 Mike Trott
Mike Trott Robin Driscoll
Robin Driscoll Shahina Pardhan
Shahina Pardhan
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med., 25 August 2022
Sec. Infectious Diseases: Pathogenesis and Therapy
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.980253
Post-COVID syndrome can be defined as symptoms of COVID-19 that persist for longer than 12 weeks, with several studies reporting persistent symptoms relating to the sensory organs (eyes, ears, and nose). The aim of this systematic review was to examine the prevalence of persistent anosmia, hyposmia, ageusia, and hypogeusia, as well as eye/vision and ear/hearing related long-COVID symptoms. Authors searched the electronic databases from inception to November 2021. Search terms included words related to long-COVID, smell, taste, eyes/vision, and ears/hearing, with all observational study designs being included. A random effects meta-analysis was undertaken, calculating the prevalence proportions of anosmia, hyposmia, ageusia, and hypogeusia, respectively. From the initial pool, 21 studies met the inclusion criteria (total n 4,707; median n per study 125; median age = 49.8; median percentage female = 59.2%) and 14 were included in the meta-analysis The prevalence of anosmia was 12.2% (95% CI 7.7–16.6%), hyposmia 29.9% (95% CI 19.9–40%), ageusia 11.7% (95% CI 6.1–17.3%), and hypogeusia 31.2% (95% 16.4–46.1%). Several eye/vision and ear/hearing symptoms were also reported. Considering that changes in the sensory organs are associated with decreases in quality of life, future research should examine the etiology behind the persistent symptoms.
Systematic review registration: [www.crd.york.ac.uk/prospero], identifier [CRD42021292804].
In March 2020, the World Health Organization (WHO) declared the COVID-19 outbreak a global pandemic, and as of March 2022, over 435,500,000 cases have been identified, including over 5,900,000 reported deaths (1). Symptoms of COVID-19 are wide ranging, with commonly reported symptoms including fever, cough, and fatigue (2), although it has also been reported that a significant proportion of infected people are asymptomatic (3, 4). Other well reported symptoms of COVID-19 include anosmia (complete loss of smell), hyposmia (reduced sense of smell), ageusia (complete loss of taste), and hypogeusia (reduced sense of taste), with a loss or changed sense of taste or smell being added to the United Kingdom National Health Service (NHS) official COVID-19 symptoms list in May 2020 (5). Several systematic reviews have identified these sensory symptoms as being highly prevalent in the acute phase of COVID-19. For example, one meta-analysis reported that anosmia or hyposmia are very strong predictors of COVID-19, with a reported risk ratio of 4.6 (6), with another meta-analysis reporting that 50% of COVID-19 patients reported ageusia or dysgeusia in the acute phase (7). COVID-19 symptoms have also been reported in eyes and ears. For example, a recent meta-analysis reported the presence of ocular manifestations of COVID-19 at 11%, with the most common manifestations being dry eye (or foreign body sensation), redness, and tearing (8). Furthermore, COVID-19 has been shown to affect the eyes indirectly, with recent systematic reviews highlighting the negative effect of increases in screen time on eyes, including digital eye strain in both adults and children (9–12). With regards to hearing, a meta-analysis have reported 3% of patients with hearing loss and 4.5% with tinnitus following COVID-19 infection (13).
Post-COVID syndrome (also referred to as “long-COVID”) has been defined as symptoms of COVID-19 that persists for longer than 12 weeks (14, 15). Systematic reviews have identified taste and smell disturbances as symptoms of long-COVID, with respective prevalence rates being reported as 13.5% and 15.2% (16). Another study found the prevalence rate of anosmia > 90 days from COVID-19 infection to be 11%, and ageusia 10% (17). Furthermore, several studies have reported eye related long-COVID symptoms, including blurring (18, 19) and red eyes (20), and also ear related symptoms including hearing loss and tinnitus (21).
One limitation of these reviews is that anosmia and hyposmia (and ageusia and hypogeusia) have not been stratified, therefore the prevalence of graded loss of smell or taste is unknown. Furthermore, current reviews do not appear to have explicitly included studies where patients had no signs of smell or taste disorders prior to COVID-19 infection, introducing an important potential bias. Furthermore, although several reviews have included the long-term effects of COVID-19 involving eyes and ears (16, 22), the wide variations of follow-up make results difficult to compare.
The aim of this systematic review was therefore to examine the prevalence of persistent anosmia, hyposmia, ageusia, hypogeusia, as well as eye and ear related symptoms related long-COVID, across all populations, that persisted for longer than 12 weeks. This research has the potential to inform practitioners, enabling them to monitor possible long-COVID related symptoms, allowing them to potentially create targeted therapeutical and/or mental health management and/or interventions. It will also highlight any need for further primary research studies.
The protocol was registered in PROSPERO (protocol number: CRD42021292804). Some changes were made to the protocol, which have been outlined and justified in Supplementary Table 1. Ethical clearance was not required as no primary data was being collected. Two authors (MT, RD) searched the electronic databases PubMed, Embase, Web of Science, and Scopus from inception to November 2021. Search terms included words related to long-COVID, smell, taste, eyes and ears (Full search terms are shown in Supplementary Table 2). In addition, the reference lists of eligible articles were searched for additional articles.
All observational study designs were eligible providing they met all the following inclusion criteria:
1. Studies that reported the prevalence of anosmia, hyposmia, ageusia, hypogeusia symptoms for longer than 12 weeks after COVID-19 diagnosis or studies that reported the prevalence of visual/eye or hearing/ear related symptoms for longer than 12 weeks after COVID-19 diagnosis.
2. Studies written in English.
3. Peer reviewed articles.
4. Participants had no evidence of respective smell/taste/visual/ear related symptoms prior to COVID-19 infection.
5. Reviews were included to manually search reference lists for additional eligible articles.
Title, abstract, and full-text screening was performed independently by two reviewers (MT, RD), and any disagreement between reviewers was resolved by a third senior reviewer (SP).
Data extraction was completed for each study by two independent researchers (MT, RD) for: (1) author details; (2) year of publication; (3) journal; (4) study type; (5) respective inclusion criteria; (6) demographic information; (7) respective method of data collection; (8) follow-up time (or time elapsed from COVID-19 diagnosis); (9) prevalence data.
For the prevalence of anosmia, hyposmia, ageuisia, and hypogeusia data, a random-effects meta-analysis was conducted using the DerSimonian and Laird method, with studies weighted according the inverse variance, using SPSS Version 28 (23). The meta-analysis was conducted using the following steps:
(1) Prevalence proportions, with associated SEs were inputted, stratified by anosmia, hyposmia, ageusia, and hypogeusia.
(2) Heterogeneity between studies was assessed using the I2 statistic (24).
(3) Publication bias was assessed with a visual inspection of funnel plots and with the Egger bias test (25).
Because the data involving ear and eye symptoms was highly heterogeneous (there was not more than one study measuring the same type of eye/ear symptoms, and due to the paucity of studies), there was not enough data to meta-analyze the prevalence rates of these symptoms. The literature regarding eye and ear symptoms, therefore, was synthesized in a narrative analysis.
To ascertain the certainty of the evidence, the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework (26) was used.
Risk of bias was assessed by two independent researchers (MT, RD) with the Newcastle Ottawa Scale (NOS) adapted for cross-sectional studies (27, 28). The NOS is a widely used tool and has well established content validity and inter-rater reliability. The NOS has a scoring system based on positive answers to questions regarding: appropriateness of research design; recruitment strategy; response rate; representativeness of sample; objectivity/reliability of outcome determination; power calculation; and appropriate statistical analyses, with points being assigned to positive answers, with a maximum quality score of 10, with higher scores indicating higher quality studies.
The initial search yielded 5,344 results, of which 2,700 were automatically removed, leaving 2,644 articles that were screened using the titles and abstracts. Of these, 195 articles were selected for full-text retrieval and assessed for eligibility. After full-text assessment, 19 extra articles were found from the reference lists and were further assessed for eligibility. Finally, 21 studies (total n 4,707; median n per study 125; median age = 49.8; median percentage female = 59.2%) met the inclusion criteria and were included in the review, 14 of which were related to amsonia, hyposmia, ageusia, and hypogeusia [19, 20, 30; 31; 32; 33; 34; 35; 36; 37; 38; 39; 40; 41]. The remaining 10 studies were related to eye and/or ear symptoms (18–21, 29–34) met the inclusion criteria and were included in the narrative analysis.
The full PRISMA diagram is shown in Figure 1. Full descriptive characteristics are shown in Table 1. The mean NOS score was 5.4 (median 5; range 4–8)—full NOS scoring can be found in the Supplementary Table 3.
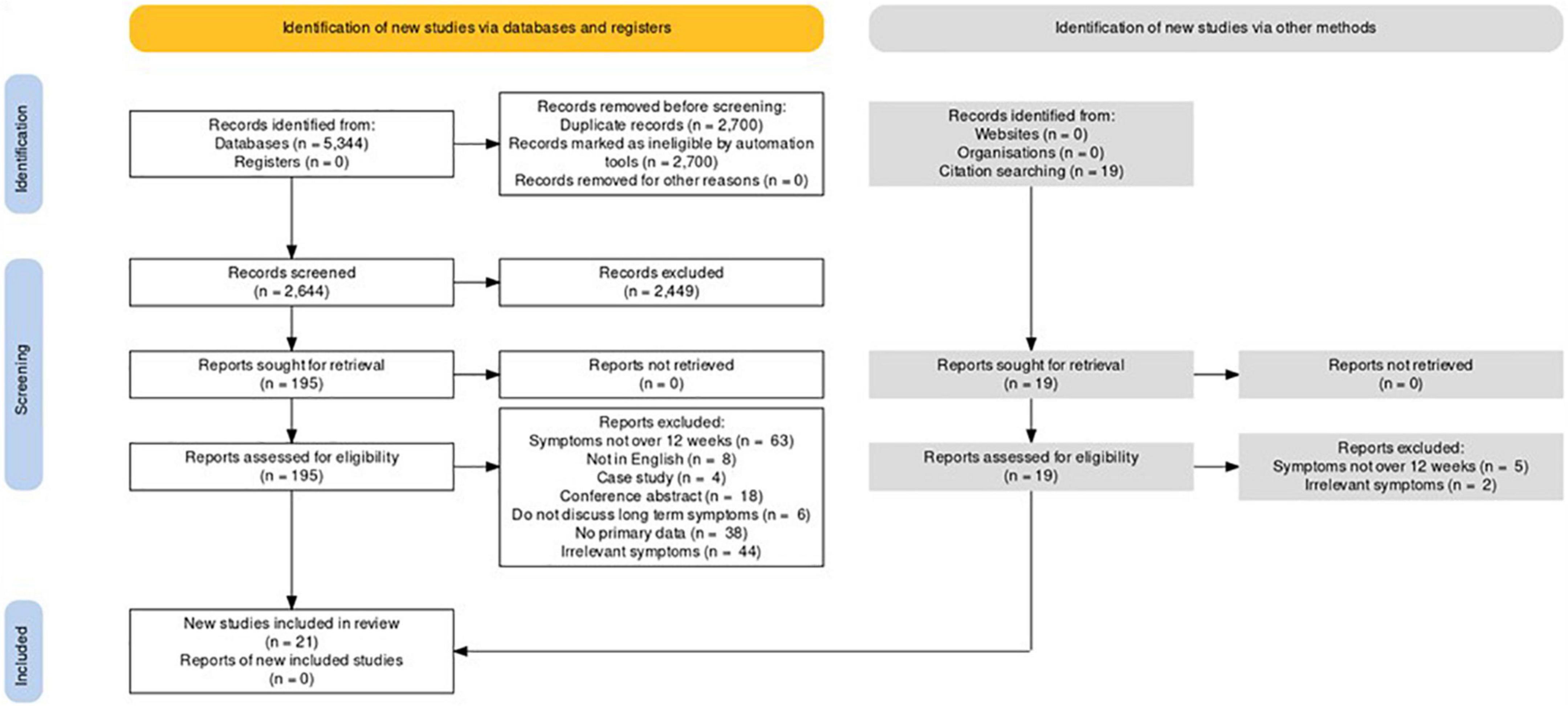
Figure 1. PRISMA flowchart of included studies.
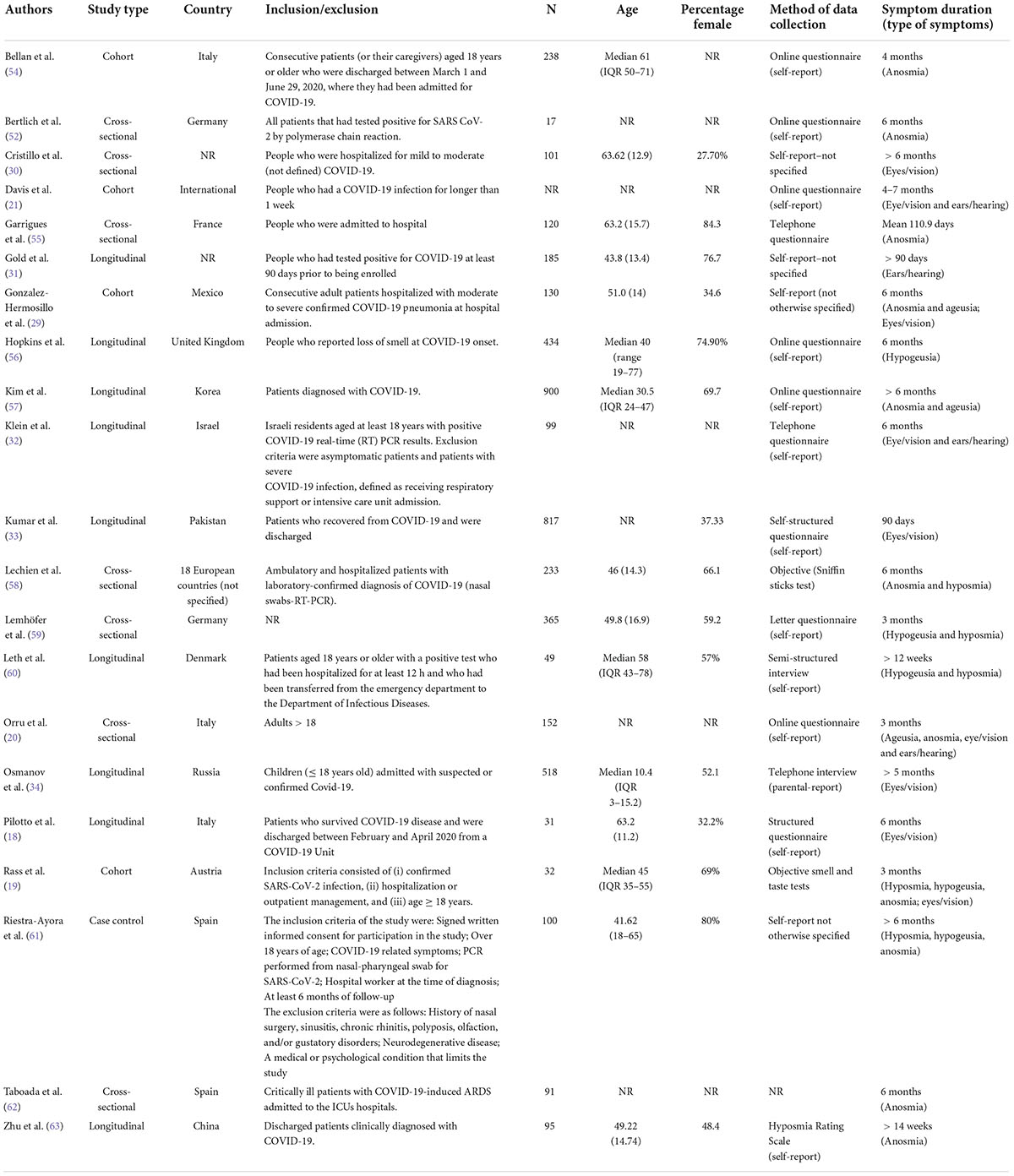
Table 1. Descriptive characteristics of included studies.
Regarding changes in smell, the prevalence of anosmia in people > 12 weeks post-COVID-19 infection was 12.2% (95% CI 7.7–16.6%), and the prevalence of hyposmia was 29.9% (95% CI 19.9–40%). With taste, the prevalence of ageusia was 11.7% (95% CI 6.1–17.3%), with the prevalence of hypogeusia being higher at 31.2% (95% 16.4–46.1%). Full details are shown in Table 2 and Figure 2. The high heterogeneity (which ranged from 89 to 96.8%) and the study designs of included studies, meant that the quality of evidence (according to the GRADE criteria) was classified as low.
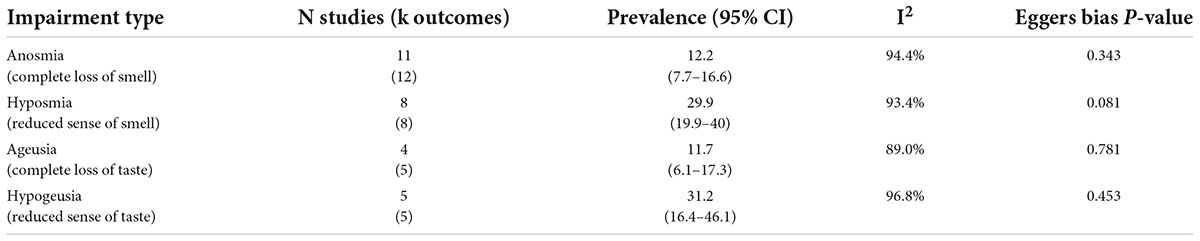
Table 2. Meta-analysis results.
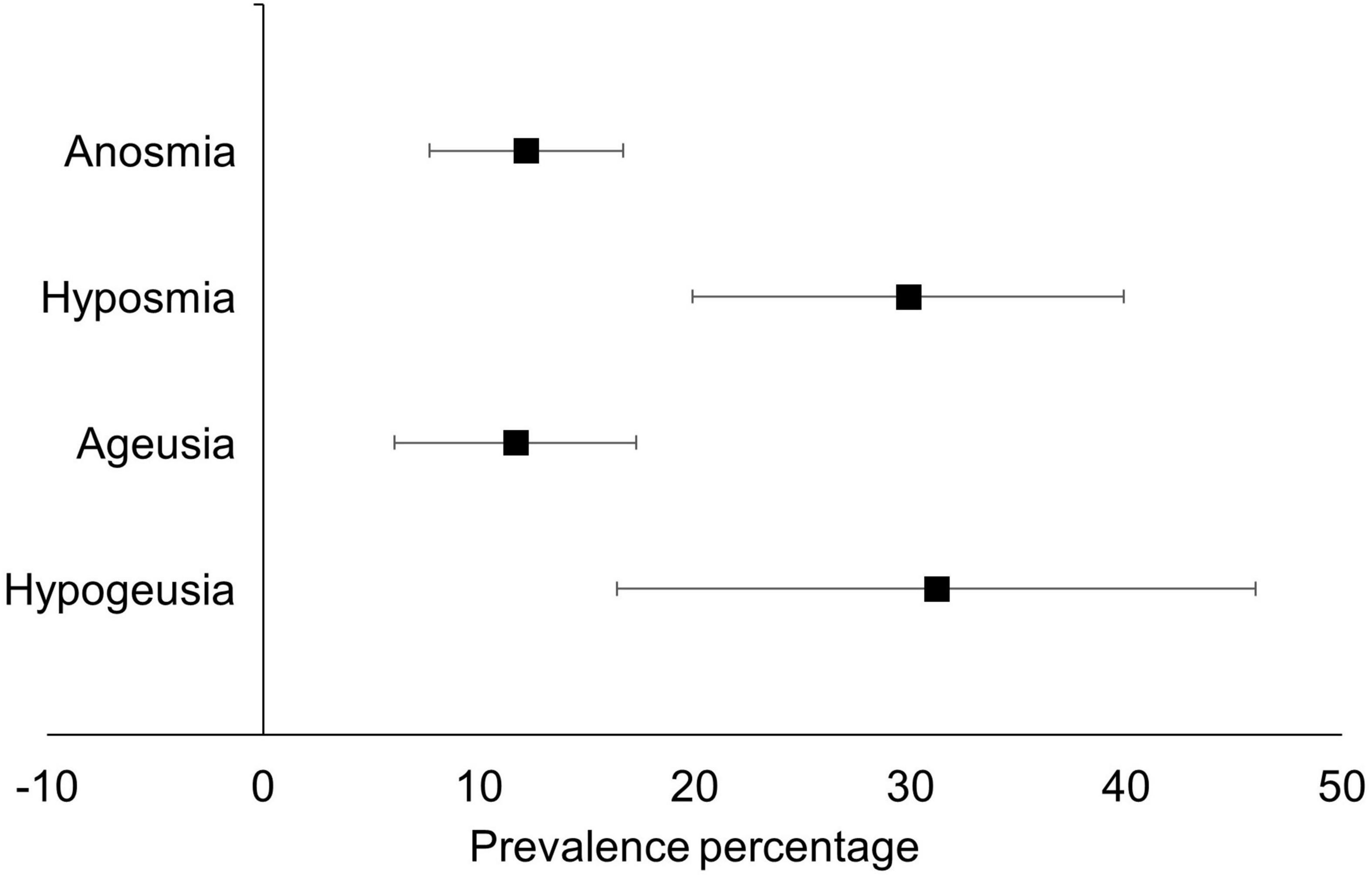
Figure 2. Meta-analytic prevalence of smell and taste related sensory loss in post-COVID syndrome.
Eight studies (18–21, 29, 30, 32, 34) examined long term visual/eye disorders, all but one of which were in adults, and all were self-reported. The prevalence of persistent blurred vision varied widely across five studies. One study reported 38.5% and 33.1% of participants (the inclusion criteria for participants in this study was not detailed) had an “inability to focus vision” at 3 and 6 months, respectively (29). Cristillo et al. (30) and Pilotto et al. (18), respectively, reported 21.8% and 19.5% prevalence of blurring/loss of vision 6 months after hospital discharge for COVID-19, while Rass et al. (19) reported 7% of participants with blurred vision 3 months after hospital discharge. In children, Osmanov et al. (34) reported a much lower prevalence of 2.1% with “problems seeing/blurred vision” > 5 months post hospital discharge.
Further exploration/analysis from one study (29) showed that prevalence rates of blurred vision or eye symptoms were significantly associated with higher rates of blurred vision in participants reporting fatigue at 3 months post COVID-19 (this was non-significant at 6-months post COVID-19). The study also found that blurred vision prevalence was lower in the “non-fatigue” group from months 3–6 post COVID-19, but not in the “fatigue” sub-group.
Other eye symptoms have been reported. Gonzalez-Hermosillo et al. (29) reported light sensitivity in 18.5% and 20% of participants after 3- and 6-months respectively. Light sensitivity was also associated with fatigue status with significantly higher rates in participants experiencing fatigue compared to those who did 3 months post COVID-19 (this was non-significant at 6-months post COVID-19). Red eyes were also reported in 15.8% of participants 3 months post COVID-19 (20). Two studies also reported non-specific eye and vision related symptoms, including 1% of participants with “eye disorders” 6 months post COVID-19 (32), 23.8% and 26.5% of participants with “vision symptoms” (21) and 2%–13.2% of participants with “other eye symptoms” 4–7 months post COVID-19.
Five eligible studies (19–21, 31, 32) reported long term hearing/ear disorders in adults, all of which were self-reported. Hearing loss was reported in 5.2–6.4% of people between months 4–7 post infection (21). The prevalence of tinnitus varied widely (7–26%) between three studies, with one study reporting rates of between 25 and 26% 4–7 months post infection (21), 14.5% 3 months post infection (20) and 6.9% > 90 days post-COVID infection (31). Vertigo was reported across two studies (19, 20), with prevalence rates ranging from 6 to 13% 3 months post-COVID-19 infection. Furthermore, Rass et al. (19) also found that the prevalence of vertigo was not influenced by the severity of COVID-19 infection. Other studies also reported ear pain and (undefined) “hearing disorder” in 1% of respondents (32), ear ache in 9.9% of respondents (20). Davis et al. (21) reported a prevalence of 8–9% of “other ear/hearing issues” between 4 and 7 months post COVID-19 infection.
This systematic review and meta-analysis pooled the prevalence of anosmia, hyposmia, ageusia, and hypogeusia in people with post-COVID syndrome, and reported on the prevalence of eye and ear related symptoms.
The pooled prevalence of anosmia was 12.2%, which is similar to other systematic reviews (11%) that have measured anosmia in people with COVID symptoms lasting more than 90 days (17). The prevalence of ageusia in our study is also similar to other meta-analyses (11.7% versus 10%). A novel finding in this review was the prevalence of hyposmia and hypogeusia, both of which were much higher than anosmia and hyposmia respectively. A review by Ahmed et al. (35) suggested five possible mechanisms behind anosmia in the acute phase of COVID-19, including the affection of the ACE-2 receptors, damage of supporting cells of the olfactory epithelium, affection of the frontal lobe, inflammatory obstruction of olfactory clefts, and zinc deficiency. In particular, several studies have reported long term damage of the olfactory epithelium in COVID-19 patients (36–38), with some authors recommending specific olfactory theory to improve long-term olfactory function (36). Other authors also suggest a genetic component, indicating that the locus of genes UGT2A1 and UGT2A2 may be a casual factor of anosmia (39). Although it is feasible that these hypotheses could also apply to long-COVID, currently the literature to support this is sparse. Further studies are warranted to ascertain the mechanisms behind smell and taste dysfunction in long-COVID.
Smell and taste dysfunction has been consistency linked with decreases in quality of life (40, 41), as has the presence of long-COVID (42). Furthermore, recent studies have found significant decreases in health-related quality of life in people with long-COVID syndrome (43), with one meta-analysis reporting that 58% of people with long-COVID suffering from poor quality of life (42). This research has the potential to inform practitioners, enabling them to monitor possible long-COVID related symptoms, allowing them to potentially create targeted therapeutical and/or mental health management and/or interventions. It also highlights the need for further primary research studies.
Regarding eye related symptoms, blurring and inability to focus vision ranged from 7 to 39% in adults > 3 months post-COVID-19, with children showing lower prevalence, however, more studies are needed to confirm this. The wide range of prevalence rates is most likely due to the high heterogeneity in various parameters between studies. For example, the inclusion criteria in two of the studies was not specific, indicating possible population bias. It is also not clear, in all of the studies, as to the exact wording of questions to ascertain the presence of blurred vision. On the other hand, it is clear, that participants are self-reporting blurred vision as a persistent post-COVID symptom. The association with fatigue suggests that the blurred vision is possibly due to ciliary muscle’s inability to focus properly, rather than the involvement of other structures of the eye, although this needs to be examined further. The fact that dry eye is also a long COVID symptom suggest a lack of tear production, which would also lead to blurred vision. Detailed clinical measurements should be able to make this clearer. Increased screen time (both leisure and non-leisure) due to the COVID-19 pandemic (11, 12) would exaggerate blurred vision and dry eyes. Signs of viral infection in the eye due to coronavirus, have been reported (44, 45), with studies reporting associations between light sensitivity and chronic fatigue (46), and with digital eye strain (47). The persistent light sensitivity reported here suggest evidence of slow recovery from the infection. Studies have also reported associations between red eyes, fatigue (48) and COVID-19. Further research is warranted to determine the exact causes and etiology of persistent eye symptoms post-COVID-19.
Regarding ear related symptoms, the prevalence of tinnitus varied from 7 to 26% across the studies, also indicating high heterogeneity across studies. Reasons for this heterogeneity could be lack of standardization of sampling techniques and ambiguity around the methods of specific data collection. While exact mechanisms of hearing related disorders in post-COVID syndrome are unknown and warrant further research, it is possible that vascular damage caused by vasculitis, shown as a symptom of COVID-19 (49, 50) may contribute, although more work is needed. It has also been suggested that hearing loss and tinnitus may be associated with other systemic infections not associated with COVID-19 (51), this requires further work.
The findings of this review should be considered within its limitations. Firstly, there was high heterogeneity in our results, which were likely caused by heterogeneous methods of, respectively, measuring anosmia, hyposmia, ageusia, and hypogeusia. In addition, the majority of data were self-reported. Future studies should aim to use homogeneous tools, and wherever possible, objective tests. Secondly, although we only included studies that stated that patients did not have any respective sensory symptoms prior to COVID-19 infection, only one study (52) included a non-COVID-19 control group. It is therefore recommended that future studies be conducted with control groups so reliable prevalence rates can be determined. Third, there were a paucity of studies found regarding eye and ear symptoms, so a meta-analysis was not possible. Fourth, meta-analyses have inherent limitations: their findings are dependent on estimates selected from each primary study and thus are dependent on the accuracy of primary studies (53). Lastly, systematic reviews in rapidly evolving fields such as this one should be considered within the time frame of the systematic literature search. Several articles are published after searches are conducted, and thus the information provided in reviews such has this should be considered as a broad overview of historical information, rather than up-to-date real-time data.
While anosmia and ageusia appear to be present in around 12% of people 12 weeks post COVID-19, the prevalence of hyposmia and hypogeusia appears to be much higher, with prevalence rates being 30% and 31% respectively. Considering that changes in taste, smell, vision, and hearing are associated with decreases in quality of life and also reduced overall well-being, future research is required to ascertain the mechanisms behind this phenomenon and the creation of therapeutic interventions.
Publicly available datasets were analyzed in this study. This data can be found here: All data in this manuscript was retrieved from already existing journal articles. Full information is available from the corresponding author.
MT: conceptualization, data collection, data analysis, and writing. RD: data collection, data analysis, and writing. SP: conceptualization, writing, and supervision. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.980253/full#supplementary-material
1. World Health Organization, WHO CORONAVIRUS. (COVID-19) Dashboard. Geneva: world health organization (2022).
2. Alimohamadi Y, Sepandi M, Taghdir M, Hosamirudsari H. Determine the most common clinical symptoms in COVID-19 patients: a systematic review and meta-analysis. J Prevent Med Hygiene. (2020) 61:E304. doi: 10.15167/2421-4248/jpmh2020.61.3.1530
3. Shakiba M, Nazemipour M, Heidarzadeh A, Mansournia M. Prevalence of asymptomatic COVID-19 infection using a seroepidemiological survey. Epidemiol Infect. (2020) 148:e300.
4. Oran DP, Topol EJ. Prevalence of asymptomatic SARS-CoV-2 infection: a narrative review. Ann Internal Med. (2020) 173:362–7.
5. National Health Service. (2022). Available online at: https://www.nhs.uk/conditions/coronavirus-covid-19/symptoms/main-symptoms/ (Accessed May 10, 2022).
6. Hariyanto TI, Rizki NA, Kurniawan A. Anosmia/hyposmia is a good predictor of coronavirus disease 2019 (COVID-19) infection: a meta-analysis. Int Arch Otorhinolaryngol. (2021) 25:170–4. doi: 10.1055/s-0040-1719120
7. Aziz M, Perisetti A, Lee-Smith WM, Gajendran M, Bansal P, Goyal H. Taste changes (dysgeusia) in COVID-19: a systematic review and meta-analysis. Gastroenterology. (2020) 159:1132.
8. Nasiri N, Sharifi H, Bazrafshan A, Noori A, Karamouzian M, Sharifi A. Ocular manifestations of COVID-19: a systematic review and meta-analysis. J Ophthalmic Vis Res. (2021) 16:103.
9. Zhang X, Cheung SSL, Chan H, Zhang Y, Wang YM, Yip BH, et al. Myopia incidence and lifestyle changes among school children during the COVID-19 pandemic: A population-based prospective study. Br J Ophthalmol. (2021). doi: 10.1136/bjophthalmol-2021-319307 [Epub ahead of print].
10. Foreman J, Salim AT, Praveen A, Fonseka D, Ting DSW, He MG, et al. Association between digital smart device use and myopia: a systematic review and meta-analysis. Lancet Digital Health. (2021) 3:e806–18. doi: 10.1016/S2589-7500(21)00135-7
11. Pardhan S, Parkin J, Trott M, Driscoll R. Risks of digital screen time and recommendations for mitigating adverse outcomes in children and adolescents. J Sch Health. (2022) 92:765–73. doi: 10.1111/josh.13170
12. Trott M, Driscoll R, Irlado E, Pardhan S. Changes and correlates of screen time in adults and children during the COVID-19 pandemic: A systematic review and meta-analysis. EClinicalMedicine. (2022) 48:101452.
13. Jafari Z, Kolb BE, Mohajerani MH. Hearing loss, tinnitus, and dizziness in COVID-19: a systematic review and meta-analysis. Canad J Neurol Sci. (2021) 49:184–95. doi: 10.1017/cjn.2021.63
14. National Institute for Health and Care Excellence. NICE, SIGN and RCGP set out further details about the UK guideline on management of the long-term effects of COVID-19. London: National Institute for Health and Care Excellence (2020).
15. National Health Service. (2022). Available online at: https://www.england.nhs.uk/coronavirus/post-covid-syndrome-long-covid/ (Accessed March 2, 2022).
16. Michelen M, Manoharan L, Elkheir N, Cheng V, Dagens A, Hastie C, et al. Characterising long COVID: a living systematic review. BMJ Glob Health. (2021) 6:e005427. doi: 10.1136/bmjgh-2021-005427
17. Fernández-de-Las-Peñas C, Palacios-Ceña D, ómez-Mayordomo VG, Florencio LL, Cuadrado ML, Plaza-Manzano G, et al. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: a systematic review and meta-analysis. Eur J Internal Med. (2021) 92:55–70. doi: 10.1016/j.ejim.2021.06.009
18. Pilotto A, Cristillo V, Cotti Piccinelli S, Zoppi N, Bonzi G, Sattin D, et al. Long-term neurological manifestations of COVID-19: prevalence and predictive factors. Neurol Sci. (2021) 42:4903–7.
19. Rass V, Beer R, Schiefecker AJ, Kofler M, Lindner A, Mahlknecht P, et al. Neurological outcome and quality of life 3 months after COVID-19: A prospective observational cohort study. Eur J Neurol. (2021) 28:3348–59.
20. Orrù G, Bertelloni D, Diolaiuti F, Mucci F, Di Giuseppe M, Biella M, et al. Long-COVID Syndrome? A Study on the persistence of neurological, psychological and physiological symptoms. Healthcare (Basel). (2021) 9:575. doi: 10.3390/healthcare9050575
21. Davis HE, Assaf GS, McCorkell L, Wei H, Low RJ, Re’em Y, et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine. (2021) 38:101019. doi: 10.1016/j.eclinm.2021.101019
22. Lopez-Leon S, Wegman-Ostrosky T, Perelman C, Sepulveda R, Rebolledo PA, Cuapio A, et al. More than 50 long-term effects of COVID-19: a systematic review and meta-analysis. Sci Rep. (2021) 11:1–12.
24. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58.
25. Egger M, Smith GD. Meta-analysis bias in location and selection of studies. BMJ (1998) 316:61–6. doi: 10.1136/bmj.316.7124.61
26. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ (2008) 336:924–6. doi: 10.1136/bmj.39489.470347.AD
27. Modesti PA, Reboldi G, Cappuccio FP, Agyemang C, Remuzzi G, Rapi S, et al. Panethnic differences in blood pressure in Europe: a systematic review and meta-analysis. PLoS One. (2016) 11:e0147601–0147601. doi: 10.1371/journal.pone.0147601
28. Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-analyses. Oxford: (2000).
29. Peterson J, Welch V, Losos M, Tugwell PJOOHRI. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. (Vol. 2). Ottawa, ON: Ottawa Hospital Research Institute (2011). p. 1–12.
30. Cristillo V, Pilotto A, Cotti Piccinelli S, Zoppi N, Bonzi G, Gipponi S, et al. Next study, age and subtle cognitive impairment are associated with long-term olfactory dysfunction after COVID-19 infection. J Am Geriatr Soc. (2021) 69:2778–80. doi: 10.1111/jgs.17296
31. Gold JE, Okyay RA, Licht WE, Hurley DJ. Investigation of Long COVID prevalence and its relationship to epstein-barr virus reactivation. Pathogens. (2021) 10:763. doi: 10.3390/pathogens10060763
32. Klein H, Asseo K, Karni N, Benjamini Y, Nir-Paz R, Muszkat M, et al. Onset, duration and unresolved symptoms, including smell and taste changes, in mild COVID-19 infection: a cohort study in Israeli patients. Clin Microbiol Infect. (2021) 27:769–74. doi: 10.1016/j.cmi.2021.02.008
33. Kumar J, Makheja K, Rahul F, Kumar S, Kumar M, Chand M, et al. Long-Term neurological impact of COVID-19. Cureus. (2021) 13:e18131.
34. Osmanov IM, Spiridonova E, Bobkova P, Gamirova A, Shikhaleva A, Andreeva M, et al. Risk factors for post-COVID-19 condition in previously hospitalised children using the ISARIC Global follow-up protocol: a prospective cohort study. Eur Respir J. (2022) 59:2101341. doi: 10.1183/13993003.01341-2021
35. Ahmed AK, Sayad R, Mahmoud IA, El-Monem AMA, Badry SH, Ibrahim IH. “Anosmia” the mysterious collateral damage of COVID-19. J Neurovirol. (2022) 28:189–200. doi: 10.1007/s13365-022-01060-9
36. Vaira LA, Lechien JR, Dore S, Boccaletti R, Saussez S, De Riu G. Specific Therapy of Olfactory Disorders in COVID-19 Patients is Essential for the Prevention of Long-term Dysfunction. Indian J Otolaryngol Head Neck Surg. (2021) 22:1–2. doi: 10.1007/s12070-021-02818-z
37. Vaira LA, Hopkins C, Sandison A, Manca A, Machouchas N, Turilli D, et al. Olfactory epithelium histopathological findings in long-term coronavirus disease 2019 related anosmia. J Laryngol Otol. (2020) 134:1123–7. doi: 10.1017/S0022215120002455
38. Doty RL. Olfactory dysfunction in COVID-19: pathology and long-term implications for brain health. Trends Mol Med. (2022):
39. Hendaus MA. Anosmia (smell failure) and dysgeusia (taste distortion) in COVID-19: it is genetic. J Biomol Struct Dyn. (2022) 93:31–5.
40. Liu DT, Prem B, Sharma G, Kaiser J, Besser G, Mueller CA. Depression symptoms and olfactory-related quality of life. Laryngoscope. (2022). doi: 10.1002/lary.30122 [Epub ahead of print].
41. Alqahtani AS, Sultan AE, Alhazmi HO, Alenazi TMAAA. Impact Of covid related anosmia on patients quality of life at hail region. Eur J Mol Clin Med. (2022) 8:721–9.
42. Malik P, Patel K, Pinto C, Jaiswal R, Tirupathi R, Pillai S, et al. Post-acute COVID-19 syndrome (PCS) and health-related quality of life (HRQoL)—A systematic review and meta-analysis. J Med Virol. (2022) 94:253–62. doi: 10.1002/jmv.27309
43. Vaira LA, Gessa C, Deiana G, Salzano G, Maglitto F, Lechien JR, et al. The effects of persistent olfactory and gustatory dysfunctions on quality of life in long-COVID-19 patients. Life. (2022) 12:141. doi: 10.3390/life12020141
44. üemes-Villahoz NG, Burgos-Blasco B, García-Feijoó J, Sáenz-Francés F, Arriola-Villalobos P, Herrera de la Muela JM. Conjunctivitis in COVID-19 patients: frequency and clinical presentation. Graefe’s Arch Clin Exp Ophthalmol. (2020) 258:2501–7.
45. Loffredo L, Pacella F, Pacella E, Tiscione G, Oliva A, Violi F. Conjunctivitis and COVID-19: a meta-analysis. J Med Virol. (2020) 92:1413–4.
46. Hutchinson CV, Maltby J, Badham SP, Jason LA. Vision-related symptoms as a clinical feature of chronic fatigue syndrome/myalgic encephalomyelitis? Evidence from the DePaul Symptom Questionnaire. Br J Ophthalmol. (2014) 98:144–5. doi: 10.1136/bjophthalmol-2013-304439
47. Sheppard AL, Wolffsohn JS. Digital eye strain: prevalence, measurement and amelioration. BMJ Open ophthalmol. (2018) 3:e000146. doi: 10.1136/bmjophth-2018-000146
48. Shigihara Y, Tanaka M, Watanabe Y. Relationship between fatigue and photosensitivity. Behav Med. (2010) 36:109–12.
49. Viola P, Ralli M, Pisani D, Malanga D, Sculco D, Messina L, et al. Tinnitus and equilibrium disorders in COVID-19 patients: preliminary results. Eur Arch Oto-Rhino-Laryngol. (2021) 278:3725–30. doi: 10.1007/s00405-020-06440-7
50. McGonagle D, Bridgewood C, Ramanan AV, Meaney JF, Watad A. COVID-19 vasculitis and novel vasculitis mimics. Lancet Rheumatol. (2021) 3:e224–33.
51. Munro KJ, Uus K, Almufarrij I, Chaudhuri N, Yioe V. Persistent self-reported changes in hearing and tinnitus in post-hospitalisation COVID-19 cases. Int J Audiol. (2020) 59:889–90. doi: 10.1080/14992027.2020.1798519
52. Bertlich M, Stihl C, Lüsebrink E, Hellmuth JC, Scherer C, Freytag S, et al. The course of subjective and objective chemosensory dysfunction in hospitalized patients with COVID-19: a 6-month follow-up. Eur Arch Otorhinolaryngol. (2021) 278:4855–61. doi: 10.1007/s00405-021-06796-4
53. Ioannidis JP. The Mass Production of Redundant, Misleading, and Conflicted Systematic Reviews and Meta-analyses. Milb Q. (2016) 94:485–514. doi: 10.1111/1468-0009.12210
54. Bellan M, Soddu D, Balbo PE, Baricich A, Zeppegno P, Avanzi GC, et al. Respiratory and psychophysical sequelae among patients with COVID-19 four months after hospital discharge. JAMA Netw Open. (2021) 4:e2036142.
55. Garrigues E, Janvier P, Kherabi Y, Le Bot A, Hamon A, Gouze H, et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J Infect. (2020) 81:e4–6.
56. Hopkins C, Surda P, Safarian M, Vaira LA, Lechien JR, Saussez S, et al. Six month follow-up of self-reported loss of smell during the COVID-19 pandemic. Rhinology. (2021) 59:26–31.
57. Kim Y, Kim SW, Chang HH, Kwon KT, Bae S, Hwang S. Significance and associated factors of long-term sequelae in patients after acute COVID-19 Infection in Korea. Infect Chemother. (2021) 53:463–76. doi: 10.3947/ic.2021.0022
58. Lechien JR, Chiesa-Estomba CM, Beckers E, Mustin V, Ducarme M, Journe F, et al. Prevalence and 6-month recovery of olfactory dysfunction: a multicentre study of 1363 COVID-19 patients. J Intern Med. (2021) 290:451–61.
59. Lemhöfer C, Sturm C, Loudovici-Krug D, Best N, Gutenbrunner C. The impact of Post-COVID-Syndrome on functioning–results from a community survey in patients after mild and moderate SARS-CoV-2-infections in Germany. J Occupat Med Toxicol. (2021) 16:1–9. doi: 10.1186/s12995-021-00337-9
60. Leth S, Gunst JD, Mathiasen V, Hansen K, Søgaard O, Østergaard L, et al. Persistent symptoms in patients recovering from COVID-19 in Denmark. Open Forum Infect Dis. (2021) 8:ofab042.
61. Riestra-Ayora J, Yanes-Diaz J, Esteban-Sanchez J, Vaduva C, Molina-Quiros C, Larran-Jimenez A, et al. Long-term follow-up of olfactory and gustatory dysfunction in COVID-19: 6 months case–control study of health workers. Eur Arch Oto-Rhino-Laryngol. (2021) 278:4831–7. doi: 10.1007/s00405-021-06764-y
62. Taboada M, Moreno E, Cariñena A, Rey T, Pita-Romero R, Leal S, et al. Quality of life, functional status, and persistent symptoms after intensive care of COVID-19 patients. Br J Anaesth. (2021) 126:e110–3.
Keywords: smell, taste, smell loss, taste loss, COVID-19
Citation: Trott M, Driscoll R and Pardhan S (2022) The prevalence of sensory changes in post-COVID syndrome: A systematic review and meta-analysis. Front. Med. 9:980253. doi: 10.3389/fmed.2022.980253
Received: 28 June 2022; Accepted: 01 August 2022;
Published: 25 August 2022.
Edited by:
Nicola Origlia, National Research Council (CNR), ItalyReviewed by:
Luigi Angelo Vaira, Azienda Ospedaliero Universitaria Sassari, ItalyCopyright © 2022 Trott, Driscoll and Pardhan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mike Trott, bWlrZS50cm90dEBhcnUuYWMudWs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.