
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med. , 02 June 2022
Sec. Ophthalmology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.926034
This article is part of the Research Topic Uveal Melanoma: From Lab Bench to Clinic - New Therapeutic Advances View all 7 articles
 Viktor Gill1,2*
Viktor Gill1,2* Christina Herrspiegel2,3Shiva Sabazade2,3Maria Fili3Louise Bergman3Bertil Damato3,4,5Stefan Seregard2,3
Christina Herrspiegel2,3Shiva Sabazade2,3Maria Fili3Louise Bergman3Bertil Damato3,4,5Stefan Seregard2,3 Gustav Stålhammar2,3
Gustav Stålhammar2,3Background: In contrast to most other cancers, uveal melanoma (UM) is characterized by an absence of major improvements in patient survival during the last several decades. In this study, we examine changes in incidence rates, patient age and tumor size at diagnosis, treatment practices and survival for patients diagnosed in Sweden during the period 1960–2010.
Methods: All patients diagnosed with posterior UM between January 1st, 1960, and December 31st, 2009, in Sweden, were included (n = 3898). Trends in incidence, primary treatment modality, patient age and tumor size were analyzed. Disease-specific survival was plotted in Kaplan–Meier curves and the cumulative incidence of UM-related mortality was evaluated in competing risk analysis.
Results: Crude (6.5–11.6 cases/million/year) and age-standardized incidence rates (5.6–9.6 cases/million/year) varied between individual years during the study period, but both had a stable linear trend overall (p ≥ 0.12). Gradually, plaque brachytherapy with ruthenium-106 replaced enucleation as the most common primary treatment. The mean patient age at diagnosis increased from 59.8 years in 1960 to 66.0 in 2009. Conversely, the mean tumor size became gradually smaller during the period. In linear regression, the basal diameter and tumor apical thickness decreased with a slope coefficient of −0.03 mm (p = 0.012) and −0.05 mm (p = 1.2 × 10–5) per year after 1960, respectively. Patients diagnosed after 1990 had significantly better disease-specific survival than patients diagnosed before 1990 (p = 2.0 × 10–17). Similarly, the cumulative incidence of UM-related mortality was highest for patients diagnosed 1960–1969 and 1970–1979, with slightly lower incidences for patients diagnosed 1980–1989 and even lower for those diagnosed after 1990 (p = 7.1 × 10–13). The incidence of mortality from other causes than UM did not differ between periods (p = 0.16).
Conclusion: In the period from 1960–2010, crude and age-standardized incidence rates of UM have remained stable in Sweden. Several other aspects have changed: Plaque brachytherapy with ruthenium-106 has replaced enucleation as the most common primary treatment modality; patients have become older and their tumors smaller at the time of diagnosis; and their survival has improved. This might indicate a beneficial survival effect of earlier diagnosis and treatment, but the potential influence from lead-time bias should be taken into consideration.
Within 10 years from diagnosis, 28–40% of patients diagnosed with uveal melanoma (UM) succumb to metastatic disease, and the relative survival has been estimated to be 66% (1–3). Although very few patients have detectable metastases at presentation, and virtually all undergo primary tumor treatment, it remains debated if primary tumor treatment has any effect on patient survival (4, 5). Calculations based on observed tumor doubling times indicate that systemic micrometastases could be present well before the primary tumor is detected (6–8). However, a recent meta-analysis of patients who underwent primary tumor treatment more than 5 years after diagnosis showed that 80–90% developed metastases, compared to the 35–50% of patients who received primary treatment, which suggests that there might be a beneficial therapeutic effect on survival after all (9).
Similarly, no effective treatment has been available once radiologically detectable metastases have developed (10, 11). Previous therapeutic regimes for metastatic disease include partial hepatectomy, conventional chemotherapy, chemoimmunotherapy, hepatic intra-arterial chemotherapy and transarterial chemoembolization. Recently, encouraging results were presented when the bispecific fusion protein tebentafusp was shown to prolong median overall survival from 16 to 22 months in a group of previously untreated HLA- A*02:01–positive patients with metastatic UM (12). This drug has now been approved by the U.S. Food and Drug Administration (FDA).
Several studies have reported no significant improvement in relative or disease-specific survival rates over the last several decades (13–17). However, at least two exceptions exist: a Danish study including patients diagnosed between 1943 and 2021, which showed improving relative survival rates and decreasing primary tumor size at diagnosis over time (18); and a study from St. Erik Eye Hospital, which indicated that patients diagnosed between 1990 and 1998 had better relative survival than patients diagnosed between 1960 and 1969 (19).
In this national retrospective cohort, we aimed to extend previous studies and determine the incidence and competing-risk survival with data from two additional decades. We also investigated patient age and tumor size at diagnosis as well as ocular treatment type.
This study was approved by the Swedish Ethical Review Authority (reference 2020-02835) and adhered to the tenets of the Declaration of Helsinki. All patients residing in Sweden who were diagnosed with posterior UM (i.e., originating in the choroid or the ciliary body) between January 1st, 1960, and December 31st, 2009, were included (n = 3898). The data for the years 1960–1979 was based on a national survey that included reports from the Swedish Cancer Registry and hospital files. For the years 1980–2009, the data was collected from the digitalized treatment registry at St. Erik Eye Hospital according to a previously described methodology (20–22). Since 1960, all Swedish UM patients have been diagnosed at St. Erik Eye Hospital and its predecessor Karolinska University Hospital, with very few exceptions. In cases with very large tumors that have been immediately enucleated in the home clinic, the eyes have been sent for histological examination at the St. Erik Ophthalmic Pathology Laboratory. Parts of this data has been published previously and it has been estimated that the survey captured more than 95% of the UM cases in the country (19, 23). Data from the Cause of Death Registry was automatically fed to the treatment registry to achieve a similar degree of capture as the survey. Thus, all data for this study had been made available previously and no additional collection of patient names, personal identification numbers, diagnoses, treatments, photographs, contact information or any other data that could be traced back to any individual was required. The Cause of Death Registry reported the underlying cause of death, according to the International Classification of Diseases (ICD) code in use at the time of the death. The method of establishing the cause of death was coded as autopsy, clinical examination or forensic investigation. The Cause of Death Registry had been cross-referenced with data from patient medical records so that misclassifications of death from UM as death from cutaneous melanoma were corrected. Data on the number of metastases and affected organs is not available. Similarly, we have no access to data on metastatic treatment for the included patients. UM diagnoses were primarily established upon histological examination of enucleated eyes throughout the study period. For the smaller proportions of patients that underwent eye-sparing plaque brachytherapy, the diagnosis was based on clinical examination with a slit-lamp biomicroscope aided by serial fundus photography, ultrasonography, fluorescein angiography and optical coherence tomography (OCT) as needed and after each respective technique has become available. Tumor dimensions (largest basal diameter and apical thickness) were measured in freshly enucleated specimens before paraffin embedding. In case of eye-preserving treatment, tumor diameters were estimated upon slit-lamp biomicroscopy and with fundus photographs, aided by reference points such as the optic disc. The introduction of plaque brachytherapy in 1979 largely coincided with the introduction of A and B-scan ultrasonography for measurements of tumor thickness.
P-values below 0.05 were considered statistically significant, all p-values being two-sided. Files from Statistics Sweden including records from the Swedish population censuses of 1960 through 1998 were used for calculation of incidence rates (24). Before 1970, the statistics were incomplete regarding the age distribution, preventing analysis for the period 1960–1969. Age-standardization of incidence numbers over the study period was performed by a direct method, with the Swedish population during the period 1970–1974 taken as a standard, according to the stratum weights (Table 1). The relative change in incidence over the period was calculated by linear regression after logarithmic transformation of incidence data. The cumulative incidence of UM-related mortality was plotted in cumulative incidence function estimates from competing risks data with the cmprsk package for R (SurvComp, RRID:SCR_003054), and the equality of survival distributions was tested with Gray’s test for equality (25). Disease-specific survival was plotted in Kaplan–Meier curves and the Wilcoxon (Gehan) test applied. All statistical analyses except competing risk analyses were performed using IBM SPSS statistics version 27 (Armonk, NY, United States, RRID:SCR_016479).
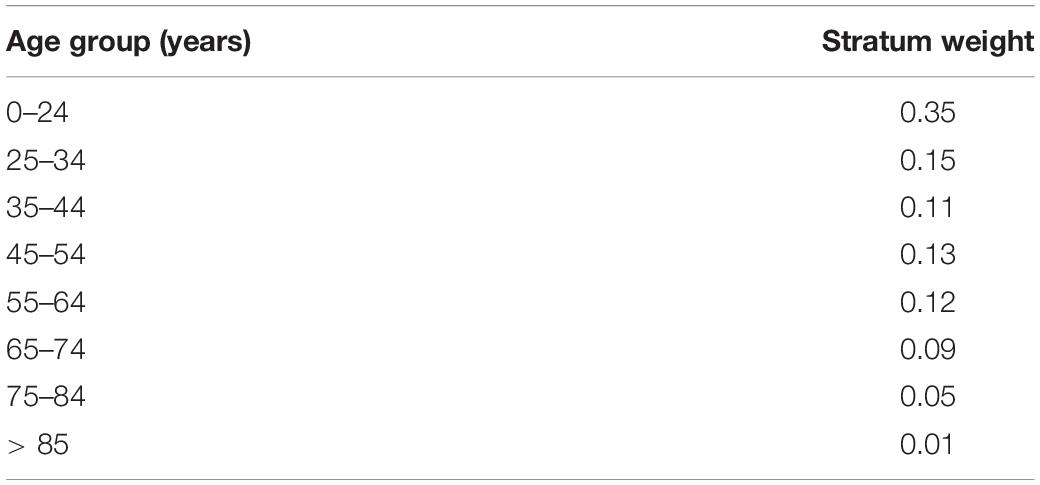
Table 1. Stratum weights of the Swedish standard population 1970–1974.
A total of 3,898 patients had been diagnosed with UM between January 1st, 1960, and December 31st, 2009. Their tumors had a mean thickness and diameter of 6.1 and 11.4 mm, respectively. In terms of primary treatment, 904 patients (23%) had been treated with ruthenium-106 plaque brachytherapy, 139 (4%) with iodine-125 brachytherapy and 2,846 (73%) by enucleation. Of the 3898 included patients, 2,511 had died by the time of data collection. Median follow-up for the 1387 survivors was 12.6 years (interquartile range 11.1, Table 2).
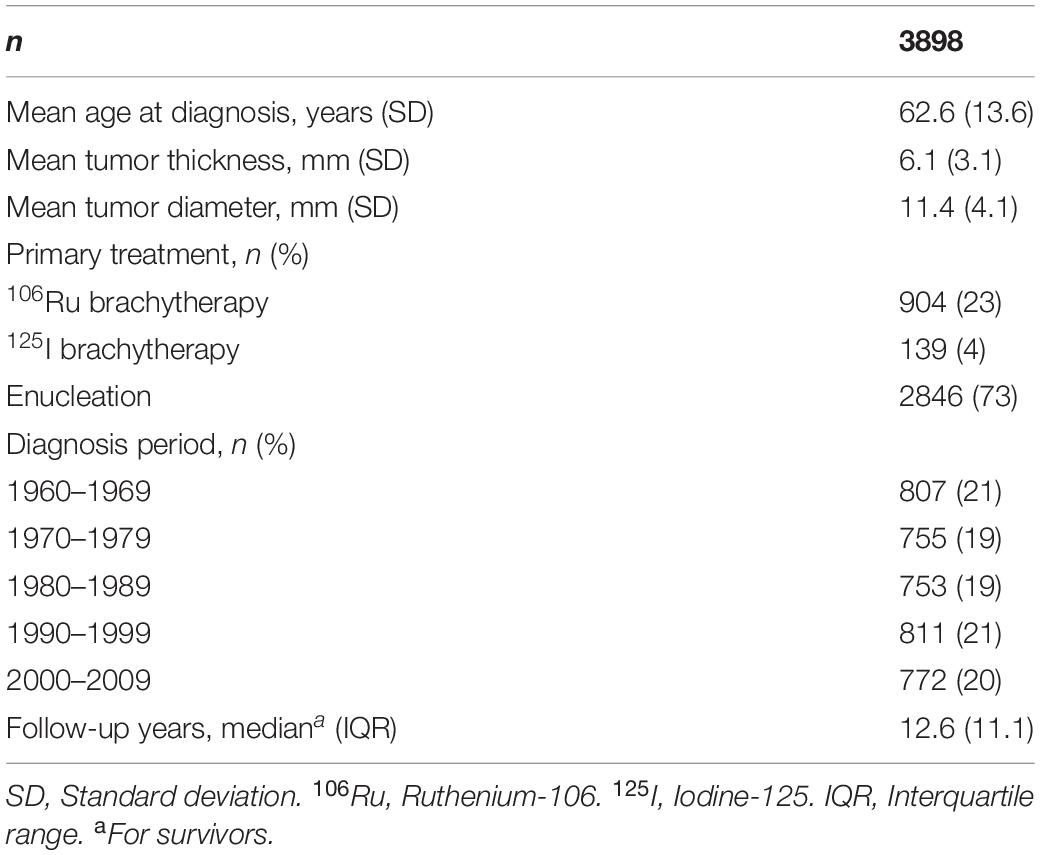
Table 2. Demographics and clinical features of study patients and tumors.
Before 1979, enucleation was the only primary treatment in use. In late 1979, the first patient was treated with ruthenium-106 plaque brachytherapy. Gradually, the latter has become the mainstay treatment. Since 1999, plaque brachytherapy with ruthenium-106 has been the most common primary treatment for UM. This year also marked the introduction of iodine-125 plaque brachytherapy, which is reserved for tumors with an apex height of more than 6 or 7 mm ever since (22). In 2009, primary treatment modalities in reducing order of frequency were (1) ruthenium-106 brachytherapy, (2) enucleation, and (3) iodine-125 brachytherapy (Figure 1).
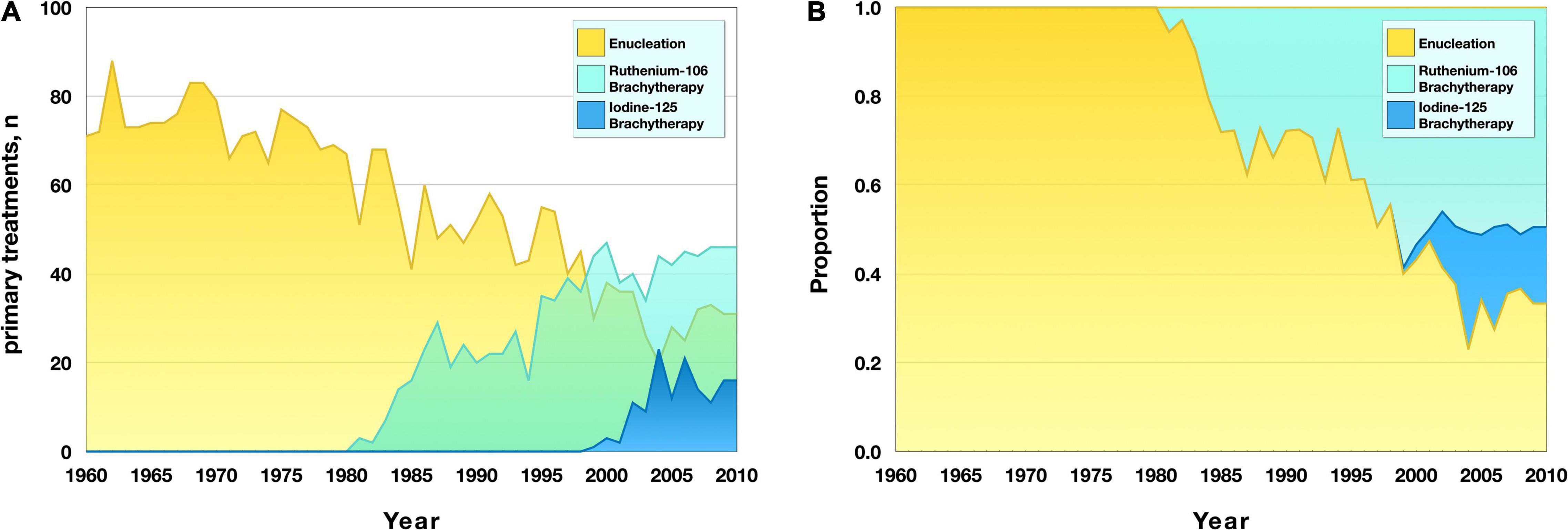
Figure 1. Primary treatment modality for uveal melanoma in the period 1960–2010. (A) Number of treatments with the respective modality. Plaque brachytherapy with ruthenium-106 was introduced in 1979 and plaque brachytherapy with iodine-125 was introduced in 1999. (B) Proportion of all tumors treated with the respective modality.
Patient age at diagnosis gradually increased throughout the study period, from a mean of 59.8 years (SD 13.1) in 1960 to a mean of 66.0 years (SD 13.5) in 2009. In linear regression, patients’ age at diagnosis increased with a slope coefficient of 0.1 per year after 1960. The patients’ age at diagnosis was fitted to a linear function (R2 = 0.4, p = 1.9 × 10–15), where x was the consecutive year after 1960: number of specimens = (0.09x) + 60.4. The slope coefficient was similar to the increase of the Swedish population = (0.1x) + 67.4 (Figure 2A).

Figure 2. Mean patient age and tumor dimensions at diagnosis in the period 1960–2010. (A) Uveal melanoma patients were gradually older at diagnosis during the period (red). The linear trend for their mean age (dashed red) increased with 0.1 years per calendar year, which was similar to the linear trend for the mean age of the Swedish population (green). (B) Reversely, the mean largest basal tumor diameter (blue) and mean tumor apical thickness (yellow) were gradually smaller at diagnosis, with linear trends (dashed) indicating a decline of 0.03 and 0.05 mm per calendar year, respectively.
Conversely, the largest basal tumor diameter and apical thickness gradually diminished during the period. In linear regression, the basal diameter decreased with a slope coefficient of −0.03 mm per year after 1960 (R2 = 0.1, p = 0.012). Tumor thickness decreased with a slope coefficient of −0.05 mm per year (R2 = 0.3, p = 1.2 × 10–5, Figure 2B).
Between 1960 and 2010, the crude incidence of UM in the Swedish population was 6.5–11.6 cases/million/year, and the age-standardized incidence rate was 5.6–9.6 cases/million/year (Table 3). In linear regression, neither crude nor age-standardized incidence rates changed significantly over time (p = 0.68 and p = 0.12, respectively, Figure 3).
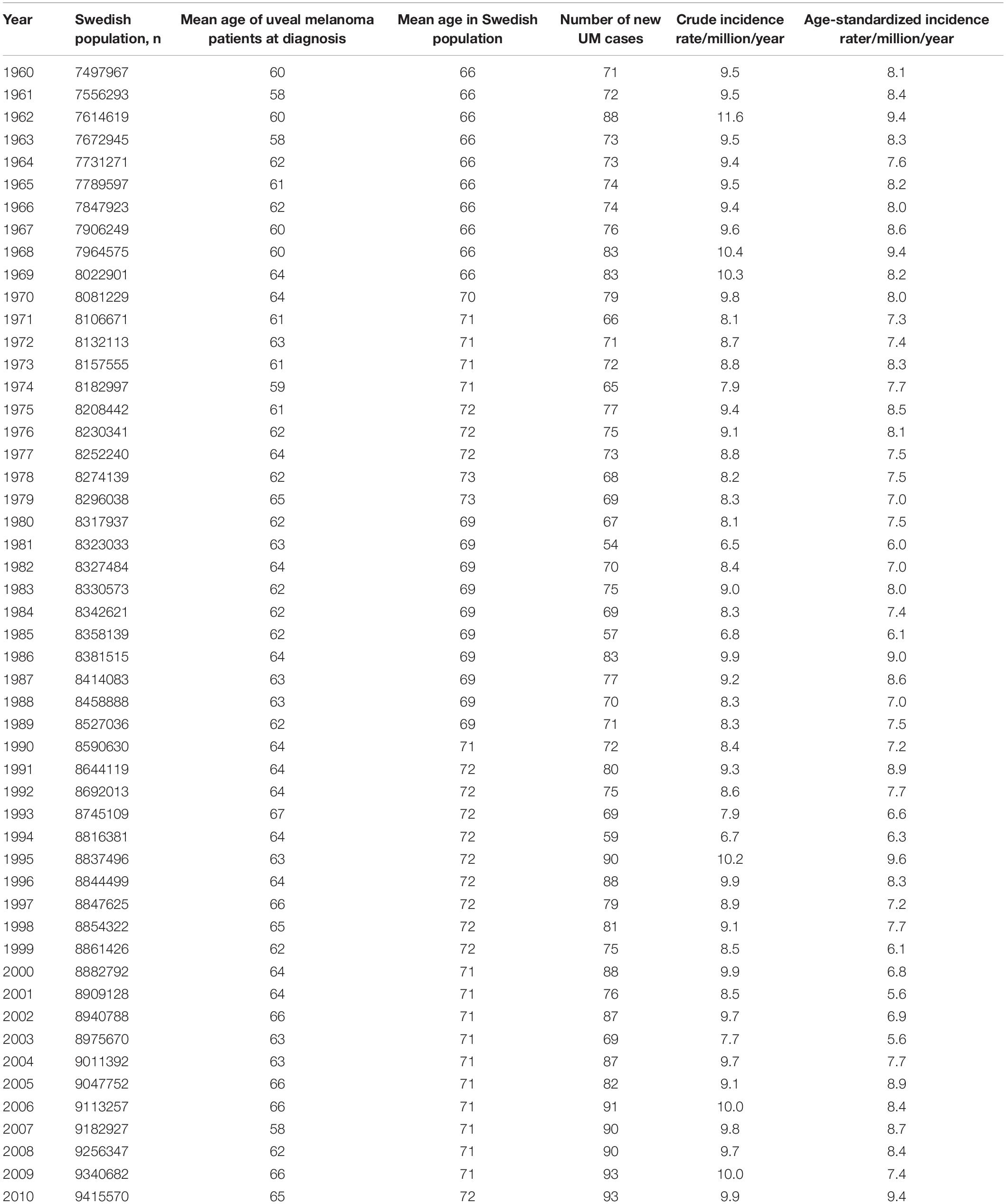
Table 3. Crude and age-standardized incidence rates of uveal melanoma (UM) in the period 1960–2010.

Figure 3. Incidence rates in the period 1960–2010. The crude (blue) and age-standardized (green) incidence rates varied between 6.5 to 11.6 cases/million/year, and 5.6–9.6 cases/million/year, respectively. In linear regression (dashed), neither crude nor age-standardized incidence rates changed significantly over time.
With Kaplan–Meier analysis, patient survival changed over time between 1960 and 2010 [Wilcoxon (Gehan) p = 1.2 × 10–11, Figure 4A]. Patients diagnosed after 1990 had significantly better disease-specific survival than patients diagnosed before 1990 (p = 2.0 × 10–17, Figure 4B).
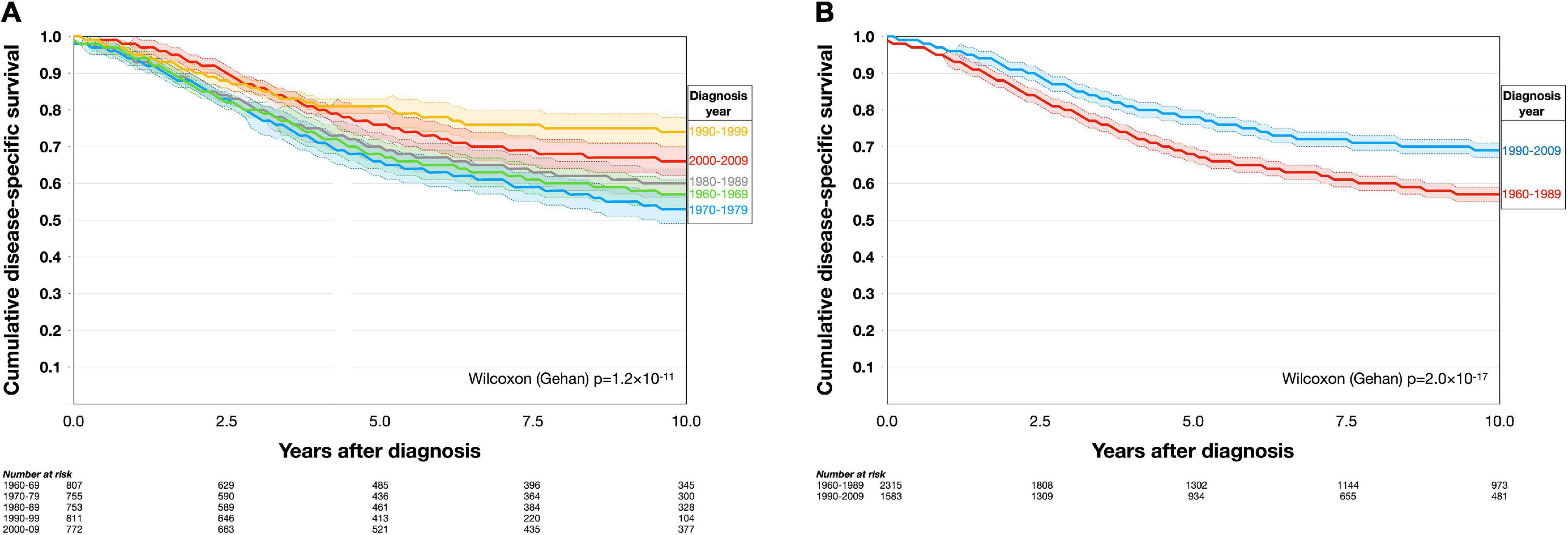
Figure 4. Kaplan–Meier disease-specific survival in the period 1960–2010. (A) Patients diagnosed in different decennia had dissimilar disease-specific survival. (B) Patients diagnosed after 1990 had significantly better disease-specific survival than patients diagnosed before 1990. Colored areas represent 95% confidence intervals.
Similarly, the cumulative incidence of UM-related mortality was highest in patients diagnosed between 1960 and 1979, with a slightly lower mortality in patients diagnosed between 1980 and 1989 and even lower mortality in those diagnosed after 1990 (Gray’s test for equality p = 7.1 × 10–13). The mortality from other causes than UM did not change between the periods (p = 0.16, Figure 5).
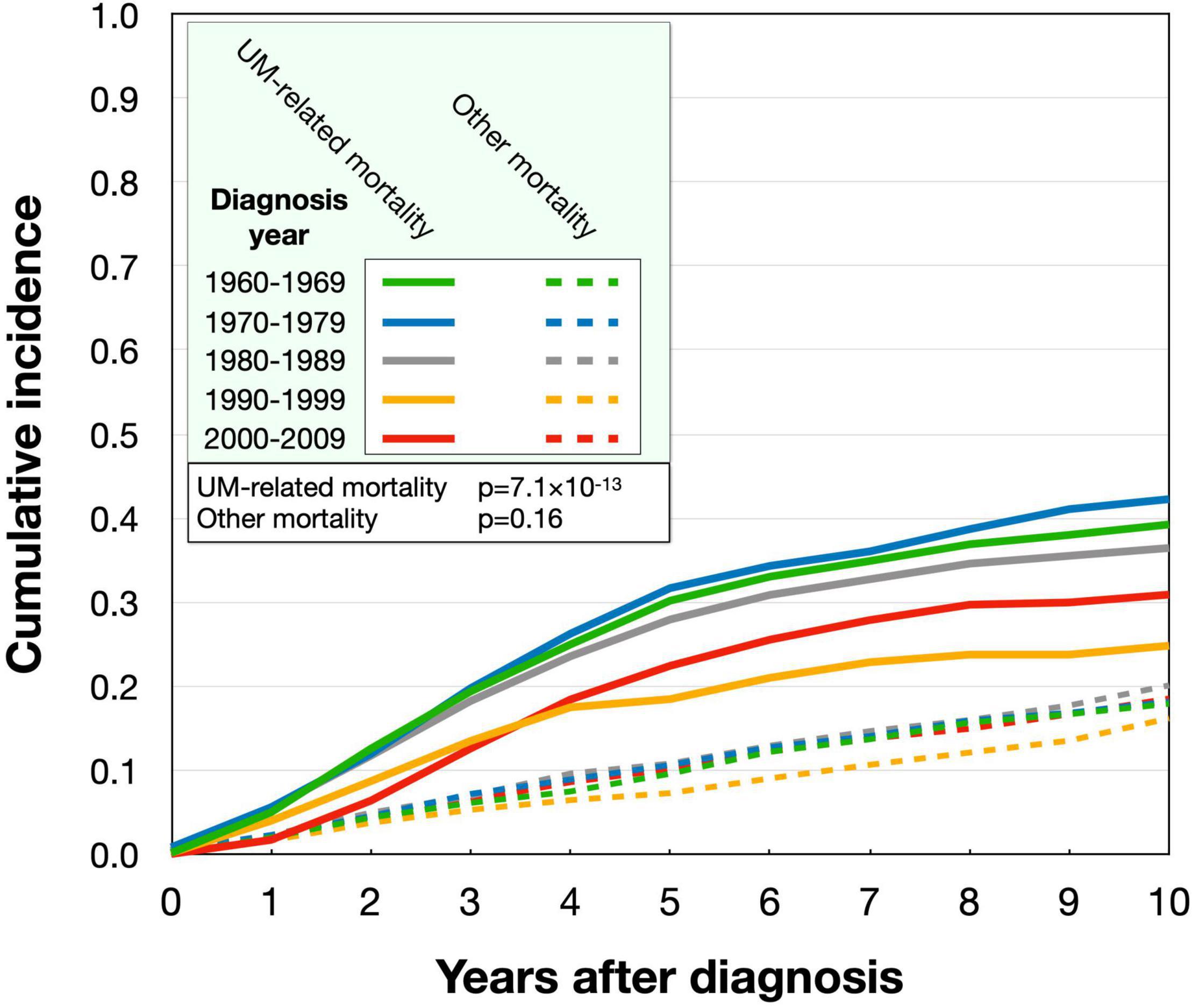
Figure 5. Cumulative incidence of uveal melanoma-related mortality and mortality from other causes in the period 1960–2010. The uveal melanoma-related mortality was highest for patients diagnosed 1960–1969 and 1970–1979, with slightly lower incidences 1980–1989 and even lower after 1990. The incidence of mortality from other causes than uveal melanoma (dashed) did not differ between the periods.
In this study, we found that the age of UM patients at diagnosis increased in the period from 1960–2010, in line with the yearly increase in the mean age of the Swedish population. Conversely, tumor size decreased slightly during this period, whereas crude and age-standardized incidence rates remained stable. Ruthenium-106 plaque brachytherapy replaced enucleation as the most common primary treatment modality. Most importantly, Kaplan–Meier disease specific survival improved, as did the cumulative incidence of UM-related mortality.
The improvement in survival could be related to the decreasing tumor size (26–28). In contrast to cutaneous melanoma, UM is characterized by a low response rate to checkpoint inhibitors and absence of druggable mutations in receptor tyrosine kinases, and recent breakthroughs in the treatment of metastatic UM has not been introduced in our clinical routine at St. Erik Eye Hospital and is not reflected in our analyzed data (10, 12, 29–31). Possible reasons for the decreasing tumor size at diagnosis include the introduction of widespread diabetic retinopathy screening and increasing frequency of cataract surgery. Diagnosis and treatment of smaller tumors may have introduced bias by increasing misdiagnosis of choroidal nevi as small melanomas (false positives); however, the incidence of UM diagnosis did not increase as would have occurred if the number of false positives had increased. We therefore interpret these results as an indication that earlier treatment of UM leads to improved patient survival. To some extent, the results may be due to lead time bias, that is, time is added to a patient’s survival because of earlier diagnosis rather than postponed time of death (32). Our interpretation may also be considered controversial as the impact of primary tumor treatment on patient prognosis is debated (4, 33). The recent observation of a 80–90% metastatic rate among patients with untreated primary tumors indicates that a beneficial effect might exist after all (9). This may be further corroborated by the observation that there are no survival differences between melanomas originating in the choroid or the iris when adjusting for tumor size, although additional studies are needed to verify this observation (34). The reason for the relatively good prognosis in iris melanoma is likely that they are typically diagnosed at a small size. All small tumors may not necessarily grow large and acquire monosomy 3, BAP1 mutations, vasculogenic mimicry or other high-risk features even if left untreated (4). Some, but not all, tumors seem to have these features from the outset, and there is marked variability in their growth rate and considerable intratumor heterogeneity of various risk factors (8, 35–39). Nonetheless, the likelihood of high-risk features increases with increasing tumor size (8, 40–42). Consequently, if tumors are smaller at treatment, a greater proportion of tumors that otherwise would have developed high-risk features at a later stage would be included, thus reducing metastatic rates overall (43).
A general assumption is that the progression from malignant transformation of a melanocytic nevus in the choroid to growth of systemic UM macrometastases is very slow, and that older patients have more long-standing, and often larger, tumors with increased risk for metastasis (8, 44, 45). In a publication by Damato et al. from 2014, younger patients had smaller tumors, lower TNM stage, lower frequency of ciliary body involvement and monosomy 3 (43). Our inverse relationship between gradually older patients and gradually smaller tumors is therefore not intuitive, but replicates what has been observed previously in Denmark (18). We would encourage further similar examinations in other cohorts over long periods of time to shed further light on this phenomenon.
In two previous publications from our institution at St. Erik eye Hospital, the incidence of UM has declined significantly for men but not women between 1960 and 1968, with the relative survival rates for both sexes improving significantly (19, 23). There was a slight shift in the curves with a tendency for increasing incidence, tumor size and mortality in the last decade, but we are content that the overall trend remains intact and that patients diagnosed in the last decade still had lower incidence of UM-related mortality than patients diagnosed during any period prior to 1990.
Limitations to this study include the retrospective analysis with limited control over confounding factors. The many factors that influence survival, which include BAP1 mutations, gene expression class, ciliary body involvement and presence of vasculogenic mimicry, were not accounted for and neither do we know how these factors were distributed in the different time periods analyzed. Secondly, estimations of disease-specific survival and the incidence of UM-related mortality rely on correct diagnosis of the cause of death, and surveys and treatment registries are not always accurate in this regard. The number of misclassifications should be reduced by cross-reference between the treatment registry and medical journals, but we cannot exclude that some UM-related deaths were coded as death from other causes and vice versa. Thirdly, we had no access to data on metastatic profiles or treatments, which would have provided important clues to changes in patient survival. Lastly, the Kaplan–Meier method may be influenced by competing risks (i.e., death from other causes than UM). The cumulative incidence of UM-related mortality in competing risk analysis is not subject to such bias.
In conclusion, this study provides further evidence that earlier ocular treatment of UM prevents metastatic death in some patients. We encourage further research to verify and clarify the observation of an inverse relationship between patient age and tumor size and the influence of lead time bias on the improved survival rates.
The cumulative incidence of UM-related mortality was plotted in cumulative incidence function estimates from competing risks data with the cmprsk package for R (SurvComp, RRID:SCR_003054). All other statistical analyses were performed using IBM SPSS statistics version 27 (Armonk, NY, United States, RRID:SCR_016479).
The data analyzed in this study is subject to the following licenses/restrictions: Anonymization is required. No patient names, personal identifiers, addresses, other contact details, photographs, or dates of diagnosis, treatment, follow-up or death may be shared. Requests to access these datasets should be directed to GS, R3VzdGF2LlN0YWxoYW1tYXJAa2kuc2U=.
The studies involving human participants were reviewed and approved by the Swedish Ethical Review Authority (reference 2020-02835). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
VG, CH, and ShS: writing – original draft. MF and LB: investigation and writing – review and editing. BD: writing – review and editing. StS: methodology and writing – review and editing. GS: conceptualization, formal analysis, resources, visualization, supervision, project administration, and funding acquisition. All authors contributed to the article and approved the submitted version.
This study was supported by Stålhammar from: The Swedish Cancer Society (20 0798 Fk), the Swedish Eye Foundation (reference 2021-04-28), Karolinska Institutet (reference FS-2021-0010), and Region Stockholm (reference 20200356).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Stalhammar G. Forty-year prognosis after plaque brachytherapy of uveal melanoma. Sci Rep. (2020) 10:11297. doi: 10.1038/s41598-020-68232-7
2. Kujala E, Mäkitie T, Kivelä T. Very long-term prognosis of patients with malignant uveal melanoma. Invest Ophthalmol Vis Sci. (2003) 44:4651–9.
3. Stålhammar G, Herrspiegel C. Long-term relative survival in uveal melanoma: a systematic review and meta-analysis. Commun Med. (2022) 2:18.
4. Damato B. Does ocular treatment of uveal melanoma influence survival? Br J Cancer. (2010) 103:285. doi: 10.1038/sj.bjc.6605765
5. Garg G, Finger PT, Kivela TT, Simpson ER, Gallie BL, Saakyan S, et al. Patients presenting with metastases: stage IV uveal melanoma, an international study. Br J Ophthalmol. (2021) 106:510–7. doi: 10.1136/bjophthalmol-2020-317949
7. Eskelin S, Pyrhönen S, Summanen P, Hahka-Kemppinen M, Kivelä T. Tumor doubling times in metastatic malignant melanoma of the uvea: tumor progression before and after treatment. Ophthalmology. (2000) 107:1443–9. doi: 10.1016/s0161-6420(00)00182-2
8. Uner OE, See TRO, Szalai E, Grossniklaus HE, Stalhammar G. Estimation of the timing of BAP1 mutation in uveal melanoma progression. Sci Rep. (2021) 11:8923.
9. Stalhammar G, Gill VT. The long-term prognosis of patients with untreated primary uveal melanoma: a systematic review and meta-analysis. Crit Rev Oncol Hematol. (2022) 172:103652. doi: 10.1016/j.critrevonc.2022.103652
10. Rantala ES, Hernberg M, Kivela TT. Overall survival after treatment for metastatic uveal melanoma: a systematic review and meta-analysis. Melanoma Res. (2019) 29:561–8. doi: 10.1097/CMR.0000000000000575
11. Khoja L, Atenafu EG, Suciu S, Leyvraz S, Sato T, Marshall E, et al. Meta-analysis in metastatic uveal melanoma to determine progression free and overall survival benchmarks: an international rare cancers initiative (IRCI) ocular melanoma study. Ann Oncol. (2019) 30:1370–80. doi: 10.1093/annonc/mdz176
12. Nathan P, Hassel JC, Rutkowski P, Baurain JF, Butler MO, Schlaak M, et al. Overall survival benefit with tebentafusp in metastatic uveal melanoma. N Engl J Med. (2021) 385:1196–206. doi: 10.1056/NEJMoa2103485
13. Singh AD, Topham A. Survival rates with uveal melanoma in the United States: 1973-1997. Ophthalmology. (2003) 110:962–5. doi: 10.1016/S0161-6420(03)00077-0
14. Aronow ME, Topham AK, Singh AD. Uveal melanoma: 5-year update on incidence, treatment, and survival (SEER 1973-2013). Ocul Oncol Pathol. (2018) 4:145–51. doi: 10.1159/000480640
15. Singh AD, Turell ME, Topham AK. Uveal melanoma: trends in incidence, treatment, and survival. Ophthalmology. (2011) 118:1881–5. doi: 10.1016/j.ophtha.2011.01.040
16. Isager P, Engholm G, Overgaard J, Storm H. Uveal and conjunctival malignant melanoma in denmark 1943-97: observed and relative survival of patients followed through 2002. Ophthalmic Epidemiol. (2006) 13:85–96. doi: 10.1080/09286580600553330
17. Roelofsen CDM, Wierenga APA, van Duinen S, Verdijk RM, Bleeker J, Marinkovic M, et al. Five decades of enucleations for uveal melanoma in one center: more tumors with high risk factors, no improvement in survival over time. Ocul Oncol Pathol. (2021) 7:133–41. doi: 10.1159/000509918
18. Smidt-Nielsen I, Bagger M, Heegaard S, Andersen KK, Kiilgaard JF. Posterior uveal melanoma incidence and survival by AJCC tumour size in a 70-year nationwide cohort. Acta Ophthalmol. (2021) 99:e1474–82. doi: 10.1111/aos.14847
19. Bergman L, Seregard S, Nilsson B, Lundell G, Ringborg U, Ragnarsson-Olding B. Uveal melanoma survival in Sweden from 1960 to 1998. Invest Ophthalmol Vis Sci. (2003) 44:3282. doi: 10.1167/iovs.03-0081
20. Fili M, Lundell G, Lundell M, Seregard S. High dose rate and low dose rate ruthenium brachytherapy for uveal melanoma. No association with ocular outcome. Br J Ophthalmol. (2014) 98:1349–54. doi: 10.1136/bjophthalmol-2014-305055
21. Stalhammar G, See TR, Fili M, Seregard S. No gender differences in long-term survival after brachytherapy of 1,541 patients with uveal melanoma. Ocul Oncol Pathol. (2019) 5:432–9. doi: 10.1159/000497186
22. Fili M, Trocme E, Bergman L, See TRO, Andre H, Bartuma K, et al. Ruthenium-106 versus iodine-125 plaque brachytherapy of 571 choroidal melanomas with a thickness of >/=5.5 mm. Br J Ophthalmol. (2020) 104:26–32. doi: 10.1136/bjophthalmol-2018-313419
23. Bergman L, Seregard S, Nilsson B, Ringborg U, Lundell G, Ragnarsson-Olding B. Incidence of uveal melanoma in Sweden from 1960 to 1998. Invest Ophthalmol Vis Sci. (2002) 43:2579–83.
24. Statistics Sweden. Summary of Population Statistics 1960–2020, Population statistics. Stockholm: Statistics Sweden (2022).
25. Scrucca L, Santucci A, Aversa F. Competing risk analysis using R: an easy guide for clinicians. Bone Marrow Transplant. (2007) 40:381–7. doi: 10.1038/sj.bmt.1705727
26. Shields CL, Furuta M, Thangappan A, Nagori S, Mashayekhi A, Lally DR, et al. Metastasis of uveal melanoma millimeter-by-millimeter in 8033 consecutive eyes. Arch Ophthalmol. (2009) 127:989–98. doi: 10.1001/archophthalmol.2009.208
27. Simpson ER, Gallie B, Saakyan S, Amiryan A, Finger PT, Chin KJ, et al. International Validation of the American Joint Committee on Cancer’s 7th Edition Classification of Uveal Melanoma. JAMA Ophthalmol. (2015) 133:376–83.
28. Arnljots TS, Al-Sharbaty Z, Lardner E, All-Eriksson C, Seregard S, Stålhammar G. Tumour thickness, diameter, area or volume? The prognostic significance of conventional versus digital image analysis-based size estimation methods in uveal melanoma. Acta Ophthalmol. (2018) 96:510–8. doi: 10.1111/aos.13668
29. Stålhammar G, Seregard S, Grossniklaus HE. Expression of immune checkpoint receptors Indoleamine 2,3-dioxygenase and T cell Ig and ITIM domain in metastatic versus nonmetastatic choroidal melanoma. Cancer Med. (2019) 8:2784–92. doi: 10.1002/cam4.2167
30. Heppt MV, Steeb T, Schlager JG, Rosumeck S, Dressler C, Ruzicka T, et al. Immune checkpoint blockade for unresectable or metastatic uveal melanoma: a systematic review. Cancer Treat Rev. (2017) 60:44–52. doi: 10.1016/j.ctrv.2017.08.009
31. Komatsubara K, Carvajal R. Immunotherapy for the treatment of uveal melanoma: current status and emerging therapies. Curr Oncol Rep. (2017) 19:45. doi: 10.1007/s11912-017-0606-5
32. Andersson TM, Rutherford MJ, Humphreys K. Assessment of lead-time bias in estimates of relative survival for breast cancer. Cancer Epidemiol. (2017) 46:50–6. doi: 10.1016/j.canep.2016.12.004
33. Damato B. Ocular treatment of choroidal melanoma in relation to the prevention of metastatic death - A personal view. Prog Retin Eye Res. (2018) 66:187–99. doi: 10.1016/j.preteyeres.2018.03.004
34. Sabazade S, Herrspiegel C, Gill V, Stålhammar G. No differences in the long-term prognosis of iris and choroidal melanomas when adjusting for tumor thickness and diameter. BMC Cancer. (2021) 21:1270. doi: 10.1186/s12885-021-09002-0
35. Herrspiegel C, Kvanta A, Lardner E, Cabaca L. Ramskold, Wells J, Bartuma K, et al. Nuclear expression of BAP-1 in transvitreal incisional biopsies and subsequent enucleation of eyes with posterior choroidal melanoma. Br J Ophthalmol. (2021) 105:582–6. doi: 10.1136/bjophthalmol-2020-316498
36. Field MG, Durante MA, Anbunathan H, Cai LZ, Decatur CL, Bowcock AM, et al. Punctuated evolution of canonical genomic aberrations in uveal melanoma. Nat Commun. (2018) 9:116. doi: 10.1038/s41467-017-02428-w
37. Jouhi S, Jager MJ, de Geus SJR, Desjardins L, Eide NA, Grange JD, et al. The small fatal choroidal melanoma study. A survey by the European ophthalmic oncology group. Am J Ophthalmol. (2019) 202:100–8. doi: 10.1016/j.ajo.2019.01.031
38. Herwig-Carl MC, Sharma A, Holler T, Holz FG, Schlitter AM, Loeffler KU. Spatial intratumor heterogeneity in uveal melanoma: tumor cell subtypes with a presumed invasive potential exhibit a particular epigenetic staining reaction. Exp Eye Res. (2019) 182:175–81. doi: 10.1016/j.exer.2019.04.001
39. Stalhammar G, Grossniklaus HE. Intratumor heterogeneity in uveal melanoma BAP-1 expression. Cancers. (2021) 13:1143. doi: 10.3390/cancers13051143
40. Gupta MP, Lane AM, DeAngelis MM, Mayne K, Crabtree M, Gragoudas ES, et al. Clinical characteristics of uveal melanoma in patients with germline BAP1 mutations. JAMA Ophthalmol. (2015) 133:881–7. doi: 10.1001/jamaophthalmol.2015.1119
41. Scholes AG, Damato BE, Nunn J, Hiscott P, Grierson I, Field JK. Monosomy 3 in uveal melanoma: correlation with clinical and histologic predictors of survival. Invest Ophthalmol Vis Sci. (2003) 44:1008–11. doi: 10.1167/iovs.02-0159
42. Thomas S, Putter C, Weber S, Bornfeld N, Lohmann DR, Zeschnigk M. Prognostic significance of chromosome 3 alterations determined by microsatellite analysis in uveal melanoma: a long-term follow-up study. Br J Cancer. (2012) 106:1171–6. doi: 10.1038/bjc.2012.54
43. Damato BE, Heimann H, Kalirai H, Coupland SE. Age, survival predictors, and metastatic death in patients with choroidal melanoma: tentative evidence of a therapeutic effect on survival. JAMA Ophthalmol. (2014) 132:605–13. doi: 10.1001/jamaophthalmol.2014.77
44. Kaliki S, Shields CL, Mashayekhi A, Ganesh A, Furuta M, Shields JA. Influence of age on prognosis of young patients with uveal melanoma: a matched retrospective cohort study. Eur J Ophthalmol. (2013) 23:208–16. doi: 10.5301/ejo.5000200
Keywords: uveal melanoma, survival, treatment, time-trend, ophthalmology (MeSH), cancer, melanoma, Sweden
Citation: Gill V, Herrspiegel C, Sabazade S, Fili M, Bergman L, Damato B, Seregard S and Stålhammar G (2022) Trends in Uveal Melanoma Presentation and Survival During Five Decades: A Nationwide Survey of 3898 Swedish Patients. Front. Med. 9:926034. doi: 10.3389/fmed.2022.926034
Received: 22 April 2022; Accepted: 17 May 2022;
Published: 02 June 2022.
Edited by:
Alan G. Palestine, University of Colorado Anschutz Medical Campus, United StatesReviewed by:
Yousef Ahmed Fouad, Ain Shams University, EgyptCopyright © 2022 Gill, Herrspiegel, Sabazade, Fili, Bergman, Damato, Seregard and Stålhammar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Viktor Gill, VmlrdG9yLkdpbGxAa2kuc2U=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.