 Silvia Vázquez-Cuesta1,2,3
Silvia Vázquez-Cuesta1,2,3 María Olmedo1,2
María Olmedo1,2 Elena Reigadas1,2,4,5*
Elena Reigadas1,2,4,5* Luis Alcalá1,2,6Mercedes Marín1,2,4,6Patricia Muñoz1,2,4,6Emilio Bouza1,2,4,5,6
Luis Alcalá1,2,6Mercedes Marín1,2,4,6Patricia Muñoz1,2,4,6Emilio Bouza1,2,4,5,6- 1Department of Clinical Microbiology and Infectious Diseases, Hospital General Universitario Gregorio Marañón, Madrid, Spain
- 2Instituto de Investigación Sanitaria Gregorio Marañón, Madrid, Spain
- 3Department of Biochemistry and Molecular Biology, Faculty of Biology, Universidad Complutense de Madrid, Madrid, Spain
- 4Department of Medicine, School of Medicine, Universidad Complutense de Madrid, Madrid, Spain
- 5ESCMID Study Group for Clostridioides difficile, Basel, Switzerland
- 6CIBER de Enfermedades Respiratorias (CIBERES CB06/06/0058), Madrid, Spain
Information on Clostridioides difficile infection (CDI) in patients with COVID-19 is scarce and points to an overall decrease of episodes during the pandemic. This situation results paradoxical, as COVID-19 patients had long periods of hospital stay and high use of antibiotics. We conducted a retrospective study from January 1st 2019 to December 31st 2020 comparing the incidence of hospital-acquired episodes of CDI (HA-CDI) among patients with and without COVID-19 admitted to our institution. During the study period, there were 47,048 patient admissions in 2019, 35,662 admissions of patients without COVID-19 in 2020 and 6,763 of COVID-19 patients. There were 68 episodes of HA-CDI in COVID-19 patients (14.75/10,000 days), 159 in 2020-non-COVID-19 patients (5.54/10,000 days) and 238 in 2019 (6.80/10,000 days). Comparison of HA-CDI in COVID-19 and non-COVID-19 patients indicates it occurs more frequently, in terms of CDI disease severity, COVID-19 does not seem to have a negative impact.
Introduction
The COVID-19 pandemic has imposed unreasonable workload on hospitals worldwide and has forced health professionals to work under unsuitable conditions (1, 2).
A high percentage of COVID-19 patients requiring hospitalization are admitted because of pneumonia -sometimes rapidly progressive-. Fear of concomitant presence of bacterial pathogens has led to massive use of antibacterial agents (3).
Under those conditions, seems logical to expect a considerable increase in the incidence of nosocomial Clostridioides difficile infection (HA-CDI) (4), although preliminary data seem to paradoxically indicate otherwise (5–8).
Data on purported HA-CDI decrease usually consider the figures of the whole hospital population and not the incidence of HA-CDI in a specific cohort of COVID-19 patients.
Our aim was to compare the incidence of HA-CDI during 2019 and 2020 in our hospital and describe the peculiarities of this disease in the COVID-19 population.
Materials and methods
Setting, design, and study population
This study was carried out at Hospital General Universitario Gregorio Marañón, Madrid (Spain), a university hospital with 1,350 beds. Determination of toxigenic C. difficile is routinely performed on all diarrheic stool samples from patients older than 2 years.
We conducted a retrospective study between January 1, 2019 and December 31, 2020, comparing HA-CDI data in COVID-19 patients against non-COVID-19 patients.
All patients fulfilling the definition of HA-CDI were considered potential cases for this study (9).
Definitions
An episode of CDI was defined as the presence of a positive toxigenic CDI test, accompanied by diarrhea (≥3 non-forming stools in 24 h) or findings of pseudomembranous colitis by colonoscopy, as per the definitions by the SHEA and IDSA guidelines (9). The severity of the CDI episode was defined according to the SHEA and IDSA guidelines (9).
We defined a HA-CDI when the diagnosis occurred at least 48 h after patients’ admission or documented overnight stay in a healthcare facility in the prior 4 weeks (9).
HO-CDI definition is when the diagnosis occurred at least 48 h after patients’ admission (9).
Recurrence of CDI (R-CDI) is present when CDI recurs within 8 weeks after a previous episode, provided the symptoms from the previous episode resolved after completion of initial treatment (10).
Death was considered to be CDI-related when there were no other attributable causes and/or it occurred within 10 days after CDI diagnosis and/or was due to known CDI-associated complications.
We considered immunosuppressed patients at admission those who presented with an compromised immunity due to any of the following: an active hematological malignancy (including leukemia, lymphoma, multiple myeloma), an active malignancy requiring recent cytotoxic chemotherapy, receipt of a prior hematopoietic stem cell transplant, receipt of a prior solid organ transplant, asplenia, neutropenia/pancytopenia due to other conditions, acquired or congenital immunodeficiency disorders or those receiving immunosuppressive agents.
Microbiological testing methods
Samples were processed using a rapid detection kit for toxigenic C. difficile. This rapid test consists of antigen detection by immunochromatography (C Diff Quik-Chek Complete assay, TechLab, Blacksburg, VA, United States) and a real-time polymerase chain reaction (PCR) of the toxin B gene (XpertTM C. Difficile Assay, GeneXpert, Cepheid, Sunnyvale, CA, United States).
In addition, all samples were cultured on C. difficile selective agar (bioMeriéux, Marcyl’Etoile, France). Suspected toxigenic C. difficile colonies were confirmed using immunochromatography (C Diff Quik-Chek Complete assay, TechLab, Blacksburg, VA, United States).
For the detection of SARS-CoV-2, nasopharyngeal swabs in viral transport medium were used. Presence of SARS-CoV-2 RNA was tested by reverse transcriptase PCR. The detected genes were the N gene and Orf1a1b (Thermo Fisher®, Waltham, MA, United States).
Clinical data
Patients’ age and sex (demographic data) were recorded. Regarding clinical data, the Charlson index (11) was used to quantify the degree of comorbidities. Other clinical data collected included antibiotic treatment, proton pump inhibitor use, need of nasogastric tube, mechanical ventilation, surgery, chemotherapy, or radiotherapy in the month prior to CDI diagnosis. Regarding CDI episodes, data on their severity, treatment received, treatment failure, recurrence, mortality, and CDI-related mortality were recorded.
Statistical analysis
Data were analyzed using R (R core Team, 2020, R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria) (12). For qualitative variables, frequencies were calculated, using 95% confidence interval for the proportions (binomial distribution). For quantitative variables, medians and interquartile ranges (IQR) or means and standard deviations (SD) were calculated.
Intergroup differences were determined using the Chi-square test. For continuous variables Student’s t-test or the Mann–Whitney U-test were used when normal distribution of the data could not be assumed. Normal distribution of continuous variables was tested with the Shapiro–Wilk test.
Ethical considerations
This study was approved by the ethics committee of Hospital General Universitario Gregorio Marañón in Madrid (number MICRO.HGUGM.2021-003).
Results
During 2019 there were a total of 47,048 admissions and during 2020 an overall of 42,445 admissions, out of which, 35,662 were non-COVID-19 and 6,763 were COVID-19 admissions to our hospital.
The number of patients with a first episode of HA-CDI was 238, 159 and 68 among the 2019, 2020-non-COVID-19 and COVID-19 patients, respectively. HA-CDI episodes per 10,000 patient days of stay were 6.80, 5.54 and 10.47 for 2019, 2020-non-COVID-19 and COVID-19 cases, respectively (p < 0.001). HO-CDI episodes per 10,000 patient days of stay were 5.06, 4.63 and 8.13 for 2019, 2020-non-COVID-19 and COVID-19 cases, respectively (p < 0.05) (Figure 1 and Table 1).
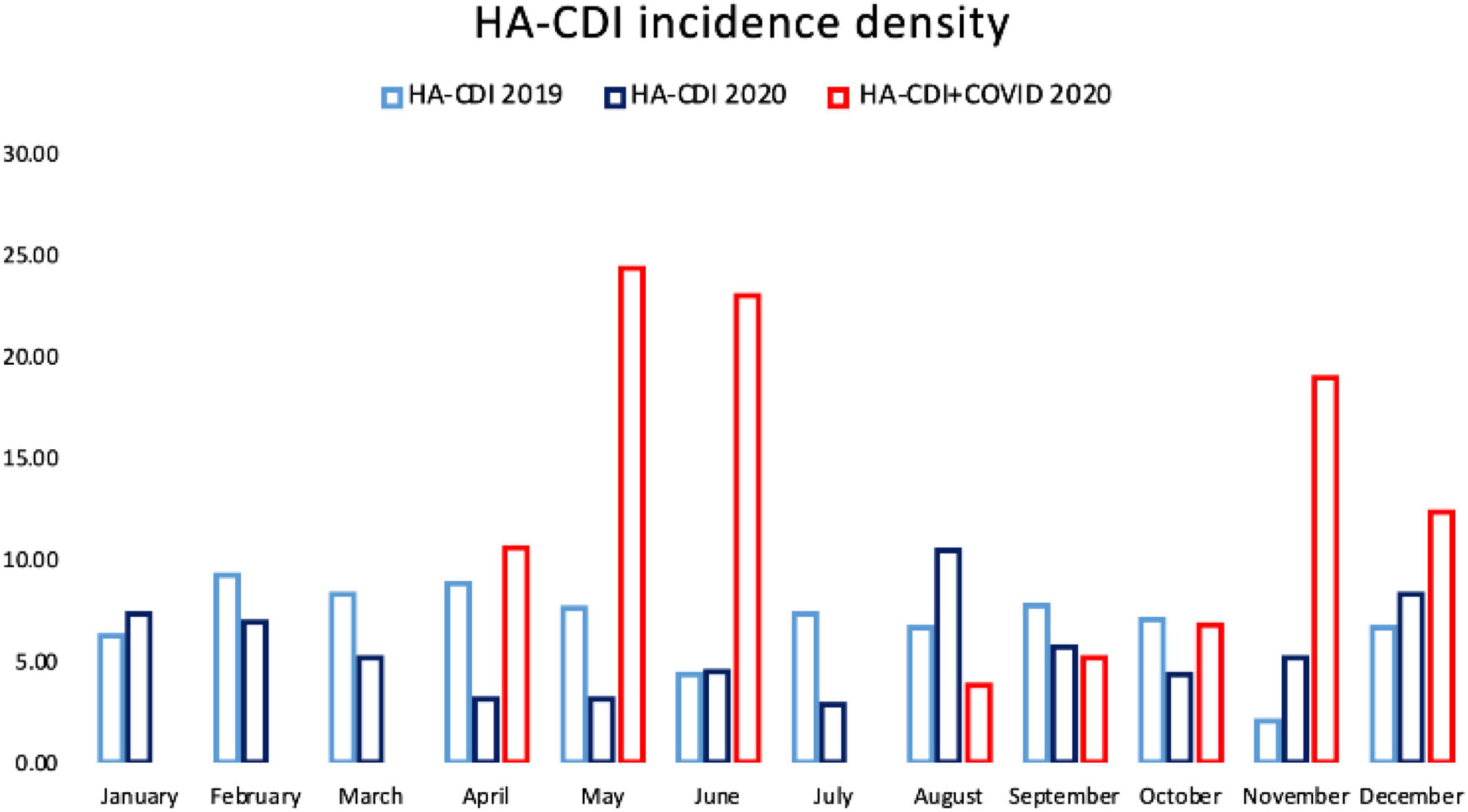
Figure 1. HA-CDI incidence in 2019, in 2020 in non-COVID-19 patients and in 2020 in COVID-19 patients.
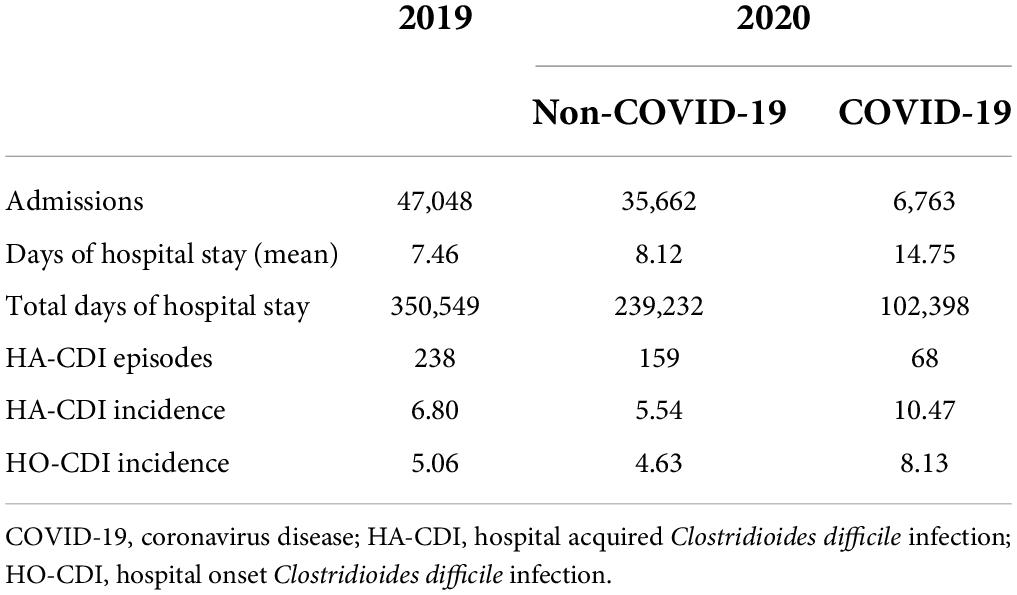
Table 1. Admissions, days of hospital stay, and incidence of hospital acquired Clostridioides difficile infection in the different study groups.
For clinical assessment, we included 138 HA-CDI episodes from 2019, 153 HA-CDI episodes from 2020 without COVID-19 and 68 HA-CDI episodes with COVID-19.
We compared the HA-CDI clinical presentation and evolution between all groups (Tables 2, 3).
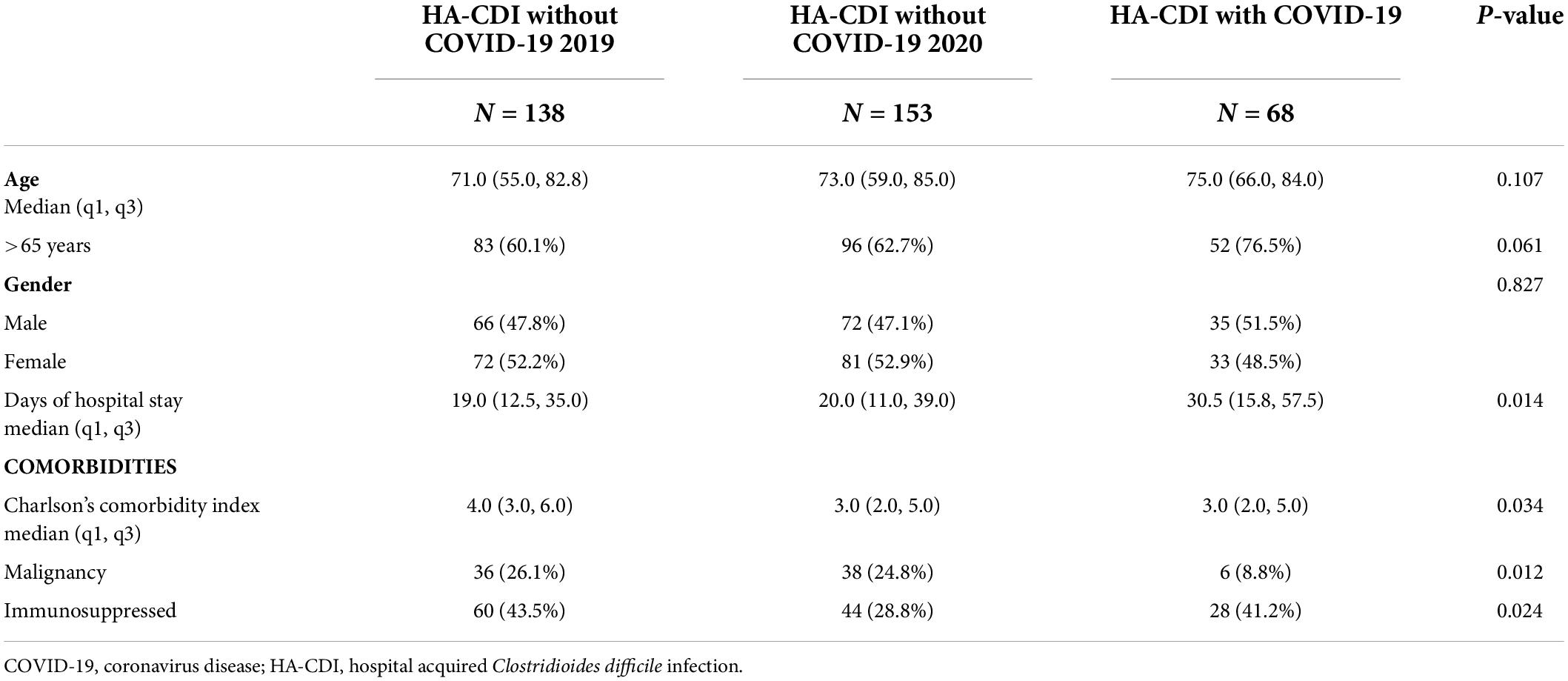
Table 2. Characteristics and clinical data of patients with hospital acquired Clostridioides difficile infection with and without coronavirus disease.
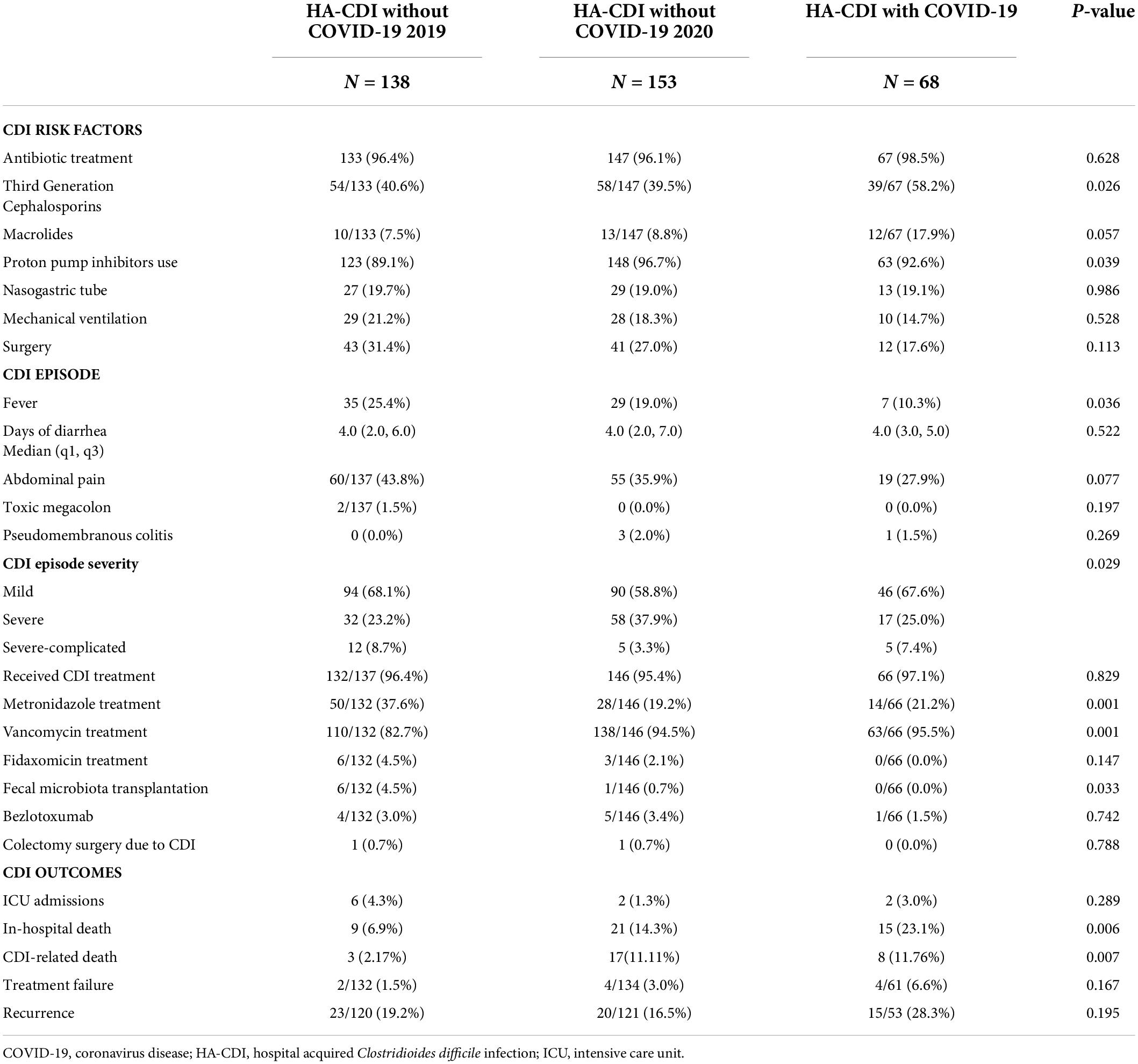
Table 3. Clostridioides difficile risk factors, episode characteristics, and outcomes in coronavirus disease and no coronavirus disease patients.
We found no significant differences between groups for sex and age. The median Charlson comorbidity index at admission was 3.0 (Q1-Q3: 2.0–5.0) in both COVID-19 and non-COVID-19 groups of 2020 and 4.0 (Q1-Q3: 3.0–6.0) in the 2019 group (p = 0.034) (Table 2).
HA-CDI cases with COVID-19 had longer hospital stays and a lower incidence of malignancies (p < 0.05) than those in the other groups. The proportion of immunosuppressed patients prior to admission was lower in the 2020 non-COVID-19 group (p = 0.024).
Concerning to the use of antibiotics in the previous month to the CDI episode, overall, there were no significant differences between all groups (96.4% HA-CDI 2019, 96.1% HA-CDI non-COVID-19 and 98.5% HA-CDI-COVID-19). In both years the number of defined daily doses (DDDs) were not significantly different, from 148,740 DDD per 100 hospital stays (DDD per 100 HS) in 2019 to 143,157 DDD per 100 HS in 2020 (p-value 0.39). However, third generation cephalosporins use was significantly higher in the COVID-19 group than in non-COVID-19 groups (p = 0.026) (Table 3).
Another CDI risk factors such as proton pump inhibitor use in the previous month was higher in the HA-CDI-2020 non-COVID group (96.7%), followed by HA-CDI-COVID group (92.6%) and HA-CDI 2019 group (89.1%) (p = 0.039). No significant differences were found in the presence of other CDI risk factors in the month prior to the CDI episode, such as the use of nasogastric tube, mechanical ventilation or surgery.
No significant differences were seen for days of diarrhea, toxic megacolon, and demonstration of pseudomembranous colitis between study groups. Overall, most of the CDI episodes were mild. CDI episodes were severe in, 23.2%, % of HA-CDI 2019 patients, 37.9%% in HA-CDI-2020 without COVID-19 and 25.0% in HA-CDI COVID-19 patients (p = 0.014).
Regarding CDI treatment, vancomycin was the most prescribed antimicrobial (82.7% HA-CDI 2019, 94.5% HA-CDI non-COVID-19 and 95.5% HA-CDI-COVID-19), followed by metronidazole (37.6% HA-CDI 2019, 19.2% HA-CDI non-COVID-19 and 21.2% HA-CDI-COVID-19). There was an increase in the use of vancomycin in detriment of metronidazole use during 2020 with respect to 2019 (p = 0.001) (Table 3). There were no significant differences in the use of fidaxomicin and bezlotoxumab. As for fecal transplantation, only one procedure was performed during the 2020 pandemic in HA-CDI patients.
Surgical treatment of CDI colonic disease was distinctly uncommon with no difference between the study groups.
Overall, in-hospital death was significantly higher in HA-CDI COVID-19 patients (23.1%) than in HA-CDI 2019 patients (6.9%) and in HA-CDI-2020 without COVID-19 (14.3%) (p = 0.006). When we tried to approach potential HA-CDI causality in the cause of death, we found mortality potentially related to CDI to be higher in 2020 with respect to HA-CDI cases in 2019 (p = 0.007), however there was no significant differences between HA-CDI-2020 without COVID-19 and HA-CDI COVID-19 patients (p = 0.88) (Table 3).
CDI treatment failure was 1.5, 3, and 6.6% of HA-CDI 2019 group, HA-CDI-2020 without COVID-19 and HA-CDI COVID-19, respectively (p = 0.167). Finally, CDI recurrence occurred in 19.2, 16.5, and 28.3% of HA-CDI 2019 group, HA-CDI-2020 without COVID-19 and HA-CDI COVID-19, respectively (p = 0.195) (Table 3).
Discussion
Our results show that in the population of patients with COVID-19, incidence of both HA-CDI and HO-CDI was higher than in non-COVID-19 cases. Regarding clinical characteristics of the CDI episode there were hardly any significant differences in the COVID-19 patients with respect to non-COVID patients, although there was a trend toward higher risk of CDI recurrence in COVID-19 patients.
The COVID-19 pandemic in our hospital started on March 1, 2020. It led to massive care of patients who needed special isolation measures and received more broad-spectrum antibiotics for fear of possible bacterial co-infection as reported by many other institutions (13, 14).
We found a significant increase in the use of third-generation cephalosporins in COVID-19 cases, which are a well-known risk factor for CDI (15). In addition, patients with COVID-19 have been reported to suffer from dysbiosis of the gut microbiota, similar to that caused by antibiotic use, a major risk for CDI infection (16).
Data on the incidence of HA-CDI in COVID-19 patients is still scarce and disparate (5–8, 14, 17–21) several studies describe a lower incidence of CDI during the pandemic (5–8). As summarized by Granata et al., most studies find a lower or equal incidence of CDI in the first phase of the pandemic than in the pre-pandemic period (19). However, in the majority of these studies, the used denominators are the days of hospital stay of the whole population and not only the COVID-19 cases.
There was a CDI incidence in COVID-19 patients in our hospital that falls within the ranges that have been observed in other hospitals (18).
Lewandowski et al. reported an increase in HA-CDI episodes, as in our study. The authors included the population of COVID-19 patients and as denominators the days of hospital stay of the COVID-19 cases (4).
Our comparison of the HA-CDI in non-COVID-19 cases between the 2019 and 2020 episodes indicate that the difference in incidence cannot be attributed to the changes of hospitals’ hygiene control measures. E. Bentivegna et al. reported a decrease of CDI in COVID-19 free units, while in COVID-19 units the incidence of CDI increased (22).
In our opinion, a paradoxical effect in the incidence of HA-CDI does not occur and the increase in the HA-CDI incidence in COVID-19 patients is concordant with the presence in this population of risk factors such as long stay and broad-spectrum antibiotic use.
Our data suggest higher recurrence rate of HA-CDI episodes and CDI treatment failure in COVID-19 patients, which should motivate a less restrictive use of drugs that showed already an ability to reduce recurrences as registered in recent guidelines (10, 23). Regarding CDI disease severity, COVID-19 does not seem to have a profound impact. During the 2020 pandemic, HA-CDI patients without COVID had more frequently severe disease than HA-CDI-2020 with COVID-19, possibly due to the fact that during the pandemic in 2020 only patients with a worse state of health sought care at the hospital.
The attribution of mortality in HA-CDI episodes is complicated; we were unable to demonstrate significant higher HA-CDI-related mortality in COVID-19 cases. Nevertheless, we did find a higher HA-CDI-related mortality in patients in the pandemic period, both with COVID-19 and without COVID-19 compared to HA-CDI patients in 2019.
The main limitation of this study is the single-centre design, but with long-term interest in the topic.
Limiting antimicrobial use in COVID-19 cases, shorter hospital stays, and better prevention are the main stay of HA-CDI prevention.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee of Hospital General Universitario Gregorio Marañón in Madrid. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
SV-C, ER, and EB designed the study and had access and verified the underlying study data. SV-C performed the collection of data and data analysis and wrote the first draft of the manuscript. All authors contributed to data interpretation, contributed with the intellectual content and approved the final draft, and had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Funding
This study was financed by Fondo de Investigaciones Sanitarias (FIS), Research Project numbers PI16/00490 and PI20/01381, and by the European Regional Development Fund (FEDER) “A way of making Europe.”
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Firew T, Sano ED, Lee JW, Flores S, Lang K, Salman K, et al. Protecting the front line: a cross-sectional survey analysis of the occupational factors contributing to healthcare workers’ infection and psychological distress during the COVID-19 pandemic in the USA. BMJ Open. (2020) 10:e042752. doi: 10.1136/bmjopen-2020-042752
2. Kang L, Li Y, Hu S, Chen M, Yang C, Yang BX, et al. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. Lancet Psychiatry. (2020) 7:e14. doi: 10.1016/S2215-0366(20)30047-X
3. Spigaglia P. Covid-19 and Clostridioides difficile infection (CDI): possible implications for elderly patients. Anaerobe. (2020) 64:102233. doi: 10.1016/j.anaerobe.2020.102233
4. Lewandowski K, Rosołowski M, Kaniewska M, Kucha P, Meler A, Wierzba W, et al. Clostridioides difficile infection in Coronavirus disease 2019 (Covid-19): an underestimated problem? Pol Arch Intern Med. (2021) 131:121–7. doi: 10.20452/pamw.15715
5. Ponce-Alonso M, Sáez de la Fuente J, Rincón-Carlavilla A, Moreno-Nunez P, Martínez-García L, Escudero-Sánchez R, et al. Impact of the coronavirus disease 2019 (Covid-19) pandemic on nosocomial Clostridioides difficile infection. Infect Control Hosp Epidemiol. (2020) 42:406–10. doi: 10.1017/ice.2020.454
6. Laszkowska M, Kim J, Faye AS, Joelson AM, Ingram M, Truong H, et al. Prevalence of Clostridioides difficile and other gastrointestinal pathogens in patients with Covid-19. Dig Dis Sci. (2021) 66:4398–405. doi: 10.1007/s10620-020-06760-y
7. Hazel K, Skally M, Glynn E, Foley M, Burns K, O’Toole A, et al. The other ‘C’: hospital-acquired. Infect Control Hosp Epidemiol. (2021) 43:540–1. doi: 10.1017/ice.2021.3
8. Ochoa-Hein E, Rajme-López S, Rodríguez-Aldama JC, Huertas-Jiménez MA, Chávez-Ríos AR, de Paz-García R, et al. Substantial reduction of healthcare facility-onset Clostridioides difficile infection (HO-CDI) rates after conversion of a hospital for exclusive treatment of Covid-19 patients. Am J Infect Control. (2020) 49:966–8. doi: 10.1016/j.ajic.2020.12.008
9. McDonald LC, Gerding DN, Johnson S, Bakken JS, Carroll KC, Coffin SE, et al. Clinical practice guidelines for clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society Of America (IDSA) and Society For Healthcare Epidemiology Of America (SHEA). Clin Infect Dis. (2018) 66:987–94. doi: 10.1093/cid/ciy149
10. van Prehn J, Reigadas E, Vogelzang EH, Bouza E, Hristea A, Guery B, et al. European society of clinical microbiology and infectious diseases: 2021 update on the treatment guidance document for Clostridioides difficile infection in adults. Clin Microbiol Infect. (2021) 27:S1–21. doi: 10.1016/j.cmi.2021.09.038
11. Charlson ME, Pompei P, Ales KL, MacKenzie CRA. New method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. (1987) 40:373–83. doi: 10.1016/0021-9681(87)90171-8
12. R core Team. R: A Language And Environment For Statistical Computing. Vienna: R core Team (2020).
13. Mirzaei R, Goodarzi P, Asadi M, Soltani A, Aljanabi HAA, Jeda AS, et al. Bacterial co-infections with Sars-Cov-2. IUBMB Life. (2020) 72:2097–111. doi: 10.1002/iub.2356
14. Manea E, Jipa R, Milea A, Roman A, Neagu G, Hristea A. Healthcare-associated Clostridioides difficile infection during the Covid-19 pandemic in a tertiary care hospital in Romania. Rom J Intern Med. (2021) 59:409–15. doi: 10.2478/rjim-2021-0020
15. de Lalla F, Privitera G, Ortisi G, Rizzardini G, Santoro D, Pagano A, et al. Third generation cephalosporins as a risk factor for Clostridium difficile-associated disease: a four-year survey in a general hospital. J Antimicrob Chemother. (1989) 23:623–31. doi: 10.1093/jac/23.4.623
16. Zuo T, Zhang F, Lui GCY, Yeoh YK, Li AYL, Zhan H, et al. Alterations in gut microbiota of patients with Covid-19 during time of hospitalization. Gastroenterology. (2020) 159:944–55.e8. doi: 10.1053/j.gastro.2020.05.048
17. Allegretti JR, Nije C, McClure E, Redd WD, Wong D, Zhou JC, et al. Prevalence and impact of Clostridioides difficile infection among hospitalized patients with Coranavirus disease 2019. JGH Open. (2021) 5:622–5. doi: 10.1002/jgh3.12497
18. Granata G, Bartoloni A, Codeluppi M, Contadini I, Cristini F, Fantoni M, et al. The burden of Clostridioides difficile infection during the Covid-19 pandemic: a retrospective case-control study in Italian hospitals (CloVid). J Clin Med. (2020) 9:3855. doi: 10.3390/jcm9123855
19. Granata G, Petrosillo N, Al Moghazi S, Caraffa E, Puro V, Tillotson G, et al. The burden of Clostridioides difficile infection in covid-19 patients: a systematic review and meta-analysis. Anaerobe. (2022) 74:102484. doi: 10.1016/j.anaerobe.2021.102484
20. Luo Y, Grinspan LT, Fu Y, Adams-Sommer V, Willey DK, Patel G, et al. Hospital-Onset Clostridioides difficile infections during the Covid-19 pandemic. Infect Control Hosp Epidemiol. (2020) 42:1165–6. doi: 10.1017/ice.2020.1223
21. Hawes AM, Desai A, Patel PK. Did Clostridioides difficile testing and infection rates change during the Covid-19 pandemic? Anaerobe. (2021) 70:102384. doi: 10.1016/j.anaerobe.2021.102384
22. Bentivegna E, Alessio G, Spuntarelli V, Luciani M, Santino I, Simmaco M, et al. Impact of Covid-19 prevention measures on risk of health care-associated Clostridium difficile infection. Am J Infect Control. (2020) 49:640–2. doi: 10.1016/j.ajic.2020.09.010
23. Bouza E, Aguado JM, Alcalá L, Almirante B, Alonso-Fernández P, Borges M, et al. Recommendations for the diagnosis and treatment of Clostridioides Difficile infection: an official clinical practice guideline of the Spanish society of chemotherapy (SEQ), Spanish society of internal medicine (SEMI) and the working group of postoperative infection of the Spanish society of anesthesia and reanimation (SEDAR). Rev Esp Quimioter. (2020) 33:151–75. doi: 10.37201/req/2065.2020
Keywords: CDI, COVID-19, SARS-CoV-2, C. difficile, nosocomial infection, hospital-acquired
Citation: Vázquez-Cuesta S, Olmedo M, Reigadas E, Alcalá L, Marín M, Muñoz P and Bouza E (2022) Clostridioides difficile infection epidemiology and clinical characteristics in COVID-19 pandemic. Front. Med. 9:953724. doi: 10.3389/fmed.2022.953724
Received: 26 May 2022; Accepted: 01 August 2022;
Published: 22 August 2022.
Edited by:
Frédéric Barbut, AP-HP, FranceReviewed by:
Stefano Bibbò, Università Cattolica del Sacro Cuore, ItalyGuido Granata, National Institute for Infectious Diseases Lazzaro Spallanzani (IRCCS), Italy
Copyright © 2022 Vázquez-Cuesta, Olmedo, Reigadas, Alcalá, Marín, Muñoz and Bouza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elena Reigadas, aGVsZW5yZWlAaG90bWFpbC5jb20=