 Menglai Wu1†
Menglai Wu1† Lijiang Luan
Lijiang Luan Jeremy Witchalls
Jeremy Witchalls Roger Adams
Roger Adams Jaquelin Bousie
Jaquelin Bousie Jia Han
Jia Han
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 15 September 2022
Sec. Rheumatology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.956188
Background: The use of physical therapy modalities, especially high intensity laser therapy (HILT), for individuals with knee osteoarthritis (KOA) is still controversial.
Objective: To compare the effects of HILT to other physical therapy modalities on symptoms and function in individuals with KOA.
Methods: Six databases (PubMed, Embase, Cochrane Library, Web of Science, EBSCO, and PEDro) were searched in March 2022. Included studies were randomized controlled trials involving HILT conducted on individuals with KOA. The end-trial weighted mean difference (WMD) and standard deviations (SD) with 95% confidence intervals (CI) were analyzed.
Results: Ten studies with 580 participants were obtained, of which nine were included in the final network meta-analysis. In terms of relieving pain, HILT demonstrated the highest probability of being among the most effective treatments, with surface under the cumulative ranking (SUCRA) = 100%, and compared to a control (placebo laser or exercise or a combination of both) on the visual analog scale (VAS) for pain it demonstrated significant benefits (WMD 1.66, 95% CI 1.48–1.84). For improving self-reported function, as measured by the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) total scores, the HILT SUCRA value led with 98.9%. When individuals with KOA were treated by HILT, the improvement in stiffness was statistically significant (WMD 0.78, 95% CI 0.52–1.04) but the amount of improvement was smaller than the minimal clinically important difference (MCID).
Conclusion: The current evidence suggests that HILT may be more effective than other physical therapy modalities for improving pain and function in individuals with KOA. For improving stiffness, however, it may not be clinically effective.
Systematic review registration: [https://www.researchregistry.com], identifier [1148].
Knee osteoarthritis (KOA) is a highly prevalent musculoskeletal disorder, occurring mostly in older adults (1). It is characterized by hypertrophy of bone at the joint margins, erosion of the articular cartilage and a wide range of biochemical and morphologic changes in the synovial membrane and joint capsule (1). Clinical manifestations of KOA include pain, joint stiffness, muscle weakness, and limited range of motion (2). Individuals with KOA often encounter difficulties in activities of daily living, such as walking and climbing, and report poor quality of life (3).
The treatment options for KOA include pharmacological, surgical and physical measures (2), while current clinical guidelines primarily recommend non-pharmacological and non-surgical conservative strategies (4, 5). Multifactorial physical therapy modalities have been widely utilized in clinical practice and are believed to be effective for improving symptoms, sport performance, and self-reported function in individuals with KOA (6, 7). These modalities usually involve hot pack treatment, electric stimulation, ultrasound, and combinations of these (4), and studies have found these physical therapy modalities to be beneficial for relieving pain and enhancing activities of daily living (5, 6).
In recent years, laser therapy has been introduced as a physical therapy modality for treating musculoskeletal conditions and has gained popularity since no evident side effects have been reported after intervention (8). Of all the laser therapies, high intensity laser therapy (HILT) is a relatively new type of electrotherapy modality (9). It is a powerful and painless physical modality that has demonstrated significant benefits in antalgic, anti-edema, and biostimulating effects (10). Research has suggested that during HILT, radiation from high intensity laser produces photo-chemical, photothermal, and photomechanical actions (11, 12), especially from neodymium-doped yttrium aluminum garnet (Nd: YAG) laser, which has been found to be powerful in penetrating into deep tissues.
Some reviews have assessed the effects of HILT on symptoms or physical performance in individuals with KOA (9, 13), and two systematic reviews have clearly reported benefits of HILT for pain and function in individuals with KOA using some self-reported scales (9, 14); however, the clinical effectiveness of these outcome measures is still unclear. In addition, little is known about the comparative intervention effects of HILT in relation to other physical therapy modalities. Although previous studies have shown that certain physical therapy modalities, including HILT, seem to be effective for reducing pain and providing physical and functional improvements in individuals with KOA (6, 9); there is yet no consensus about which of currently used physical therapy interventions may have the most benefit for improving symptoms and function in KOA. An answer would be helpful for physiotherapists wanting to select the optimal measurement and intervention in order to provide the most efficient and effective management for KOA.
Accordingly, the aim of current systematic review was to conduct a network meta-analysis (NMA) to compare the effects of HILT and other physical therapy modalities on symptoms and function in individuals with KOA. NMA has been introduced as a generalization of pairwise meta-analysis (15), where indirect effect estimates are calculated with the effect estimates from two comparisons having a common comparator (16); when there is a same object of comparison among the studies, the connections may be built with each other (15). It has been utilized to derive summary comparison measures from a variety of evidence, in order to clarify the effectiveness of one treatment compared to another (17). Additionally, this review aimed to use meta-analysis to further assess the effects of HILT on symptoms and function, and their associated minimal clinically important difference (MCID) values, in persons with KOA.
The current study was registered in the Research Registry1 (registration no. Reviewregistry1148), in accordance with the Preferred Reporting Items for Systematic Reviews Incorporating Network Meta-Analyses (PRISMA Extension Statement) guidelines and Systematic Reviews and Meta-Analyses (PRISMA 2020 statement) guidelines (18, 19).
A literature search was conducted in March 2022 in PubMed, Embase, Cochrane Library, Web of Science, EBSCO, and PEDro. No restriction was applied on language or the publication year. The search strategy used a mix of MeSH (or Publication Type) and free text terms from the following three key areas: knee osteoarthritis, high intensity laser therapy, and randomized controlled trial.
The entries were set in two steps: (1) In the PubMed database, the key word as “MeSH” was first identified according to the subject, and all relevant items were collected in the “Entry Terms” of “All MeSH Categories” by searching the “MeSH column”; (2) In the Embase database, the key word was again retrieved in the “Emtree column”; if there are new items in the “use preferred term” of “find term,” they would be supplemented. The PubMed search strategy is as follow: (osteoarthritis, knee [MeSH] OR osteoarthritis knee [Title/Abstract] OR knee osteoarthritides [Title/Abstract] OR knee osteoarthritis [Title/Abstract] OR osteoarthritides, knee [Title/Abstract] OR osteoarthritis of knee [Title/Abstract] OR knee, osteoarthritis of [Title/Abstract] OR knees, osteoarthritis of [Title/Abstract] OR osteoarthritis of knees [Title/Abstract]) AND (high intensity laser [MeSH] OR high intensity laser therapy [Title/Abstract] OR high intensity laser therapies [Title/Abstract] OR therapies, high intensity laser [Title/Abstract] OR therapy, high intensity laser [Title/Abstract]) AND (randomized controlled trial [Publication Type] OR randomized [Title/Abstract] OR double-blind [Title/Abstract] OR placebo [Title/Abstract] OR controlled clinical trial [Publication Type] OR controlled [Title/Abstract] OR random [Title/Abstract] OR trial [Title/Abstract]).
Two assessors (M.W. and L.L.) independently assessed all searched studies, screening all titles and abstracts. Full articles of the potential studies were evaluated to obtain eligible trials, and the references in the obtained studies were examined to make sure that all relevant studies were included.
Studies were included by following the PICOS criteria: (1) Participants: individuals with knee osteoarthritis; (2) Interventions: high intensity laser therapy; (3) Comparators: no restriction; (4) Outcomes: no restriction was applied to outcome measures, however, the present network meta-analysis focused on the symptoms and function; (5) Study design: randomized controlled trials.
The exclusion criteria were: (1) Trials performed in vitro, with animals, cadavers, simulators, or prosthesis, and those conducted after total knee replacement; (2) Studies that were case reports, or descriptive studies, or not published as peer-reviewed journal articles.
The literature quality evaluation and risk of bias assessment were conducted independently by two assessors using the Physiotherapy Evidence Database (PEDro) scale and the Cochrane Risk of Bias tool, respectively. Research has shown that both tools are reliable for assessing the quality of studies and evaluating risk of bias (20, 21). The scores for each paper were achieved by the two assessors reaching an agreement through discussion, and any disagreements were resolved by a third reviewer.
Output from the PEDro scale contains 11 items with a total score out of 10 (item 1 is not scored). Each item is scored “no” (0 point) or “yes” (1 point); a score above 6 indicates high quality study, and scores of less than 6 reflect greater potential for biases to affect the results of the trial (22, 23).
Output from the Cochrane Risk of Bias tool is shown as illustrations covering random sequence generation and allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and “other bias.” Each entry is then judged to be at an unclear, low, or high risk of bias (24, 25).
All data were extracted by two independent reviewers and included; KOA inclusion criteria, participant characteristics (age, sex, height, and weight), HILT or control treatment protocols, the type of laser device, and outcome measures appropriate for analysis. Furthermore, because the purpose of the current study was to compare the effects of HILT and other physical therapy modalities, the HILT intervention was assigned the experimental group, and the control group was any physical therapy modality that was not HILT. Disagreements were resolved by discussion with a third reviewer.
With regard to outcome measures, those of high reliability and practicability, frequently adopted in studies of HILT for KOA were considered. In addition, outcome measures that are representative for the evaluation of knee function in persons with KOA were included. Moreover, they should employ measures suitable for network meta-analysis, presenting baseline and post-intervention data, and able to be compared with their MCID.
The following were documented; the visual analog scale (VAS) (score: 0–10) that evaluates intensity of pain (26), with the MCID for pain in knee osteoarthritis estimated to be 0.9 units (27); and scores from the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), that consists of the three sub-scales of pain (0–20), stiffness (0–8), and function (0–68) (a lower score indicates less dysfunction) (28), covering the basic symptoms and characteristics of osteoarthritis, with MCID in KOA being 1.42, 1.30, and 7.65 points respectively (29). MCID values were adjusted for ease of comparison, as the original text adopted the 0–100 scale.
In this review, the outcome measurements (VAS pain points, WOMAC sub-scales, and total scores) were calculated as the mean change score (continuous data) between before and after treatment, with the weighted mean differences (WMD) and standard deviations (SD) [95% confidence intervals (CI)].
When comparing the effects of different physical therapy modalities, STATA was used to perform the network meta-analysis for conducting indirect comparisons. The network of HILT and other physical therapy modalities was presented using a network plot, and the surface under the cumulative ranking (SUCRA) probability was utilized to rank the effectiveness of different physical therapy modalities.
In addition, the meta-analyses were performed using RevMan (Version 5.3) to evaluate the effect of HILT compared to a control such as placebo. The randomized effects model with the inverse variance method was used, and I2 tests were applied to evaluate the statistical heterogeneity (values exceeding 50% implied a moderate to high heterogeneity), and a p-value less than 0.05 taken to indicate a statistically significant difference.
A total of 209 relevant studies from the six electronic databases were obtained, and 10 RCTs involving 580 participants were selected (30–39), of which 9 were included in the final network meta-analysis (31–39). The one study not included had no post-intervention outcome measures (30). The detailed selection process is shown in Figure 1.
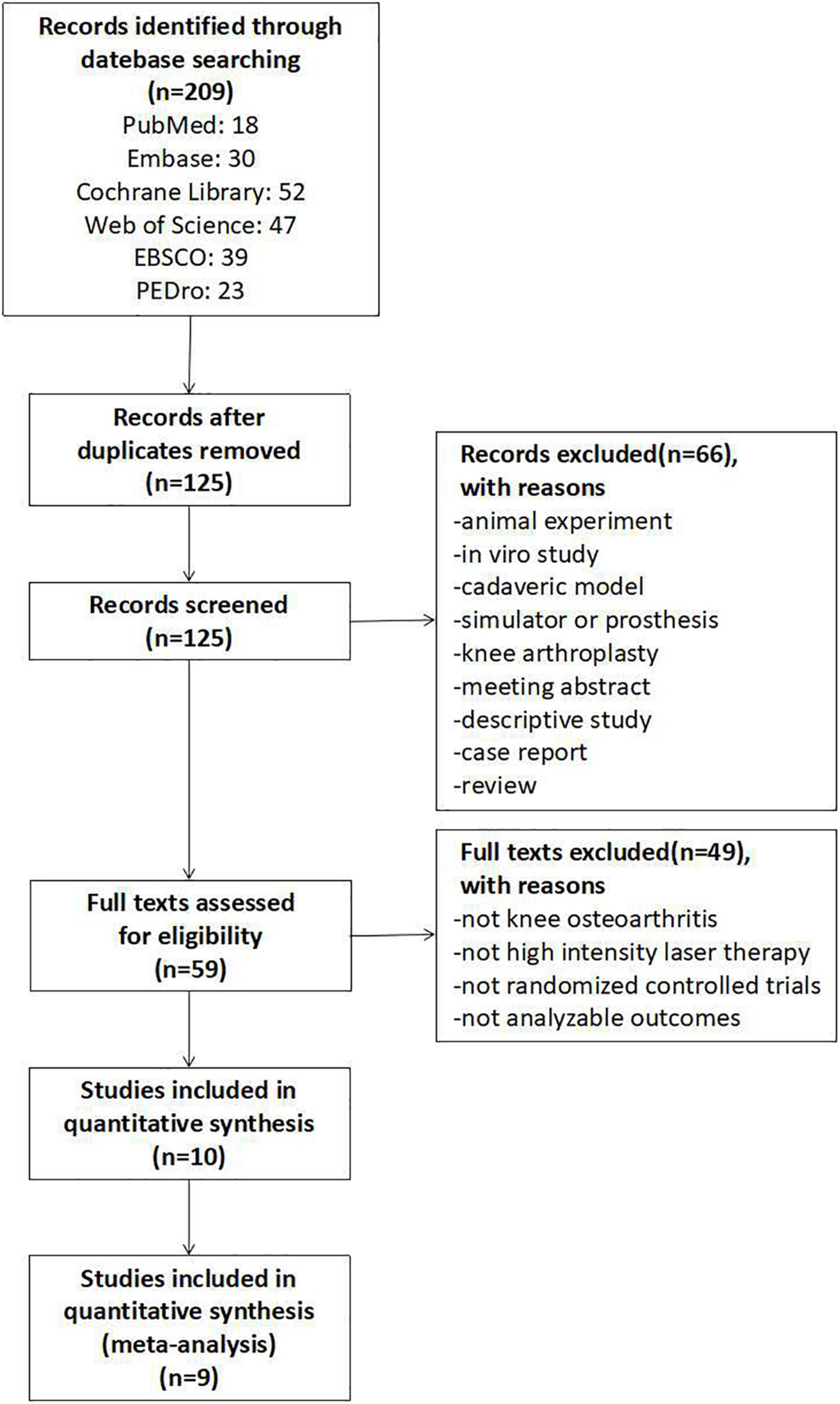
Figure 1. Flowchart of study selection.
For all included studies, the average score on the PEDro scale, which ranges from 5 to 8, was 6.3, and the quality evaluation details are presented in Table 1. The most frequent shortcomings of the obtained trials were: unclear description of concealed allocation, ambiguous information about the outcome measures, and inadequate blinding methods. Overall, the quality of the included studies was moderate.
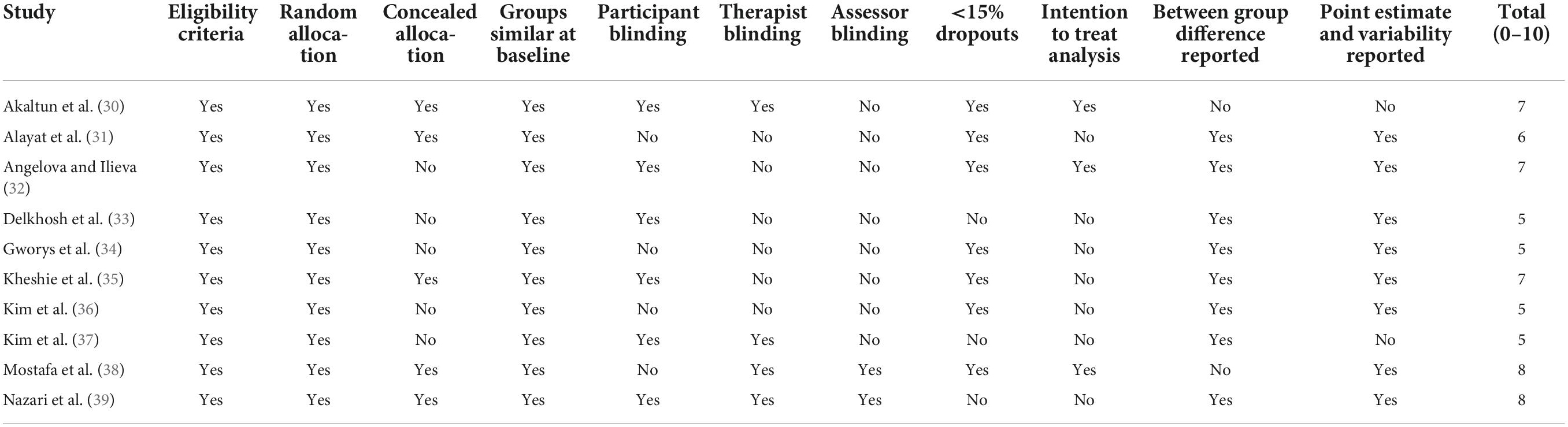
Table 1. Physiotherapy evidence database (PEDro) scores of included studies.
The summary risk of bias assessment with the Cochrane Collaboration criteria is reported in Figure 2. The included studies all described a low risk of bias within the process of random sequence generation. However, the allocation concealment and outcome data were unclear in several trials (32–34, 36, 37). In addition, some studies were classified as having high risk of bias in performance and detection because the researchers participated in the interventions and/or assessments (30–37), or the participants were not blinded to the treatment (31, 34, 36, 38).
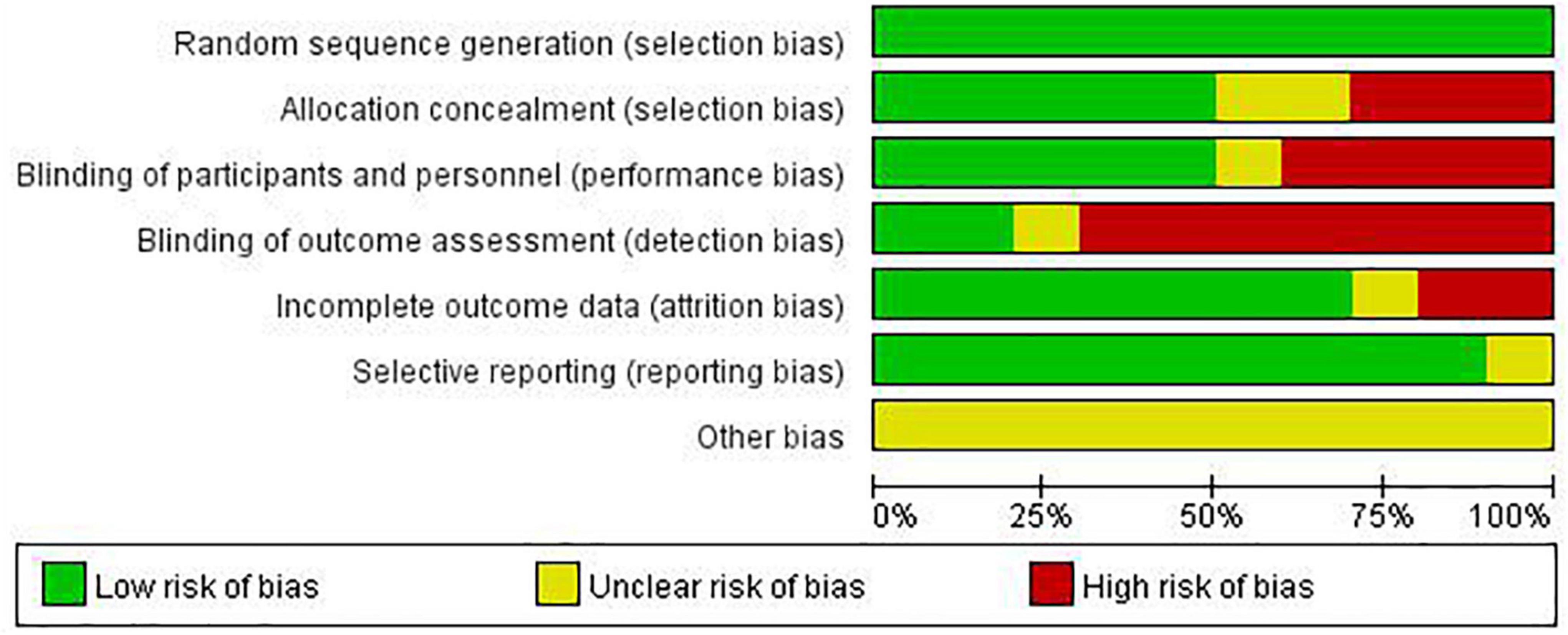
Figure 2. Risk of bias graph.
The included studies were published from 2009 to 2022 (30–39). All participants had a diagnosis of KOA, and their characteristics and measures of intervention are summarized in Table 2.
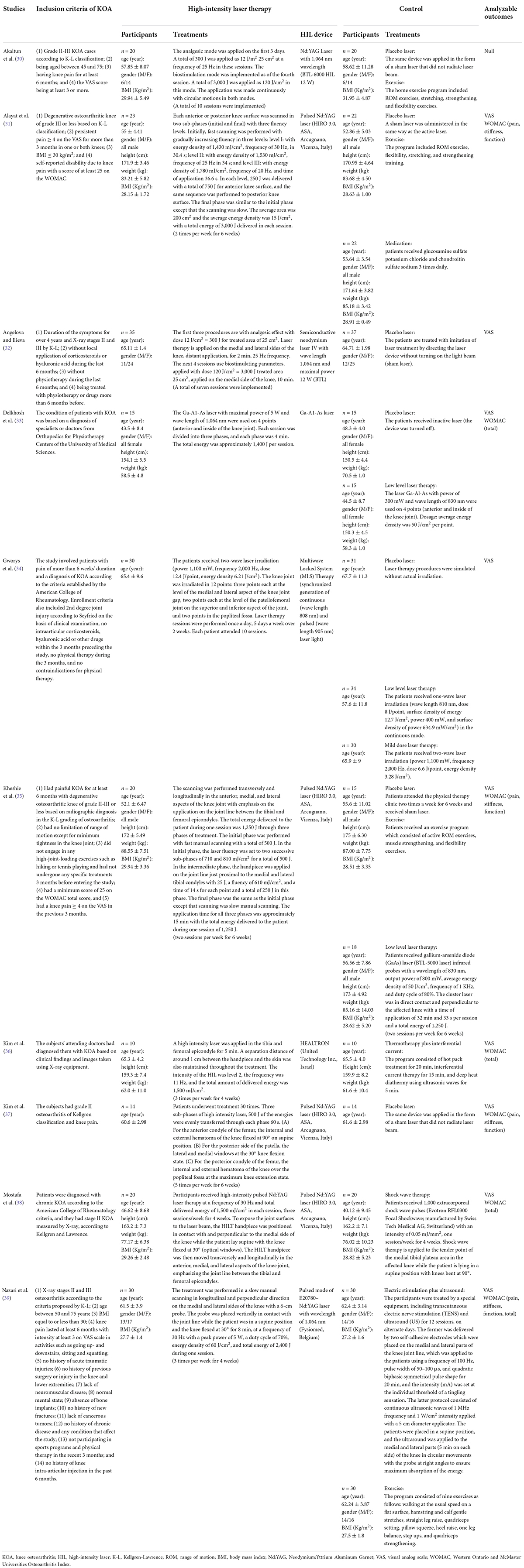
Table 2. Characteristics of included studies.
In terms of high intensity laser therapy, the devices employed and programs adopted were different between trials, however, the main components of each protocol could be identified. With regard to the control group, in this review placebo laser or exercise or a combination of both were classified into one category—placebo laser (plus exercise)—since the placebo laser was almost completely ineffective and exercise was only an auxiliary measure in the included studies when it was used as a control. For other physical therapy modalities, the classification was based on the treatment characteristics as described in the original study.
Specifically, treatments analyzed included eight for placebo laser (plus exercise) (30–35, 37, 39), ten for HILT (30–39), three for low level laser therapy (33–35), one for mild dose laser therapy (34), one for thermotherapy plus interferential current (36), one for shock wave therapy (38), and one for electric stimulation plus ultrasound (39).
To assess the efficacy of HILT and other physical therapy modalities for relieving pain in persons with KOA, a network of treatment was conducted, consisting of seven competing interventions (Figure 3). Except for high intensity laser therapy with 197 participants and placebo laser (plus exercise) with 164 participants, there are relatively more studies using low level laser therapy, with 67 participants; while the experiments of adopting mild dose laser therapy, thermotherapy plus interferential current, shock wave therapy, and electric stimulation plus ultrasound were all with 30 or fewer subjects.
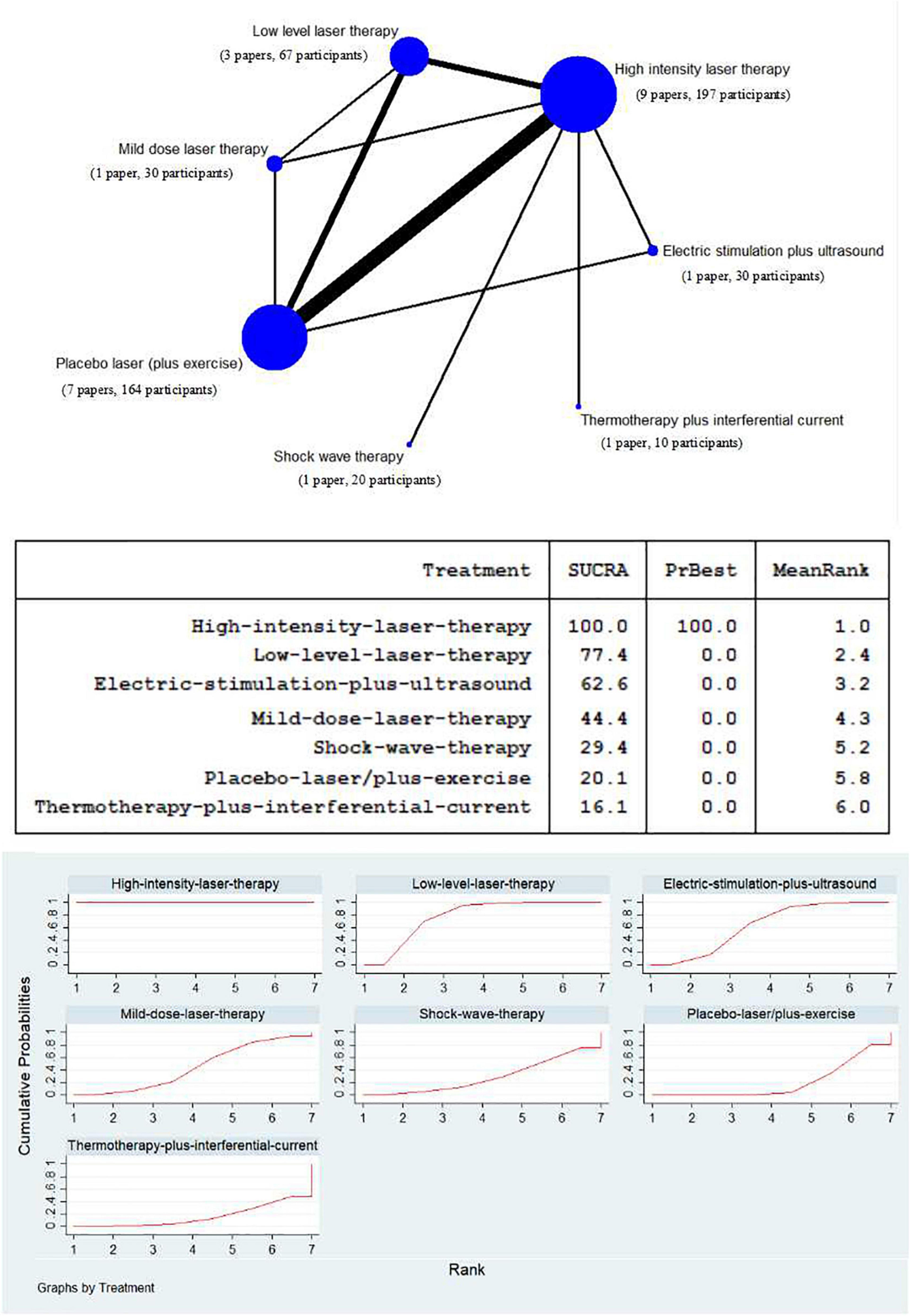
Figure 3. Network meta-analysis plot for the assessment of high intensity laser therapy (HILT) and other physical therapy modalities (nodes are weighted in accordance with the number of trials including the respective treatments. The larger the size of node and the thicker the lines are, the more studies are involved). Treatment relative ranking [the PrBest means the estimated probability that the treatment is the best one. The lower the value of Mean Rank is, the higher the efficacy of the treatment may be. The ranking probability plot for the assessment of improved visual analog scale (VAS) pain at the end of the physical therapy modalities is shown].
The SUCRA data synthesis (Figure 3) showed that high intensity laser therapy had the highest probability (100.0%) of being among the most effective treatments. In addition, low level laser therapy was superior to mild dose laser therapy, where the former was at 77.4% and the latter at 44.4%. Furthermore, with regard to other physical therapy modalities, apart from placebo laser (plus exercise) (20.1%), electric stimulation plus ultrasound, shock wave therapy, and thermotherapy plus interferential current stood at 62.6, 29.4, and 16.1%, respectively.
When compared to low level laser therapy, the effect of HILT measured by VAS pain scores was significantly greater (WMD: 0.81, 95% CI: 0.44–1.18, I2 = 46%, p < 0.0001; Figure 4).

Figure 4. Forest plot of the visual analog scale (VAS)-pain in high intensity laser therapy (HILT) vs. Low level laser therapy.
High intensity laser therapy was significantly superior to control [placebo laser (plus exercise)] when compared using outcomes assessed by VAS pain scores (WMD: 1.66, 95% CI: 1.48–1.84, I2 = 0%, p < 0.00001; Figure 5), with an effect which exceeded its MCID value of 0.9 (Table 3).
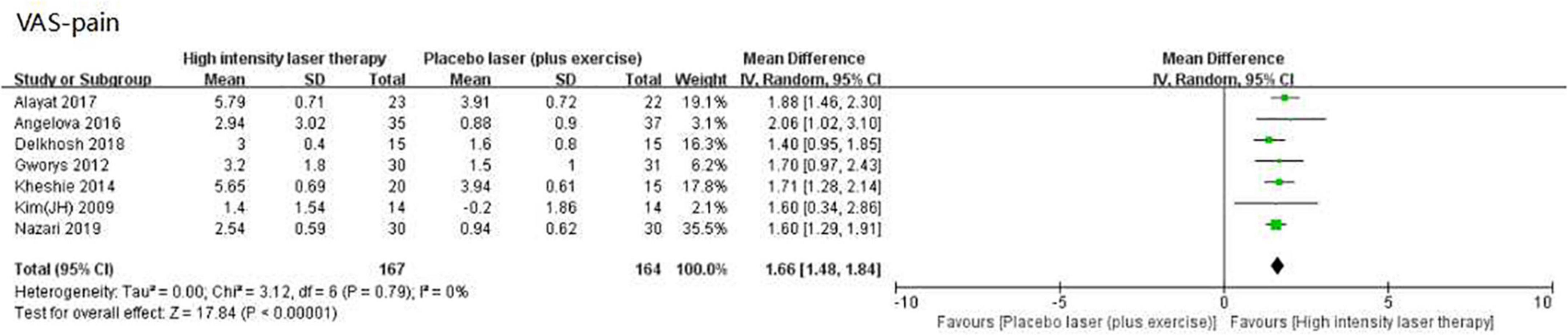
Figure 5. Forest plot of the visual analog scale (VAS)-pain in high intensity laser therapy (HILT) vs. Placebo laser (plus exercise).
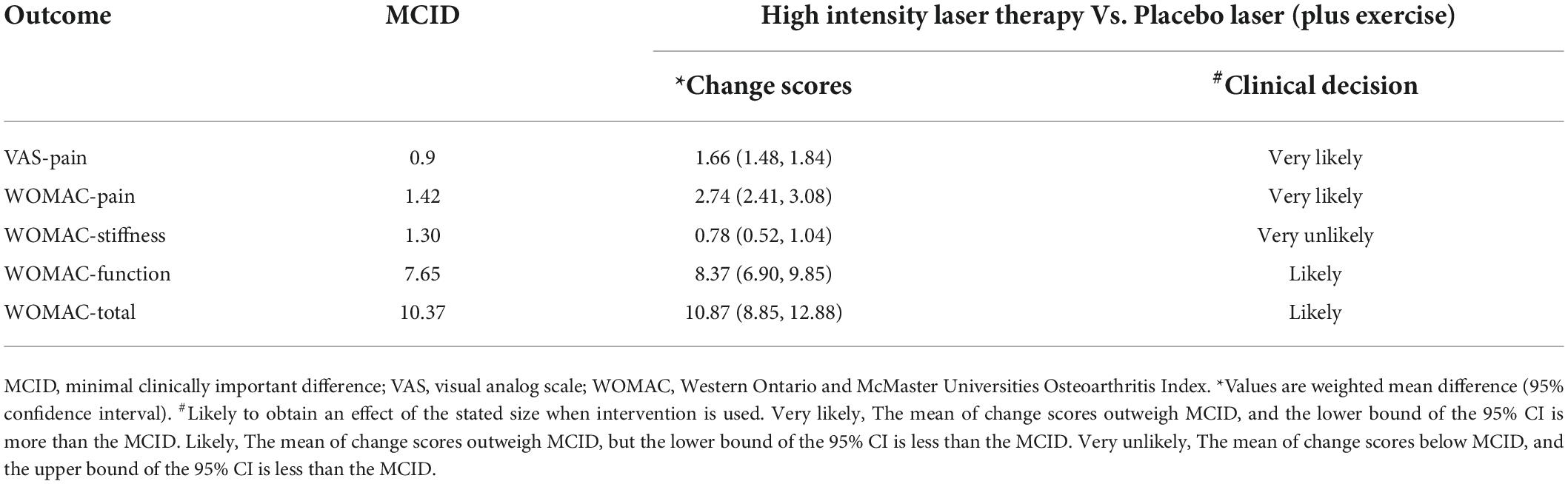
Table 3. Comparison of intervention effects and MCID.
Due to the limitation of insufficient number of studies with three WOMAC sub-scales (only four studies), the WOMAC total scores of the eligible studies were counted to conduct a network of treatment, comparing the efficacy of HILT and other physical therapy modalities in terms of improving symptoms and function in individuals with KOA, which consisted of six competing interventions as follows: 132 participants of high intensity laser therapy, 96 participants of placebo laser (plus exercise), 33 participants of low level laser therapy, 30 participants of electric stimulation plus ultrasound, 20 participants of shock wave therapy, and 10 participants of thermotherapy plus interferential current (Figure 6).
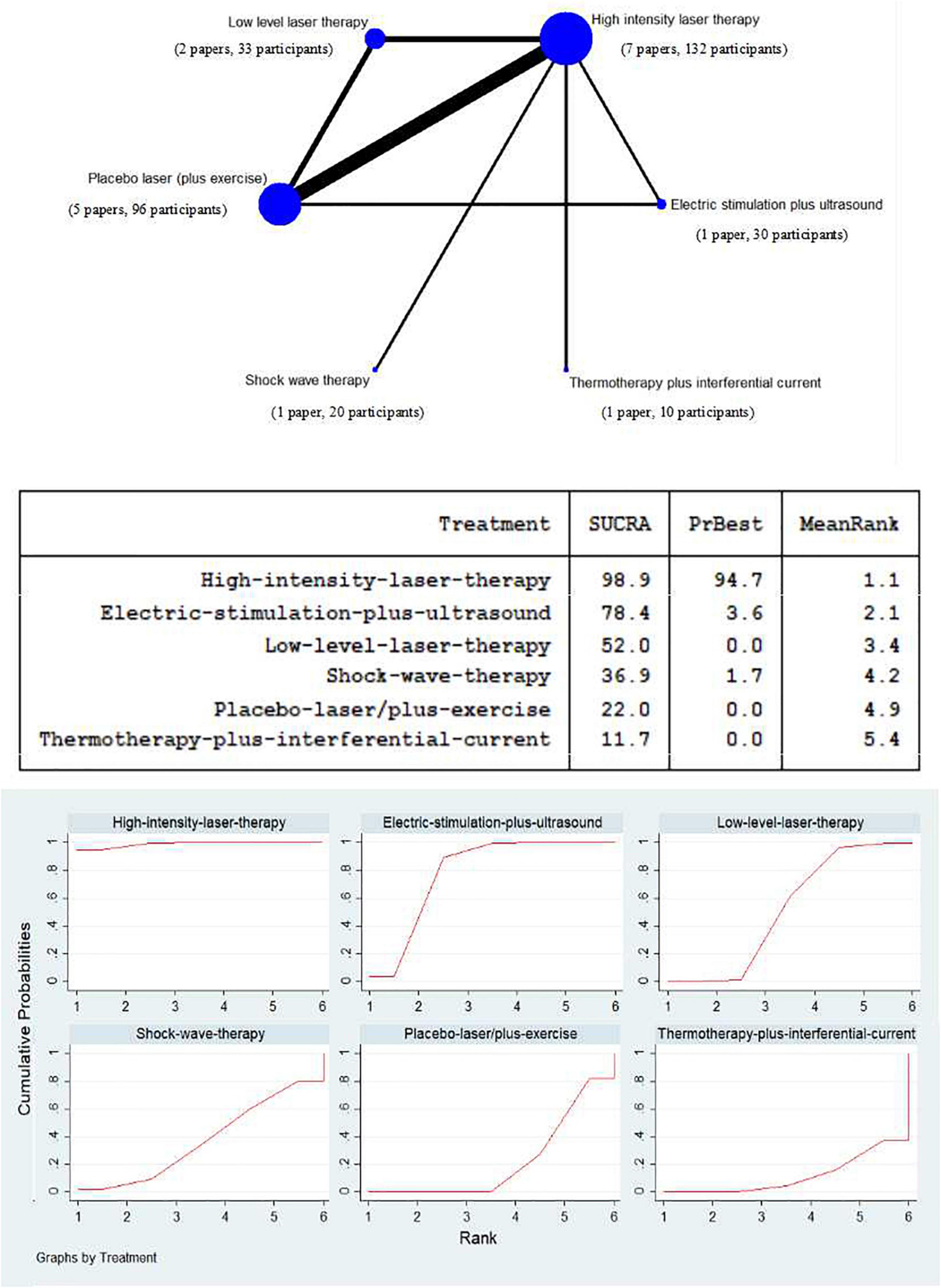
Figure 6. Network meta-analysis plot for the assessment of high intensity laser therapy (HILT) and other physical therapy modalities (nodes are weighted in accordance with the number of trials including the respective treatments. The larger the size of node and the thicker the lines are, the more studies are involved). Treatment relative ranking (the PrBest means the estimated probability that the treatment is the best one. The lower the value of Mean Rank is, the higher the efficacy of the treatment may be. The ranking probability plot for the assessment of improved WOMAC total at the end of the physical therapy modalities is shown).
The SUCRA value of high intensity laser therapy, at 98.9%, was the highest in the compared treatments. The next two were electric stimulation plus ultrasound (SUCRA = 78.4%) and low level laser therapy (SUCRA = 52.0%). The SUCRA values of shock wave therapy, placebo laser (plus exercise), and thermotherapy plus interferential current were at relatively low levels, and scored 36.9, 22.0, and 11.7%, respectively (Figure 6).
Compared to low level laser therapy, when HILT was used there was greater improvement as reflected by the WOMAC total, with a difference which was statistically significant (WMD: 6.48, 95% CI: 4.07–8.89, I2 = 0%, p < 0.00001; Figure 7).

Figure 7. Forest plot of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)-total in high intensity laser therapy (HILT) vs. Low level laser therapy.
High intensity laser therapy demonstrated several benefits as measured by the WOMAC, with findings for its three sub-scales and total scores shown in Figure 8, all of which were statistically significant: (1) pain (WMD: 2.74, 95% CI: 2.41–3.08, I2 = 0%, p < 0.00001; Figure 8A); (2) stiffness (WMD: 0.78, 95% CI: 0.52–1.04, I2 = 0%, p < 0.00001; Figure 8B); (3) Function (WMD: 8.37, 95% CI: 6.90–9.85, I2 = 53%, p < 0.00001; Figure 8C); (4) Total (WMD: 10.87, 95% CI: 8.85–12.88, I2 = 65%, p < 0.00001; Figure 8D). The comparison of these meta-analysis results and their relevant MCID values are presented in Table 3.

Figure 8. Forest plot of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)-pain (A), WOMAC-stiffness (B), WOMAC-function (C), and WOMAC-total (D) in high intensity laser therapy (HILT) vs. Placebo laser (plus exercise).
The present network meta-analysis showed that the effect of HILT may be superior to other physical therapy modalities in the management of KOA. Although the results of the meta-analysis demonstrated that HILT was more effective than placebo laser (plus exercise), as judged by the WMD for VAS pain as well as for the WOMAC sub-scales and total, for WOMAC stiffness the WMD value did not reach its MCID.
In addition, a previous systematic review (14) was noteworthy, which conducted the meta-analysis, including some studies that are the same as those included in this review. However, there are some significant differences between the paper and this review. First, the previous review included 6 studies; while this study included 10 articles, and 9 of them were involved in meta-analysis. There were certain new information in the additional four studies (30, 33, 36, 38). Also, there was no language restriction in this systematic review; for example, this review included an article (33) that was written in Persian. Most importantly, this review did not only analyze the outcomes of comparing HILT with control, while it actually focused on comparing HILT to other existing physical therapy modalities for treating KOA by a network meta-analysis, which was aimed at drawing a guiding recommendation for therapists to choose physical therapy modality in the management of KOA. This was not available in previous studies.
Admittedly, comparing HILT to control, the data included in this review were not much more than that in the previous review. Only three studies (33, 36, 38) (105 participants) were added in meta-analysis (40 subjects, 45 subjects, and 20 subjects, respectively), which may not cause significant changes on the effects of HILT for individuals with KOA comparing to previous studies. However, the clinical effectiveness of HILT could be found in this study, which was previously unavailable, by comparing the result of meta-analysis with the MCID; moreover, this systematic review and meta-analysis is that the most studies were included at present, and its sample size and level of evidence are the most up-to-date and complete review of this body of literature.
High intensity laser such as Pulsed Nd:YAG has a high peak power laser (3 kW) with a wavelength (up to 1,000 nm), and can deliver sufficient dosage to reach deep target tissue, which has a positive effect on reducing pain in various types of musculoskeletal pain (31). Moreover, HILT that has several photochemistry effects projects a strong optical energy into the tissues where it can generate oscillatory stimulation, which has been demonstrated to improve tissue metabolism and blood circulation (37). This results in a rapid removal of inflammatory substances, improvement of mitochondrial oxidation and production of adenosine triphosphate that help to facilitate more efficient absorption of tissue edema (36, 37).
Additionally, due to its biostimulation, analgesic, and anti-inflammatory effects, HILT is a modality that can be used in many painful conditions (32, 39). The physiological mechanism by which HILT provides pain relief is proposed to occur through the necrotic cells being subjected to extremely high temperature, then exfoliated for a short time (32, 40). This laser application increases local blood circulation in joints, promotes exchange of nutrients within the cartilage, improves tissue regeneration, and consequently seems to be helpful in eliminating inflammation and reducing pain and edema (36, 39, 41).
Compared to other currently available physical therapy modalities as a control, HILT seems to be the most effective treatment for relieving pain in individuals with KOA (SUCRA = 100.0%). The second most effective treatment may be low level laser therapy (LLLT), which uses low intensity laser that has the potential to produce photochemical reactions and improve the metabolism of cells, without causing heat, in order to stimulate or inhibit the cells (42). LLLT has been used with several different diseases, mainly for pain relief (42). Moreover, LLLT is a safe and non-invasive method which has recently attracted the attention of many researchers interested in modalities for treatment of KOA (42).
In previous studies, LLLT has been found to effectively relieve pain and enhance function for individuals with KOA, and these were significant findings (42, 43). LLLT as a therapeutic approach does not release heat, does not damage tissue, and has a relatively mild amount of energy delivered to target tissues (43). The low penetration of low level laser, with power density (below 5 W/cm2) and wavelength (540–830 nm), has been widely shown to be secure and stable (42), and most of the technologies used in applications such as scanning, points, and acupuncture are already well-established in musculoskeletal conditions such as pain and arthritis (44). Many studies have also reported a significant effect of LLLT in reducing periarticular inflammation and swelling, as well as for enhancing knee microcirculation, ambulation, and quality of life, because it affects the mitochondrial membrane potential and protein conformational modulation (42, 43, 45).
According to the current research on laser therapy, both HILT and LLLT are commonly used, and it is possible for individuals with KOA to adopt either as a treatment in the management of pain (34, 35). However, while LLLT is adequately effective, and may be an appropriate treatment for KOA, from this review (SUCRA = 77.4%), HILT is able to penetrate tissues and joints strongly, so that it is more able than LLLT to enhance the metabolism of substances associated with pain, inflammation, and swelling (31, 34, 35), which may yield better improvement (HILT vs. LLLT on VAS pain, WMD: 0.81) (32). Admittedly, a further point is the cost of laser therapy. At present, on the market, high intensity laser is more expensive than low level laser to purchase (12, 33). Compared with low level laser, hospitals or physical therapy institutions need to spend more money to configure high intensity laser equipment, and, for patients, the cost of using HILT is also greater (33). Based on this, LLLT may be more suitable for both patients and therapists because it is more economical than HILT.
It is noteworthy that when using high intensity laser equipment for treatment, if the dose is insufficient, the resulting effect may not be as good as that with LLLT in individuals with KOA (34); so in this sense, mild dose laser therapy may not be recommended (SUCRA = 44.4%). Also, the SUCRA value of electric stimulation plus ultrasound, at 62.6%, was between that of LLLT and mild dose laser therapy, which may also have a positive effect on pain relief since the stimulation of sensory nerves by electricity can lead to an increase of the pain threshold (39).
The last three treatments were shock wave therapy, placebo laser (plus exercise), and thermotherapy plus interferential current. Shock wave therapy may be beneficial for relieving pain (38), but its effect may not be significant compared with the above treatments (SUCRA = 29.4%). Moreover, the SUCRA value of placebo laser (plus exercise) was more than that of thermotherapy plus interferential current, which indicated that it is possible that exercise therapy is more effective in relieving pain than thermotherapy involving items such as hot compress, hot pack, and heat dressing. The former improves local metabolism and blood circulation in knee joints (39), while the latter may only act on the skin, with little effect (36). Admittedly, the evidence associated with these findings was very limited (included studies were very few), thus they cannot be fully verified.
Lastly, in terms of pain management of individuals with KOA, as measured by VAS pain and WOMAC pain scores, the present meta-analysis has demonstrated that, when compared to a placebo laser (plus exercise), HILT achieved a significant improvement, with statistical significance and clear homogeneity. Notably, in the VAS pain scores of comparing HILT to control, a previous systematic review included six studies (14), and its result of meta-analysis was highly heterogeneous (I2 = 90); while this review included one more study and showed good homogeneity, indicating that the result of the current meta-analysis may have a higher credibility. Furthermore, as for pain change scores measured by whether VAS or WOMAC, not only the WMD but also the lower bound of the 95% CI was significantly more than the relevant MCID value (Table 3). These results further support the conclusion that HILT can significantly relieve pain in individuals with KOA.
High intensity laser therapy has been widely employed in the field of physical therapy, with many studies describing its effects in alleviating pain, inflammation, and swelling (9, 14, 36), and the above has further verified the effect of HILT on pain relief in individuals with KOA. In addition, HILT was beneficial for improving physical function in KOA (31, 35, 39), and the current systematic review also shows that HILT has a significant effect on improvement in self-reported function as measured by WOMAC total score and function sub-scale. Additionally, HILT may also be superior to LLLT for improving physical function (WOMAC total, WMD: 6.48).
This outcome is probably as a direct effect of pain reduction, which makes individuals feel more comfortable and compliant in their limbs, so that physical activity becomes easier to achieve (36, 39). In addition, HILT may be beneficial for improving sport performance since short-term treatment with high-intensity laser enhances cardio-vascular function, as the activity of hemoglobin increases after being heated (30, 31, 46). Such an effect, potentially generated by HILT, is well-reflected in the function sub-scale of the WOMAC, which is largely based on questionnaire items related to physical activities such as stepping, standing, squatting, walking, and housework (28).
Judging from the SUCRA value of included physical therapy modalities, HILT may still be the best option in the management of physical function for individuals with KOA. Additionally, electric stimulation plus ultrasound may be better than LLLT in improvement of physical function, which may be due to more stimulation of neuromuscular control by electricity and thus more facilitation of limb movements (39). The next three treatments are the same as the bottom three in the ranking of the effect of HILT on pain: shock wave therapy, placebo laser (plus exercise), and thermotherapy plus interferential current.
The effect of shock wave therapy on physical function was similar to that on pain, showing a relatively low probability of improvement (SUCRA = 36.9%). Previous research has shown that shock wave has a certain effect on the enhancement of the function in KOA, but this effect may not be substantial (6, 38). Finally, the SUCRA value for placebo laser (plus exercise) was still higher than that of thermotherapy plus interferential current, suggesting that thermotherapy may not be as effective as exercise in terms of functional improvement. Hot compress applied on the skin can improve local blood circulation, but has little effect in terms of improvement in physical function (36).
Compared to placebo laser (plus exercise), when HILT was used as a physical therapy intervention for persons with KOA, improvements were evident in function, stiffness, and total of the WOMAC. However, only changes on two sub-scales and total scores were statistically significant, other differences did not exceed the relevant MCID values.
For physical function, the positive effect of HILT compared to placebo laser (plus exercise) can also be observed in the WOMAC function scale, although the lower bound of the 95% CI for the effect (6.90) was below the specified MCID value of 7.65 (29). Of particular interest here was that there was heterogeneity in the pooled studies, largely as a result of one study involving exercise that consisted of nine events (39), measured by WOMAC function, which showed significantly superior effects to other trials for individuals with KOA. Comparing with a previous study (14), the current review found the clear cause of heterogeneity within WOMAC function. This finding suggests that combining HILT with a variety of exercises may have a greater effect with respect to improving physical function in individuals with KOA (47, 48).
In terms of other symptoms of KOA, specifically joint stiffness, the present review indicated that HILT enhancements may not be at a sufficient level to be beneficial. Although this result was similar to the previous review (14), the clinical significance of HILT for stiffness has not been explained; therefore, this study further explored this phenomenon. Specifically, results here showed that gains on the stiffness sub-scale of the WOMAC were less than its relevant MCID value, despite being statistically significant. There are two possible explanations for this finding: (1) individuals treated with high intensity laser are always in a static state (37), while the improvement of stiffness typically requires range of motion training that involves repeated flexion and extension of the knee joint (44, 49, 50). Consequently, HILT does not bring about changes that promotes utilization of knee range of motion (30). (2) Most of the studies included in the review involved trials that conducted a treatment protocol with a relatively short duration, usually of 4–6 weeks, where changes in range of motion due to slower neuromuscular adaptation may not be achievable. Typically, improving knee range of motion can be achieved in 8–12 weeks (51).
Finally, HILT yielded a significant benefit in KOA, seen from using outcomes assessed by the WOMAC total, although the lower bound of the 95% CI for the effect was below the specified MCID value, which is a meta-analysis that no study has conducted so far. This gain was mainly due to the improvement of pain and function caused by HILT in individuals with KOA. Yet its effect on stiffness was not ideal, which was possibly also the reason why the values in confidence interval did not all exceed its MCID. There was heterogeneity in this result from the meta-analysis, but this arose because of the study that involved multiple exercises (39). Had this study been excluded, the results of meta-analysis would be very homogeneous (I2 = 0). This again suggests that exercise plays a vital role in the rehabilitation of individuals with KOA.
There are several limitations associated with this study. First, some studies may have been missed because the databases searched were limited to those listed, and there may have been some potentially relevant trials that were not included due to the search terms used. Further, the evidence needed to draw conclusions may not be sufficient as a result of the fact that only nine studies were selected for network meta-analysis, and the sample size in some trials was relatively small. In addition, the participants were not perfectly homogeneous with respect to their demographics, including age, gender, height, weight, and KOA grade; however, there is a strength in this heterogeneity, in that the results are more generalizable, and able to be applied to a wider population demographic. Also, there were differences in the high intensity laser devices and the protocols of treatment among the included studies, such as treatment position, laser wavelength, duration, and frequency. Finally, the classification of physical therapy modality may not be accurate enough. In particular, the definition of placebo laser (plus exercise) may be imprecise due to the inclusion of a variety of exercise programs, and there were some uncertain effects when a physical therapy modality included supplementary treatments such as ultrasound and interferential current.
The current network meta-analysis showed that the effects of HILT may be superior to the effects obtained from other physical therapy modalities on pain and self-reported function in individuals with KOA. Given that the number of studies was limited, more high quality trials are needed to verify these findings. In addition, compared to placebo laser or exercise or a combination of both, HILT was able to relieve pain and may improve function in individuals with KOA, but may not be as clinically effective for improving knee stiffness. Clinicians working with individuals with KOA, when deciding whether to use HILT, should first determine which of pain or stiffness most need relief.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
MW and LL: conceptualization, methodology, formal analysis, investigation, and writing—original draft. AP, JW, RA, and JB: conceptualization, methodology, formal analysis, and writing—review and editing. JH: conceptualization, methodology, formal analysis, investigation, writing—review and editing, supervision, and funding acquisition. All authors read and approved the final version of the manuscript.
We acknowledge the support received from the National Natural Science Foundation of China (Grant No. 31870936) and the Science and Technology Commission of Shanghai Municipality (Grant No. 20XD1423200).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Brosseau L, Taki J, Desjardins B, Thevenot O, Fransen M, Wells GA, et al. The Ottawa panel clinical practice guidelines for the management of knee osteoarthritis. Clin Rehabil. (2017) 31:582–624. doi: 10.1177/0269215517691083
2. Jevsevar DS. Treatment of osteoarthritis of the knee: evidence-based guideline, 2nd edition. J Am Acad Orthop Surg. (2013) 21:571–6. doi: 10.5435/JAAOS-21-09-571
3. National Clinical Guideline Centre. National Institute for Health and Clinical Excellence: Guidance. In: Osteoarthritis: Care and Management in Adults. London: National Institute for Health and Care Excellence (2014). p. 8–28.
4. Bannuru RR, Osani MC, Vaysbrot EE, Arden NK, Bennell K, Bierma-Zeinstra SMA, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr Cartil. (2019) 27:1578–89. doi: 10.1016/j.joca.2019.06.011
5. Woods B, Manca A, Weatherly H, Saramago P, Sideris E, Giannopoulou C, et al. Cost-effectiveness of adjunct non-pharmacological interventions for osteoarthritis of the knee. PLoS One. (2017) 12:e0172749. doi: 10.1371/journal.pone.0172749
6. Bennell KL, Buchbinder R, Hinman RS. Physical therapies in the management of osteoarthritis: current state of the evidence. Curr Opin Rheumatol. (2015) 27:304–11. doi: 10.1097/BOR.0000000000000160
7. Bjordal JM, Johnson MI, Lopes-Martins RA, Bogen B, Chow R, Ljunggren AE. Short-term efficacy of physical interventions in osteoarthritic knee pain. A systematic review and meta-analysis of randomised placebo-controlled trials. BMC Musculoskelet Disord. (2007) 8:51. doi: 10.1186/1471-2474-8-51
8. Jang H, Lee H. Meta-analysis of pain relief effects by laser irradiation on joint areas. Photomed Laser Surg. (2012) 30:405–17. doi: 10.1089/pho.2012.3240
9. Wyszynska J, Bal-Bochenska M. Efficacy of high-intensity laser therapy in treating knee osteoarthritis: a first systematic review. Photomed Laser Surg. (2018) 36:343–53. doi: 10.1089/pho.2017.4425
10. Dundar U, Turkmen U, Toktas H, Solak O, Ulasli AM. Effect of high-intensity laser therapy in the management of myofascial pain syndrome of the trapezius: a double-blind, placebo-controlled study. Lasers Med Sci. (2015) 30:325–32. doi: 10.1007/s10103-014-1671-8
11. Dundar U, Turkmen U, Toktas H, Ulasli AM, Solak O. Effectiveness of high-intensity laser therapy and splinting in lateral epicondylitis; a prospective, randomized, controlled study. Lasers Med Sci. (2015) 30:1097–107. doi: 10.1007/s10103-015-1716-7
12. Venosa M, Romanini E, Padua R, Cerciello S. Comparison of high-intensity laser therapy and combination of ultrasound treatment and transcutaneous nerve stimulation in patients with cervical spondylosis: a randomized controlled trial. Lasers Med Sci. (2019) 34:947–53. doi: 10.1007/s10103-018-2682-7
13. Ahmad MA, Hamid MSA, Yusof A. Effects of low-level and high-intensity laser therapy as adjunctive to rehabilitation exercise on pain, stiffness and function in knee osteoarthritis: a systematic review and meta-analysis. Physiotherapy. (2022) 114:85–95. doi: 10.1016/j.physio.2021.03.011
14. Song HJ, Seo HJ, Kim D. Effectiveness of high-intensity laser therapy in the management of patients with knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. J Back Musculoskelet Rehabil. (2020) 33:875–84. doi: 10.3233/BMR-191738
15. Li L, Tian J, Tian H, Moher D, Liang F, Jiang T, et al. Network meta-analyses could be improved by searching more sources and by involving a librarian. J Clin Epidemiol. (2014) 67:1001–7. doi: 10.1016/j.jclinepi.2014.04.003
16. Thorlund K, Mills EJ. Sample size and power considerations in network meta-analysis. Syst Rev. (2012) 1:41. doi: 10.1186/2046-4053-1-41
17. Hutton B, Salanti G, Chaimani A, Caldwell DM, Schmid C, Thorlund K, et al. The quality of reporting methods and results in network meta-analyses: an overview of reviews and suggestions for improvement. PLoS One. (2014) 9:e92508. doi: 10.1371/journal.pone.0092508
18. Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. (2015) 162:777–84. doi: 10.7326/M14-2385
19. Page MJ, Mckenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. J Clin Epidemiol. (2021) 134:103–12. doi: 10.1016/j.jclinepi.2021.02.003
20. Moseley AM, Rahman P, Wells GA, Zadro JR, Sherrington C, Toupin-April K, et al. Agreement between the cochrane risk of bias tool and physiotherapy evidence database (PEDro) scale: a meta-epidemiological study of randomized controlled trials of physical therapy interventions. PLoS One. (2019) 14:e0222770. doi: 10.1371/journal.pone.0222770
21. Armijo-Olivo S, Saltaji H, da Costa BR, Fuentes J, Ha C, Cummings GG. What is the influence of randomisation sequence generation and allocation concealment on treatment effects of physical therapy trials? A meta-epidemiological study. BMJ Open. (2015) 5:e008562. doi: 10.1136/bmjopen-2015-008562
22. Herbert R, Moseley A, Sherrington C. PEDro: a database of randomised controlled trials in physiotherapy. Health Inf Manag. (2016) 28:186–8. doi: 10.1177/183335839902800410
23. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomised controlled trials. Phys Ther. (2003) 83:713–21. doi: 10.1093/ptj/83.8.713
24. Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Collaboration (2011). Available online at: http://handbook.cochrane.org (accessed December 03, 2015).
25. Moseley AM, Herbert RD, Maher CG, Sherrington C, Elkins MR. Reported quality of randomized controlled trials of physiotherapy interventions has improved over time. J Clin Epidemiol. (2011) 64:594–601. doi: 10.1016/j.jclinepi.2010.08.009
26. Revill SI, Robinson JO, Rosen M, Hogg MIJ. The reliability of a linear analogue for evaluating pain. Anaesthesia. (1976) 31:1191–8. doi: 10.1111/j.1365-2044.1976.tb11971.x
27. Bellamy N, Hochberg M, Tubach F, Martin-Mola E, Awada H, Bombardier C, et al. Development of multinational definitions of minimal clinically important improvement and patient acceptable symptomatic state in osteoarthritis. Arthritis Care Res. (2015) 67:972–80. doi: 10.1002/acr.22538
28. Woolacott NF, Corbett MS, Rice SJC. The use and reporting of WOMAC in the assessment of the benefit of physical therapies for the pain of osteoarthritis of the knee: findings from a systematic review of clinical trials. Rheumatology. (2012) 51:1440–6. doi: 10.1093/rheumatology/kes043
29. Angst F, Benz T, Lehmann S, Aeschlimann A, Angst J. Multidimensional minimal clinically important differences in knee osteoarthritis after comprehensive rehabilitation: a prospective evaluation from the bad Zurzach osteoarthritis study. RMD Open. (2018) 4:e000685. doi: 10.1136/rmdopen-2018-000685
30. Akaltun MS, Altindag O, Turan N, Gursoy S, Gur A. Efficacy of high intensity laser therapy in knee osteoarthritis: a double-blind controlled randomized study. Clin Rheumatol. (2021) 40:1989–95. doi: 10.1007/s10067-020-05469-7
31. Alayat MSM, Aly THA, Elsayed AEM, Fadil ASM. Efficacy of pulsed Nd:YAG laser in the treatment of patients with knee osteoarthritis: a randomized controlled trial. Lasers Med Sci. (2017) 32:503–11. doi: 10.1007/s10103-017-2141-x
32. Angelova A, Ilieva EM. Effectiveness of high intensity laser therapy for reduction of pain in knee osteoarthritis. Pain Res Manag. (2016) 2016:9163618. doi: 10.1155/2016/9163618
33. Delkhosh CT, Fatemi E, Ghorbani R, Mohammadi R. Comparing the immediate and long-term effects of low and high power laser on the symptoms of knee osteoarthritis. J Mazandaran Univ Med Sci. (2018) 28:69–77.
34. Gworys K, Gasztych J, Puzder A, Gworys P, Kujawa J. Influence of various laser therapy methods on knee joint pain and function in patients with knee osteoarthritis. Ortop Traumatol Rehabil. (2012) 14:269–77. doi: 10.5604/15093492.1002257
35. Kheshie A, Alayat M, Ali M. High-intensity versus low-level laser therapy in the treatment of patients with knee osteoarthritis: a randomized controlled trial. Lasers Med Sci. (2014) 29:1371–6. doi: 10.1007/s10103-014-1529-0
36. Kim GJ, Choi J, Lee S, Jeon C, Lee K. The effects of high intensity laser therapy on pain and function in patients with knee osteoarthritis. J Phys Ther Sci. (2016) 28:3197–9. doi: 10.1589/jpts.28.3197
37. Kim JH, Lee S, Kim JH, Kim KS, Yoo CW, Chun TH. Efficacy of high intensity laser therapy in the mild osteoarthritis of the knee: a randomized double-blind controlled trial. J Korean Orthop Res Soc. (2009) 12:53–9.
38. Mostafa MSEM, Hamada HA, Kadry AM, Zahran SS, Helmy NA. Effect of high-power laser therapy versus shock wave therapy on pain and function in knee osteoarthritis patients: a randomized controlled trial. Photobiomodul Photomed Laser Surg. (2022) 40:198–204. doi: 10.1089/photob.2021.0136
39. Nazari A, Moezy A, Nejati P, Mazaherinezhad A. Efficacy of high-intensity laser therapy in comparison with conventional physiotherapy and exercise therapy on pain and function of patients with knee osteoarthritis: a randomized controlled trial with 12-week follow up. Lasers Med Sci. (2019) 34:505–16. doi: 10.1007/s10103-018-2624-4
40. Marquina N, Dumoulin-White R, Mandel A, Lilge L. Laser therapy applications for osteoarthritis and chronic joint pain – a randomized placebo-controlled clinical trial. Photon Lasers Med. (2012) 1:299–307. doi: 10.1515/plm-2012-0030
41. Helianthi DR, Simadibrata C, Srilestari A, Wahyudi ER, Hidayat R. Pain reduction after laser acupuncture treatment in geriatric patients with knee osteoarthritis: a randomized controlled trial. Acta Med Indones. (2016) 48:114–21.
42. Rayegani SM, Raeissadat SA, Heidari S, Moradi-Joo M. Safety and effectiveness of low-level laser therapy in patients with knee osteoarthritis: a systematic review and meta-analysis. J Lasers Med Sci. (2017) 8:S12–9. doi: 10.15171/jlms.2017.s3
43. Stausholm MB, Naterstad IF, Joensen J, Lopes-Martins RÁB, Sæbø H, Lund H, et al. Efficacy of low-level laser therapy on pain and disability in knee osteoarthritis: systematic review and meta-analysis of randomised placebo-controlled trials. BMJ Open. (2019) 9:e31142. doi: 10.1136/bmjopen-2019-031142
44. Meneses SF, Hunter DJ, Marques AP. Effect of low-level laser therapy (904nm) and static stretching exercises in patients with knee osteoarthritis: a randomised controlled trial. Osteoarthr Cartil. (2015) 23:A167–8. doi: 10.1016/j.joca.2015.02.932
45. Rayegani SM, Bahrami MH, Elyaspour D, Saeedi M, Sanjari H. Therapeutic effects of low level laser therapy (LLLT) in knee osteoarthritis, compared to therapeutic ultrasound. J Lasers Med Sci. (2012) 3:71–4.
46. Youssef EF, Muaidi QI, Shanb AA. Effect of laser therapy on chronic osteoarthritis of the knee in older subjects. J Lasers Med Sci. (2016) 7:112–9. doi: 10.15171/jlms.2016.19
47. Yavuz M, Ataoglu S, Özşahin M, Baki AE, Içmeli C. Compared effects and effectiveness in applications of isokinetic exercise, laser, and diclophenac iontophoresis in primary osteoarthritis of knee. Duzce Med J. (2013) 15:15–21.
48. Nejati P, Farzinmehr A, Moradi-Lakeh M. The effect of exercise therapy on knee osteoarthritis: a randomized clinical trial. Med J Islam Repub Iran. (2015) 29:186.
49. Luan L, Bousie J, Pranata A, Adams R, Han J. Stationary cycling exercise for knee osteoarthritis: a systematic review and meta-analysis. Clin Rehabil. (2021) 35:522–33. doi: 10.1177/0269215520971795
50. Suzuki Y, Iijima H, Tashiro Y, Kajiwara Y, Zeidan H, Shimoura K, et al. Home exercise therapy to improve muscle strength and joint flexibility effectively treats pre-radiographic knee OA in community-dwelling elderly: a randomized controlled trial. Clin Rheumatol. (2019) 38:133–41. doi: 10.1007/s10067-018-4263-3
51. Nahayatbin M, Ghasemi M, Rahimi A, Khademi-Kalantari K, Naimi SS, Tabatabaee SM, et al. The effects of routine physiotherapy alone and in combination with either tai chi or closed kinetic chain exercises on knee osteoarthritis: a comparative clinical trial study. Iran Red Cres Med J. (2018) 20:e62600. doi: 10.5812/ircmj.62600
Keywords: high intensity laser therapy, physical therapy, knee osteoarthritis, systematic review, network meta-analysis
Citation: Wu M, Luan L, Pranata A, Witchalls J, Adams R, Bousie J and Han J (2022) Is high intensity laser therapy more effective than other physical therapy modalities for treating knee osteoarthritis? A systematic review and network meta-analysis. Front. Med. 9:956188. doi: 10.3389/fmed.2022.956188
Received: 30 May 2022; Accepted: 19 August 2022;
Published: 15 September 2022.
Edited by:
Maria Maslinska, National Institute of Geriatrics, Rheumatology and Rehabilitation, PolandReviewed by:
Michał Jakubaszek, National Institute of Geriatrics, Rheumatology and Rehabilitation, PolandCopyright © 2022 Wu, Luan, Pranata, Witchalls, Adams, Bousie and Han. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jia Han, SmlhLkhhbkBDYW5iZXJyYS5lZHUuYXU=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.