 Chung-Feng Liu1†Chao-Ming Hung2,3†Shian-Chin Ko4Kuo-Chen Cheng5Chien-Ming Chao6,7Mei-I Sung4Shu-Chen Hsing4Jhi-Joung Wang8,9Chia-Jung Chen10Chih-Cheng Lai11Chin-Ming Chen12*
Chung-Feng Liu1†Chao-Ming Hung2,3†Shian-Chin Ko4Kuo-Chen Cheng5Chien-Ming Chao6,7Mei-I Sung4Shu-Chen Hsing4Jhi-Joung Wang8,9Chia-Jung Chen10Chih-Cheng Lai11Chin-Ming Chen12* Chong-Chi Chiu2,13,14,15*
Chong-Chi Chiu2,13,14,15*- 1Department of Medical Research, Chi Mei Medical Center, Tainan, Taiwan
- 2Department of General Surgery, E-Da Cancer Hospital, Kaohsiung, Taiwan
- 3College of Medicine, I-Shou University, Kaohsiung, Taiwan
- 4Department of Respiratory Therapy, Chi Mei Medical Center, Tainan, Taiwan
- 5Department of Internal Medicine, Chi Mei Medical Center, Tainan, Taiwan
- 6Department of Intensive Care Medicine, Chi Mei Medical Center, Liouying, Taiwan
- 7Department of Dental Laboratory Technology, Min-Hwei College of Health Care Management, Liouying, Taiwan
- 8Department of Anesthesiology, Chi Mei Medical Center, Tainan, Taiwan
- 9Department of Anesthesiology, National Defense Medical Center, Taipei, Taiwan
- 10Department of Information Systems, Chi Mei Medical Center, Tainan, Taiwan
- 11Division of Hospital Medicine, Department of Internal Medicine, Chi Mei Medical Center, Tainan, Taiwan
- 12Department of Intensive Care Medicine, Chi Mei Medical Center, Tainan, Taiwan
- 13School of Medicine, College of Medicine, I-Shou University, Kaohsiung, Taiwan
- 14Department of Medical Education and Research, E-Da Cancer Hospital, Kaohsiung, Taiwan
- 15Department of General Surgery, Chi Mei Medical Center, Tainan, Taiwan
Background: For the intensivists, accurate assessment of the ideal timing for successful weaning from the mechanical ventilation (MV) in the intensive care unit (ICU) is very challenging.
Purpose: Using artificial intelligence (AI) approach to build two-stage predictive models, namely, the try-weaning stage and weaning MV stage to determine the optimal timing of weaning from MV for ICU intubated patients, and implement into practice for assisting clinical decision making.
Methods: AI and machine learning (ML) technologies were used to establish the predictive models in the stages. Each stage comprised 11 prediction time points with 11 prediction models. Twenty-five features were used for the first-stage models while 20 features were used for the second-stage models. The optimal models for each time point were selected for further practical implementation in a digital dashboard style. Seven machine learning algorithms including Logistic Regression (LR), Random Forest (RF), Support Vector Machines (SVM), K Nearest Neighbor (KNN), lightGBM, XGBoost, and Multilayer Perception (MLP) were used. The electronic medical records of the intubated ICU patients of Chi Mei Medical Center (CMMC) from 2016 to 2019 were included for modeling. Models with the highest area under the receiver operating characteristic curve (AUC) were regarded as optimal models and used to develop the prediction system accordingly.
Results: A total of 5,873 cases were included in machine learning modeling for Stage 1 with the AUCs of optimal models ranging from 0.843 to 0.953. Further, 4,172 cases were included for Stage 2 with the AUCs of optimal models ranging from 0.889 to 0.944. A prediction system (dashboard) with the optimal models of the two stages was developed and deployed in the ICU setting. Respiratory care members expressed high recognition of the AI dashboard assisting ventilator weaning decisions. Also, the impact analysis of with- and without-AI assistance revealed that our AI models could shorten the patients’ intubation time by 21 hours, besides gaining the benefit of substantial consistency between these two decision-making strategies.
Conclusion: We noticed that the two-stage AI prediction models could effectively and precisely predict the optimal timing to wean intubated patients in the ICU from ventilator use. This could reduce patient discomfort, improve medical quality, and lower medical costs. This AI-assisted prediction system is beneficial for clinicians to cope with a high demand for ventilators during the COVID-19 pandemic.
Introduction
Mechanical ventilation (MV) is frequently applied in the intensive care unit (ICU). Approximately eight hundred thousand patients receive MV annually in the United States (1). Extubation decision is critical during an ICU stay. An early trial of the weaning process and successful extubation may lower the medical costs and ventilator-related complication rates. Besides, it could improve the patient’s prognosis (2–4). Therefore, after the recovery of the critical illness, clinicians should immediately prepare to liberate the patients from MV. Evaluation of an ICU patient’s fitness for weaning and subsequent extubation is objectively referred to the airway, respiratory, neurological parameters, etc. (5). Most of the times, liberation from MV requires three steps – readiness testing, weaning, and extubating and the process of MV liberation is dynamic and complicated. In daily practice, extubation is usually left to the discretion of the clinician (6); therefore, various protocols for ventilator weaning have been established and assessed to increase the extubation rate (7–18).
Despite following the recommended extubation process established in the American Thoracic Surgery weaning protocol, the failure rate still ranges from 10 to 15% of ICU patients in the United States (19). Truthfully, there has been no significant decrease in extubation failure in the past decades. Therefore, an advanced strategy is mandatory to increase the prediction accuracy (20). Several multivariate outcome prediction models have evolved in many aspects of health care research in these years. They include artificial neural networks (ANN), logistic regression (LR) models, random forest (RF) models, and support vector machines (SVM) (21–26). Machine learning (ML) is a subject of computer science that incorporates numerous components to empower the systems to learn from currently acquired data, predict the outcome, and make changes in action when faced with a new problem. Clinically, ML could increase the prediction rate of successful weaning from ventilatory support. The parameters considered in the prediction of successful weaning and extubation were based on literature (27–34) and clinical experience.
Many studies (35–38) have reported the usefulness of AI in the ICU, such as the early warning systems that predict the risk of physiological deterioration in acutely ill patients, the development of acute respiratory distress syndrome, the early development of sepsis and the pathogen that causes it, and clinical outcome and mortality. However, studies on the utility of AI in predicting the weaning and extubation process among critically ill patients requiring MV are limited (39–43), while those that explore AI’s capacity to predict the weaning timing for intubated patients are rare.
This study aims to develop an AI digital dashboard to remind the ICU clinicians of the optimal timing for weaning initiation, propose an individualized treatment recommendation, and assist in making extubation decisions. Data that can be conveniently collected were chosen as variables for building the prediction model, including patients’ characteristics and respiratory pattern parameters during spontaneous breathing trials (SBTs). A preliminary impact analysis was performed after AI assistance to predict successful extubation in ICU patients.
Materials and methods
Ethical consideration
This study was reviewed and accepted by the CMMC (IRB Serial No.: 10912-016). The process was performed according to the approved guidelines and regulations, and informed consent was waived from the patients because of the nature of our retrospective study.
Study design
The study flow chart is demonstrated in Figure 1. In the beginning, we established a professional team, including clinicians, respiratory therapists, data scientists, and information technology engineers, and held regular meetings and discussions. We retrospectively collected data from adult ventilated patients (≥20 years old) who stayed at the ICU of CMMC from January 2016 to December 2019. Patients who signed the DNR (Do not resuscitate) were excluded. According to clinical experience, if the try-weaning timing is appropriate, the success probability of the final complete weaning ventilator will also increase. Therefore, this study divided the complete assessment of ventilator use into two stages: (1) the try-weaning stage and (2) the complete weaning MV stage (Figure 2).
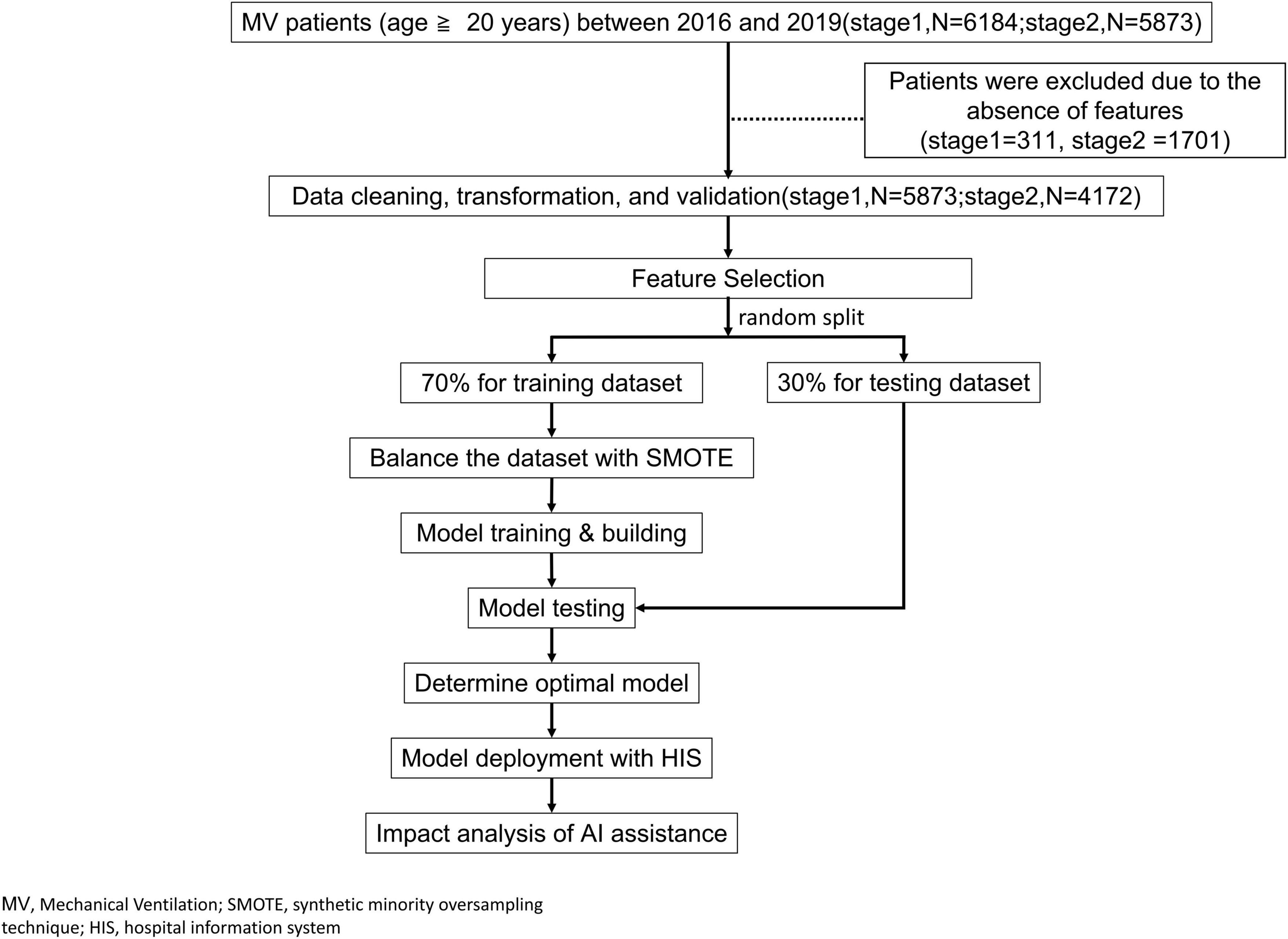
Figure 1. Study flow.
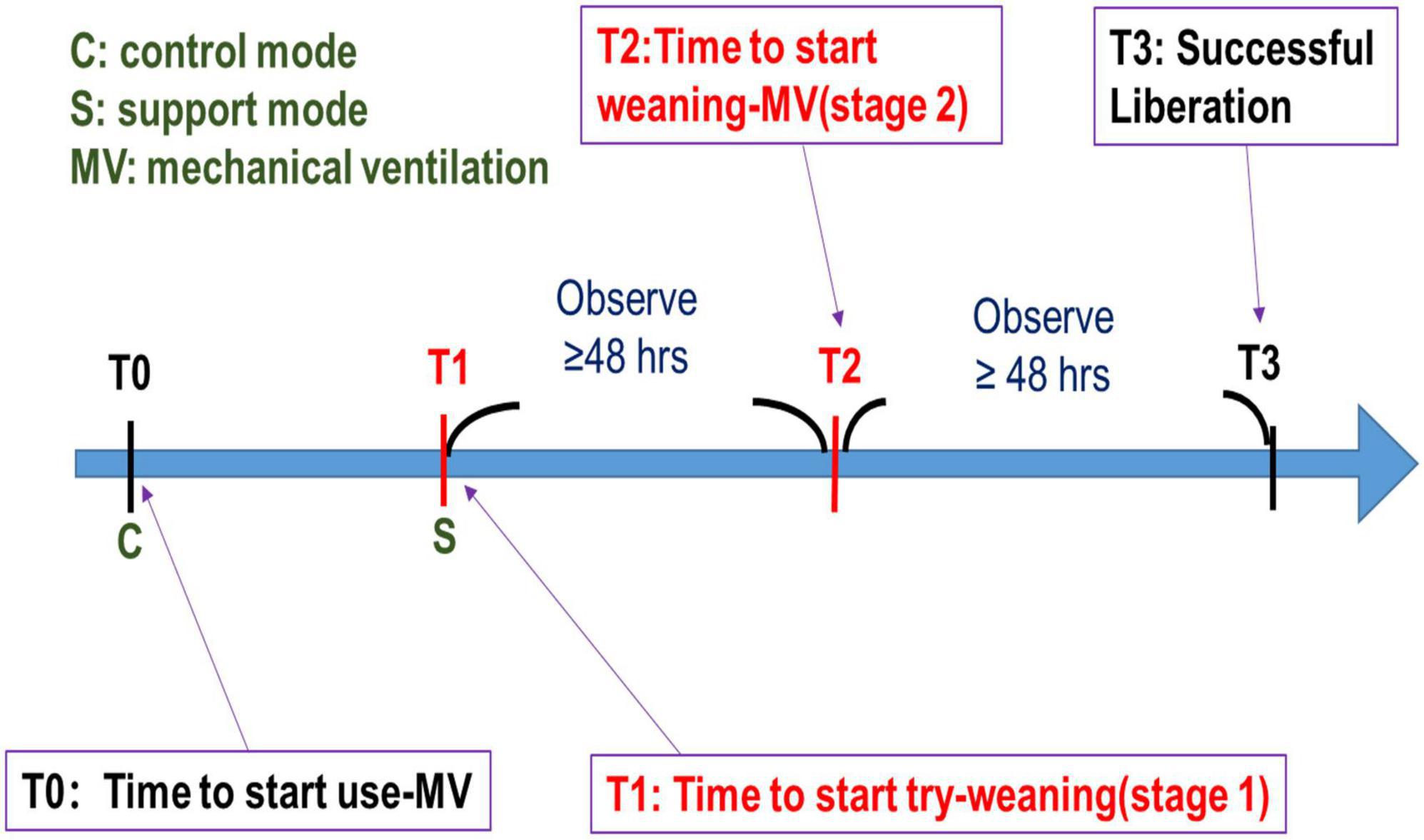
Figure 2. Two-stage weaning assessment.
Try-weaning stage means switching the ventilator from control mode to support mode for an ICU patient, while the complete weaning MV stage means transitioning from support mode ventilation to oxygen therapy or extubation for an ICU patient.
Setting and data source
Chi Mei Medical Center is a large hospital in Tainan, Taiwan with 1288 beds, including 109 ICU beds. It has a comprehensive hospital information system to store each kind of clinical data such as demographics, diagnoses, vital signs, laboratory data, and prescribed medications in the database. Since 2016, CMMC adopted IoT technology to capture parameters from the MV in ICUs automatically per minute. So far, big data from MV was cumulated and ready for further AI and machine learning study.
Features and outcome variables
The first stage model used 25 features, including primary patient data of age, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, Therapeutic Intervention Scoring System (TISS) score, and the first and last Internet of Thing (IoT) data of the respirator consisting of inspired oxygen fraction (FiO2), positive end-expiratory pressure (PEEP), respiratory rate (RR), minute ventilation (Mv), peak inspiratory pressure (Ppeak), mean airway pressure (mPaw), peripheral oxygen saturation (SpO2), expiratory tidal volume (Vte), heart rate (HR), systolic blood pressure (SBP), and diastolic blood pressure (DBP). Based on clinical experience, the outcome variable was binary coded with 1 (i.e., successful try-weaning), which means that MV was shifted from the control mode to the support mode for at least 48 h, otherwise it was coded with 0.
The second stage model used 20 features, including primary data consisting of age, APACHE II score, and TISS score; and the last respirator IoT data before extubation consisting of FiO2, PEEP, RR, Mv, Ppeak, mPaw, SpO2, pressure support level (PSL), tidal volume with pressure support (PSLvolume), body temperature (BT), HR, SBP, DBP, Glasgow Coma Scale eye-opening (GCS_E), GCS motor response (GCS_M), SBT count during support mode, and sputum suction count within 24 hours before extubation (Suction). The outcome variable was binary coded with 1 (i.e., successful weaning MV), which means weaning from MV for at least 48 h, otherwise coded with 0. This is also accepted as a basis for the provision of government-related health subsidies in Taiwan.
All potential features were selected based on the literature (6, 7, 44, 45), clinic availability and the experience of clinicians. We performed correlation analysis between features and outcomes to assist in feature selection decisions. Features with the raw data were obtained from the hospital information system (HIS) and real-time IoT transferring from ventilators.
Model building and measurement
Raw data was collected from the electronic medical records of ICU to build the models for stage 1 and stage2. We randomly divided the cleaned data into 70% training and 30% testing data. Due to the data imbalance problem (fewer cases in the minority class), we applied the Synthetic minority over-sampling technique (SMOTE) method to process the training data (46). We performed a grid search for five-fold cross-validation on the training dataset to obtain the best hyper-parameters for modeling. Finally, we used the testing dataset (also called hold-out dataset) for the final evaluation of the model quality. Four model quality indicators of accuracy, sensitivity, specificity, and AUC (area under the ROC) were applied to assess the model quality. However, the overall model performance is generally evaluated by AUC in many medical studies since both true/false positive and true/false negative are fairly considered. Thus, AUC was used in this study as the main indicator to determine the optimal model. We used the optimal models for subsequent implementation of the predictive system.
Each outcome used a variety of ML algorithms to build models, including LR, RF, SVM, K Nearest Neighbor (KNN), lightGBM, XGBoost, and Multilayer Perception (MLP). The ML models were performed based on Sklearn library and related ML modules in Python.
The main purpose of this study was to predict the optimal timing to wean MV, not just successful weaning or not; thus, we divided each stage into 11 time periods based on clinical experience, and built 11 prediction models with the period data rather than building a single model with the end-point data of ICU patients with MV. That is, it is of great value to predict whether a patient can successfully wean or not over time. After all, most patients with MV in ICU will eventually be successfully weaned but we expect timely or even early safe weaning of MV to avoid overuse rather than just predicting success or not (in CMMC, the average extubation success rate exceeds 85%). However, hospitals can reduce or increase the predictive periods according to their needs while implementing.
Stage 1 of timing prediction for successful try-weaning involves the following: After the patient enters the ICU for intubation, we built 11 models for 11 prediction time points, namely: 8th hour, 12th hour, 24th hour, 36th hour, 48th hour, 60th hour, 72nd hour, 84th hour, 96th hour, 108th hour, and 120th hour. The first stage is considered a success if the MV is shifted from assist control to support mode for at least 48 h.
Stage 2 of timing prediction for successful weaning-MV involves the following: We built 11 models in days (after the patient completed the first stage successfully). The second stage is considered a success if the patient can last longer than 48 h after extubation from the support mode or leave the ICU safely for shorter than 48 h (47).
The data used in each model came from the data collected at this time point. For example, the 60th HR model used data of patients, which was collected at or nearer the 60th hour time point of using the respirator.
Two-stage artificial intelligence prediction system development of the optimal models
We chose the optimal models for each stage to develop a two-stage prediction system in a digital dashboard style to assist the weaning decision of respiratory medical teams. The system was developed using Microsoft Visual Studio® with VB language.
The web-based dashboard is linked to the real-time database of the existing HIS which could retrieve the required feature values of a specific model. The clinical staff could obtain the related predictive data and figure out the best timing of MV weaning by just previewing the patient’s data in the dashboard. The dashboard automatically retrieves the clinical data of the patient for AI prediction without the need for manual input and immediately displays the probabilities of successful MV weaning at each time from the beginning of ventilator use to the nearest future time point. The dashboard would automatically refresh the prediction for all patients every 60 min.
For example, if a patient has used MV for over 50 hours, the dashboard will show the probability of the 24th, 48th, and 72nd hour. The respiratory care team can further double-click on the targeted patient to prompt a new page to overview the detailed feature values at that predicting period. By monitoring the trend curve of the successful probabilities (in colored balls) and detailed feature values, the respiratory care team could evaluate whether each patient is eligible to start trying weaning or liberate the individual from MV more objectively and efficiently at this time point.
Results
Demographics
We retrospectively collected 6,184 cases of patients who used MV in CMMC ICU from 2016/1/1 to 2019/12/31. After excluding the cases with missing values, 5,873 cases were included for modeling in Stage 1 and 4,172 cases were included in Stage 2. Tables 1, 2 show the patients’ demographics in Stage 1 and Stage 2 respectively.
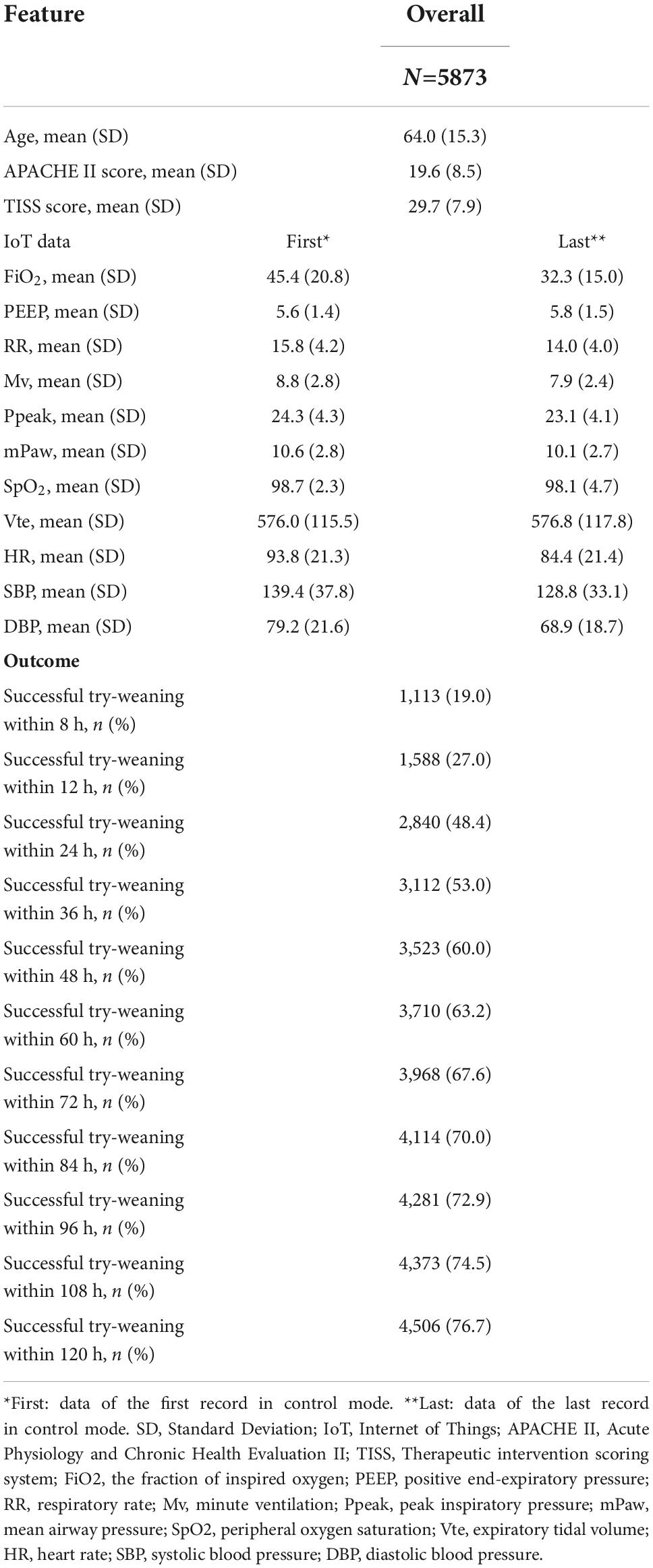
Table 1. Stage 1 demography.
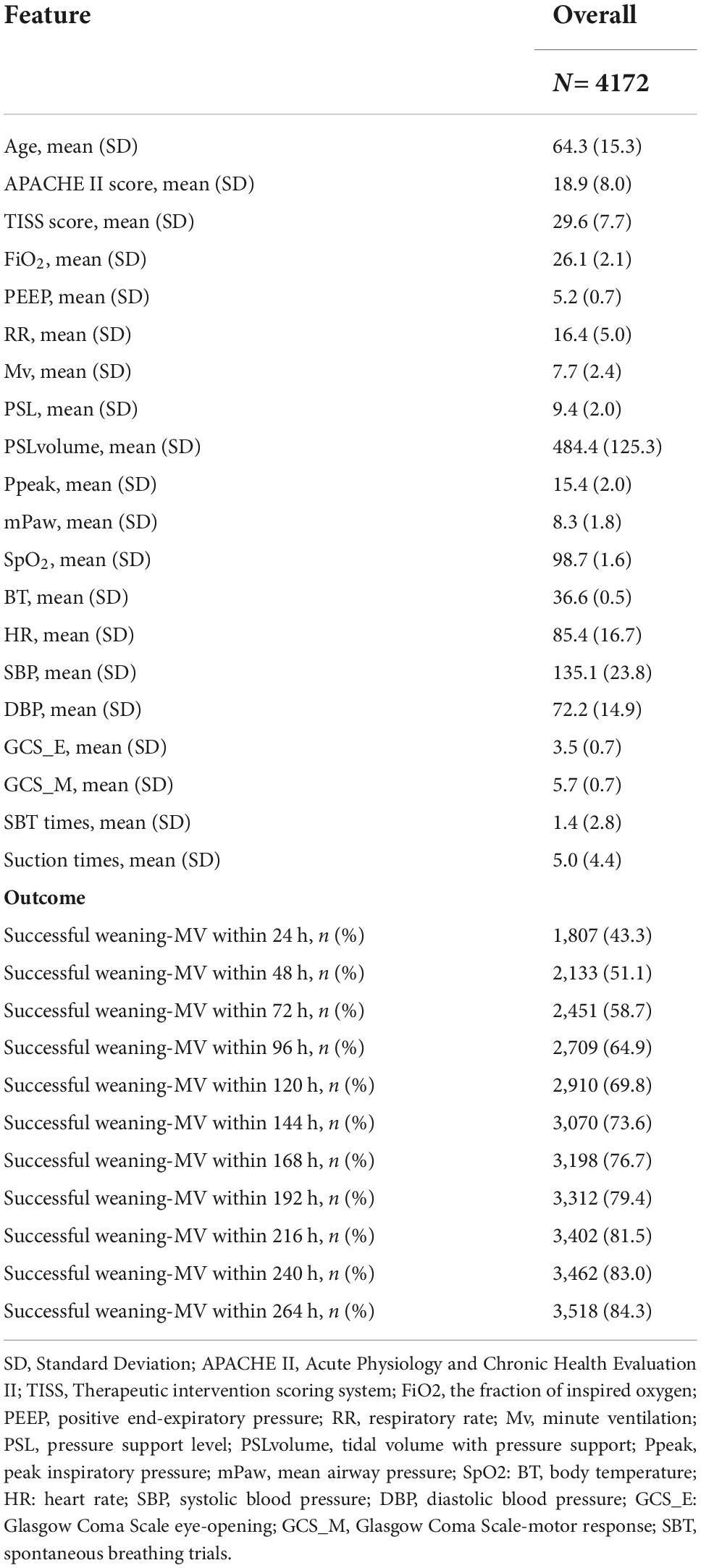
Table 2. Stage 2 demography.
For example in Stage 1, Spearman correlation analysis for the 60th hour model (Figure 3) showed that the most relevant to the timing of successful try-weaning was the first FiO2, followed by APACHE II score, and the last PEEP and mPaw. Spearman correlation analyses for all models in Stage 1 are shown in Figure 4. Moreover, for Stage 2, Spearman correlation analysis for the 120th hour model (Figure 5) showed that the number of SBTs was most relevant to the timing of successful weaning-MV, followed by the number of Suctions. Spearman correlation analyses for all models in Stage 2 are shown in Figure 6.
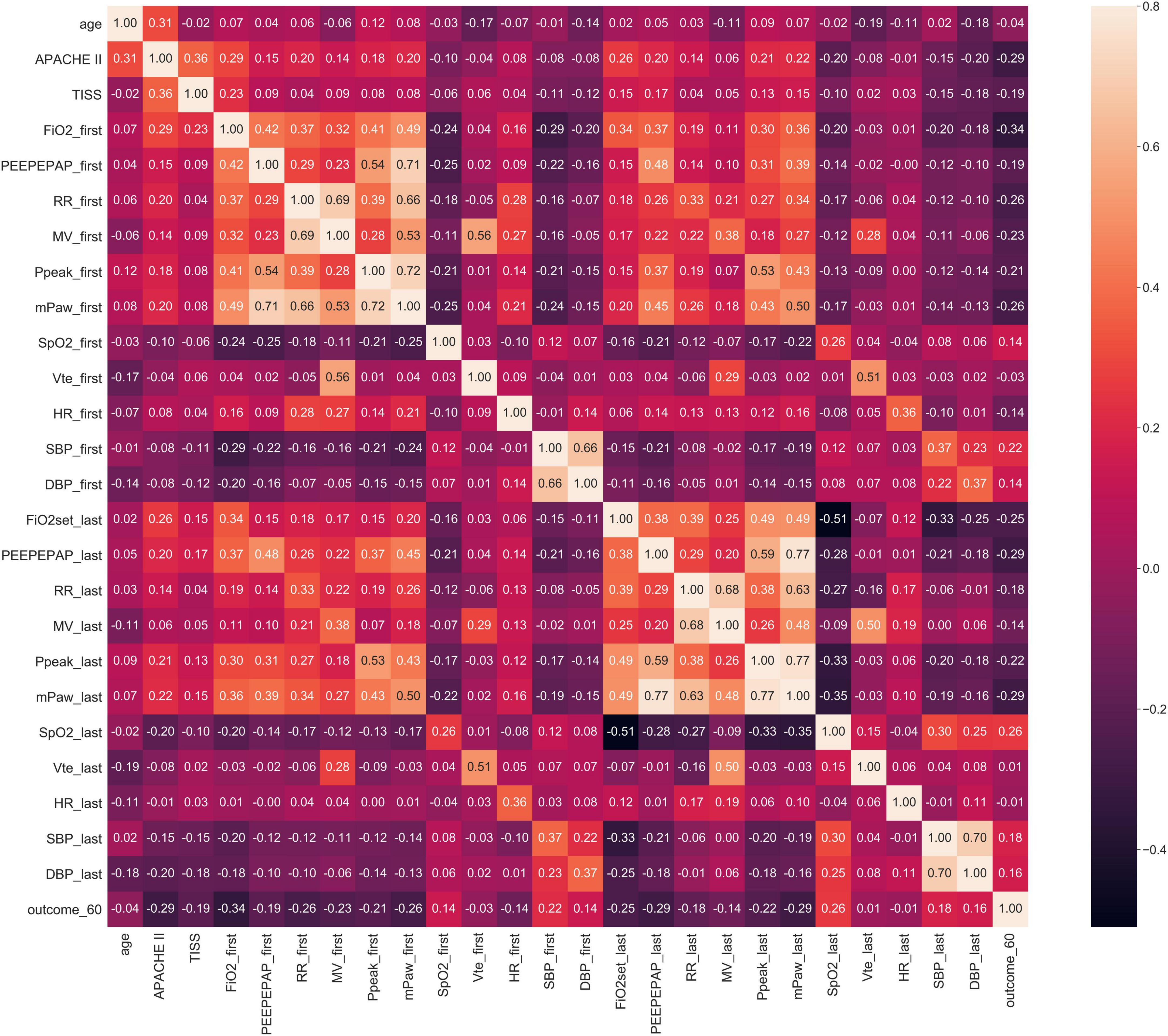
Figure 3. Stage 1 Spearman correlation (the 60th hour model). Note: outcome_60: Successful weaning or not before using 60 h of MV; FiO2_first, _last: the first/last value of FiO2 after using MV within 60 h, others are labeled similar.
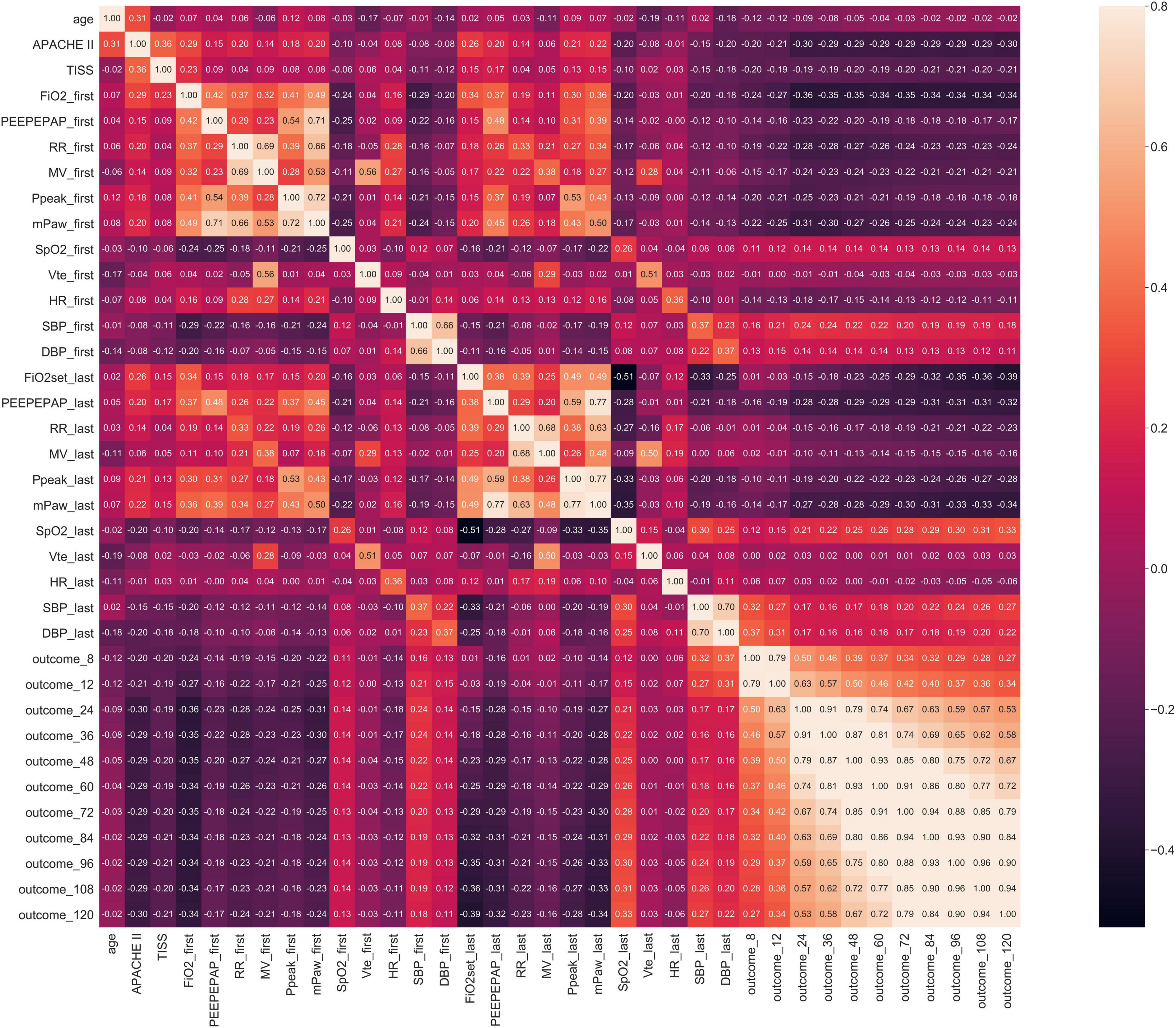
Figure 4. Stage 1 Spearman correlation.
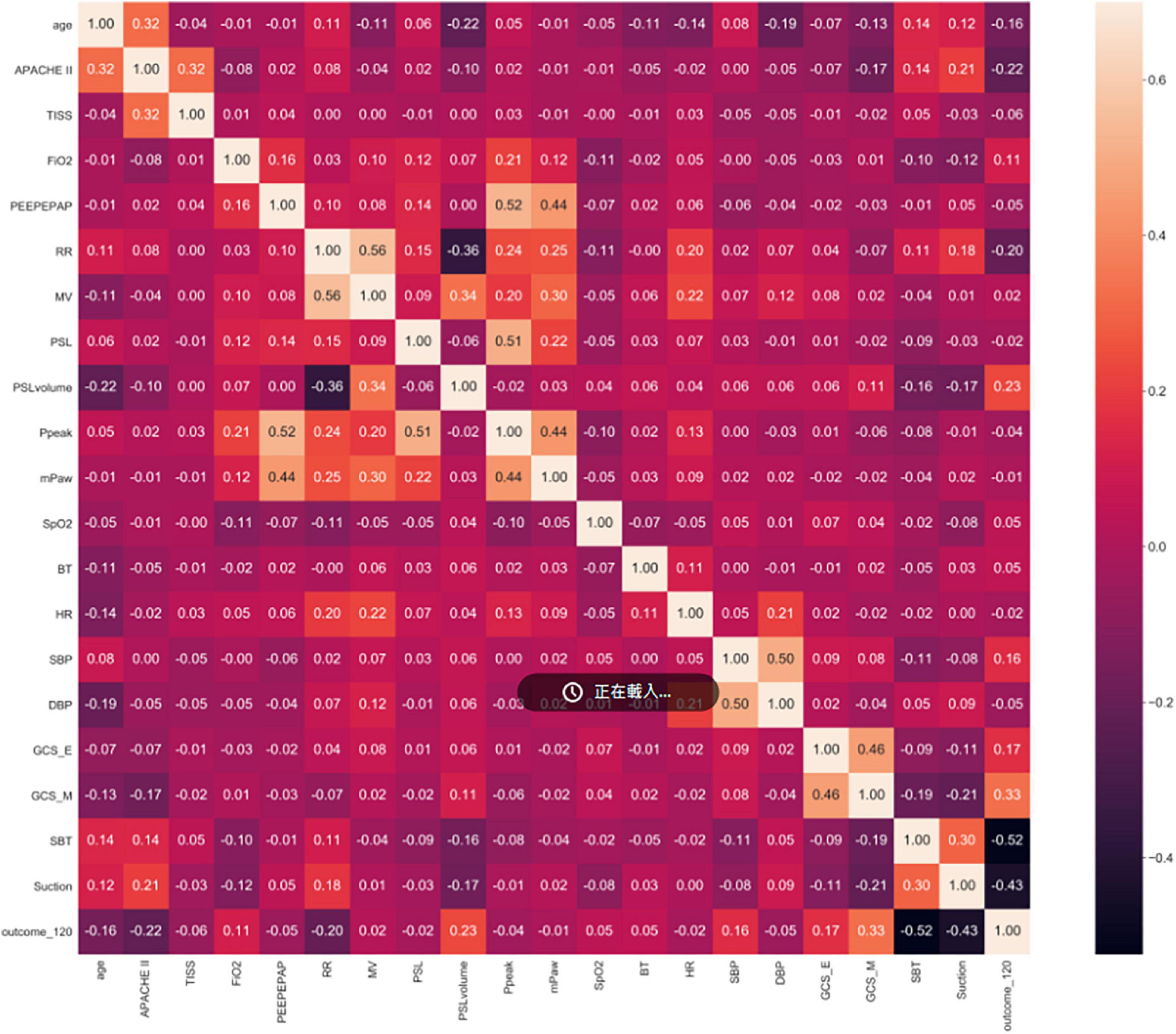
Figure 5. Stage 2 Spearman correlation (the 120th Hour model). Note: outcome_120: Successful weaning or not before using 120 h of MV, others are labeled similar.
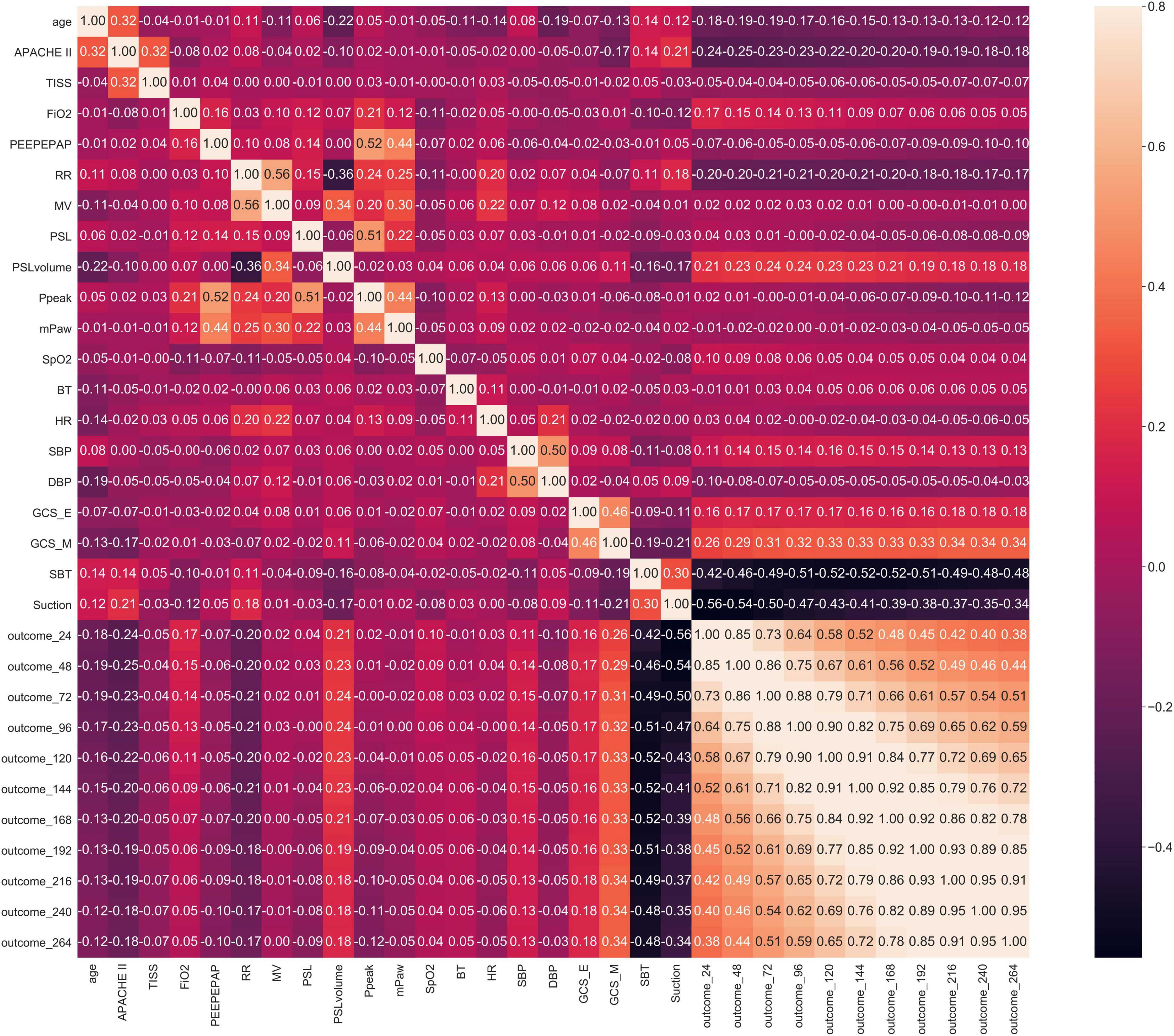
Figure 6. Stage 2 Spearman correlation.
Modeling results
In this study, eleven models were established in each of the two stages. In Stage 1, the 60th-hour model was taken as an example. Each model used seven algorithms with optimal hyper-parameters. Models’ performances with the seven ML algorithms are shown in Table 3 (Stage 1) (Supplementary Table 1 for other models in Stage 1). With the 60th-hour model as an example, according to the value of AUC model, the lightGBM model obtained the maximum value (AUC = 0.860) and was used as the basis for implementing the online prediction system. Besides, ROC curve is a performance measurement for a classification model at various thresholds. Figure 7 covers the ROC curves of the seven algorithms and the three highest AUCs (lightGBM, XGBoost and Random forest) ranged from 0.860 to 0.847 showing good model quality with smooth empirical ROC curves and AUCs near to 1.
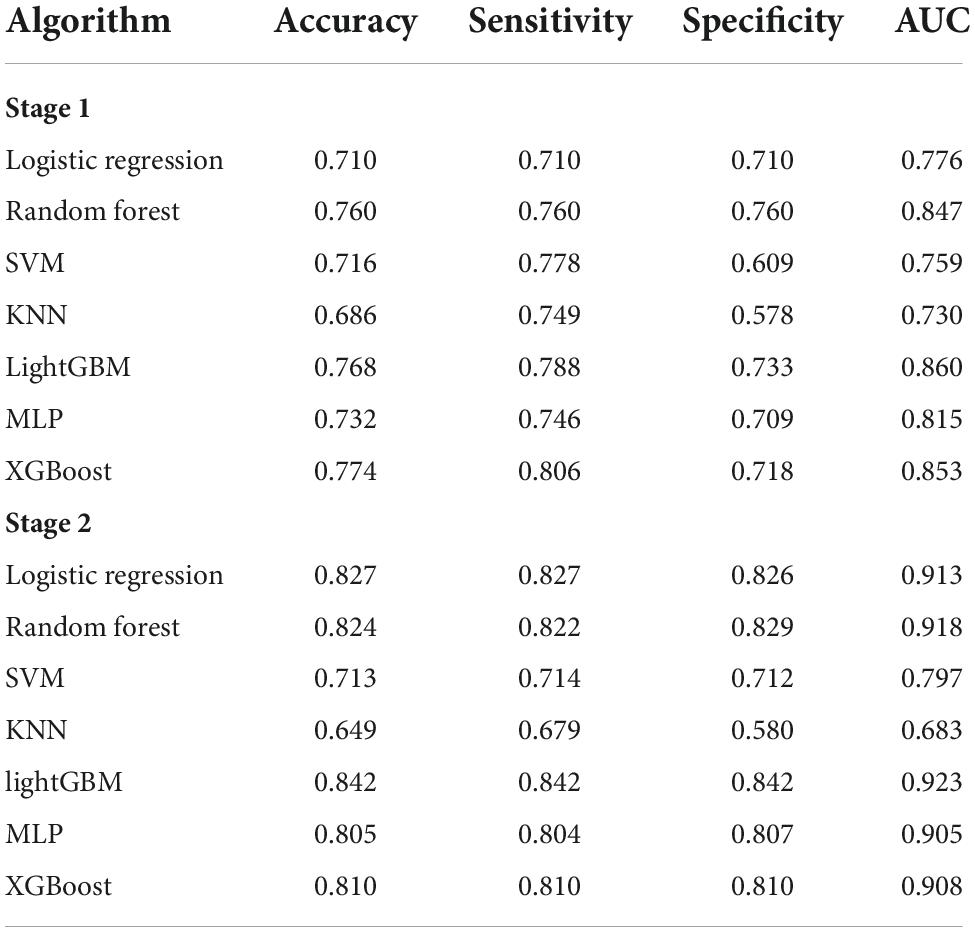
Table 3. Testing results of the predictive models: Stage 1 try-weaning model of the 60th HR and Stage 2 MV-weaning model of the 120th HR.
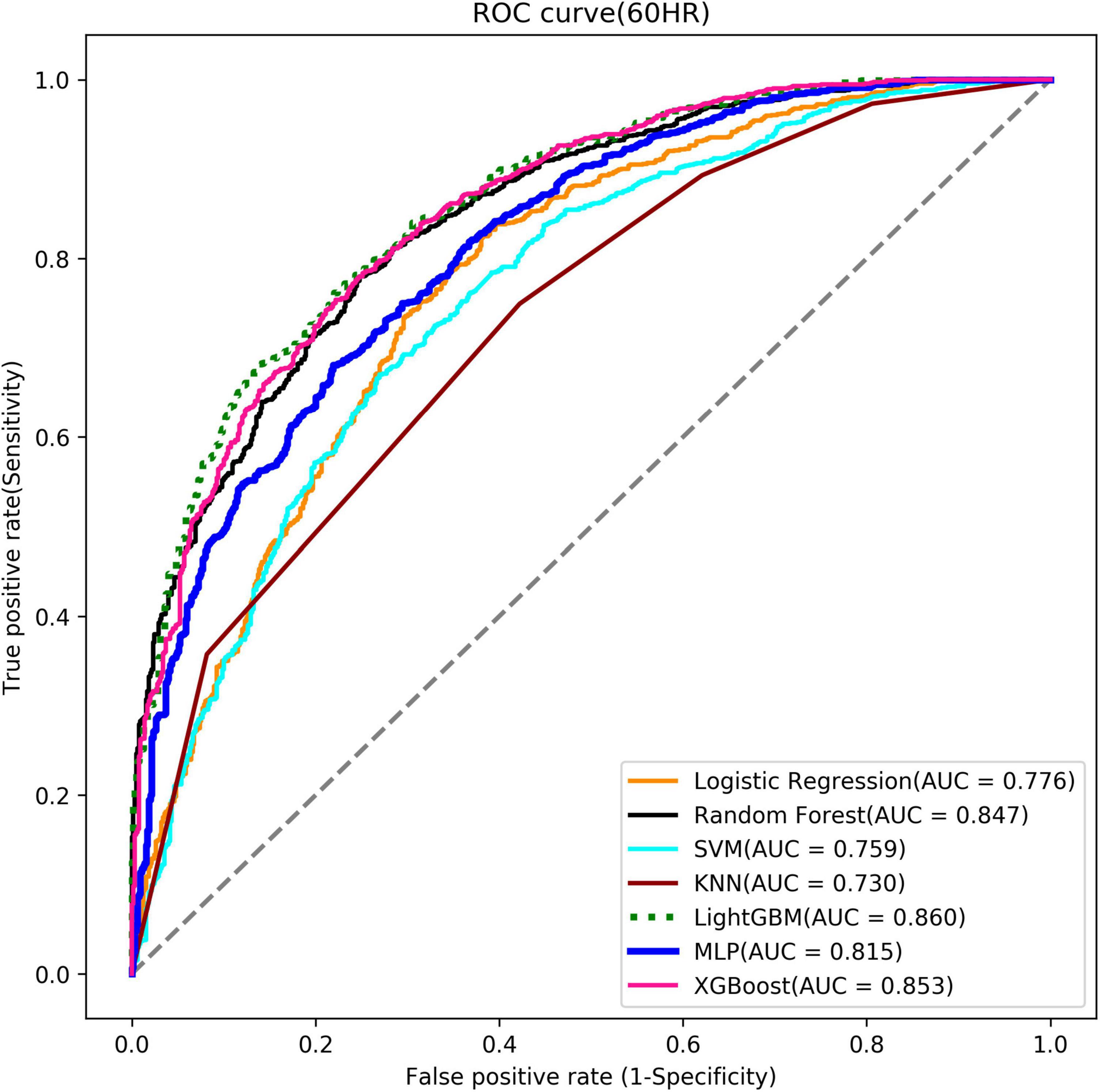
Figure 7. Stage 1 ROC curve (the 60th Hour model).
In Stage 2, the 120th hour (5th day) model was taken as an example. The lightGBM model was selected for implementation based on the AUCs of the seven algorithms (AUC = 0.923) [Table 3 (Stage 2)] (Supplementary Table 2 for other models in Stage 2). Figure 8 shows the ROC curves of the seven algorithms and the three highest AUCs (lightGBM, Random forest and Logistic regression) ranged from 0.913 to 0.923. It also shows excellent models. Hyper-parameters used for building optimal model for each algorithm are listed in Supplementary Table 3.
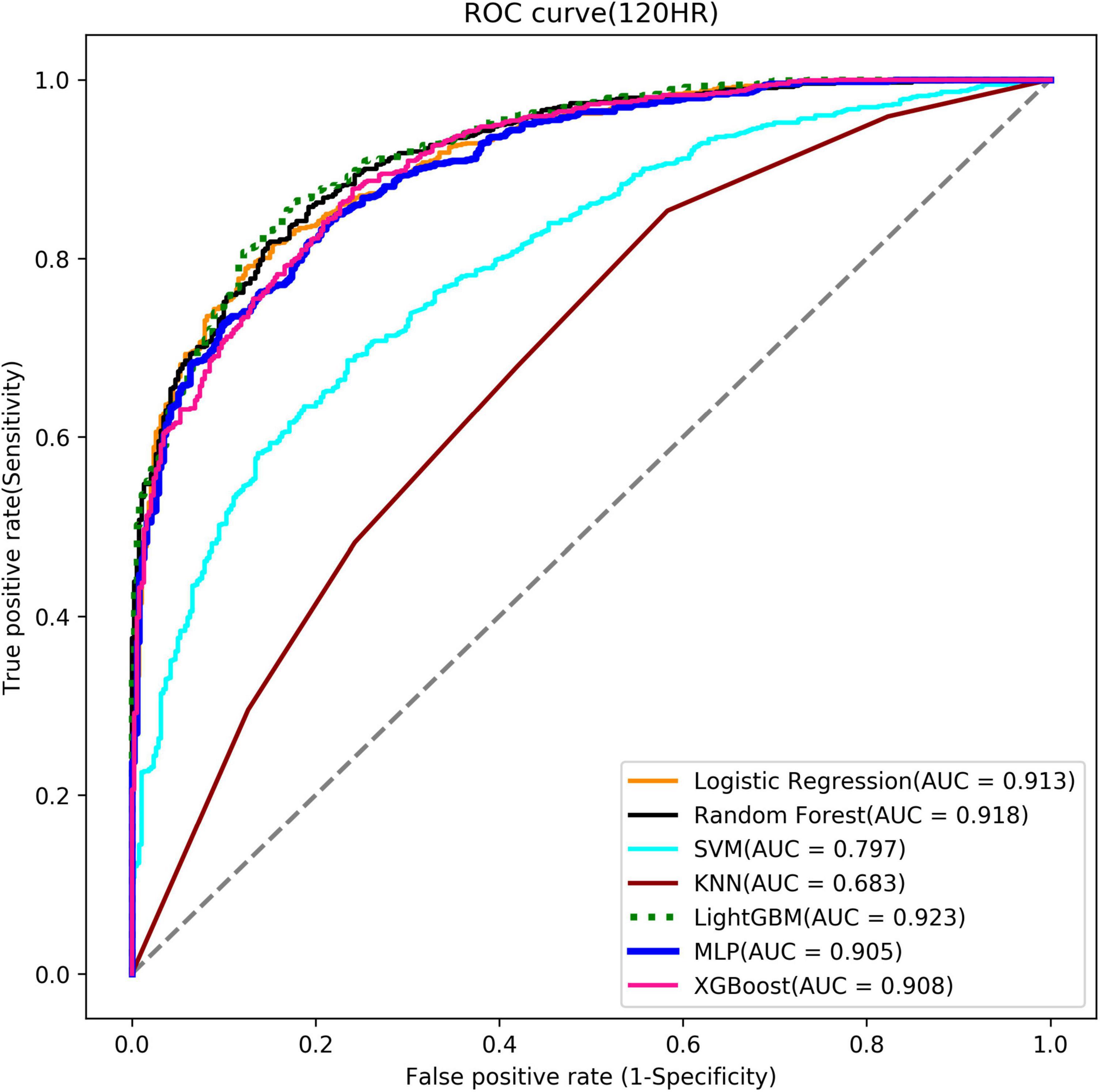
Figure 8. Stage 2 ROC curve (the 120th Hour model).
Moreover, we randomly chose patients A, B, and C who successfully weaned from MV in 2021 (weaning time points at the 144th hr, 216th hr, and 242th hr, respectively) and observed them retrospectively. Taking the data at the 48th-hour ventilator use as features (the patients all failed to wean at the 48th hr), the probabilities predicted by our 48th-hr model were all <50%, which mean a tendency for unsuccessful weaning (probabilities were 32.58, 40.24, and 20.1%, respectively). These predictions were correct. We then fed the same data to a single model (usually the last model, represented here by our 264th-hr model) and all displayed a tendency for successful weaning (probabilities were 95.23, 79.06, and 61.38%). These predictions were incorrect. This proves that, adopting in practical, using multiple models is more appropriate to the prediction of weaning time than when using a single model only.
Prediction system development and deployment
Using the optimal prediction models, the AI Center and the Department of Information Systems of CMMC jointly developed the timing prediction system (a dashboard) for try-weaning and weaning MV and integrated it with the existing hospital information system (respiratory care system). Such graphical presentation and drill-down interactive function help track the status of patients and enhance users’ acceptance of the AI dashboard. Our results showed that this system could predict the optimal timing for try-weaning and weaning MV during the decision-making process of the clinicians. Moreover, the reference data from this system could be used effectively for communication with the patient’s family.
Use case scenario
The interface of the AI dashboard is shown in Figure 9. Stage 1 (try-weaning) displayed the patient’s basic information (bed number, medical record number, name), the time when ventilator use was started, the current number of hours of use, and the probability of success in each period. For example, the first patient of Stage 1 had used the ventilator for 63 h; the system captured the patient’s characteristic data and displayed the predictions for the nearest future. It could be seen that the probability of successful try-weaning within 72 h of this patient was 56.35%, which implies that the medical team may switch the mode of the patient’s ventilator (start try-weaning) during this time. Stage 2 (weaning MV) presented content similar to Stage 1, which included basic information, starting time of support mode, current total hours of support mode, and the success probability of each period. For example, the first patient in Stage 2 had been in the support model for 51 h; the system predicted that the success probability of liberating the patient in MV within three days (72 h) was 33.36%, so it was not recommended to wean during this period.
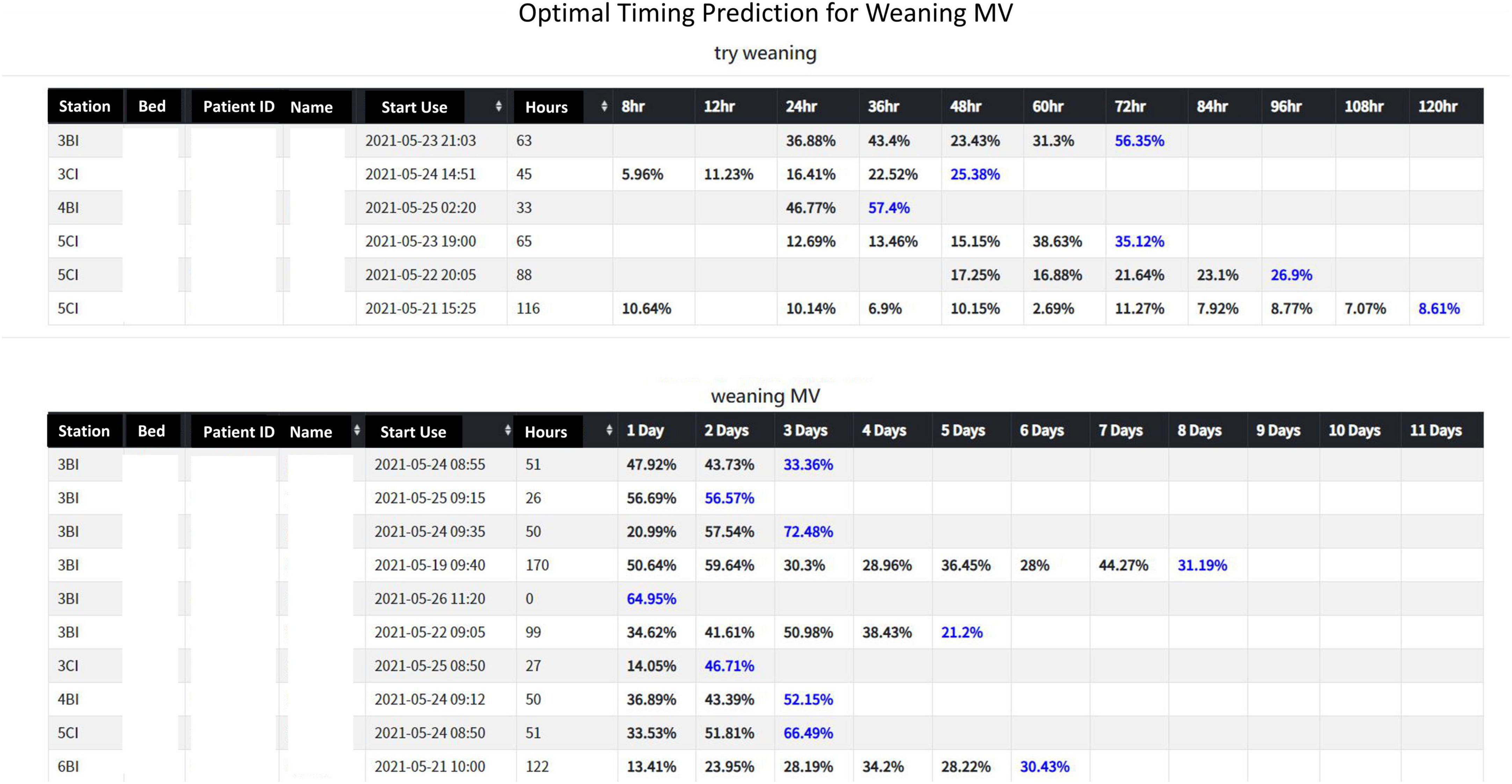
Figure 9. A screenshot of the artificial intelligence (AI) prediction system interface.
User evaluation and impact analysis of artificial intelligence assistance
After the hospital launched the dashboard system and implemented it for one month, we interviewed some of the respiratory care members (3 physicians and 5 therapists) and gained high positive feedback. They thought that the dashboard was a very useful tool in helping them determine the optimal timing for trying to wean a patient from the ventilator. According to them, it was also a useful tool for shared decision-making (SDM) especially when communicating with patients or their families. Also, they raised expectations for improvement. For example, they hoped that the predicted value at each time point could be drawn as a polyline to easily see the trend of the predicted probabilities for a patient. These expectations were later realized.
So far, this AI dashboard has been online in ICU for nearly two years. Therefore, we conducted an anonymous 5-scaled questionnaire survey (with Google Form) for all 10 ICU physicians during September 30, 2022 and October 5, 2022, and received 8 valid questionnaires. Overall, they believe that the AI is easy to use (mean = 4.5), the prediction results provided by the AI are of reference value (mean = 4.0), and the AI is helpful to the MV weaning decision (mean = 4.25). However, 2 physicians answered “seldom use AI”, 4 physicians answered “frequent use of AI”, and the remaining 2 physicians answered “already use AI regularly”. One of the physicians who answered “seldom use of AI” left a comment saying that physicians have had extensive experience in assessing MV weaning and AI assistance is not very necessary.
Moreover, we selected an ICU ward and recorded the successful extubation time and associated data. The collected data was then compared with that of the previous year. In other words, the parameters collected from July to November 2019 (without AI assistance) was contrasted with those of July to November 2020 (with AI assistance). Intubated adult patients weaned from MV successfully were enrolled in the study implementation. Patients with tracheostomy and transferred to the respiratory care ward were excluded. The analysis results of Table 4A showed no statistically significant difference in the demographic distribution between these two groups, including the age, gender, and disease severity (Apache II, TISS, COMA) of patients. It provided a fair basis for AI intervention comparison. It also showed that there was no significant difference in successful extubation-rate, indicating that patient safety was not compromised (actually slightly improved) with AI. However, in Table 4B, we noticed the average intubation hours after AI intervention were about 21 hours shorter than that without AI intervention, and the average stay in ICU was reduced by 0.5 days, showing that our AI-assisted system does boost patients wean from ventilators earlier, which could improve the quality of care.
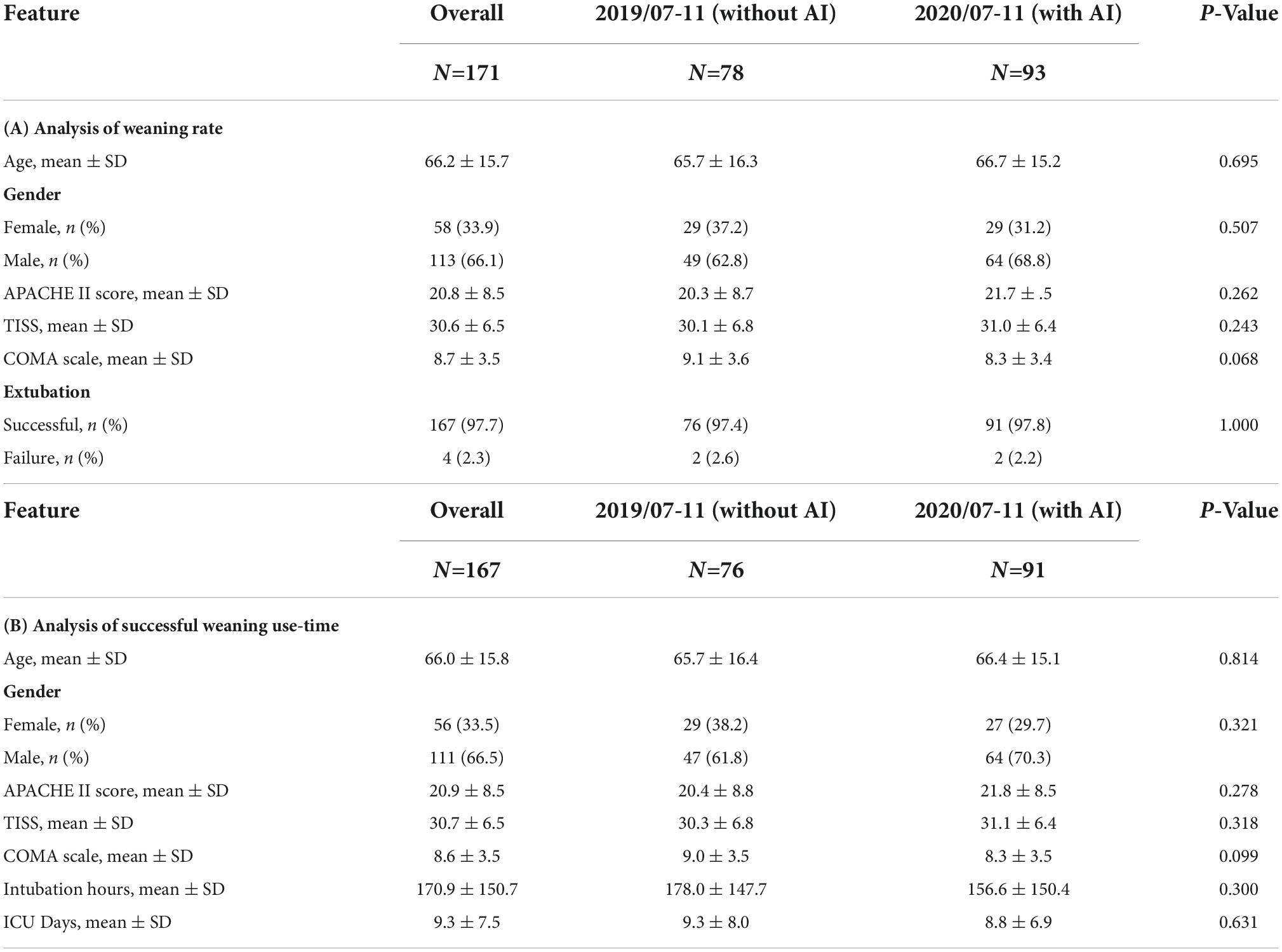
Table 4. The results of clinical evaluation and comparison.
We also performed Kappa analysis (P < 0.05 for significance) on the patients with AI to estimate the consistency of AI prediction and regular care procedure. As shown in Table 5, all values of Kappa are above 0.61 indicating that all models have substantial consistency between these two decision-making strategies (48).
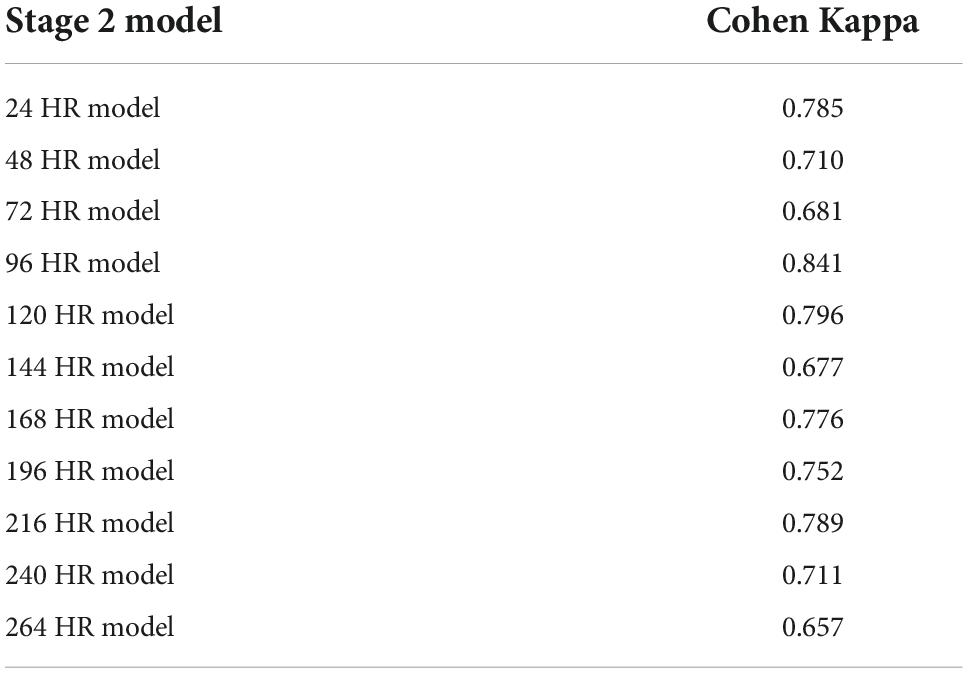
Table 5. Analysis of Kappa values in 11 models of Stage 2.
Discussion
Most related studies in the past explored the factors that affect weaning from the ventilator or predicted the success of weaning. However, this study argues that precise weaning decisions should consist of two phases, try-weaning and complete weaning MV, and that each should have a separate predictive model built. In addition, we believe that, clinically, deciding on the optimal timing for weaning is more crucial than predicting the final success, so we built 11 models at 11 time points for each stage. More importantly, we used the optimal models to build a prediction system (AI dashboard) for monitoring all patients with MV in ICU to validate the feasibility of our comprehensive AI approach. The impact study confirmed that the average intubation time was shortened by 21 h after AI intervention. Overall, this study has significant academic and practical values.
Mechanical ventilation use is a life-guarding technique providing critically ill respiratory support, and it is one of the most common interventions given to ICU patients (49). In this study, correlation analyses for all models in Stage 1 showed that FiO2, mPaw, APACHE II score, PEEP, SpO2 tend to be higher correlated to the predictive models. It implies that oxygenation, hemodynamics and disease severity have great influence on full support mode shift to partial support mode. Increasing FiO2, mPaw and PEEP is to improve the patient’s oxygenation status, but too high mPaw and PEEP will cause lung overdistension and affect cardiac output. Similar, frequency of suction, numbers of SBT, GCS_M, APACHE II score, PSL volume, RR tend to higher correlate to the predictive models in Stage 2. It implies that cough strength, respiratory capacity and disease severity affected weaning success. This reminds clinical staff to assess the amount of sputum or secretions, the patient’s mobility, ability to cough, and breathing patterns to ensure successful extubation. However, the biomedical etiology and pathophysiology of weaning failure are complex and often multifactorial, including airway and lung dysfunction, brain dysfunction, cardiac dysfunction, diaphragm dysfunction, and endocrine dysfunction. Accordingly, determining the reason and subsequently developing a treatment strategy require a dedicated clinician with in-depth knowledge of these parameters of weaning failure (50). Moreover, earlier recognition of the patient’s capacity for some level of autonomous respiration is fundamental to progressively initiating the weaning of the patient from MV and finally gaining full independent respiratory function (51). Thus, our study provides a new AI-enabled solution to realize the expectation.
Ideally, the clinical weaning parameters collected in critical care need to be objective and easy to acquire, and the process would not impede patient management. The physiological mechanisms resulting in respiratory failure vary for different individuals, and diverse weaning parameters will contribute to one aspect of the pathophysiological mechanism. It has been proved that it is insufficient to improve the outcomes of ventilated patients by applying the weaning index only (52). Our AI models, which incorporate a full range of patients’ basic parameters, physiological parameters, and respiratory parameters, and consider the dynamic changes in time series, were used to establish a two-stage, multi-time series prediction model, which significantly improves the success in predicting weaning and conforms to clinical experience.
There have been several studies in the past that explored the prediction of related ICU respirator use with machine learning methods or traditional statistical methods (e.g., regression analysis method). Our research found that ML methods roughly outperformed traditional statistics. In the studies of ML method, we also obtained more excellent results. Our models are not only of high quality (AUC >0.94) but also the two-stage design is closer to clinical experience of weaning decision-making than a single-stage design. Cheng (53) also proposed a two-stage decision-making approach; however, our prediction model quality was more superior to theirs since we also subdivided each stage into 11 time points which helped to precisely grasp the timing of weaning MV and even shorten the intubation time. More importantly, among these studies, only our research realized the ML models in practice. We summarized the comparison of our study with previous works (53–56) in Table 6.
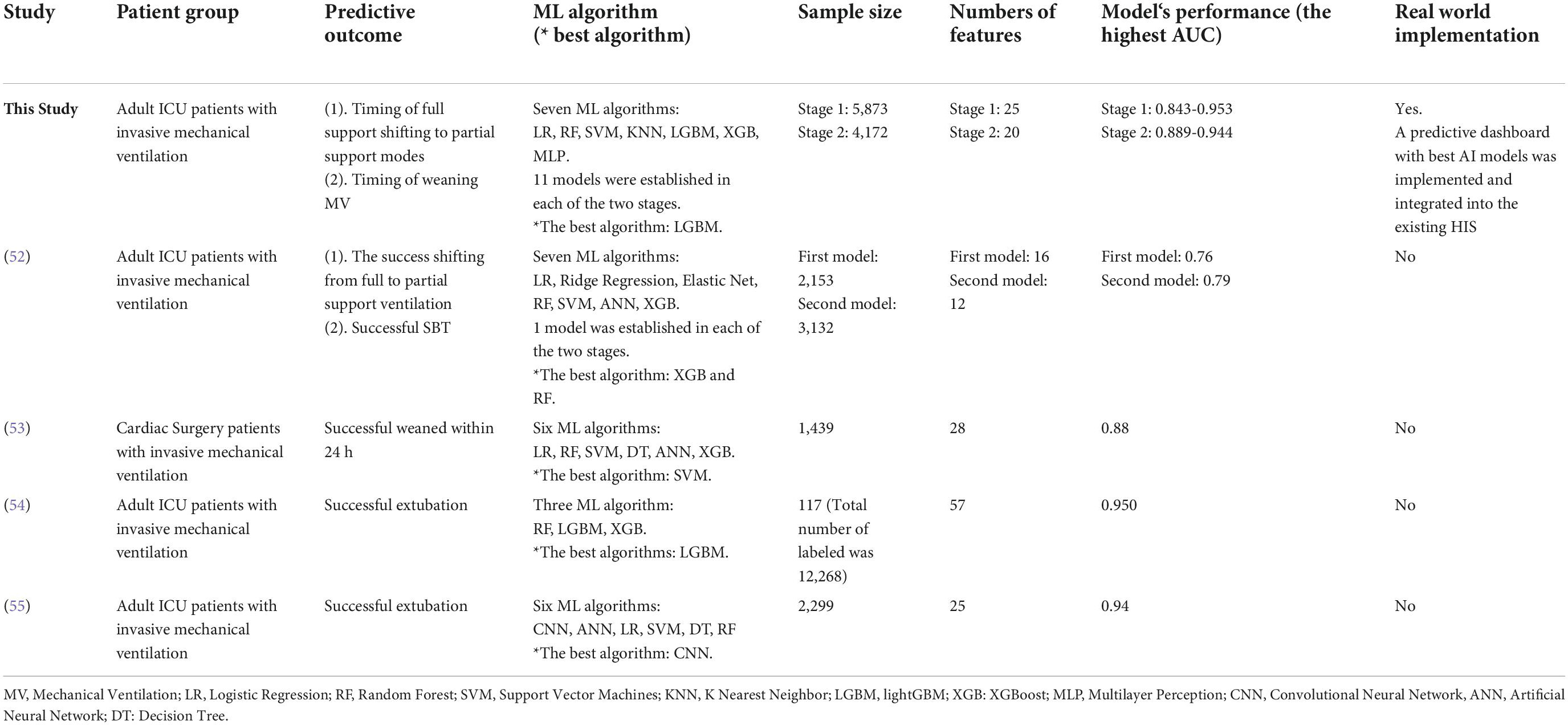
Table 6. A comparison with related studies.
Furthermore, LightGBM models were noted with the highest AUC values amidst the seven ML algorithms, consistent with Chen et al. (57). Moreover, LightGBM has been regarded as the most effective model to predict extubation success when compared with XGBoost, MLP, and SVM. LightGBM is a gradient boosting framework of tree-based learning algorithms with faster training speed and better accuracy, but with lower memory usage.
Further analysis indicated that our models had convinced predictability regarding the Swets classification (0.5 ≤ AUC ≤ 0.7, lower predicted; 0.7 ≤ AUC ≤ 0.9, certain predictive ability; AUC > 0.9, high predictive ability) (58). However, it was found that the models over time have a tendency of decreasing AUC (0.953∼0.864, lightGBM models in Stage 1; 0.943∼916, lightGBM models in Stage 2), which may imply that the longer the patient uses the ventilator, the more complicated it becomes when considering whether the patient can undergo try-weaning. This finding can also support why we use multiple periods instead of single period to predict weaning MV.
Our AI system could allow the clinicians to grasp the appropriate weaning time precisely, which could prevent the worthless dangers due to delayed or premature weaning process. Thus, with our AI system, the risks of complications and medical costs related to ventilatory support for patients are expected to decrease. More importantly, our AI system could lessen the effect of inter-clinician variability and improve the overall ICU care quality.
The deficiency of thorough evidence and the difference of results between individuals and subpopulations demonstrates there is scanty consensus on the issue of the best weaning protocol in clinical literature (59, 60). Our research results could provide useful solution to this long-standing clinical difficulty. AI applications should be aptly weighed parallel to other information sources and certified by well-designed prospective studies before comprehensive implementation. Although we noticed a substantial and even almost perfect consistency in the prediction of successful weaning from ventilators after AI intervention, we position our AI system as an auxiliary, not as a determiner for diagnosis.
Clinical decision assistance systems could aid clinicians in their decision-making (61) and provide individualized management protocols based on the patients’ clinical data and updated knowledge (62). Besides, AI is a powerful instrument that lowers the medical error rate and improves healthcare consistency and efficacy (63). However, there has been a lot of concern about the demerits of AI model applications in the decision of MV weaning. First, deep learning lacks explanatory power and related potential bias is hard to identify (64). Moreover, new ethical issues have been presented such as issues of erroneous decisions by AI, legal responsibility, and private information security crisis are taken into consideration (65).
There are limitations to our study. First, it is a single-center study, and we do not have an external cohort to validate our obtained models despite using data routinely collected in a real-world setting. Thus, extra care in terms of research generality must be given when extrapolating the findings to other centers. Second, some weaning-relevant data, like rehabilitation program arrangement, were not assessed in our dataset. We consider the model’s accuracy could be improved significantly after assessing this detailed information. Third, our enrolled patient number was relatively small, impacting the result. Fourth, our study failed to include essential features and modalities, like chest X-ray images, cuff-leak test, diaphragm ultrasonography, and fluid balance, which are widely assessed to predict successful extubation. Further, no information related to laryngeal edema after extubation was trained in our models. Therefore, it could be difficult for the developed model to forecast the extubation failure rate due to post-extubation laryngeal edema.
Conclusion
Weaning timing assessment in ICU patients with MV is one of the most critical steps for respiratory care teams. We employed AI technology to develop a comprehensive system and embedded it into the existing HIS to predict the timing of weaning MV; this proves the clinical innovation of AI intervention in critical care. According to our knowledge, such a study with valuable academic and practical implications is rare.
Most studies only report the quality of predictive models; thus, it may be difficult to judge its actual clinical value. Our study established a predictive model and validated the model in the clinical field, which proved that it has better benefits than traditional ones. Therefore, our study supports that AI could be a promising approach in predicting MV weaning timing in ICU and is expected to advance clinical research in this field.
Although we can see that the AI prediction dashboard we proposed can be an effective tool to assist weaning decision-making, it should be noted that it cannot be regarded as the only dependence for final decision-making. That is, after referring to the AI’s prediction, the medical team still need to conduct and discuss a professional and comprehensive observation and evaluation of the patient again before making the final weaning decision.
Our study showed that the use of ML approaches could obtain better predictive ability in ICU, however, some physicians also reported that AI assistance is not very necessary. Thus, how to increase physicians’ willingness to accept AI is indeed a key research topic. Besides, AI algorithms are difficult to understand (so-called black-box), which may affect the trust of clinical staff. Therefore, follow-up research to improve the explainability of AI must be done. Furthermore, intensivists expect that AI can be applied to build a decision support tool for integrated consideration of a patient rather than simply providing predictions on an illness. This is a challenge that should be taken seriously. However, we still have a long way to go at this moment.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were reviewed and approved by Chi Mei Medical Center (IRB Serial No.: 10912-016). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
C-MChen, K-CC, C-FL, and C-CC: conceptualization. C-MH, J-JW, C-CL, and C-CC: data curation. C-FL, M-IS, C-JC, and C-CC: formal analysis. C-MH, C-MChen, and C-CC: investigation. C-FL, M-IS, and C-JC: methodology. C-CL and C-MChen: project administration. S-CK, K-CC, M-IS, S-CH, and C-MChen: resources. C-FL and C-JC: software. C-CC: supervision. C-MH, S-CK, C-MChao, and C-CC: validation. C-MChao and C-MChen: visualization. C-FL and C-CC: writing—original draft. C-CC: writing—review and editing. All authors read and approved the submitted version.
Funding
This research was partially supported by the Ministry of Science and Technology of Taiwan (No. MOST111-2410-H-384-001-MY2).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.935366/full#supplementary-material
References
1. Wunsch H, Linde-Zwirble WT, Angus DC, Hartman ME, Milbrandt EB, Kahn JM. The epidemiology of mechanical ventilation use in the United States. Crit Care Med. (2010) 38:1947–53. doi: 10.1097/CCM.0b013e3181ef4460
2. Eskandar N, Apostolakos MJ. Weaning from mechanical ventilation. Crit Care Clin. (2007) 23:263–74. doi: 10.1016/j.ccc.2006.12.002
3. Navalesi P, Bruni A, Garofalo E, Biamonte E, Longhini F, Frigerio P. Weaning off mechanical ventilation: much less an art, but not yet a science. Ann Transl Med. (2019) 7:S353. doi: 10.21037/atm.2019.09.83
4. Schweickert WD, Gehlbach BK, Pohlman AS, Hall JB, Kress JP. Daily interruption of sedative infusions and complications of critical illness in mechanically ventilated patients. Crit Care Med. (2004) 32:1272–6. doi: 10.1097/01.ccm.0000127263.54807.79
5. Tsai TL, Huang MH, Lee CY, Lai WW. Data science for extubation prediction and value of information in surgical intensive care unit. J Clin Med. (2019) 8:1709. doi: 10.3390/jcm8101709
6. Asehnoune K, Seguin P, Lasocki S, Roquilly A, Delater A, Gros A, et al. Extubation success prediction in a multicentric cohort of patients with severe brain injury. Anesthesiology. (2017) 127:338–46. doi: 10.1097/ALN.0000000000001725
7. Strickland JH Jr., Hasson JH. A computer-controlled ventilator weaning system. A clinical trial. Chest. (1993) 103:1220–6. doi: 10.1378/chest.103.4.1220
8. Ely EW, Baker AM, Dunagan DP, Burke HL, Smith AC, Kelly PT, et al. Effect on the duration of mechanical ventilation of identifying patients capable of breathing spontaneously. N Engl J Med. (1996) 335:1864–9. doi: 10.1056/NEJM199612193352502
9. Kollef MH, Shapiro SD, Silver P, St John RE, Prentice D, Sauer S, et al. A randomized, controlled trial of protocol-directed versus physician-directed weaning from mechanical ventilation. Crit Care Med. (1997) 25:567–74. doi: 10.1097/00003246-199704000-00004
10. Marelich GP, Murin S, Battistella F, Inciardi J, Vierra T, Roby M. Protocol weaning of mechanical ventilation in medical and surgical patients by respiratory care practitioners and nurses: effect on weaning time and incidence of ventilator-associated pneumonia. Chest. (2000) 118:459–67. doi: 10.1378/chest.118.2.459
11. Krishnan JA, Moore D, Robeson C, Rand CS, Fessler HE. A prospective, controlled trial of a protocol-based strategy to discontinue mechanical ventilation. Am J Respir Crit Care Med. (2004) 169:673–8. doi: 10.1164/rccm.200306-761OC
12. Namen AM, Ely EW, Tatter SB, Case LD, Lucia MA, Smith A, et al. Predictors of successful extubation in neurosurgical patients. Am J Respir Crit Care Med. (2001) 163:658–64. doi: 10.1164/ajrccm.163.3.2003060
13. Navalesi P, Frigerio P, Moretti MP, Sommariva M, Vesconi S, Baiardi P, et al. Rate of reintubation in mechanically ventilated neurosurgical and neurologic patients: evaluation of a systematic approach to weaning and extubation. Crit Care Med. (2008) 36:2986–92. doi: 10.1097/CCM.0b013e31818b35f2
14. Rose L, Presneill JJ, Johnston L, Cade JF. A randomised, controlled trial of conventional versus automated weaning from mechanical ventilation using SmartCare/PS. Intensive Care Med. (2008) 34:1788–95. doi: 10.1007/s00134-008-1179-4
15. Simeone F, Biagioli B, Scolletta S, Marullo ACM, Marchet-Ti L, Caciorgna M, et al. Optimization of mechanical ventilation support following cardiac surgery. J Cardiovasc Surg. (2002) 43:633–41.
16. Piotto RF, Maia LN, de Nassau Machado M, Orrico SP. Effects of the use of mechanical ventilation weaning protocol in the coronary care unit: randomized study. Rev Bras Cir Cardiovasc. (2011) 26:213–21. doi: 10.1590/s0102-76382011000200011
17. Béduneau G, Pham T, Schortgen F, Piquilloud L, Zogheib E, Jonas M, et al. Epidemiology of Weaning Outcome according to a new definition. The WIND study. Am J Respir Crit Care Med. (2017) 195:772–83. doi: 10.1164/rccm.201602-0320OC
18. Jeong BH, Ko MG, Nam J, Yoo H, Chung CR, Suh GY, et al. Differences in clinical outcomes according to weaning classifications in medical intensive care units. PLoS One. (2015) 10:e0122810. doi: 10.1371/journal.pone.0122810
19. Girard TD, Alhazzani W, Kress JP, Ouellette DR, Schmidt GA, Truwit JD, et al. An official American thoracic society/American college of chest physicians clinical practice guideline: liberation from mechanical ventilation in critically ill adults. Rehabilitation protocols, ventilator liberation protocols, and cuff leak tests. Am J Respir Crit Care Med. (2017) 195:120–33. doi: 10.1164/rccm.201610-2075ST
20. Epstein SK, Ciubotaru RL, Wong JB. Effect of failed extubation on the outcome of mechanical ventilation. Chest. (1997) 112:186–92. doi: 10.1378/chest.112.1.186
21. DiRusso SM, Sullivan T, Holly C, Cuff SN, Savino J. An artificial neural network as a model for prediction of survival in trauma patients: validation for a regional trauma area. J Trauma. (2000) 49:212–20. doi: 10.1097/00005373-200008000-00006
23. Hsieh MH, Hsieh MJ, Chen CM, Hsieh CC, Chao CM, Lai CC. An artificial neural network model for predicting successful extubation in intensive care units. J Clin Med. (2018) 7:240. doi: 10.3390/jcm7090240
24. Tu JV. Advantages and disadvantages of using artificial neural networks versus logistic regression for predicting medical outcomes. J Clin Epidemiol. (1996) 49:1225–31. doi: 10.1016/s0895-4356(96)00002-9
25. Yang F, Wang HZ, Mi H, Lin CD, Cai WW. Using random forest for reliable classification and cost-sensitive learning for medical diagnosis. BMC Bioinformatics. (2009) 10:S22. doi: 10.1186/1471-2105-10-S1-S22
26. Furey TS, Cristianini N, Duffy N, Bednarski DW, Schummer M, Haussler D. Support vector machine classification and validation of cancer tissue samples using microarray expression data. Bioinformatics. (2000) 16:906–14. doi: 10.1093/bioinformatics/16.10.906
27. Videtta W, Vallejos J, Roda G, Collazos H, Naccarelli N, Tamayo A, et al. Predictors of Successful Extubation in Neurocritical Care Patients. Acta Neurochir Suppl. (2021) 131:91–3.
28. Baptistella AR, Mantelli LM, Matte L, Carvalho MEDRU, Fortunatti JA, Costa IZ, et al. Prediction of extubation outcome in mechanically ventilated patients: development and validation of the Extubation Predictive Score (ExPreS). PLoS One. (2021) 16:e0248868. doi: 10.1371/journal.pone.0248868
29. Chung WC, Sheu CC, Hung JY, Hsu TJ, Yang SH, Tsai JR. Novel mechanical ventilator weaning predictive model. Kaohsiung J Med Sci. (2020) 36:841–9.
30. Fathy S, Hasanin AM, Raafat M, Mostafa MMA, Fetouh AM, Elsayed M, et al. Thoracic fluid content: a novel parameter for predicting failed weaning from mechanical ventilation. J Intensive Care. (2020) 8:20. doi: 10.1186/s40560-020-00439-2
31. Formenti P, Umbrello M, Dres M, Chiumello D. Ultrasonographic assessment of parasternal intercostal muscles during mechanical ventilation. Ann Intensive Care. (2020) 10:120. doi: 10.1186/s13613-020-00735-y
32. Mesquida J, Gruartmoner G, Espinal C, Masip J, Sabatier C, Villagrá A, et al. Thenar oxygen saturation (StO(2)) alterations during a spontaneous breathing trial predict extubation failure. Ann Intensive Care. (2020) 10:54. doi: 10.1186/s13613-020-00670-y
33. Chawla S, Natarajan G, Shankaran S, Carper B, Brion LP, Keszler M, et al. Markers of successful extubation in extremely preterm infants, and morbidity after failed extubation. J Pediatr. (2017) 189:113–9.e2. doi: 10.1016/j.jpeds.2017.04.050
34. Manley BJ, Doyle LW, Owen LS, Davis PG. Extubating extremely preterm infants: predictors of success and outcomes following failure. J Pediatr. (2016) 173:45–9. doi: 10.1016/j.jpeds.2016.02.016
35. Muralitharan S, Nelson W, Di S, McGillion M, Devereaux PJ, Barr NG, et al. Machine learning-based early warning systems for clinical deterioration: systematic scoping review. J Med Internet Res. (2021) 23:e25187. doi: 10.2196/25187
36. Fleuren LM, Klausch TLT, Zwager CL, Schoonmade LJ, Guo T, Roggeveen LF, et al. Machine learning for the prediction of sepsis: a systematic review and meta-analysis of diagnostic test accuracy. Intensive Care Med. (2020) 46:383–400.
37. Parreco J, Hidalgo A, Kozol R, Namias N, Rattan R. Predicting mortality in the surgical intensive care unit using artificial intelligence and natural language processing of physician documentation. Am Surg. (2018) 84:1190–4.
38. Zheng L, Lin F, Zhu C, Liu G, Wu X, Wu Z, et al. Machine learning algorithms identify pathogen-specific biomarkers of clinical and metabolomic characteristics in septic patients with bacterial infections. Biomed Res Int. (2020) 2020:6950576. doi: 10.1155/2020/6950576
39. Mueller M, Almeida JS, Stanislaus R, Wagner CL. Can machine learning methods predict extubation outcome in premature infants as well as clinicians? J Neonatal Biol. (2013) 2:1000118. doi: 10.4172/2167-0897.1000118
40. Mueller M, Wagner CC, Stanislaus R, Almeida JS. Machine learning to predict extubation outcome in premature infants. Proc Int Jt Conf Neural Netw. (2013) 2013:1–6. doi: 10.1109/IJCNN.2013.6707058
41. Hsieh MH, Hsieh MJ, Chen CM, Hsieh CC, Chao CM, Lai CC. Comparison of machine learning models for the prediction of mortality of patients with unplanned extubation in intensive care units. Sci Rep. (2018) 8:17116. doi: 10.1038/s41598-018-35582-2
42. Hsieh MH, Hsieh MJ, Cheng AC, Chen CM, Hsieh CC, Chao CM, et al. Predicting weaning difficulty for planned extubation patients with an artificial neural network. Medicine. (2019) 98:e17392. doi: 10.1097/MD.0000000000017392
43. Chang YJ, Hung KC, Wang LK, Yu CH, Chen CK, Tay HT, et al. A real-time artificial intelligence-assisted system to predict weaning from ventilator immediately after lung resection surgery. Int J Environ Res Public Health. (2021) 18:2713. doi: 10.3390/ijerph18052713
44. Lai CC, Chen CM, Chiang SR, Liu WL, Weng SF, Sung MI, et al. Establishing predictors for successfully planned endotracheal extubation. Medicine. (2016) 95:41. doi: 10.1097/MD.0000000000004852
45. Meade M, Guyatt G, Cook D, Griffith L, Sinuff T, Kergl C, et al. Predicting success in weaning from mechanical ventilation. Chest. (2001) 120:400S–24S.
46. Chawla NV, Bowyer KW, Hall LO, Kegelmeyer WP. SMOTE: synthetic minority over-sampling technique. J Artif Int Res. (2002) 16:321–57.
47. Rose L, Adhikari NK, Leasa D, Fergusson DA, McKim D. Cough augmentation techniques for extubation or weaning critically ill patients from mechanical ventilation. Cochrane Database Syst Rev. (2017) 1:CD011833. doi: 10.1002/14651858.CD011833.pub2
48. Viera A, Garrett J. Understanding interobserver agreement: the kappa statistic. Fam Med. (2005) 37:360–3.
49. Lovejoy CA, Buch V, Maruthappu M. Artificial intelligence in the intensive care unit. Crit Care. (2019) 23:7. doi: 10.1186/s13054-018-2301-9
50. Heunks LM, van der Hoeven JG. Clinical review: the ABC of weaning failure–a structured approach. Crit Care. (2010) 14:245. doi: 10.1186/cc9296
51. Kwong MT, Colopy GW, Weber AM, Ercole A, Bergmann JHM. The efficacy and effectiveness of machine learning for weaning in mechanically ventilated patients at the intensive care unit: a systematic review. Biodes Manuf. (2019) 2:31–40. doi: 10.1186/s13054-016-1208-6
52. Huo Y, Guo S, Zhang K, Zhang T, Li B, Zhang Q, et al. A clinical study on the ability of the integrative weaning index to predict weaning from mechanical ventilation. Ann Palliat Med. (2020) 9:3162–9. doi: 10.21037/apm-20-1335
53. Cheng KH, Tan MC, Chang YJ, Lin CW, Lin YH, Chang TM, et al. The feasibility of a machine learning approach in predicting successful ventilator mode shifting for adult patients in the medical intensive care unit. Medicina. (2022) 58:360. doi: 10.3390/medicina58030360
54. Chen WT, Huang HL, Ko PS, Su W, Kao CC, Su SL. A simple algorithm using ventilator parameters to predict successfully rapid weaning program in cardiac intensive care unit patients. J Pers Med. (2022) 12:501. doi: 10.3390/jpm12030501
55. Otaguro T, Tanaka H, Igarashi Y, Tagami T, Masuno T, Yokobori S, et al. Machine learning for prediction of successful extubation of mechanical ventilated patients in an intensive care unit: a retrospective observational study. J Nippon Med Sch. (2021) 88:408–17. doi: 10.1272/jnms.JNMS.2021_88-508
56. Jia Y, Kaul C, Lawton T, Murray-Smith R, Habli I. Prediction of weaning from mechanical ventilation using convolutional neural networks. Artif Intell Med. (2021) 117:102087. doi: 10.1016/j.artmed.2021.102087
57. Chen T, Xu J, Ying H, Chen X, Feng R, Fang X, et al. Prediction of extubation failure for intensive care unit patients using light gradient boosting machine. IEEE Access. (2019) 7:150960–68. doi: 10.1186/s13040-022-00309-7
58. Swets JA. Measuring the accuracy of diagnostic systems. Science. (1988) 240:1285–93. doi: 10.1126/science.3287615
59. Conti G, Mantz J, Longrois D, Tonner P. Sedation and weaning from mechanical ventilation: time for ‘best practice’ to catch up with new realities? Multidiscip Respir Med. (2014) 9:45. doi: 10.1186/2049-6958-9-45
60. Goldstone J. The pulmonary physician in critical care. 10: difficult weaning. Thorax. (2002) 57:986–91. doi: 10.1136/thorax.57.11.986
61. Montani S, Striani M. Artificial intelligence in clinical decision support: a focused literature survey. Yearb Med Inform. (2019) 28:120–7.
62. Reddy S, Fox J, Purohit MP. Artificial intelligence-enabled healthcare delivery. J R Soc Med. (2019) 112:22–8.
63. Hung CM, Shi HY, Lee PH, Chang CS, Rau KM, Lee HM, et al. Potential and role of artificial intelligence in current medical healthcare. Artif Intell Cancer. (2022) 3:1–10.
64. Tarassenko L, Watkinson P. Artificial intelligence in health care: enabling informed care. Lancet. (2018) 391:1260. doi: 10.1016/S0140-6736(18)30701-3
Keywords: artificial intelligence, machine learning, intensive care unit, weaning mechanical ventilation, optimal weaning timing
Citation: Liu C-F, Hung C-M, Ko S-C, Cheng K-C, Chao C-M, Sung M-I, Hsing S-C, Wang J-J, Chen C-J, Lai C-C, Chen C-M and Chiu C-C (2022) An artificial intelligence system to predict the optimal timing for mechanical ventilation weaning for intensive care unit patients: A two-stage prediction approach. Front. Med. 9:935366. doi: 10.3389/fmed.2022.935366
Received: 03 May 2022; Accepted: 11 October 2022;
Published: 18 November 2022.
Edited by:
Qinghe Meng, Upstate Medical University, United StatesReviewed by:
I-Shiang Tzeng, National Taipei University, TaiwanRishikesan Kamaleswaran, Emory University, United States
Copyright © 2022 Liu, Hung, Ko, Cheng, Chao, Sung, Hsing, Wang, Chen, Lai, Chen and Chiu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chong-Chi Chiu, Y2hpdWNob25nY2hpQGdtYWlsLmNvbQ==; Chin-Ming Chen, Y2hlbmNtMzM4M0BnbWFpbC5jb20=
†These authors have contributed equally to this work