 Pascal Owusu-Agyemang
Pascal Owusu-Agyemang Lei Feng3
Lei Feng3 Juan P. Cata
Juan P. Cata
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 18 August 2022
Sec. Intensive Care Medicine and Anesthesiology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.950444
This article is part of the Research Topic New Trends in Regional Analgesia and Anesthesia View all 12 articles
Background: Where applicable, regional anesthesia has been shown to be superior to opioid or non-opioid analgesic modalities alone. However, some studies have shown ethnic-based disparities in the use of regional anesthesia in patients undergoing surgical procedures. In this study of patients who had undergone major oncologic surgery, our main objective was to compare the use of regional anesthesia between patients of different ethnicities.
Methods: A retrospective review of adults who had undergone major open abdominal surgical procedures between 2016 and 2021 was performed. Logistic regression models were used to assess the association between baseline patient characteristics and the use of regional anesthesia.
Results: A total of 4,791 patients were included in the analysis. The median age was 60.5 years [interquartile range, 49, 69], the majority were female (65%), and of American Society of Anesthesiologists Physical Status Class (ASA) 3 (94.7%). Regional anesthesia was used in 2,652 patients (55.4%) and was not associated with race or ethnicity (p = 0.287). Compared to White patients, the odds of regional anesthesia use in other racial/ethnic groups were: Asian {odds ratio (OR) 0.851 [95% confidence interval (CI), 0.660–1.097]; p = 0.2125}, Black/African American [OR 0.807 (95% CI, 0.651–1.001); p = 0.0508], Hispanic/Latino [OR 0.957 (95% CI, 0.824–1.154); p = 0.7676], Other race [OR 0.957 (95% CI, 0.627–1.461); p = 0.8376]. In the multivariable analysis, age [OR 0.995 (95% CI, 0.991–1.000); p = 0.0309] and female gender [OR 1.231 (95% CI, 1.090–1.390); p = 0.0008] were associated with the use of regional anesthesia.
Conclusion: In this single-institution retrospective study of adults who had undergone major open abdominal surgery, the use of regional anesthesia was not associated with race or ethnicity. In the multivariable analysis, age and female gender were associated with the use of regional anesthesia.
Racial and ethnic-based disparities in healthcare delivery have been long studied. These disparities are not only associated with higher morbidity and mortality among ethnic minorities from diseases such as diabetes, cardiovascular disease, and cancer, but have also been associated with a lesser likelihood of receiving optimal pain management (1–3).
The inclusion of regional anesthesia in perioperative pain control regimens has been shown to be superior to opioid or non-opioid analgesic modalities alone (4–6). However, some studies have shown ethnic-based disparities in the use of regional anesthesia (1, 7–11). For example, in a retrospective study of 639 patients in an enhanced recovery program, the use of epidural anesthesia or transversus abdominis plane (TAP) blocks was 13% lower in non-White patients than in White patients (1). In another retrospective cohort study of 5,810 adults who had undergone inguinal hernia repair, patients who identified as Black and those of other ethnic minority groups were up to 68% less likely to receive epidural anesthesia compared with their White counterparts (8). A similar observation was made in 81, 345 patients who had undergone mastectomy, where compared to White patients, the odds of receipt of regional anesthesia was up to 21% lower in non-White patients (9). Potential reasons for these disparities have included implicit bias (1, 8, 11), language barriers (10, 11), and cultural preferences (11).
On the other hand, other studies including some with very large cohorts, have not shown an association between race or ethnicity and the receipt of regional anesthesia. For example, in a retrospective propensity matched cohort study of patients in the American College of Surgeons-National Surgical Quality Improvement Program (ACS NSQIP) database, patient race or ethnicity was not associated with the type of anesthesia received for total joint arthroplasty (12). In another a single-center study of 25,664 children undergoing surgery at a tertiary children's hospital, race and ethnicity were not associated with the odds of receiving regional anesthesia (13). These differences in findings suggest ethnic-based disparities in the use of regional anesthesia may vary from institution to institution.
To effectively identify and address any such disparities, studies in different patient populations and at local and institutional levels are required. To the best of our knowledge, racial or ethnic-based differences in the use of regional anesthesia in patients undergoing major abdominal surgery for cancer has not been evaluated. To that end, we conducted a retrospective study of adult patients who had undergone major open abdominal surgery, with the primary objective of comparing the use of regional anesthesia (epidural or truncal blocks) between non-Hispanic White patients and patients of different races and ethnicities. Based on the results of previous studies (1, 8, 9), our hypothesis was that non-Hispanic White patients were more likely to receive regional anesthesia than patients of other racial or ethnic groups. The secondary objectives included racial or ethnic-based comparisons of intraoperative and immediate postoperative opioid administration, and early postoperative pain intensity scores.
This study was approved by the Institutional Review Board (IRB) of the University of Texas MD Anderson Cancer Center on September 27, 2021 (IRB # 2021-0738).
The institutional data warehouse was used to identify patient admissions for surgical procedures between March 1, 2016, and August 1, 2021. The patient selection process was designed to include only those patients who would have been offered a regional anesthetic preoperatively. Thus, non-abdominal procedures and those performed by surgical services who do not use regional anesthesia were excluded. Additionally, due to the lesser likelihood of use of epidural anesthesia or truncal blocks, patients of American Society of Anesthesiologists Physical Status (ASA PS) 4 and above, and those undergoing emergency and outpatient procedures were excluded. Furthermore, due to the higher likelihood of surgeon-performed local anesthetic block, laparoscopic and robotic assisted procedures were excluded. To avoid over-representation of individual patients, only data from their index admission for open abdominal surgery was evaluated. The patient selection process is illustrated in Figure 1.
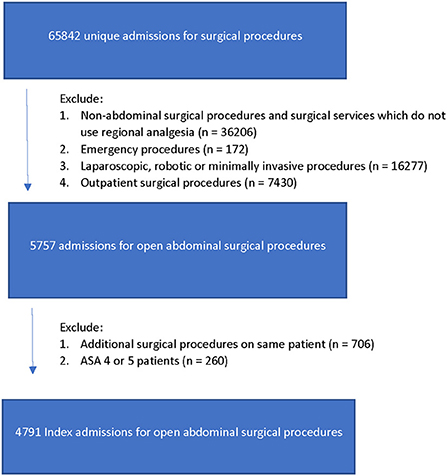
Figure 1. Patient selection process.
Perioperative variables were extracted from subsections of the institutional data warehouse including the Anesthesia, Pharmacy, Orders, Order Reconciliation, and Oncology Universes.
Patient demographics, a history of anxiety, depression, chronic pain, opioid use within the 3 months prior to surgery (preoperative opioid use), as well as any history of smoking, alcohol or drug abuse were recorded. Baseline coagulation parameters including platelet count, prothrombin time (PT), international normalized ratio (INR), and activated partial thromboplastin time (aPTT) were also recorded.
The use of epidural anesthesia or truncal blocks which were performed as a part of the initial anesthetic were recorded as “Regional Anesthesia” (Yes/No). The use of rescue blocks, and regional anesthetics which were performed postoperatively was not evaluated for this study. Intraoperative opioid administration, Post Anesthesia Care Unit (PACU) opioid consumption in morphine daily dose equivalents (MEDD), PACU pain intensity using verbal numeric rating scores (0 = no pain, 10 = worst pain ever), PACU length of stay (hours), and verbal numeric rating pain scores on postoperative day one were also recorded.
At our institution, the decision to use regional anesthesia or not is largely determined by our surgeons' established preferences. The type of regional anesthetic is also largely determined by surgeons' preferences. For the most part, regional anesthesia for open abdominal procedures involves either a thoracic epidural catheter or bilateral transversus abdominis plane (TAP) and quadratus lumborum blocks. Occasionally, paravertebral blocks and erector spinae plane blocks are used. All regional anesthetics which are performed for postoperative management are performed prior to the surgical incision. Other aspects of anesthetic management including intraoperative opioid administration and the use of multimodal analgesic techniques are not standardized. In particular, multimodal analgesic techniques are used to varying degrees by different practitioners.
In the PACU, a standardized order-set with preset dosages and limits for opioid and non-opioid analgesic medications is used. Additional doses are ordered for inadequate pain control. After discharge from the PACU, pain control in patients who did not receive regional anesthesia is managed by the surgical services according to service-based customized order-sets. Patients who received regional anesthesia continue to be managed by the acute pain service until regional anesthesia catheters have been discontinued, or adequate pain control has been established with the use of opioid and non-opioid analgesics. During this period, pain assessment is initially performed every hour for the first 12 h, then every 4 h thereafter. In addition, pain assessments are performed 1 h after any change in medication administration.
Patients' demographics, treatment, and clinical outcomes were summarized through descriptive statistics. The Wilcoxon rank sum test or Kruskal-Wallis test was used to compare location parameters of continuous distributions between or among patient groups. The Chi-square test was used to evaluate the association between two categorical variables. A multivariable logistic regression model was fitted to estimate the effects of important covariates on regional anesthesia use and highest or average PACU pain score using 5 as the cutoff point. Statistical software SAS 9.4 (SAS, Cary, NC) and Splus 8.2 (TIBCO Software Inc., Palo Alto, CA) were used for all the analyses.
A total of 4,791 patients were included in the analysis. The median age [Interquartile Range (IQR)] was 60.5 years [IQR, 49, 69], the majority were female (65%), and of ASA class 3 (94.7%).
Information about race and ethnicity was missing for 34 patients. Among those patients with information, 257 (5.4%) were Asian, 373 (7.8%) were Black or African American, 652 (13.7%) were Hispanic or Latino, 3,391 (71.3%) were non-Hispanic White (White), and due the small numbers in their individual groups, 89 (1.9%) were classified together as Other race. Of the patients who were classified together as Other race, 66 (1.4%) self-identified as Other race, 17 (0.4%) as American Indian or Alaska Native, and 6 (0.1%) as Native Hawaiian or Other Pacific Islander.
Baseline characteristics of the study population are shown in Table 1. Compared to patients of other races or ethnicities, the group of White patients were older [median 61 years, interquartile range (IQR) 50, 69] and had the highest proportion of proportion of patients with a diagnosis of anxiety or depression (683/3,391 [20.1%]). Black or African American patients had the highest proportion of female patients (189/368 [51.4%]), and highest values for platelet counts (median 241, IQR [193, 305]), PT (median 13.7, IQR [13.1, 14.4]), and INR (median 1.04, IQR [1.0, 1.1]). The group of Asian patients had the highest median value for aPTT (median 31.1, IQR [29.2, 33.8]), and the lowest proportion of patients with a BMI > 25 (108/255 [42.4%]). Preoperative opioid use was highest within the group of patients categorized as “Other race”.
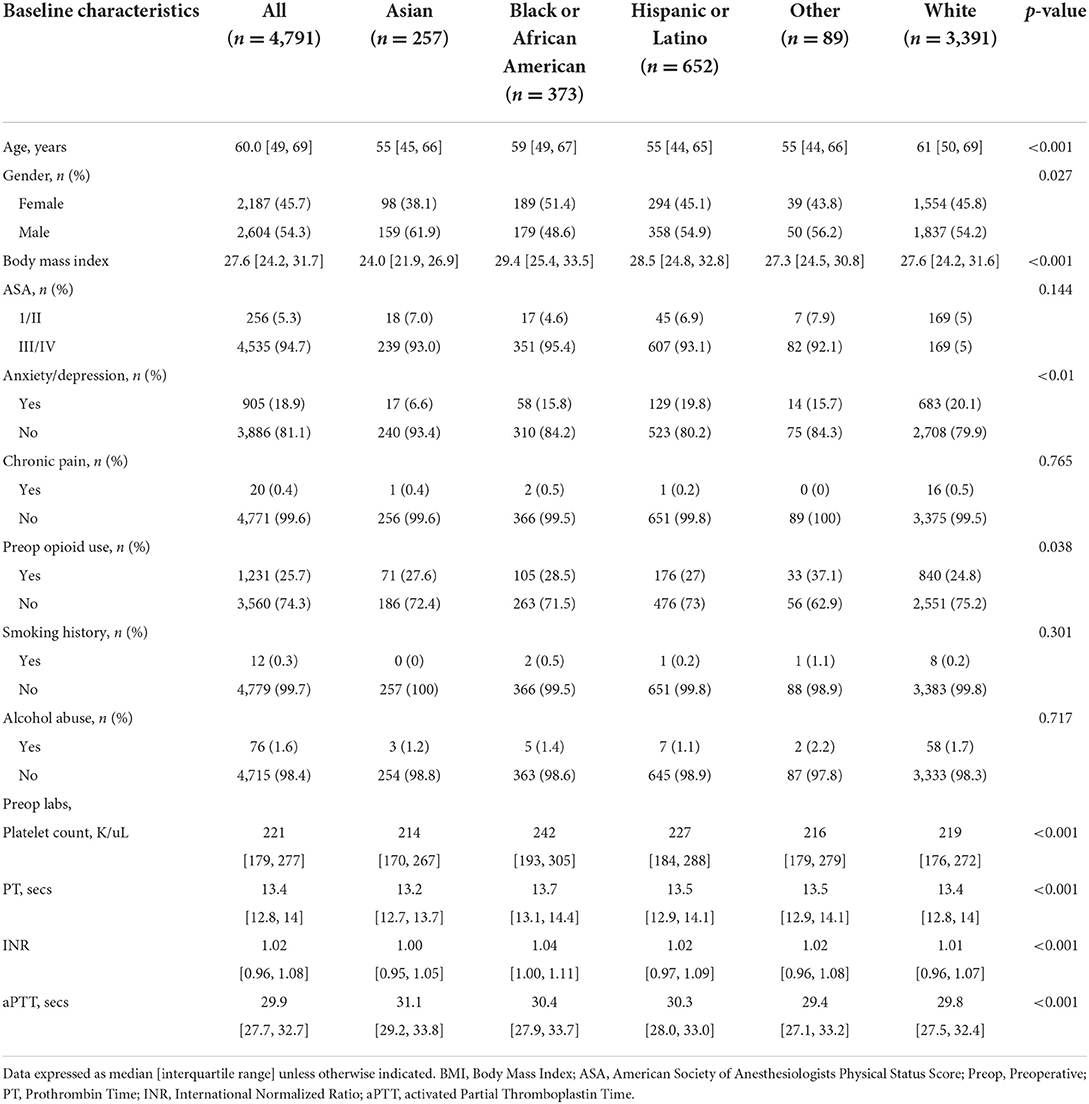
Table 1. Demographic and baseline characteristics of 4,791 adults undergoing open abdominal surgery.
Regional anesthesia was used in 2,652/4,791 patients (55.4%) and included epidural catheters (1,221/4,791, 25.5%), TAP/quadratus lumborum blocks (1,429/4,791, 29.8%), paravertebral blocks (1/4,791, 0.02%), and erector spinae plane blocks (1/4791, 0.02%). A larger proportion of females than males received regional anesthesia (58.4 vs. 52.8% males, p = 0.0001).
Patients who received regional anesthesia were also younger than those who did not receive regional anesthesia (median 59.5 years, IQR [48, 68], vs. 61 years, IQR [49, 69], p = 0.0029).
The use of regional anesthesia was not associated with statistically significant differences based on race or ethnicity (p = 0.287). The proportions of patients who received regional anesthesia within each racial or ethnic group were; Asian (52.1%), Black or African American (50.8%), Hispanic or Latino (55.5%), Other race (55.1%), and White (56.1%). The univariate analysis (Table 2) showed that age {odds ratio (OR) 0.995 [95% confidence interval (CI), 0.991–1.000]; p = 0.0296}, female gender [OR 1.259 (95% CI, 1.122–1.412); p < 0.0001], ASA class (56.3% of ASA 3 or higher vs. 38.3% of ASA 2; p < 0.001), and a history of anxiety or depression [OR 1.215 (95% CI, 1.049–1.407); p = 0.0093] were associated with the use of regional anesthesia. Higher values of PT [OR 0.838 (95% CI, 0.794–0.885); p < 0.0001], and INR [OR 0.335 (95% CI, 0.203–0.553); p < 0.0001] were associated with decreased odds for the receipt of regional anesthesia. The multivariate analysis indicated that only age [OR 0.995 (95% CI, 0.991–1.000); p = 0.0309] and female gender [OR 1.231 (95% CI, 1.090–1.390); p = 0.0008] were independent predictors of the use of regional anesthesia (Table 2).
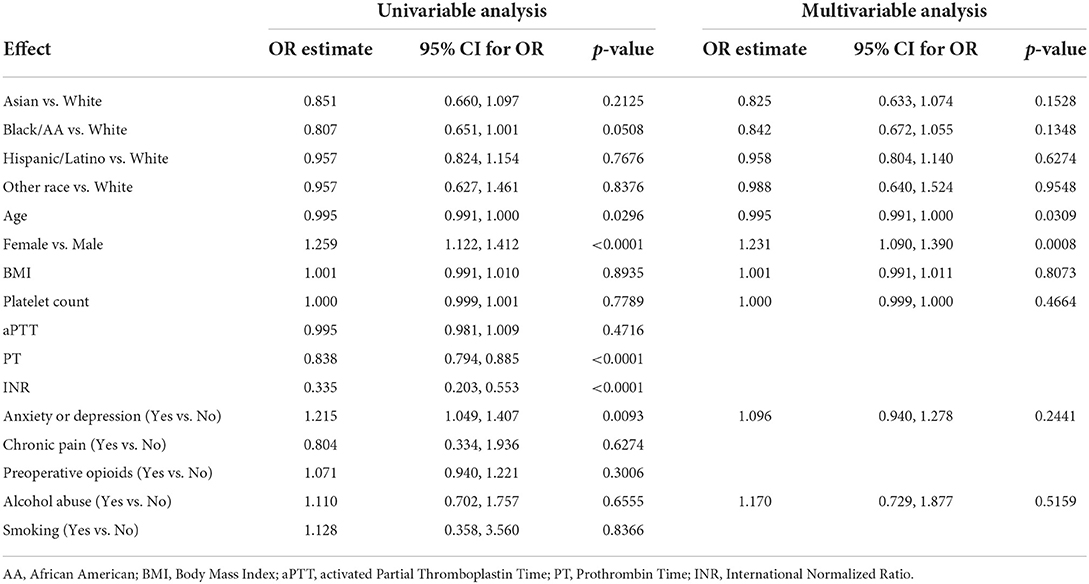
Table 2. Association between baseline patient characteristics and the use of regional anesthesia.
Intraoperative opioid administration was not associated with patient race or ethnicity (Table 3). However, opioid administration in the PACU was associated with race/ethnicity (p = 0.038) with the highest administration observed in patients who were categorized as Other race.
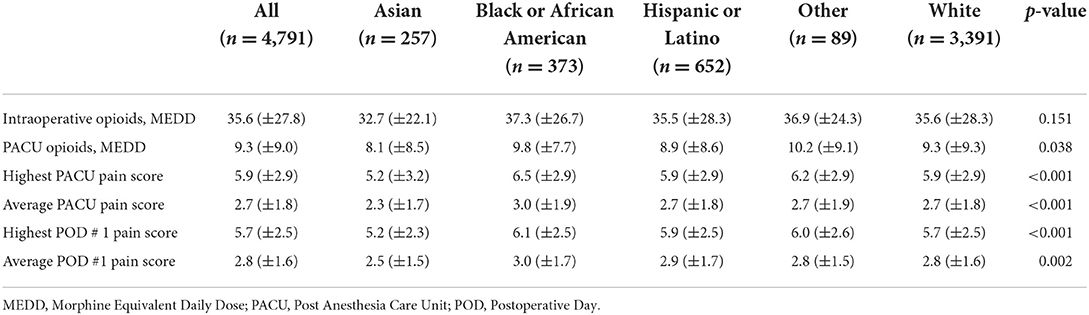
Table 3. Opioid administration and average pain scores of 4,791 adults undergoing open abdominal surgery for cancer.
Pain intensity in the PACU was associated with race and ethnicity (p < 0.001). The highest and average PACU pain scores were significantly lower in Asian patients, and highest in Black or African American Patients (Table 3). Pain intensity on postoperative day one was also significantly associated with race/ethnicity. Similar to pain intensity in the PACU, the highest and average pain scores on postoperative day one were significantly lower in the group of Asian patients, and highest in the group of Black or African American patients (Table 3).
Regarding highest PACU pain scores ≥ 5, patients who were 60 years of age or older (1,646/2,468 [66.7%]; p < 0.001), male patients (1,777/2,599 [68.4%]; p < 0.001), Asian patients (154/257 [59.9%]; p = 0.0001), those without a history of anxiety or depression (2,713/3,881 [69.9%]; p < 0.001), and those who did not use opioids prior to surgery (2,464/3,559 [69.2%]; p < 0.001) had significantly lower proportions of patients with a highest PACU pain score of 5 or higher (Table 4). In the multivariable analysis (Table 5), the association between race/ethnicity and a highest PACU pain score ≥ 5 was significant (p < 0.001). In this regard, compared to White patients, Asian patients had a significantly lower likelihood of having a highest PACU pain score of 5 or greater [OR 0.581 (95% CI, 0.443–0.762); p < 0.001], and Black or African American patients had greater than a 30% likelihood of having a score of 5 or greater [OR 1.384 (95% CI, 1.066–1.797); p = 0.015]. Furthermore, patients who used opioids preoperatively [OR 1.372 (95% CI, 1.178–1.598); p < 0.001], and those with a history of anxiety or depression [OR 1.229 (95% CI, 1.034–1.461); p = 0.019] had greater odds of having a highest PACU pain score of 5 or greater. Additionally, the likelihood of having a highest PACU pain score ≥ 5 lessened with increasing patient age [OR 0.917 (95% CI, 0.895–0.939); p < 0.001].
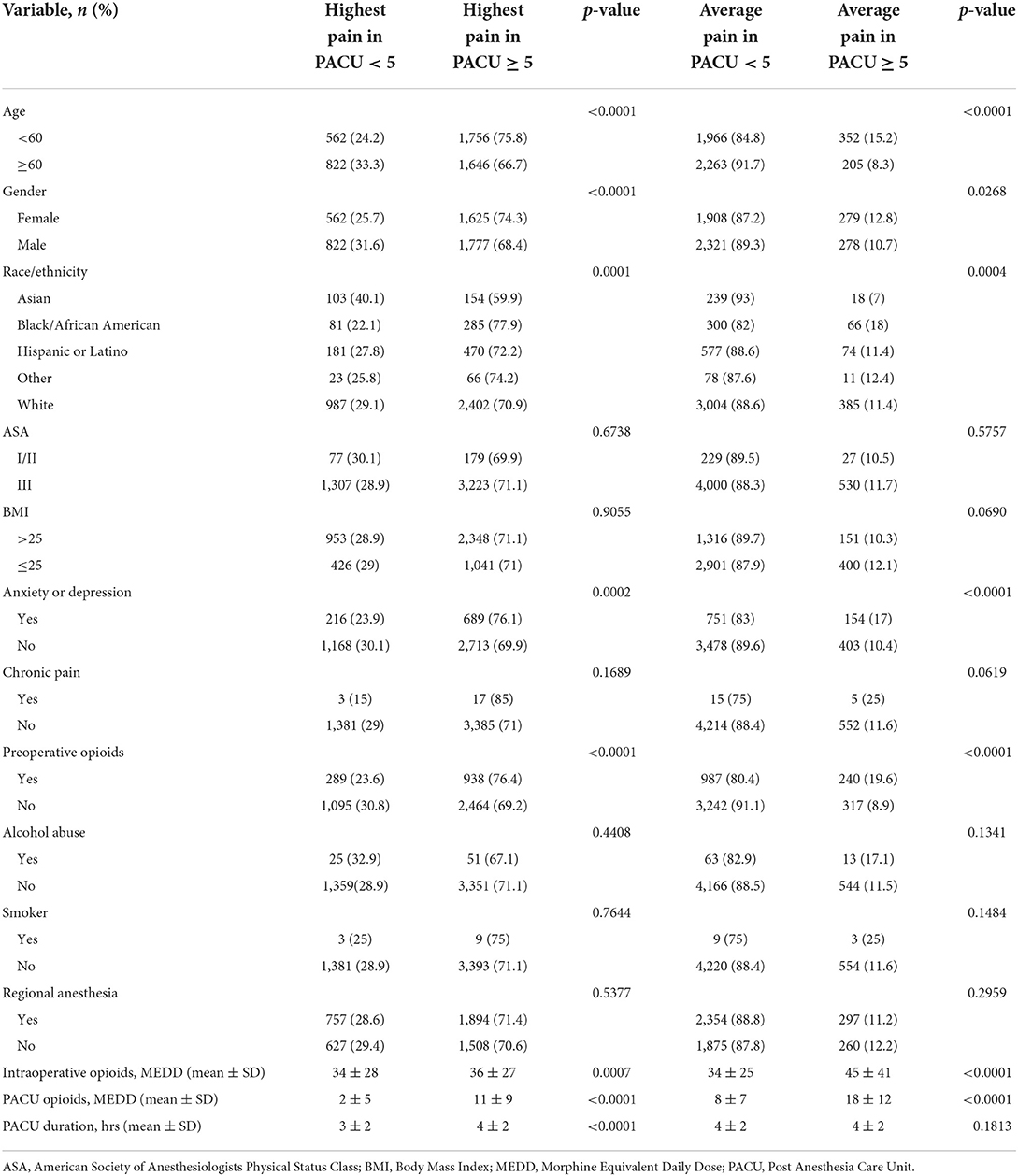
Table 4. Univariable analysis of the association between highest and average PACU pain scores and the perioperative characteristics of 4,791 adults undergoing open abdominal surgery.
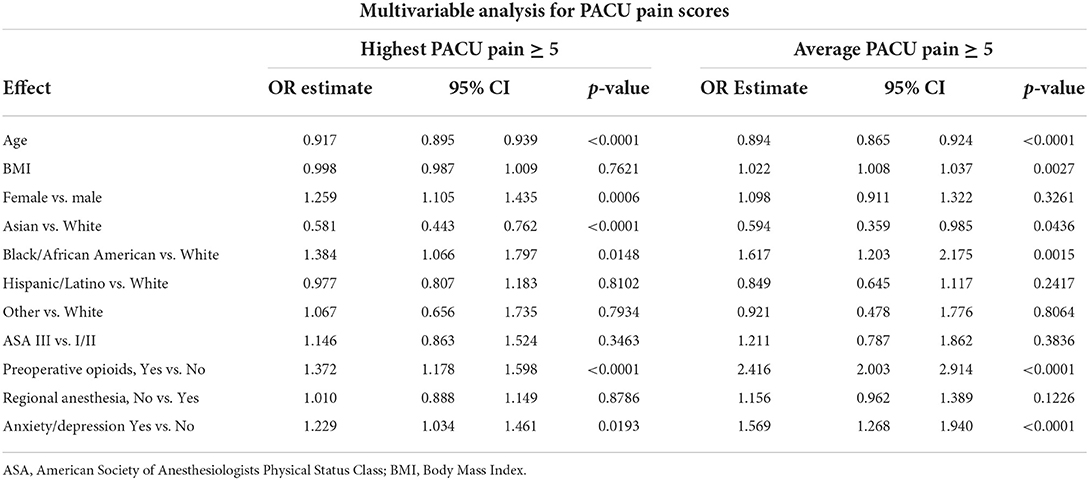
Table 5. Multivariable analysis of the association between highest and average PACU pain scores and the perioperative characteristics of 4,791 adults undergoing open abdominal surgery.
The proportion of patients with an average PACU pain score of 5 or higher was significantly lower among patients who were 60 years of age or older (205/2,468 [8.3%]; p < 0.001), male patients (278/2,599 [10.7%]; p < 0.027), Asian patients (18/257 [7%]; p = 0.0004), those without a history of anxiety or depression (403/3,881 [10.4%]; p < 0.001), and those who did not use opioids prior to surgery (317/3,559 [8.9%]; p < 0.001). The multivariable model (Table 5) demonstrated a significant association between race/ethnicity and an average PACU pain score of 5 or higher (p = 0.0015). Compared to White patients, Asian patients had a lesser likelihood of having an average pain score of 5 or higher [OR 0.594 (95% CI, 0.359–0.985); p = 0.044]. On the other hand, Black or African American patients had a >60% likelihood of having an average PACU pain score of 5 or higher [OR 1.617 (95% CI, 1.203–2.175); p = 0.002]. Patient age [OR 0.894 (95% CI, 0.865–0.924); p < 0.001], BMI [OR 1.002 (95% CI, 1.008–1.037); p = 0.003], preoperative opioid use [OR 2.416 (95% CI, 2.003–2.914); p < 0.001], and a history of anxiety and/or depression [OR 1.569 (95% CI, 1.268–1.940); p < 0.001] were also independently associated with an average PACU pain score of 5 or higher.
In this single-center retrospective study, there were no statistically significant racial or ethnic-based differences in the use of regional anesthesia or in intraoperative opioid administration. However, significant racial and ethnic-based differences were observed in terms of postoperative pain intensity and in the administration of opioids in the PACU. In this regard, the severity of postoperative pain was lowest in the group of Asian patients and highest in Black or African American patients. Postoperative opioid administration was highest in patients who were grouped together as “Other Race”.
Similar to our findings, the absence of an association between the use of regional anesthesia and patient race or ethnicity has been reported in other patient populations (12, 13). For example, in a retrospective cohort study by Elsharydah et al. (12), the proportion of African American patients who underwent total hip and knee arthroplasty with regional anesthesia was 2.3% less than in White patients. However, this observed difference was not detectable after propensity score matching. Similarly, in a large single-center study of pediatric patients, the proportion of minority patients who received regional anesthesia for their procedures was 1.4% less than their White counterparts. However, there was no statistically significant difference after multivariable and sensitivity analyses.
One of the major challenges in addressing racial or ethnic-based disparities in healthcare delivery is the difficulty in determining the reasons for its existence or absence. Regarding our study, the decision to use regional anesthesia or not was largely based on individual surgeons' established preferences. On any given day, modifications or changes to this established preference was discussed between the surgeon and the anesthesiologist. We speculate that this added level of discussion may have aided in ameliorating any potential racial or ethnic-based biases in offering regional anesthesia to patients.
In this study, younger age and female gender were independently associated with higher odds of receiving regional anesthesia. The reasons for these significant associations are not discernible from our data. With regard to age, the difference in age between the study groups, although statistically significant, may not be clinically significant. Thus, it is difficult to speculate about possible reasons for this statistical significance. With regard to female patients having higher odds of receiving regional anesthesia, a survey investigating patient perceptions of regional anesthesia revealed that more patients, especially females, would accept regional anesthesia if reassured appropriately (14). Furthermore, patients were more likely to accept regional anesthesia if they had chosen it in the past. Based on the findings of this survey, it may be possible that prior experience with labor epidurals contributed to a higher rate of acceptance of regional anesthesia among females patients in our study population.
In our study population, postoperative pain intensity was statistically different based on race and ethnicity. In this regard, Asian patients had the lowest and Black or African American had the highest pain scores in the PACU and on postoperative day one. The results of studies evaluating postoperative and experimental pain in the Asian population have been mixed (15–18). These mixed results may be due to the complex interaction of cultural, social, biologic and genetic factors. The diverse nature of the population on the Asian continent may also contribute to the mixed findings.
On the other hand, several studies have demonstrated that Black patients have a lower threshold to painful stimuli and report more postoperative pain than White patients (16, 17, 19). Some have reported on this disparity even when regional anesthesia has been used (20). This higher burden of pain has been attributed to physiological, social, cultural and provider-level reasons (21).
In our study, higher BMI was independently associated with greater odds of an average PACU score of 5 or higher. Furthermore, BMI was significantly associated with race and ethnicity, with the group of Black or African American patients having the highest median BMI among all racial or ethnic groups. The association between BMI and postoperative pain has been reported by other studies as well (22, 23). Postulated mechanisms for the decreased effectiveness of regional anesthetic techniques in obese patients include an increased rate of failure to accurately identify anatomical landmarks (23, 24), and altered pharmacokinetics of local anesthetics in adipose tissue (22). Other authors have suggested that compared to ultrasound guided transversus abdominis plane block, ultrasound guided erector spinae block may be more feasible and effective in providing intra and postoperative analgesia in patients with high BMI (25).
Other factors which were independently associated with a higher intensity of postoperative pain included younger patient age, female gender, preoperative opioid use, and a history of anxiety or depression. In a recent systematic review and meta-analysis representing 53,362 patients, Yang et al. identified similar factors to be predictive of poor acute postoperative pain control (26). In the current study, despite having significantly higher odds of receiving regional anesthesia, younger patients and female patients had significantly higher pain intensity. This finding suggests that other measures may have been necessary to attain adequate pain control in this group of patients. For example, in women undergoing breast cancer surgery, preoperative interventions such as music therapy and aromatherapy have been shown to be effective in reducing preoperative anxiety, whilst music therapy and acupuncture were shown to be effective in minimizing postoperative pain (27). With regard to preoperative anxiety, preoperative complimentary therapies such as music therapy, aromatherapy and guided imagery have been shown to reduce preoperative anxiety, albeit to varying degrees (27, 28).
With regard to the association between preoperative opioid use and higher postoperative pain intensity, chronic opioid use has been associated with tolerance to opioids and opioid induced hyperalgesia (OIH), both of which could result in higher postoperative pain intensity and increased opioid requirements (29, 30). In our study, the group of patients who were classified as “Other” race had a significantly higher proportion of patients who used opioids preoperatively. Accordingly, postoperative opioid requirements were significantly higher in this sub-group of patients. The molecular mechanisms of tolerance and OIH may be due to neuroplastic changes in the peripheral and central nervous systems that result in sensitization of pronociceptive pathways, and the N-methyl-D-aspartate (NMDA) receptor system has been shown to play a significant role (31). The inclusion of NMDA receptor modulators such as methadone and ketamine in pain control regimens has been shown to reduce opioid usage and improve pain control in patients who may be tolerant to opioids and in those who are susceptible to OIH (32, 33).
This study has several limitations. Firstly, the retrospective nature of this study meant details of the decision to use or not to use regional anesthesia could not be determined with certainty. Second, several missing values for platelet counts, PT, INR, and aPTT meant they could not be included in the multivariable analysis to determine their effect on the use of regional anesthesia. Lastly, the lack of available studies on ethnic disparities in the use of regional anesthesia during major abdominal surgery meant we could not perform an a priori sample-size analysis.
In conclusion, in this single-center retrospective study of adults who had undergone major abdominal surgery for cancer, the use of regional anesthesia was not associated with patient race or ethnicity. However, postoperative pain intensity and PACU opioid consumption were associated with race/ethnicity with the group of Asian patients having significantly lower pain scores, and the group of patients classified together as “Other race” having the highest PACU opioid consumption.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Institutional Review Board (IRB) of the University of Texas MD Anderson Cancer Center (IRB # 2021-0738). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
PO-A: conceptualization of study, data collection, and writing of manuscript. JC: conceptualization of study, critical review of data, and writing of manuscript. VP and UW: critical review of data and writing of manuscript. LF: statistical analysis. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Leeds IL, Alimi Y, Hobson DR, Efron JE, Wick EC, Haut ER, et al. Racial and socioeconomic differences manifest in process measure adherence for enhanced recovery after surgery pathway. Dis Colon Rectum. (2017) 60:1092–101. doi: 10.1097/DCR.0000000000000879
2. Meghani SH, Byun E, Gallagher RM. Time to take stock: a meta-analysis and systematic review of analgesic treatment disparities for pain in the United States. Pain Med. (2012) 13:150–74. doi: 10.1111/j.1526-4637.2011.01310.x
3. Burgess DJ, Phelan S, Workman M, Hagel E, Nelson DB, Fu SS, et al. The effect of cognitive load and patient race on physicians' decisions to prescribe opioids for chronic low back pain: a randomized trial. Pain Med. (2014) 15:965–74. doi: 10.1111/pme.12378
4. Salicath JH, Yeoh EC, Bennett MH. Epidural analgesia versus patient-controlled intravenous analgesia for pain following intra-abdominal surgery in adults. Cochrane Database Syst Rev. (2018) 8:CD010434. doi: 10.1002/14651858.CD010434.pub2
5. Dudek P, Zawadka M, Andruszkiewicz P, Gelo R, Pugliese F, Bilotta F. Postoperative analgesia after open liver surgery: systematic review of clinical evidence. J Clin Med. (2021) 10:3662. doi: 10.3390/jcm10163662
6. Qin C, Liu Y, Xiong J, Wang X, Dong Q, Su T, et al. The analgesic efficacy compared ultrasound-guided continuous transverse abdominis plane block with epidural analgesia following abdominal surgery: a systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. (2020) 20:52. doi: 10.1186/s12871-020-00969-0
7. Memtsoudis SG, Poeran J, Zubizarreta N, Rasul R, Opperer M, Mazumdar M. Anesthetic care for orthopedic patients: is there a potential for differences in care? Anesthesiology. (2016) 124:608–23. doi: 10.1097/ALN.0000000000001004
8. Memtsoudis SG, Besculides MC, Swamidoss CP. Do race, gender, and source of payment impact on anesthetic technique for inguinal hernia repair? J Clin Anesth. (2006) 18:328–33. doi: 10.1016/j.jclinane.2005.08.006
9. Beletsky A, Burton BN, Finneran Iv JJ, Alexander BS, Macias A, Gabriel RA. Association of race and ethnicity in the receipt of regional anesthesia following mastectomy. Reg Anesth Pain Med. (2021) 46:118–23. doi: 10.1136/rapm-2020-101818
10. Meier J, Stevens A, Berger M, Hogan TP, Reisch J, Cullum CM, et al. Racial and ethnic disparities in access to local anesthesia for inguinal hernia repair. J Surg Res. (2021) 266:366–72. doi: 10.1016/j.jss.2021.04.026
11. DelPizzo K, Fiasconaro M, Wilson LA, Liu J, Poeran J, Freeman C, et al. The utilization of regional anesthesia among pediatric patients: a retrospective study. HSS J. (2020) 16 (Suppl. 2):425–35. doi: 10.1007/s11420-020-09805-0
12. Elsharydah A, Embabi AS, Minhajuddin A, Joshi GP. Racial disparity in the perioperative care for patients undergoing total knee and hip arthroplasty: a retrospective propensity-matched cohort study. J Racial Ethn Health Disparities. (2018) 5:632–7. doi: 10.1007/s40615-017-0409-2
13. King MR, De Souza E, Rosenbloom JM, Wang E, Anderson TA. Association between race and ethnicity in the delivery of regional anesthesia for pediatric patients: a single-center study of 3189 regional anesthetics in 25,664 surgeries. Anesth Analg. (2020) 131:255–62. doi: 10.1213/ANE.0000000000004456
14. Dove P, Gilmour F, Weightman WM, Hocking G. Patient perceptions of regional anesthesia: influence of gender, recent anesthesia experience, and perioperative concerns. Reg Anesth Pain Med. (2011) 36:332–5. doi: 10.1097/AAP.0b013e318217a89b
15. Rivas E, Cohen B, Adegboye J, Salih A, Chelnick D, Qiu Y, et al. Ethnic differences in analgesic efficacy and safety of liposomal bupivacaine among asian and caucasian surgical patients: a retrospective matched-cohort analysis. Asian J Anesthesiol. (2020) 58:99–110. doi: 10.6859/aja.202009_58(3).0003
16. Al-Hashimi M, Scott S, Griffin-Teall N, Thompson J. Influence of ethnicity on the perception and treatment of early post-operative pain. Br J Pain. (2015) 9:167–72. doi: 10.1177/2049463714559254
17. Rahim-Williams B, Riley JL, Williams AK, Fillingim RB. A quantitative review of ethnic group differences in experimental pain response: do biology, psychology, and culture matter? Pain Med. (2012) 13:522–40. doi: 10.1111/j.1526-4637.2012.01336.x
18. Kim HJ, Yang GS, Greenspan JD, Downton KD, Griffith KA, Renn CL, et al. Racial and ethnic differences in experimental pain sensitivity: systematic review and meta-analysis. Pain. (2017) 158:194–211. doi: 10.1097/j.pain.0000000000000731
19. Perry M, Baumbauer K, Young EE, Dorsey SG, Taylor JY, Starkweather AR. The influence of race, ethnicity and genetic variants on postoperative pain intensity: an integrative literature review. Pain Manag Nurs. (2019) 20:198–206. doi: 10.1016/j.pmn.2018.11.002
20. Mehdiratta JE, Saab R, Chen Z, Li YJ, Habib AS. Patient and procedural risk factors for increased postoperative pain after cesarean delivery under neuraxial anesthesia: a retrospective study. Int J Obstet Anesth. (2020) 44:60–7. doi: 10.1016/j.ijoa.2020.07.006
21. Campbell CM, Edwards RR. Ethnic differences in pain and pain management. Pain Manag. (2012) 2:219–30. doi: 10.2217/pmt.12.7
22. Zengin M, Ulger G, Baldemir R, Sazak H, Alagoz A. Is there a relationship between body mass index and postoperative pain scores in thoracotomy patients with thoracic epidural analgesia? Medicine. (2021) 100:e28010. doi: 10.1097/MD.0000000000028010
23. Ruiz-Tovar J, Albrecht E, Macfarlane A, Coluzzi F. The TAP block in obese patients: pros and cons. Minerva Anestesiol. (2019) 85:1024–31. doi: 10.23736/S0375-9393.19.13545-6
24. Kula AO, Riess ML, Ellinas EH. Increasing body mass index predicts increasing difficulty, failure rate, and time to discovery of failure of epidural anesthesia in laboring patients. J Clin Anesth. (2017) 37:154–8. doi: 10.1016/j.jclinane.2016.11.010
25. Elshazly M, El-Halafawy YM, Mohamed DZ, Wahab KAE, Mohamed TMK. The feasibility and efficacy of erector spinae plane block versus transversus abdominis plane block in laparoscopic bariatric surgery: a randomized comparative trial. Korean J Anesthesiol. (2022). doi: 10.4097/kja.22169. [Epub ahead of print].
26. Yang MMH, Hartley RL, Leung AA, Ronksley PE, Jetté N, Casha S, et al. Preoperative predictors of poor acute postoperative pain control: a systematic review and meta-analysis. BMJ Open. (2019) 9:e025091. doi: 10.1136/bmjopen-2018-025091
27. Tola YO, Chow KM, Liang W. Effects of non-pharmacological interventions on preoperative anxiety and postoperative pain in patients undergoing breast cancer surgery: a systematic review. J Clin Nurs. (2021) 30:3369–84. doi: 10.1111/jocn.15827
28. Álvarez-García C, Yaban Z. The effects of preoperative guided imagery interventions on preoperative anxiety and postoperative pain: a meta-analysis. Complement Ther Clin Pract. (2020) 38:101077. doi: 10.1016/j.ctcp.2019.101077
29. Chu LF, Angst MS, Clark D. Opioid-induced hyperalgesia in humans: molecular mechanisms and clinical considerations. Clin J Pain. (2008) 24:479–96. doi: 10.1097/AJP.0b013e31816b2f43
30. Chu LF, Clark DJ, Angst MS. Opioid tolerance and hyperalgesia in chronic pain patients after one month of oral morphine therapy: a preliminary prospective study. J Pain. (2006) 7:43–8. doi: 10.1016/j.jpain.2005.08.001
31. Lee M, Silverman SM, Hansen H, Patel VB, Manchikanti L. A comprehensive review of opioid-induced hyperalgesia. Pain Physician. (2011) 14:145–61. doi: 10.36076/ppj.2011/14/145
32. Kreutzwiser D, Tawfic QA. Methadone for pain management: a pharmacotherapeutic review. CNS Drugs. (2020) 34:827–39. doi: 10.1007/s40263-020-00743-3
Keywords: regional anesthesia (RA), race, ethnicity, postoperative pain, opioids
Citation: Owusu-Agyemang P, Feng L, Porche VH, Williams UU and Cata JP (2022) Race, ethnicity, and the use of regional anesthesia in cancer patients undergoing open abdominal surgery: A single-center retrospective cohort study. Front. Med. 9:950444. doi: 10.3389/fmed.2022.950444
Received: 29 June 2022; Accepted: 02 August 2022;
Published: 18 August 2022.
Edited by:
Shun Ming Chan, Tri-Service General Hospital, TaiwanReviewed by:
Yuhe Ke, Singapore General Hospital, SingaporeCopyright © 2022 Owusu-Agyemang, Feng, Porche, Williams and Cata. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pascal Owusu-Agyemang, cG9hZ3llbWFuZ0BtZGFuZGVyc29uLm9yZw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.