
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 06 July 2022
Sec. Nephrology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.948177
 Katharina Dörr1
Katharina Dörr1 Sebastian Hödlmoser1
Sebastian Hödlmoser1 Michael Kammer1,2
Michael Kammer1,2 Roman Reindl-Schwaighofer1
Roman Reindl-Schwaighofer1 Matthias Lorenz3
Matthias Lorenz3 Bianca Reiskopf1
Bianca Reiskopf1 Rahel Jagoditsch1
Rahel Jagoditsch1 Rodrig Marculescu4
Rodrig Marculescu4 Rainer Oberbauer1*
Rainer Oberbauer1*Secondary hyperparathyroidism in chronic kidney disease poses a major risk factor for vascular calcification and high bone turnover, leading to mineralization defects. The aim was to analyze the effect of active vitamin D and calcimimetic treatment on fibroblast growth factor 23 (FGF23), serum calcification propensity (T50), a surrogate marker of calcification stress and bone specific alkaline phosphatase (BAP) in hemodialysis. This is a subanalysis of a randomized trial comparing etelcalcetide vs. alfacalcidol in 62 hemodialysis patients for 1 year. We compared the change of BAP and serum calcification propensity between the two medications and assessed the influence of FGF23 change over time. We found no significant differences in the change of BAP or serum calcification propensity (T50) levels from baseline to study end between treatment arms (difference in change of marker between treatment with etelcalcetide vs. alfacalcidol: BAP : 2.0 ng/ml [95% CI-1.5,5.4], p = 0.3; T50: –15 min [95% CI –49,19], p = 0.4). Using FGF23 change over time, we could show that BAP levels at study end were associated with FGF23 change (–0.14 [95% CI –0.21, –0.08], p < 0.001). We did not observe the same association between FGF23 change and T50 (effect of FGF23 change on T50: 3.7 [95% CI –5.1, 12], p = 0.4; R2 = 0.07 vs. R2 = 0.06). No significant difference was found in serum calcification propensity (T50) values between treatment arms. FGF23 was not associated with serum calcification propensity (T50), but was negatively correlated with BAP underlying its role in the bone metabolism.
Clinical Trial Registration: [www.ClinicalTrials.gov], identifier [NCT03182699].
The substantially increased risk of cardiovascular morbidity and mortality in chronic kidney disease (CKD) is promoted by calcification of soft tissues and the vasculature (1). By the time patients reach dialysis, the prevalence and progression of vascular calcification (VC) rises rapidly (2). Secondary hyperparathyroidism (sHPT) is present in up to 80% of patients with end-stage kidney disease (ESKD) and poses a key risk factor for the initiation and development of VC as well as high bone turnover and bone mineral loss (3–5). Calcimimetic therapy is effective in lowering serum concentrations of fibroblast growth factor 23 (FGF23), which is a risk factor for left ventricular hypertrophy (LVH) and cardiovascular events in people with CKD (6, 7). Calcimimetics bind to the parathyroid calcium sensing receptor, causing a leftward shift in the set-point for calcium-regulated parathyroid hormone (PTH) secretion and therefore decrease the PTH concentration and serum calcium levels (8). Yu et al. showed that etelcalcetide (ETL) prevented VC in a rat model with CKD and sHPT (3). ETL can effectively reduce the levels of intact PTH, calcium, phosphate and FGF23 in ESRD patients (9, 10). In contrast, VC was found to be enhanced under the treatment with vitamin D analogs, which frequently led to hypercalcemia, hyperphosphatemia and increased levels of FGF23 (11, 12). Both calcimimetics and vitamin D analogs are common therapeutic options of sHPT.
The serum calcification propensity test (T50) was performed as a surrogate marker of calcification stress and mortality in CKD patients (13, 14). Bundy et al. showed that these patients exhibit a shortened time to serum calcification (15). Furthermore, Shoji et al. reported that treatment with ETL is more effective in increasing the T50 value indicating a lower serum calcification propensity than the selective vitamin D receptor activator maxacalcitol in hemodialysis patients (4).
Another marker of vascular calcification is the activity of bone specific alkaline phosphatase (BAP) (16). Andrukhova et al. from Vienna published that FGF23 suppresses the expression of osteocytic tissue non-specific AP in an autocrine/paracrine manner. This contributes to the mineralization defect, which is one of the hallmarks of CKD-mineral and bone disorder (MBD) (17, 18).
We recently performed a randomized, controlled trial on hemodialysis patients with sHPT, confirming the suppression of FGF23 by calcimimetic treatment with ETL and its increase under alfacalcidol (ALFA) (19). In the present study we sought to evaluate the effect of the study medication on markers of calcification and bone turnover.
The primary objective of the study was to elucidate, whether ETL vs. ALFA treatment differently effect the serum calcium propensity determined by serum calcification propensity test (T50) and the bone turnover marker BAP. In addition, the effect of FGF23 on these two parameters was analyzed.
Data were obtained from the randomized, controlled, single-blinded trial of people on maintenance hemodialysis with sHPT and LVH. Sixty-two patients were randomized in a 1:1 ratio to intravenous ETL or ALFA for 1 year. We enrolled patients who were on dialysis treatment between 3 and 36 months with sHPT. The trial was approved by the ethics committee of the Medical University of Vienna [MUV (EK # 1127/2017)], the national regulatory authorities (AGES # 10087746) and conducted in accordance with the principles of the Declaration of Helsinki. Details on the trial design, including a complete list of inclusion and exclusion criteria were published previously (19–21).
Biochemical data were collected prior to the hemodialysis session and before the start of ETL or ALFA treatment. For the serum calcification propensity (T50) analysis two serum samples per patient were collected, one at baseline and one after 52 weeks of treatment. In case of discontinuation of the trial prior to 1 year, the second analysis was performed on the last day of treatment. The samples were stored at –80°C and shipped on dry ice to the Calciscon Laboratory in Switzerland where the calcification propensity, i.e., the conversion time from primary to secondary calciprotein particles was quantified (22). A Nephelostar nephelometer was used to detect the time-resolved changes of laser light scattering associated with the transformation.
BAP was measured at 9 timepoints during the trial from frozen serum probes (chemiluminescent immunoassay, DiaSorin®, measurement batched, duplicate, CV 7–8%). Intact PTH (electrochemiluminescence immunoassay, Roche®, measurement in real time, duplicate, CV < 1.7%), calcium (NM-BAPTA photometric test, Roche, measurement in real time, duplicate, CV ≤ 2%), phosphate (ammonium molybdate UV photometric test, Roche, measurement in real time, duplicate, CV 0.9%), 25-hydroxyvitamin D [25(OH)D] and 1,25-dihydroxyvitamin D [1.25(OH)2D] (chemiluminescent immunoassay, Roche®, measurement batched, duplicate, CV 7–9% for 25-OH and 5.9% for 1.25OH) were measured every 2 weeks in the first 10 weeks, followed by measurements every 4 weeks. Serum calcium was corrected for albumin (bromcresol green method CV ≤ 1.8%) (23). Intact FGF23 (chemiluminescent immunoassay, DiaSorin®, measurement batched, duplicate, CV ≤ 3.8%). And αKlotho (FluoBolt™, Fianostics, batched, duplicate, CV ≤ 8%) were measured in 8-week-intervals.
We summarized baseline characteristics of the study cohort using median (IQR) for continuous variables and counts (%) for categorical variables. To visualize biomarker trajectories over time, we depicted boxplots for each treatment arm at baseline and in 12-week increments. For each interval after baseline, the boxplots represent all data in the preceding 12 weeks. We added non-parametric smooth curves (from the “loess” function in R) to the boxplots to underline the mean biomarker trajectories over time.
To assess the effect of the treatment (ETL vs. ALFA) on BAP and serum calcification propensity (T50), we used ANCOVA models for each marker to estimate the difference between baseline and study end, adjusted for the respective baseline value and the two stratification factors, i.e., residual kidney function (≥ 500 mL/d vs. < 500 mL/d) and dialysis center (MUV vs. WDZ). To model the effect of FGF23 on BAP and serum calcification propensity (T50), we first fitted a linear mixed effects regression model to estimate the change of FGF23 over time per patient. Due to its skew distribution, FGF23 entered the model on a log2 scale. The model included an intercept and slope as fixed effects, as well as a random intercept and slope per patient. We interpreted the sum of the fixed and random slope parameter as FGF23 change per time unit. This approach allowed us to include all available FGF23 measurements to estimate FGF23 change over time per patient. In a second step, we modeled biomarker levels at the end of the study by two linear regression models for BAP and serum calcification propensity (T50), respectively. The first model included FGF23 change and baseline BAP/serum calcification propensity (T50) as covariates, in the second model we excluded FGF23 change. We then compared the parameter estimates as well as explained variance (R2) of the two approaches to assess the influence of FGF23 change on model fit.
For all models, we conducted distribution and residual analysis to check for model assumptions and possible outliers. Due to some very high outliers, we clipped the BAP and serum calcification propensity (T50) levels at baseline and at study end at the respective 97.5% quantiles. In all analyses, we regarded two-sided P-values < 0.05 as significant. Because of the descriptive nature of this subanalysis of a randomized controlled trail, we did not adjust any P-values for multiple testing. All statistical analysis was conducted using R 4.0.4.
The study cohort included 62 patients from the original trial, 32 of whom were treated with ETL and another 30 with ALFA. Table 1 summarizes the study cohort characteristics at baseline and shows, that the two treatment groups were well balanced at the beginning of the two treatment arms. A detailed description of the study cohort and the original study design are published elsewhere (19, 20).
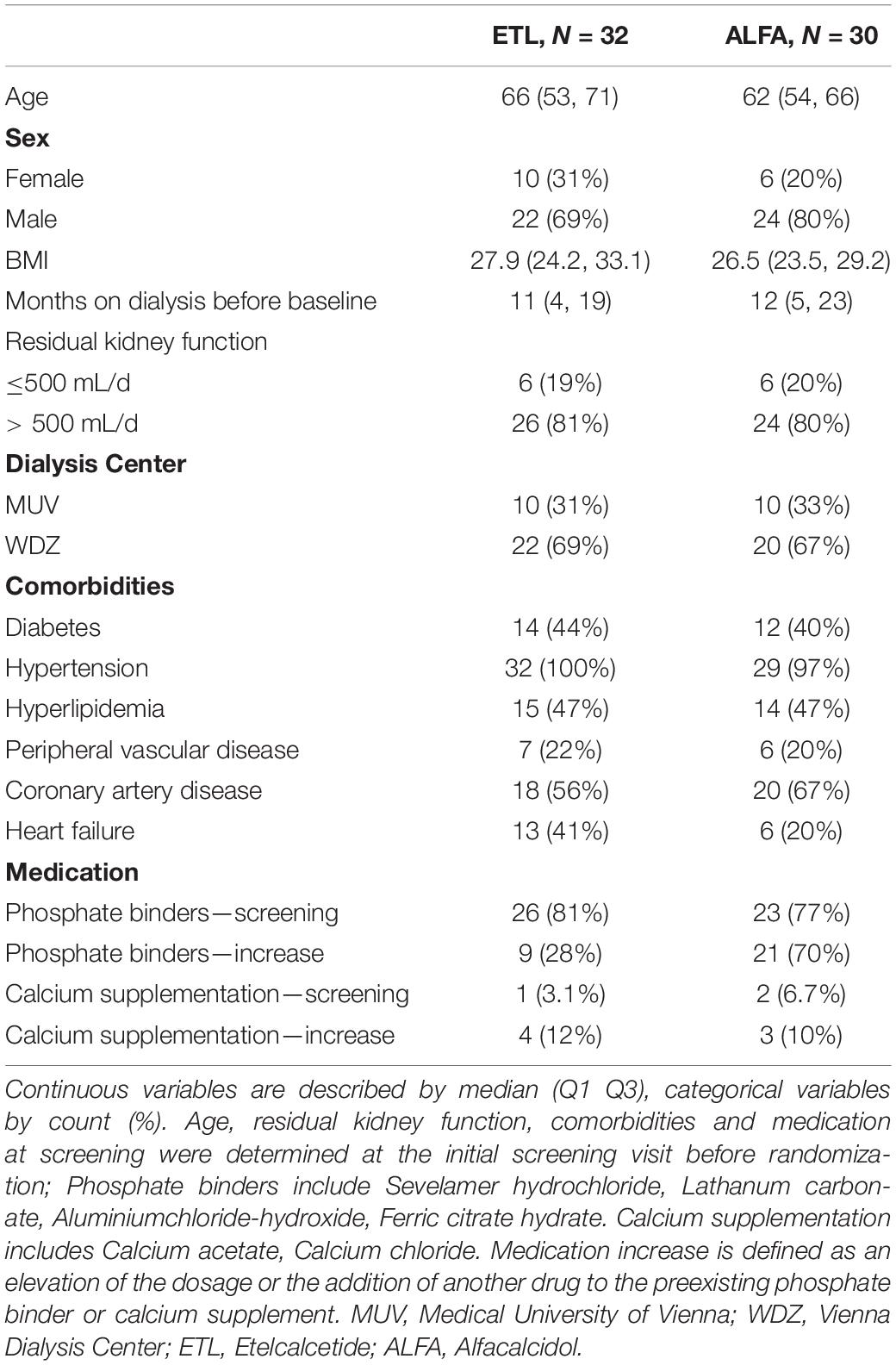
Table 1. Study population characteristics at baseline in the two treatment arms, etelcalcetide and vitamin D.
The serum levels of FGF23 (pg/ml), iPTH (ng/l), calcium (mmol/l), phosphate (mmol/l), BAP (ng/ml), klotho (ng/ml), 1.25-OH2-Vitamin D (pg/ml), and 25-OH-Vitamin D (nmol/l) at baseline and over time is provided in Figure 1. Mean baseline levels were similar for all biomarkers. Trajectories of 1.25-OH2-Vitamin D, calcium and FGF23 diverged over time in the two treatment groups, while the other markers did show a similar course in the ETL and ALFA group. Ten patients dropped out of the trial before completing 1 year of treatment, five in each treatment arm. Laboratory analyses were performed using probes from all 62 patients. In case of drop-out, the last collected probe was used for serum calcification propensity (T50) measurement.
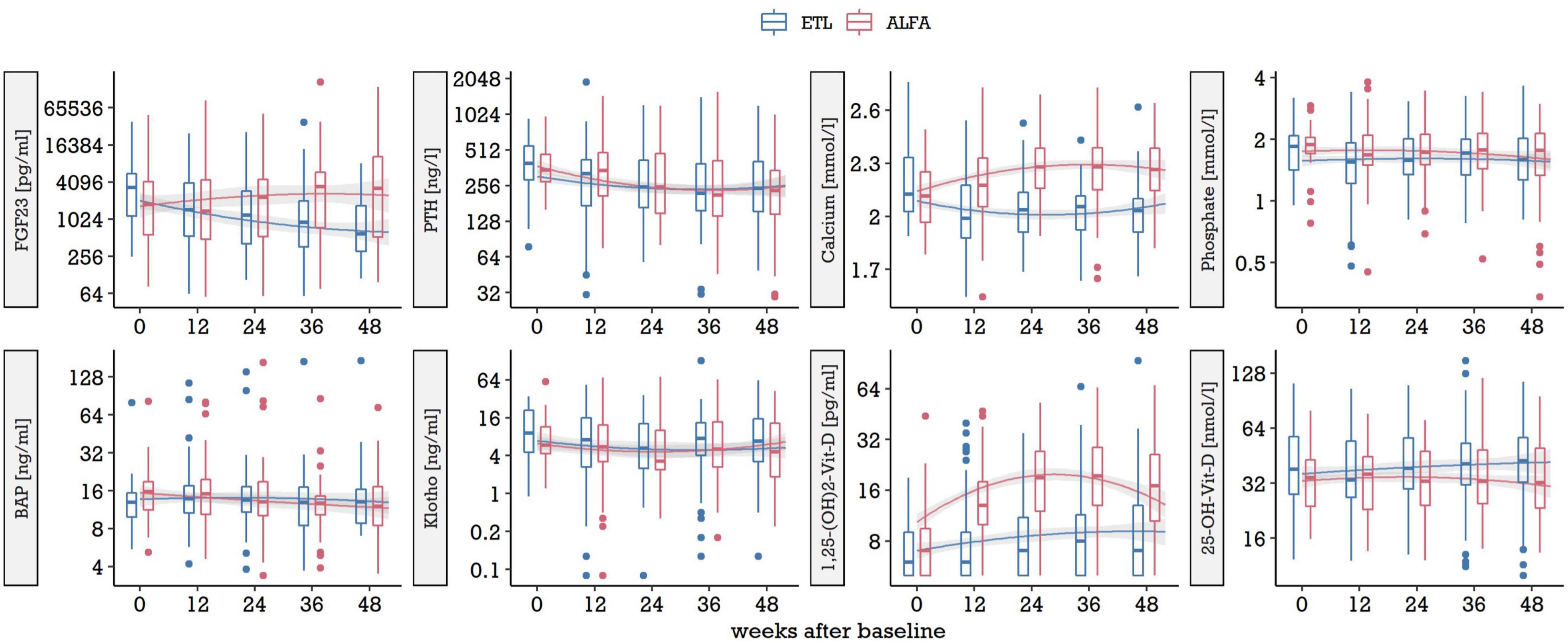
Figure 1. Biomarker levels at baseline and over time in the two treatment arms, ETL and ALFA. The boxplots in 12-week-increments represent all data in the preceding 12 weeks, by treatment, on a log2 scale. Trajectories are represented by non-parametric smoothing (loess curves). ETL, Etelcalcetide; ALFA, Alfacalcidol.
We found no significant differences in the change of BAP or serum calcification propensity (T50) with respect to the two treatment arms, ETL and ALFA. Figure 2 compares BAP and serum calcification propensity (T50) at baseline and at study end for both medications, after clipping very high outliers at the 97.5% quantile (3 observations of BAP, 4 observations of T50). Median [IQR] change in BAP throughout the study period was 0.05 [–3.17, 2.75] under ETL treatment and –1.85 [–6.15, –0.02] in the ALFA group. In serum calcification propensity (T50), median change amounted to –1.5 [–59.25, 56.25] in ETL treatment and 19.9 [–32.25, 77.25] in ALFA treatment. We assessed differences between baseline and study end in ANCOVA models, in which we modeled the adjusted change in marker levels per patient. The models were summarized in Table 2. Both ANCOVA models showed that after controlling for baseline value and randomization factors, there were no significant differences in BAP and serum calcification propensity (T50) change between the treatment arms (estimated difference in change of BAP, ETL vs. ALFA: 2.0 ng/ml [95% CI –1.5, 5.4], p = 0.3; estimated difference in T50, ETL vs. ALFA: –15 min [95% CI –49, 19], p = 0.4).
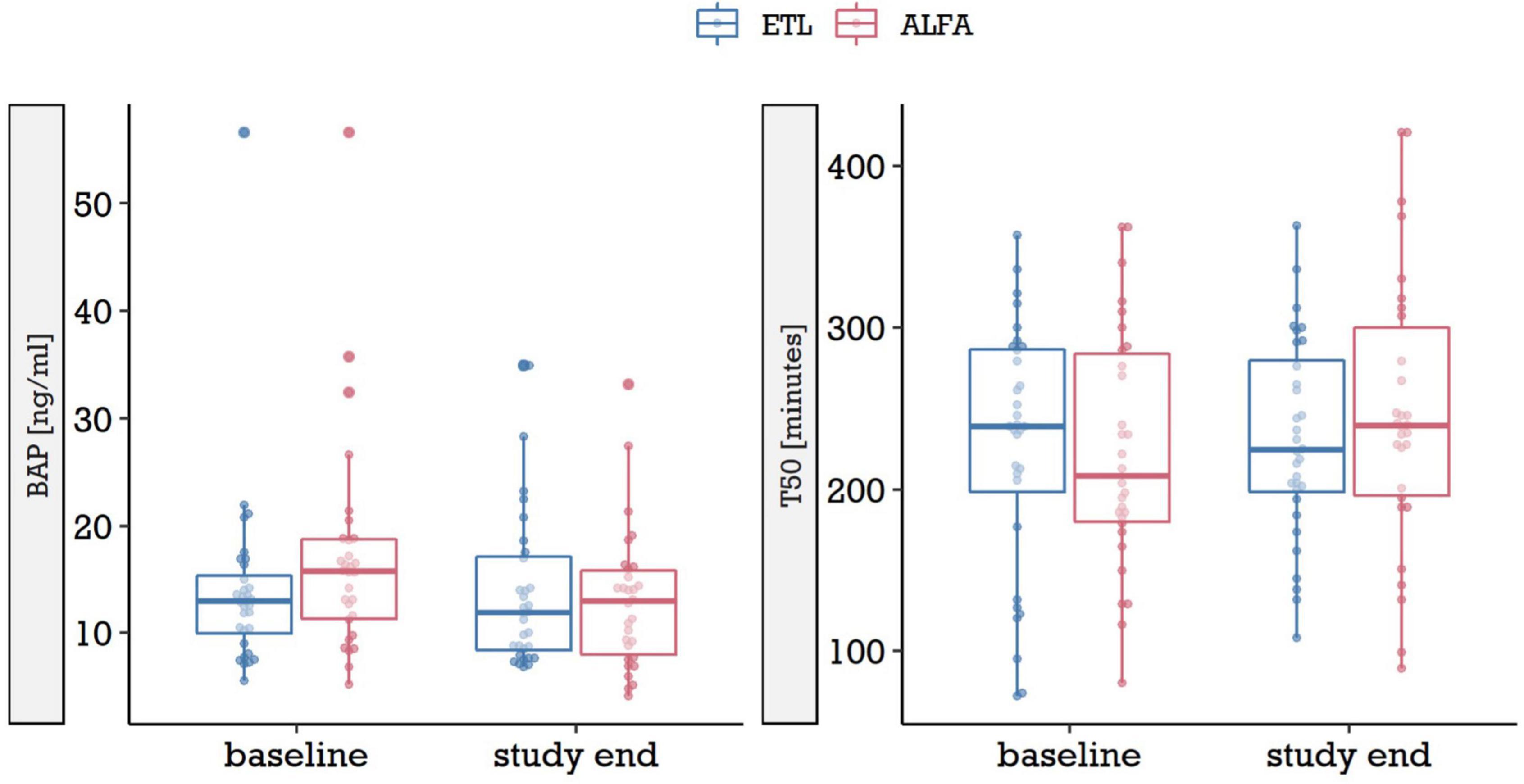
Figure 2. BAP and serum calcification propensity score test (T50) at baseline and study end in the two treatment arms, ETL and ALFA. Due to outliers with very high levels, for each marker and point in time the data was clipped at the respective 97.5% quantile, i.e., levels above it were set to the 97.5% quantile [3 observations in BAP, 4 in serum calcification propensity score test (T50)]. ETL, Etelcalcetide; ALFA, Alfacalcidol.
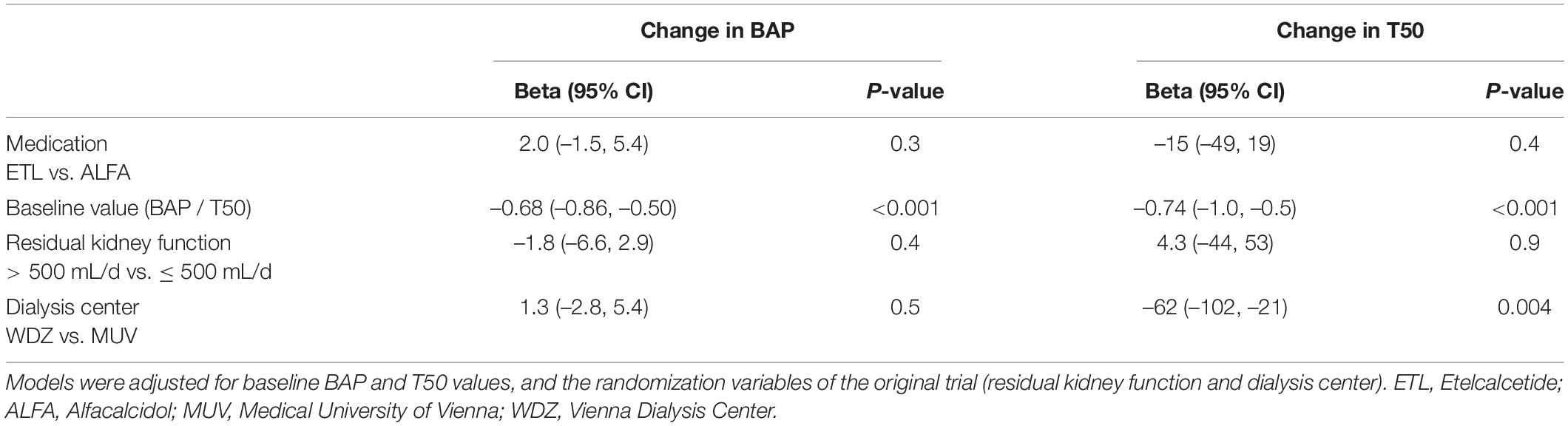
Table 2. ANCOVA models for change in BAP and serum calcification propensity score test (T50) from baseline to study end.
We found indications that FGF23 change over time was associated with BAP at study end, but not with serum calcification propensity (T50). The linear mixed model to assess FGF23 change per patient delivered a marginal R squared of and a conditional R squared of The latter seems, in comparison to ordinary linear regression, rather high. However, for a mixed effects model, denotes the explained variance when the (population level) fixed effects as well as the (individual level) random effects are taken into account. This flexibility per individual contributes to the high goodness-of-fit. While a high is of limited value for prediction purposes, in the context of this study, were we used the mixed model to describe a trait per individual, it shows that the approach is adequate to assess FGF23 change per patient.
In Table 3, we summarized the models for BAP and serum calcification propensity (T50) at study end with and without FGF23 change as covariate. Again, we clipped the baseline and study end levels at the respective 97.5% quantiles. We could show that the estimated effect of FGF23 change on BAP at study end was significant (–0.14 [95% CI –0.21, –0.08], p < 0.001) and that the inclusion of FGF23 change into the model substantially increased model fit (R2 = 0.27 for model without, and R2 = 0.46 for model with FGF23 change as covariate). Interpretation of these regression coefficients is not straight forward, since the outcome (BAP) was modeled on a log2 scale. When transformed to the original scale, the additive regression coefficients turn into multiplicative factors. This means that for every unit step of FGF23 change [which denotes the change of log2(FGF23)], BAP levels are multiplied (or divided, when the covariate is reduced) by a factor of 2–0.14 = 0.91. We found no indication for an effect of FGF23 change on serum calcification propensity test (T50), as neither the regression coefficient was significant, nor did the model performance decrease when FGF23 change was excluded (effect of FGF23 change on T50: 3.7 [95% CI –5.1, 12], p = 0.4; R2 = 0.06 in the full model vs. R2 = 0.07 when FGF23 was excluded).
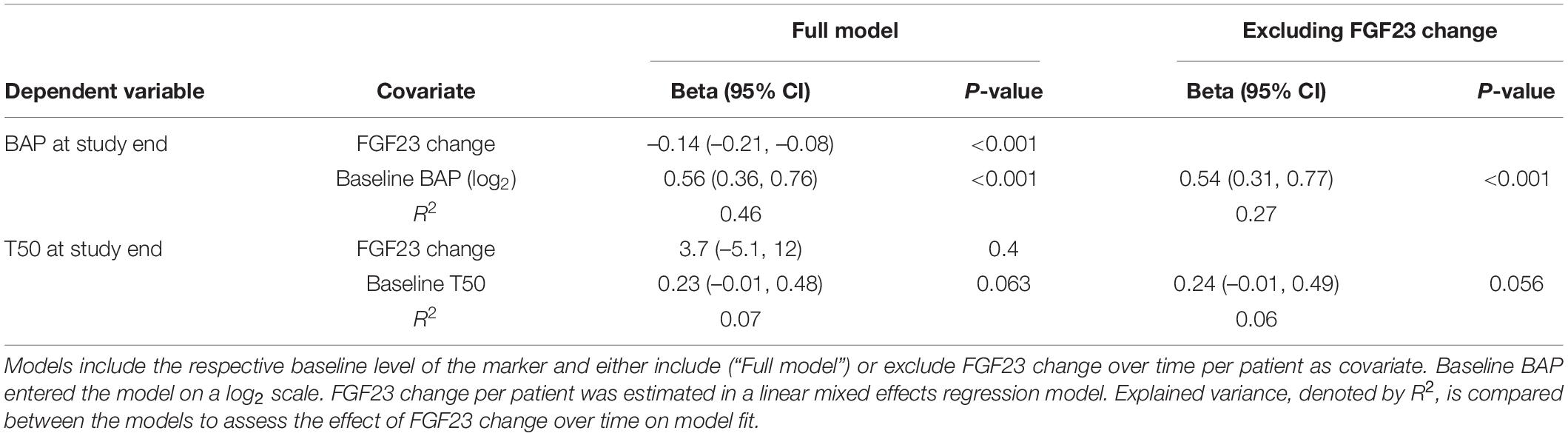
Table 3. Linear regression models for BAP and serum calcification propensity score test (T50) at study end.
In this trial the effects of ETL and ALFA on serum calcification propensity test (T50) and BAP were compared in hemodialysis patients with sHPT. In addition, the association of FGF23 with these markers was analyzed. We found no significant differences between change in T50 between medication groups after 1 year of treatment. Mean T50 increased under ALFA while it decreased under ETL, which stands in contrasts to the results by Shoji et al.
The change in FGF23, i.e., its decrease under ETL and increase under ALFA, was also not associated with serum calcification propensity (T50). In Shoji’s trial both ETL and vitamin D increased T50, while its increase was more effective under ETL. The authors explained this between-group difference by the different effects of the drugs on calcium and phosphate levels, which serum calcification propensity test (T50) itself was reported to be inversely correlated with in the past (24). In our trial, serum calcium levels also decreased under calcimimetic treatment and increased under ALFA therapy. However, we showed similar courses of phosphate levels in both treatment groups. As reported before, this unexpected finding could be explained by an increased use of phosphate binder therapy in the ALFA group in our study. In Shoji’s trial on the other hand, phosphate trajectories were lower in the ETL group. In addition, even though the proportion of patients under phosphate binder therapy was comparable between groups at baseline, the graph showing the changes in the medications during the course of the trial indicate a slightly higher use of phosphate binders in the ETL group, possibly explaining the differences between trials in phosphate levels under the same therapy. It is also important to point out, that the serum calcification propensity values in Shoji’s trial were much lower than those reported for CKD patients from western countries. The explanation for this occurrence remains unclear. In addition, the trial used different target ranges of sHPT parameters. Especially in the case of iPTH, the target range was 60–240 ng/l as recommended by the clinical practice guideline for the management of CKD-MBD by the Japanese Society for Dialysis Therapy and patients were included when iPTH was above 240 ng/l, which is lower in comparison to our trial (inclusion if iPTH > 300 ng/l, target range between 100 and 300 ng/l). Furthermore, concomitant therapy differed, allowing for oral calcimimetic use in the vitamin D group, which was prohibited in our trial. As the authors correctly point out, the results of the Japanese study may not be applicable to patients in other countries.
In the present study, we showed an inverse association of FGF23 with BAP. So far, the isoenzyme BAP, which comprises approximately 50% of total circulating alkaline phosphatase (AP) is mostly known as a bone turnover marker in CKD-MBD patients reflecting the bone formation in skeletal tissue (25–27). High levels of BAP were shown to be strongly associated with mortality in dialysis patients (28). In animal models FGF23 suppresses tissue non-specific alkaline phosphatase (TNAP) transcription and also phosphate production in osteoblastic cells through FGF receptor-3 independent of klotho, leading to a bone mineralization defect in an autocrine/paracrine manner (29, 30). A trial by Slouma et al. showed that both FGF23 and BAP can be used as markers of bone fragility in hemodialysis patients (31). Regarding VC, higher BAP was significantly associated with its presence in hand arteries in a trial with 167 hemodialysis patients (32). It was also positively correlated with abdominal aortic calcification in the same patient collective (33). Total AP was shown to be lowered under oral calcimimetic in the past, but BAP was not assessed in that analysis in hemodialysis patients (34).
There are some limitations in our study. First, this is a subanalysis of a randomized controlled trial, powered to compare the effects of ETL and ALFA on LVH in hemodialysis, not to detect a difference of the study medication or FGF23 on calcification and bone turnover markers. Second, it also did not compare the effects of the study drugs on clinical hard end points but rather on surrogate biomarkers of bone and mineral disorders. Trial participants were also not regularly investigated by skeletal imaging. Third, considering that the per protocol analysis of the trial by Shoji et al. included a much higher number of participants (n = 319), our trial had a comparatively low sample size.
The strengths of the trial, however, include its prospective, randomized design, a completed follow-up and the use of intravenously administered drugs, avoiding the issue of non-adherence, which is known to be very high especially for calcimimetics in hemodialysis patients (35). In addition, the T50 test which was used in this trial was previously shown to accurately assess the formation rate of calciprotein particles and therefore reflect the calcification risk in ESKD and was also shown to be associated with mortality in this collective (24).
In conclusion, this study showed that treatment with ETL was not effective in decreasing the serum calcification propensity in comparison with ALFA and unrelated to BAP change. FGF23 was associated with BAP, but not with serum calcification propensity (T50). The translation of our findings into clinical end points necessitates a different trial setting with a much higher number of patients and a longer follow-up period. From our experience, the use of calcimimetics in hemodialysis patients is a safe, effective and well tolerated option for the treatment of sHPT. We would recommend the use of intravenous calcimimetics and close monitoring of calcium levels.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the Medical University of Vienna [MUV (EK # 1127/2017)]. The patients/participants provided their written informed consent to participate in this study.
KD, RO, RR-S, and SH were responsible for the conceptualization and methodology of the trial. KD was tasked with the investigation, including data collection, with support by ML, BR, and RJ. SH and MK were assigned with the formal analysis and software. RM was responsible for laboratory analysis. Writing of the original draft was performed by KD and reviewed and edited by the co-authors. All authors contributed to the article and approved the submitted version.
This study was sponsored by the Medical University of Vienna and by an unrestricted investigator-initiated research grant from Amgen (IIP #20167811).
RO reports grants from Amgen during the conduct of the study. In addition, RO, KD, and RR-S have a patent “Methods of treating left ventricle hypertrophy” pending.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank the nursing staff of the General Hospital of Vienna and Vienna Dialysis Center for their assistance in the blood sample collections from subjects. In addition, we thank the lab technicians of the Department of Laboratory Medicine (Medical University of Vienna) and for their assistance in study procedures.
AP, alkaline phosphatase; BAP, bone specific alkaline phosphatase; CKD, chronic kidney disease; CKD-MBD, chronic kidney disease – mineral and bone disorder; ESKD, end-stage kidney disease; EtECAR-HD, Effect of etelcalcetide on cardiac hypertrophy in hemodialysis patients–a randomized controlled trial; ETL, etelcalcetide; FGF23, fibroblast growth factor 23; LVH, left ventricular hypertrophy; MUV, Medical University of Vienna; iPTH, intact parathyroid hormone; sHPT, secondary hyperparathyroidism; VC, vascular calcification; WDZ, Vienna dialysis center.
1. Paloian NJ, Giachelli CM. A current understanding of vascular calcification in CKD. Am J Physiol Ren Physiol. (2014) 15:F891–900. doi: 10.1152/ajprenal.00163.2014
2. Shroff R, Long DA, Shanahan C. Mechanistic insights into vascular calcification in CKD. J Am Soc Nephrol. (2013) 2:179–89. doi: 10.1681/ASN.2011121191
3. Yu L, Tomlinson JE, Alexander ST. Etelcalcetide, a novel calcimimetic, prevents vascular calcification in a rat model of renal insufficiency with secondary hyperparathyroidism. Calcif Tissue Int. (2017) 101:641–53. doi: 10.1007/s00223-017-0319-7
4. Shoji T, Nakatani S, Kabata D, Mori K, Shintani A, Emoto M. Comparative effects of etelcalcetide and maxacalcitol on serum calcification propensity in secondary hyperparathyroidism a randomized clinical trial. Clin J Am Soc Nephrol. (2021) 4:599–612. doi: 10.2215/CJN.16601020
5. Levin A, Bakris GL, Molitch M, Smulders M, Tian J, Williams LA, et al. Prevalence of abnormal serum vitamin D, PTH, calcium, and phosphorus in patients with chronic kidney disease: results of the study to evaluate early kidney disease. Kidney Int. (2007) 71:31–8. doi: 10.1038/sj.ki.5002009
6. Scialla JJ, Xie H, Rahman M. Fibroblast growth factor-23 and cardiovascular events in CKD. Clin J Am Soc Nephrol. (2014) 25:349–60. doi: 10.1681/ASN.2013050465
7. Moe SM, Chertow GM, Parfrey PS, Kubo Y, Block GA, Correa-Rotter R, et al. Cinacalcet, fibroblast growth factor-23, and cardiovascular disease in hemodialysis: the evaluation of cinacalcet HCL therapy to lower cardiovascular events (EVOLVE) trial. Circulation. (2015) 132:27–39. doi: 10.1161/CIRCULATIONAHA.114.013876
8. Nemeth EF, Bennett SA. Tricking the parathyroid gland with novel calcimimetic agents. Nephrol Dial Transplant. (1998) 8:1923–5. doi: 10.1093/ndt/13.8.1923
9. Block GA, Bushinsky DA. Effect of etelcalcetide vs placebo on serum parathyroid hormone in patients receiving hemodialysis with secondary hyperparathyroidism: two randomized clinical trials. J Am Med Assoc. (2017) 317:146–55. doi: 10.1001/jama.2016.19456
10. Block GA, Bushinsky DA. Effect of etelcalcetide vs cinacalcet on serum parathyroid hormone in patients receiving hemodialysis with secondary hyperparathyroidism. J Am Med Assoc. (2017) 17:156–64. doi: 10.1001/jama.2016.19468
11. Wetmore JB, Gurevich K, Spraque S, Da Roza G, Buerkert J, Reiner M, et al. A randomized trial of cinacalcet versus vitamin d analogs as monotherapy in secondary hyperparathyroidism (PARADIGM). Clin J Am Soc Nephrol. (2015) 10:1031–40. doi: 10.2215/CJN.07050714
12. Briese S, Wiesner S, Will JC, Lembcke A, Opgen-Rhein B, Nissel R, et al. Arterial and cardiac disease in young adults with childhood-onset end-stage renal disease-impact of calcium and vitamin D therapy. Nephrol Dial Transplant. (2006) 21:1906–14. doi: 10.1093/ndt/gfl098
13. Bojic M, Bielesz B, Cejka D, Gerit-Schernthaner H, Höbaus C. Calcification propensity in serum and cardiovascular outcome in peripheral artery disease. Thromb Haemost. (2021) doi: 10.1055/s-0041-1736444
14. Eelderink C, Velde-Keyzer CA, Frenay AR, Vermeulen EA, Bachtler M, Aghagolzadeh P, et al. Serum calcification propensity and the risk of cardiovascular and all-cause mortality in the general population: the PREVEND study. Arterioscler Thromb Vasc Biol. (2020) 8:1942–51. doi: 10.1161/ATVBAHA.120.314187
15. Bundy JD, Cai X, Scialla JJ, Dobre MA, Chen J, Hsu CY, et al. Serum calcification propensity and coronary artery calcification among patients with CKD: the CRIC (chronic renal insufficiency cohort) study. Am J Kidney Dis. (2019) 6:806–14. doi: 10.1053/j.ajkd.2019.01.024
16. Iba K, Takada J, Yamashita T. The serum level of bone-specific alkaline phosphatase activity is associated with aortic calcification in osteoporosis patients. J Bone Miner Metab. (2004) 6:594–6.
17. Andrukhova O, Schüler C, Bergow C, Petric A, Erben RG. Augmented fibroblast growth factor-23 secretion in bone locally contributes to impaired bone mineralization in chronic kidney disease in mice. Front Endocrinol. (2018) 9:311. doi: 10.3389/fendo.2018.00311
18. Murali SK, Andrukhova O, Clinkenbeard EL, White KE, Erben RG. Excessive osteocytic fgf23 secretion contributes to pyrophosphate accumulation and mineralization defect in hyp mice. PLoS Biol. (2016) 4:e1002427. doi: 10.1371/journal.pbio.1002427
19. Dörr K, Kammer M, Reindl-Schwaighofer R, Lorenz M, Prikoszovich T, Marculescu R, et al. Randomized trial of etelcalcetide for cardiac hypertrophy in hemodialysis. Circ Res. (2021) 11:1616–25. doi: 10.1161/CIRCRESAHA.120.318556
20. Dörr K, Kammer M, Reindl-Schwaighofer R, Lorenz M, Loewe C, Marculescu R, et al. Effect of etelcalcetide on cardiac hypertrophy in hemodialysis patients: a randomized controlled trial (ETECAR-HD). Trials. (2019) 20:601.
21. Dörr K, Kammer M, Reindl-Schwaighofer R, Lorenz M, Marculescu R, Poglitsch M, et al. The effect of FGF23 on cardiac hypertrophy is not mediated by systemic renin-angiotensin- aldosterone system in hemodialysis. Front Med. (2022) 9:878730. doi: 10.3389/fmed.2022.878730
22. Pasch A, Farese S, Gräber S, Wald J, Richtering W, Floege J, et al. Nanoparticle-based test measures overall propensity for calcification in serum. J Am Soc Nephrol. (2012) 23:1744–52. doi: 10.1681/ASN.2012030240
23. Figge J, Jabor A, Kazda A, Fencl V. Anion gap and hypoalbuminemia. Crit Care Med. (1998) 26:1807–10. doi: 10.1097/00003246-199811000-00019
24. Pasch A, Block GA, Bachtler M, Smith ER, Jahnen-Dechent W, Arampatzis S, et al. Blood calcification propensity, cardiovascular events, and survival in patients receiving hemodialysis in the EVOLVE trial. Clin J Am Soc Nephrol. (2017) 12:315–22. doi: 10.2215/CJN.04720416
25. Sardiwal S, Gardham C, Coleman AE, Stevens PE, Delaney MP, Lamb EJ. Bone-specific alkaline phosphatase concentrations are less variable than those of parathyroid hormone in stable hemodialysis patients. Kidney Int. (2012) 1:100–5. doi: 10.1038/ki.2012.77
26. Bergman A, Qureshi AR, Haarhaus M, Lindholm B, Barany P, Heimburger O, et al. Total and bone-specific alkaline phosphatase are associated with bone mineral density over time in end-stage renal disease patients starting dialysis. J Nephrol. (2017) 2:255–62. doi: 10.1007/s40620-016-0292-7
27. Haarhaus M, Gilham D, Kulikowski E, Magnusson P, Kalantar-Zadeh K. Pharmacologic epigenetic modulators of alkaline phosphatase in chronic kidney disease. Curr Opin Nephrol Hypertens. (2020) 29:4–15. doi: 10.1097/MNH.0000000000000570
28. Drechsler C, Verduijn M, Pilz S, Krediet RT, Dekker FW, Wanner C, et al. Bone alkaline phosphatase and mortality in dialysis patients. Clin J Am Soc Nephrol. (2011) 7:1752–9. doi: 10.2215/CJN.10091110
29. Murali SK, Roschger P, Zeitz U, Klaushofer K, Andrukhova O, Erben RG. FGF23 regulates bone mineralization in a 1,25(OH)2 D3 and klotho-independent manner. J Bone Miner Res. (2016) 1:129–42. doi: 10.1002/jbmr.2606
30. Beck-Nielsen SS, Mughal Z, Haffner D, Nilsson O, Levtchenko E, Ariceta G, et al. FGF23 and its role in X-linked hypophosphatemia-related morbidity. Orohanet J Rare Dis. (2019) 14:58. doi: 10.1186/s13023-019-1014-8
31. Slouma M, Aissaoui T, Abbes M, Bahlous A, Laadhar L, Smaoui W, et al. New markers of bone fragility in hemodialysis patients: a monocentric study. J Clin Densitom. (2021) 24:22–7. doi: 10.1016/j.jocd.2020.11.002
32. Ishimura E, Okuno S, Okazaki H, Norimine K, Yamakawa K, Yamakawa T, et al. Significant association between bone-specific alkaline phosphatase and vascular calcification of the hand arteries in male hemodialysis patients. Kidney Blood Press Res. (2014) 4:299–307. doi: 10.1159/000355807
33. Yan J, Li L, Zhang M, Cai H, Ni Z. Circulating bone-specific alkaline phosphatase and abdominal aortic calcification in maintenance hemodialysis patients. Biomark Med. (2018) 12:1231–9. doi: 10.2217/bmm-2018-0089
34. Belozeroff V, Goodman WG, Ren L, Kalantar-Zadeh K. Cinacalcet lowers serum alkaline phosphatase in maintenance hemodialysis patients. Clin J Am Soc Nephrol. (2009) 4:673–9. doi: 10.2215/CJN.03790808
Keywords: calcimimetic, vitamin D, calcification, bone turn over, hemodialysis
Citation: Dörr K, Hödlmoser S, Kammer M, Reindl-Schwaighofer R, Lorenz M, Reiskopf B, Jagoditsch R, Marculescu R and Oberbauer R (2022) Bone Specific Alkaline Phosphatase and Serum Calcification Propensity Are Not Influenced by Etelcalcetide vs. Alfacalcidol Treatment, and Only Bone Specific Alkaline Phosphatase Is Correlated With Fibroblast Growth Factor 23: Sub-Analysis Results of the ETACAR-HD Study. Front. Med. 9:948177. doi: 10.3389/fmed.2022.948177
Received: 19 May 2022; Accepted: 20 June 2022;
Published: 06 July 2022.
Edited by:
Chia-Ter Chao, National Taiwan University Hospital, TaiwanReviewed by:
Emanuel Zitt, Landeskrankenhaus Feldkirch, AustriaCopyright © 2022 Dörr, Hödlmoser, Kammer, Reindl-Schwaighofer, Lorenz, Reiskopf, Jagoditsch, Marculescu and Oberbauer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rainer Oberbauer, cmFpbmVyLm9iZXJiYXVlckBtZWR1bml3aWVuLmFjLmF0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.