 Jianguo Zhang
Jianguo Zhang Nan Chen2†
Nan Chen2† Zhimin Tao
Zhimin Tao- 1Department of Emergency Medicine, The Affiliated Hospital, Jiangsu University, Zhenjiang, China
- 2Jiangsu Province Key Laboratory of Medical Science and Laboratory Medicine, School of Medicine, Jiangsu University, Zhenjiang, China
- 3Department of Critical Care Medicine, The First Affiliated Hospital of Soochow University, Suzhou, China
- 4Department of Critical Care Medicine, The Affiliated Hospital, Jiangsu University, Zhenjiang, China
Background: Currently, as the omicron variant of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) surges amid the coronavirus disease 2019 (COVID-19) pandemic, its clinical characteristics with intrinsic severity and the protection from vaccination have been understudied.
Methods: We reported 169 COVID-19 patients that were infected with the omicron variant of SARS-CoV-2 and hospitalized in Suzhou, China, from February to March 2022, with their demographic information, medical/immunization history, clinical symptom, and hematological profile. At the same time, patients with none/partial (one-dose), full (two-dose) and three–dose vaccination were also compared to assess the vaccine effectiveness.
Findings: For the omicron COVID-19 patients included in this study, their median age was 33.0 [interquartile range (IQR): 24.0–45.5], 53.3% were male and the median duration from illness onset to hospitalization was 2 days. Hypertension, bronchitis, and diabetes were the leading comorbidities among patients. While the common clinical symptoms included cough, fever, expectoration, and fatigue, etc., asymptomatic patients took up a significant portion (46.7%). For hematological parameters, most values revealed the alleviated pathogenicity induced by the omicron variant infection. No critically ill or deceased patients due to COVID-19 infection were reported in this study.
Interpretation: Our results supported that the viremic effect of the omicron variant became milder than the previous circulating variants, while full vaccination or booster shot was greatly desired for an effective protection against clinical severity.
Introduction
The unprecedented pandemic of coronavirus disease 2019 (COVID-19) started more than 2 years ago (1). Ever since, the world has been jolted by serial waves of COVID-19 outbreaks triggered by the evolving mutants from the responsible pathogen, i.e., severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (2, 3). So far, the alpha, beta, gamma, delta, and omicron variants of SARS-CoV-2 have been designated as variants of concern (VOCs) with high infectivity and virulence, while each later one surfaces with the higher transmissibility than the previous (4). As of March 20, 2022, the reported COVID-19 cases exceeded 468 million with an estimated fatality rate of 1.3% (5).
Presently, the omicron variant of SARS-CoV-2 outpaces others to be the dominant circulating strain, sweeping across the world (6). The major omicron sublineages that prevail among the local COVID-19 outbreaks in China are BA.1 and BA.2 (7–9). It was first discovered in November 2021 in South Africa, when the early study on the characteristics and outcomes of hospitalized COVID-19 patients infected by the omicron variant indicated that the infection was associated with significantly lessened length of hospital stays and reduced severity and mortality, when compared to the previous COVID-19 hits (10, 11). However, the omicron variant possessed much more mutations in viral genome than any of the other VOCs (12). Furthermore, convalescent sera from recovered patients infected by the alpha, beta or delta variant could not neutralize the omicron variant, while sera from fully vaccinated persons (two doses of mRNA or vector vaccines) enabled neutralization of the omicron variant to a lesser extent than that of the delta variant (13). For those reasons, there are raising concerns about whether the immune evasion and pathogenic influence of the omicron variant would be more severe than the previous strains.
In the earlier reports we analyzed and compared the clinical characteristics between patients infected by the wild-type or delta variant SARS-CoV-2 (14, 15). Herein we investigated the demographic information and baseline characteristics of confirmed COVID-19 patients infected with the omicron variants during the recent coronavirus flareup in the city of Suzhou, China, in February and March 2022. Through this study we seek to understand the clinical manifestations of COVID-19 patients infected by the omicron variant of SARS-CoV-2 and how the vaccination status might protect from severity.
Methods
Patient Information
The retrospective study included 169 COVID-19 patients who were admitted to the Fifth People's Hospital of Suzhou (TFPHS, the Affiliated Infectious Diseases Hospital of Soochow University), Jiangsu Province, China, from February 13 to March 21, 2022. COVID-19 infections were confirmed as reported (16). Exclusion criteria were as follows: patients with malignancy, pregnancy, blood disease, or autoimmune deficiency, and patients who failed to complete blood examinations, and patients who were younger than 12 years. The study was approved by the Research Ethics Commission of TFPHS. Patient information remained anonymous, and written consents were waived due to a major infectious disease outbreak.
Procedure and Vaccination
COVID-19 patients infected by the omicron variant of SARS-CoV-2 were hospitalized and treated as reported (17). Blood cell analysis was conducted by an automated XN1000 hematology analyzer (SYSMEX, Japan), and biochemical indicators were analyzed using VITROS 350 autoanalyzer (Johnson &. Johnson, USA). Computed tomography (CT) was performed using BrightSpeed 16 CT Scanner (GE Healthcare, USA). The scanning parameters were set as 120 kVp, 80 mA, 1.5-mm collimation, reconstruction matrix of 512 × 512, slice thickness of 5.0 mm, scan field of view (FOV) of 25 × 25 cm, and high spatial resolution algorithm. For most of admitted COVID-19 patients in TFPHS, two types of inactivated vaccines (Sinovac or Sinopharm) have been administered. Serological tests of patients based on detection of SARS-CoV-2-specific immunoglobulin M (IgM) and immunoglobulin G (IgG) were conducted, using 2019-nCoV Ab test kit (colloidal gold), manufactured by Innovita Biological Technology Co. Ltd., China.
Statistical Analysis
Data were summarized as the median and IQR values for continuous variables and frequencies for categorical variables. For comparisons between two groups, Mann-Whitney U test was used for continuous variables. Categorical variables were examined by Chi-squared test. All calculated p-values were two-sided, and p-values < 0.05 were considered statistically significant. All statistical analyses were performed using SPSS version16.0 (SPSS Inc., Chicago, IL).
Results
Baseline Characteristics of COVID-19 Patients Infected by the Omicron Variant of SARS-CoV-2
In this study 169 COVID-19 patients infected by the omicron variant of SARS-CoV-2 were hospitalized in Suzhou, Jiangsu Province, China, from February to March 2022. Their median age was 33.0 (IQR: 24.0–45.5), 53.3% were male, and the median duration time from illness onset to hospitalization was 2.00 days (IQR: 2.00–3.00) (Table 1). We further grouped the patients into three subgroups; that is, one with none (34 patients, 20.1%) or partial (one-dose) vaccination (12 patients, 7.1%) (a total of 46 patients or 27.2% of the total patients in this subgroup), one with full (two-dose) vaccination (78 patients, 46.2%), and one that received booster shots (i.e., three-dose vaccination) (45 patients, 26.6%). Then, demographic information, medical history, clinical symptom, and antibody response were analyzed for all patients, together with comparisons of those baseline characteristics between patients none/partially vaccinated and patients fully vaccinated (indicated by p1 values), and between patients none/partially vaccinated and patients three doses vaccinated (indicated by p2 values) (Table 1).
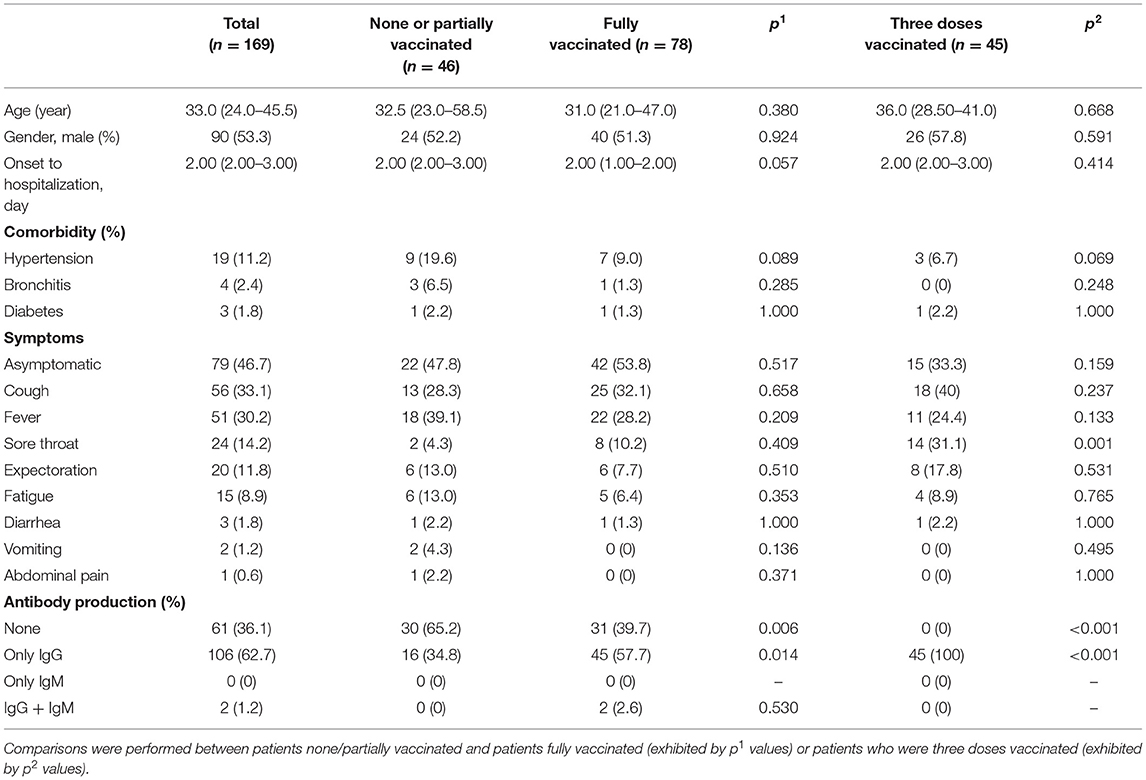
Table 1. Demographic information, medical/immunization history, clinical symptom, and antibody production in the COVID-19 patients infected by the omicron variant in Suzhou, China, in February and March 2022.
Among all patients, hypertension, bronchitis, and diabetes were the leading comorbidities. Notably, in addition to those with typical symptoms of cough, fever, sore throat, expectoration, and fatigue, etc., asymptomatic patients occupied a nearly half portion of total infections. Irrespective of immunization status, 36.1% COVID-19 patients infected by the omicron variant did not develop antibody response, while 62.7% produced only IgG and only 1.2% produced both IgG and IgM. There was no noticeable difference between patients fully vaccinated or booster shot (three doses) vaccinated and patients none/partially vaccinated in terms of the baseline characteristics, except that IgG production significantly increased as the vaccination times added up.
Laboratory Parameters of COVID-19 Patients Infected by the Omicron Variant of SARS-CoV-2
A substantial portion of the omicron COVID-19 patients demonstrated abnormal levels of white blood cells, neutrophils, lymphocytes, and monocytes, showing signs of leukocytosis, neutrophilia, lymphocytopenia and monocytosis (Table 2). In contrast, the count of red blood cells (RBCs), and the levels of hemoglobin and hematocrit among most omicron COVID-19 patients remained within the normal range, indicating that anemia was insignificant among the majority of patients. Similarly, thrombocytopenia was also marginal with only 4.1% patients tested abnormal, as the platelet levels in most omicron variant infections were regular. Nevertheless, coagulopathy was found in a moderate proportion of omicron COVID-19 patients. For instance, the D-dimer levels of most patients fell in the normal range, still leaving 11.8% patients (20 out of 169) with abnormally high values. Similar coagulopathic incidents included the prolonged prothrombin time and activated partial thromboplastin time. Thereby, examining the viremia of the omicron variant on blood profiles of patients, mild hematological impairment was spotted, implying a modest degree of virulence.
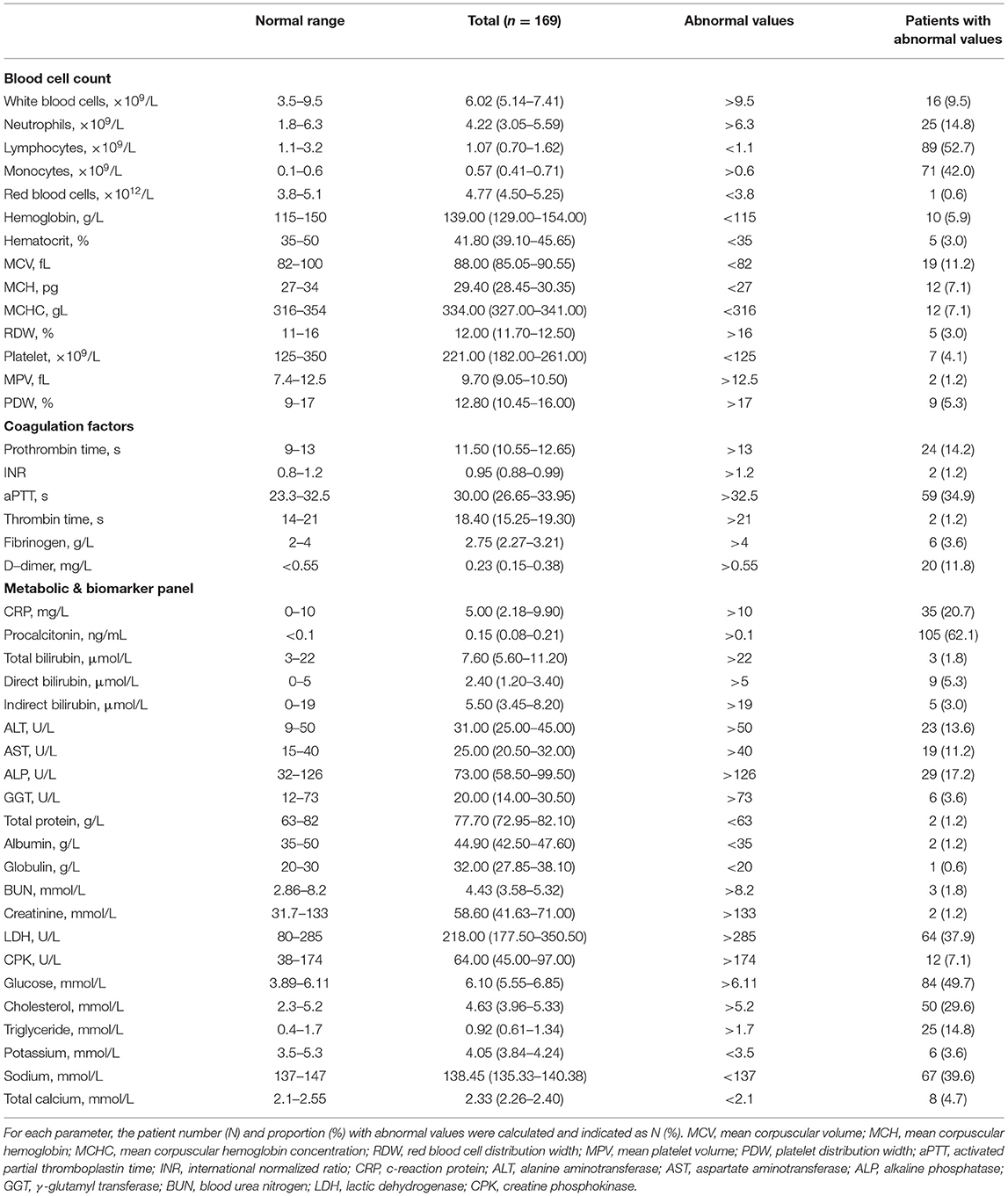
Table 2. Baseline characteristics of COVID-19 patients infected by the omicron variant in their hematological profiles.
Most biochemical indicators in the omicron COVID-19 patients revealed the mild impact. Markedly, the median level of procalcitonin in all patients was abnormally elevated with 62.1% patients possessing higher values than normal. Similarly, the portions of patients with aberrant values of c-reactive proteins, alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, lactic dehydrogenase, glucose, cholesterol, triglyceride, and sodium were substantial or considerable. Those results indicated that the infection of the omicron variant still caused noticeable injuries on major organs, such as liver and heart. As shown in Table 3, compared to patients who were none/partially vaccinated, patients fully vaccinated did not exhibit a significant difference in their hematological profile, and patients with booster vaccination demonstrated some alleviated characteristics, including mitigations in thrombocytopenia, thrombin time prolonging, and alkaline phosphatase elevation, with most baseline characteristics undifferentiable from those in patients who were none/partially vaccinated.
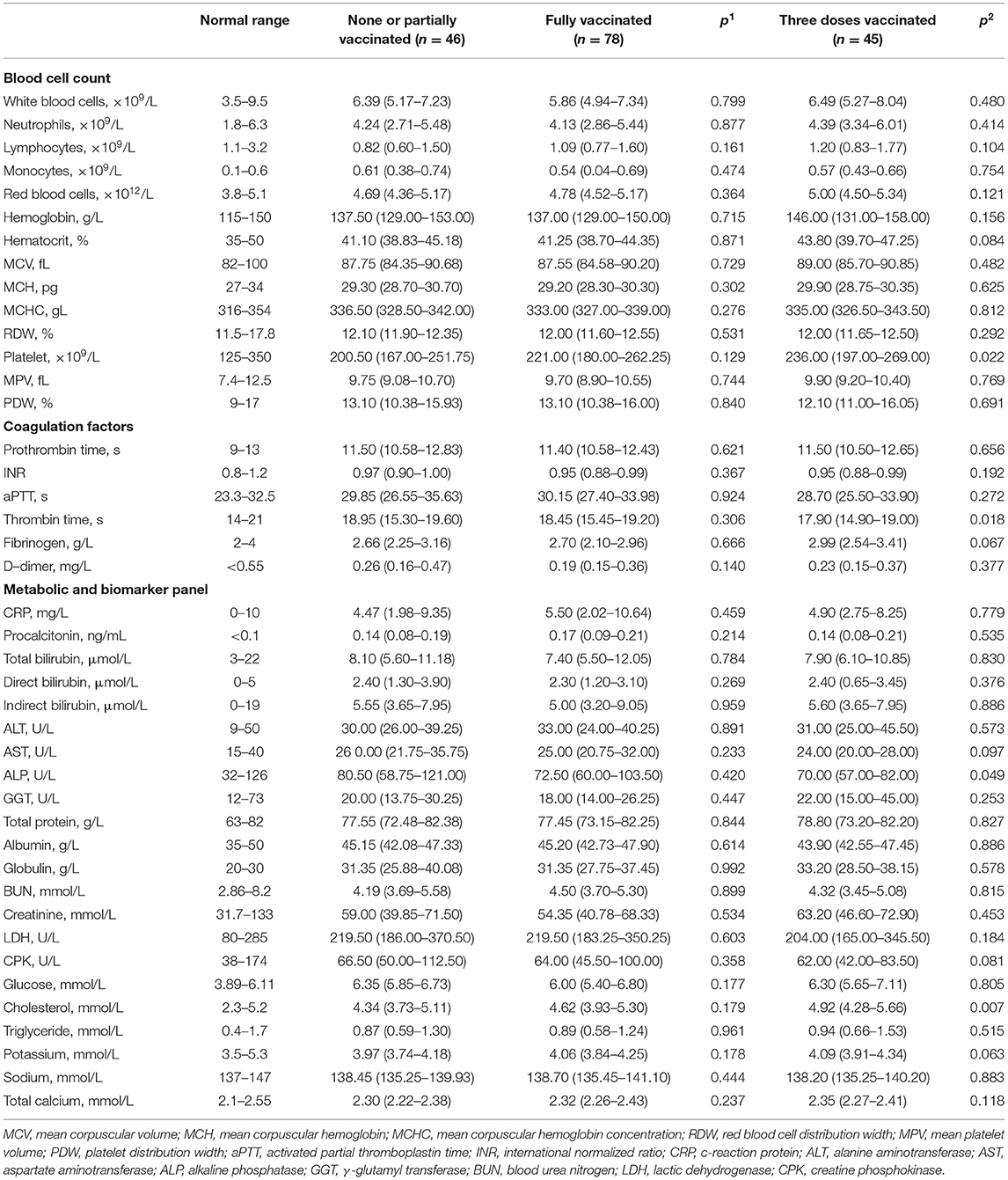
Table 3. The hematological profiles of COVID-19 patients infected by the omicron variant were divided into three subgroups and thereby compared between patients with none or partial vaccination and patients with full vaccination (exhibited by p1 values), or between patients with none or partial vaccination and patients with three-dose vaccination (exhibited by p2 values).
CT Features of COVID-19 Patients Infected by the Omicron Variant of SARS-CoV-2
Table 4 lists all common CT features of the omicron COVID-19 patients in our study. The individual proportion of patients with each CT feature was calculated in each subgroup and compared between different subgroups. The pathological characters in patients' lungs exhibited a high occurrence of unilateral and bilateral involvement, lesions located at left or right lower lobes and peripheral distribution. CT features were typified by ground glass opacities (GGOs), linear opacities, and air bronchogram (Figure 1). Among all patients, the incidences of consolidation or craze paving pattern became much lessened, showing milder pathological changes in lungs caused by the omicron variant. Furthermore, compared to those in the patient subgroup of none/partial vaccination, the CT characteristics in the patient subgroup of full vaccination did not reveal any noticeable difference, while some CT features in the patient subgroup of booster vaccination, including the bilateral involvement, lesion location at right middle and lower lobes, and crazy paving pattern, showed much reduced incidence.
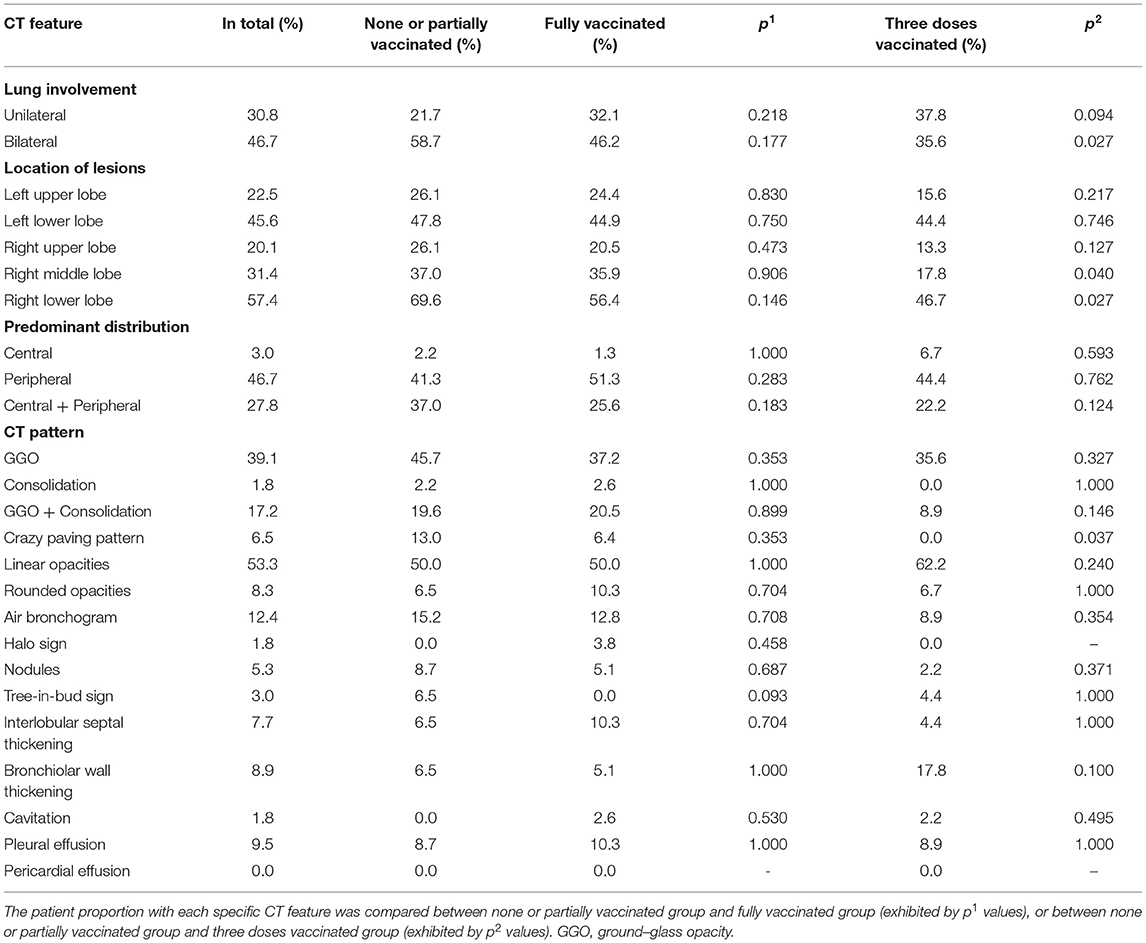
Table 4. The CT features of COVID-19 patients infected by the omicron variant were divided into three subgroups as indicated.
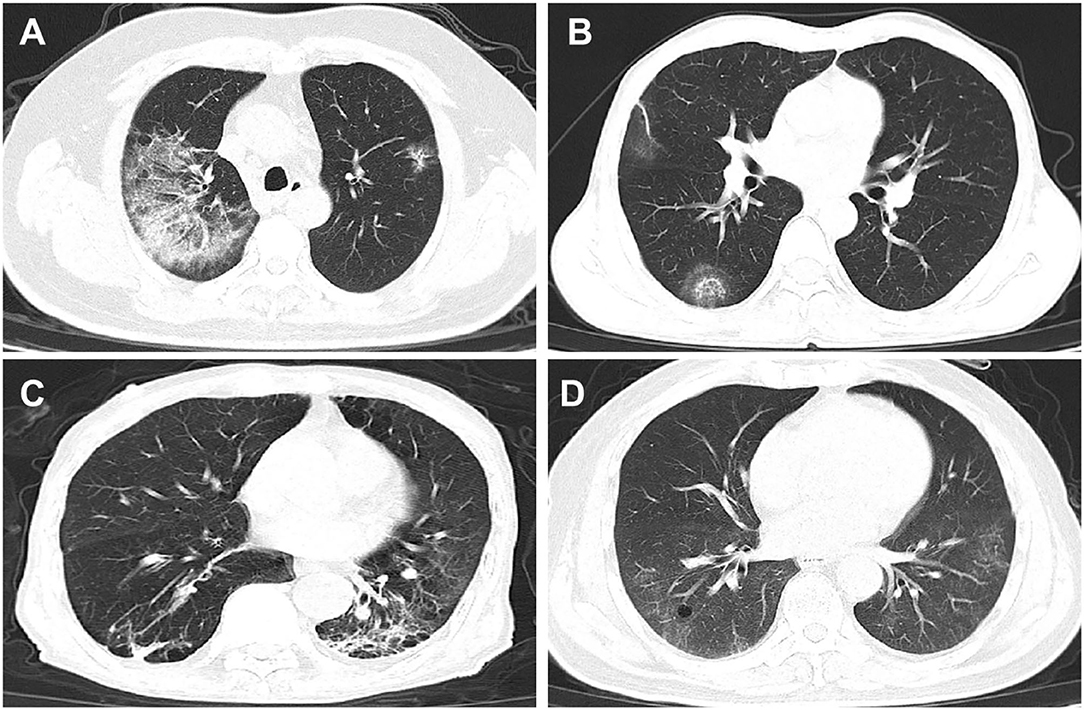
Figure 1. Selected CT graphs of COVID-19 patients infected by the omicron variant of SARS-CoV-2 in Suzhou, China in 2022, taken upon hospital admission, showing representative pathological changes in lungs. (A) From a 64-year-old man with fever and cough symptoms. Axial CT image showed GGOs and consolidation in the right upper lobe, taken on the fifth day from illness onset. (B) From a 53-year-old man having cough and fever. CT image showed rounded opacities in the right lower lobe, taken on the eighth day from illness onset. Lesions were peripherally distributed. (C) From a 61-year-old man with fever. CT image showed linear opacities in the right and left lobes, and lesions were peripherally distributed. Image was taken on the fifth day from illness onset. (D) From a 75-year-old man with cough and fever. Axial CT image showed GGOs and cavitation in the right lobe, and lesion distributions were central and peripheral. Image was taken on the tenth day from illness onset.
Discussion
Early studies reported by South African researchers, where the omicron variant was first discovered after nearly half population had been vaccinated and over half population had been exposed to SARS-CoV-2, suggested much attenuated pathogenicity with plummeted severity and mortality during the wide spreading of the omicron variant (10, 11, 18). Similar findings were also reported from other countries, including the United States, France, and South Korea (19–21), where vaccination coverage and population infection were both substantially high. Thereby, questions remain whether this reduced pathogenicity is due to the weakened intrinsic viremia or the strengthened acquired immunity by previous infection or/and sufficient vaccination, or both.
Differing from most of other countries, China has a high vaccination coverage but a low population of COVID-19 infection where reinfection cases are rare. Therefore, the acquired immunity against COVID-19 basically comes from effective vaccination rather than previous natural infection. Here our study that included 169 COVID-19 patients infected with the omicron variant of SARS-CoV-2 demonstrated a reduced clinical severity where mild infection profiles were observed. No critically ill or deceased patients were reported due to the omicron infection. This result mirrors an attenuated pathogenicity of the omicron variant compared to that induced by the wild-type strain or other VOCs and accents the importance of timely vaccination (with a booster shot) in order to significantly reduce the severity and lower the fatality.
Being a rapidly evolving RNA virus, SARS-CoV-2 recently mutates into its omicron variant with a much higher effective reproduction number than that of the delta variant (3.6–4.2 times), demonstrating an astounding infectivity and transmissibility (22, 23). Insofar, among all five VOCs, the omicron variant possessed the highest mutations in the genome structure (~50 mutations), where more than 32 mutations occurred in the spike protein (24). Those mutations take responsibility for the enhanced binding capacity to angiotensin-converting enzyme 2 (ACE2) (e.g., T478K, N501Y) and/or the increased cleavage activity by host furin (e.g., N679K, P681H), leading to much elevated infectivity and transmissibility of this variant; simultaneously, particular amino acid changes (e.g., E484A) in the spike protein enable to dodge the neutralizing antibodies, which eventually results in the heightened ability of immune escape (12, 15, 24, 25).
As a matter of fact, convalescent sera from the wild-type SARS-CoV-2 infection revealed a significantly lower degree of neutralization against the omicron variant than the delta variant (26). Sera from unvaccinated individuals infected with the alpha, beta, or delta variant of SARS-CoV-2 barely neutralized the omicron variant (13). Similarly, sera from patients infected by the omicron variant had residual cross-reactivity with other VOC (27). In parallel, sera from fully (two doses) vaccinated individuals reacted the least with the omicron variant among all reactions to VOCs (28). Those could explain why the breakthrough infection incidents in the omicron COVID-19 cases occurred frequently regardless of previous infection or vaccination history. Nevertheless, a booster vaccine, irrespective of vaccine type (e.g., mRNA or inactivated), could be efficient in improving the production of the neutralizing antibodies against the omicron variant infection, so offering effective protection from symptomatic infection or severe illness (26, 29–31). Notably, this neutralization response and vaccine effectiveness wane over time. Here our results came in line with those facts, showing that more than half proportion of patients with none or incomplete vaccination generated no antibody response. At the same time, among all patients infected by the omicron variant of SARS-CoV-2, antibody production increased as the dosing times of vaccines added.
Upon viral invasion, only a small subset of antibodies produced by B cells in the host is able to neutralize, while the majority of non-neutralizing antibodies as generated, albeit they do not counteract the viral infectivity, initiates the opsonophagocytic process by one region binding specifically to the viral particles via opsonization and the other region (Fc region) activating the Fc-receptor-mediated endocytosis of viral particles by phagocytes, such as natural killer cells, neutrophils, monocytes and macrophages (32). Since the non-neutralizing antibodies per se cannot nullify the viral infectivity, this antibody-dependent enhancement might be a double-bladed sword, mitigating or worsening the viral infection (32). Nevertheless, for a genetically labile RNA virus, such as influenza virus or human immunodeficiency virus (HIV), the non-neutralizing antibodies have been proven to contribute significantly to efficient viral clearance (33, 34). So far, those functional non-neutralizing antibody responses have been demonstrated to render protection against SARS-CoV-2 infection in its wild-type, alpha, beta, epsilon, and gamma form (35–37). Whether this protection reoccurs against other highly mutated SARS-CoV-2 variants, including delta and omicron, awaits to be soon unraveled. Our results showed that the omicron variant infection resulted in a substantial proportion of patients with signs of leukocytosis, neutrophilia, lymphocytopenia, monocytosis and coagulopathy, while leaving the levels and the major functional indices of RBCs and platelets minimally harmed. This corroborates the active interaction between the cell immunity and the omicron variant.
Beside the antibody-mediated immunity, the cell-mediated immunity induced by infection or vaccination has shown largely preserved T cell responses to the omicron variant (38–40). It has been hypothesized that memory CD4+ T cells mainly target the conserved motif in the spike protein that harbors a minority of mutations, where CD8+ T cells are frequently directed to the mutation site in the SARS-CoV-2 (38, 39). When encountering the omicron variant of SARS-CoV-2, memory CD4+ T cell responses wakened by previous infection or vaccination remain intact (41). On the other hand, only one low-prevalence epitope in the spike protein has been found to undertake single amino acid change (T95I) in the omicron variant, where CD8+ T cell recognition can be minimally compromised (42). Therefore, despite the fact that the omicron variant owns the highest mutations among the five VOCs, its T cell escape is minimal and comparable to other VOCs. On top of that, a booster vaccine effectively enhances T-cell responses (41, 43).
Due to key mutations in the spike protein of SARS-CoV-2 omicron variant, especially Q493R and N501Y, it binds to human and mouse ACE2 with much higher affinity than the wild type or other VOCs (44). However, viral entry into the host cells via ACE2 has to be primed and facilitated by transmembrane serine protease 2 (TMPRSS2), which is efficiently utilized by the wild type or the alpha, beta and delta variants, but not the omicron variant, possibly owing to the critical mutations at S1/S2 region and the reduced cleavage (45, 46). Thus, the omicron variant may enter the host via a differing endocytotic pathway from the wild type and other variants. As a result, the replication of the omicron variant is significantly attenuated, leading to mitigated pro-inflammatory responses, diminished lung pathology and improved survival rate in animal models (45, 47). Concurrently, the independence of TMPRSS2 renders the omicron variant a broader spectrum of cellular tropism to infect ACE2+ cells which are more abundant in human bronchi than lungs (48). This explains why the omicron variant prefers to accumulate in upper airways over deep lungs, causing alleviated intrinsic severity once patients are infected (49). Our results became consistent with those findings, where nearly half proportion of patients went through asymptomatic manifestations and lung infiltration did not induce severe pathological changes in most patients (e.g., consolidation, crazy paving pattern).
Here our study had limitations. First, our patient number was small. This further made the patient number in different subgroups even smaller. Given the recent escalation of the omicron outbreak and the increasing portion of patients with no symptom or no need for hospitalization, clinical data became less available. Second, there was no severe or deceased patient in our study, so we could not have access to analyze the possible risk factors associated with severity or mortality of COVID-19 infection by the omicron variant. Similarly, our study contained patients with a median age of 33.0 (IQR: 24.0–45.5). Thus, this study might not elucidate much of vaccine effectiveness and viremic effect in the aged population (>60 years old). Third, this study lacked a continuous monitoring of COVID-19 patients during hospitalization and post hospital discharge. This would make more complete research on the long-term outcome of the omicron variant infection to justify its pathogenic feature and consequence.
Conclusions
In closing, we investigated the baseline characteristics of COVID-19 patients infected by the omicron variant of SARS-CoV-2 together with findings on its reduced clinical severity. Albeit the high mutation in the omicron variant may effectuate its evasion from the neutralizing antibodies, the functional non-neutralizing machinery and the effective cell-mediated immunity constitute the secure frontline defensing against the viral attack of the omicron variant. Simultaneously, the infection route and intrinsic virulence of the omicron variant greatly alter, thereby attenuating its detrimental effect on lungs. Nonetheless, booster jabs can provide the reinforced protection against COVID-19 severity and mortality, especially for those with compromised immune system.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Research Ethics Commission of the Fifth People's Hospital of Suzhou (TFPHS, the Affiliated Infectious Diseases Hospital of Soochow University), China. Written informed consent from the participants or their legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author Contributions
JiaZ and ZT conceived the idea and designed the study. JiaZ, NC, DZ, ZH, and ZT contributed to the data processing and table/figure preparation. NC, JinZ, and ZT contributed to the statistical analysis. All authors contributed to the manuscript writing and approved the manuscript submission.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank Jiangsu University and Soochow University for the financial support.
References
1. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Biomed. (2020) 91:157–60. doi: 10.23750/abm.v91i1.9397
2. Wu F, Zhao S, Yu B, Chen YM, Wang W, Song ZG, et al. A new coronavirus associated with human respiratory disease in China. Nature. (2020) 579:265–9. doi: 10.1038/s41586-020-2008-3
3. Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. (2020) 579:270–3.
4. Hirabara SM, Serdan TDA, Gorjao R, Masi LN, Pithon-Curi TC, Covas DT, et al. SARS-COV-2 variants: differences and potential of immune evasion. Front Cell Infect Microbiol. (2022) 11:781429. doi: 10.3389/fcimb.2021.781429
5. WH Organization. COVID-19 Weekly Epidemiological Update, 84 edition (2022) (accessed March 22, 2022).
6. del Rio C, Omer SB, Malani PN. Winter of omicron—the evolving COVID-19 pandemic. JAMA. (2022) 327:319–20. doi: 10.1001/jama.2021.24315
7. Zhang D, Wu S, Ren Z, Sun Y, Dou X, Feng Z, et al. A local cluster of omicron variant COVID-19 likely caused by internationally mailed document—Beijing municipality, China, January 2022. China CDC Wkly. (2022) 4:302–4. doi: 10.46234/ccdcw2022.031
8. Ruan F, Zhang X, Xiao S, Ni X, Yin X, Ye Z, et al. An outbreak of the COVID-19 omicron variant—Zhuhai City, Guangdong Province, China, January 13, 2022. China CDC Wkly. (2022) 4:41–3. doi: 10.46234/ccdcw2022.032
9. GuoQ, Ruhan A, Liang L, Zhao X, Deng A, Hu Y, et al. an imported case of ba. 2 lineage of omicron variant COVID-19—Guangdong Province, China, December 28, 2021. China CDC Wkly. (2022) 4:98–9. doi: 10.46234/ccdcw2022.001
10. Maslo C, Friedland R, Toubkin M, Laubscher A, Akaloo T, Kama B. Characteristics and outcomes of hospitalized patients in South Africa during the COVID-19 omicron wave compared with previous waves. JAMA. (2022) 327:583–4. doi: 10.1001/jama.2021.24868
11. Wolter N, Jassat W, Walaza S, Welch R, Moultrie H, Groome M, et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: a data linkage study. Lancet. (2022) 399:437–46. doi: 10.1016/S0140-6736(22)00017-4
12. Tian D, Sun Y, Xu H, Ye Q. The emergence and epidemic characteristics of the highly mutated SARS-CoV-2 omicron variant. J Med Virol. (2022) 94:2376–83. doi: 10.1002/jmv.27643
13. Rössler A, Riepler L, Bante D, von Laer D, Kimpel J. SARS-CoV-2 omicron variant neutralization in serum from vaccinated and convalescent persons. N Eng J Med. (2022) 386:698–700. doi: 10.1056/NEJMc2119236
14. Zhang J, Hu J, Huang X, Fu S, Ding D, Tao Z. Association between red blood cell distribution width and COVID-19 severity in delta variant SARS-CoV-2 infection. Front Med. (2022) 9:837411. doi: 10.3389/fmed.2022.837411
15. Hu Z, Huang X, Zhang J, Fu S, Ding D, Tao Z. Differences in clinical characteristics between delta variant and wild-type SARS-CoV-2 infected patients. Front Med. (2021) 8:792135. doi: 10.3389/fmed.2021.792135
16. Zhang J, Huang X, Ding D, Tao Z. Platelet-driven coagulopathy in COVID-19 patients: in comparison to seasonal influenza cases. Exp Hematol Oncol. (2021) 10:34. doi: 10.1186/s40164-021-00228-z
17. Li M, Liu Q, Wu D, Tang L, Wang X, Yan T, et al. Association of COVID-19 vaccination and clinical severity of patients infected with delta or omicron variants—China, May 21, 2021-February 28, 2022. China CDC Wkly. (2022) 4:293–7. doi: 10.46234/ccdcw2022.074
18. Madhi SA, Kwatra G, Myers JE, Jassat W, Dhar N, Mukendi CK, et al. Population immunity and Covid-19 severity with omicron variant in South Africa. N Eng J Med. (2022) 386:1314–26. doi: 10.1101/2021.12.20.21268096
19. Modes ME, Directo MP, Melgar M, Johnson LR, Yang H, Chaudhary P, et al. Clinical characteristics and outcomes among adults hospitalized with laboratory-confirmed SARS-CoV-2 infection during periods of B. 1.617. 2 (Delta) and B. 1.1. 529 (Omicron) variant predominance—one hospital, California, July 15-September 23, 2021, and December 21, 2021-January 27, 2022. MMWR Morb Mortal Wkly Rep. (2022) 71:217–23. doi: 10.15585/mmwr.mm7106e2
20. Houhamdi L, Gautret P, Hoang VT, Fournier P-E, Colson P, Raoult D. Characteristics of the first 1119 SARS-CoV-2 omicron variant cases, in Marseille, France, November–December 2021. J Med Virol. (2022) 94:2290–5. doi: 10.1002/jmv.27613
21. Kim MK, Lee B, Choi YY, Um J, Lee KS, Sung HK, et al. Clinical characteristics of 40 patients infected with the SARS-CoV-2 omicron variant in Korea. J Korean Med Sci. (2022) 37:e31. doi: 10.3346/jkms.2022.37.e31
22. Liu Y, Rocklöv J. The effective reproduction number for the omicron SARS-CoV-2 variant of concern is several times higher than Delta. J Travel Med. (2022). doi: 10.1093/jtm/taac037. [Epub ahead of print].
23. Nishiura H, Ito K, Anzai A, Kobayashi T, Piantham C, Rodríguez-Morales AJ. Relative reproduction number of SARS-CoV-2 omicron (B.1.1.529) compared with delta variant in South Africa. J Clin Med. (2022) 11:30. doi: 10.3390/jcm11010030
24. Ingraham NE, Ingbar DH. The omicron variant of SARS-CoV-2: Understanding the known and living with unknowns. Clin Transl Med. (2021) 11:e685. doi: 10.1002/ctm2.685
25. Saxena SK, Kumar S, Ansari S, Paweska JT, Maurya VK, Tripathi AK, et al. Characterization of the novel SARS-CoV-2 Omicron (B.1.1.529) variant of concern and its global perspective. J Med Virol. (2022) 94:1738–44. doi: 10.1002/jmv.27524
26. Ma C, Chen X, Mei F, Xiong Q, Liu Q, Dong L, et al. Drastic decline in sera neutralization against SARS-CoV-2 Omicron variant in Wuhan COVID-19 convalescents. Emerg Microbes Infect. (2022) 11:567–72. doi: 10.1080/22221751.2022.2031311
27. Rössler A, Knabl L, von Laer D, Kimpel J. Neutralization profile after recovery from SARS-CoV-2 Omicron infection. N Eng J Med. (2022). doi: 10.1056/NEJMc2201607. [Epub ahead of print].
28. Dejnirattisai W, Shaw RH, Supasa P, Liu C, Stuart ASV, Pollard AJ, et al. Reduced neutralisation of SARS-CoV-2 omicron B.1.1.529 variant by post-immunisation serum. Lancet. (2022) 399:234–6. doi: 10.1016/S0140-6736(21)02844-0
29. Yu J, Collier A-rY, Rowe M, Mardas F, Ventura JD, Wan H, et al. Neutralization of the SARS-CoV-2 Omicron BA.1 and BA.2 variants. N Eng J Med. (2022) 386:1579–80. doi: 10.1056/NEJMc2201849
30. Yu X, Qi X, Cao Y, Li P, Lu L, Wang P, et al. Three doses of an inactivation-based COVID-19 vaccine induces cross-neutralizing immunity against the SARS CoV-2 omicron variant. Emerg Microbes Infect. (2022) 11:749–52. doi: 10.1080/22221751.2022.2044271
31. Accorsi EK, Britton A, Fleming-Dutra KE, Smith ZR, Shang N, Derado G, et al. Association between 3 doses of mRNA COVID-19 vaccine and symptomatic infection caused by the SARS-CoV-2 omicron and delta variants. JAMA. (2022) 327:639–51. doi: 10.1001/jama.2022.0470
32. Bournazos S, Gupta A, Ravetch JV. The role of IgG Fc receptors in antibody-dependent enhancement. Nat Rev Immunol. (2020) 20:633–43. doi: 10.1038/s41577-020-00410-0
33. Fujisawa H. Neutrophils play an essential role in cooperation with antibody in both protection against and recovery from pulmonary infection with influenza virus in mice. J Virol. (2008) 82:2772–83. doi: 10.1128/JVI.01210-07
34. Huber VC, Lynch JM, Bucher DJ, Le J, Metzger DW. Fc receptor-mediated phagocytosis makes a significant contribution to clearance of influenza virus infections. J Immunol. (2001) 166:7381–8. doi: 10.4049/jimmunol.166.12.7381
35. Bahnan W, Wrighton S, Sundwall M, Bläckberg A, Larsson O, Höglund U, et al. Spike-dependent opsonization indicates both dose-dependent inhibition of phagocytosis and that non-neutralizing antibodies can confer protection to SARS-CoV-2. Front Immunol. (2022) 12:808932. doi: 10.3389/fimmu.2021.808932
36. Gorman MJ, Patel N, Guebre-Xabier M, Zhu AL, Atyeo C, Pullen KM, et al. Fab and Fc contribute to maximal protection against SARS-CoV-2 following NVX-CoV2373 subunit vaccine with Matrix-M vaccination. Cell Rep Med. (2021) 2:100405. doi: 10.1016/j.xcrm.2021.100405
37. Alter G, Yu J, Liu J, Chandrashekar A, Borducchi EN, Tostanoski LH, et al. Immunogenicity of Ad26.COV2.S vaccine against SARS-CoV-2 variants in humans. Nature. (2021) 596:268–72. doi: 10.1038/s41586-021-03681-2
38. Keeton R, Tincho MB, Ngomti A, Baguma R, Benede N, Suzuki A, et al. T cell responses to SARS-CoV-2 spike cross-recognize Omicron. Nature. (2022) 603:488–92. doi: 10.1038/s41586-022-04460-3
39. Mazzoni A, Vanni A, Spinicci M, Capone M, Lamacchia G, Salvati L, et al. SARS-CoV-2 spike-specific CD4+ T cell response is conserved against variants of concern, including omicron. Front Immunol. (2022) 13:801431. doi: 10.3389/fimmu.2022.801431
40. GeurtsvanKessel CH, Geers D, Schmitz KS, Mykytyn AZ, Lamers MM, Bogers S, et al. Divergent SARS-CoV-2 Omicron–reactive T and B cell responses in COVID-19 vaccine recipients. Sci Immunol. (2022) 7:eabo2202. doi: 10.1126/sciimmunol.abo2202
41. Naranbhai V, Nathan A, Kaseke C, Berrios C, Khatri A, Choi S, et al. T cell reactivity to the SARS-CoV-2 Omicron variant is preserved in most but not all individuals. Cell. (2022) 185:1041–51. doi: 10.1016/j.cell.2022.01.029
42. Redd AD, Nardin A, Kared H., Bloch E, Abel B, Pekosz A. al. Minimal crossover between mutations associated with omicron variant of SARS-CoV-2 and CD8+ T-Cell epitopes identified in COVID-19 convalescent individuals. mBio (2022) 13:e03617-21. doi: 10.1128/mbio.03617-21
43. Madelon N, Heikkilä N, Sabater Royo I, Fontannaz P, Breville G, Lauper K, et al. Omicron-specific cytotoxic T-cell responses after a third dose of mRNA COVID-19 vaccine among patients with multiple sclerosis treated with ocrelizumab. JAMA Neurol. (2022) 79:399–404. doi: 10.1101/2021.12.20.21268128
44. Cameroni E, Bowen JE, Rosen LE, Saliba C, Zepeda SK, Culap K, et al. Broadly neutralizing antibodies overcome SARS-CoV-2 omicron antigenic shift. Nature. (2022) 602:664–70. doi: 10.1038/s41586-021-04386-2
45. Shuai H, Chan JF-W, Hu B, Chai Y, Yuen TT-T, Yin F, et al. Attenuated replication and pathogenicity of SARS-CoV-2 B.1.1.529 Omicron. Nature. (2022) 603:693–9. doi: 10.1038/s41586-022-04442-5
46. Zhang J, Ding D, Huang X, Zhang J, Chen D, Fu P, et al. Differentiation of COVID-19 from seasonal influenza: a multicenter comparative study. J Med Virol. (2021) 93:1512-9. doi: 10.1002/jmv.26469
47. Suzuki R, Yamasoba D, Kimura I, Wang L, Kishimoto M, Ito J, et al. Attenuated fusogenicity and pathogenicity of SARS-CoV-2 Omicron variant. Nature. (2022) 603:700–5. doi: 10.1038/s41586-022-04462-1
48. Hui KPY, Ho JCW, Cheung M-c, Ng K-c, Ching RHH, Lai K-l, et al. SARS-CoV-2 Omicron variant replication in human bronchus and lung ex vivo. Nature. (2022) 603:715–20. doi: 10.1038/s41586-022-04479-6
49. Nyberg T, Ferguson NM, Nash SG, Webster HH, Flaxman S, Andrews N, et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: a cohort study. Lancet. (2022) 399:1303–12. doi: 10.1016/S0140-6736(22)00462-7
Keywords: SARS-CoV-2, omicron variant, COVID-19, pathogenicity, vaccination
Citation: Zhang J, Chen N, Zhao D, Zhang J, Hu Z and Tao Z (2022) Clinical Characteristics of COVID-19 Patients Infected by the Omicron Variant of SARS-CoV-2. Front. Med. 9:912367. doi: 10.3389/fmed.2022.912367
Received: 04 April 2022; Accepted: 19 April 2022;
Published: 09 May 2022.
Edited by:
Pragya Dhruv Yadav, ICMR-National Institute of Virology, IndiaReviewed by:
Safdar Ali, Aliah University, IndiaShilpi Jain, Centers for Disease Control and Prevention (CDC), United States
Copyright © 2022 Zhang, Chen, Zhao, Zhang, Hu and Tao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhimin Tao, anN1dGFvJiN4MDAwNDA7dWpzLmVkdS5jbg==
†These authors have contributed equally to this work