
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Med., 22 July 2022
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.920016
This article is part of the Research TopicCOVID-19: Epidemiologic Trends, Public Health Challenges, and Evidence-Based Control InterventionsView all 55 articles
 Miklós Szabó1
Miklós Szabó1 Zsófia Kardos2,3
Zsófia Kardos2,3 Csaba Oláh4Péter Tamáska5Katalin Hodosi6
Csaba Oláh4Péter Tamáska5Katalin Hodosi6 Eszter Csánky1
Eszter Csánky1 Zoltán Szekanecz6*
Zoltán Szekanecz6*Introduction: Numerous clinical and laboratory scores that include C-reactive protein (CRP), D-dimer, ferritin, lactate dehydrogenase (LDH), interleukin 6 (IL-6), procalcitonin (PCT), blood urea nitrogen (BUN), creatinine levels and oxygenation (PaO2 and SaO2) have been used for the prognosis of COVID-19. In addition, composite scores have been developed for the assessment of general state and risk in community-acquired pneumonia (CAP) that may be applied for COVID-19 as well. In this study, we assessed severity and potential prognostic risk factors for unfavorable outcome among hospitalized COVID-19 patients. We also applied the A-DROP general scoring system used in CAP to COVID-19.
Patients and methods: Altogether 233 patients admitted to our center with COVID-19 were included in the study. Clinical status, several laboratory biomarkers described above, indicators of oxygenation were determined at hospital admission. We also applied the A-DROP composite scoring system that includes Age (≥ 70 years in males and ≥ 75 years in females), Dehydration (BUN ≥ 7.5 mmol/l), Respiratory failure (SaO2 ≤ 90% or PaO2 ≤ 60 mmHg), Orientation disturbance (confusion) and low blood Pressure (systolic BP ≤ 90 mmHg) to COVID-19.
Results: At the time of admission, most patients had elevated CRP, LDH, ferritin, D-dimer, and IL-6 levels indicating multisystemic inflammatory syndrome (MIS). Altogether 49 patients (21.2%) required admission to ICU, 46 (19.7%) needed ventilation and 40 patients (17.2%) died. In the binary analysis, admission to ICU, the need for ventilation and death were all significantly associated with the duration of hospitalization, history of hypertension or obesity, confusion/dizziness, as well as higher absolute leukocyte and neutrophil and lower lymphocyte counts, elevated CRP, PCT, LDH, ferritin, IL-6, BUN, and creatinine levels, low PaO2 and SaO2 and higher A-DROP score at the time of admission (p < 0.05).
Conclusion: Numerous laboratory biomarkers in addition to obesity, dizziness at the time of admission and the history of hypertension may predict the need for ICU admission and ventilation, as well as mortality in COVID-19. Moreover, A-DROP may be a suitable scoring system for the assessment of general health and disease outcome in COVID-19.
In late 2019, a new strain of β coronavirus called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was identified in Wuhan, China, which caused a worldwide epidemic due to its rapid spread (1, 2). The COVID-19 pandemic puts an extreme load on healthcare systems including intensive care units (ICU) all over the world (1, 3–5). In the first waves of the epidemic, the hospitalization rate was 5–10 percent, while global mortality was 2–3 percent. In the majority of patients, the disease is asymptomatic or mild, but in some patient groups it may be severe with potentially fatal outcome (6). SARS-CoV-2 virus-induced pneumonia is a part of multisystemic inflammatory syndrome (MIS) associated with the advanced stages of COVID-19. MIS often leads to the damage of multiple organs and death (3, 4, 7).
The initial assessment of the severity of community-acquired pneumonia (CAP) is important for patient management (8). In addition the number of patients diagnosed with COVID-19 pneumonia in this epidemic is high, while health resources are finite. Identification of high risk patients are of paramount importance for the optimal use of hospital capacity and patient safety. There have been attempts to identify prognostic factors that might predict the outcome of early SARS-CoV-2 infection and COVID-19-associated pneumonia (4, 9–11). Comorbidities, such as hypertension, hyperlipidemia, ischemic heart disease, congestive heart failure, chronic pulmonary disease, diabetes mellitus, cerebrovascular disease, dementia, liver disease, chronic kidney disease, malignancies, sickle cell disease, organ transplantation, and other immunocompromising conditions have been associated with a higher risk of severe disease and death (12–15). Symptoms including dyspnea, coughs, expectoration, hemoptysis, abdominal pain, anorexia, diarrhea, fatigue, myalgia, arthralgia, and fever have been reported more common in severe than in mild COVID-19 patients (16). Physical examination provides valuable information about a patient’s severity and prognosis. Tachypnea, tachycardia, hypotension, hypoxemia, confusion observed on physical examination are poor prognostic signs in COVID-19 patients (17, 18).
Laboratory tests are essential to determine hospitalization and therapy in patients with symptoms of infection. Several laboratory parameters monitoring hematological status or biochemical, inflammatory, immunological, and coagulation processes have been identified as prognostic factors for COVID-19 disease. Severe and fatal cases tended to show higher white blood cell, lower lymphocyte and platelet count, lower percentages of monocytes, eosinophils, and basophils, higher leukocyte and neutrophil-counts and a higher neutrophil lymphocyte ratio compared to mild cases (19, 20).
Some laboratory biomarkers including C-reactive protein (CRP), interleukin 6 (IL-6), ferritin, D-dimer, lactate dehydrogenase (LDH), leukopenia and cardiac troponin (cTn), in addition to clinical symptoms, such as fever have been identified as markers of MIS and cytokine storm associated with COVID-19 (21–23). For example, both CRP and D-dimer levels were elevated in patients in need for transfer to ICU compared to non-ICU patients (22). D-dimer > 3,500 ng/ml was associated with poor survival (24). Procalcitonin is a reliable indicator of bacterial co- or superinfection, the latter being a characteristic factor in the mortality of respirated patients (15).
Several composite scores have been developed for the assessment of general state and risk in CAP that may be applied for COVID-19 as well (25). These include APACHE, qSOFA, PSI, CURB65, and A-DROP (25). Among these scoring systems, CURB65 [confusion, blood urea nitrogen (BUN) > 7 mmol/l, respiratory rate ≥ 30/min, low blood pressure (BP; diastolic BP ≤ 60 mmHg or systolic BP < 90 mmHg) and age ≥ 65 years] has been introduced by the British Thoracic Society (8, 25, 26). More recently, A-DROP, a modified version of CURB65 has been validated by the Japanese Respiratory Society (8, 25). The A-DROP scoring system includes Age (≥70 years in males and ≥ 75 years in females), Dehydration (BUN ≥ 7.5 mmol/l), Respiratory failure (SaO2 ≤ 90% or PaO2 ≤ 60 mmHg), Orientation disturbance (confusion) and low blood Pressure (systolic BP ≤ 90 mmHg (8, 25). It has been confirmed that A-DROP and CURB65 are equivalent for predicting CAP severity (8, 25). The prognostic value of A-DROP has been studied in only very few cohorts (25, 27, 28).
In this study, we assessed severity and potential prognostic risk factors for unfavorable outcome among hospitalized COVID-19 patients admitted to our center. We also applied the A-DROP general scoring system used in CAP to COVID-19.
This single-center, retrospective cohort study was conducted at the dedicated COVID-19 department of the Borsod Academic County Hospital, Miskolc, Hungary. Data from patients hospitalized for COVID-19 pneumonia between October 1, 2020, and March 31, 2021 were retrospectively analyzed. Confirmation of SARS-CoV-2 infection was performed by RT-PCR method from throat-swab specimens. Pneumonia was confirmed by radiological imaging performing chest CT in 227 and plain X-ray in 6 cases. Most patients received favipiravir, corticosteroid (dexamethasone or methylprednisolone), enoxaparine treatment, as well as oxygen supplementation. In selected cases, remdesivir or tocilizumab was also introduced. The clinical criteria for hospital discharge included absence of fever for at least 3 days, cessation or significant improvement of respiratory symptoms, as well as clear improvement of the radiological picture.
The Ethics Committee of the Borsod Academic County Hospital approved this study (BORS 04/2021). We conducted this study according to the Declaration of Helsinki.
We reviewed all clinical electronic medical records and laboratory reports, as well as chest CT and X-ray images. We collected data on age, sex, as well as history of smoking, chronic comorbidities including hypertension, coronary arterial disease (CAD), chronic obstructive pulmonary disease (COPD) or bronchial asthma, previous stroke, diabetes mellitus, current malignancy, chronic kidney disease (CKD), obesity, as well as the use of systemic immunosuppressive therapy within 1 month prior to the analysis. We also recorded the duration and type of symptoms (fever: axillary temperature ≥ 38°C, cough, dyspnea, confusion), vital signs (blood pressure, oxygen saturation [SaO2] by pulse oximetry), laboratory values [white blood cell, absolute lymphocyte and platelet counts, serum CRP, ferritin, IL-6, LDH, D-dimer, procalcitonin (PCT), BUN, creatinine, alanine aminotransferase (ALT), aspartate aminotransferase (AST), D-dimer], partial arterial oxygen pressure (PaO2) as determined by blood gas analysis, as well as treatment (corticosteroids, antiviral, and antibacterial agents, targeted therapies) at hospital admission and during the time of hospitalization. We also recorded the occurrence of pulmonary embolism and Clostridium difficile infection during hospitalization. A-DROP scores were calculated from the data obtained at the time of hospital admission (8).
All data were evaluated by two physicians (MS, ZK) and a third researcher (ZS) adjudicated any difference in interpretation between the two primary reviewers.
The primary outcome parameters were the need for intensive care, need for invasive (IV) vs. Non-invasive ventilation (NIV) and mortality. Mortality was calculated from mortality observed during hospitalization, and the disease-related mortality 30 days after discharge. The time of hospitalization was also recorded.
Statistical analysis was performed using the SPSS software v.26.0 (IBM, Armonk, NY, United States). Data are expressed as mean ± SD for continuous and case number plus percentages (n, %) for categorical variables. The distribution of continuous variables was determined by Kolmogorov-Smirnov test. Continuous variables were assessed by Mann-Whitney U-tests. Nominal variables were compared by χ2 or Fisher’s exact test. Spearman’s analysis was used to test for correlations. Receiver Operating Characteristic (ROC) curves show the sensitivity and specificity for every possible cut-off for a test. Area under the ROC curve is measure of the usefulness of a characteristic, where a greater area means a more useful test. P-values < 0.05 were considered significant in all tests mentioned above.
Altogether 233 patients were included in this study. Their main characteristics are included in Table 1. The patient cohort included 148 men and 85 women with a mean age of 56.8 ± 8.7 years (range: 40–76 years). Disease duration (time from the first symptom to hospital admission) was 8.5 ± 5.3 days (range: 1–35 days). Altogether 7.3% received immunosuppression, 19.1% were current smokers. The medical history of the patients included hypertension (65.1%), CAD (22%), stroke (6%), CKD (5.6%), diabetes mellitus (27.2%), obesity (30.6%), malignancies (4.3%), and COPD/asthma (22%). At the time of admission, about two-third of patients had fever, dyspnea and/or coughs, while 4.3% had confusion/dizziness (Table 1). According to the mean laboratory values, most of these patients had elevated CRP, LDH, ferritin, D-dimer and IL-6 levels indicating systemic inflammation (MIS) (Table 1). Out of the 233 hospitalized patients, 49 (21.2%) required admission to ICU. Altogether 46 patients (19.7%) needed ventilation, out of which 9 (3.9%) required NIV and 37 (15.9%) invasive ventilation (IV). Forty patients (17.2%) died. The mean (± SD) duration of hospitalization was 12.1 ± 6.8 days (range: 2–48 days) (Table 1).
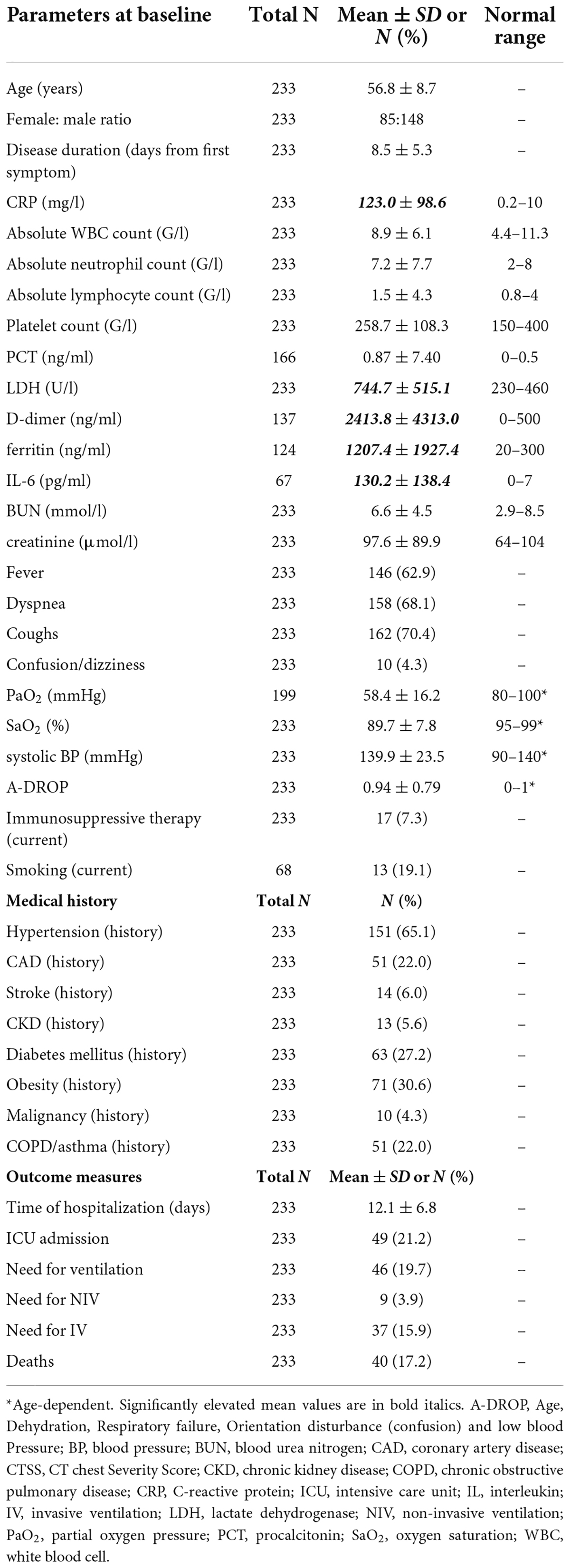
Table 1. Patient characteristics.
In the binary analysis, admission to ICU was significantly more often associated with the duration of hospitalization (p < 0.001), hypertension (p = 0.002) or obesity (p = 0.014) in the medical history, as well as with confusion/dizziness at hospital admission (p = 0.034). Among the laboratory parameters, ICU admission was associated with higher absolute leukocyte (p = 0.045), higher neutrophil (p = 0.034) and lower lymphocyte counts (p = 0.007), CRP (p < 0.001), PCT (p < 0.001), LDH (p < 0.001), ferritin (p = 0.042), IL-6 (p = 0.026), BUN (p = 0.015), creatinine (p = 0.001), PaO2 (p = 0.001) and SaO2 (p = 0.001) (Table 2).
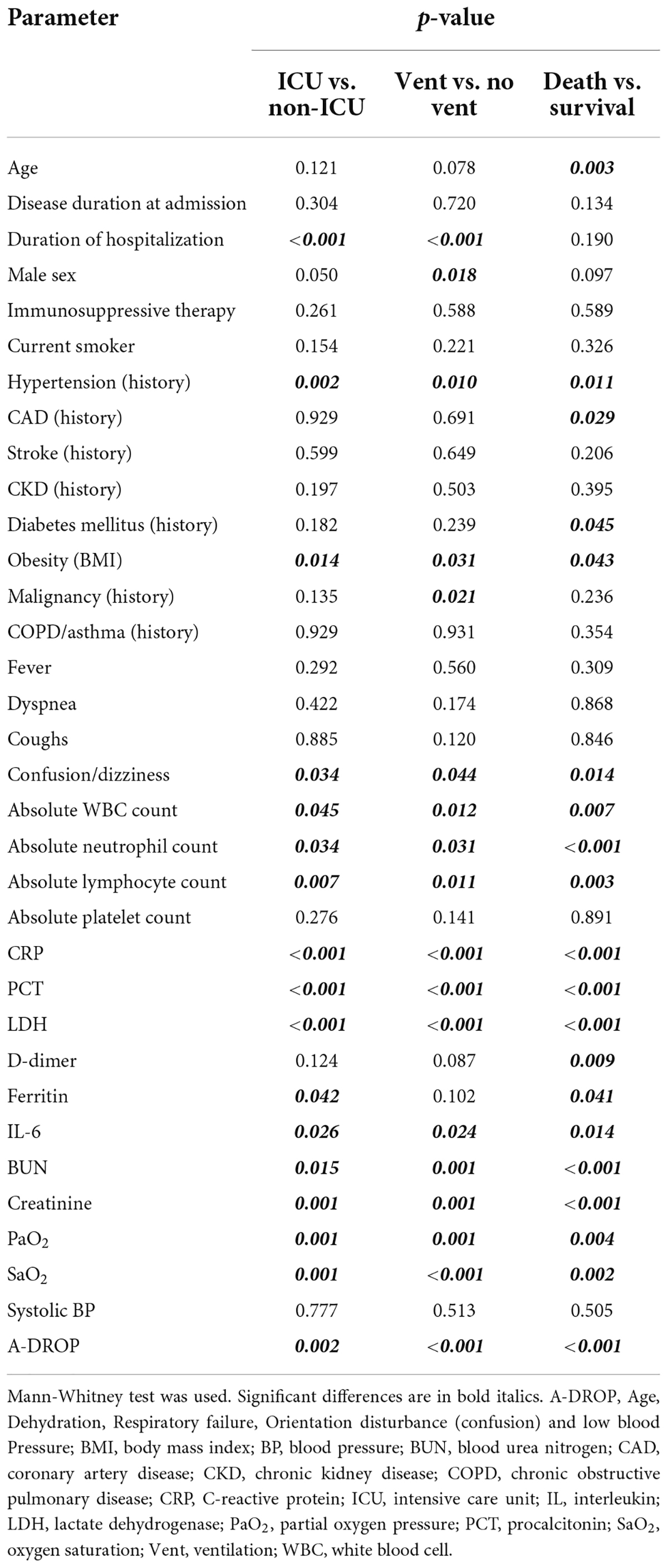
Table 2. Determinants of ICU admission, need for ventilation and survival.
The need for ventilation was significantly associated with days of hospitalization (p < 0.001), male sex (p = 0.018), history of hypertension (p = 0.010), obesity (p = 0.031) or malignancy (p = 0.021), as well as with confusion/dizziness upon admission (p = 0.044). Among the laboratory parameters, the need for ventilation was associated with leukocytosis (p = 0.012), neutrophilia (p = 0.031) and lymphopenia (p = 0.011), as well as CRP (p < 0.001), PCT (p < 0.001), LDH (p < 0.001), IL-6 (p = 0.024), BUN (p = 0.001), creatinine (p = 0.001), PaO2 (p = 0.001), and SaO2 (p < 0.001) (Table 2).
Finally, death was associated with age (p = 0.003), hypertension (p = 0.011), CAD (p = 0.029), diabetes mellitus (p = 0.045) or obesity (p = 0.043) in the medical history, as well as with confusion/dizziness at hospital admission (p = 0.014). Poor survival was associated with higher absolute leukocyte (p = 0.007) and neutrophil (p < 0.001) but lower lymphocyte counts (p = 0.003), as well as CRP (p < 0.001), PCT (p < 0.001), LDH (p < 0.001), D-dimer (p = 0.009), ferritin (p = 0.041), IL-6 (p = 0.014), BUN (p < 0.001), creatinine (p < 0.001), PaO2 (p = 0.004) and SaO2 (p = 0.002) (Table 2).
We also assessed possible predictors of ICU admission and survival by ROC curve analysis. Again, higher age was significantly associated with mortality (p = 0.003), but not with the need for ICU admission (p = 0.121) (Table 3). Both lower arterial PaO2 and SaO2 were associated with increased need for ICU admission (p = 0.002 and p = 0.010, respectively) and death (p = 0.004 and p = 0.012, respectively) (Table 3).
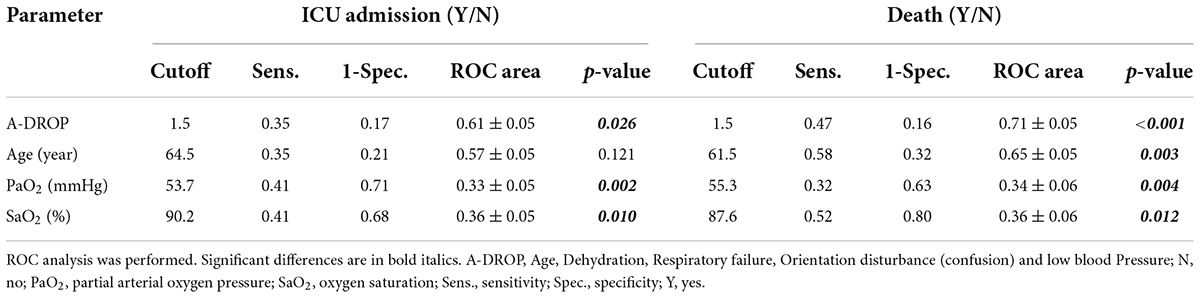
Table 3. Determinants of ICU admission and death.
In the binary analysis, admission to ICU (p = 0.002), the need for ventilation (p < 0.001) and death (p < 0.001) were significantly associated with higher A-DROP (Table 2). In the ROC analysis, A-DROP > 1.5 significantly predicted admission to ICU (p = 0.026) and mortality (p < 0.001) (Table 3 and Figure 1). In the simple Spearman’s correlation analysis, A-DROP significantly and positively correlated with absolute WBC and neutrophil counts, CRP, PCT, LDH, D-dimer, ferritin, IL-6, and creatinine (Table 4).
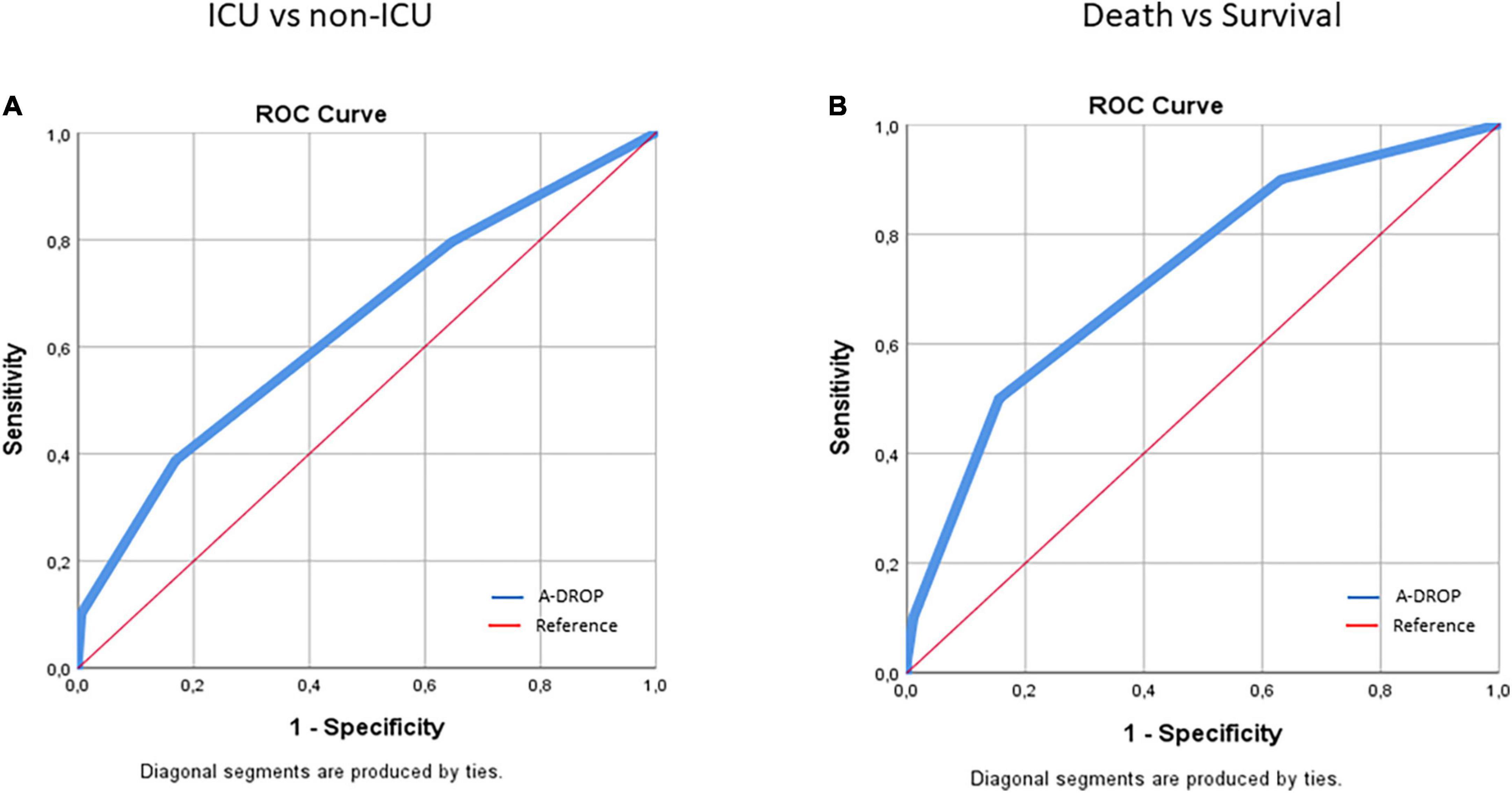
Figure 1. ROC curve analysis of the association of A-DROP values with the need for ICU admission (A) and death (B) in COVID-19 patients.
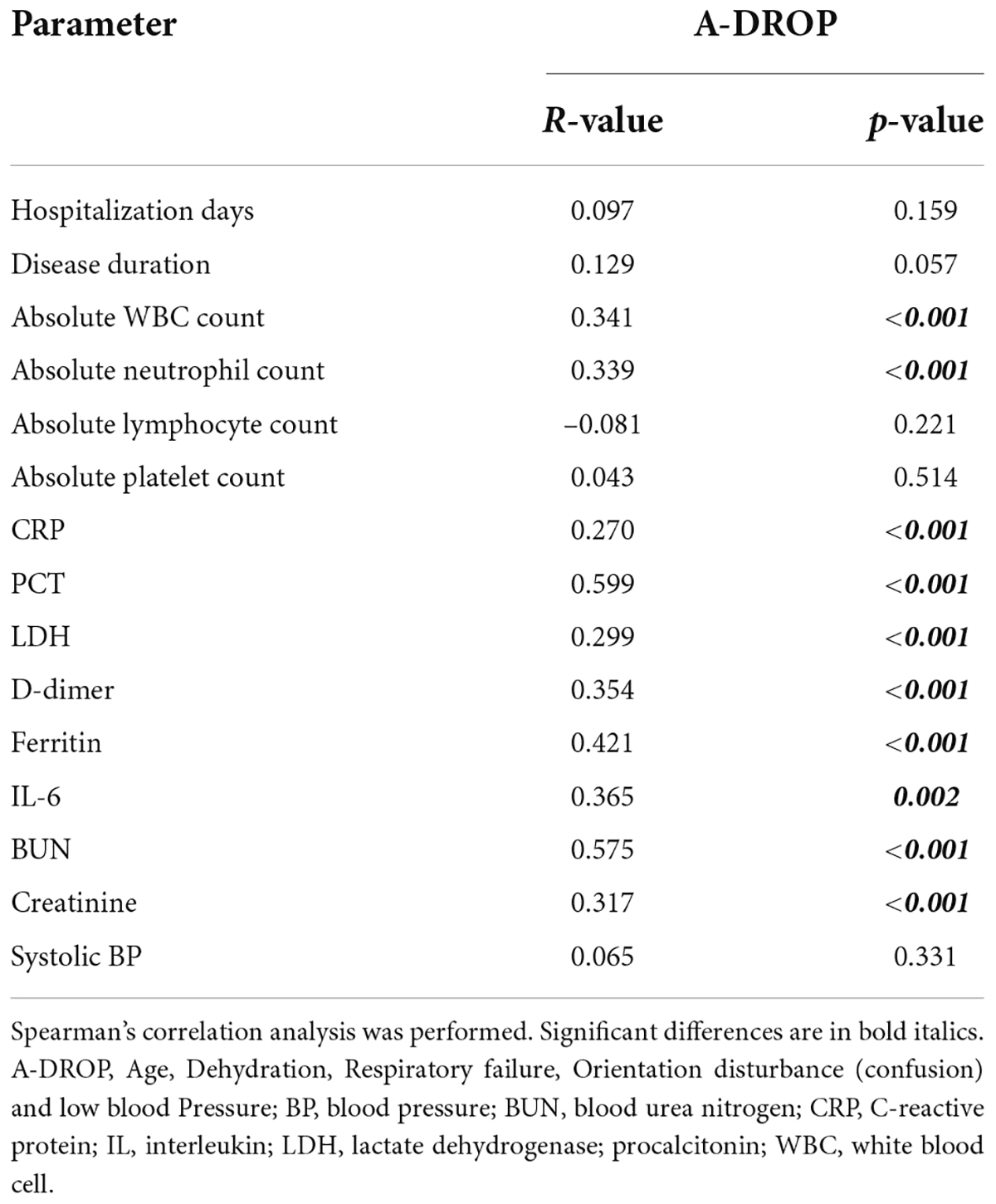
Table 4. Correlations of A-DROP with clinical and laboratory parameters.
In this single-center study of 233 COVID-19 patients admitted to hospital, we assessed elements of medical history, as well as numerous clinical and laboratory parameters in association with the need for admission to ICU, need for ventilation and death. We also focused on the value of the A-DROP scoring system in the assessment of general health and prediction of outcome in hospitalized COVID-19 patients.
At the time of admission, among laboratory biomarkers, patients had elevated CRP, LDH, D-dimer, ferritin, and IL-6 levels. All these parameters, as well as higher absolute WBC and neutrophil and lower absolute lymphocyte counts, PCT, BUN, creatinine, PaO2, and SaO2 were associated with ICU admission, need for ventilation and death. Among clinical and other factor, age was associated with death only, male sex with the need for ventilation only and the duration of hospitalization with the need for ICU admission and ventilation. CRP, IL-6, ferritin, D-dimer, LDH and high neutrophil/lymphocyte, as well as BUN/creatinine ratios have been identified as markers of MIS/cytokine storm associated with SARS-CoV-2 infection (21–23). Both CRP and D-dimer levels were elevated in patients in need for transfer to ICU compared to non-ICU patients (22). D-dimer > 3,500 ng/ml was associated with poor survival (24). Obesity and confusion (dizziness) at the time admission, as well as the history of hypertension were associated with all three outcome measures. Obesity may be associated with increased mortality in COVID-19 (29). Dizziness has also been reported as an indicator of critical outcome in COVID-19 (30).
In addition to other known scoring systems, A-DROP has recently been validated for the assessment of health status in CAP (8, 25). In other studies, A-DROP has proven to be of great value in predicting CAP severity (8, 25). In the present cohort, the mean value of A-DROP at the time of admission was 0.94 on a 0–5 scale. A-DROP value of two or above were significantly associated with the need for ICU admission and ventilation, as well as with death. A-DROP also significantly correlated with absolute WBC and neutrophil counts, CRP, PCT, LDH, D-dimer, ferritin, IL-6, BUN, and creatinine. As discussed above, most of these parameters have been associated with severe COVID-19 including MIS and cytokine storm (21–23).
In other studies, various cardio-pulmonary, renal, hepatic, hematologic, and immunologic comorbidities have been associated with poor COVID-19 outcome (12–15). In addition, similarly to our findings, CRP, IL-6, ferritin, D-dimer, LDH, and troponin have been identified as severity and prognostic markers of COVID-19-associated MIS (21–23).
This study has certain strengths and limitations. The major strength of this study is that this is the first relatively large study assessing the prognostic value of A-DROP in a complex way, in association with numerous clinical and laboratory markers of outcome including ICU admission, ventilation and death in COVID-19. Possible limitations may include the single-center nature of the study. In addition, we have not included chest CT scans in this analysis, we have not validated our findings against other cohorts and we have not considered for population-specific biases.
In conclusion, A-DROP may be a suitable scoring system for predicting the need for ICU admission and ventilation, as well as mortality in COVID-19. In our study, we identified several clinical and laboratory parameters that, when combined with the A-DROP scoring system, could further increase its sensitivity and specificity, providing clinicians with an appropriate risk assessment tool to identify high-risk patients in need of advanced health care. Further studies are planned to develop a scoring system with sufficient sensitivity and specificity.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by the Borsod Academic County Hospital (BORS 04/2021). The patients/participants provided their written informed consent to participate in this study.
MS: study design, patient recruitment, data collection, manuscript drafting, and finalization. ZK, PT, CO, and EC: patient recruitment and data collection. KH: statistical analysis and data interpretation. ZS: supervisor, study design, manuscript drafting, and finalization. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. (2020) 395:470–3. doi: 10.1016/S0140-6736(20)30185-9
2. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. (2020) 58:711–2. doi: 10.1016/j.jemermed.2020.04.004
3. Bhaskar S, Sinha A, Banach M, Mittoo S, Weissert R, Kass JS, et al. Cytokine storm in COVID-19-immunopathological mechanisms, clinical considerations, and therapeutic approaches: the reprogram consortium position paper. Front Immunol. (2020) 11:1648. doi: 10.3389/fimmu.2020.01648
4. Gandhi RT, Lynch JB, Del Rio C. Mild or moderate covid-19. N Engl J Med. (2020) 383:1757–66. doi: 10.1056/NEJMcp2009249
5. Juul S, Nielsen EE, Feinberg J, Siddiqui F, Jorgensen CK, Barot E, et al. Interventions for treatment of COVID-19: a living systematic review with meta-analyses and trial sequential analyses (The LIVING Project). PLoS Med. (2020) 17:e1003293. doi: 10.1371/journal.pmed.1003293
6. Salzberger B, Buder F, Lampl B, Ehrenstein B, Hitzenbichler F, Holzmann T, et al. Epidemiology of SARS-CoV-2. Infection. (2021) 49:233–9. doi: 10.1007/s15010-020-01531-3
7. Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ, et al. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. (2020) 395:1033–4. doi: 10.1016/S0140-6736(20)30628-0
8. Shindo Y, Sato S, Maruyama E, Ohashi T, Ogawa M, Imaizumi K, et al. Comparison of severity scoring systems A-DROP and CURB-65 for community-acquired pneumonia. Respirology. (2008) 13:731–5. doi: 10.1111/j.1440-1843.2008.01329.x
9. Arnold DT, Attwood M, Barratt S, Morley A, Elvers KT, McKernon J, et al. Predicting outcomes of COVID-19 from admission biomarkers: a prospective UK cohort study. Emerg Med J. (2021) 38:543–8. doi: 10.1136/emermed-2020-210380
10. Couderc AL, Correard F, Hamidou Z, Nouguerede E, Arcani R, Weiland J, et al. Factors associated With COVID-19 hospitalizations and deaths in french nursing homes. J Am Med Dir Assoc. (2021) 22:1581–1587e1583. doi: 10.1016/j.jamda.2021.06.023
11. Gessler N, Gunawardene MA, Wohlmuth P, Arnold D, Behr J, Gloeckner C, et al. Clinical outcome, risk assessment, and seasonal variation in hospitalized COVID-19 patients-Results from the CORONA Germany study. PLoS One. (2021) 16:e0252867. doi: 10.1371/journal.pone.0252867
12. Harrison SL, Fazio-Eynullayeva E, Lane DA, Underhill P, Lip GYH. Comorbidities associated with mortality in 31,461 adults with COVID-19 in the United States: a federated electronic medical record analysis. PLoS Med. (2020) 17:e1003321. doi: 10.1371/journal.pmed.1003321
13. Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature. (2020) 584:430–6. doi: 10.1038/s41586-020-2521-4
14. Rosenthal N, Cao Z, Gundrum J, Sianis J, Safo S. Risk factors associated with in-hospital mortality in a US national sample of patients with COVID-19. JAMA Netw Open. (2020) 3:e2029058. doi: 10.1001/jamanetworkopen.2020.29058
15. Guan WJ, Liang WH, Zhao Y, Liang HR, Chen ZS, Li YM, et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: a nationwide analysis. Eur Respir J. (2020) 55:2000547. doi: 10.1183/13993003.01227-2020
16. He X, Cheng X, Feng X, Wan H, Chen S, Xiong M. Clinical symptom differences between mild and severe COVID-19 patients in China: a meta-analysis. Front Public Health. (2020) 8:561264. doi: 10.3389/fpubh.2020.561264
17. Izcovich A, Ragusa MA, Tortosa F, Lavena Marzio MA, Agnoletti C, Bengolea A, et al. Prognostic factors for severity and mortality in patients infected with COVID-19: a systematic review. PLoS One. (2020) 15:e0241955. doi: 10.1371/journal.pone.0241955
18. Gallo Marin B, Aghagoli G, Lavine K, Yang L, Siff EJ, Chiang SS, et al. Predictors of COVID-19 severity: a literature review. Rev Med Virol. (2021) 31:1–10. doi: 10.1002/rmv.2146
19. Henry BM, de Oliveira MHS, Benoit S, Plebani M, Lippi G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): a meta-analysis. Clin Chem Lab Med. (2020) 58:1021–8. doi: 10.1515/cclm-2020-0369
20. Ponti G, Maccaferri M, Ruini C, Tomasi A, Ozben T. Biomarkers associated with COVID-19 disease progression. Crit Rev Clin Lab Sci. (2020) 57:389–99. doi: 10.1080/10408363.2020.1770685
21. Webb BJ, Peltan ID, Jensen P, Hoda D, Hunter B, Silver A, et al. Clinical criteria for COVID-19-associated hyperinflammatory syndrome: a cohort study. Lancet Rheumatol. (2020) 2:e754–63. doi: 10.1016/S2665-9913(20)30343-X
22. Reyes AZ, Hu KA, Teperman J, Wampler Muskardin TL, Tardif JC, Shah B, et al. Anti-inflammatory therapy for COVID-19 infection: the case for colchicine. Ann Rheum Dis. (2021) 80:550–7. doi: 10.1136/annrheumdis-2020-219174
23. Caricchio R, Gallucci M, Dass C, Zhang X, Gallucci S, Fleece D, et al. Preliminary predictive criteria for COVID-19 cytokine storm. Ann Rheum Dis. (2021) 80:88–95. doi: 10.1136/annrheumdis-2020-218323
24. Sciascia S, Apra F, Baffa A, Baldovino S, Boaro D, Boero R, et al. Pilot prospective open, single-arm multicentre study on off-label use of tocilizumab in patients with severe COVID-19. Clin Exp Rheumatol. (2020) 38:529–32.
25. Fan G, Tu C, Zhou F, Liu Z, Wang Y, Song B, et al. Comparison of severity scores for COVID-19 patients with pneumonia: a retrospective study. Eur Respir J. (2020) 56:2002113. doi: 10.1183/13993003.02113-2020
26. Barlow G, Nathwani D, Davey P. The CURB65 pneumonia severity score outperforms generic sepsis and early warning scores in predicting mortality in community-acquired pneumonia. Thorax. (2007) 62:253–9. doi: 10.1136/thx.2006.067371
27. Miyashita N, Matsushima T, Oka M, Japanese Respiratory S. The JRS guidelines for the management of community-acquired pneumonia in adults: an update and new recommendations. Intern Med. (2006) 45:419–28. doi: 10.2169/internalmedicine.45.1691
28. Ucan ES, Ozgen Alpaydin A, Ozuygur SS, Ercan S, Unal B, Sayiner AA, et al. Pneumonia severity indices predict prognosis in coronavirus disease-2019. Respir Med Res. (2021) 79:100826. doi: 10.1016/j.resmer.2021.100826
29. Kristensen NM, Gribsholt SB, Andersen AL, Richelsen B, Bruun JM. Obesity augments the disease burden in COVID-19: updated data from an umbrella review. Clin Obes. (2022) 2022:e12508. doi: 10.1111/cob.12508
Keywords: COVID-19, tocilizumab (IL-6 inhibitor), prognosis, pneumonia, outcome, A-DROP score
Citation: Szabó M, Kardos Z, Oláh C, Tamáska P, Hodosi K, Csánky E and Szekanecz Z (2022) Severity and prognostic factors of SARS-CoV-2-induced pneumonia: The value of clinical and laboratory biomarkers and the A-DROP score. Front. Med. 9:920016. doi: 10.3389/fmed.2022.920016
Received: 14 April 2022; Accepted: 04 July 2022;
Published: 22 July 2022.
Edited by:
Zisis Kozlakidis, International Agency For Research on Cancer (IARC), FranceReviewed by:
Hussein Kadhem Al-Hakeim, University of Kufa, IraqCopyright © 2022 Szabó, Kardos, Oláh, Tamáska, Hodosi, Csánky and Szekanecz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zoltán Szekanecz, c3pla2FuZWN6QGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.