 Jérôme Ghidaglia
Jérôme Ghidaglia Nicolas Golse2,3
Nicolas Golse2,3 Florent L. Besson
Florent L. Besson
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Med., 07 July 2022
Sec. Nuclear Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.924824
This article is part of the Research TopicNuclear Medicine in Cancer DiagnosisView all 11 articles
Background: Post-operative recurrence remains the strongest prognostic factor of resected hepatocellular carcinoma (HCC), making the accurate selection of patients with curable HCC a crucial issue. PET imaging combining both 18F-FDG and fatty acid synthase (FAS) radiotracers—such as Choline—has shown its interest for the initial staging and therapeutic management of patients with HCC, but its use is still not consensual. Importantly, the very first dual-tracer PET studies suggested 18F-FDG/FAS PET behavior be linked to the degree of differentiation of HCC, a major predictive factor of post-operative recurrence. Although this key molecular imaging concept may impact how dual-tracer PET will be used in early-stage HCC, its level of evidence remains largely unexplored. In this study, we conducted a systematic review of the available evidence-based data to clarify the relevance of dual 18F-FDG/18F-Choline PET in characterizing the degree of differentiation of HCC tumors.
Methods: A systematic search of the PubMed/Medline and Embase databases was performed up to November 2021. A systematic review of the dual-tracer 18F-FDG/18F-Choline PET behavior of histology-proven HCC according to their degree of differentiation was conducted. The overall quality of the included studies was critically assessed based on the STROBE guidelines. Information on study date, design, patient cohort characteristics, grade of differentiation of HCC tumors, and the dual-tracer PET behavior per HCC was independently extracted and summarized.
Results: From 440 records initially available, 6 full-text articles (99 histology-proven HCC) provided dual-tracer 18F-FDG/18F-Choline PET behavior per HCC tumor grade were included in the systematic review. Based on our analysis, 43/99 HCCs were reported to be well-differentiated, and 56/99 HCCs were reported to be less-differentiated tumors. In the well-differentiated subgroup, more than half were exclusively positive for 18F-Choline (51%), whereas 39% were positive for both 18F-FDG and 18F-Choline. In the less-differentiated subgroup, 37% of HCC patients were positive exclusively for FDG, 36% were positive for both 18F-FDG and 18F-Choline, and 25% were positive exclusively for 18F-Choline.
Conclusion: The 18F-FDG/18F-Choline dual-tracer PET behavior of uptake shows high overlap between well- and less differentiated HCC, making the characterization of tumors challenging based on such PET combination alone. Given our growing knowledge of the molecular complexity of HCC, further studies are necessary to refine our understanding of radiotracers’ behavior in this field and improve the usefulness of PET imaging in the clinical decision process of HCC.
Hepatocellular carcinoma (HCC), the most common primary liver cancer and the third leading cause of cancer death worldwide, represents a major health challenge (1). Chronic liver disease—cirrhosis—which can be related to alcohol, NASH, HBV or HCV infection, or less frequently primary biliary cholangitis, hemochromatosis, or α1-antitrypsin deficiency, is the strongest risk factor of HCC development, concerning more than 90% of the cases. The treatment strategy is currently mainly driven by the Barcelona Clinic Liver Cancer staging system (BCLC), a five-stage classification scale integrating the characteristics of the primary tumor (size, number of nodules), the disease extent (portal invasion, N+ and M+ status), the liver function (Child-Pugh), and the performance status (ECOG). Very early and early-stage HCC patients may benefit from various curative options (resection, ablation or liver transplantation), whereas more advanced stages are candidate to chemoembolization, systemic therapies including immunotherapy, or best supportive care. In early-stage HCC, post-operative recurrence remains the strongest survival prognostic factor (2) making the accurate selection of patients with curable HCC a crucial issue. Tumor differentiation is a major predictive factor of post-operative recurrence in HCC (3, 4). However, the histological analysis of tumor differentiation, which remains the gold standard, is currently carried out only in atypical cases. Conventional imaging is essential for the management of HCC patients (5–8), but its limited value in such atypical cases and the need for non-invasive biomarkers of tumor differentiation have progressively motivated the use of PET imaging in this field (9), while this functional imaging is still not consensually recommended. Because 18F-fluorodeoxyglose (18F-FDG) shows mitigated performance to detect HCC (10, 11) but excellent specificity for HCC metastases (9), PET radiotracers of fatty acid synthase (FAS) have been proposed as complements, such radiolabeled choline, the most widely used FAS-targeted radiotracer in clinical practice (12, 13). Although 18F-FDG and FAS PET radiotracers have shown their complementarity for the initial staging and treatment management of HCC patients (14–17) their combined use is still not consensual, making dedicated recommendations challenging (18).
The very first dual 18F-FDG/18F-Choline PET studies suggested 18F-FDG/FAS PET behavior be linked to the degree of differentiation of HCC tumors (19, 20). Although this key concept could impact the rational for using dual-tracer PET in HCC, its level of evidence remains largely unexplored. In this study, we conducted a systematic review of the available evidence-based data, to clarify whether 18F-FDG/18F-Choline dual-tracer PET behavior is a relevant imaging biomarker of tumor differentiation in HCC.
This methodological study was conducted according to the PRISMA 2020 statement for systematic review reports (21).
Two authors (JG and FLB) independently performed a comprehensive search of PubMed/Medline and Embase databases to find studies using 18F-FDG and 18F-Choline dual PET tracers for HCC purposes. The search strategy combined the following keywords: “HCC + PET” or “HCC + FDG” AND “HCC + Choline.” No starting date was used, and the search procedure was updated until 10 November 2021. Moreover, references of the retrieved articles were also screened for additional studies. The inclusion criteria were as follows: (i) articles exclusively in English; (ii) the combined use of 18F-FDG and 18F/11C-Choline dual PET tracers for each HCC tumor, in order to assess the dual-tracer PET behavior without a priori; (iii) histology-confirmed HCC diagnosis; and (iv) available description of HCC differentiation for each patient. All the articles not fulfilling the inclusion criteria mentioned above, together with review articles, editorials, letters, comments, or case reports, were excluded from the analysis. For each eligible study, the following information was independently extracted: study date; design; patient cohort characteristics, including sample size, number of patients with HCC, and number of HCC lesions per patient confirmed by histology (either by surgery or biopsy); delay time between the 18F-FDG and 18F-Choline PET acquisitions; histological differentiation of HCC; and dual PET radiotracer behavior of HCC patients per histological subtype. For all included studies, the same predefined definition of PET positivity was considered: any focal uptake superior to the locoregional background was considered positive, whereas iso or hypometabolic lesions were considered negative for the radiotracer of interest.
The overall quality of each included study was critically assessed by two authors (JG and FLB) based on the “STROBE guidelines” (22). Because the dual PET tracer behavior according to the level of differentiation of HCC was never considered the primary outcome, a general standardized checklist of 22 items covering the overall quality statements of non-interventional studies (22) was independently applied by the two readers as follows: each item was quoted “yes” if present, “no” if absent, or “unclear” if the statement was equivocal. All disagreements between the two readers were resolved by consensus.
The need for ethical approval was waived due to the nature of the study (review article).
The PRISMA flow diagram of the literature search is provided in Figure 1. The comprehensive literature search from PubMed/MEDLINE and Embase identified the following records: 440 records using the “HCC + PET CT” keywords; 353 records using the “HCC + FDG” keywords; 192 records using the “HCC + Choline” keywords; and 19 records using the “HCC + FDG + Choline” keywords. Among the 19 articles, 12 were discarded due to study type (reviews n = 4), analysis of metastatic disease (n = 1), cholangiocarcinoma study (n = 1), use of Choline only in 18F-FDG-negative patients (n = 1), and preclinical studies (n = 2). At the end of the screening process, 7 full-text articles were retrieved. Among them, one article was discarded because no explicit HCC differentiation status per patient was provided (23), and two studies presented patient data overlap (20, 24). Of the two studies with patient data overlap, we discarded the second study (24). Finally, 6 full-text articles over the last 15 years (2006–2021) were included in the systematic review (14, 16, 19, 20, 25, 26).
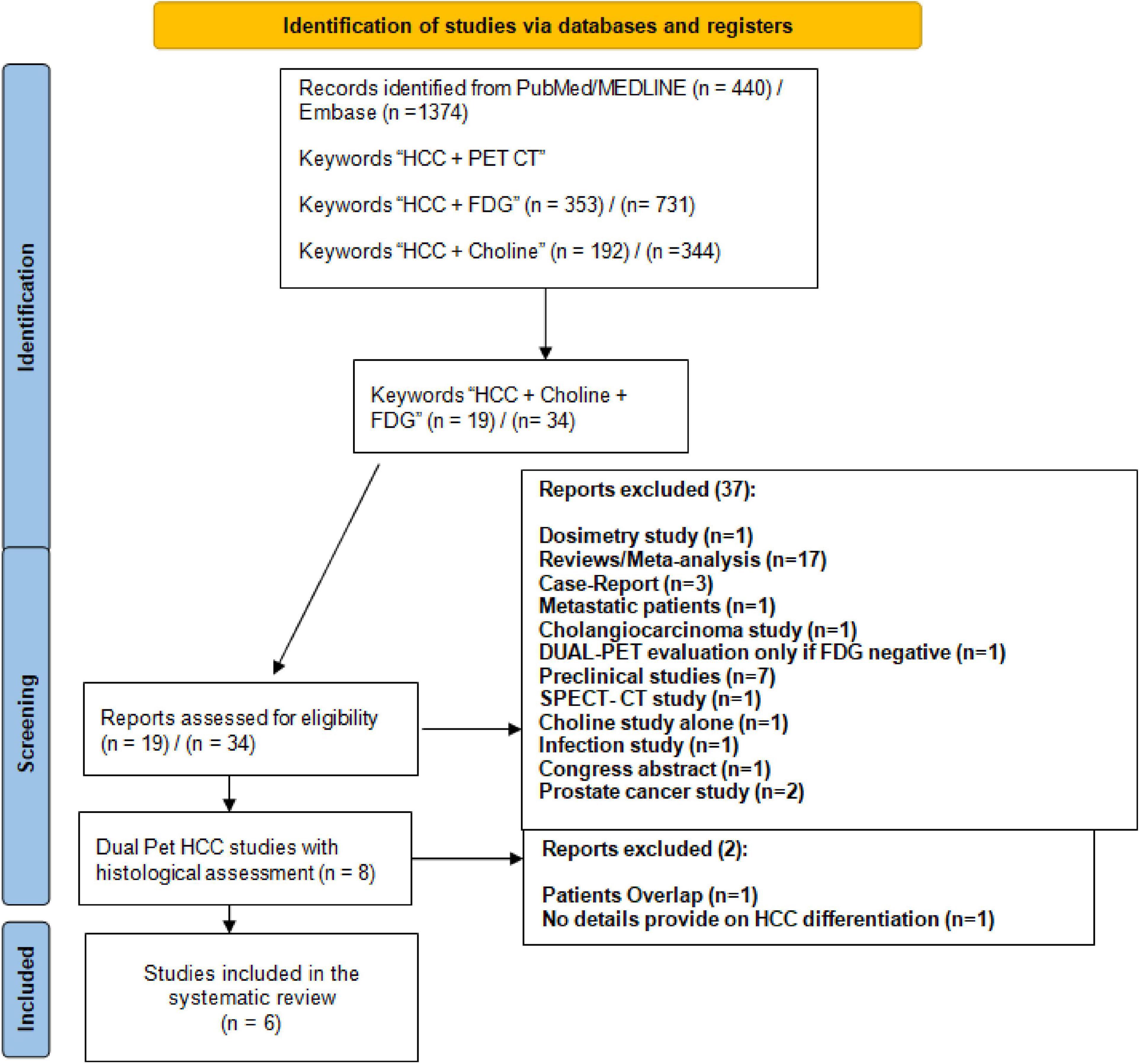
Figure 1. PRISMA flowchart of the systematic review.
The overall quality assessment of the 6 included studies is shown in Figure 2. The studies were of limited quality with 12 items (55%) considered present (range = 9–16), 3 items (14%) considered absent (range = 0–6) and 6 items (27%) considered unclear after a double blinded reading (range = 5–11). In particular, only two studies provided a majority of unequivocal item statements for the results section (19, 26), and one study provided unclear or no information for the majority of the STROBE statements of the discussion section (25). Considering these statements, the level of evidence for the dedicated use of dual 18F-FDG/18F-Choline PET tracer for the characterization of HCC differentiation was considered a level 4–5 (grade C-D of recommendation) according to the Oxford Centre for Evidence-Based Medicine.
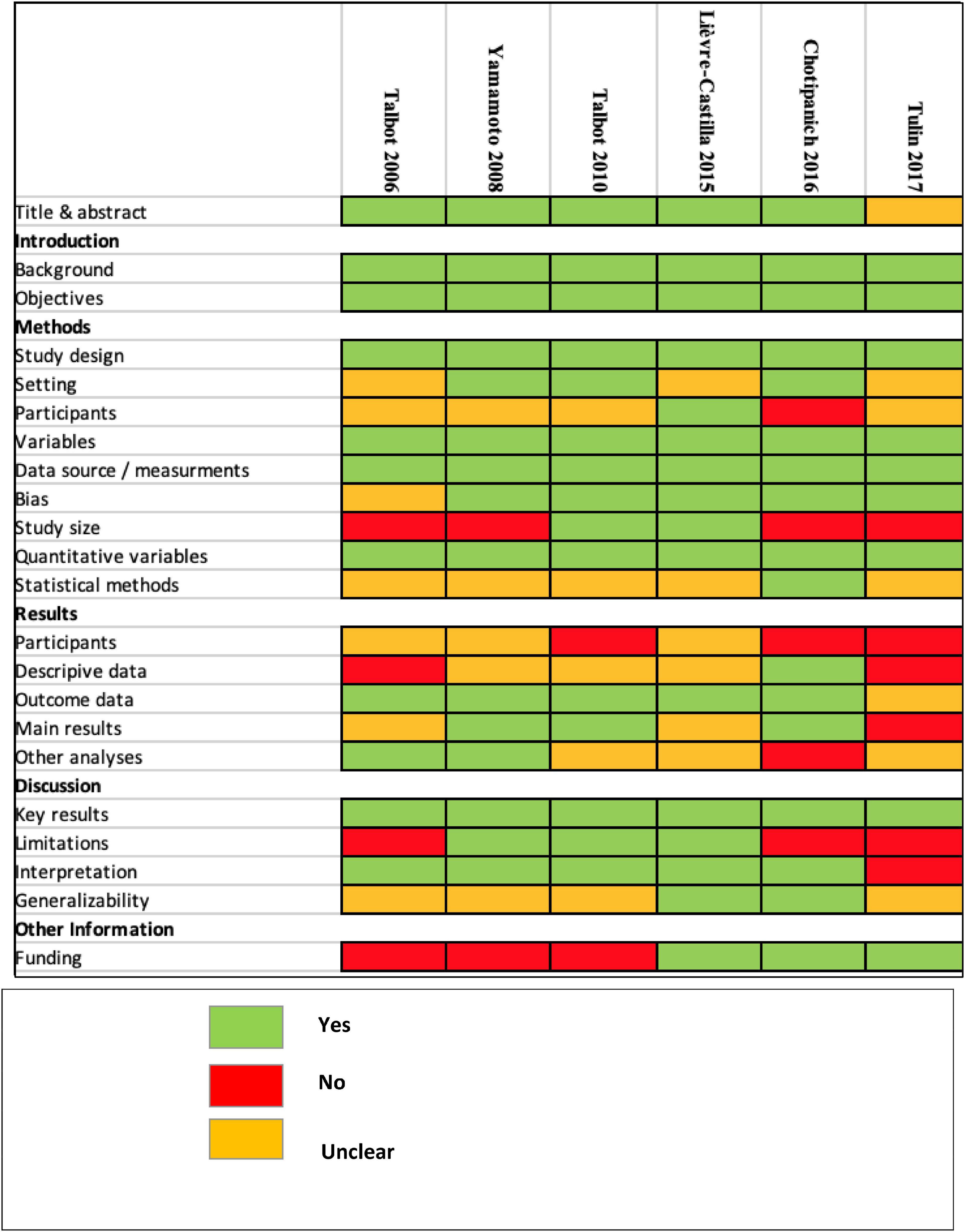
Figure 2. STROBE quality assessment.
The main characteristics of the 6 included studies are provided in Table 1. The primary outcomes were as follows: the detection rate of 18F-FDG and 18F-Choline PET tracers for HCC tumors (16, 19); the diagnostic performance of 18F-FDG and 18F-Choline PET tracers for detecting and staging HCC in patients with chronic liver disease (14, 20); and the assessment of dual 18F-FDG and 18F-Choline PET with perfusion CT behaviors of HCC tumors (25). The dual radiotracer PET data of 99 biopsy-proven HCC patients were reanalyzed. The study samples were mainly limited with only two prospective studies reaching more than 20 histologically proven HCC samples (14, 20). Talbot et al. (20) included a case mix of 34 HCC patients (27 biopsy proven), 2 hepato-cholangiocarcinoma patients, 10 patients with other malignancies, and 8 patients with benign conditions. Castilla-Lièvre et al. (14) included 38 HCC patients (22 biopsy proven) with 4 cholangiocarcinoma patients and one adenoma patient. The other 4 studies exclusively focused on HCC patients. Among the pooled 99 HCC tumors, 43 were considered well-differentiated tumors, and 56 were considered moderate to poorly differentiated tumors. The classification used for tumor differentiation (Edmonson Steiner or WHO) was mentioned for only 57% of the HCC tumors as follows: biopsy for 14 HCC tumors (14, 16) surgery for 37 HCC tumors (14, 19), and a case mix of biopsy/surgery for the rest of the dataset without any information concerning the ratio. Additionally, 50 HCC patients were explicitly qualified as having unifocal HCC tumors (14, 16, 19), and 25 HCC patients were explicitly qualified as having multifocal HCC tumors (14, 16, 19, 25). In all studies, PET positivity was defined visually as non-physiological focal liver radiotracer uptake in four studies (14, 16, 19, 25), whereas one study also proposed a “photopenic” pattern for Choline PET positivity (20).
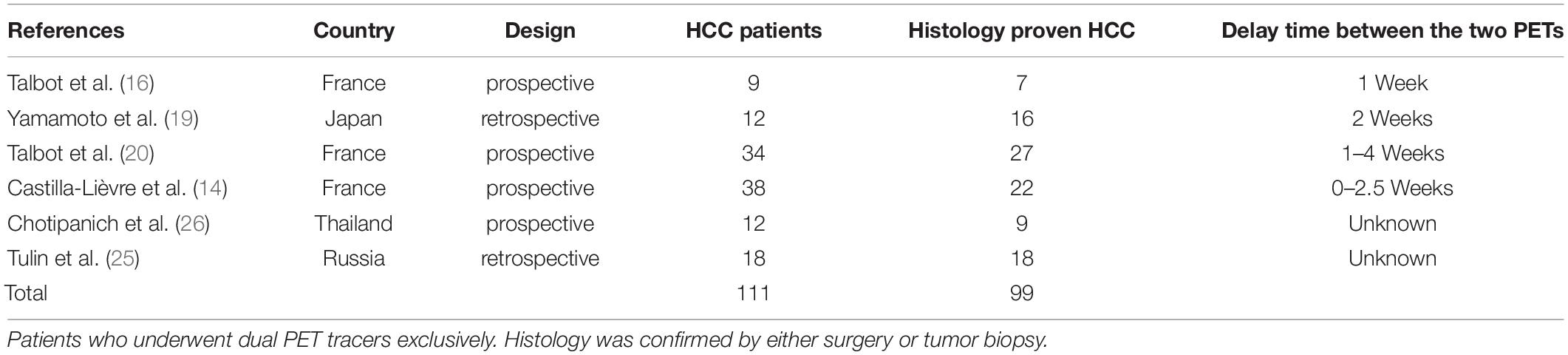
Table 1. Characteristics of the included studies with dual PET tracer.
The 18F-FDG and 18F-Choline PET tumor behaviors according to the differentiation of the tumors are shown in Table 2. In the well-differentiated subgroup, 51% were exclusively positive for 18F-Choline, 39% were positive for both 18F-FDG and 18F-Choline, and only 5% were exclusively positive for FDG. Two patients were negative for the two PET radiotracers (20, 26). In the poorly differentiated subgroup, 37% of HCC patients were exclusively positive for 18F-FDG, 36% were positive for both 18F-FDG and 18F-Choline, and 25% were exclusively positive for Choline. One patient was considered negative for both radiotracers (20).
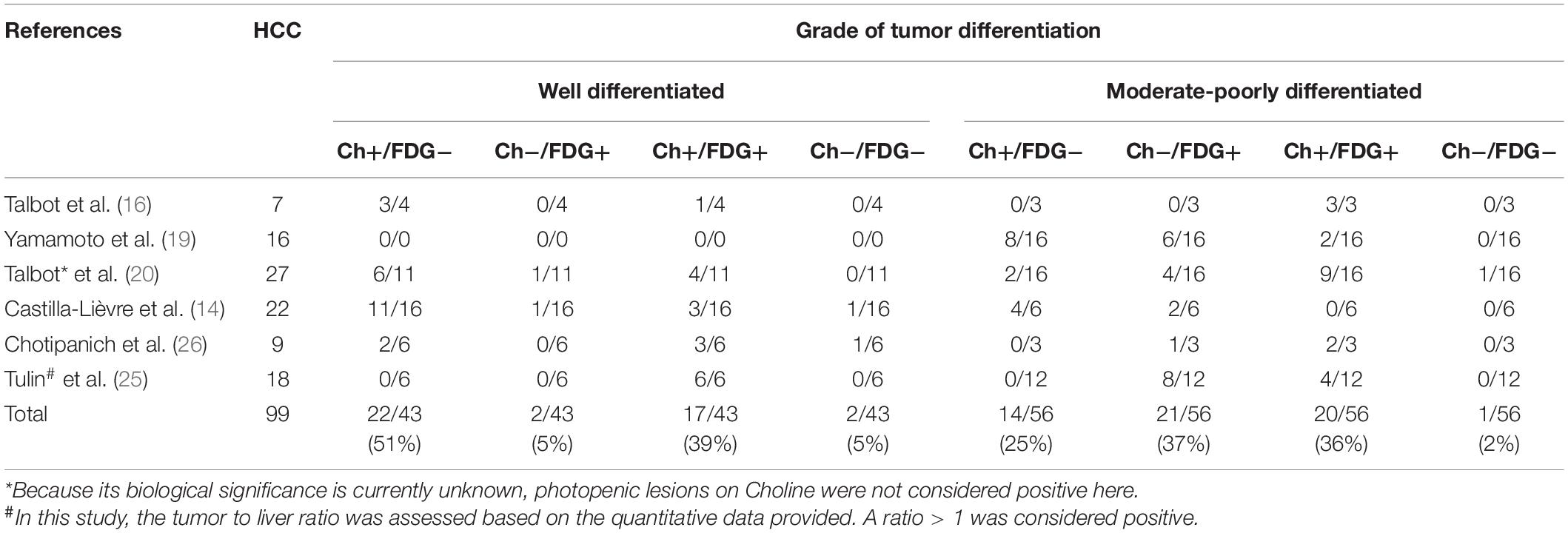
Table 2. Dual PET radiotracer behaviors function of HCC level of differentiation.
Five studies also performed SUV-based semiquantitative analyses (14, 16, 19, 25, 26) with discrepant results. In one study, no significant difference was observed between the 18F-FDG or 18F-Choline signal-to-noise ratio irrespective of the HCC level of differentiation (16). Yamamoto et al. found no significant difference in radiotracer uptake between the histological subgroups (19). Tulin et al. reported a significant difference in radiotracer uptake according to the liver areas (well-differentiated HCC, poorly differentiated HCC, or normal parenchyma) (25). Chotipanich et al. found a significant difference between well- and poorly differentiated HCC only for 18F-FDG (26). The last study did not perform any comparative analyses (14).
Based on our analysis of the literature data, well-differentiated HCC patients were positive for 18F-FDG in approximately 44% of the reported cases and positive for 18F-Choline in 90% of the reported cases. For the less-differentiated HCC tumors (moderate to poorly differentiated HCC), 73% of reported HCC cases were 18F-FDG-positive, and 61% of reported HCC cases were 18F-Choline-positive. Among the 56 less differentiated tumors considered in the present study, 16 were explicitly mentioned as poorly differentiated HCC, of which 100% were 18F-FDG-positive and 31% were 18F-Choline-positive. However, the 8 poorly differentiated tumors all considered 18F-FDG-positive and 18F-Choline-negative in one study had no information regarding the motivation of their inclusion criteria (25). Focusing on the 8 remaining poorly differentiated HCC patients (16, 19, 26), 100% were reported to be positive for 18F-FDG, of whom 63% were also positive for 18F-Choline. Moreover, more than one-third of patients showed dual PET tracer positivity regardless of the degree of HCC differentiation.
A trend toward an inverse gradient of dual-PET HCC tumor behavior has been previously suggested (16, 20), but our systematic review showed that a strong mirrored dual-PET tumor behavior according to HCC differentiation should be considered with caution. First, the lack of standardized histological grading of HCC remains a major issue. Although Edmonson Steiner and WHO classifications share similarities (4-level grades and structural/cellular features), the respective definitions for well- and less differentiated grades are not fully concordant with a related impact on subgroup outcomes (27). In our systematic review, only two of the six included studies explicitly mentioned either Edmonson Steiner (19) or WHO (14) classifications (39% of the included HCC). As 61% of the biopsy-proven reported HCC cases were potentially a blinded case mix of ES/WHO definitions, any generalizability of 18F-FDG/18F-Choline dual PET tracer behavior according to HCC grading would be ambiguous. Second, a significant association between glucose metabolism assessed by FDG PET and microvascular invasion (MVI), another strong prognostic factor in HCC (28, 29), has been widely reported (23, 30–32). Surprisingly, Kornberg et al. reported that 14 of the 16 HCC patients who were positive for 18F-FDG PET had MVI (87.5%), of whom only 1/3 were poorly differentiated (5 patients) (30). Although an extensive review by Gouw et al. showed that high-grade tumors but also tumor size and number of nodules to be predictive of MVI (33), MVI has also been reported in 29% of HCCs with a size ranging from 2 to 5 cm (34). Sabaté-Llobera et al. reported that the ratios of well- to less differentiated tumors ranged from 1.3 in the 18F-FDG-positive group to 5.7 in the 18F-FDG-negative group (31). However, nearly 50% of 18F-FDG-positive cases in the present study were well-differentiated HCC. Consequently, 18F-FDG PET positivity may reflect both MVI and tumor differentiation, which are two prognostic factors that are not highly interlinked. Third, studies by Okazumi, Torizuka, and Trojan (35–37) have suggested that a loss of FDG 6-phosphatase activity in undifferentiated tumor cells explains the higher 18F-FDG avidity of poorly differentiated HCC. Importantly, the studies by Okazumi and Torizuka were mainly dynamic PET studies (35, 36). The tissue behavior of advanced PET kinetic parameters, especially k3 or k4 microparameters, cannot be directly extrapolated to static PET metrics, such as SUV, a surrogate of the glucose retention index in cells. Trojan et al. reported that the 18F-FDG uptake (SUV) was more efficient not only in poorly differentiated tumors but also in large tumors and elevated AFP (37). In particular, the vast majority of the reported FDG-positive tumors also showed multiple nodules, all being predictive factors of MVI (38).
Evidence-based analysis of the literature over the past 20 years suggests complex interlinks between tumor grade and MVI, and the related FDG PET behaviors in HCC patients. In contrast, 18F-Choline appears not as informative as 18F-FDG to characterize tumor aggressiveness in HCC patients. In 29 HCC patients, Mulé et al. showed a higher 18F-FDG uptake for MVI-positive HCC cases compared to MVI-negative HCC cases (SUVr 2.65 vs. 1, p = 0.003) without any significant difference in 18F-Choline uptake (39). This lack of prognostic significance of 18F-Choline was also reported by Castilla-Lièvre et al. (14). Notably, a combined photopenic 18F-Choline with a positive 18F-FDG-PET pattern has been suggested to be a pejorative prognostic factor of HCC recurrence (24). In light of this methodological review, the question of the leading prognostic value of 18F-FDG PET arises. The biological significance of glucose- and Choline-based PET tracer behaviors in HCC patients remains poorly understood.
Recently, a better understanding of biological pathways of HCC tumors has led to the emergence of a new molecular-based classification of HCC, dichotomizing the tumors into proliferation and non-proliferation classes based on their multidimensional molecular pattern (40–45). While the proliferative class is characterized by poorly differentiated tumors, high vascular invasion, and elevated AFP, the non-proliferative class corresponds to well to moderately differentiated tumors, less vascular invasion, and lower level of AFP. In both groups, the characteristics of T-cell infiltrates further define four immune-related subclasses (46). Because the characterization of tumor heterogeneity at the molecular level is emerging in HCC (47, 48), the powerful capabilities of vectorized PET molecular imaging in this field would gain in relevance. Although several 18F-FDG/FAS studies emphasize the clinical usefulness of PET to manage HCC patients (17, 49), future multitracer PET studies are mandatory to better understand the deep biological meaning of multitracer PET behavior in this field.
Our systematic review had several limitations. The limited number of dual 18F-FDG/18F-Choline PET articles with available per patient-based HCC tumor differentiation hampered any quantitative analysis. However, our pooled semiquantitative analysis revealed the high overlap of 18F-FDG/18F-Choline PET behavior between well- and less differentiated HCC. Additionally, we did not include acetate PET studies in this systematic review (11, 50–52). Initially, evaluated in cardiac (53) and urological oncology settings (54, 55), acetate shows a biodistribution quite similar to that of Choline. Although both substrates are fed into fatty acid synthesis, also known as the Kennedy pathway (56–58), Choline and acetate have various other biological functions (59, 60), making them not strictly comparable. Additionally, 18F-Choline is currently the most widely used FAS-targeted PET tracer of HCC in clinical practice, which is why we focused on this PET radiotracer in this study.
The 18F-FDG/18F-Choline dual-tracer PET behavior of uptake shows high overlap between well- and less differentiated HCC, making the characterization of tumors challenging based on such PET combination alone. Given our growing knowledge of the molecular complexity of HCC, further studies are necessary to refine our understanding of radiotracers’ behavior in this field and improve the usefulness of PET imaging in the clinical decision process of HCC.
All authors: design, acquisition analysis, revising for intellectual content, final approval, and agreement to be accountable for all aspects of this work (accuracy and integrity of any part of the work).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
PET, Positron emission tomography; HCC, Hepatocellular carcinoma; 18F-FDG, 18F-Fluorodeoxyglucose; FAS, Fatty acid synthase; BCLC, Barcelona Clinic Liver Cancer staging system; NASH, Non-Alcoholic SteatoHepatitis; HBV, Hepatitis B Virus; HBC, Hepatitis C Virus; SUV, Standard Uptake Value.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Colecchia A. Prognostic factors for hepatocellular carcinoma recurrence. World J Gastroenterol. (2014) 20:5935.
3. Imamura H, Matsuyama Y, Tanaka E, Ohkubo T, Hasegawa K, Miyagawa S, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol. (2003) 38:200–7. doi: 10.1016/s0168-8278(02)00360-4
4. Cucchetti A, Piscaglia F, Caturelli E, Benvegnù L, Vivarelli M, Ercolani G, et al. Comparison of recurrence of hepatocellular carcinoma after resection in patients with cirrhosis to its occurrence in a surveilled cirrhotic population. Ann Surg Oncol. (2009) 16:413–22. doi: 10.1245/s10434-008-0232-4
5. Chernyak V, Fowler KJ, Kamaya A, Kielar AZ, Elsayes KM, Bashir MR, et al. Liver imaging reporting and data system (LI-RADS) version 2018: imaging of hepatocellular carcinoma in at-risk patients. Radiology. (2018) 289:816–30. doi: 10.1148/radiol.2018181494
6. van der Pol CB, Lim CS, Sirlin CB, McGrath TA, Salameh JP, Bashir MR, et al. Accuracy of the liver imaging reporting and data system in computed tomography and magnetic resonance image analysis of hepatocellular carcinoma or overall malignancy-a systematic review. Gastroenterology. (2019) 156:976–86. doi: 10.1053/j.gastro.2018.11.020
7. Llovet JM, Lencioni R. mRECIST for HCC: performance and novel refinements. J Hepatol. (2020) 72:288–306. doi: 10.1016/j.jhep.2019.09.026
8. Llovet JM, Villanueva A, Marrero JA, Schwartz M, Meyer T, Galle PR, et al. Trial design and endpoints in hepatocellular carcinoma: AASLD consensus conference. Hepatology. (2021) 73:158–91. doi: 10.1002/hep.31327
9. Sharma B, Martin A, Zerizer I. Positron emission tomography-computed tomography in liver imaging. Semin Ultrasound CT MR. (2013) 34:66–80.
10. Khan MA, Combs CS, Brunt EM, Lowe VJ, Wolverson MK, Solomon H, et al. Positron emission tomography scanning in the evaluation of hepatocellular carcinoma. J Hepatol. (2000) 32:792–7. doi: 10.1016/s0168-8278(00)80248-2
11. Park JW, Kim JH, Kim SK, Kang KW, Park KW, Choi JI, et al. A prospective evaluation of 18F-FDG and 11C-acetate PET/CT for detection of primary and metastatic hepatocellular carcinoma. J Nucl Med. (2008) 49:1912–21. doi: 10.2967/jnumed.108.055087
12. Bertagna F, Bertoli M, Bosio G, Biasiotto G, Sadeghi R, Giubbini R, et al. Diagnostic role of radiolabelled choline PET or PET/CT in hepatocellular carcinoma: a systematic review and meta-analysis. Hepatol Int. (2014) 8:493–500. doi: 10.1007/s12072-014-9566-0
13. Signore G, Nicod-Lalonde M, Prior JO, Bertagna F, Muoio B, Giovanella L, et al. Detection rate of radiolabelled choline PET or PET/CT in hepatocellular carcinoma: an updated systematic review and meta-analysis. Clin Transl Imaging. (2019) 7:237–53.
14. Castilla-Lièvre MA, Franco D, Gervais P, Kuhnast B, Agostini H, Marthey L, et al. Diagnostic value of combining 11C-choline and 18F-FDG PET/CT in hepatocellular carcinoma. Eur J Nucl Med Mol Imaging. (2016) 43:852–9. doi: 10.1007/s00259-015-3241-0
15. Wu HB, Wang QS, Li BY, Li HS, Zhou WL, Wang QY. F-18 FDG in conjunction with 11C-choline PET/CT in the diagnosis of hepatocellular carcinoma. Clin Nucl Med. (2011) 36:1092–7. doi: 10.1097/RLU.0b013e3182335df4
16. Talbot JN, Gutman F, Fartoux L, Grange JD, Ganne N, Kerrou K, et al. PET/CT in patients with hepatocellular carcinoma using [(18)F]fluorocholine: preliminary comparison with [(18)F]FDG PET/CT. Eur J Nucl Med Mol Imaging. (2006) 33:1285–9. doi: 10.1007/s00259-006-0164-9
17. Chalaye J, Costentin CE, Luciani A, Amaddeo G, Ganne-Carrié N, Baranes L, et al. Positron emission tomography/computed tomography with 18F-fluorocholine improve tumor staging and treatment allocation in patients with hepatocellular carcinoma. J Hepatol. (2018) 69:336–44. doi: 10.1016/j.jhep.2018.02.018
18. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. (2018) 69:182–236.
19. Yamamoto Y, Nishiyama Y, Kameyama R, Okano K, Kashiwagi H, Deguchi A, et al. Detection of hepatocellular carcinoma using 11C-choline PET: comparison with 18F-FDG PET. J Nucl Med. (2008) 49:1245–8. doi: 10.2967/jnumed.108.052639
20. Talbot JN, Fartoux L, Balogova S, Nataf V, Kerrou K, Gutman F, et al. Detection of hepatocellular carcinoma with PET/CT: a prospective comparison of 18F-fluorocholine and 18F-FDG in patients with cirrhosis or chronic liver disease. J Nucl Med. (2010) 51:1699–706. doi: 10.2967/jnumed.110.075507
21. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
22. Vandenbroucke JP, von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, et al. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. Ann Intern Med. (2007) 147:W163–94.
23. Mulé S, Chalaye J, Legou F, Tenenhaus A, Calderaro J, Galletto Pregliasco A, et al. Hepatobiliary MR contrast agent uptake as a predictive biomarker of aggressive features on pathology and reduced recurrence-free survival in resectable hepatocellular carcinoma: comparison with dual-tracer 18F-FDG and 18F-FCH PET/CT. Eur Radiol. (2020) 30:5348–57. doi: 10.1007/s00330-020-06923-5
24. Fartoux L, Balogova S, Nataf V, Kerrou K, Huchet V, Rosmorduc O, et al. A pilot comparison of 18F-fluorodeoxyglucose and 18F-fluorocholine PET/CT to predict early recurrence of unifocal hepatocellular carcinoma after surgical resection. Nucl Med Commun. (2012) 33:757–65. doi: 10.1097/MNM.0b013e328350fb9f
25. Tulin PE, Dolgushin MB, Odzharova AA, Mikhaylov AI, Medvedeva BM, Shiryaev SV, et al. Perfusion CT and PET with 18F-FDG and 18F-FCh in the complex diagnosis of hepatocellular carcinoma. Eur J Hybrid Imaging. (2017) 1:13. doi: 10.1186/s41824-017-0018-7
26. Chotipanich C, Kunawudhi A, Promteangtrong C, Tungsuppawattanakit P, Sricharunrat T, Wongsa P. Diagnosis of hepatocellular carcinoma using C11 choline PET/CT: comparison with F18 FDG, contrastenhanced MRI and MDCT. Asian Pac J Cancer Prev. (2016) 17:3569–73.
27. Martins-Filho SN, Paiva C, Azevedo RS, Alves VAF. Histological grading of hepatocellular carcinoma-a systematic review of literature. Front Med. (2017) 4:193. doi: 10.3389/fmed.2017.00193
28. Rodríguez-Perálvarez M, Luong TV, Andreana L, Meyer T, Dhillon AP, Burroughs AK. A systematic review of microvascular invasion in hepatocellular carcinoma: diagnostic and prognostic variability. Ann Surg Oncol. (2013) 20:325–39. doi: 10.1245/s10434-012-2513-1
29. Sumie S, Nakashima O, Okuda K, Kuromatsu R, Kawaguchi A, Nakano M, et al. The significance of classifying microvascular invasion in patients with hepatocellular carcinoma. Ann Surg Oncol. (2014) 21:1002–9. doi: 10.1245/s10434-013-3376-9
30. Kornberg A, Freesmeyer M, Bärthel E, Jandt K, Katenkamp K, Steenbeck J, et al. 18F-FDG-uptake of hepatocellular carcinoma on PET predicts microvascular tumor invasion in liver transplant patients. Am J Transplant. (2009) 9:592–600. doi: 10.1111/j.1600-6143.2008.02516.x
31. Sabaté-Llobera A, Mestres-Martí J, Reynés-Llompart G, Lladó L, Mils K, Serrano T, et al. 2-[18F]FDG PET/CT as a predictor of microvascular invasion and high histological grade in patients with hepatocellular carcinoma. Cancers. (2021) 13:2554. doi: 10.3390/cancers13112554
32. Cuccurullo V, Di Stasio GD, Mazzarella G, Cascini GL. Microvascular invasion in HCC: the molecular imaging perspective. Contrast Media Mol Imaging. (2018) 2018:9487938. doi: 10.1155/2018/9487938
33. Gouw ASH, Balabaud C, Kusano H, Todo S, Ichida T, Kojiro M. Markers for microvascular invasion in hepatocellular carcinoma: where do we stand? Liver Transplant. (2011) 17(Suppl. 2):S72–80. doi: 10.1002/lt.22368
34. Yamashita Y, Tsuijita E, Takeishi K, Fujiwara M, Kira S, Mori M, et al. Predictors for microinvasion of small hepatocellular carcinoma ≤ 2 cm. Ann Surg Oncol. (2012) 19:2027–34. doi: 10.1245/s10434-011-2195-0
35. Okazumi S, Isono K, Enomoto K, Kikuchi T, Ozaki M, Yamamoto H, et al. Evaluation of liver tumors using fluorine-18-fluorodeoxyglucose PET: characterization of tumor and assessment of effect of treatment. J Nucl Med. (1992) 33:333–9.
36. Torizuka T, Tamaki N, Inokuma T, Magata Y, Sasayama S, Yonekura Y, et al. In vivo assessment of glucose metabolism in hepatocellular carcinoma with FDG-PET. J Nucl Med. (1995) 36:1811–7.
37. Trojan J, Schroeder O, Raedle J, Baum RP, Herrmann G, Jacobi V, et al. Fluorine-18 FDG positron emission tomography for imaging of hepatocellular carcinoma. Am J Gastroenterol. (1999) 94:3314–9.
38. Zhao WC, Fan LF, Yang N, Zhang HB, Chen BD, Yang GS. Preoperative predictors of microvascular invasion in multinodular hepatocellular carcinoma. Eur J Surg Oncol. (2013) 39:858–64. doi: 10.1016/j.ejso.2013.04.003
39. Mulé S, Pigneur F, Quelever R, Tenenhaus A, Baranes L, Richard P, et al. Can dual-energy CT replace perfusion CT for the functional evaluation of advanced hepatocellular carcinoma? Eur Radiol. (2018) 28:1977–85. doi: 10.1007/s00330-017-5151-y
40. Lee JS, Heo J, Libbrecht L, Chu IS, Kaposi-Novak P, Calvisi DF, et al. A novel prognostic subtype of human hepatocellular carcinoma derived from hepatic progenitor cells. Nat Med. (2006) 12:410–6. doi: 10.1038/nm1377
41. Boyault S, Rickman DS, de Reyniès A, Balabaud C, Rebouissou S, Jeannot E, et al. Transcriptome classification of HCC is related to gene alterations and to new therapeutic targets. Hepatology. (2007) 45:42–52. doi: 10.1002/hep.21467
42. Chiang DY, Villanueva A, Hoshida Y, Peix J, Newell P, Minguez B, et al. Focal gains of VEGFA and molecular classification of hepatocellular carcinoma. Cancer Res. (2008) 68:6779–88. doi: 10.1158/0008-5472.CAN-08-0742
43. Hoshida Y, Nijman SMB, Kobayashi M, Chan JA, Brunet JP, Chiang DY, et al. Integrative transcriptome analysis reveals common molecular subclasses of human hepatocellular carcinoma. Cancer Res. (2009) 69:7385–92. doi: 10.1158/0008-5472.CAN-09-1089
44. Cancer Genome Atlas Research Network. Comprehensive and integrative genomic characterization of hepatocellular carcinoma. Cell. (2017) 169:1327–41.e23. doi: 10.1016/j.cell.2017.05.046
45. Llovet JM, Kelley RK, Villanueva A, Singal AG, Pikarsky E, Roayaie S, et al. Hepatocellular carcinoma. Nat Rev Dis Primer. (2021) 7:6.
46. Sia D, Jiao Y, Martinez-Quetglas I, Kuchuk O, Villacorta-Martin C, Castro de Moura M, et al. Identification of an immune-specific class of hepatocellular carcinoma, based on molecular features. Gastroenterology. (2017) 153:812–26. doi: 10.1053/j.gastro.2017.06.007
47. Ding X, He M, Chan AWH, Song QX, Sze SC, Chen H, et al. Genomic and epigenomic features of primary and recurrent hepatocellular carcinomas. Gastroenterology. (2019) 157:1630–45.e6.
48. Zhang Q, Lou Y, Bai XL, Liang TB. Intratumoral heterogeneity of hepatocellular carcinoma: from single-cell to population-based studies. World J Gastroenterol. (2020) 26:3720–36. doi: 10.3748/wjg.v26.i26.3720
49. Cheung TT, Ho CL, Chen S, Chan SC, Poon RTP, Fan ST, et al. Reply: underestimated role of 18F-FDG PET for HCC evaluation and promise of 18F-FDG PET/MR imaging in this setting. J Nucl Med. (2013) 54:1511–2. doi: 10.2967/jnumed.113.126185
50. Ho CL, Yu SCH, Yeung DWC. 11C-acetate PET imaging in hepatocellular carcinoma and other liver masses. J Nucl Med. (2003) 44:213–21.
51. Hwang KH, Choi DJ, Lee SY, Lee MK, Choe W. Evaluation of patients with hepatocellular carcinomas using [(11)C]acetate and [(18)F]FDG PET/CT: a preliminary study. Appl Radiat Isot. (2009) 67:1195–8. doi: 10.1016/j.apradiso.2009.02.011
52. Au KP, Dai WC, Chi-Yan Chan A, Cheung TT, Lo CM, Chok KSH. Performance of dual-tracer PET-CT for staging post-liver transplant hepatocellular carcinoma recurrence. Transplant Direct. (2021) 7:e769. doi: 10.1097/TXD.0000000000001213
53. Brown M, Marshall DR, Sobel BE, Bergmann SR. Delineation of myocardial oxygen utilization with carbon-11-labeled acetate. Circulation. (1987) 76:687–96. doi: 10.1161/01.cir.76.3.687
54. Shreve P, Chiao PC, Humes HD, Schwaiger M, Gross MD. Carbon-11-acetate PET imaging in renal disease. J Nucl Med. (1995) 36:1595–601.
55. Oyama N, Akino H, Kanamaru H, Suzuki Y, Muramoto S, Yonekura Y, et al. 11C-acetate PET imaging of prostate cancer. J Nucl Med. (2002) 43:181–6.
56. Podo F. Tumour phospholipid metabolism. NMR Biomed. (1999) 12:413–39. doi: 10.1002/(sici)1099-1492(199911)12:7<413::aid-nbm587>3.0.co;2-u
57. Gibellini F, Smith TK. The Kennedy pathway–de novo synthesis of phosphatidylethanolamine and phosphatidylcholine. IUBMB Life. (2010) 62:414–28. doi: 10.1002/iub.337
58. Deford-Watts LM, Mintz A, Kridel SJ. The potential of 11C-acetate PET for monitoring the fatty acid synthesis pathway in tumors. Curr Pharm Biotechnol. (2013) 14:300–12. doi: 10.2174/1389201011314030006
59. Wellen KE, Hatzivassiliou G, Sachdeva UM, Bui TV, Cross JR, Thompson CB. ATP-citrate lyase links cellular metabolism to histone acetylation. Science. (2009) 324:1076–80. doi: 10.1126/science.1164097
Keywords: HCC, PET, FDG, choline, molecular imaging
Citation: Ghidaglia J, Golse N, Pascale A, Sebagh M and Besson FL (2022) 18F-FDG /18F-Choline Dual-Tracer PET Behavior and Tumor Differentiation in HepatoCellular Carcinoma. A Systematic Review. Front. Med. 9:924824. doi: 10.3389/fmed.2022.924824
Received: 20 April 2022; Accepted: 07 June 2022;
Published: 07 July 2022.
Edited by:
Francesco Cicone, Magna Græcia University, ItalyReviewed by:
Giorgio Treglia, Ente Ospedaliero Cantonale (EOC), SwitzerlandCopyright © 2022 Ghidaglia, Golse, Pascale, Sebagh and Besson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jérôme Ghidaglia, amVyb21lLmdoaWRhZ2xpYUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.