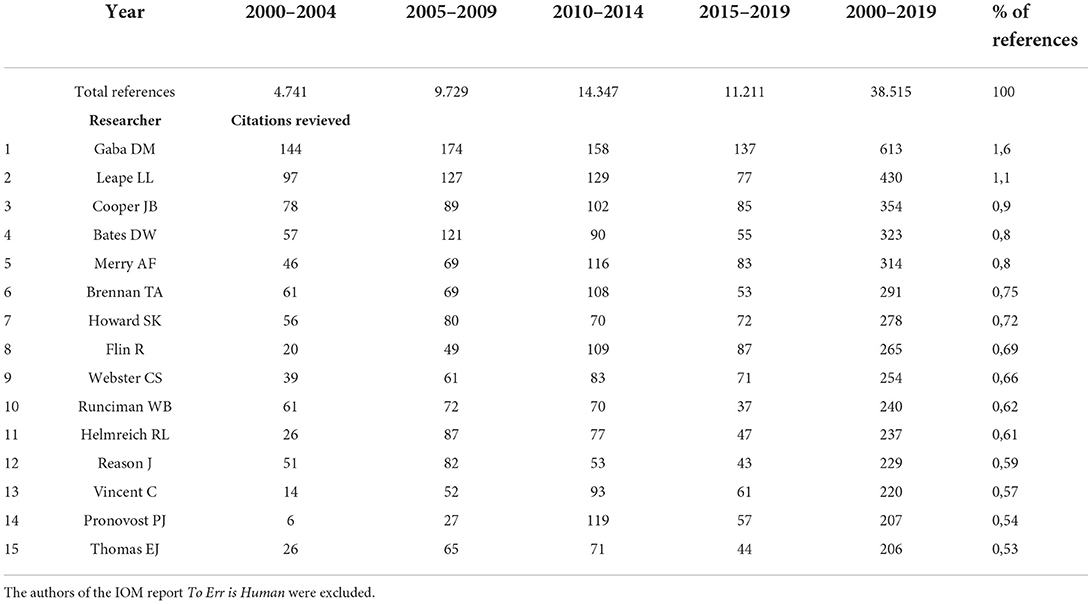
Table 8. Overview of the 20 most locally cited authors within the anesthesiologic dataset.
Co-word analysis and thematic evolution
One of the aims of this study is to identify and visualize the main concepts that patient safety researchers in anesthesiology connected with the IOM report and to analyze how research content and orientation might have expanded or narrowed over time. To best capture the scientific content stored in the database, the parameters ”author keywords,” “Keywords Plus,” “titles of publications,” and “abstracts” were applied to compare the top twenty words of the sub-periods. We aggregated interchangeable terms into a single primary category (e.g., “errors,” “error,” “medical error”).
A comparison of Keywords Plus showed a 64.5% overlap of key terms. The most common terms were: “adult,” 84anesthesia,” “anesthesiologist,” “male,” “female,” “human(s)”, “healthcare quality,” “United States,” and “patient care.” However, beginning in 2010 two new terms emerged: “education” and “simulation training.” The term “clinical competence” was present since 2004, which is in stark contrast to non-anesthesiologic patient safety literature (7).
A comparison of the abstract words showed an 62.5% overlap of key terms within all four data bases. The most common terms were “an(a)esthesia,” “adverse,” “clinical,” “care,” “error(s)“, 84events,” “patient(s)”, “training,” and “health”.
The top twenty title words showed a 55% overlap, with the most common terms being “safety”, “care,” “patient,” “management,” “errors,” “simulation” and “training.” From 2010 onward, the terms “perioperative,” “review,” “checklist,” “team” and “practice” signify a thematic development. This also applies to Author keywords (63% overlap), which displayed a thematic evolution: “patient safety,” “education,” “crisis management” and “simulation” were supplemented by “perioperative care,” “quality improvement” and “teamwork” starting in 2010.
Based on the keywords that authors provide to characterize their research, it is possible to create a co-occurrence network that reveals the conceptual structure of a research area and to visualize them on a strategic diagram with its two dimensions of centrality and density (80). While centrality measures the intensity of a given cluster's links with other clusters, density characterizes the strength of the links that tie the words making up the cluster together. All clusters can be divided into four general categories by ordering them horizontally (along the x-axis) by increasing order of centrality, and vertically (along the y-axis) by increasing order of density (Figure 6). If the time span is futher differentiated into different time slices, a dynamic analysis based on the synthetic and simplified presentation of the network's morphology is possible.
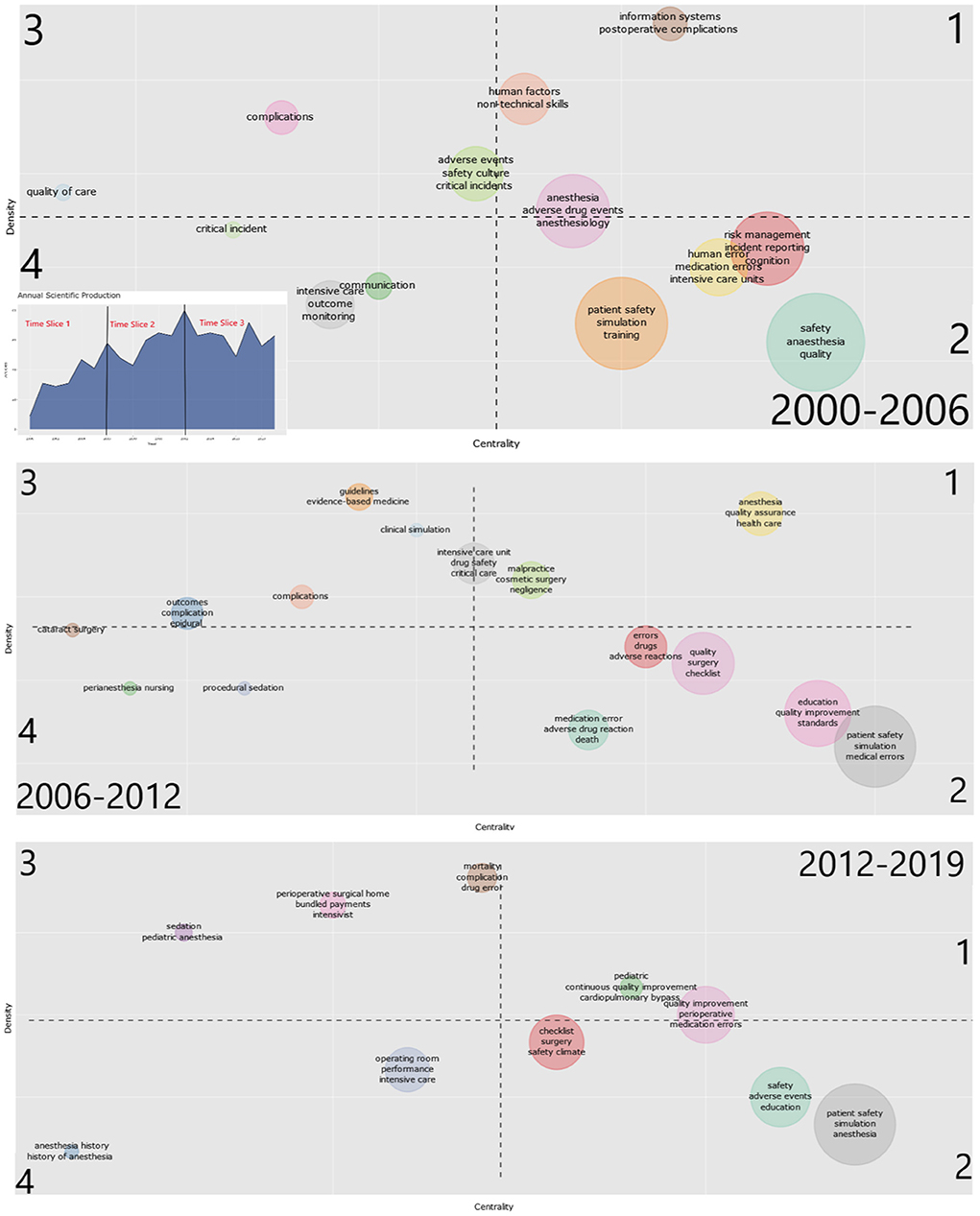
Figure 6. Strategic diagram of the 2000–2006, 2006–2012, and 2012–2019 sub-periods. The numbers indicate the type of clusters defined by their centrality and density as proposed by Michel Callon (80). Each cluster is labeled with the corresponding three most frequent keywords within the cluster. Inserted figure: Distribution of documents per year with 2 cutting points at the two publication peaks in 2006 and 2012. The cluster colors were randomly assigned by biblioshiny and therefore differ across subperiods.
During the first period (2000–2006, Figure 6), the most highly developed cluster that had been dealt with systematically over a longer period (quadrant 1) is research on information systems and postoperative complications as well as adverse drug events. Central themes, but with weaker internal correlations, are quality and safety issues in anesthesia. The study of error in a variety of forms and settings and the role of incident reporting are emerging as central themes with weaker internal correlations (quadrant 2), underscoring the pioneering influence of anesthesia when compared to a more general medical database (7).
During the second sub-period (2006–2012, Figure 6), previously underdeveloped topics started to become more central to the scientific debate, such as medication safety and intensive care; the latter being catapulted from decentralized and poorly recognized subject to focus of contested debate within only a few years. Moreover, publications concerning the use and merit of guidelines and evidence-based medicine emerged as strongly linked and became more central.
In the third sub-period (2012–2019, Figure 6), yet another discursive shift can be recognized, with quality-related topics (e.g., management, improvement, performance) more central than ever to the scientific debate. The cluster comprising simulation and medical education remains important, however many of the previously found topics closely associated (e.g., non-technical skills, human factors, safety culture) are no longer represented. Almost two decades after the release of To Err Is Human, “errors” remain central to the debate (quadrant 1 and 2), with an emphasis on medication errors. Also, perioperative communication, often linked to checklists, retain an important position in the scientific landscape, although many publications exist since 2004. Interest in other core topics previously in the spotlight, like intensive care, fades quickly and is seemingly replaced by a more managerial agenda.
Discussion
The current study aimed to gain an understanding of the impact of the IOM report To Err Is Human on patient safety research in anesthesiology, to identify the research activity explicitly related to this seminal publication and to see how the ideas presented in To Err Is Human might have affected the diversity of the safety science discourse in anesthesiology over the last 20 years. Therefore, bibliometric methods were applied to a data set which was linked to the IOM report through a reference (i.e., bibliographic coupling). This constitutes an established methodological approach in bibliometric literature, where references are understood to represent an author's conscious decision to express a relationship between his own manuscript and the cited document (81), rather than a random event or mere bibliographic data at the end of a manuscript.
Core themes and resulting changes in the patient safety discourse over time were visualized on a strategic diagram by applying a clustering algorithm on the co-occurrence network of author keywords. One noticeable result of our analysis is the observation that “errors,” while initially a core topic in the scientific discourse within the anesthetic database, are subsequently replaced by terms representing a somewhat more granular, team-oriented and educational approach. Contrary to the perceived tendency of healthcare to reframe the problem of medical harm into the problem of “human error” as an objectively identifiable, measurable and countable, unique category of human performance (7), these findings underscore a central argument of Wears and Sutcliffe (1) about “the special case of anesthesia” within the patient safety discourse: In the two decades preceding the IOM report, anesthesiologists had already developed substantive and sustained partnerships with the safety sciences. Human factors professionals were not merely consultants on a clinical research project but rather embedded within departments, combining forces with clinicians to learn about managing the complexities and risks of anesthetic practice (82, 83). In following this research tradition and contrary to the broader patient safety movement, anesthesia seemed less distracted by “fruitless and sterile” efforts of eliminating errors (1), likely influenced by the emerging consensus among safety scientists that errors had to be interpreted rather as symptoms than causes and were representative of deeper trouble within complex adaptive systems that required further investigation rather than elimination (3, 84). When comparing the data from the co-word analysis with the arguments of To Err is Human, this is remarkable, as the initial development within anesthesia was in line with the IOM report's stated objective of moving the focus from individual errors to systemic issues; adverse events were understood as a property of a system of care rather than the result of deficient health care professionals.
However, our findings also indicate that patient safety related research in anesthesia, while profiting from a certain intellectual and conceptual head start, was not immune to a discursive shift toward more managerial, quality-management related topics as observed in the health care system as a whole (7). These topics were representative for a type of scientific-bureaucratic medicine with strong conceptual roots in public health and epidemiology and the explicit valuing of aggregate data over individual cases, as exemplified by the movements for clinical practice guidelines and evidence-based medicine.
Consequently, the mainstream patient safety movement seems to have gradually taken over safety approaches in anesthesia, dominated by a narrative of competence and control that implicitly pushed back on outside intervention (85), effectively silencing the diversity that had created progress in the first place.
The most frequently cited safety scholar in our database was James Reason (39, 45). While the IOM report mentions a variety of safety theories and frameworks, the heavy emphasis on Reason's work together with a tendency of medical professionals to oversimplify theoretical foundations in safety science might have inadvertently contributed to what can be characterized as a consolidation of the error narrative. The models proposed by Reason (39, 45, 86, 87) provided medical metaphors (e.g., resident pathogens) as well as memorable graphical representations (e.g., Swiss Cheese Model) that resonated well with health care providers, and created the impression of an intuitive simplicity which made clinicians believe that they had understood the model when in fact they hadn't (88). Instead of developing a systems approach in healthcare based on the systemic aspects of Reason's framework (89), patient safety research by clinicians ended up becoming just another attack on “human error,” a focus implicitly encouraged by the title of James Reason's bestselling book.
Also, it is surprising to note the low presentation of research on incident reporting. Given the importance the IOM report placed on mandatory and voluntary reporting systems, it is remarkable that only the early years after publication of the IOM report show much research focusing on incident reporting or reporting systems. We explicitly checked the frequency of the term “reporting” in the document titles during all four sub-periods to compensate for limitations with relying on author keywords, however the results confirmed the initial findings that research on incident reporting was not a key concern in any of the clusters. As with the discussion about research traditions, it again seems as if anesthesia, after a perceived head start due to independent research efforts during the 1980's and 1990's, had become increasingly aligned with a broader patient safety agenda dominated by health professionals focused on programmatic activity that was more concerned with the large-scale transfer of interventions successful in other fields (e.g., checklists from aviation) than the contextual understanding of their internal mechanisms (90).
Limitations
The main limitation of this study, both regarding the records identified through database searching and in thematic diversity, is that the data set was limited to documents referencing To Err Is Human. Therefore, the results do not claim to portray a comprehensive picture of all the research on patient safety done since To Err Is Human was first published, but rather reflect the analysis of a specific subgroup of those authors that have identified and referenced a connection between their work and the arguments presented in the IOM report. This is based on the assumption that a reference to the IOM report in our data base represents the conscious decision made by an author to connect a particular argument in the document he was writing to the work he was citing (81). Despite all the arguments in the bibliometric literature claiming reliable reference motives, it is conceivable that many authors cited the publication of To Err is Human as global representation of a new era in patient safety research rather than referring to a specific argument within the IOM report. In this case, the point of reference would not be the content of the report, but rather the historical impact it had on subsequent years. Unfortunately, the bibliometric method itself does not allow any discrimination between both possibilities.
Another potential limitation regarding the analysis of the academic discourse on patient safety is the inclusion of other documents such as book chapters, conference papers, and editorials rather than peer-reviewed manuscripts only in our data base. This approach was chosen to gain a comprehensive impression of the academic impact as reflected in the variety of written communications that constitute the exchange and development of scientific ideas. A focus on the assessment of the academic quality would have made the restriction to high-quality, peer reviewed journals mandatory.
Conclusion
The current study contributes to an understanding of the seminal IOM report's scientific impact on patient safety research in anesthesiology from 2000 to 2019. During this period, the research context expanded from the initial focus set forth by the report, which ultimately led to an underrepresentation of research on a systems approach and incident reporting. Important collaborations with safety researchers from outside of health care dating back to the 1990's were gradually reduced, while previous research within anesthesiology was aligned with a broader, more managerial patient safety agenda. For future safety efforts, anesthesiologists might be well-advised to rekindle these old collaborations to resume a vanguard role in patient safety research. This will also entail renewed discussions about the understanding and role of “human error,” harnessing expertise from domains outside of healthcare, and a reluctance to simplify human interactions within complex systems into easily digestible bites that might suit safety campaigns and managerial agendas but fall short in addressing the needs of patients and practitioners alike.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: www.scopus.com; using the search terms as specified in the methods section.
Author contributions
CN: conceptualization, formal analysis, validation, and writing—original draft. PG: investigation, data curation, and formal analysis. JB: conceptualization, supervision, and writing—review and editing. MS: conceptualization, validation, supervision, and writing—review and editing. All authors contributed to the article and approved the submitted version.
Funding
For the publication fee we acknowledge financial support by Deutsche Forschungsgemeinschaft (DFG) within the funding programme Open Access Publikationskosten as well as by Heidelberg University.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Wears B, Sutcliffe KM. Still Not Safe. Patient Safety and the Middle-Managing of American Medicine: Oxford University Press (2020). doi: 10.1093/oso/9780190271268.001.0001
2. Cooper JB, Newbower RS, Long CD, McPeek B. Preventable anesthesia mishaps: a study of human factors. Anesthesiology. (1978) 49:399–406. doi: 10.1097/00000542-197812000-00004
3. Woods DD, Dekker S, Cook R, Johannesen L, Sarter N. Behind Human Error. 2nd ed. Farnham: Ashgate (2010). XX, 271 S. p.
4. Gaba DM. Anaesthesiology as a model for patient safety in health care. Bmj. (2000) 320:785–8. doi: 10.1136/bmj.320.7237.785
5. Kohn L, Corrigan J, Donaldson M, editors. To Err Is Human: Building a Safer Health System. Committee on Quality of Health Care in America, Institute of Medicine (Iom). Washington DC: National Academy Press (1999).
6. Loeb JM, O'Leary DS. The Fallacy of the Body Count: Why the Interest in Patient Safety and Why Now. In:Youngberg BJ, Hatlie M, , editors. The Patient Safety Handbook. Sudbury, MA: Jones and Bartlett Publishers (2004). p. 83-94.
7. St.Pierre M, Grawe P, Bergstrom J, Neuhaus C. 20 years after to err is human: a bibliometric analysis of ‘the iom report's' impact on research on patient safety. Safety Sci. (2022) 147:105593. doi: 10.1016/j.ssci.2021.105593
8. Gutiérrez-Salcedo M, Martínez MÁ, Moral-Munoz JA, Herrera-Viedma E, Cobo MJ. Some bibliometric procedures for analyzing and evaluating research fields. Appl Intell. (2018) 48:1275–87. doi: 10.1007/s10489-017-1105-y
9. Zupic I, Cater T. Bibliometric methods in management and organization. Organ Res Methods. (2014) 18:429–72. doi: 10.1177/1094428114562629
10. Peters H, Van Raan A. Structuring scientific activities by co-author analysis: an exercise on a university faculty level. Scientometrics. (1991) 20:235–55. doi: 10.1007/BF02018157
11. Kessler MM. Bibliographic coupling between scientific papers. Am Doc. (1963) 14:10–25. doi: 10.1002/asi.5090140103
12. Small H. Co-citation in the scientific literature: a new measure of the relationship between two documents. J Am Soc Inform Sci. (1973) 24:265–9. doi: 10.1002/asi.4630240406
13. Aria M, Misuraca M, Spano M. Mapping the evolution of social research and data science on 30 years of social indicators research. Soc Indic Res. (2020) 149:803–31. doi: 10.1007/s11205-020-02281-3
14. Glänzel W, Schubert A. Analysing Scientific Networks through Co-Authorship. In:Moed HF, Glänzel W, Schmoch U, , editors. Handbook of Quantitative Science and Technology Research. Dordrecht: Kluwer Academic Publishers (2004). p. 257-76. doi: 10.1007/1-4020-2755-9_12
15. Callon M, Courtial J-P, Turner WA, Bauin S. From translations to problematic networks: an introduction to co-word analysis. Social Science Information. (1983) 22:191–235. doi: 10.1177/053901883022002003
16. Aria M, Cuccurullo C. Bibliometrix: an R-tool for comprehensive science mapping analysis. J Informetr. (2017) 11:959–75. doi: 10.1016/j.joi.2017.08.007
17. Moral-Muñoz JA, Herrera-Viedma E, Santisteban-Espejo A, Cobo MJ. Software tools for conducting bibliometric analysis in science: an up-to-date review. El Profesional de la Información. (2020) 29:e290103. doi: 10.3145/epi.2020.ene.03
18. Lingard L, Espin S, Whyte S. Communication failures in the operating room: an observational classification of recurrent types and effects. Qual Saf Health Care. (2004) 13:330–4. doi: 10.1136/qshc.2003.008425
19. Webster CS, Merry AF, Larsson L, Mcgrath KA, Weller J. the frequency and nature of drug administration error during anesthesia. Anesth Int Care. (2001) 29:494–500. doi: 10.1177/0310057X0102900508
20. Lagasse RS. Anesthesia safety: model or myth? A review of the published literature and analysis of current original data. Anesthesiology. (2002) 97:1609–17. doi: 10.1097/00000542-200212000-00038
21. Manser T. Teamwork and patient safety in dynamic domains of healthcare: a review of the literature. Acta Anaesthesiol Scand. (2009) 53:143–51. doi: 10.1111/j.1399-6576.2008.01717.x
22. Mellin–Olsen J, Staender S, Whitaker DK, Smith AF. The Helsinki declaration on patient safety in anaesthesiology. Eur J Anaesthesiol. (2010) 27:592–7. doi: 10.1097/EJA.0b013e32833b1adf
23. Jensen LS. Evidence–based strategies for preventing drug administration errors during anesthesia. Anesthesia. (2004) 59:493–504. doi: 10.1111/j.1365-2044.2004.03670.x
24. Abeysekera A, Bergman IJ, Kluger MT, Short TG. Drug error in anesthetic practice: a review of 896 reports from the australian incident monitoring study database. Anesthesia. (2005) 60:220–7. doi: 10.1111/j.1365-2044.2005.04123.x
25. Amalberti R, Auroy Y, Berwick D, Barach P. Five system barriers to achieving ultrasafe health care. Ann Intern Med. (2005) 142:756–64. doi: 10.7326/0003-4819-142-9-200505030-00012
26. Makary MA, Daniel M. Medical error–the third leading cause of death in the US. Bmj. (2016) 353:I2139. doi: 10.1136/bmj.i2139
27. Merry AF. A new, safety–oriented, integrated drug administration and automated anesthesia record system. Anesth Analg. (2004) 93:91. doi: 10.1213/00000539-200108000-00030
28. Mazzocco K, Petitti DB, Fong KT. Surgical team behaviors and patient outcomes. Am J Surg. (2009) 197:678–85. doi: 10.1016/j.amjsurg.2008.03.002
29. Awad SS, Fagan SP, Bellows C. Bridging the communication gap in the operating room with medical team training. Am J Surg. (2005) 190:770–4. doi: 10.1016/j.amjsurg.2005.07.018
32. Mahajan RP. Critical incident reporting and learning. Br J Anaesth. (2010) 105:69–75. doi: 10.1093/bja/aeq133
33. Merry AF. Multimodal system designed to reduce errors in recording and administration of drugs in anesthesia: prospective randomized clinical evaluation. Bmj. (2004) 22:343. doi: 10.1136/bmj.d5543
34. Zhan C. Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization. J Am Med Assoc. (2004) 290:1868–74. doi: 10.1001/jama.290.14.1868
35. Flin R. Anaesthetists' attitudes to teamwork and safety. Anesthesia. (2004) 58:233–42. doi: 10.1046/j.1365-2044.2003.03039.x
36. Merry AF. Evaluation in an anesthetic simulator of a prototype of a new drug administration system designed to reduce error. Anesthesia. (2004) 57:256–63. doi: 10.1046/j.0003-2409.2001.02397.x
37. Haynes AB, Weiser TG, Berry WR, Lipsitz SR, Breizat AH, Dellinger EP, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. (2009) 360:491–9. doi: 10.1056/NEJMsa0810119
38. Cooper JB, Newbower RS, Kitz RJ. An analysis of major errors and equipment failures in anesthesia management: considerations for prevention and detection. Anesthesiology. (1984) 60:34–42. doi: 10.1097/00000542-198401000-00008
39. Reason J. Human error: models and management. West J Med. (2000) 172:393–6. doi: 10.1136/ewjm.172.6.393
40. Gawande AA, Thomas EJ, Zinner MJ, Brennan TA. The incidence and nature of surgical adverse events in Colorado and Utah in 1992. Surgery. (1999) 126:66–75. doi: 10.1067/msy.1999.98664
41. Lunn JN, Devlin HB. Lessons From the confidential enquiry into perioperative deaths in three Nhs regions. Lancet. (1987) 2:1384–6. doi: 10.1016/S0140-6736(87)91269-4
42. Sexton JB, Thomas EJ, Helmreich RL. Error stress and teamwork in medicine and aviation: cross sectional surveys. Bmj. (2000) 320:745–9. doi: 10.1136/bmj.320.7237.745
44. Greenberg CC, Regenbogen SE, Studdert DM. Patterns of communication breakdowns resulting in injury to surgical patients. J Am Coll Surg. (2007) 204:533–40. doi: 10.1016/j.jamcollsurg.2007.01.010
46. Leape LL, Berwick DM. 5 years after to err is human: what have we learned? Jama. (2005) 293:2384–90. doi: 10.1001/jama.293.19.2384
47. Eichhorn JH. Prevention of intraoperative anesthesia accidents and related severe injury through safety monitoring. Anesthesiology. (1989) 70:572–7. doi: 10.1097/00000542-198904000-00002
48. Boulet JR, Murray DJ. Simulation–based assessment in anesthesiology: requirements for practical implementation. Anesthesiology. (2010) 112:1041–52. doi: 10.1097/ALN.0b013e3181cea265
49. Pronovost P, Needham D, Berenholtz S, Sinopoli D, Chu H, Cosgrove S, et al. An intervention to decrease catheter–related bloodstream infections in the Icu. N Eng J Med. (2006) 355:2725–32. doi: 10.1056/NEJMoa061115
50. Silber JH, Kennedy SK. Even—Shoshan O. Anesthesiologist direction and patient outcomes. Anesthesiology. (2000) 93:152–63. doi: 10.1097/00000542-200007000-00026
51. Vincent C, Neale G, Woloshynowych M. Adverse events in british hospitals: preliminary retrospective record review. Bmj. (2001) 322:517–9. doi: 10.1136/bmj.322.7285.517
52. Brennan TA, Leape LL, Laird NM. Incidence of adverse events and negligence in hospitalized patients: results of the harvard medical practice study I. N Engl J Med. (1991) 324:370–6. doi: 10.1056/NEJM199102073240604
53. Cheney FW. The American society of anesthesiologists closed claims project: what have we learned how has it affected practice and how will it affect practice in the future? Anesthesiology. (1999) 91:552–6. doi: 10.1097/00000542-199908000-00030
54. Cooper JB, Gaba D. No myth: anesthesia is a model for addressing patient safety. Anesthesiology. (2002) 97:1335–7. doi: 10.1097/00000542-200212000-00003
55. Helmreich RL, Merritt AC, Wilhelm JA. The evolution of crew resource management training in commercial aviation. Int J Aviat Psychol. (1999) 9:19–32. doi: 10.1207/s15327108ijap0901_2
56. Howard SK, Gaba DM, Fish KJ. Anesthesia crisis resource management training: teaching anesthesiologists to handle critical incidents. Aviat Space Environ Med. (1992) 63:763–70.
57. Fletcher G, Flin R, Mcgeorge P, Glavin R, Maran N, Patey R. Anaesthetists' Non–technical skills. (ants): evaluation of a behavioral marker system. Br J Anaesth. (2003) 90:580–588. doi: 10.1093/bja/aeg112
58. Leape LL, Brennan TA, Laird N. The nature of adverse events in hospitalized patients results of the harvard medical practice study Ii. N Engl J Med. (1991) 324:377–84. doi: 10.1056/NEJM199102073240605
59. James JT. A new evidence–based estimate of patient harms associated with hospital care. J Patient Saf. (2013) 9:122–8. doi: 10.1097/PTS.0b013e3182948a69
60. Mcdonald CJ, Weiner M, Hui SL. Deaths due to medical errors are exaggerated in institute of medicine report. Jama. (2000) 284:93–5. doi: 10.1001/jama.284.1.93
61. Helmreich RL. On error management: lessons from aviation. Bmj. (2000) 320:781–5. doi: 10.1136/bmj.320.7237.781
62. Thomas EJ, Studdert DM, Newhouse JP. Costs of medical injuries in Utah and Colorado. Inquiry. (1999) 36:255–64.
63. Holzman RS, Cooper JB, Gaba DM. Anesthesia crisis resource management: real–life simulation training in operating room crises. J Clin Anesth. (1995) 7:675–87. doi: 10.1016/0952-8180(95)00146-8
64. Neily J, Mills PD, Young–Xu Y. Association between implementation of a medical team training program and surgical mortality. Jama. (2010) 304:1693–700. doi: 10.1001/jama.2010.1506
65. Nanji KC, Patel A, Shaikh S, Seger DL, Bates, DW. Evaluation of perioperative medication errors and adverse drug events. Anesthesiology. (2016) 124:25–34. doi: 10.1097/ALN.0000000000000904
66. An Organization With A Memory. Report Of An Expert Group On Learning From Adverse Events In The Nhs. London: The Stationary Office (2000).
67. Reason JT. Beyond the organizational accident: the need for “error wisdom” on the frontline. Quality And Safety In Health Care. (2004) 13:28–33. doi: 10.1136/qshc.2003.009548
68. Bates DW, Leape LL, Cullen DJ. Effect of computerized physician order entry and a team intervention on prevention of serious medication errors. Jama. (1998) 280:1311–6. doi: 10.1001/jama.280.15.1311
69. Smith AF, Pope C, Goodwin D, Mort M. Interprofessional handover and patient safety in anesthesia: observational study of handovers in the recovery room. Br J Anaesth. (2008) 101:332–7. doi: 10.1093/bja/aen168
70. Weick KE. The Reduction Of Medical Errors Through Mindful Interdependence. Medical Errors: What Do We Know? What Do We Do? 1st Edn. Rosenthal MM, Sutcliffe KM, eds San Francisco Ca: Jossey–Bass (2002):177–199.
71. Berwick DM, Leape LL. Reducing errors in medicine. Bmj. (1999) 319:136–7. doi: 10.1136/bmj.319.7203.136
72. Lawton R, Parker D. Barriers to incident reporting in a healthcare system. Qual Saf Health Care. (2002) 11:15–8. doi: 10.1136/qhc.11.1.15
73. Catchpole KR, De Leval MR, Mcewan A. Patient handover from surgery to intensive care: using formula 1 pit–stop and aviation models to improve safety and quality. Paediatr Anaesth. (2007) 17:470–8. doi: 10.1111/j.1460-9592.2006.02239.x
74. Blumenthal D. Making medical errors into medical treasures. Jama. (1994) 272:1867–8. doi: 10.1001/jama.1994.03520230077043
75. Arbous MS, Grobbee DE, Van Kleef JW. Mortality associated with anesthesia: a qualitative analysis to identify risk factors. Anesthesia. (2001) 56:1141–53. doi: 10.1111/j.1365-2044.2001.02051.x
76. Cooper JB, Taqueti VR. A brief history of the development of mannequin simulators for clinical education and training. Qual Saf Health Care. (2004) 13:I11–8.
77. Gaba DM, Deanda A. A Comprehensive anesthesia simulation environment: re–creating the operating room for research and training. Anesthesiology. (1988) 69:387–94. doi: 10.1097/00000542-198809000-00017
78. Barach P, Small SD. Reporting and preventing medical mishaps: lessons from non–medical near miss reporting systems. Bmj. (2000) 320:759–63. doi: 10.1136/bmj.320.7237.759
79. De Vries EN, Ramrattan MA, Smorenburg SM, Gouma DJ, Boermeester MA. The incidence and nature of in–hospital adverse events: a systematic review. Qual Saf Health Care. (2008) 17:216–23. doi: 10.1136/qshc.2007.023622
80. Callon M, Courtial J-P, Laville F. Co-word analysis as a tool for describing the network of interactions between basic and technological research: the case of polymer chemsitry. Scientometrics. (1991) 22:155–205. doi: 10.1007/BF02019280
82. Cook RI. Lessons from the war on cancer: the need for basic research on safety. J Patient Saf. (2005) 1:7–8. doi: 10.1097/01209203-200503000-00004
83. Nemeth CP, Cook RI, Woods DD. The messy details: insights from the study of technical work in healthcare. IEEE Transact Sys Man Cybern Part A Sys Hum. (2004) 34:689–92. doi: 10.1109/TSMCA.2004.836802
84. Rasmussen J. Risk management in a dynamic society: a modelling problem. Saf Sci. (1997) 27:183–213. doi: 10.1016/S0925-7535(97)00052-0
85. Jerak-Zuiderent S. Certain uncertainties: modes of patient safety in healthcare. Soc Stud Sci. (2012) 42:732–52. doi: 10.1177/0306312712448122
86. Reason JA. Systems approach to organizational error. Ergonomics. (1995) 38:1708–21. doi: 10.1080/00140139508925221
88. Perneger TV. The Swiss cheese model of safety incidents: are there holes in the metaphor? BMC Health Serv Res. (2005) 5:71. doi: 10.1186/1472-6963-5-71
89. Larouzee J, Le Coze JC. Good and bad reasons: the Swiss cheese model and its critics. Saf Sci. (2020) 126. doi: 10.1016/j.ssci.2020.104660
Keywords: patient safety, safety, human factors, anesthesiology, safety research, bibliometrics, bibliometric analysis
Citation: Neuhaus C, Grawe P, Bergström J and St.Pierre M (2022) The impact of “To Err Is Human” on patient safety in anesthesiology. A bibliometric analysis of 20 years of research. Front. Med. 9:980684. doi: 10.3389/fmed.2022.980684
Received: 28 June 2022; Accepted: 31 October 2022;
Published: 16 November 2022.
Edited by:
Yue Dong, Mayo Clinic, United StatesReviewed by:
Juergen Hinkelmann, St. Josefs Hospital Dortmund-Hörde, GermanyJannicke Mellin-Olsen, Bærum sykehus, Norway
Copyright © 2022 Neuhaus, Grawe, Bergström and St.Pierre. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christopher Neuhaus, Yy5uZXVoYXVzQHVuaS1oZWlkZWxiZXJnLmRl