
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 16 August 2022
Sec. Geriatric Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.967952
This article is part of the Research Topic Frailty: Risks and Management View all 13 articles
 Nicolò Granata1
Nicolò Granata1 Martina Vigoré2*
Martina Vigoré2* Andrea Steccanella2Luca Ranucci2Simona Sarzi Braga3
Andrea Steccanella2Luca Ranucci2Simona Sarzi Braga3 Paola Baiardi4
Paola Baiardi4 Antonia Pierobon2
Antonia Pierobon2Background: The Clinical Frailty Scale (CFS) is a well-established tool that has been widely employed to assess patients' frailty status and to predict clinical outcomes in the acute phase of a disease, but more information is needed to define the implications that this tool have when dealing with Non-Communicable Diseases (NCDs).
Methods: An electronic literature search was performed on PubMed, Scopus, EMBASE, Web of Science, and EBSCO databases to identify studies employing the CFS to assess frailty in patients with NCDs.
Findings: After database searching, article suitability evaluation, and studies' quality assessment, 43 studies were included in the systematic review. Researches were conducted mostly in Japan (37.5%), and half of the studies were focused on cardiovascular diseases (46.42%), followed by cancer (25.00%), and diabetes (10.71%). Simplicity (39.29%), efficacy (37.5%), and rapidity (16.07%) were the CFS characteristics mostly appreciated by the authors of the studies. The CFS-related results indicated that its scores were associated with patients' clinical outcomes (33.92%), with the presence of the disease (12.5%) and, with clinical decision making (10.71%). Furthermore, CFS resulted as a predictor of life expectancy in 23 studies (41.07%), clinical outcomes in 12 studies (21.43%), and hospital admissions/readmissions in 6 studies (10.71%).
Discussion: CFS was found to be a well-established and useful tool to assess frailty in NCDs, too. It resulted to be related to the most important disease-related clinical characteristics and, thus, it should be always considered as an important step in the multidisciplinary evaluation of frail and chronic patients.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/display_record.asp? PROSPERO 2021, ID: CRD42021224214.
It is well known that one of the most compelling challenges of our time is population aging (1). In recent years, as to the World Health Organization report on aging (1), the number of people aged 65 years or over is progressively increased: it is estimated that for the year 2050 the population over 60 years old will double, reaching almost 22% of the total one. In parallel, the number of people aged 80 years or over is growing even faster, and it is expected to triple by 2050 (2). Aging is often associated with chronicity and multimorbidity and their prevalence increases in people aged 65 years and older (3, 4).
Elderly people often are affected by Non-Communicable Diseases (NCDs), also defined as chronic diseases. It is estimated that each year NCDs are responsible for 71% of all deaths (5). The NCDs can be clustered into four main categories: Cardiovascular, Chronic respiratory diseases, Cancer, and Diabetes. Cardiovascular diseases are responsible for most NCDs deaths, followed by cancers, respiratory diseases, and diabetes (5). Furthermore, old age and chronicity are often associated with frailty syndrome.
Despite the importance and the interest toward frailty, there is no agreement on the definition (6). In fact, according to the literature, two theoretical paradigms try to define frailty: the biomedical and bio-psycho-social paradigms. As to the biomedical paradigm, frailty is considered a biological syndrome in which there is an important reduction in the functional reserves and a diminished resistance to stressors. These features result in a cumulative impairment of the multiple physiological systems that cause a state of increased vulnerability and adverse consequences (7). Conversely, the bio-psycho-social paradigm defines frailty as a dynamic state that affects an individual that loses one or more functional domains (physical, psychological, and social) due to the influence of different variables that increase the risk of adverse health outcomes (8). Despite the differences between the two considered paradigms, it is possible to underline a common conclusion: frailty is associated with the loss of different functional domains, which leads to an increased vulnerability to adverse events such as risk of falls, hospitalization, disability, and mortality (9). Anyhow, it is universally recognized that frailty is a clinical condition that can impair several areas (e.g., general health and operative risk) (10) and, according to the criteria established by Fried, its prevalence is around 10% in ≥65 and between 25–50% in over 85 years old (11). Moreover, in a recent systematic review and meta-analysis, the prevalence data collected from 62 countries and territories showed that the pooled prevalence in studies using physical frailty measures was 12% (95% CI = 11–13%; n = 178), compared with 24% (95% CI = 22–26%; n = 71) for the deficit accumulation model (those using the Frailty Index, FI) (12).
The overall result of the interaction between the aging process and clinical conditions is the progressive deterioration of the homeostatic balance, so it follows that a deteriorated homeostasis may result in an increased difficulty in coping with stressors (10). People affected by frailty syndrome are more susceptible to health status changes following a minor stress event than non-frail people.
Rockwood et al. proposed an operational definition of frailty with the Frailty Index (FI), by counting the number of deficits accumulated over time, within an extensive list (13, 14). This definition was based on the idea that frailty is a state of chaotic disorganization of physiological systems that can be estimated by evaluating certain indexes such as functional status, diseases, physical and cognitive deficits, psychosocial risk factors, and geriatric syndromes. Furthermore, in 2005, Rockwood et al. described a different approach in frailty evaluation, which was embedded in the Clinical Frailty Scale (CFS), a screening tool based on clinical judgment (14).
CFS, originally developed in Canada, is entirely based on clinical judgment, fast and easy to use, and it has proven to be an effective instrument for frailty assessment (1= Very Fit; 2= Well; 3= Managing Well; 4= Vulnerable; 5= Mildly Frail; 6= Moderately Frail; 7= Severely frail; 8= Very severely Frail; 9= Terminally Ill) (13–16).
According to the scientific literature, the use of CFS in frailty assessment has been widely used to predict patients' outcomes in the acute phase of the disease (16–18). Few studies tried to understand the impact of frailty on rehabilitation outcomes, for example, Holland and colleagues (18) by focusing on pulmonary rehabilitation and Pandey and colleagues (17) on heart failure patients.
More information is needed to define the implications of frailty syndrome, not only in the acute phase of a disease but also in the presence of chronic disease, therefore, this systematic review aims to evaluate the use of CFS for frailty assessment, with a specific focus on chronic and non-communicable diseases.
The systematic review was registered on the PROSPERO database that was previously searched for similar reviews in order to avoid duplication: “The Clinical Frailty Scale (CFS) employment in the frailty assessment of patients suffering from Non-Communicable Diseases (NCDs): a systematic review” (PROSPERO 2021 CRD42021224214).
Data were reported according to the international PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (19) and, a meta-analysis was not conducted due to the wide heterogeneity of the methodologies (20, 21) adopted by the studies considered, so we have conducted a narrative synthesis.
An electronic literature search was performed on PubMedMedline through Pubmed, Scopus, EMBASE, Web of Science, and EBSCO databases, considering all the publications until December 2021, to describe how CFS is employed with patients suffering from chronic conditions (Appendix a). Different combinations of keywords, including Clinical Frailty Scale, noncommunicable (or non-communicable) disease/s, chronic disease/s, heart disease/s, cardiovascular disease/s, heart failure, coronary heart disease, hypertension, stroke, cancer, diabetes, chronic obstructive pulmonary disease (or COPD), chronic respiratory disease/s, chronic lung disease/s, and asthma, were entered and applied in the title and abstract sections.
A support from the Microsoft OfficeTM pack was used: after the Comma-Separated Values (CSV) files were downloaded from the online databases, the organization functions of Microsoft Excel were used to unify all the results in a single sheet and to remove all the duplicated records.
After the electronic search was completed, two reviewers (AS, LR) independently performed the screening of the records retrieved and subsequently, after a full text analysis, they identified the eligible papers. Doubts and concerns about inclusion and exclusion criteria were discussed by all researchers through a triangulation process (NG, MV, AS, LR, AP).
Studies were considered suitable for inclusion if written in English, published in peer-reviewed journals, and where the CFS was employed to screen patients' frailty. There were no limits concerning patients' age, sample size, type of disease/s, and settings where the studies were performed.
Articles that did not deal with frailty, meeting abstract, books/book chapters, comment/editorial, protocol/design, reviews, and meta-analysis, were excluded.
Information collected through the full-text analysis was extracted by two independent reviewers (NG, MV) and it was organized in a synoptic table, according to the following categories: [A] Characteristics of the study: first author, year of study, nation of the study, nation ranking according to the Human Development Index (HDI) (22), study design, study setting, and professional figures involved; [B] Characteristics of the participants: sample size, mean age, and type of disease/s; [C] CFS-related characteristics: reason/s for CFS utilization, time at which CFS was used (e.g., during outpatient or inpatient visits, retrospectively based on clinical records), study authors' comment on CFS, and CFS related results; [D] Other eventual frailty indexes employed and other eventual outcomes considered (e.g., clinical, functional, and psychological outcomes).
The quality of each study was assessed by two independent reviewers (NG, MV) with the Newcastle Ottawa Scale (NOS) (23). In particular, two adapted versions were used, one for cohort and case-control studies, and one for cross-sectional studies. Using these scales, each study was judged on eight or ten items, categorized into three groups: the selection of the study groups, the comparability of the groups, and frailty-related outcomes. As to cohort and case-control studies, stars are awarded for each quality item, and the highest quality studies are awarded up to nine stars. A study is considered of good quality if there are 3 or 4 stars in the selection domain AND 1 or 2 stars in the comparability domain AND 2 or 3 stars in the outcome/exposure domain. Concerning cross-sectional studies, each study is judged on a 10-point scale and divided into four groups: very good studies (9–10 points), good studies (7–8 points), satisfactory studies (5–6 points), and unsatisfactory studies (0–4 points).
After database searching and duplication removal, 969 records were found. Following the title/abstract screening, 236 suitable articles were found and after the full-text reading, 58 studies were considered for quality assessment. Most of the excluded records were not focused on chronic disease/s (n = 63), did not include CFS (n = 47) or had no focus on CFS (n = 37) (Figure 1).
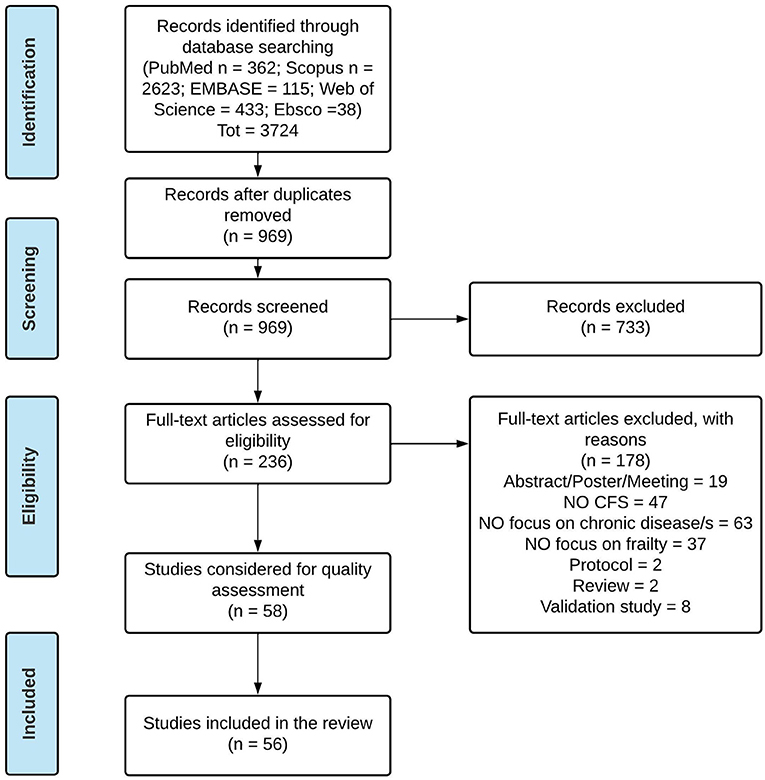
Figure 1. PRISMA Flow Diagram of the systematic review.
Most studies were of good quality as assessed by the Newcastle-Ottawa Scale (NOS), both for cohort and case-control studies (mean 7.33 ± 0.81), and cross-sectional studies (mean 7.71 ± 0.71). Two articles were excluded as they were judged “fair” quality, particularly in the methodological description of their studies, and they could affect the reliability of the results: for this reason, 56 studies were included and analyzed in the present review.
The information collected is represented in a synoptic table (Appendix a) (24–79). Most of the studies were observational studies (67.86%), followed by retrospective studies (32.14%). The total number of patients in the included studies was 20,497 and the sample sizes varied widely, ranging from 20 patients to 2,588 patients, with most of the studies including more than 100 patients (87.5%) (mean age range: from 42.9 ± 9.4 to 87.4 ± 4.96). Most of the studies were conducted in a hospital (85.71% inpatients and 10.71% outpatients), one study was performed both in inpatient and outpatient settings (1.79%), and only one in a community-dwelling center (1.79%). In all of the studies, CFS was used to assess frailty and for statistical analysis, and in almost half of the studies, it was employed for sample stratification (46.43%) too. In the considered studies, besides CFS, these outcomes were evaluated too: 35.71% functional measures (basic and instrumental activities of daily living, mobility, gait speed, etc.), 23.21% psychological status (anxiety, depression), and 17.86% cognitive functioning. Almost in all of the studies, a physician assessed the CFS score (82.14%), in six cases it was assessed by a nurse (10.71%), in two cases alternatively by a physician or a nurse (3.57%), in one case by an occupational therapist (1.97%), and in one study the patients performed a CFS self-assessment (1.97%). In 10 studies (17.86%), in addition to the CFS, other frailty indexes were employed: the Fried frailty criteria (53, 55, 58, 62), Sarcopenia (44, 45), Frailty index (51, 53), CKD Frailty Index Lab (67), Liver frailty index (55), PARTNER frailty scale (53), Derby frailty scale (51, 52), and Acute frailty (51, 52).
Tables 1a,1b summarize the results concerning the nations of the studies, the type of disease/s, data used for CFS compilation, the CFS evaluation timing, the authors' comment on CFS, and the CFS related results. Tables 1a,1b show that studies were conducted mostly in Japan (37.5%), and almost half of the studies were focused on cardiovascular diseases (46.42%). The other chronic diseases that have been found most frequently were cancer (25.00%) and diabetes (10.71%). In many studies clinical judgement (41.07%), ADL (28.57%), functional capacity status (19.64%), comorbidities (14.29%) and mobility (14.29%) data were used for CFS compilation. The evaluation timing of CFS was: during inpatient clinical visits (19.64%), in the preoperative phase (28.57%), at patients' admission (16.07%), on clinical records of hospitalized patients (10.71%), and retrospectively on clinical records (10.71%). Simplicity (39.29%), efficacy (37.5%), and rapidity (16.07%) were the major authors' comments on CFS. The CFS-related results indicated that CFS was associated with clinical outcomes (33.92%), with the presence of the disease (12.5%), and with clinical decision-making (10.71%). Furthermore, CFS resulted a good predictor of life expectancy (41.07%) and clinical outcomes (21.43%).
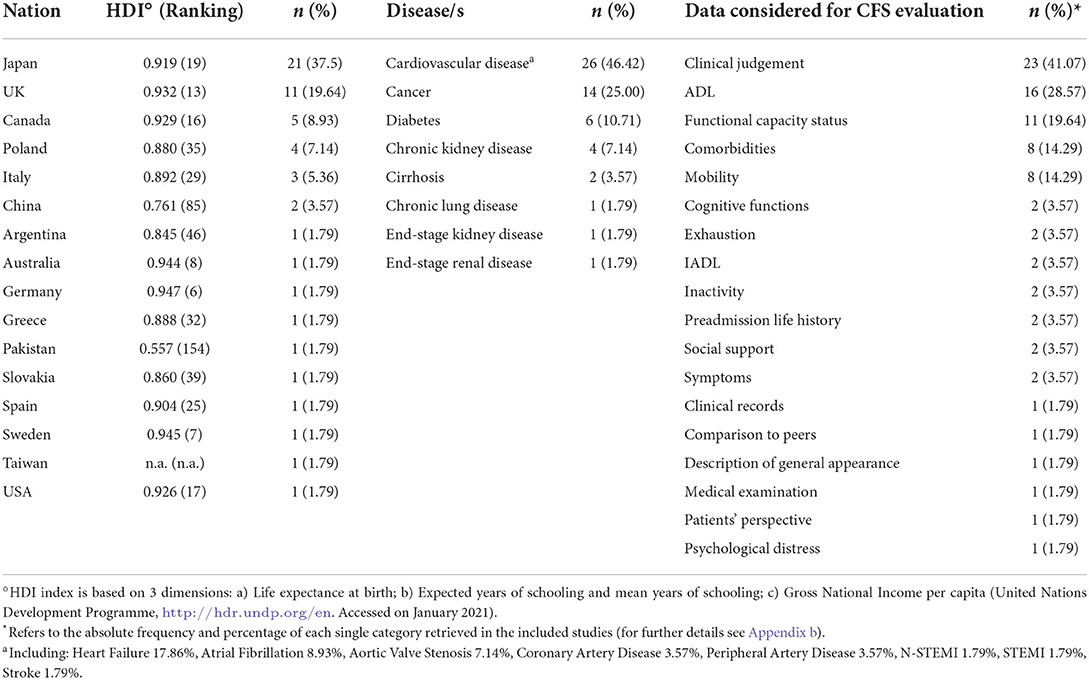
Table 1a. Main features of the studies included (n = 56).
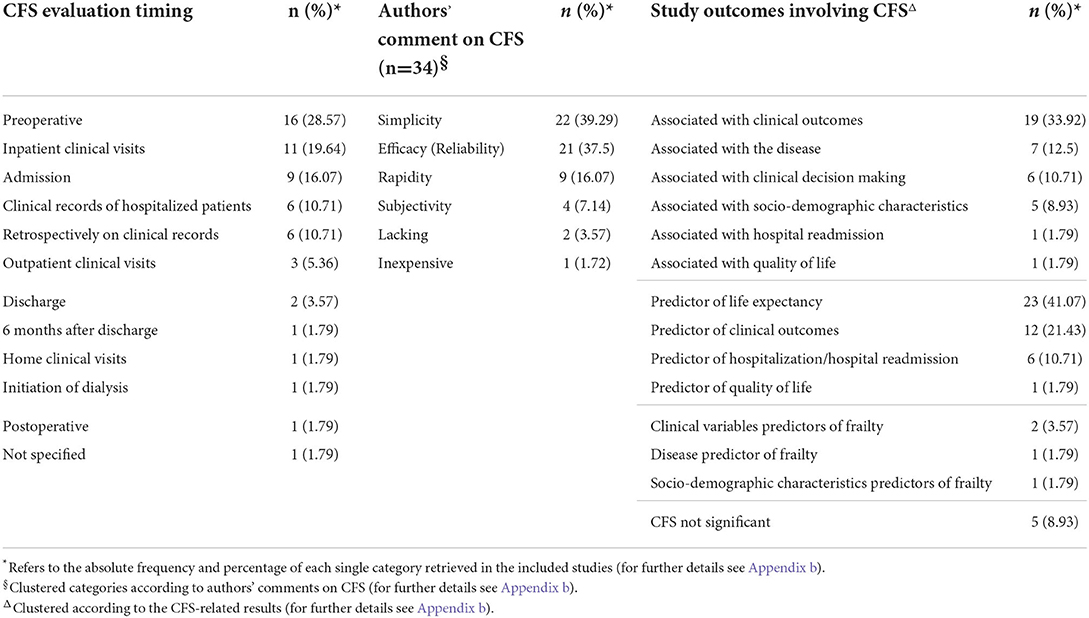
Table 1b. Main features of the studies included (n = 56).
This systematic review was focused on the CFS utilization in patients suffering from chronic diseases (or NCDs), its dissemination in the different nations, the clinical data used to complete it, and the evaluation timing. Moreover, specific attention was dedicated to investigating the CFS characteristics concerning its usability, reliability, and efficacy in predicting disease-related outcomes.
Although CFS is a well-established tool and used worldwide, most of the included studies were conducted in Japan. In a recent scoping review, it was reported that most of the studies were conducted in Canada (80). This inconsistency with the results of the present study could be explained by the specific focus on NCDs, while in the Church and colleagues' review were considered also critical illnesses. Additionally, the elderly population in Japan amounts to more than 30% of the total population (1) and this might explain the dedicated attention to this topic.
In recent years, the number of studies that provided a CFS evaluation is considerably increased, underlining specific attention dedicated to frailty syndrome in different clinical settings and diseases (80). Most of the included studies involved patients affected by chronic cardiovascular diseases (46.42%) and by different types of cancer (25.00%). This prevalence could be due to the impact that these clinical conditions have on mortality since, as highlighted in the WHO report, these diseases account for most of NCDs deaths per year (5).
Frailty is largely considered a geriatric syndrome, but many studies highlight that frailty syndrome has a notable impact on the younger population as well (81). In the present review, five studies (36, 55, 56, 58, 64) considered a sample size of patients with a mean age of <65 years. Although chronic conditions are often associated with the elderly population, scientific evidence shows that NCDs are responsible for 15 million deaths per year in people aged 30–69 years (5). Furthermore, it has been shown that, even though absolute mortality in relation to frailty was higher with increasing age, the relative risk of mortality in relation to frailty was highest for younger people (81). Therefore, efforts to identify, manage, and prevent frailty should include middle-aged individuals with multimorbidity, in whom frailty is significantly associated with mortality, even after adjustment for the number of long-term conditions, sociodemographic characteristics, and lifestyle (82).
All the studies were conducted with an observational or retrospective design. There are no studies in which is described a specific intervention for disease-related frailty and it could be interesting to evaluate the CFS reliability in pre and post-study designs. Indeed, in a recent scoping review, the authors found only few studies conducted in rehabilitation settings (80). Among these, different types and timing of rehabilitation were taken into account, for example, pre-operatory (83, 84) or post-acute rehabilitation (85, 86), and none was focused on NCDs or on chronic diseases. Moreover, a meta-analysis performed by Attwell and Vassallo found only three studies focused on COPD frail patients' rehabilitation (87). This data is consistent with our results since no articles were found about NCDs rehabilitation and it highlights a lack of studies focused on the use of CFS in NCDs rehabilitation. Therefore, specific attention should be given to deepening and shedding light on this topic.
Even though CFS is based on clinical judgment, in six studies (10.71%), the CFS score has been attributed retrospectively based on patients' medical records. This scoring method was reported to be reliable, provided that the charts (medical records, nurse records, etc.,) contain all the elements required to assign a CFS score (88). Also, evidence reports a consistency between CFS scores attributed considering medical records and CFS scores attributed through interviews with patients or their families (89). Moreover, CFS should be administered by medical doctors, but, despite this, ten studies included in this review show that CFS is not always administered by physicians (42, 46, 55–57, 59, 68, 70, 75, 77). This is made possible by the multidimensionality of this tool because it relies on data other than clinical judgment.
In a recent study, the results obtained with the CFS were compared with those obtained with the Edmonton Frail Scale (EFS) (90). The findings of this study imply that the CFS is a valid measurement tool for frailty in critically ill patients, compared with a multidimensional and more comprehensive tool. Similarly, Ritt and colleagues (91), compared this instrument with the Frailty Index, finding that the predictive accuracy of mortality was similar between the two instruments, but the CFS score was even able to predict unplanned hospital admission. Moreover, CFS was found to be an easy-to-use tool and had high inter-rater reliability in addition to a good prognostic value (92). Also in the present review, most of the included studies (82.14%) used only CFS to evaluate frailty. This data is supported by existing literature that reports a high degree of effectiveness of the CFS as a screening instrument (93). Besides, these data may be consistent with this review's results related to the observations on CFS, since most authors commented that it was a simple (Simplicity, 39.29%), reliable (Efficacy, 37.5%), and fast (Rapidity, 16.07%) instrument for frailty assessment.
As for CFS-related results, different studies find associations between CFS score and the disease taken into account, and, conversely, one study finds that the presence of the disease is a predictor of CFS score. These results are supported by the literature, since it was found that chronic diseases contribute to the frailty status development (10) and, in addition, another study suggests a bidirectional association between frailty and the disease, specifically in presence of multimorbidity (94). Same results were found concerning CFS and clinical outcomes: in most of the studies, CFS was found to be associated with or a predictor of patients' clinical outcomes. Literature supports these findings both when it deals with frailty, evaluated with different frailty indexes (95, 96), and when frailty is evaluated specifically with CFS (80). Our results are consistent with the aforementioned studies although they were not focused specifically on chronic diseases.
Moreover, CFS was found to be associated with clinical decision-making, as well. This result is in line with recent literature that outlines the importance of taking into account frailty when dealing with chronic diseases (97, 98). Indeed, frailty is a syndrome that could interact with therapeutic prescriptions for other diseases, worsening the clinical condition, or, on the other side, its course could be accelerated by the implementation of disease-related clinical practices (97, 98).
Socio-demographic characteristics were found to be associated with CFS in different studies. This result is in line with previous literature since frailty is a syndrome that affects particularly older people (99). Moreover, in a recent study, it was found that people with worsening economic conditions over time simultaneously experience a rapid increase in the frailty symptoms (100).
In several articles frailty resulted to be associated with or a predictor of mortality and rehospitalizations. A recent meta-analysis conducted on Chronic Heart Failure (CHF) found that frailty is a significant predictor of all-cause mortality and CHF-related hospitalizations (95). Similar findings are reported in a systematic review on Chronic Kidney Disease and on End-Stage Renal Disease, which suggests that frailty is an independent risk factor of overall mortality in patients affected by these diseases (101). Moreover, Church and colleagues report that several outcomes are associated with CFS score, such as mortality, length of hospitalization, readmissions, and also institutionalizations (80).
Even though different studies focus on the relationship between frailty and quality of life, only one study in this systematic review finds this result. In literature, frailty is associated with worse quality of life in patients affected by different diseases, such as breast and prostate cancer (96, 102), or in cardiovascular diseases (103, 104). Uchmanowicz and colleagues underline that all the areas forming the construct of quality of life (physical, psychological, social, and environmental) are negatively affected by frailty status (103).
In this systematic review, an eventual limitation lies in the labels assigned to group the findings of the included studies, which were created arbitrarily to provide an immediate understanding. Nevertheless, this procedure was conducted by a triangulation process between the reviewers (NG, MV, AS, LR), and supervised by all the authors, to guarantee the best level of objectivity.
On the other side, as far as we know, this is the first systematic review specifically focused on the use of CFS in NCDs, and it could provide useful information both for a further investigation through a meta-analysis and for clinical practice.
This systematic review provides a specific focus on the utilization of CFS in patients suffering from NCDs that adds useful information in the field of frailty assessment. Indeed, CFS seems to be an easy-to-use and reliable instrument to assess frailty in this kind of disease, it resulted to be associated with a variety of disease-related characteristics, and it is a good predictor of clinical outcomes, life expectancy, hospitalizations, and quality of life. Further research is needed to corroborate these findings, particularly related to CFS predictivity in clinical settings, in order to support a routine assessment of frailty in NCDs patients with this tool. This kind of assessment might be provided also in rehabilitation settings since it provides an overview of patients' frailty status and adds useful information that could be implemented in the tailored rehabilitation program and subsequent intervention.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Conceptualization and methodology: NG, MV, SSB, and AP. Investigation: AS and LR. Data curation: NG, MV, AS, and LR. Supervision: SSB and PB. Writing—original draft: NG, MV, AS, and LR. Writing—review and editing: PB and AP. All authors contributed to the article and approved the submitted version.
This work was supported by the National Funding (5x1000): Project Name Decadimento cognitivo, fragilità e outcome riabilitativo in pazienti anziani affetti da patologia cardiorespiratoria. DEC_FRAinRIAB (Grant Agreement Number 2424_20 04 20).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.967952/full#supplementary-material
1. World Health Organization. World Report on Ageing and Health. Geneva: World Health Organization (2015). p. 246.
2. United Nations PDD of E and SA. World Aging Population 2017. United Nations PDD of E and SA (2017). p. 1–40.
3. Violan C, Foguet-Boreu Q, Flores-Mateo G, Salisbury C, Blom J, Freitag M, et al. Prevalence, determinants and patterns of multimorbidity in primary care: a systematic review of observational studies. PLoS ONE. (2014) 9:e102149. doi: 10.1371/journal.pone.0102149
4. Marengoni A, Angleman S, Melis R, Mangialasche F, Karp A, Garmen A, et al. Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev. (2011) 10:430–9. doi: 10.1016/j.arr.2011.03.003
5. World Health Organization. Global Status Report On Noncommunicable Diseases 2014. Geneva: World Health Organization (2014)
6. Xue Q-L. The frailty syndrome: definition and natural History. Clin Geriatr Med. (2011) 27:1–15. doi: 10.1016/j.cger.2010.08.009
7. Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. (2004) 59:255–63. doi: 10.1093/gerona/59.3.M255
8. Gobbens RJJ, Luijkx KG, Wijnen-Sponselee MT, Schols JMGA. In search of an integral conceptual definition of frailty: opinions of experts. J Am Med Dir Assoc. (2010) 11:338–43. doi: 10.1016/j.jamda.2009.09.015
9. McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane database Syst Rev. (2015) 2:CD003793. doi: 10.1002/14651858.CD003793.pub3
10. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. (2013) 381:752–62. doi: 10.1016/S0140-6736(12)62167-9
11. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. (2001) 56:M146–56. doi: 10.1093/gerona/56.3.M146
12. O'Caoimh R, Sezgin D, O'Donovan MR, Molloy DW, Clegg A, Rockwood K, et al. Prevalence of frailty in 62 countries across the world: a systematic review and meta-analysis of population-level studies. Age Ageing. (2021) 50:96–104. doi: 10.1093/ageing/afaa219
13. Rockwood K, Stadnyk K, MacKnight C, McDowell I, Hébert R, Hogan DB, et al. brief clinical instrument to classify frailty in elderly people. Lancet. (1999) 353:205–6. doi: 10.1016/S0140-6736(98)04402-X
14. Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, et al. global clinical measure of fitness and frailty in elderly people. CMAJ. (2005) 173:489–95. doi: 10.1503/cmaj.050051
15. Rockwood K, Andrew M, Mitnitski A. A comparison of two approaches to measuring frailty in elderly people. J Gerontol Ser A. (2007) 62:738–43. doi: 10.1093/gerona/62.7.738
16. Strini V, Schiavolin R. Scale di valutazione della fragilità nell'anziano: Una revisione della letteratura. Assist Inferm e Ric. (2019) 38:87–98.
17. Pandey A, Kitzman D, Whellan DJ, Duncan PW, Mentz RJ, Pastva AM, et al. Frailty among older decompensated heart failure patients: prevalence, association with patient-centered outcomes, and efficient detection methods. JACC Hear Fail. (2019) 7:1079–88. doi: 10.1016/j.jchf.2019.10.003
18. Holland AE, Harrison SL, Brooks D. Multimorbidity, frailty and chronic obstructive pulmonary disease: are the challenges for pulmonary rehabilitation in the name? Chron Respir Dis. (2016) 13:372–82. doi: 10.1177/1479972316670104
19. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. (2010) 8:336–41. doi: 10.1016/j.ijsu.2010.02.007
20. Eysenck HJ. Meta-analysis of best-evidence synthesis? J Eval Clin Pract. (1995) 1:29–36. doi: 10.1111/j.1365-2753.1995.tb00005.x
21. Greco T, Zangrillo A, Biondi-Zoccai G, Landoni G. Meta-analysis: pitfalls and hints. Hear lung Vessel. (2013) 5:219–25.
22. United Nations Development Programme. Human Development Report 2019: Beyond Income, Beyond Averages, Beyond Today. New York, NY: United Nations Development Programme (2019). p. 366.
23. Wells GA, Wells G, Shea B, Shea B, O'Connell D, Peterson J. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. (2014). Available online at: https://www.ohri.ca//programs/clinical_epidemiology/oxford.asp
24. Amano H, Noike R, Yabe T, Watanabe I, Okubo R, Koizumi M, et al. Frailty and coronary plaque characteristics on optical coherence tomography. Heart Vessels. (2020) 35:750–61. doi: 10.1007/s00380-019-01547-2
25. Artiles-Armas M, Roque-Castellano C, Fariña-Castro R, Conde-Martel A, Acosta-Mérida MA, Marchena-Gómez J. Impact of frailty on 5-year survival in patients older than 70 years undergoing colorectal surgery for cancer. World J Surg Oncol. (2021) 19:106. doi: 10.1186/s12957-021-02221-6
26. Hubbard RE, Andrew MK, Fallah N, Rockwood K. Comparison of the prognostic importance of diagnosed diabetes, co-morbidity and frailty in older people. Diabet Med. (2010) 27:603–6. doi: 10.1111/j.1464-5491.2010.02977.x
27. Iyasere O, Brown EA, Johansson L, Davenport A, Farrington K, Maxwell AP, et al. Quality of life with conservative care compared with assisted peritoneal dialysis and haemodialysis. Clin Kidney J. (2019) 12:262–8. doi: 10.1093/ckj/sfy059
28. Kanenawa K, Isotani A, Yamaji K, Nakamura M, Tanaka Y, Hirose-Inui K, et al. The impact of frailty according to Clinical Frailty Scale on clinical outcome in patients with heart failure. ESC Hear Fail. (2021) 8:1552–61. doi: 10.1002/ehf2.13254
29. Komici K, Gnemmi I, Bencivenga L, Vitale DF, Rengo G, Di Stefano A, et al. Impact of Galectin-3 circulating levels on frailty in elderly patients with systolic heart failure. J Clin Med. (2020) 9:229. doi: 10.3390/jcm9072229
30. Labenz C, Toenges G, Schattenberg JM, Nagel M, Huber Y, Marquardt JU, et al. Health-related quality of life in patients with compensated and decompensated liver cirrhosis. Eur J Intern Med. (2019) 70:54–9. doi: 10.1016/j.ejim.2019.09.004
31. Lefebvre M-CD, St-Onge M, Glazer-Cavanagh M, Bell L, Kha Nguyen JN, Viet-Quoc Nguyen P, et al. The effect of bleeding risk and frailty status on anticoagulation patterns in octogenarians with atrial fibrillation: the FRAIL-AF study. Can J Cardiol. (2016) 32:169–76. doi: 10.1016/j.cjca.2015.05.012
32. Liu Y, Liu S, Wang K, Liu H. Association of frailty with antiplatelet response among elderly Chinese patients with coronary artery disease undergoing percutaneous coronary intervention. Clin Appl Thromb. (2020) 26:1076029620915994. doi: 10.1177/1076029620915994
33. MacKenzie HT, Tugwell B, Rockwood K, Theou O. Frailty and diabetes in older hospitalized adults: the case for routine frailty assessment. Can J Diabetes. (2020) 44:241–245.e1. doi: 10.1016/j.jcjd.2019.07.001
34. Meguro T, Meguro Y, Kunieda T. Atrophy of the parahippocampal gyrus is prominent in heart failure patients without dementia. ESC Hear Fail. (2017) 4:632–40. doi: 10.1002/ehf2.12192
35. Mima K, Miyanari N, Kosumi K, Tajiri T, Kanemitsu K, Takematsu T, et al. The efficacy of adjuvant chemotherapy for resected high-risk stage II and stage III colorectal cancer in frail patients. Int J Clin Oncol. (2021) 26:903–12. doi: 10.1007/s10147-021-01876-1
36. Atif M, Saleem Q, Asghar S, Malik I, Ahmad N. Extent and predictors of poor glycaemic control among elderly pakistani patients with type 2 diabetes mellitus: a multi-centre cross-sectional study. Medicina. (2019) 55:21. doi: 10.3390/medicina55010021
37. Mima K, Miyanari N, Morito A, Yumoto S, Matsumoto T, Kosumi K, et al. Frailty is an independent risk factor for recurrence and mortality following curative resection of stage I–III colorectal cancer. Ann Gastroenterol Surg. (2020) 4:405–12. doi: 10.1002/ags3.12337
38. Misawa N, Higurashi T, Tachikawa J, Tanabe H, Yoshihara T, Ashikari K, et al. Clinical impact of evaluation of frailty in endoscopic submucosal dissection for early gastric cancer in elderly patients. Geriatr Gerontol Int. (2020) 20:461–6. doi: 10.1111/ggi.13905
39. Mlynarska A, Mlynarski R, Biernat J, Sosnowski M, Golba KS. Frailty syndrome in heart failure patients who are receiving cardiac resynchronization. Pacing Clin Electrophysiol. (2016) 39:370–4. doi: 10.1111/pace.12800
40. Moth EB, Blinman P, Stefanic N, Naganathan V, Grimison P, Stockler MR, et al. Estimating survival time in older adults receiving chemotherapy for advanced cancer. J Geriatr Oncol. (2020) 11:617–25. doi: 10.1016/j.jgo.2019.08.013
41. Nishikawa K, Ebisawa S, Miura T, Kato T, Yusuke K, Abe N, et al. Impact of frailty and age on clinical outcomes in patients who underwent endovascular therapy. J Endovasc Ther. (2021) 15266028211067728. doi: 10.1177/15266028211067729
42. Nixon AC, Brown J, Brotherton A, Harrison M, Todd J, Brannigan D. Implementation of a frailty screening programme and Geriatric Assessment Service in a nephrology centre : a quality improvement project. J Nephrol. (2020) 34:1215–24. doi: 10.1007/s40620-020-00878-y
43. Noguchi M, Tabata M, Obunai K, Shibayama K, Ito J, Watanabe H, et al. Clinical outcomes of transcatheter aortic valve implantation (TAVI) in nonagenarians from the optimized catheter valvular intervention-TAVI registry. Catheter Cardiovasc Interv Off J Soc Card Angiogr Interv. (2021) 97:E113–20. doi: 10.1002/ccd.28935
44. Okabe H, Ohsaki T, Ogawa K, Ozaki N, Hayashi H, Akahoshi S, et al. Frailty predicts severe postoperative complications after elective colorectal surgery. Am J Surg. (2019) 217:677–81. doi: 10.1016/j.amjsurg.2018.07.009
45. Okabe H, Osaki T, Ogawa K, Yusa T, Takeyama H, Ozaki N, et al. Frailty predicts severe postoperative complications after elective minimally invasive surgery in patients with colorectal cancer. Indian J Surg. (2020) 217:677–81. doi: 10.1007/s12262-019-02001-3
46. O'Mahony M, Mohammed K, Kasivisvanathan R. Cardiopulmonary exercise testing versus frailty, measured by the clinical frailty score, in predicting morbidity in patients undergoing major abdominal cancer surgery. World J Surg. (2021) 45:116–25. doi: 10.1007/s00268-020-05779-6
47. Bagienski M, Tokarek T, Wiktorowicz A, Dziewierz A, Rzeszutko L, Sorysz D, et al. Sex-related differences in clinical outcomes and quality of life after transcatheter aortic valve implantation for severe aortic stenosis. Postep w Kardiol interwencyjnej = Adv Interv Cardiol. (2017) 13:233–9. doi: 10.5114/aic.2017.70195
48. Papakonstantinou PE, Asimakopoulou NI, Papadakis JA, Leventis D. Frailty status affects the decision for long - term anticoagulation therapy in elderly patients with atrial fibrillation. Drugs Aging. (2018) 35:897–905. doi: 10.1007/s40266-018-0587-6
49. Parmar KR, Xiu PY, Chowdhury MR, Patel E, Cohen M. In-hospital treatment and outcomes of heart failure in specialist and non-specialist services: a retrospective cohort study in the elderly. Open Hear. (2015) 2:e000095. doi: 10.1136/openhrt-2014-000095
50. Paterni S, Okoye C, Calabrese AM, Niccolai F, Polini A, Caraccio N, et al. Prognostic value of glycated hemoglobin in frail older diabetic patients with hip fracture. Front Endocrinol. (2021) 12:770400. doi: 10.3389/fendo.2021.770400
51. Perego S, Zambon A, Nistri S, Bruni A, Motta S, Cavalieri D'Oro L, Rossi E, Annoni G, Bellelli G. Prevalence, clinical correlates, and burden of undiagnosed aortic stenosis in older patients: a prospective study in a non-cardiologic acute hospital ward. Aging Clin Exp Res. (2020) 32:1533–40. doi: 10.1007/s40520-020-01471-w
52. Pugh J, Aggett J, Goodland A, Prichard A, Thomas N, Donovan K, et al. Frailty and comorbidity are independent predictors of outcome in patients referred for pre-dialysis education. Clin Kidney J. (2016) 9:324–9. doi: 10.1093/ckj/sfv150
53. Saji M, Higuchi R, Tobaru T, Iguchi N, Takanashi S, Takayama M, et al. Impact of frailty markers for unplanned hospital readmission following transcatheter aortic valve implantation. Circ J. (2018) 82:2191–8. doi: 10.1253/circj.CJ-17-0816
54. Sakatoku K, Takeoka Y, Miura A, Araki T, Fujitani Y, Yamamura R, et al. Combination of frailty status and comorbidity score improves the stratification of survival in patients with myelodysplastic syndrome owing to good predictive capability for infection-related mortality. Clin Lymphoma Myeloma Leuk. (2019) 19:799–805. doi: 10.1016/j.clml.2019.09.610
55. Skladany L, Drotarova Z, Vnencakova J, Jancekova D, Molcan P, Koller T. Applicability and prognostic value of frailty assessment tools among hospitalized patients with advanced chronic liver disease. Croat Med J. (2021) 62:8–16. doi: 10.3325/cmj.2021.62.8
56. Stanjek-Cichoracka A, Wozniak-Grygiel E, Łaszewska A, Zembala M, Ochman M. Assessment of cytokines, biochemical markers of malnutrition and frailty syndrome patients considered for lung transplantation. Transplant Proc. (2019) 51:2009–13. doi: 10.1016/j.transproceed.2019.04.046
57. Sun C-Y, Huang C-C, Tsai Y-S, Chang Y-T, Ou C-H, Su W-C, et al. Clinical frailty scale in predicting postoperative outcomes in older patients undergoing curative surgery for urologic malignancies: a prospective observational cohort study. Urology. (2020) 144:38–45. doi: 10.1016/j.urology.2020.06.069
58. Buganza-Torio E, Mitchell N, Abraldes JG, Thomas L, Ma M, Bailey RJ, et al. Depression in cirrhosis - a prospective evaluation of the prevalence, predictors and development of a screening nomogram. Aliment Pharmacol Ther. (2019) 49:194–201. doi: 10.1111/apt.15068
59. Sunaga A, Hikoso S, Yamada T, Yasumura Y, Uematsu M, Tamaki S, et al. Prognostic impact of Clinical Frailty Scale in patients with heart failure with preserved ejection fraction. ESC Hear Fail. (2021) 8:3316–26. doi: 10.1002/ehf2.13482
60. Sze S, Pellicori P, Zhang J, Weston J, Squire IB, Clark AL. Effect of frailty on treatment, hospitalisation and death in patients with chronic heart failure. Clin Res Cardiol. (2021) 110:1249–58. doi: 10.1007/s00392-020-01792-w
61. Sze S, Zhang J, Pellicori P, Morgan D, Hoye A, Clark AL. Prognostic value of simple frailty and malnutrition screening tools in patients with acute heart failure due to left ventricular systolic dysfunction. Clin Res Cardiol. (2017) 106:533–41. doi: 10.1007/s00392-017-1082-5
62. Sze S, Pellicori P, Zhang J, Weston J, Clark AL. Identification of frailty in chronic heart failure. JACC Hear Fail. (2019) 7:291–302. doi: 10.1016/j.jchf.2018.11.017
63. Tanaka T, Suda K, Inaba K, Umeki Y, Gotoh A, Ishida Y, et al. Impact of frailty on postoperative outcomes for laparoscopic gastrectomy in patients older than 80 years. Ann Surg Oncol. (2019) 26:4016–26. doi: 10.1245/s10434-019-07640-0
64. Vinson AJ, Bartolacci J, Goldstein J, Swain J, Clark D, Tennankore KK. Predictors of need for first and recurrent emergency medical service transport to emergency department after dialysis initiation. Prehospital Emerg Care. (2020) 24:822–30. doi: 10.1080/10903127.2019.1701157
65. Wall SA, Huang Y, Keiter A, Funderburg A, Kloock C, Yuhasz N, et al. Integration of a geriatric assessment with intervention in the care of older adults with hematologic malignancies. Front Oncol. (2021) 11:775050. doi: 10.3389/fonc.2021.775050
66. Wojszel ZB, Kasiukiewicz A. Determinants of anticoagulant therapy in atrial fibrillation at discharge from a geriatric ward: cross sectional study. J Thromb Thrombolysis. (2020) 49:18–26. doi: 10.1007/s11239-019-01937-3
67. Wu HHL, Van Mierlo R, McLauchlan G, Challen K, Mitra S, Dhaygude AP, et al. Prognostic performance of clinical assessment tools following hip fracture in patients with chronic kidney disease. Int Urol Nephrol. (2021) 53:2359–67. doi: 10.1007/s11255-021-02798-7
68. Yamada S, Shimada M, Morine Y, Imura S, Ikemoto T, Arakawa Y, et al. Significance of frailty in prognosis after hepatectomy for elderly patients with hepatocellular carcinoma. Ann Surg Oncol. (2021) 28:439–46. doi: 10.1245/s10434-020-08742-w
69. Costa D, Aladio M, Girado CA, Pérez de la Hoz R, Sara Berensztein C. Frailty is independently associated with 1-year mortality after hospitalization for acute heart failure. Int J Cardiol Hear Vasc. (2018) 21:103–6. doi: 10.1016/j.ijcha.2018.10.004
70. Yamada S, Shimada M, Morine Y, Imura S, Ikemoto T, Saito Y, et al. Significance of frailty in prognosis after surgery in patients with pancreatic ductal adenocarcinoma. World J Surg Oncol. (2021) 19:94. doi: 10.1186/s12957-021-02205-6
71. Yamamoto T, Yamashita K, Miyamae K, Koyama Y, Izumimoto M, Kamimura Y, et al. The influence of frailty under direct oral anticoagulant use in patients with atrial fibrillation. Heart Asia. (2019) 11:e011212. doi: 10.1136/heartasia-2019-011212
72. Yanagita I, Fujihara Y, Eda T, Tajima M, Yonemura K, Kawajiri T, et al. Low glycated hemoglobin level is associated with severity of frailty in Japanese elderly diabetes patients. J Diabetes Investig. (2018) 9:419–425. doi: 10.1111/jdi.12698
73. Yanagita I, Fujihara Y, Iwaya C, Kitajima Y, Tajima M, Honda M, et al. Low serum albumin, aspartate aminotransferase, and body mass are risk factors for frailty in elderly people with diabetes-a cross-sectional study. BMC Geriatr. (2020) 20:200. doi: 10.1186/s12877-020-01601-z
74. Yoshida M, Takanashi Y, Harigai T, Sakurai N, Kobatake K, Yoshida H, et al. Evaluation of frailty status and prognosis in patients aged over 75 years with chronic kidney disease (CKD). Ren Replace Ther. (2020) 6:60. doi: 10.1186/s41100-020-00300-0
75. Yoshioka N, Takagi K, Morishima I, Morita Y, Uemura Y, Inoue Y, et al. Influence of preadmission frailty on short- and mid-term prognoses in octogenarians with ST-elevation myocardial infarction. Circ J. (2019) 84:109–18. doi: 10.1253/circj.CJ-19-0467
76. Du X. Frailty and anticoagulant therapy in patients aged 65 years or older with atrial fibrillation. Cardiovasc Innov Appl. (2019) 4:153–61. doi: 10.15212/CVIA.2019.0562
77. Ekerstad N, Swahn E, Janzon M, Alfredsson J, Löfmark R, Lindenberger M, et al. Frailty is independently associated with short-term outcomes for elderly patients with non-ST-segment elevation myocardial infarction. Circulation. (2011) 124:2397–404. doi: 10.1161/CIRCULATIONAHA.111.025452
78. Evans NR, Wall J, To B, Wallis SJ, Romero-Ortuno R, Warburton EA. Clinical frailty independently predicts early mortality after ischaemic stroke. Age Ageing. (2020) 49:588–91. doi: 10.1093/ageing/afaa004
79. Houghton JS, Nickinson AT, Helm JR, Dimitrova J, Dubkova S, Rayt HS, et al. Associations of clinical frailty with severity of limb threat and outcomes in chronic limb-threatening ischaemia. Ann Vasc Surg. (2021) 76:406–16. doi: 10.1016/j.avsg.2021.04.017
80. Church S, Rogers E, Rockwood K, Theou O. A scoping review of the Clinical Frailty Scale. BMC Geriatr. (2020) 20:393. doi: 10.1186/s12877-020-01801-7
81. Rockwood K, Song X, Mitnitski A. Changes in relative fitness and frailty across the adult lifespan: evidence from the Canadian National Population Health Survey. CMAJ. (2011) 183:E487–94. doi: 10.1503/cmaj.101271
82. Hanlon P, Nicholl BI, Jani BD, Lee D, McQueenie R, Mair FS. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: a prospective analysis of 493 737 UK Biobank participants. Lancet Public Heal. (2018) 3:e323–32. doi: 10.1016/S2468-2667(18)30091-4
83. Waite I, Deshpande R, Baghai M, Massey T, Wendler O, Greenwood S. Home-based preoperative rehabilitation (prehab) to improve physical function and reduce hospital length of stay for frail patients undergoing coronary artery bypass graft and valve surgery. J Cardiothorac Surg. (2017) 12:91. doi: 10.1186/s13019-017-0655-8
84. Stammers AN, Kehler DS, Afilalo J, Avery LJ, Bagshaw SM, Grocott HP, et al. Protocol for the PREHAB study-pre-operative rehabilitation for reduction of hospitalization after coronary bypass and valvular surgery: a randomised controlled trial. BMJ Open. (2015) 5:e007250. doi: 10.1136/bmjopen-2014-007250
85. Coleman SA, Cunningham CJ, Walsh JB, Coakley D, Harbison J, Casey M, et al. Outcomes among older people in a post-acute inpatient rehabilitation unit. Disabil Rehabil. (2012) 34:1333–8. doi: 10.3109/09638288.2011.636136
86. Nolan M, Power D, Long J, Horgan F. Frailty and its association with rehabilitation outcomes in a post-acute older setting. Int J Ther Rehabil. (2016) 23:33–40. doi: 10.12968/ijtr.2016.23.1.33
87. Attwell L, Vassallo M. Response to pulmonary rehabilitation in older people with physical frailty, sarcopenia and chronic lung disease. Geriatr. (2017) 2:9. doi: 10.3390/geriatrics2010009
88. Davies J, Whitlock J, Gutmanis I, Kane S-L. Inter-rater reliability of the retrospectively assigned clinical frailty scale score in a geriatric outreach population. Can Geriatr J. (2018) 21:1–5. doi: 10.5770/cgj.21.263
89. Shears M, Takaoka A, Rochwerg B, Bagshaw SM, Johnstone J, Holding A, et al. Assessing frailty in the intensive care unit: a reliability and validity study. J Crit Care. (2018) 45:197–203. doi: 10.1016/j.jcrc.2018.02.004
90. Darvall JN, Greentree K, Braat MS, Story DA, Lim WK. Contributors to frailty in critical illness: Multi-dimensional analysis of the Clinical Frailty Scale. J Crit Care. (2019) 52:193–9. doi: 10.1016/j.jcrc.2019.04.032
91. Ritt M, Schwarz C, Kronawitter V, Delinic A, Bollheimer LC, Gassmann KG, et al. Analysis of rockwood et al.'s clinical frailty scale and fried et al.'s frailty phenotype as predictors of mortality and other clinical outcomes in older patients who were admitted to a geriatric ward. J Nutr Health Aging. (2015) 19:1043–8. doi: 10.1007/s12603-015-0667-9
92. Tandon P, Tangri N, Thomas L, Zenith L, Shaikh T, Carbonneau M, et al. A rapid bedside screen to predict unplanned hospitalization and death in outpatients with cirrhosis: a prospective evaluation of the clinical frailty scale. Am J Gastroenterol. (2016) 111:1759–67. doi: 10.1038/ajg.2016.303
93. Moreno-Ariño M, Torrente Jiménez I, Cartanyà Gutiérrez A, Oliva Morera JC, Comet R. Assessing the strengths and weaknesses of the Clinical Frailty Scale through correlation with a frailty index. Aging Clin Exp Res. (2020) 32:2225–32. doi: 10.1007/s40520-019-01450-w
94. Vetrano DL, Palmer K, Marengoni A, Marzetti E, Lattanzio F, Roller-Wirnsberger R, et al. Frailty and multimorbidity: a systematic review and meta-analysis. J Gerontol A Biol Sci Med Sci. (2019) 74:659–66. doi: 10.1093/gerona/gly110
95. Uchmanowicz I, Lee CS, Vitale C, Manulik S, Denfeld QE, Uchmanowicz B, et al. Frailty and the risk of all-cause mortality and hospitalization in chronic heart failure: a meta-analysis. ESC Hear Fail. (2020) 7:3427–37. doi: 10.1002/ehf2.12827
96. Hamaya T, Hatakeyama S, Momota M, Narita T, Iwamura H, Kojima Y, et al. Association between the baseline frailty and quality of life in patients with prostate cancer (FRAQ-PC study). Int J Clin Oncol. (2021) 26:199–206. doi: 10.1007/s10147-020-01798-4
97. Onder G, Vetrano DL, Marengoni A, Bell JS, Johnell K, Palmer K. Accounting for frailty when treating chronic diseases. Eur J Intern Med. (2018) 56:49–52. doi: 10.1016/j.ejim.2018.02.021
98. Zazzara MB, Vetrano DL, Carfì A, Onder G. Frailty and chronic disease. Panminerva Med. (2019) 61:486–92. doi: 10.23736/S0031-0808.19.03731-5
99. World Health Organization. Topic Focus : Frailty and Intrinsic Capacity. Geneva: World Health Organization (2016).
100. Sirven N, Dumontet M, Rapp T. The dynamics of frailty and change in socio-economic conditions: evidence for the 65+ in Europe. Eur J Public Health. (2020) 30:715–9. doi: 10.1093/eurpub/ckaa068
101. Zhang Q, Ma Y, Lin F, Zhao J, Xiong J. Frailty and mortality among patients with chronic kidney disease and end-stage renal disease: a systematic review and meta-analysis. Int Urol Nephrol. (2020) 52:363–70. doi: 10.1007/s11255-019-02369-x
102. Williams GR, Deal AM, Sanoff HK, Nyrop KA, Guerard EJ, Pergolotti M, et al. Frailty and health-related quality of life in older women with breast cancer. Support Care Cancer. (2019) 27:2693–8. doi: 10.1007/s00520-018-4558-6
103. Uchmanowicz I, Lisiak M, Wleklik M, Gurowiec P, Kałuzna-Oleksy M. The relationship between frailty syndrome and quality of life in older patients following acute coronary syndrome. Clin Interv Aging. (2019) 14:805–16. doi: 10.2147/CIA.S204121
Keywords: frailty, Clinical Frailty Scale, Non-Communicable Diseases, chronic diseases, systematic review
Citation: Granata N, Vigoré M, Steccanella A, Ranucci L, Sarzi Braga S, Baiardi P and Pierobon A (2022) The Clinical Frailty Scale (CFS) employment in the frailty assessment of patients suffering from Non-Communicable Diseases (NCDs): A systematic review. Front. Med. 9:967952. doi: 10.3389/fmed.2022.967952
Received: 13 June 2022; Accepted: 26 July 2022;
Published: 16 August 2022.
Edited by:
Leonardo Bencivenga, CHU de Toulouse, FranceReviewed by:
KM Saif-Ur-Rahman, National University of Ireland Galway, IrelandCopyright © 2022 Granata, Vigoré, Steccanella, Ranucci, Sarzi Braga, Baiardi and Pierobon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martina Vigoré, bS50LnZpZ29yZUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.