 Ioannis Parodis
Ioannis Parodis Mariele Gatto
Mariele Gatto Christopher Sjöwall
Christopher Sjöwall- 1Division of Rheumatology, Department of Medicine Solna, Karolinska Institutet and Karolinska University Hospital, Stockholm, Sweden
- 2Department of Rheumatology, Faculty of Medicine and Health, Örebro University, Örebro, Sweden
- 3Unit of Rheumatology, Department of Medicine, University of Padua, Padua, Italy
- 4Division of Inflammation and Infection, Department of Biomedical and Clinical Sciences, Linköping University, Linköping, Sweden
B cell hyperactivity is a hallmark of the complex autoimmune disease systemic lupus erythematosus (SLE), which has justified drug development focusing on B cell altering agents during the last decades, as well as the off-label use of B cell targeting biologics. About a decade ago, the anti-B cell activating factor (BAFF) belimumab was the first biological agent to be licensed for the treatment of adult patients with active yet non-renal and non-neuropsychiatric SLE, to later be expanded to include treatment of pediatric SLE and, recently, lupus nephritis. B cell depletion is recommended as an off-label option in refractory cases, with the anti-CD20 rituximab having been the most used B cell depleting agent to date while agents with a slightly different binding specificity to CD20 such as obinutuzumab have also shown promise, forming a part of the current pipeline. In addition, terminally differentiated B cells have also been the targets of experimental therapies, with the proteasome inhibitor bortezomib being one example. Apart from being promising drug targets, B and plasma cells have also shown promise in the surveillance of patients with SLE, especially for monitoring B cell depleting or B cell altering therapies. Inadequate B cell depletion may signify poor expected clinical response to rituximab, for example, while prominent reductions in certain B cell subsets may signify a protection against flare development in patients treated with belimumab. Toward an era with a richer therapeutic armamentarium in SLE, including to a large extent B cell altering treatments, the challenge that emerges is to determine diagnostic means for evidence-based therapeutic decision-making, that uses clinical information, serological markers, and gene expression patterns to guide individualized precision strategies.
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune inflammatory disease that is characterized by a multiple organ involvement and a prominent heterogeneity of clinical symptoms and disease severity (1). While the treatment of SLE has been non-targeted for many years, mainly comprising antimalarial agents (2), glucocorticoids, and broad immunosuppressants that hamper inflammation in a non-specific manner (3), more selective therapeutic modalities have been used for SLE during the last decades (4), including B cell targeting therapies (5).
Belimumab, a monoclonal antibody that binds to the soluble form of the B cell activating factor belonging to the tumor necrosis family (BAFF; also known as B lymphocyte stimulator, BLyS), was approved for the treatment of SLE in 2011 after two successful phase III clinical trials (6, 7); it was the first in history biological agent to be approved for SLE (8), lending credence to the notion that B cells are central in the pathogenesis of SLE (9). Rituximab, an anti-CD20 B cell depleting monoclonal antibody has been used as an off-label therapeutic option since even earlier (10, 11), and is still used in difficult to treat or refractory cases despite serial failures of clinical trials to show added value on top of standard therapy (3). In this review, we summarize evidence for B cell and plasma cell targeting therapies in SLE, and advocate for the use of B cells as important tools not only as treatment targets, but also disease surveillance.
Loss of self-tolerance is a distinctive feature in SLE pathogenesis, leading up to immune responses toward endogenous nuclear and cytoplasmic components. Terminally differentiated antibody-secreting B cells i.e., plasmablast and long-lived plasma cell clones constitute the main producers of autoantibodies against such endogenous antigens, contributing to tissue injury and maintenance of the inflammatory milieu through immune complex formation and induction of type I interferon-mediated proinflammatory cytokine production. Autoantibodies such as anti-double stranded DNA (anti-dsDNA) and anti-Smith (Sm) antibodies are considered fairly specific for SLE and are associated with clinical disease features (12), while circulating anti-dsDNA levels oftentimes follow SLE disease activity (13, 14). Importantly, autoantibody production is not the only mechanism through which B cells contribute to SLE pathogenesis, as evidenced in murine lupus models where B cells that did not secrete autoantibodies still were important for disease progression (15); thus, the constantly hyperactive B cell lineages in SLE are also important for antigen presentation to T cells and cytokine secretion (16), or expression of toll-like receptors (TLRs) (17).
To characterize B cells, surface markers are used, such as CD19, CD20, and CD22, expressed at different stages of B cell maturation. B cell responses in SLE are currently hampered by two main means i.e., (i) BAFF inhibition through belimumab, and (ii) B cell depletion through anti-CD20 agents, such as rituximab, obinutuzumab, and ofatumumab. BAFF is a member of the tumor necrosis factor ligand superfamily and is mainly produced by myeloid and stromal cells (18). BAFF contributes to B cell survival, proliferation, and antibody production, through binding to three receptors expressed on the surface of B cells at different maturation stages i.e., the BAFF-Receptor (BAFF-R; also known as BLyS receptor 3, BR3), transmembrane activator and calcium modulator and cyclophilin ligand interactor (TACI), and B cell maturation antigen (BCMA) (19). Notably, BAFF levels have been demonstrated to be elevated in patients with SLE compared with healthy controls and show correlates with disease activity (20–23). Apart from BAFF, B cell stimulation is also induced by cytokines such as type I interferons, interleukin (IL)-6, IL-21, as well as a proliferation-inducing ligand (APRIL), the latter mainly contributing to plasma cell survival (24, 25).
Targeting B cells to treat SLE
Early uncontrolled studies of the chimeric anti-CD20 monoclonal antibody rituximab in SLE showed promise, but two phase III randomized controlled trials (RCTs), the EXPLORER trial in non-renal SLE (26) and the LUNAR trial in lupus nephritis (27), failed to meet their primary endpoints (28). This notwithstanding, rituximab has been used off-label for the treatment of cases of SLE and lupus nephritis that have not been responsive to standard therapy (3, 29, 30). While lupus nephritis, a potentially life-threatening condition (31), has been the most common SLE manifestation managed with rituximab in several centers, rituximab has also been used to treat severe polyarthritis, hematological SLE disease, especially severe haemolytic anemia or autoimmune thrombocytopenia, and neuropsychiatric SLE (32–37). However, it is worth noting that rituximab use has also raised concerns regarding adverse events, such as infusion-related reactions (38–40), late-onset neutropenia (41), and hypogammaglobulinaemia (42, 43).
In addition to rituximab, the humanized anti-CD20 monoclonal antibody ocrelizumab was evaluated in a phase III trial of severe lupus nephritis, which however was terminated due to serious infections (44); for this reason, ocrelizumab was not studied further in the context of SLE. The humanized anti-CD20 monoclonal antibody obinutuzumab has a different binding specificity to the CD20 molecule, resulting in superior cytotoxic effects for B cells over rituximab (45); obinutuzumab was studied in a phase II trial of lupus nephritis and showed ability to induce complete renal response (46). The prospect of obinutuzumab for the treatment of lupus nephritis is currently tested in a phase III clinical trial (NCT04221477). Ofatumumab is a fully human anti-CD20 monoclonal antibody that is approved for the treatment of chronic lymphocytic leukemia (47) and has shown promise in small studies of SLE, mainly used to treat lupus nephritis, immune-mediated thrombocytopenia, and autoimmune haemolytic anemia (48–51). Obinutuzumab and ofatumumab are considered viable options for patients in whom rituximab was effective but adverse events, namely infusion reactions, resulted in discontinuation (49), or for patients in whom rituximab did not induce complete B cell depletion (39).
Lastly, the humanized monoclonal antibody epratuzumab is directed against CD22, and while it showed promising results regarding both tolerability and efficacy in a phase IIb trial (52, 53), two subsequent phase III trials failed to prove efficacy (54).
Targeting plasma cells
While most B cell targeting drugs currently used in SLE mainly exert their effects on B cells of early maturation stages, plasmablasts, and short-lived plasma cells (55), proteasome inhibition affects long-lived plasma cells and has been used in severe therapy-resistant SLE cases (56–60). Proteasome inhibition results in accumulation of defective immunoglobulin chains, endoplasmic reticulum stress, misfolded proteins, and ultimately plasma cell apoptosis (61, 62). Being large-scale antibody producers, long-lived plasma cells are highly sensitive to proteasome inhibition (58). In addition, proteasome inhibitors also hamper the production of pro-inflammatory cytokines through regulation of NF-κB signaling (63).
Bortezomib, a dipeptide containing a boron atom that exerts its effects on plasma cells by binding with high affinity and specificity the catalytic site of the 26S proteasome, is approved for the treatment of mantle cell lymphoma and multiple myeloma (64). The prospect of bortezomib in SLE (65) gained promise after experiments in murine lupus, and reports of bortezomib use to treat allograft rejection after kidney transplantation (66, 67). In a recent nationwide study from Sweden, the current clinical experience based on 12 patients who received bortezomib for refractory SLE was reported (68). The therapeutic effects of bortezomib combined with glucocorticoids were beneficial in a majority of the patients with severe and life-threatening SLE manifestations that had been irresponsive to conventional immunosuppressive agents; these effects included alleviation of proteinuria levels and complement consumption, as well as seroconversion from positive to negative anti-dsDNA antibody status (68). Safety signals that emerged in this study mainly comprised the potential risk for infections and hypogammaglobulinemia (68).
On the other hand, concerns may argue that sole bortezomib treatment might not be as sufficient in autoimmune conditions as in non-autoimmune hematological diseases, due to a rapid bone marrow repopulation with short-lived plasma cells and subsequent rise in autoantibody levels that occur upon bortezomib withdrawal, which is likely attributable to the limited effects of bortezomib on bone marrow B and T cell precursors (62). Additionally, the only randomized trial that employed bortezomib in SLE did not demonstrate superiority of bortezomib over placebo in clinical or serological efficacy (69). Nevertheless, careful interpretation of these results should be entailed due to the limited number of patients enrolled and the choice of endpoints. In fact, proteasome inhibition in SLE might be an option in severe, refractory cases (68), and might require additional subsequent B cell depleting modalities to ensure long-term efficacy. In this regard, plasma cells may also by targeted through blockade of CD38. Daratumumab is a monoclonal antibody against CD38 approved for multiple myeloma, which has been successfully used in patients with refractory SLE who previously had received bortezomib (70), lending merit for targeting terminally differentiated B cells in recalcitrant forms of SLE using one or multiple agents.
Targeting B cell-related cytokines
BAFF has been a central target molecule in drug development for SLE, due to is key roles in B cell homeostasis. Targeting BAFF has been proven a successful therapeutic strategy with the approval of the anti-BAFF monoclonal antibody belimumab, formerly also known as Lympho-Stat B, after two successful phase III RCTs (6, 7). In different studies, patients with low B cell counts, high BAFF levels, serologically active disease, limited or no established organ damage, and no exposure to cigarette smoking have been shown to be more benefited from belimumab therapy (71–80). Safety signals reported during belimumab therapy mostly concern infusion reactions and mild infectious events (6, 7, 72, 81), and some caution was raised during the early post-market phase about the risk of psychiatric disorders (82), but the drug has shown an excellent overall safety profile, also over a longer term (83).
Another BAFF-inhibiting agent is atacicept, a receptor construct that combines TACI with the Fc fraction of human IgG, thus inhibiting both BAFF and APRIL (84). Atacicept was evaluated in a clinical trial of lupus nephritis, which was terminated prematurely due to adverse events such as hypogammaglobulinemia and infections (85); however, the development of atacicept for the treatment of SLE has not been fully abandoned.
The fusion protein blisibimod consists of four high-affinity BAFF-binding domains and the Fc domain of human IgG1; in contrast to belimumab that only binds to the soluble counterpart of BAFF, blisibimod targets both soluble and membrane-bound BAFF. Following a promising dose-ranging phase IIb clinical trial of SLE that determined a safe and effective dose (86), a subsequent phase III clinical trial failed unfortunately to prove efficacy (87).
Tabalumab is a fully human monoclonal antibody that also targets both soluble and membrane-bound BAFF. Two phase III clinical trials of tabalumab in SLE have been completed, of which only one met its primary endpoint (88, 89), being the reason why its development for SLE was stopped. However, it is worth noting that key secondary endpoints were met in both trials, justifying the rationale of targeting both the cleaved and membrane-bound BAFF molecule (90, 91).
Anifrolumab is a recently developed monoclonal antibody against the type I interferon (IFN) receptor (IFNAR), hence with inhibitory capability on the type I IFN pathway. While type I IFNs are mainly produced by plasmacytoid dendritic cells (pDCs) and resident cells in target tissues (92), B cells are highly sensitive to the IFN pleiotropic action and are prompted to differentiation and activation upon IFN-mediated signaling (24). The successful phase IIb trial of anifrolumab in patients with moderate or severe SLE (93) put the grounds for the conception of patient stratification based on endotypic features, e.g., the magnitude of the IFN signature, and in contrast to the failure of the first phase III trial of anifrolumab in SLE (TULIP1) (94), the drug was successful in the subsequent phase III trial TULIP2 (95). Based on an overall evaluation of the primary and key secondary endpoints of the TULIP trials, anifrolumab received approval by regulatory authorities for use in SLE. Additionally, a phase II trial of anifrolumab in active lupus nephritis showed initial promise (96) and prompted an ongoing phase III trial. Safety signals reported for anifrolumab therapy mostly concern reactivation of opportunistic infections, particularly by varicella zoster virus (VZV), due to the IFN blockade, especially in patients with kidney involvement (97).
While the therapeutic armamentarium for SLE has been enriched with new therapeutic modalities that directly or indirectly target B cells of diverse maturation stages, the identification of the best patient candidates for the different treatments remains lacunose. Clinical features and traditional serological markers (71–80), as well as particular immunological signatures (94, 95), have been introduced as potential predictors of therapeutic responses, representing important steps toward more informed decision-making processes, yet optimisation is still limited by major knowledge gaps regarding in-depth characterization of underlying mechanisms, and the impact those mechanisms have on the individual patient.
Combination therapies to target B cells
The observed rise in BAFF levels upon treatment with rituximab (98) has been speculated to be one of the reasons why clinical trials of rituximab in SLE have failed, providing grounds to the rationale for combining rituximab with belimumab to achieve better B cell responses (23, 98–100). This approach has recently been evaluated in patients with SLE within the frame of e.g., the BEAT Lupus (101, 102) and BLISS-BELIEVE (103) trials. The latter, however, failed to show superior disease control with the addition of a single cycle of rituximab on top of belimumab treatment over that achieved by belimumab treatment alone, while more serious infections were seen in the combination group (104). Furthermore, the concept of combining B cell therapies has also been studied in the context of lupus nephritis, e.g., in the Rituximab and Belimumab for Lupus Nephritis (CALIBRATE; NCT02260934) (105) and Synergetic B cell Immunomodulation in SLE (SynBioSe) trials (SynBioSe 1: NCT02284984 (106); SynBioSe 2: NCT03747159). While the CALIBRATE study failed to reach its primary endpoint i.e., achievement of renal response at week 48, biological effects in the form of decreased anti-dsDNA antibody levels and modification of the B cell pool composition favored the addition of belimumab to a therapeutic regimen comprising rituximab and cyclophosphamide. Importantly, no safety signals emerged for this combination.
A summary of recent or ongoing trials of agents that directly or indirectly alter the B cell constitution in patients with SLE and lupus nephritis is presented in Table 1. Figure 1 illustrates the main mode of action of compounds discussed in the present review.
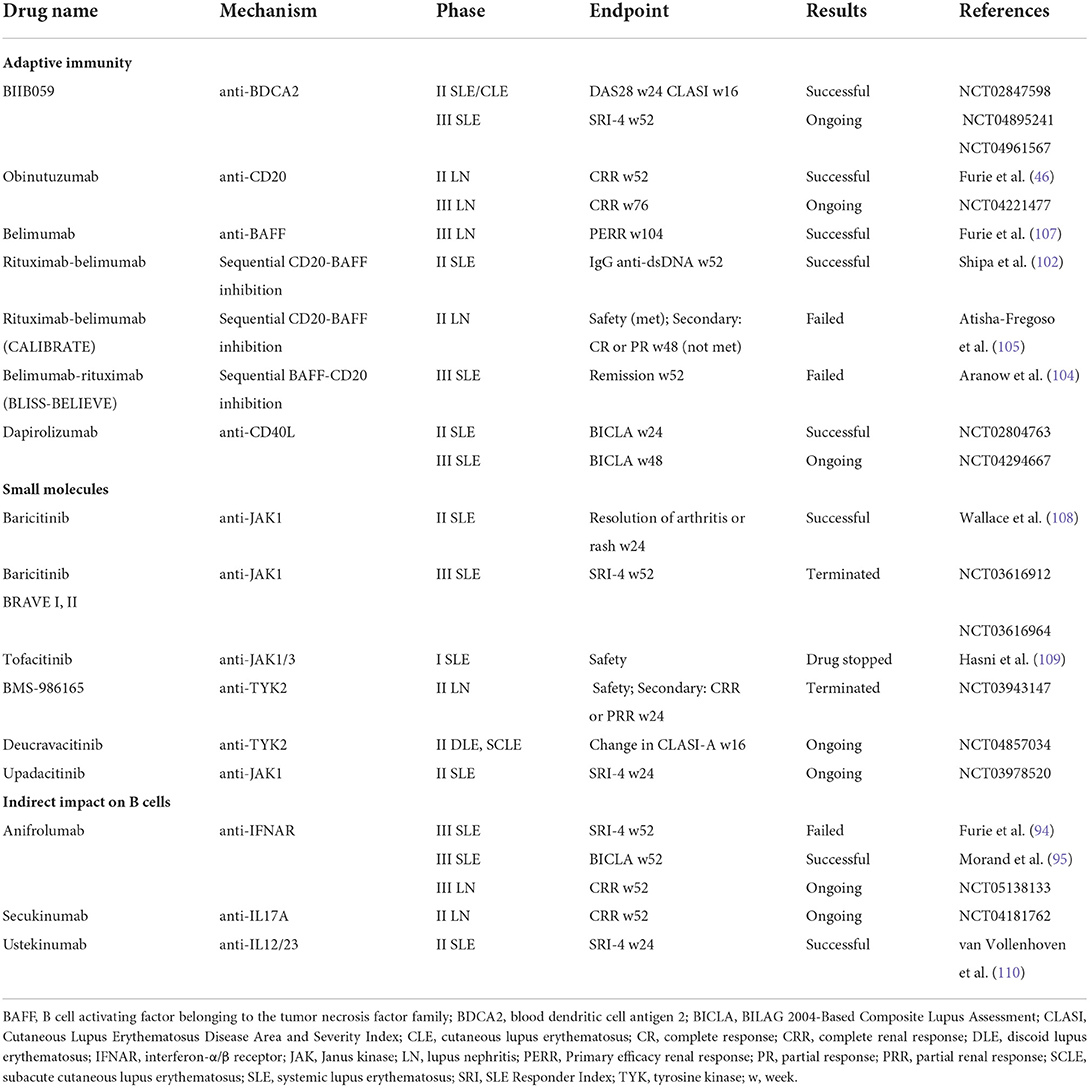
Table 1. Selected drugs studied for SLE and LN that exert direct or indirect effects on B cells.
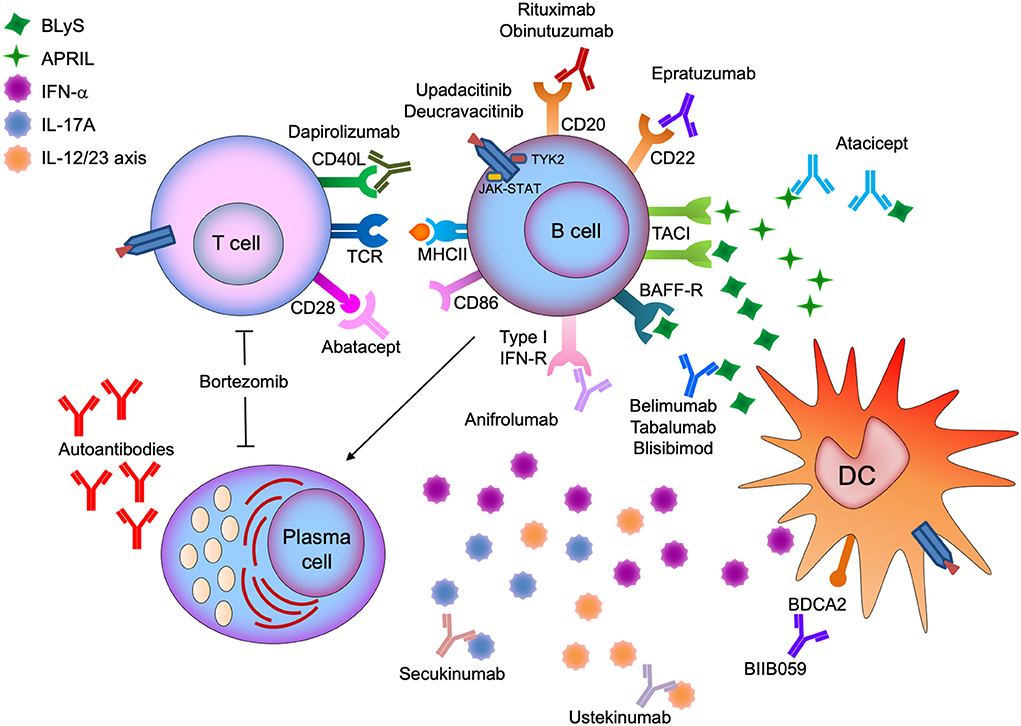
Figure 1. Illustration of the main mode of action of compounds studied for the treatment of systemic lupus erythematosus (SLE) and lupus nephritis (LN) that exert direct or indirect effects on B cells.
The prospect of B cells as surveillance tools
Changes in the circulating B cell pool are expected upon B cell targeting therapies and have been described in response to anti-CD20 (22, 39, 111) and anti-BAFF (74, 112, 113) therapies. On the other hand, little data has piled up so far concerning the potential role of B cell changes as measurable biomarkers of response to therapy or as heralders of disease flares.
Recently, we analyzed data from three phase III RCTs of belimumab i.e., BLISS-76 (NCT00410384) (7), BLISS-SC (NCT01484496) (114), and BLISS Northeast Asia (NEA; NCT01345253) (115) and pinpointed specific relative to baseline percentage changes across different circulating CD19+ B cell and plasma cell subsets occurring in SLE patients after treatment commencement for active disease with standard therapy with or without add-on belimumab to be associated with treatment response (116) or disease flares (117). Within a pooled cohort of 1712 patients with SLE, treatment responders showed more prominent decreases from baseline through week 52 in CD19+CD20+CD27− naïve B cells, CD19+CD20−CD27bright plasmablasts, and CD19+CD20−CD138+ long-lived plasma cells, and a more prominent rapid (through week 8) and early (through week 24) expansion of CD19+CD20+CD27+ memory B cells compared with non-responders (116). Conversely, patients who developed severe flares showed less prominent early decreases in CD19+CD20−CD138+ long-lived plasma cells and CD19+CD27brightCD38bright SLE-associated plasma cells (117).
In an analysis of B cell changes in relation to renal flare development within the same SLE population from trials of belimumab (unpublished data), patients who developed renal flares showed a more prominent rapid decrease in CD19+CD20+CD138+ short-lived plasma cells and CD19+CD20−CD27bright plasmablasts compared with patients who did not flare, followed by a subsequent return. Remarkably, more prominent rapid reductions in CD19+CD27−CD24brightCD38bright transitional B cells and CD19+CD20−CD138+ peripheral long-lived plasma cells were associated with a protection against renal flares in belimumab-treated patients.
It is worth noting that B cell changes in these analyses were mainly related to treatment effectiveness rather than the mechanism of the drug employed. However, considering its mode of action, belimumab is expected to impact on B cells of early maturation stages, as shown previously (74, 112, 113, 118), and decreasing B cell counts may be expected to predict favorable responses to belimumab, as previously demonstrated for rituximab in patients achieving adequate B cell depletion (22, 39). Moreover, in a real-life observational study, immunological responses to belimumab preceded overt clinical improvements (74). Thus, since changes in circulating B cell subsets may be expected to occur shortly upon therapy commencement, such changes could prove a useful tool in the treatment and disease monitoring in patients with SLE, complemental to traditional serological biomarkers such as anti-dsDNA and complement levels, which may be less sensitive to change. Lastly, the use of relevant molecules in the prediction of response to therapies is expected to advance treatment selection and monitoring in the future. High BAFF levels, for instance, have been associated with favorable clinical response to treatment with belimumab (72), but also imminent flare in patients with SLE on non-biological standard therapy (119).
Concluding remarks
SLE is characterized by breach of self-tolerance and constant B cell hyperactivity. While the contribution of B cells to disease initiation is unclear, they have key roles in the pathogenesis of established SLE and the maintenance of the chronic inflammatory milieu. Several B cell targeting therapeutic modalities have an established role in the SLE treatment armamentarium, while other are in the pipeline. Optimized use of B cell altering therapeutic approaches would require effective identification of patients who would be more likely to benefit from B cell therapies based on their clinical and immunological phenotypes. In this regard, the usefulness of B cell and plasma cell levels and alterations as markers of treatment response or flare development has not been thoroughly explored, but recent data show merit and ratify further survey.
Author contributions
All authors contributed to the manuscript draft, critically reviewed all parts of the manuscript, accepted its final version prior to submission, and account for its content.
Funding
IP was funded by grants from the Swedish Rheumatism Association (R-941095), King Gustaf V's 80-year Foundation (FAI-2020-0741), Professor Nanna Svartz Foundation (2020-00368), Ulla and Roland Gustafsson Foundation (2021-26), Region Stockholm (FoUI-955483) and Karolinska Institutet. CS was funded by the Swedish Rheumatism Association (R-939149), Region Östergötland (ALF grants; RÖ-960604), King Gustaf V's 80-year Anniversary foundation (FAI-2020-0663), and King Gustaf V and Queen Victoria's Freemasons foundation. The funders had no role in the design of the study, the analyses or interpretation of data, or the writing of the manuscript.
Acknowledgments
The authors would like to thank GlaxoSmithKline for providing data from the BLISS-76 (NCT00410384), BLISS-SC (NCT01484496), and BLISS-NEA (NCT01345253) trials through the CSDR consortium.
Conflict of interest
Author IP has received research funding and/or honoraria from Amgen, AstraZeneca, Aurinia Pharmaceuticals, Elli Lilly and Company, Gilead Sciences, GlaxoSmithKline, Janssen Pharmaceuticals, Novartis, and F. Hoffmann-La Roche AG.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kaul A, Gordon C, Crow MK, Touma Z, Urowitz MB, van Vollenhoven R, et al. Systemic lupus erythematosus. Nat Rev Dis Primers. (2016) 2:16039. doi: 10.1038/nrdp.2016.39
2. Ruiz-Irastorza G, Ramos-Casals M, Brito-Zeron P, Khamashta MA. Clinical efficacy and side effects of antimalarials in systemic lupus erythematosus: a systematic review. Ann Rheum Dis. (2010) 69:20–8. doi: 10.1136/ard.2008.101766
3. Fanouriakis A, Kostopoulou M, Alunno A, Aringer M, Bajema I, Boletis JN, et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheum Dis. (2019) 78:736–45. doi: 10.1136/annrheumdis-2019-215089
4. Gatto M, Zen M, Iaccarino L, Doria A. New therapeutic strategies in systemic lupus erythematosus management. Nat Rev Rheumatol. (2019) 15:30–48. doi: 10.1038/s41584-018-0133-2
5. Parodis I, Stockfelt M, Sjowall C. B cell therapy in systemic lupus erythematosus: from rationale to clinical practice. Front Med (Lausanne). (2020) 7:316. doi: 10.3389/fmed.2020.00316
6. Navarra SV, Guzman RM, Gallacher AE, Hall S, Levy RA, Jimenez RE, et al. Efficacy and safety of belimumab in patients with active systemic lupus erythematosus: a randomised, placebo-controlled, phase 3 trial. Lancet. (2011) 377:721–31. doi: 10.1016/S0140-6736(10)61354-2
7. Furie R, Petri M, Zamani O, Cervera R, Wallace DJ, Tegzova D, et al. A phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus. Arthritis Rheum. (2011) 63:3918–30. doi: 10.1002/art.30613
8. Parodis I, Axelsson M, Gunnarsson I. Belimumab for systemic lupus erythematosus: a practice-based view. Lupus. (2013) 22:372–80. doi: 10.1177/0961203313476154
9. Harvey PR, Gordon C. B-cell targeted therapies in systemic lupus erythematosus: successes and challenges. BioDrugs. (2013) 27:85–95. doi: 10.1007/s40259-013-0015-8
10. Leandro MJ, Edwards JC, Cambridge G, Ehrenstein MR, Isenberg DA. An open study of B lymphocyte depletion in systemic lupus erythematosus. Arthritis Rheum. (2002) 46:2673–7. doi: 10.1002/art.10541
11. Gunnarsson I, Sundelin B, Jonsdottir T, Jacobson SH, Henriksson EW, van Vollenhoven RF. Histopathologic and clinical outcome of rituximab treatment in patients with cyclophosphamide-resistant proliferative lupus nephritis. Arthritis Rheum. (2007) 56:1263–72. doi: 10.1002/art.22505
12. Swaak AJ, Huysen V, Nossent JC, Smeenk RJ. Antinuclear antibody profiles in relation to specific disease manifestations of systemic lupus erythematosus. Clin Rheumatol. (1990) 9:82–94. doi: 10.1007/BF02205555
13. Enocsson H, Sjöwall C, Wirestam L, Dahle C, Kastbom A, Rönnelid J, et al. Four anti-dsdna antibody assays in relation to systemic lupus erythematosus disease specificity and activity. J Rheumatol. (2015) 42:817–25. doi: 10.3899/jrheum.140677
14. Frodlund M, Wetterö J, Dahle C, Dahlström Ö, Skogh T, Rönnelid J, et al. Longitudinal anti-nuclear antibody (ANA) seroconversion in systemic lupus erythematosus: a prospective study of Swedish cases with recent-onset disease. Clin Exp Immunol. (2020) 199:245–54. doi: 10.1111/cei.13402
15. Chan OT, Hannum LG, Haberman AM, Madaio MP, Shlomchik MJ. A novel mouse with B cells but lacking serum antibody reveals an antibody-independent role for B cells in murine lupus. J Exp Med. (1999) 189:1639–48. doi: 10.1084/jem.189.10.1639
16. Suzuki N, Sakane T. Induction of excessive B cell proliferation and differentiation by an in vitro stimulus in culture in human systemic lupus erythematosus. J Clin Invest. (1989) 83:937–44. doi: 10.1172/JCI113979
17. Klonowska-Szymczyk A, Wolska A, Robak T, Cebula-Obrzut B, Smolewski P, Robak E. Expression of toll-like receptors 3, 7, and 9 in peripheral blood mononuclear cells from patients with systemic lupus erythematosus. Mediators Inflamm. (2014) 2014:381418. doi: 10.1155/2014/381418
18. Mackay F, Schneider P. Cracking the BAFF code. Nat Rev Immunol. (2009) 9:491–502. doi: 10.1038/nri2572
19. Vincent FB, Morand EF, Schneider P, Mackay F. The BAFF/APRIL system in SLE pathogenesis. Nat Rev Rheumatol. (2014) 10:365–73. doi: 10.1038/nrrheum.2014.33
20. Petri M, Stohl W, Chatham W, McCune WJ, Chevrier M, Ryel J, et al. Association of plasma B lymphocyte stimulator levels and disease activity in systemic lupus erythematosus. Arthritis Rheum. (2008) 58:2453–9. doi: 10.1002/art.23678
21. Salazar-Camarena DC, Ortiz-Lazareno PC, Cruz A, Oregon-Romero E, Machado-Contreras JR, Munoz-Valle JF, et al. Association of BAFF, APRIL serum levels, BAFF-R, TACI and BCMA expression on peripheral B-cell subsets with clinical manifestations in systemic lupus erythematosus. Lupus. (2016) 25:582–92. doi: 10.1177/0961203315608254
22. Vital EM, Dass S, Buch MH, Henshaw K, Pease CT, Martin MF, et al. B cell biomarkers of rituximab responses in systemic lupus erythematosus. Arthritis Rheum. (2011) 63:3038–47. doi: 10.1002/art.30466
23. Parodis I, Zickert A, Sundelin B, Axelsson M, Gerhardsson J, Svenungsson E, et al. Evaluation of B lymphocyte stimulator and a proliferation inducing ligand as candidate biomarkers in lupus nephritis based on clinical and histopathological outcome following induction therapy. Lupus Sci Med. (2015) 2:e000061. doi: 10.1136/lupus-2014-000061
24. Rönnblom L, Leonard D. Interferon pathway in SLE: one key to unlocking the mystery of the disease. Lupus Sci Med. (2019) 6:e000270. doi: 10.1136/lupus-2018-000270
25. Yu G, Boone T, Delaney J, Hawkins N, Kelley M, Ramakrishnan M, et al. APRIL and TALL-I and receptors BCMA and TACI: system for regulating humoral immunity. Nat Immunol. (2000) 1:252–6. doi: 10.1038/79802
26. Merrill JT, Neuwelt CM, Wallace DJ, Shanahan JC, Latinis KM, Oates JC, et al. Efficacy and safety of rituximab in moderately-to-severely active systemic lupus erythematosus: the randomized, double-blind, phase II/III systemic lupus erythematosus evaluation of rituximab trial. Arthritis Rheum. (2010) 62:222–33. doi: 10.1002/art.27233
27. Rovin BH, Furie R, Latinis K, Looney RJ, Fervenza FC, Sanchez-Guerrero J, et al. Efficacy and safety of rituximab in patients with active proliferative lupus nephritis: the Lupus Nephritis Assessment with Rituximab study. Arthritis Rheum. (2012) 64:1215–26. doi: 10.1002/art.34359
28. Touma Z, Urowitz MB, Gladman DD. Systemic lupus erythematosus: an update on current pharmacotherapy and future directions. Expert Opin Biol Ther. (2013) 13:723–37. doi: 10.1517/14712598.2013.764411
29. Eko SL, van Vollenhoven RF. Rituximab and lupus–a promising pair? Curr Rheumatol Rep. (2014) 16:444. doi: 10.1007/s11926-014-0444-5
30. Fanouriakis A, Kostopoulou M, Cheema K, Anders HJ, Aringer M, Bajema I, et al. 2019 Update of the Joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of lupus nephritis. Ann Rheum Dis. (2020) 79:713–23. doi: 10.1136/annrheumdis-2020-216924
31. Anders HJ, Saxena R, Zhao MH, Parodis I, Salmon JE, Mohan C. Lupus nephritis. Nat Rev Dis Primers. (2020) 6:7. doi: 10.1038/s41572-019-0141-9
32. Jonsdottir T, Gunnarsson I, Risselada A, Henriksson EW, Klareskog L, van Vollenhoven RF. Treatment of refractory SLE with rituximab plus cyclophosphamide: clinical effects, serological changes, and predictors of response. Ann Rheum Dis. (2008) 67:330–4. doi: 10.1136/ard.2007.079095
33. Terrier B, Amoura Z, Ravaud P, Hachulla E, Jouenne R, Combe B, et al. Safety and efficacy of rituximab in systemic lupus erythematosus: results from 136 patients from the French AutoImmunity and Rituximab registry. Arthritis Rheum. (2010) 62:2458–66. doi: 10.1002/art.27541
34. Ramos-Casals M, Garcia-Hernandez FJ, de Ramon E, Callejas JL, Martinez-Berriotxoa A, Pallares L, et al. Off-label use of rituximab in 196 patients with severe, refractory systemic autoimmune diseases. Clin Exp Rheumatol. (2010) 28:468–76.
35. Witt M, Grunke M, Proft F, Baeuerle M, Aringer M, Burmester G, et al. German Registry of Autoimmune Diseases, Clinical outcomes and safety of rituximab treatment for patients with systemic lupus erythematosus (SLE) - results from a nationwide cohort in Germany (GRAID). Lupus. (2013) 22:1142–9. doi: 10.1177/0961203313503912
36. Ryden-Aulin M, Boumpas D, Bultink I, Callejas Rubio JL, Caminal-Montero L, et al. Off-label use of rituximab for systemic lupus erythematosus in Europe. Lupus Sci Med. (2016) 3:e000163. doi: 10.1136/lupus-2016-000163
37. Alshaiki F, Obaid E, Almuallim A, Taha R, El-Haddad H, Almoallim H. Outcomes of rituximab therapy in refractory lupus: a meta-analysis. Eur J Rheumatol. (2018) 5:118–26. doi: 10.5152/eurjrheum.2018.17096
38. Karmacharya P, Poudel DR, Pathak R, Donato AA, Ghimire S, Giri S, et al. Rituximab-induced serum sickness: a systematic review. Semin Arthritis Rheum. (2015) 45:334–40. doi: 10.1016/j.semarthrit.2015.06.014
39. Md Yusof MY, Shaw D, El-Sherbiny YM, Dunn E, Rawstron AC, Emery P, et al. Predicting and managing primary and secondary non-response to rituximab using B-cell biomarkers in systemic lupus erythematosus. Ann Rheum Dis. (2017) 76:1829–36. doi: 10.1136/annrheumdis-2017-211191
40. Hennessey A, Lukawska J, Cambridge G, Isenberg D, Leandro M. Adverse infusion reactions to rituximab in systemic lupus erythematosus: a retrospective analysis. BMC Rheumatol. (2019) 3:32. doi: 10.1186/s41927-019-0082-7
41. Parodis I, Soder F, Faustini F, Kasza Z, Samuelsson I, Zickert A, et al. Rituximab-mediated late-onset neutropenia in systemic lupus erythematosus - distinct roles of BAFF and APRIL. Lupus. (2018) 27:1470–8. doi: 10.1177/0961203318777116
42. Tieu J, Smith RM, Gopaluni S, Kumararatne DS, McClure M, Manson A, et al. Rituximab associated hypogammaglobulinemia in autoimmune disease. Front Immunol. (2021) 12:671503. doi: 10.3389/fimmu.2021.671503
43. Padoan R, Felicetti M, Gatto M, Polito P, Doria A, Schiavon F. Rituximab-associated hypogammaglobulinaemia in ANCA-associated vasculitis and connective tissue diseases: a longitudinal observational study. Clin Exp Rheumatol 38 Suppl. (2020) 124:188–94.
44. Mysler EF, Spindler AJ, Guzman R, Bijl M, Jayne D, Furie RA, et al. Efficacy and safety of ocrelizumab in active proliferative lupus nephritis: results from a randomized, double-blind, phase III study. Arthritis Rheum. (2013) 65:2368–79. doi: 10.1002/art.38037
45. Illidge T, Klein C, Sehn LH, Davies A, Salles G, Cartron G. Obinutuzumab in hematologic malignancies: lessons learned to date. Cancer Treat Rev. (2015) 41:784–92. doi: 10.1016/j.ctrv.2015.07.003
46. Furie RA, Aroca G, Cascino MD, Garg JP, Rovin BH, Alvarez A, et al. B-cell depletion with obinutuzumab for the treatment of proliferative lupus nephritis: a randomised, double-blind, placebo-controlled trial. Ann Rheum Dis. (2022) 81:100–7. doi: 10.1136/annrheumdis-2021-220920
47. Wierda WG, Kipps TJ, Mayer J, Stilgenbauer S, Williams CD, Hellmann A, et al. Ofatumumab as single-agent CD20 immunotherapy in fludarabine-refractory chronic lymphocytic leukemia. J Clin Oncol. (2010) 28:1749–55. doi: 10.1200/JCO.2009.25.3187
48. Haarhaus ML, Svenungsson E, Gunnarsson I. Ofatumumab treatment in lupus nephritis patients. Clin Kidney J. (2016) 9:552–5. doi: 10.1093/ckj/sfw022
49. Masoud S, McAdoo SP, Bedi R, Cairns TD, Lightstone L. Ofatumumab for B cell depletion in patients with systemic lupus erythematosus who are allergic to rituximab. Rheumatology (Oxford). (2018) 57:1156–61. doi: 10.1093/rheumatology/key042
50. Poulet A, Jarrot PA, Mazodier K, Jean R, Kaplanski G. Successful treatment of systemic lupus erythematosus-related refractory autoimmune hemolytic anemia with ofatumumab. Lupus. (2019) 28:1735–6. doi: 10.1177/0961203319881500
51. Cinar OK, Marlais M, Al Obaidi M, Cheng IL, Tullus K, Brogan P, et al. Ofatumumab use in juvenile systemic lupus erythematosus: a single centre experience. Lupus. (2021) 30:527–30. doi: 10.1177/0961203320981137
52. Wallace DJ, Goldenberg DM. Epratuzumab for systemic lupus erythematosus. Lupus. (2013) 22:400–5. doi: 10.1177/0961203312469692
53. Wallace DJ, Kalunian K, Petri MA, Strand V, Houssiau FA, Pike M, et al. Efficacy and safety of epratuzumab in patients with moderate/severe active systemic lupus erythematosus: results from EMBLEM, a phase IIb, randomised, double-blind, placebo-controlled, multicentre study. Ann Rheum Dis. (2014) 73:183–90. doi: 10.1136/annrheumdis-2012-202760
54. Clowse ME, Wallace DJ, Furie RA, Petri MA, Pike MC, Leszczynski P, et al. Efficacy and safety of epratuzumab in moderately to severely active systemic lupus erythematosus: results from two phase III randomized, double-blind, placebo-controlled trials. Arthritis Rheumatol. (2017) 69:362–75. doi: 10.1002/art.39856
55. Alexander T, Thiel A, Rosen O, Massenkeil G, Sattler A, Kohler S, et al. Depletion of autoreactive immunologic memory followed by autologous hematopoietic stem cell transplantation in patients with refractory SLE induces long-term remission through de novo generation of a juvenile and tolerant immune system. Blood. (2009) 113:214–23. doi: 10.1182/blood-2008-07-168286
56. Hoyer BF, Moser K, Hauser AE, Peddinghaus A, Voigt C, Eilat D, et al. Short-lived plasmablasts and long-lived plasma cells contribute to chronic humoral autoimmunity in NZB/W mice. J Exp Med. (2004) 199:1577–84. doi: 10.1084/jem.20040168
57. Benson MJ, Dillon SR, Castigli E, Geha RS, Xu S, Lam KP, et al. Cutting edge: the dependence of plasma cells and independence of memory B cells on BAFF and APRIL. J Immunol. (2008) 180:3655–9. doi: 10.4049/jimmunol.180.6.3655
58. Neubert K, Meister S, Moser K, Weisel F, Maseda D, Amann K, et al. The proteasome inhibitor bortezomib depletes plasma cells and protects mice with lupus-like disease from nephritis. Nat Med. (2008) 14:748–55. doi: 10.1038/nm1763
59. Alexander T, Sarfert R, Klotsche J, Kühl AA, Rubbert-Roth A, Lorenz HM, et al. The proteasome inhibitior bortezomib depletes plasma cells and ameliorates clinical manifestations of refractory systemic lupus erythematosus. Ann Rheum Dis. (2015) 74:1474–8. doi: 10.1136/annrheumdis-2014-206016
60. Sjowall C, Hjorth M, Eriksson P. Successful treatment of refractory systemic lupus erythematosus using proteasome inhibitor bortezomib followed by belimumab: description of two cases. Lupus. (2017) 26:1333–8. doi: 10.1177/0961203317691371
61. Richardson PG, Sonneveld P, Schuster MW, Irwin D, Stadtmauer EA, Facon T, et al. Assessment of proteasome inhibition for extending remissions, bortezomib or high-dose dexamethasone for relapsed multiple myeloma. N Engl J Med. (2005) 352:2487–98. doi: 10.1056/NEJMoa043445
62. Alexander T, Cheng Q, Klotsche J, Khodadadi L, Waka A, Biesen R, et al. Proteasome inhibition with bortezomib induces a therapeutically relevant depletion of plasma cells in SLE but does not target their precursors. Eur J Immunol. (2018) 48:1573–9. doi: 10.1002/eji.201847492
63. van der Vlag J, Berden JH. Proteasome inhibition: a new therapeutic option in lupus nephritis? Nephrol Dial Transplant. (2008) 23:3771–2. doi: 10.1093/ndt/gfn536
64. Obeng EA, Carlson LM, Gutman DM, Harrington WJ Jr, Lee KP, Boise LH. Proteasome inhibitors induce a terminal unfolded protein response in multiple myeloma cells. Blood. (2006) 107:4907–16. doi: 10.1182/blood-2005-08-3531
65. Nencioni A, Grunebach F, Patrone F, Ballestrero A, Brossart P. Proteasome inhibitors: antitumor effects and beyond. Leukemia. (2007) 21:30–6. doi: 10.1038/sj.leu.2404444
66. Everly MJ, Everly JJ, Susskind B, Brailey P, Arend LJ, Alloway RR, et al. Bortezomib provides effective therapy for antibody- and cell-mediated acute rejection. Transplantation. (2008) 86:1754–61. doi: 10.1097/TP.0b013e318190af83
67. Walsh RC, Alloway RR, Girnita AL, Woodle ES. Proteasome inhibitor-based therapy for antibody-mediated rejection. Kidney Int. (2012) 81:1067–74. doi: 10.1038/ki.2011.502
68. Walhelm T, Gunnarsson I, Heijke R, Leonard D, Trysberg E, Eriksson P, et al. Clinical experience of proteasome inhibitor bortezomib regarding efficacy and safety in severe systemic lupus erythematosus: a nationwide study. Front Immunol. (2021) 12:756941. doi: 10.3389/fimmu.2021.756941
69. Ishii T, Tanaka Y, Kawakami A, Saito K, Ichinose K, Fujii H, et al. Multicenter double-blind randomized controlled trial to evaluate the effectiveness and safety of bortezomib as a treatment for refractory systemic lupus erythematosus. Mod Rheumatol. (2018) 28:986–92. doi: 10.1080/14397595.2018.1432331
70. Ostendorf L, Burns M, Durek P, Heinz GA, Heinrich F, Garantziotis P, et al. Targeting CD38 with daratumumab in refractory systemic lupus erythematosus. N Engl J Med. (2020) 383:1149–55. doi: 10.1056/NEJMoa2023325
71. van Vollenhoven RF, Petri MA, Cervera R, Roth DA, Ji BN, Kleoudis CS, et al. Belimumab in the treatment of systemic lupus erythematosus: high disease activity predictors of response. Ann Rheum Dis. (2012) 71:1343–9. doi: 10.1136/annrheumdis-2011-200937
72. Parodis I, Sjowall C, Jonsen A, Ramskold D, Zickert A, Frodlund M, et al. Smoking and pre-existing organ damage reduce the efficacy of belimumab in systemic lupus erythematosus. Autoimmun Rev. (2017) 16:343–51. doi: 10.1016/j.autrev.2017.02.005
73. Parodis I, Gomez A, Frodlund M, Jonsen A, Zickert A, Sjowall C, et al. Smoking reduces the efficacy of belimumab in mucocutaneous lupus. Expert Opin Biol Ther. (2018) 18:911–20. doi: 10.1080/14712598.2018.1494719
74. Ramskold D, Parodis I, Lakshmikanth T, Sippl N, Khademi M, Chen Y, et al. B cell alterations during BAFF inhibition with belimumab in SLE. EBioMedicine. (2019) 40:517–27. doi: 10.1016/j.ebiom.2018.12.035
75. Parodis I, Johansson P, Gomez A, Soukka S, Emamikia S, Chatzidionysiou K. Predictors of low disease activity and clinical remission following belimumab treatment in systemic lupus erythematosus. Rheumatology (Oxford). (2019) 58:2170–6. doi: 10.1093/rheumatology/kez191
76. Sohrabian A, Parodis I, Carlstromer-Berthen N, Frodlund M, Jonsen A, Zickert A, et al. Increased levels of anti-dsDNA antibodies in immune complexes before treatment with belimumab associate with clinical response in patients with systemic lupus erythematosus. Arthritis Res Ther. (2019) 21:259. doi: 10.1186/s13075-019-2056-y
77. Parodis I, Gomez A, Emamikia S, Chatzidionysiou K. Established organ damage reduces belimumab efficacy in systemic lupus erythematosus. Ann Rheum Dis. (2019) 78:1006–7. doi: 10.1136/annrheumdis-2018-214880
78. Gatto M, Saccon F, Zen M, Regola F, Fredi M, Andreoli L, et al. Early disease and low baseline damage as predictors of response to belimumab in patients with systemic lupus erythematosus in a real-life setting. Arthritis Rheumatol. (2020) 72:1314–24. doi: 10.1002/art.41253
79. Parodis I, Åkerström E, Sjöwall C, Sohrabian A, Jönsen A, Gomez A, et al. Autoantibody and cytokine profiles during treatment with belimumab in patients with systemic lupus erythematosus. Int J Mol Sci. (2020) 21:3463. doi: 10.3390/ijms21103463
80. Gatto M, Saccon F, Andreoli L, Bartoloni E, Benvenuti F, Bortoluzzi A, et al. Durable renal response and safety with add-on belimumab in patients with lupus nephritis in real-life setting (BeRLiSS-LN). Results from a large, nationwide, multicentric cohort. J Autoimmun. (2021) 124:102729. doi: 10.1016/j.jaut.2021.102729
81. Iaccarino L, Andreoli L, Bocci EB, Bortoluzzi A, Ceccarelli F, Conti F, et al. Clinical predictors of response and discontinuation of belimumab in patients with systemic lupus erythematosus in real life setting. Results of a large, multicentric, nationwide study. J Autoimmun. (2018) 86:1–8. doi: 10.1016/j.jaut.2017.09.004
82. Xie W, Huang H, Zhan S, Zhang Z. Risk of psychiatric disorders and all-cause mortality with belimumab therapy in patients with systemic lupus erythematosus: a meta-analysis of randomised controlled trials. Lupus Sci Med. (2021) 8:e000534. doi: 10.1136/lupus-2021-000534
83. Wallace DJ, Ginzler EM, Merrill JT, Furie RA, Stohl W, Chatham WW, et al. Safety and efficacy of belimumab plus standard therapy for up to thirteen years in patients with systemic lupus erythematosus. Arthritis Rheumatol. (2019) 71:1125–34. doi: 10.1002/art.40861
84. van Vollenhoven RF, Kinnman N, Vincent E, Wax S, Bathon J. Atacicept in patients with rheumatoid arthritis and an inadequate response to methotrexate: results of a phase II, randomized, placebo-controlled trial. Arthritis Rheum. (2011) 63:1782–92. doi: 10.1002/art.30372
85. Ginzler EM, Wax S, Rajeswaran A, Copt S, Hillson J, Ramos E, et al. Atacicept in combination with MMF and corticosteroids in lupus nephritis: results of a prematurely terminated trial. Arthritis Res Ther. (2012) 14:R33. doi: 10.1186/ar3738
86. Furie RA, Leon G, Thomas M, Petri MA, Chu AD, Hislop C, et al. A phase 2, randomised, placebo-controlled clinical trial of blisibimod, an inhibitor of B cell activating factor, in patients with moderate-to-severe systemic lupus erythematosus, the PEARL-SC study. Ann Rheum Dis. (2015) 74:1667–75. doi: 10.1136/annrheumdis-2013-205144
87. Merrill JT, Shanahan WR, Scheinberg M, Kalunian KC, Wofsy D, Martin RS. Phase III trial results with blisibimod, a selective inhibitor of B-cell activating factor, in subjects with systemic lupus erythematosus (SLE): results from a randomised, double-blind, placebo-controlled trial. Ann Rheum Dis. (2018) 77:883–9. doi: 10.1136/annrheumdis-2018-213032
88. Isenberg DA, Petri M, Kalunian K, Tanaka Y, Urowitz MB, Hoffman RW, et al. Efficacy and safety of subcutaneous tabalumab in patients with systemic lupus erythematosus: results from ILLUMINATE-1, a 52-week, phase III, multicentre, randomised, double-blind, placebo-controlled study. Ann Rheum Dis. (2016) 75:323–31. doi: 10.1136/annrheumdis-2015-207653
89. Merrill JT, van Vollenhoven RF, Buyon JP, Furie RA, Stohl W, Morgan-Cox M, et al. Efficacy and safety of subcutaneous tabalumab, a monoclonal antibody to B-cell activating factor, in patients with systemic lupus erythematosus: results from ILLUMINATE-2, a 52-week, phase III, multicentre, randomised, double-blind, placebo-controlled study. Ann Rheum Dis. (2016) 75:332–40. doi: 10.1136/annrheumdis-2015-207654
90. Gatto M, Saccon F, Zen M, Bettio S, Iaccarino L, Punzi L, et al. Success and failure of biological treatment in systemic lupus erythematosus: a critical analysis. J Autoimmun. (2016) 74:94–105. doi: 10.1016/j.jaut.2016.06.014
91. Houssiau FA, Doria A. Targeting BAFF/BLyS in lupus: is the glass half-full or half-empty? Ann Rheum Dis. (2016) 75:321–2. doi: 10.1136/annrheumdis-2015-208312
92. Psarras A, Alase A, Antanaviciute A, Carr IM, Md Yusof MY, Wittmann M, et al. Functionally impaired plasmacytoid dendritic cells and non-haematopoietic sources of type I interferon characterize human autoimmunity. Nat Commun. (2020) 11:6149. doi: 10.1038/s41467-020-19918-z
93. Furie R, Khamashta M, Merrill JT, Werth VP, Kalunian K, Brohawn P, et al. Anifrolumab, an anti-interferon-α receptor monoclonal antibody, in moderate-to-severe systemic lupus erythematosus. Arthritis Rheumatol. (2017) 69:376–86. doi: 10.1002/art.39962
94. Furie RA, Morand EF, Bruce IN, Manzi S, Kalunian KC, Vital EM, et al. Type I interferon inhibitor anifrolumab in active systemic lupus erythematosus (TULIP-1): a randomised, controlled, phase 3 trial. Lancet Rheumatol. (2019) 1:e208–19. doi: 10.1016/S2665-9913(19)30076-1
95. Morand EF, Furie R, Tanaka Y, Bruce IN, Askanase AD, Richez C, et al. Trial of Anifrolumab in Active Systemic Lupus Erythematosus. N Engl J Med. (2020) 382:211–21. doi: 10.1056/NEJMoa1912196
96. Jayne D, Rovin B, Mysler EF, Furie RA, Houssiau FA, Trasieva T, et al. Phase II randomised trial of type I interferon inhibitor anifrolumab in patients with active lupus nephritis. Ann Rheum Dis. (2022) 81:496–506. doi: 10.1136/annrheumdis-2021-221478
97. Steiger S, Anders HJ. Interferon blockade in lupus: effects on antiviral immunity. Nat Rev Nephrol. (2022) 18:415–6. doi: 10.1038/s41581-022-00581-0
98. Vallerskog T, Heimburger M, Gunnarsson I, Zhou W, Wahren-Herlenius M, Trollmo C, et al. Differential effects on BAFF and APRIL levels in rituximab-treated patients with systemic lupus erythematosus and rheumatoid arthritis. Arthritis Res Ther. (2006) 8:R167. doi: 10.1186/ar2076
99. Cambridge G, Stohl W, Leandro MJ, Migone TS, Hilbert DM, Edwards JC. Circulating levels of B lymphocyte stimulator in patients with rheumatoid arthritis following rituximab treatment: relationships with B cell depletion, circulating antibodies, and linical relapse. Arthritis Rheum. (2006) 54:723–32. doi: 10.1002/art.21650
100. Carter LM, Isenberg DA, Ehrenstein MR. Elevated serum BAFF levels are associated with rising anti-double-stranded DNA antibody levels and disease flare following B cell depletion therapy in systemic lupus erythematosus. Arthritis Rheum. (2013) 65:2672–9. doi: 10.1002/art.38074
101. Jones A, Muller P, Dore CJ, Ikeji F, Caverly E, Chowdhury K, et al. Belimumab after B cell depletion therapy in patients with systemic lupus erythematosus (BEAT Lupus) protocol: a prospective multicentre, double-blind, randomised, placebo-controlled, 52-week phase II clinical trial. BMJ Open. (2019) 9:e032569. doi: 10.1136/bmjopen-2019-032569
102. Shipa M, Embleton-Thirsk A, Parvaz M, Santos LR, Muller P, Chowdhury K, et al. Effectiveness of belimumab after rituximab in systemic lupus erythematosus : a randomized controlled trial. Ann Intern Med. (2021) 174:1647–57. doi: 10.7326/M21-2078
103. Teng YKO, Bruce IN, Diamond B, Furie RA, van Vollenhoven RF, Gordon D, et al. Phase III, multicentre, randomised, double-blind, placebo-controlled, 104-week study of subcutaneous belimumab administered in combination with rituximab in adults with systemic lupus erythematosus (SLE): BLISS-BELIEVE study protocol. BMJ Open. (2019) 9:e025687. doi: 10.1136/bmjopen-2018-025687
104. Aranow C, Allaart C, Amoura Z, Bruce I, Cagnoli P, Furie R, et al. Efficacy and Safety of Subcutaneous Belimumab (BEL) and Rituximab (RTX) Sequential Therapy in Patients with Systemic Lupus Erythematosus: The Phase 3, Randomized, Placebo-Controlled BLISS-BELIEVE Study [abstract]. Arthritis Rheumatol. (2021) 73 (suppl 10).
105. Atisha-Fregoso Y, Malkiel S, Harris KM, Byron M, Ding L, Kanaparthi S, et al. Phase II randomized trial of rituximab plus cyclophosphamide followed by belimumab for the treatment of lupus nephritis. Arthritis Rheumatol. (2021) 73:121–31. doi: 10.1002/art.41466
106. Kraaij T, Kamerling SWA, de Rooij ENM, van Daele PLA, Bredewold OW, Bakker JA, et al. The NET-effect of combining rituximab with belimumab in severe systemic lupus erythematosus. J Autoimmun. (2018) 91:45–54. doi: 10.1016/j.jaut.2018.03.003
107. Furie R, Rovin BH, Houssiau F, Malvar A, Teng YKO, Contreras G, et al. Randomized, controlled trial of belimumab in lupus nephritis. N Engl J Med. (2020) 383:1117–28. doi: 10.1056/NEJMoa2001180
108. Wallace DJ, Furie RA, Tanaka Y, Kalunian KC, Mosca M, Petri MA, et al. Baricitinib for systemic lupus erythematosus: a double-blind, randomised, placebo-controlled, phase 2 trial. Lancet. (2018) 392:222–31. doi: 10.1016/S0140-6736(18)31363-1
109. Hasni SA, Gupta S, Davis M, Poncio E, Temesgen-Oyelakin Y, Carlucci PM, et al. Phase 1 double-blind randomized safety trial of the Janus kinase inhibitor tofacitinib in systemic lupus erythematosus. Nat Commun. (2021) 12:3391. doi: 10.1038/s41467-021-23361-z
110. van Vollenhoven RF, Hahn BH, Tsokos GC, Lipsky P, Gordon RM, Fei K, et al. Efficacy and safety of ustekinumab in patients with active systemic lupus erythematosus: results of a phase II open-label extension study. J Rheumatol. (2022) 49:380–7. doi: 10.3899/jrheum.210805
111. Lee DSW, Rojas OL, Gommerman JL. B cell depletion therapies in autoimmune disease: advances and mechanistic insights. Nat Rev Drug Discov. (2021) 20:179–99. doi: 10.1038/s41573-020-00092-2
112. Jacobi AM, Huang W, Wang T, Freimuth W, Sanz I, Furie R, et al. Effect of long-term belimumab treatment on B cells in systemic lupus erythematosus: extension of a phase II, double-blind, placebo-controlled, dose-ranging study. Arthritis Rheum. (2010) 62:201–10. doi: 10.1002/art.27189
113. Stohl W, Hiepe F, Latinis KM, Thomas M, Scheinberg MA, Clarke A, et al. Belimumab reduces autoantibodies, normalizes low complement levels, and reduces select B cell populations in patients with systemic lupus erythematosus. Arthritis Rheum. (2012) 64:2328–37. doi: 10.1002/art.34400
114. Stohl W, Schwarting A, Okada M, Scheinberg M, Doria A, Hammer AE, et al. Efficacy and safety of subcutaneous belimumab in systemic lupus erythematosus: a fifty-two-week randomized, double-blind, placebo-controlled study. Arthritis Rheumatol. (2017) 69:1016–27. doi: 10.1002/art.40049
115. Zhang F, Bae SC, Bass D, Chu M, Egginton S, Gordon D, et al. A pivotal phase III, randomised, placebo-controlled study of belimumab in patients with systemic lupus erythematosus located in China, Japan and South Korea. Ann Rheum Dis. (2018) 77:355–63. doi: 10.1136/annrheumdis-2017-211631
116. Parodis I, Gomez A, Lindblom J, Chow JW, Doria A, Gatto M. Early Changes in B and plasma cell subsets and traditional serological markers as predictors of SRI-4 response to therapy in systemic lupus erythematosus. Front Med (Lausanne). (2022) 9:852162. doi: 10.3389/fmed.2022.852162
117. Parodis I, Gomez A, Chow JW, Borg A, Lindblom J, Gatto M. Early B cell and plasma cell kinetics upon treatment initiation portend flares in systemic lupus erythematosus: a post-hoc analysis of three phase III clinical trials of belimumab. Front Immunol. (2022) 13:796508. doi: 10.3389/fimmu.2022.796508
118. Regola F, Piantoni S, Lowin T, Archetti S, Reggia R, Kumar R, et al. Association between changes in BLyS levels and the composition of B and T cell compartments in patients with refractory systemic lupus erythematosus treated with belimumab. Front Pharmacol. (2019) 10:433. doi: 10.3389/fphar.2019.00433
Keywords: systemic lupus erythematosus, B cells, B lymphocyte, plasma cells, plasmablasts, therapy, biologics, lupus nephritis
Citation: Parodis I, Gatto M and Sjöwall C (2022) B cells in systemic lupus erythematosus: Targets of new therapies and surveillance tools. Front. Med. 9:952304. doi: 10.3389/fmed.2022.952304
Received: 24 May 2022; Accepted: 15 August 2022;
Published: 30 August 2022.
Edited by:
Chris Wincup, King's College Hospital NHS Foundation Trust, United KingdomReviewed by:
Gerard Espinosa, Hospital Clinic of Barcelona, SpainMatteo Piga, University of Cagliari, Italy
Copyright © 2022 Parodis, Gatto and Sjöwall. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ioannis Parodis, aW9hbm5pcy5wYXJvZGlzQGtpLnNl