
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Med., 11 July 2022
Sec. Rheumatology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.926500
This article is part of the Research TopicNew Insights into Autoinflammatory Diseases: From Bench to BedsideView all 13 articles
 Antonio Vitale1
Antonio Vitale1 Valeria Caggiano1
Valeria Caggiano1 Francesca Della Casa2
Francesca Della Casa2 José Hernández-Rodríguez3
José Hernández-Rodríguez3 Micol Frassi4
Micol Frassi4 Sara Monti5,6
Sara Monti5,6 Abdurrahman Tufan7
Abdurrahman Tufan7 Salvatore Telesca1Edoardo Conticini1
Salvatore Telesca1Edoardo Conticini1 Gaafar Ragab8,9Giuseppe Lopalco10
Gaafar Ragab8,9Giuseppe Lopalco10 Ibrahim Almaghlouth11,12
Ibrahim Almaghlouth11,12 Rosa Maria R. Pereira13
Rosa Maria R. Pereira13 Derya Yildirim7
Derya Yildirim7 Marco Cattalini14Achille Marino15
Marco Cattalini14Achille Marino15 Teresa Giani16
Teresa Giani16 Francesco La Torre17Piero Ruscitti18Emma Aragona19
Francesco La Torre17Piero Ruscitti18Emma Aragona19 Ewa Wiesik-Szewczyk20
Ewa Wiesik-Szewczyk20 Emanuela Del Giudice21
Emanuela Del Giudice21 Petros P. Sfikakis22
Petros P. Sfikakis22 Marcello Govoni23
Marcello Govoni23 Giacomo Emmi24
Giacomo Emmi24 Maria Cristina Maggio25
Maria Cristina Maggio25 Roberto Giacomelli26
Roberto Giacomelli26 Francesco Ciccia27
Francesco Ciccia27 Giovanni Conti28
Giovanni Conti28 Djouher Ait-Idir29Claudia Lomater30Vito Sabato31
Djouher Ait-Idir29Claudia Lomater30Vito Sabato31 Matteo Piga32Ali Sahin33Daniela Opris-Belinski34Ruxandra Ionescu34
Matteo Piga32Ali Sahin33Daniela Opris-Belinski34Ruxandra Ionescu34 Elena Bartoloni35
Elena Bartoloni35 Franco Franceschini4
Franco Franceschini4 Paola Parronchi24
Paola Parronchi24 Amato de Paulis2,36
Amato de Paulis2,36 Gerard Espinosa3Armin Maier37Gian Domenico Sebastiani38
Gerard Espinosa3Armin Maier37Gian Domenico Sebastiani38 Antonella Insalaco39Farhad Shahram40
Antonella Insalaco39Farhad Shahram40 Paolo Sfriso41Francesca Minoia42Maria Alessio43Joanna Makowska44
Paolo Sfriso41Francesca Minoia42Maria Alessio43Joanna Makowska44 Gülen Hatemi45
Gülen Hatemi45 Nurullah Akkoç46
Nurullah Akkoç46 Francesca Li Gobbi47
Francesca Li Gobbi47 Antonio Gidaro48
Antonio Gidaro48 Alma Nunzia Olivieri49
Alma Nunzia Olivieri49 Sulaiman M. Al-Mayouf50
Sulaiman M. Al-Mayouf50 Sükran Erten51Stefano Gentileschi52Ibrahim Vasi7Maria Tarsia1Ayman Abdel-Monem Ahmed Mahmoud8Bruno Frediani52Musa Fares Alzahrani53Ahmed Hatem Laymouna8Francesca Ricci14
Sükran Erten51Stefano Gentileschi52Ibrahim Vasi7Maria Tarsia1Ayman Abdel-Monem Ahmed Mahmoud8Bruno Frediani52Musa Fares Alzahrani53Ahmed Hatem Laymouna8Francesca Ricci14 Fabio Cardinale17
Fabio Cardinale17 Karina Jahnz-Rózyk20
Karina Jahnz-Rózyk20 Gian Marco Tosi54
Gian Marco Tosi54 Francesca Crisafulli4Alberto Balistreri55Marília A. Dagostin13Mahmoud Ghanema8
Francesca Crisafulli4Alberto Balistreri55Marília A. Dagostin13Mahmoud Ghanema8 Carla Gaggiano1Jurgen Sota1
Carla Gaggiano1Jurgen Sota1 Ilenia Di Cola18
Ilenia Di Cola18 Claudia Fabiani54
Claudia Fabiani54 Henrique A. Mayrink Giardini13
Henrique A. Mayrink Giardini13 Alessandra Renieri56,57,58Alessandra Fabbiani56,57,58Anna Carrer56,57,58Monica Bocchia59
Alessandra Renieri56,57,58Alessandra Fabbiani56,57,58Anna Carrer56,57,58Monica Bocchia59 Federico Caroni59
Federico Caroni59 Donato Rigante60,61†
Donato Rigante60,61† Luca Cantarini1*†
Luca Cantarini1*†Objective: The aim of this paper is to present the AutoInflammatory Disease Alliance (AIDA) international Registry dedicated to Vacuoles, E1 enzyme, X-linked, Autoinflammatory, Somatic (VEXAS) syndrome, describing its design, construction, and modalities of dissemination.
Methods: This Registry is a clinical, physician-driven, population- and electronic-based instrument designed for the retrospective and prospective collection of real-life data. Data gathering is based on the Research Electronic Data Capture (REDCap) tool and is intended to obtain real-world evidence for daily patients' management. The Registry may potentially communicate with other on-line tools dedicated to VEXAS syndrome, thus enhancing international collaboration and data sharing for research purposes. The Registry is practical enough to be easily modified to meet future needs regarding VEXAS syndrome.
Results: To date (April 22nd, 2022), 113 Centers from 23 Countries in 4 continents have been involved; 324 users (114 Principal Investigators, 205 Site Investigators, 2 Lead Investigators, and 3 data managers) are currently able to access the registry for data entry (or data sharing) and collection. The Registry includes 4,952 fields organized into 18 instruments designed to fully describe patient's details about demographics, clinical manifestations, symptoms, histologic details about skin and bone marrow biopsies and aspirate, laboratory features, complications, comorbidities, therapies, and healthcare access.
Conclusion: This international Registry for patients with VEXAS syndrome will allow the achievement of a comprehensive knowledge about this new disease, with the final goal to obtain real-world evidence for daily clinical practice, especially in relation to the comprehension of this disease about the natural history and the possible therapeutic approaches. This Project can be found on https://clinicaltrials.gov NCT05200715.
VEXAS (Vacuoles, E1 enzyme, X-linked, Autoinflammatory, Somatic) syndrome is a recently recognized pathological entity first reported in December 2020. VEXAS represents a monogenic autoinflammatory condition caused by acquired somatic mutations in UBA1, gene encoding one of the two E1 enzyme isoforms that initiates ubiquitylation in cell's cytoplasm. Unlike other genetic autoinflammatory syndromes, which are due to germline mutations in most of cases, VEXAS syndrome is caused by acquired variants in blood cells precursors, especially myeloid progenitors (1). Because of its recent identification, VEXAS clinical features, complications, outcome, and treatment strategies are not fully established at current. However, it is clearly characterized by prominent inflammation involving almost all organs and tissues with highly increased inflammatory markers. The skin, eyes, lungs, joints, and gastrointestinal system are frequently affected by the disease, with a quite protean range of inflammatory manifestations. Besides these clinical features, which account for a common ground with other “historical” autoinflammatory diseases, hematologic involvement represent the most typical disease manifestation. Indeed, hematological involvement is observed in at least 50% of patients, with myelodysplastic syndrome (MDS) representing the most frequent bone marrow affection. Monoclonal gammopathy with unknown significance (MGUS), macrocytic anemia with normal vitamin B12 and folate levels, leukopenia, and thrombocytopenia are additional hematological features. Noteworthy, marked cytoplasmic vacuolization in hematopoietic precursors are often observed in bone marrow aspirate smears, which represent a good diagnostic clue. Vacuoles are generally identified in erythroid and myeloid precursors (blasts, promyelocytes, and pronormoblasts), but are also observed in eosinophils, monocytes, plasma cells, and megakaryocytes to a lesser degree (2).
At current there is no data about the effective epidemiological burden of VEXAS syndrome, which as to be consider a rare disease based on the current prevalence. Therefore, as with other rare diseases, VEXAS syndrome may benefit from patient registries capable of leading to a better understanding of the disease in a relatively short time. In particular, patient registries are overcoming current research approaches, especially for rare diseases. International registries have the potential to recruit a wide number of patients worldwide and follow enrolled subjects for very long periods of time. The importance of patient registries in the field of rare diseases is shown by the relevance provided by the European Union (EU) to this online tool, making available specific guidelines for high-quality registries (3–5).
Regarding autoinflammatory diseases, the AutoInflammatory Disease Alliance (AIDA) has already developed and launched eight international registries for patients with many rare autoinflammatory diseases (6–8). The AIDA Project has already allowed the construction of an international Network of physicians and researchers interested in putting together information to expand current evidence about monogenic autoinflammatory diseases, Still's disease, Schnitzler's syndrome, Behçet's disease, periodic fever, aphthous stomatitis, pharyngitis, cervical adenitis (PFAPA) syndrome, non-infectious uveitis, non-infectious scleritis, and undifferentiated systemic autoinflammatory diseases (USAIDs). For more details, the AIDA Network may be accessed at the following website: https://aidanetwork.org/en/.
Based on the experience of the AIDA Network in developing registries for rare autoinflammatory diseases, an international patient Registry specifically dedicated to VEXAS syndrome has been developed. This manuscript aims to illustrate the objectives, design, methodology and modalities of diffusion underlying the development and activation of the VEXAS Registry.
The AIDA Registry presented in this work has been created as an international, clinical, physician-driven, population- and electronic-based registry dedicated to patients diagnosed with VEXAS syndrome.
Data collection includes a retrospective phase, for data gathered up to the time of the enrolment in the Registry, and a prospective phase for progressive data available starting from the time of the enrolment. The prospective phase requires the collection of at least one follow-up visit per year. However, prospective data collection should be performed whenever a change in the treatment strategy occurs.
The Registry is designed to collect demographic, genetic, clinical, laboratory and treatment data starting since the disease onset. These data will be essentially derived from the routine follow-up visits performed to guarantee the best standard of care, while no additional information will be required. In the same way, none of the treatment choices and drug adjustments will be influenced by the participation to this Project. Indeed, physicians' clinical judgement based on current evidence represents the only factor capable of determining the therapeutic management of the patient.
The access is open for all Centers dealing with the management, diagnosis, and treatment of VEXAS syndrome. The Centers that would like to participate, may join the AIDA Network by contacting the Promoter or sending an email to the AIDA Team by writing to c3VwcG9ydEBhaWRhcmVnaXN0cnkub3Jn or using a specific form, that may be found at the following page: https://aidanetwork.org/en/aida.
All clinical specialities are included in the AIDA Network; the location and the type of practice setting do not influence the inclusion in this Project. As data inserted in the Registry are usually included in the standard management of VEXAS patients, no costs or financial fees are settled. As an essential prerequisite for the inclusion in this Project, each Center must obtain the approval from the local ethics committee. Also, it is essential to identify a Principal Investigator for the local coordination of the study and at least a Site Investigator, who will manage documentation and take care of data collection. Both the Principal Investigator and the Site Investigator will receive the credentials to enter the Registry and start patients' enrolment after having expressed the formal intention to participate in the VEXAS Registry.
The Registry for patients with VEXAS syndrome is primarily aimed at gathering information from the larger number of patients as possible. A large cohort of patients is critical to obtain solid evidence from data analysis and transfer the results into daily clinical practice. A further objective of the Registry is to learn about VEXAS syndrome in detail and in a rapid manner, avoiding the delays that would inevitably result from traditional clinical research, which generally relies on limited study populations available at a single research center.
Additional objectives of this Project are: (I) to fully characterize the wide spectrum of inflammatory manifestations and their frequency; (II) to eventually identify different disease subtypes; (III) to describe mutations that will be found in the UBA1 gene, to differentiate among pathogenic or likely pathogenic variants from benign polymorphisms; (IV) to search for genotype-phenotype associations; (V) to study the influence of other mutations on genes associated with monogenic autoinflammatory diseases; (VI) to identify any pathognomonic features to facilitate diagnosis; (VII) to develop classification criteria and diagnostic algorithms to be applied in clinical practice to select patients for genetic assessment; (VIII) to identify variables capable of distinguishing VEXAS patients from other mimicking diseases; (IX) to fully understand the possible spectrum of haematologic disorders; (X) to describe hematologic and non-hematologic complications occurred in the long-term; (XI) to better characterize information from bone marrow biopsy and aspirate; (XII) to search for prognostic factors able to select patients with a higher probability to develop complications; (XIII) to recognize predisposing factors and triggers associated with the onset and disease's exacerbations, quantifying and stratifying the severity of the features; (XIV) to describe treatment attempts, taking in to account their efficacy as a whole and the impacts on the different aspect of the disease; (XV) to report the safety profile of single treatment approaches in VEXAS patients; (XVI) identifying the better treatment approach tapered on the patient's features and disease characteristics; (XVII) to carefully study treatment dosages and their changes to develop standardized treatment protocols; (XVIII) to asses any influence of the environmental background and the ethnic origin on the VEXAS syndrome phenotype; (XIX) to assess any impact of the socioeconomic status in terms of access to healthcare and patients' absenteeism due to the disease; (XX) to monitor the cardiovascular risk in such patients; (XXI) to monitor the causes of death in VEXAS syndrome.
Other pioneering studies will be eventually designed according to the unmet needs arising from patients' management over time.
Table 1 summarizes primary and additional objectives of this Registry.
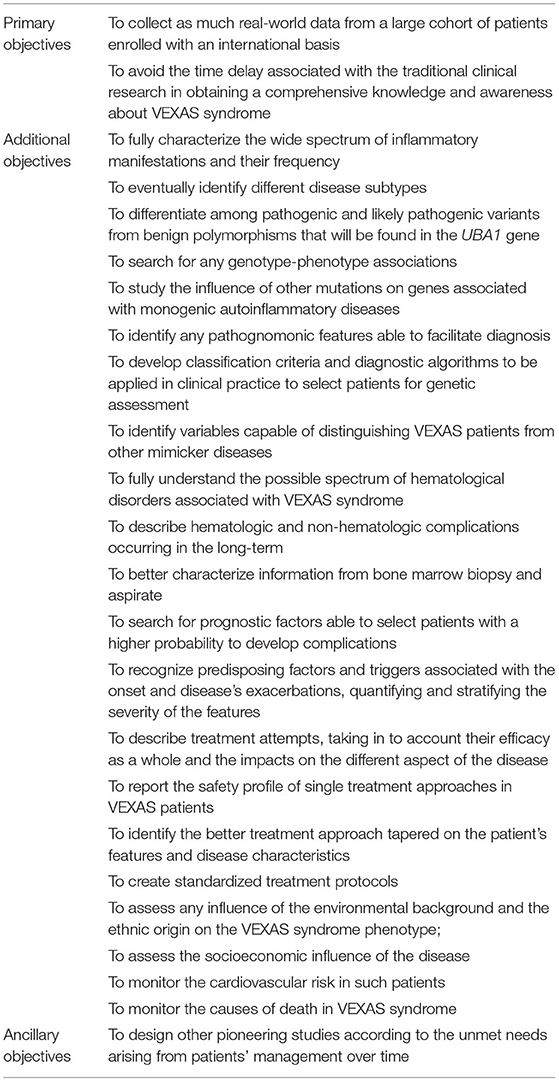
Table 1. Objectives considered for the implementation of the AIDA registry for patients with VEXAS (vacuoles, E1 enzyme, X-linked, autoinflammatory, somatic) syndrome.
Patients carrying a UBA1 gene somatic mutation and showing an inflammatory phenotype may be included in the Registry.
The patient has to give the written and informed consent after a careful explanation of the Project: the objectives of the Registry, the lack of implications on clinical management and treatment, the opportunity to withdraw the consent at any time, and the laws to comply with to guarantee patients' privacy, anonymity and security of data. Patients have to be ensured about the lack of consequences deriving from her/his will to participate or not to the study.
For patients unable to provide their consent, this should be given by legally authorized representatives, who must observe the study requirements for the entire duration of the study or until the consent withdrawal. In any case, the patient's assent is essential for patients aged ≥12 years.
No exclusion criteria or conditions are previewed to the enrolment.
The Research Electronic Data Capture (REDCap) instrument has been used for data gathering and storing. REDCap is an electronic data collector produced at Vanderbilt University Medical Center (VUMC). It is currently located at the Virginia Commonwealth University (Award Number UL1TR002649). The employment of the REDCap platform is free to all the members of the REDCap consortium, which may benefit from using the tool in return for technical support. At current, take part in the REDCap consortium from the 4 continents over 5,600 worldwide institutions from 144 Countries already (9). To access the Registry, Principal Investigators and Site Investigators have to enter their own username and password. The Registry is available at the webpage https://aidanetwork.org/en/register/vexas. Data are kept on the servers of the University of Siena, Siena, Italy. Privacy is ensured for each Centre's data, with Principal and Site Investigators unable to access data collected in other Centers.
The Registry's browser interface provided for the data entry is entirely supplied in English in order to reduce the language barriers and facilitate the international data collection.
The retrospective assessment requires the collection of clinical and laboratory data referring to the symptoms of the disease at the onset, at the diagnosis, and at the enrollment into the Registry; clinical and laboratory data would be inserted referring to the start of each treatment performed, the 3-, 6- and 12-month visits and at the last assessment. On the other hand, follow-up visits will be added at the visits performed after the inclusion in the AIDA Registry; follow-up assessments should be filled in at least every year and at any change in the treatment strategy, as for the introduction of new drugs and posology changes. Socioeconomic data include variables embedded to assess the impact of VEXAS syndrome on the national health care system (access to primary care physician, specialist visits, laboratory examinations, imaging tests, access to emergency care and hospitalization) and on the working world (absenteeism and presenteeism).
The Investigators will be responsible for the own study data introduced in the online Registry and for the precision of the information accrued; the Principal Investigator is required to check for the accuracy of the data. The online access through personal username and password guarantees the security of the patients' information.
In June 2019 the Ethics Committee of the Azienda Ospedaliero-Universitaria Senese, Siena, Italy (Ref. N. 14951) granted the first national regulatory approval for the AIDA Project. After that, Centers experienced with diagnosis, clinical management, and treatment of autoinflammatory diseases have joined the AIDA Network from Europe, Middle East, Africa and America.
Patients' information is kept in accordance with the EU General Data Protection Regulations (GDPR) on the processing of personal data and the protection of privacy (2016/679/EU) (10), or other counterparts.
Regarding the patients' voluntary informed consent, the AIDA registries meet the recommendations from the Declaration of Helsinki. For minor patients aged ≥12 years the assent is also required when the patient is not competent to provide the consent. In these cases, parents/legal guardians have to provide their authorization to allow the patient's participation in the Project.
Consent for processing data for statistical or research purposes may be withdrawn at any time by either patients or Principal Investigators. In these cases, no further information will be captured; moreover, the patient has the right to obtain the complete erasure of all personal data already gathered in the Registry if required and notified to the study Promoter (University of Siena).
No financial remuneration is planned for patients or physicians for the study participation; in addition, there is no evidence of any billing relationships with the national health systems or insurance companies.
Statistical analysis will be based on the specific type and nature of data undergoing computation and will be performed according to the specific objectives of the studies conducted on behalf of the AIDA Network. In any case, the analysis will embrace general principles of descriptive statistics, correlations between groups and comparisons between subgroups. Details about statistics will be provided in the future papers obtained from data collected in the VEXAS Registry.
Principal Investigators and Site Investigators are encouraged to put forward their study proposals during the AIDA meetings. The data collected in a center may be analyzed by satellite centers independently from the other centers on condition that the AIDA Network appears among acknowledgments. On the contrary, the totality of data collected in the Registry will be managed by statistics and physicians involved in the network and selected based on their field of expertise.
The development and activation of this AIDA Registry is a first fundamental result of the AIDA Network. In this regard, an international registry dedicated to VEXAS syndrome is essential to extensively gather real-life data in a quick manner.
To date, 23 nations in 4 continents (Algeria, Argentina, Belgium, Brazil, Chile, Egypt, Germany, Ghana, Greece, Iran, Italy, Lebanon, Morocco, Mexico, Poland, Portugal, Romania, Saudi Arabia, Spain, Taiwan, Turkey, United States, Zimbabwe) have already joined the AIDA Network. The Figure 1 highlights the current (April 22nd, 2022) worldwide distribution of the AIDA Network.
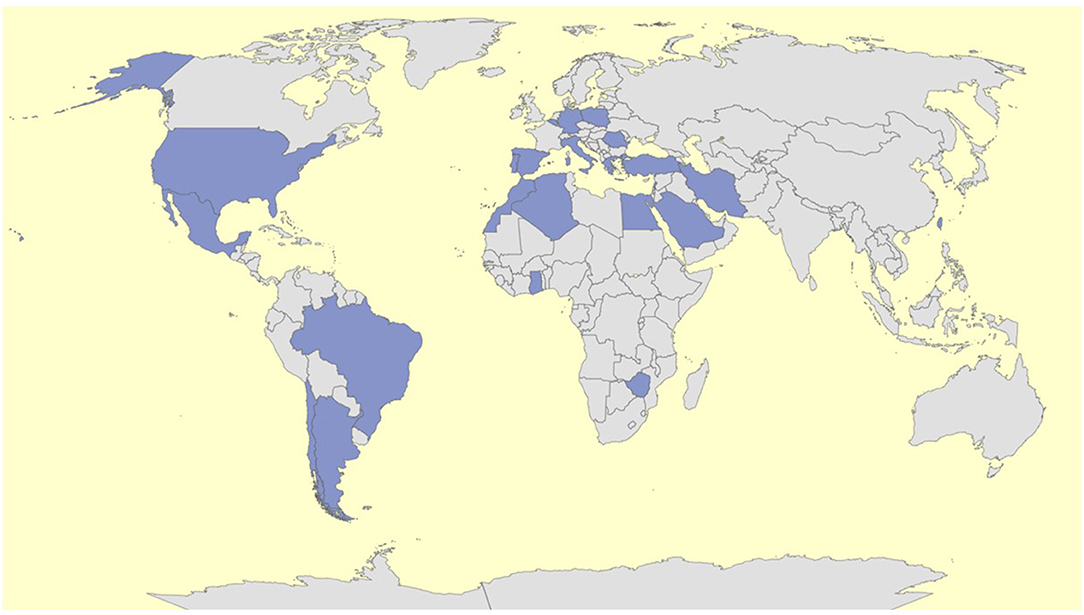
Figure 1. Worldwide distribution of the AIDA network on 22nd of April 2022.
Overall, 113 Centers around the world have joined the AIDA project for a total of 324 users (114 principal investigators, 205 site investigators, 2 lead investigators, 3 data managers). This Project was registered at ClinicalTrials.gov (ID: NCT05200715).
When choosing the clinical variables constituting the Registry, information useful for a valuable knowledge of VEXAS syndrome was included, in order to quickly obtain data and comprehensively understand this new clinical entity in a relatively short time. For this reason, the registry was developed to comprehensively trace the entire clinical and therapeutic history of the patients enrolled. To date (April 22nd, 2022), the Registry contain 4,952 common data elements (each corresponding to a study variable) organized into 18 instruments. Thirteen of these instruments are specifically built to collect retrospective information, one instrument is dedicated to the prospective phase and 4 instruments should be used both to collect retrospective information and to describe any change starting from the time of the enrolment. Table 2 provides more detailed information about the instruments included in this Registry, the phases they refer to and the number of fields they include.
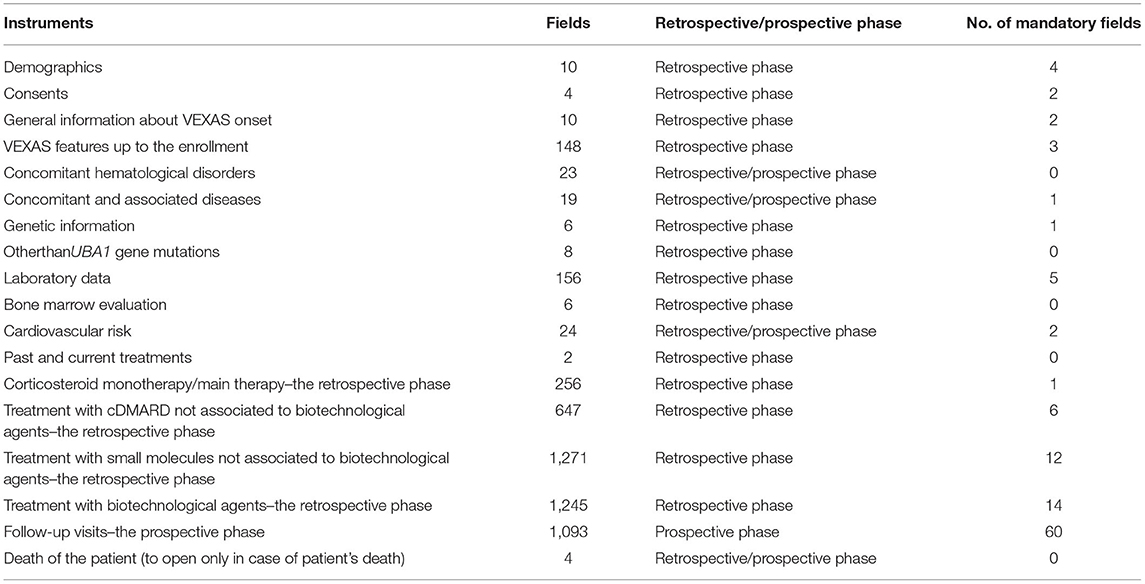
Table 2. Panel of instruments constituting the registry dedicated to subject with VEXAS (vacuoles, E1 enzyme, X-linked, autoinflammatory, somatic) syndrome; the number of common data elements are also provided along with the phase (i.e., retrospective/prospective) at which they should refer.
Common data elements consist of demographic, clinical, instrumental, histological, laboratory, therapeutic and any other medical variable required to fully describe disease course. Many of these are shared with other AIDA registries dedicated to different autoinflammatory and non-infectious ocular diseases, to facilitate the merging of data among different Registries.
Each variable will require to be answered only in case it is useful according with the patient's clinical picture. This is allowed by a branching mechanism that will drive the opening of the answers only in case it will be necessary to complete a previously provided information. Therefore, only a small number of the 4,952 variables will appear to the investigators.
As for other autoinflammatory diseases, patients and patients' associations play a pivotal role in supporting data collection and the diffusion of the Project. Indeed, patients may stimulate Centers to join the Project, provide their own time for data collection, and supply patient's reported outcomes.
The associations of patients were invited to furnish patients' opinion about how to develop this AIDA Registry since the very beginning of the project. In particular, patients' point of view and impressions were required before creating variables and instruments of the Registry, while concerns, related to the use of sensitive data were solved together. In order to meet patients' expectations, a Registry focused on the different aspects of VEXAS syndrome was developed. In this way, clinical, laboratory, and therapeutic unmet needs will be widely investigated without giving preference to a single field.
The AIPF (Associazione Italiana Febbri Periodiche), the ANMAR (Associazione Nazionale Malati Reumatici) and the APMARR (Associazione Nazionale Persone con Malattie Reumatologiche e Rare) are currently giving their active support. To date, on Italian patients' organizations are included in the project; however, other international patient advocatory groups are about to join AIDA worldwide.
VEXAS syndrome is a very recently identified autoinflammatory disorder caused by acquired somatic mutations of UBA1 gene in blood cells precursors. Despite the genetic origin, the epidemiological burden could be much higher than that characterizing hereditary periodic fevers. In addition to the knowledge gap about the prevalence, all the clinical aspects of the disease should be widely explored, especially in relation to the optimal therapeutic approach to use. As for other autoinflammatory diseases (11), treatment should be based on the specific disease manifestations, the long-term outcome, and complications arising over time. The use of a patient registry can dramatically facilitate these goals, allowing a better knowledge of the disease in a relatively shorter time.
Regardless of the real impact that this disease has in the population, VEXAS is to be considered a rare disease at present. Therefore, as for other autoinflammatory diseases (6–8), we have developed and launched a Registry capable of gathering the few real-life data available worldwide. While waiting for randomized controlled clinical trials, which are likely to take many years for their conduction, a registry dedicated to VEXAS syndrome can lead to the rapid collection of real-life data from a sufficiently large number of patients. This will allow the scientific community to achieve solid results that may be applied on VEXAS patients in daily clinical practice.
Of note, the AIDA Network is intended both to enable a broad population-based data collection and to enhance international collaboration, focusing the research efforts on international projects. In this regard, the first steps will be to reach a full knowledge about VEXAS clinical manifestations and their frequency, pointing out rare and atypical disease expressions. Furthermore, it is essential to describe the UBA1 mutations really capable of determining VEXAS syndrome, highlighting pathogenic or likely pathogenic variants from benign polymorphisms. Actually, as for other genetic autoinflammatory conditions, low-penetrance variants and genotype-phenotype correlations may be described (12, 13).
It would be useful to search for any pathognomonic element capable to easily direct the diagnosis and genetic examination. In this regard, the presence of vacuoles and their number could be a central diagnostic factor, but their sensitivity and specificity should be confirmed on a wide number of patients (14). Similarly, bone marrow biopsy and aspirate can provide diagnostic or prognostic data that should be clarified.
Another focus of research should be to comprehensively disclose all the possible expressions of long-term hematologic involvement, revealing any predictive factors and complications. To date, it is well-known that VEXAS patients often present a hematological involvement with myelodysplastic syndrome, monoclonal gammopathy with unknown significance (MGUS), macrocytic anemia, and thrombocytopenia. However, myeloid malignancies are also frequently described in such patients (2, 15). These data must be confirmed and expanded in large cohorts, while a proper long-term follow-up should reveal all the various hematological aspects.
If VEXAS syndrome is only little known as a whole, the lesser-known aspect is the proper therapeutic approach. Many treatments have been tested in VEXAS syndrome, including glucocorticoids, conventional disease-modifying antirheumatic drugs (cDMARDs), azacytidine, biologically targeted agents and janus kinase (JAK) inhibitors. Except for corticosteroids, which are especially useful at high dosage, preliminary data show a significant interindividual variability in the effectiveness of these therapeutic strategies (1, 16). Therefore, identifying the better treatment approach based on the patient's features could allow the optimal treatment in the perspective of a personalized medicine. Similarly, the identification of the best dosages and the assessment of long-term safety profile represent indispensable goals to ensure a correct management.
As for other AIDA registries (6–8), the assessment of the socioeconomic influence of the disease on the national healthcare systems, on patients' social role and job impact represent an intriguing subject of analysis. Other objectives will be identified based on the challenges that clinical practice and scientific research will bring forward in the coming years. The Registry benefits from a remarkable plasticity and it may adapt to changes that will be required according to future acquisitions. In addition, the registry boasts the capability to communicate with other present or future registries dedicated to VEXAS syndrome; this will further enhance research projects through the merging of collected information.
Noteworthy, a new online tool defined as “AIDA for patients” is under development. “AIDA for patients” is an instrument primarily aimed at including patients in the network in terms of diffusion of the project, sharing of research strategies, outreach to physicians in the various centers toward a better and wider enrollment, and involvement of the patients themselves in providing their own data.
Since this disorder has been discovered only in recent times, there are not yet associations specifically dedicated to VEXAS syndrome; for this reason, existing associations of patients with rare rheumatological diseases have been involved.
The AIDA Registry for patients with VEXAS syndrome shows the typical limitations of observational studies. In particular, the completeness and accuracy of information accrued in the Registry accounts for the main issues of the retrospective phase. Furthermore, there is no obligation to consecutively enroll all the patients followed in the AIDA Centers, and this may cause an unintended selection bias. Enrolling patients in the Registry needs much time and attention, especially when the patient's history is remarkably long due to the complex clinical framework and numerous treatments approaches. Therefore, both investigators and patients enrolled have to be sensitized as to provide their time for the study purposes. This is especially true for the retrospective phase, which requires from 1–3 h for a complete data collection. Conversely, the prospective phase does not affect substantially physicians and patients' time, as 10 min are required to fill-in the follow-up page. Beyond these limitations, this Registry represents an unvaluable tool to fully understand the disease in terms of clinical management and treatment. Furthermore, the Registry may be a source for patients' enrolment in future randomized clinical trials.
The AIDA international Registry dedicated to patients affected by VEXAS syndrome has been made available for data collection. Joining the AIDA project in reference to the VEXAS Registry will allow the achievement of a comprehensive knowledge about this new disease in a relatively short time. The final goal of this Project will be to conduct observational and prospective studies leading to real-world evidence to be applied in the everyday clinical practice for patients with VEXAS syndrome.
The studies involving human participants were reviewed and approved by Ethics Committee of the Azienda Ospedaliero-Universitaria Senese, Siena, Italy (Ref. N. 14951). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
AV wrote the first draft of the manuscript, conceived and designed the study, and the registry for VEXAS syndrome. VC, FD, JH-R, MF, SM, AT, ST, and EC actively enrolled patients in the registry for VEXAS syndrome. GR, GL, IA, RP, DY, MC, AMar, TG, FLT, PR, EA, EW-S, ED, PSfi, MGo, GEm, MM, RG, FCi, GC, DA-I, CL, VS, MP, AS, DO-B, RI, EB, FF, PP, AP, GEs, AMai, GS, AI, FS, PSfr, FM, MAle, JM, GH, NA, FLG, AG, AO, SA-M, SE, and SG were the principal investigators of centers actively enrolling in the AIDA registries. IV, MT, AMah, MAlz, AL, FR, FCard, KJ-R, FCr, MD, MGh, CG, JS, ID, CF, HG, AF, AC, MB, and FCaro were included in the authorship as investigators from to the three top contributor centers for any of the other AIDA registries. GT, AR, BF, and MB actively contributed to the launching of the registry dedicated to VEXAS syndrome. AB involved in the technical management of the platform and registries. DR took care of the final revision of the manuscript. LC conceived and designed the study and accounted for AIDA registries coordinator. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Beck DB, Ferrada MA, Sikora KA, Ombrello AK, Collins JC, Pei W, et al. Somatic mutations in UBA1 and severe adult-onset autoinflammatory disease. N Engl J Med. (2020) 383:2628–38. doi: 10.1056/NEJMoa2026834
2. Obiorah IE, Patel BA, Groarke EM, Wang W, Trick M, Ombrello AK, et al. Benign and malignant hematologic manifestations in patients with VEXAS syndrome due to somatic mutations in UBA1. Blood Adv. (2021) 5:3203–15. doi: 10.1182/bloodadvances.2021004976
3. Rare diseases. Public Health - European Commission. (2016). Available online at: https://ec.europa.eu/health/non_communicable_diseases/rare_diseases_en (accessed December 4, 2021).
4. Boulanger V, Schlemmer M, Rossov S, Seebald A, Gavin P. Establishing patient registries for rare diseases: rationale and challenges. Pharmaceut Med. (2020) 34:185–90. doi: 10.1007/s40290-020-00332-1
5. Kodra Y, Weinbach J, Posada-de-la-Paz M, Coi A, Lemonnier SL, van Enckevort D, et al. Recommendations for Improving the Quality of Rare Disease Registries. Int J Environ Res Public Health. (2018) 15:1644. doi: 10.3390/ijerph15081644
6. Della Casa F, Vitale A, Pereira RM, Guerriero S, Ragab G, Lopalco G, et al. Development and implementation of the AIDA international registry for patients with non-infectious scleritis. Ophthalmol Ther. (2022) 11:887–97. doi: 10.1007/s40123-022-00466-2
7. Della Casa F, Vitale A, Pereira RM, Guerriero S, Ragab G, Lopalco G, et al. Development and implementation of the AIDA international registry for patients with non-infectious uveitis. Ophthalmol Ther. (2022) 11:899–911. doi: 10.1007/s40123-022-00459-1
8. Vitale A, Della Casa F, Lopalco G, Pereira RM, Ruscitti P, Giacomelli R, et al. Development and implementation of the AIDA international registry for patients with Still's disease. Front Med. (2022) 9:878–797. doi: 10.3389/fmed.2022.878797
9. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG, et al. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
10. EUR-Lex - 32016R0679 - EN - EUR-Lex. Available online at: https://eur-lex.europa.eu/eli/reg/2016/679/oj (accessed December 21, 2021).
11. ter Haar NM, Oswald M, Jeyaratnam J, Anton J, Barron KS, Brogan PA, et al. Recommendations for the management of autoinflammatory diseases. Ann Rheum Dis. (2015) 74:1636–44. doi: 10.1136/annrheumdis-2015-207546
12. Dundar M, Fahrioglu U, Yildiz SH, et al. Clinical and molecular evaluation of MEFV gene variants in the Turkish population: a study by the National Genetics Consortium. Funct Integr Genomics. (2022) 22:291–315. doi: 10.1007/s10142-021-00819-3
13. Papa R, Doglio M, Lachmann HJ, Ozen S, Frenkel J, Simon A, et al. A web-based collection of genotype-phenotype associations in hereditary recurrent fevers from the Eurofever registry. Orphanet J Rare Dis. (2017) 12:167. doi: 10.1186/s13023-017-0720-3
14. Lacombe V, Prevost M, Bouvier A, Thépot S, Chabrun F, Kosmider O, et al. Vacuoles in neutrophil precursors in VEXAS syndrome: diagnostic performances and threshold. Br J Haematol. (2021) 195:286–9. doi: 10.1111/bjh.17679
15. Staels F, Betrains A, Woei-A-Jin FJSH, Boeckx N, Beckers M, Bervoets A, et al. Case report: VEXAS syndrome: from mild symptoms to life-threatening macrophage activation syndrome. Front Immunol. (2021) 12:678927. doi: 10.3389/fimmu.2021.678927
Keywords: autoinflammatory diseases, clinical management, precision medicine, rare diseases, research, treatment
Citation: Vitale A, Caggiano V, Della Casa F, Hernández-Rodríguez J, Frassi M, Monti S, Tufan A, Telesca S, Conticini E, Ragab G, Lopalco G, Almaghlouth I, Pereira RMR, Yildirim D, Cattalini M, Marino A, Giani T, La Torre F, Ruscitti P, Aragona E, Wiesik-Szewczyk E, Del Giudice E, Sfikakis PP, Govoni M, Emmi G, Maggio MC, Giacomelli R, Ciccia F, Conti G, Ait-Idir D, Lomater C, Sabato V, Piga M, Sahin A, Opris-Belinski D, Ionescu R, Bartoloni E, Franceschini F, Parronchi P, de Paulis A, Espinosa G, Maier A, Sebastiani GD, Insalaco A, Shahram F, Sfriso P, Minoia F, Alessio M, Makowska J, Hatemi G, Akkoç N, Li Gobbi F, Gidaro A, Olivieri AN, Al-Mayouf SM, Erten S, Gentileschi S, Vasi I, Tarsia M, Mahmoud AA-MA, Frediani B, Fares Alzahrani M, Laymouna AH, Ricci F, Cardinale F, Jahnz-Rózyk K, Tosi GM, Crisafulli F, Balistreri A, Dagostin MA, Ghanema M, Gaggiano C, Sota J, Di Cola I, Fabiani C, Giardini HAM, Renieri A, Fabbiani A, Carrer A, Bocchia M, Caroni F, Rigante D and Cantarini L (2022) Development and Implementation of the AIDA International Registry for Patients With VEXAS Syndrome. Front. Med. 9:926500. doi: 10.3389/fmed.2022.926500
Received: 22 April 2022; Accepted: 21 June 2022;
Published: 11 July 2022.
Edited by:
Dario Roccatello, University of Turin, ItalyReviewed by:
Martin Krusche, University of Hamburg, GermanyCopyright © 2022 Vitale, Caggiano, Della Casa, Hernández-Rodríguez, Frassi, Monti, Tufan, Telesca, Conticini, Ragab, Lopalco, Almaghlouth, Pereira, Yildirim, Cattalini, Marino, Giani, La Torre, Ruscitti, Aragona, Wiesik-Szewczyk, Del Giudice, Sfikakis, Govoni, Emmi, Maggio, Giacomelli, Ciccia, Conti, Ait-Idir, Lomater, Sabato, Piga, Sahin, Opris-Belinski, Ionescu, Bartoloni, Franceschini, Parronchi, de Paulis, Espinosa, Maier, Sebastiani, Insalaco, Shahram, Sfriso, Minoia, Alessio, Makowska, Hatemi, Akkoç, Li Gobbi, Gidaro, Olivieri, Al-Mayouf, Erten, Gentileschi, Vasi, Tarsia, Mahmoud, Frediani, Fares Alzahrani, Laymouna, Ricci, Cardinale, Jahnz-Rózyk, Tosi, Crisafulli, Balistreri, Dagostin, Ghanema, Gaggiano, Sota, Di Cola, Fabiani, Giardini, Renieri, Fabbiani, Carrer, Bocchia, Caroni, Rigante and Cantarini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luca Cantarini, Y2FudGFyaW5pbHVjYUBob3RtYWlsLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.