 Huan Wang1†
Huan Wang1† Dengpiao Xie
Dengpiao Xie
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 06 July 2022
Sec. Nephrology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.904299
This article is part of the Research Topic Integrated Management of Chronic Kidney Disease Patients View all 24 articles
Background and Aim: Vascular function is associated with an increased risk of cardiovascular events in patients with chronic kidney disease (CKD). Whether exercise improves vascular function in such patients remains controversial. This study aimed to conduct a meta-analysis on the effect of exercise training on the vascular function of patients with CKD.
Methods: Embase, the Cochrane Central Register of Controlled Trials, and Medline were searched from inception until November 15, 2021. The terms exercise, CKD, dialysis, kidney transplant, and randomized controlled trial (RCT) were searched alone or in combination. RCTs were included when studies compared exercise with active control, usual care, or no intervention, and the studies reported vascular function on patients with CKD.
Results: This meta-analysis included 18 RCTs with 817 patients. Exercise training was significantly associated with decreased pulse wave velocity weighted mean difference (WMD), −0.56; 95% confidence interval (CI), −1.02 to −0.09, P = 0.02 and augmentation index (WMD, −3.26; 95% CI, −5.46 to −1.05, P = 0.004). It was also significantly associated with improved peak VO2 (WMD, 2.64; 95% CI, 1.94–3.35, P < 0.00001), general health (WMD, 7.03; 95% CI, 0.65–13.42, P = 0.03), and vitality (WMD, 9.1; 95% CI, 2.50–15.69, P = 0.007).
Conclusions: The meta-analysis suggested that exercise training improved vascular function in patients with CKD. An exercise program should be considered as one of the management strategies for vascular dysfunction in patients with CKD. Further studies are needed to demonstrate that exercise training improves cardiovascular diseases in patients with CKD.
The increasing number of patients with chronic kidney disease (CKD) poses a challenge to health care. More than 15% of American adults or 37 million people were estimated to have CKD in 2021 based on data from the Centers for Disease Control and Prevention. Patients with CKD are twice more likely to develop cardiovascular disease (CVD). CVD remains the leading cause of mortality in patients with CKD (1). The increased arterial stiffness is one of the major factors contributing to CVD in such patients. The mechanisms that lead to the arterial disease in CKD include endothelial dysfunction, disorders of nitric oxide metabolism, vascular calcification, and elevation of the levels of pro-inflammatory cytokines (2–4). The complicated mechanisms explain why the treatment focusing on a single risk factor cannot achieve satisfactory outcomes. Previous studies showed that aortic stiffness and carotid stiffness are strongly associated with CVD in patients with CKD (5, 6). Therefore, improving vascular function might bring benefits to these patients.
The safety of exercise training is questioned in patients with CKD because renal perfusion is reduced and proteinuria is more severe in some cases during exercise (7). However, studies also proved the benefits of exercise in patients with CKD. The studies demonstrated that voluntary exercise was an effective therapy to improve endothelial function in rats with CKD (8, 9). In addition, exercise training was shown to improve endothelial function, physical function, inflammatory status, hypertension, nitric oxide availability, and lipid metabolism disorders (10, 11).
Some studies were conducted to assess the effect of exercise on arterial stiffness in patients with CKD. However, most of the studies were non-randomized controlled trials (RCTs), the sample sizes were small, and the results were inconsistent. Therefore, the conclusion was not convincing. Given the lack of high-quality evidence on the effects of exercise on the vascular function of patients with CKD, we conducted a meta-analysis of randomized trials to assess the effect of exercise on the vascular function of such patients.
The meta-analysis was performed and reported following Preferred Reporting Items for Systematic Reviews and Meta-analysis (12). The study protocol was registered in the International Prospective Register of Systematic Reviews; registration number: CRD42021283470. Studies were searched in the following databases; Medline, Cochrane Trials, and Embase. The search deadline was November, 12, 2021. The details of the search strategy and terms are presented in Supplementary Table 1. In addition, clinical trial registries and references of similar clinical studies, as well as review articles or systemic reviews on a similar topic, were reviewed to search for potentially relevant studies.
Two independent reviewers (H.W, and D.P.X) evaluated the titles and abstracts and screened the full-text versions of the relevant trials. Disagreements were resolved by consensus between the reviewers, and if necessary, by consulting with other reviewers. The studies were considered for inclusion if they compared exercise with active control, usual care, or no intervention, or they were randomized trials and reported the vascular function in patients with CKD. The flow diagram of study selection is outlined in Figure 1.
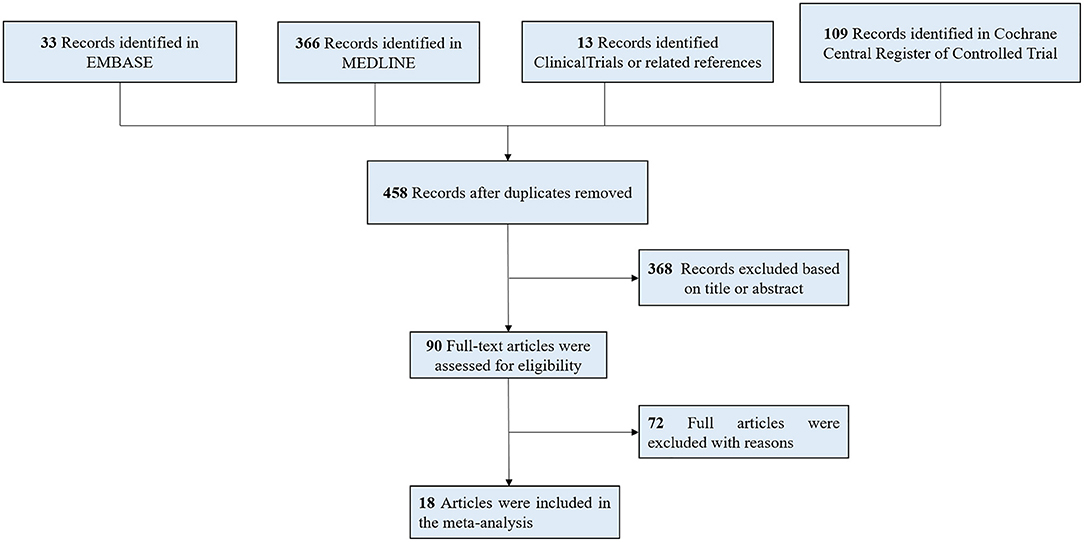
Figure 1. Flow of the search strategy and included studies.
Patients with CKD, including non-dialysis and dialysis, or patients with kidney transplants were included in the study. The outcome should include indices of vascular function, pulse wave velocity (PWV), or augmentation index. All RCTs that compared exercise with control in managing patients with CKD were also included. This review focused on exercise training. Non-exercise management, such as electrical stimulation and water-based therapy, were excluded. The exercise training included aerobic exercises (such as walking, and cycling on a treadmill, ergometer, or elliptical machine) or resistance training (such as lifting or suppressing the muscle groups). Trials were excluded if they were case reports, comments, letters, or reviews.
The data on the characteristics of methods, participants, interventions, and outcomes were extracted by two independent reviewers. The Cochrane risk-of-bias tool was used to assess the included trials. It contained the following criteria: selection bias, performance and detection bias, attrition bias, reporting bias, and other sources of bias. Two independent reviewers performed the assessment. The third author resolved the discrepancies. The corresponding authors were responsible for obtaining missing information and unpublished data.
The primary outcome was defined as the changes in vascular function, including PWV or augmentation index from baseline to the end of treatment. The changes in peak VO2, health-related quality of life (HRQoL), blood pressure, and C-reactive protein (CRP) level were regarded as the secondary outcomes. If clinical outcomes were measured more than once in a study, we selected the data reported the last time. Data reported as median, interquartile range, 95% confidence interval (CI), or standard error were converted into mean and standard deviation (SD) using the formula (13, 14). We assessed effect size by weighted mean differences (WMDs) for continuous outcomes. The CI was 95%. We assessed heterogeneity with I2 statistics. An I2 value <25%, between 25 and 50%, and >75% indicated a low degree of heterogeneity, a moderate degree of heterogeneity, and significant heterogeneity, respectively (15). If the results were not significantly heterogeneous, a fixed-effects model was used. If the results were significantly heterogeneous, a random-effects model was used. The possibility of publication bias for the primary outcome was evaluated using the Egger test and the visual estimate of funnel plot. Sensitivity analyses were conducted by outlier identification and influence analysis using Stata 15. The subgroup analyses were performed based on the duration of the intervention. Exercise training lasting <6 months was defined as short term, while the training lasting ≥6 months was defined as long term. The data were assessed using Review Manager, version 5.3 (Oxford, UK).
We identified 521 relevant studies or abstracts by the initial search. After removing 63 duplicates and 368 studies by screening the titles and abstracts, 90 full-text studies were further reviewed in detail. Two articles were considered as the same study for the analyses (16, 17). One study was removed for combining exercise with other lifestyle interventions (18). Finally, 18 studies were included in this meta-analysis.
The summary characteristics of studies included in the meta-analysis are shown in Table 1. All studies were RCTs, enrolling 817 patients. The sample size ranged from 12 to 156 patients, mean sample size of 45 (SD 37). A total of 7 trials (19–24) and NCT03197038 included pre-dialysis patients with CKD, 10 trials included dialysis patients (25–33), and 2 trials included kidney transplant patients (17, 34). Participants received aerobic training in these trials and NCT0319703, resistance training in these trials (17), and both aerobic and resistance trainings in these trials (22, 34). Most of the trials had an exercise frequency of three to four times per week; exercise was performed daily in only one trial (23). The exercise duration varied from 10 to 65 min as can be seen in references (23) and (29), respectively, in each session; only one trial did not report the exercise duration (27). The duration of exercise management was from 2.5 months to 12 months. Two trials contributed to two comparator categories (17, 26). One trial was a cross-over study (25).
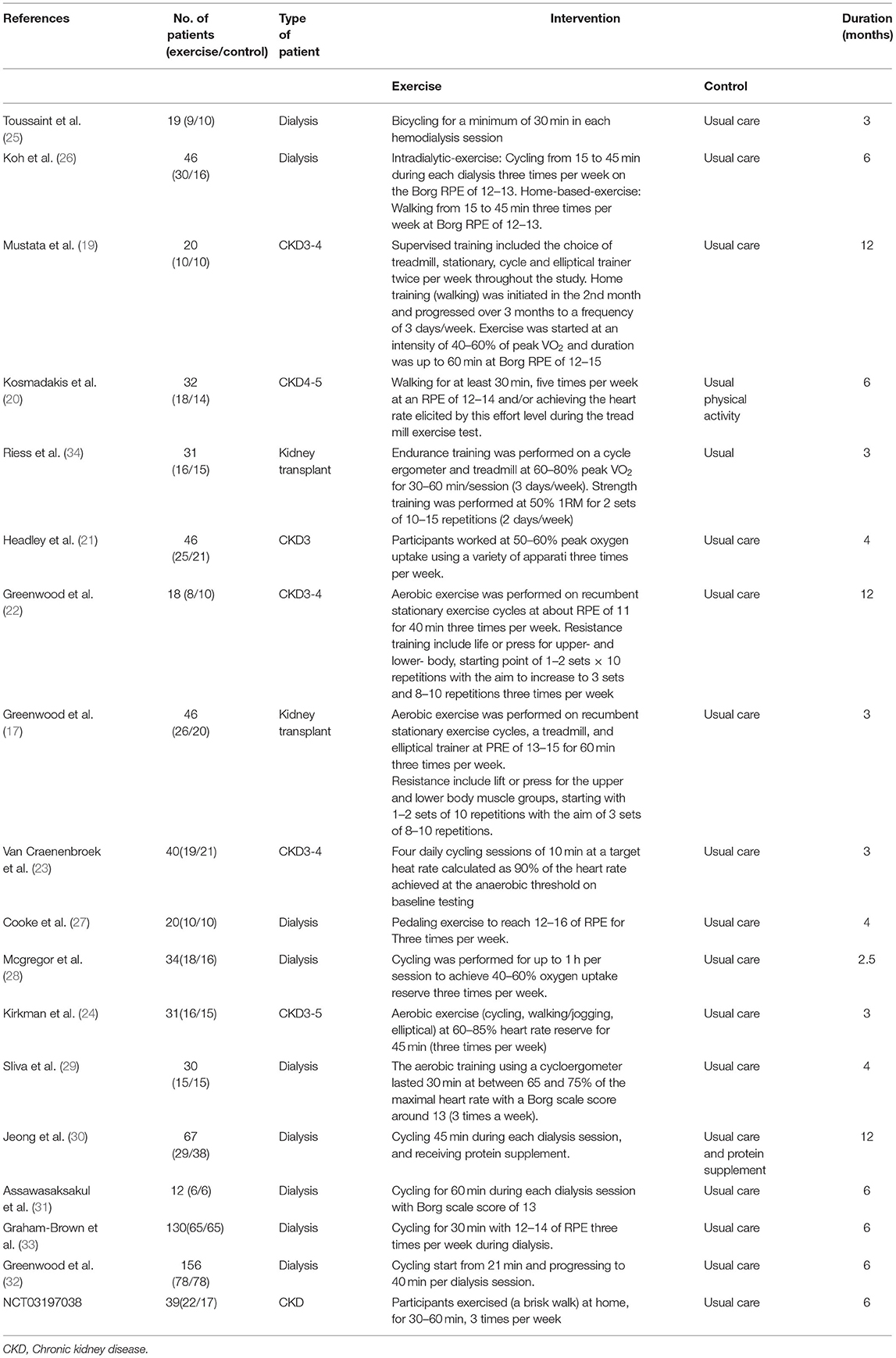
Table 1. Basic characteristics of subjects and treatments of trials.
All studies were randomized trials included in this meta-analysis. Among these studies, 12 trials (17, 19, 21–26, 28, 31, 32, 34) reported the concrete randomization methods. The performance bias was considered as high risk in all trials because it was impossible to blind the participants and researches for the exercise training. The intention-to-treat approach was employed in these trials (19, 29, 33). The risk-of-bias assessments are presented in Figure 2 in the supplement.
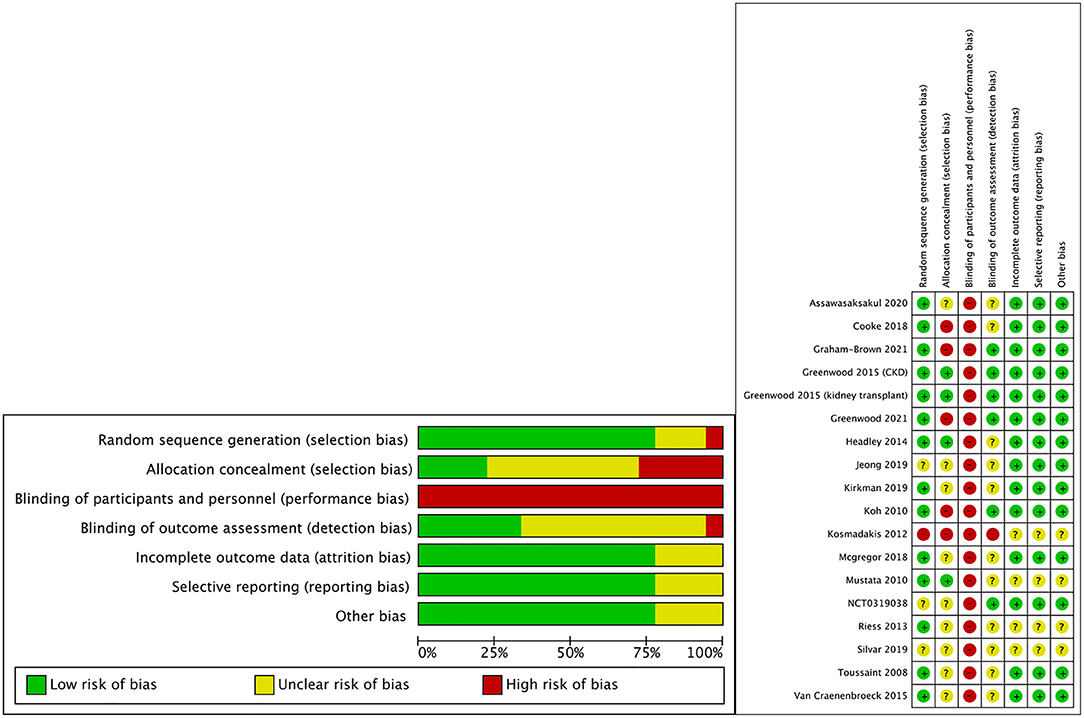
Figure 2. Risk of bias graph of included studies.
A total of 17 trials (17, 20–34) and NCT03197038 were included in the meta-analysis for PWV between the two groups. The result showed that exercise training significantly decreased PWV in patients with CKD (WMD, −0.56; 95% CI, −1.02 to −0.09, P = 0.02, without significant heterogeneity; P = 0.005, I2 = 52%, Figure 3).
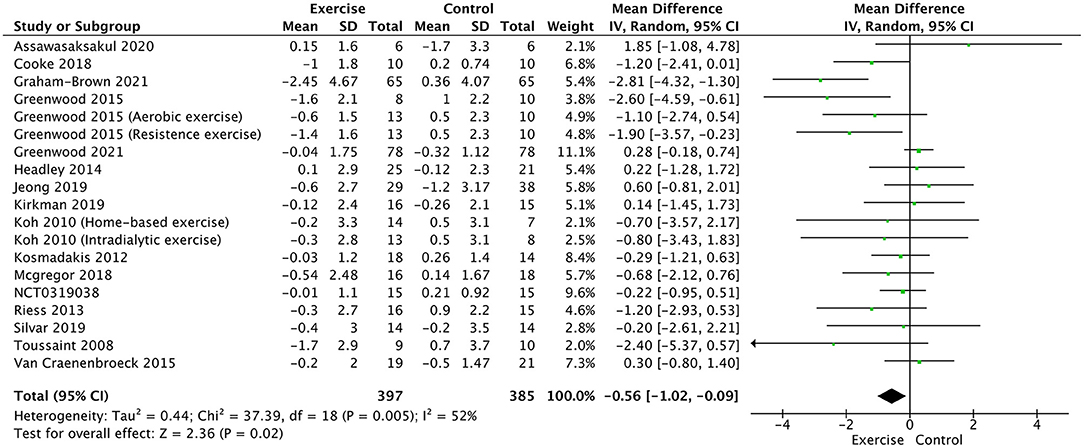
Figure 3. Forest plot of exercise training on PWV.
The augmentation index was measured in 11 trials (19–21, 23–27, 29, 30) and NCT03197038. The pooled result showed that exercise training significantly decreased the augmentation index (WMD, −3.26; 95% CI, −5.46 to −1.05, P = 0.004; without heterogeneity: P = 0.90, I2 = 0%, Figure 4).
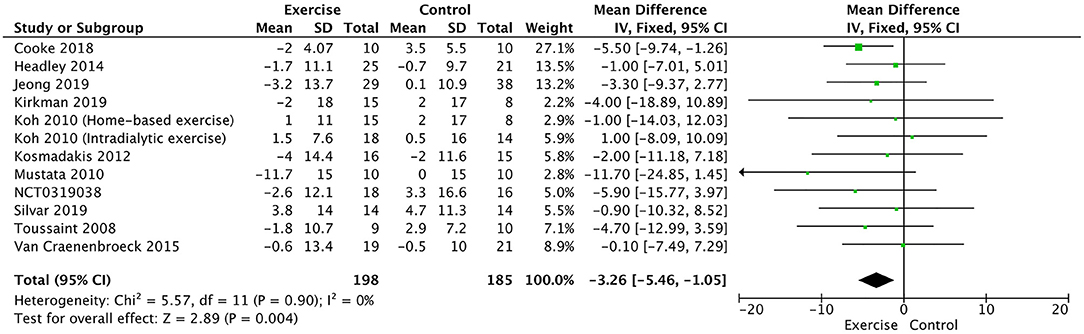
Figure 4. Forest plot of exercise training on augmentation index.
Peak VO2 was compared in 10 trials (17, 19, 21–24, 28, 31, 32, 34). It significantly increased in the exercise training group compared with the usual control group (WMD, 2.64; 95% CI, 1.94–3.35, P < 0.00001; without heterogeneity: P = 0.24, I2 = 22%, Figure 5).
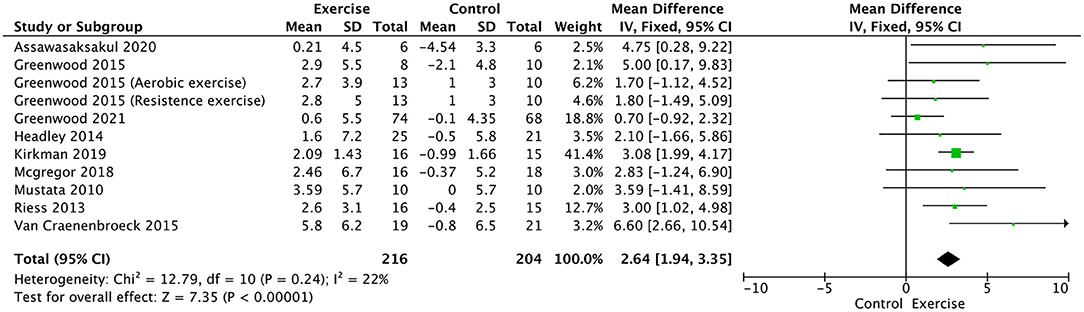
Figure 5. Forest plot of exercise training on peak VO2.
The blood pressure was compared in 11 trials (17, 21–28, 30, 33). the exercise training had no effect on either systolic blood pressure (WMD, −0.70; 95% CI, −4.28 to 2.87, P = 0.70; without heterogeneity: P = 0.87, I2 = 0%, Supplementary Figure 1) or diastolic blood pressure (WMD, −0.55; 95% CI, −2.83 to 1.74, P = 0.64; without heterogeneity: P = 0.84, I2 = 0%, Supplementary Figure 2).
CRP was compared in seven trials (17, 21, 23, 25, 29–31). The exercise training had no effect on the levels of CRP (WMD, −0.09; 95% CI, −0.26 to 0.09, P = 0.33; without heterogeneity: P = 0.57, I2 = 0%, Supplementary Figure 3).
HRQoL was compared in four trials (19, 21, 23, 26), including vitality, general health, social function pain, and mental health. No significant difference in mental health was found between the training and control groups (WMD, 1.09; 95% CI, −4.21 to 6.4, P = 0.69; without heterogeneity: P = 0.31, I2 = 16%, Supplementary Figure 4), social function (WMD, 4.08; 95% CI, −2.52 to 10.69, P = 0.23; without heterogeneity: P = 0.88, I2 = 0%, Supplementary Figure 5). However, exercising training improved general health (WMD, 7.03; 95% CI, 0.65–13.42, P = 0.03; without heterogeneity: P = 0.75, I2 = 0%, Supplementary Figure 6) and vitality (WMD, 9.1; 95% CI, 2.50–15.69, P = 0.007; without heterogeneity: P = 0.91, I2 = 0%, Supplementary Figure 7).
The subgroup analysis revealed that PWV was significantly lower in patients with short-term exercise training and without heterogeneity (Supplementary Figure 8). However, no difference was observed between the long-term exercise training group and the control group in patients with significant heterogeneity (Supplementary Figure 8).
Among the studies, nine trials (17, 19, 22, 24–28, 31, 34) reported no adverse events with exercise. Two trials (31, 32) reported no difference in adverse events between exercise training groups and control group. One trial (33) reported that the exercise training groups had more adverse events than the control group; the adverse events were judged to have no relationship with exercise. The study by Graham-Brown et al. (33) reported two deaths in each group, while Greenwood et al. (32) reported three deaths in the exercise training group and four deaths in the control group.
The sensitivity analysis was performed by leave-one-out analysis in the primary outcomes. The leave-one-out analysis showed that the pooled result and heterogeneity had no significant change in PWV (Figure 6) and augmentation index (Figure 7).
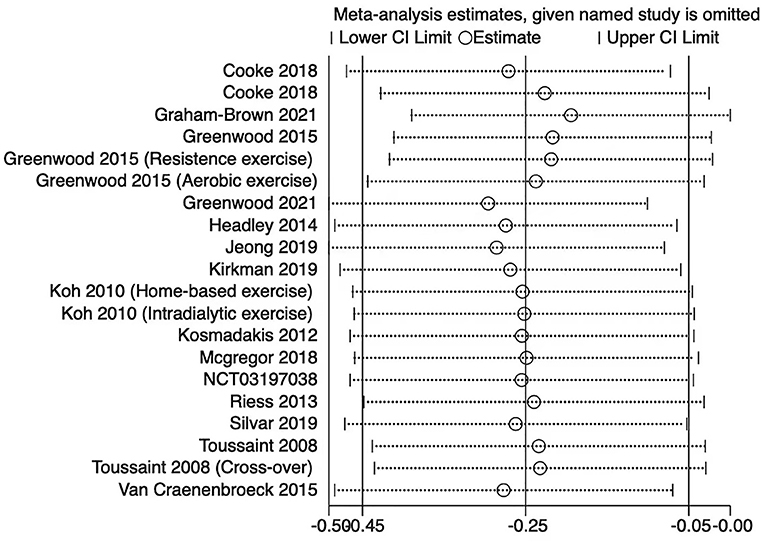
Figure 6. Leave-one-out forest plot for the PWV.
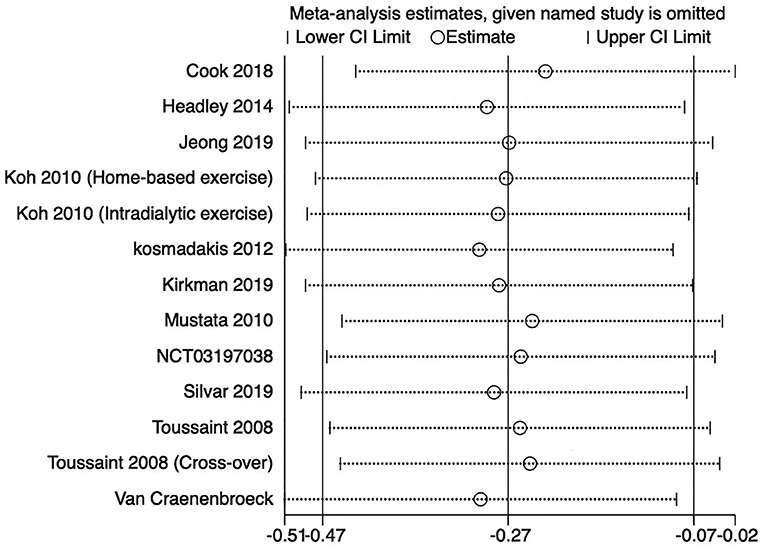
Figure 7. Leave-one-out forest plot for the augmentation index.
The funnel plot analysis showed the symmetry in Figure 8, and the Egger test (P > 0.05) did not detect the significant publication bias for the augmentation index. However, the funnel plot analysis showed some asymmetry in Figure 9, and the Egger test (P < 0.05) detected the publication bias for PWV.
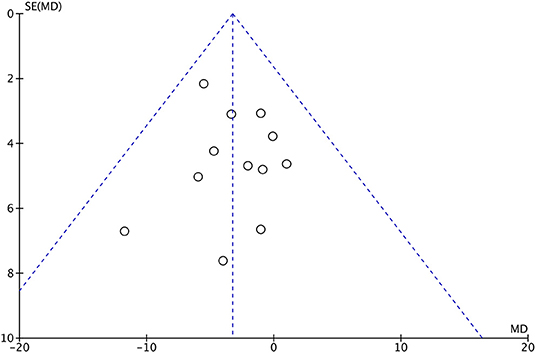
Figure 8. Funnel plot for augmentation index.
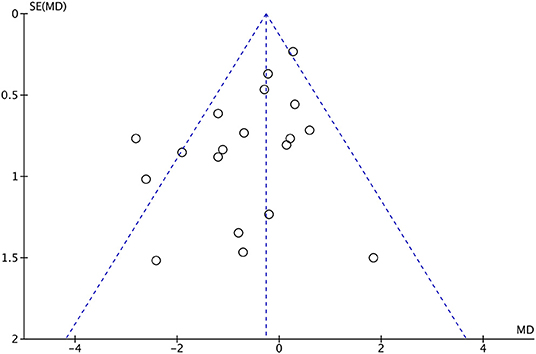
Figure 9. Funnel plot for PWV.
This meta-analysis involved 18 trials with 817 patients and showed that exercise training was significantly associated with reduced arterial stiffness evidenced by decreased PWV and augmentation index. In addition, exercise training was associated with improved peak VO2, general health, and vitality. However, no association of exercise training with improved CRP, mental health, and social function was found in this meta-analysis. Finally, this meta-analysis found no association between exercise training and adverse events.
Vascular stiffness is common in patients with CKD, and worsens as kidney function declines (35). The calcification of arteries is associated with vascular stiffness, which is an independent risk factor for CVD (36). PWV is the most widely used parameter for assessing arterial stiffness; it has become a useful method for diagnosis, risk stratification, and prognosis of cardiovascular diseases (37). It has been demonstrated to be associated with cardiovascular and all-cause mortality in patients with end-stage renal disease (ESRD) (38). Blacher et al. demonstrated an increase of 1 m/s in PWV in patients with ESRD, while the all-cause mortality increased by 1.39 times (6). The augmentation index is another useful tool to reflect the arterial stiffness and predict cardiovascular outcomes (39, 40). London et al. provided direct evidence that an increased effect of augmentation index was a predictor of all-cause and cardiovascular mortality in patients with CKD (41). Therefore, PWV and augmentation index were considered as the primary outcomes in this meta-analysis. Although PWV and augmentation index are independent predictors of cardiovascular events, they are affected by different factors. PWV might be affected by blood pressure, distensibility of the arterial wall, and peripheral vascular resistance, while augmentation index might be affected by ventricular ejection and heart rate (42, 43). This meta-analysis had similar results, showing that exercise training reduced PWV and augmentation index, which made the conclusion of this meta-analysis more convincing. In these non-RCTs, the results showed that exercise improved vascular function, as evidenced by improved flow-mediated dilation (44, 45), which were consistent with our results.
Several meta-analyses assessed the effect of exercise on patients with CKD. However, these studies focused on aerobic capacity, muscular function, or health-related quality of life. No meta-analysis study focused on the effect of exercise on arterial stiffness in patients with CKD. In 2014, a meta-analysis included 928 patients with CKD. It found that exercise improved aerobic capacity, muscular function, and health-related quality of life (46). In 2019, similar meta-analyses found that aerobic exercise improved aerobic capacity, exercise duration, and health-related quality of life (47, 48) in patients with CKD and those undergoing hemodialysis. In 2019, a meta-analysis helped reinforce our findings. The review found that exercise improved PWV; however, only two trials were included (49).
Considering limited data on patients with CKD in terms of the benefits and risks of exercise interventions, the Kidney Disease Improving Global Outcomes (KDIGO) guideline followed the guideline of the American Heart Association (AHA), in which exercise was suggested for preventing cardiovascular diseases in patients with CKD. This meta-analysis provided a rationale for the KDIGO and AHA recommendation of exercise in the management strategy for cardiovascular diseases in patients with CKD. These findings indicated that three to four times of aerobic exercise was appropriate for such patients. However, the optimal duration of exercise each time and the beginning exercise of the CKD stage to achieve maximal benefits remain unknown. Further trials are needed to examine the suitable duration and type of exercise with a personalized condition for patients with CKD who are more likely to adhere and achieve benefit.
This review had some limitations. First, we observed moderate levels of heterogeneity in PWV using I2 statistics. We further conducted subgroups analysis to reduce heterogeneity based on the duration of exercise training. The heterogeneity of PWV decreased significantly in short-term exercise training; however, the heterogeneity of PWV was even higher in long-term exercise training, which might be the main reason for the reverse outcome. We were unable to use more meaningful subgroups to reduce heterogeneity for PWV. Second, although we conducted a comprehensive search of clinical trial registries and literature to reduce the risk of missing any study, an asymmetry funnel plot and Egger test detected publication bias. The potential sources of publication bias might include selective outcome reporting, English language bias, and differences in methodological quality among trials (50). Third, we did not evaluate the important covariates, such as the association of age with the primary outcomes, due to the low number of trials to conduct a convincing meta-regression. Fourth, this meta-analysis found that exercise training reduced arterial stiffness. However, we did not compare the effects of aerobic exercise training and resistance exercise training on these patients due to the low number of trials.
The meta-analysis suggested that exercise training improved vascular function in patients with CKD. An exercise program should be considered as one of the management strategies for vascular dysfunction in patients with CKD. Further studies are needed to demonstrate that exercise training improves CVD in patients with CKD.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
HW, DX, and LZ contributed to the collection of data, bias assessment, data analysis, and manuscript writing. LW and LZ contributed to bias assessment and data extraction. LZ and DX contributed to the design of the study. All authors contributed to the article and approved the submitted version.
This work was supported by the Sichuan Administration of Traditional Chinese Medicine (Grant no. 2021MS123) and Special Project for the Development of Traditional Chinese Medicine (Grant no. CYW2022046).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.904299/full#supplementary-material
RCTs, randomized controlled trials; CKD, chronic kidney disease; PWV, pulse wave velocity; WMD, weighted mean difference; CI, confidence interval; CVD, cardiovascular disease; PRISMA, Systematic Reviews and Meta-analysis; HRQoL, health-related quality of life; CRP, C-reactive protein; SD, standard deviation; WMD, weighted mean difference.
1. Ali S, Dave N, Virani SS, Navaneethan SD. Primary and secondary prevention of cardiovascular disease in patients with chronic kidney disease. Curr Atherosclerosis Rep. (2019) 21:32. doi: 10.1007/s11883-019-0794-6
2. Cai H, Harrison DG. Endothelial dysfunction in cardiovascular diseases: the role of oxidant stress. Circulat Res. (2000) 87:840–4. doi: 10.1161/01.RES.87.10.840
3. Zoccali C, Mallamaci F, Tripepi G. Inflammatory proteins as predictors of cardiovascular disease in patients with end-stage renal disease. Nephrol Dialysis Transplant. (2004) 19:V67–72. doi: 10.1093/ndt/gfh1059
4. Vallianou NG, Mitesh S, Gkogkou A, Geladari E. Chronic kidney disease and cardiovascular disease: is there any relationship? Curr Cardiol Rev. (2019) 15:55–63. doi: 10.2174/1573403X14666180711124825
5. Blacher J, Pannier B, Guerin AP, Marchais SJ, Safar ME, London GM. Carotid arterial stiffness as a predictor of cardiovascular and all-cause mortality in end-stage renal disease. Hypertension. (1998) 32:570–4. doi: 10.1161/01.HYP.32.3.570
6. Blacher J, Guerin AP, Pannier B, Marchais SJ, Safar ME, London GM. Impact of aortic stiffness on survival in end-stage renal disease. Circulation. (1999) 99:2434–9. doi: 10.1161/01.CIR.99.18.2434
7. Headley S, Germain M, Milch C, Pescatello L, Coughlin MA, Nindl BC, et al. Exercise training improves HR responses and V?O2peak in predialysis kidney patients. Med Sci Sports Exerc. (2012) 44:2392–9. doi: 10.1249/MSS.0b013e318268c70c
8. Adams GR, Zhan CD, Haddad F, Vaziri ND. Voluntary exercise during chronic renal failure in rats. Med Sci Sports Exerc. (2005) 37:557–62. doi: 10.1249/01.MSS.0000159006.87769.67
9. Martens CR, Kuczmarski JM, Kim J, Guers JJ, Harris MB, Lennon-Edwards S, et al. Voluntary wheel running augments aortic l-arginine transport and endothelial function in rats with chronic kidney disease. Am J Physiol Renal Physiol. (2014) 307:F418–26. doi: 10.1152/ajprenal.00014.2014
10. Roberts CK, Vaziri ND, Barnard RJ. Effect of diet and exercise intervention on blood pressure, insulin, oxidative stress, and nitric oxide availability. Circulation. (2002) 106:2530–2. doi: 10.1161/01.CIR.0000040584.91836.0D
11. Khan AA, Mundra PA, Straznicky NE, Nestel PJ, Wong G, Tan R, et al. Weight loss and exercise alter the high-density lipoprotein lipidome and improve high-density lipoprotein functionality in metabolic syndrome. Arteriosclerosis Thrombosis Vasc Biol. (2018) 38:438–47. doi: 10.1161/ATVBAHA.117.310212
12. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6, e1000097. doi: 10.1371/journal.pmed.1000097
13. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. (2018) 27:1785–805. doi: 10.1177/0962280216669183
14. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. (2014) 14:135. doi: 10.1186/1471-2288-14-135
15. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
16. O'Connor EM, Koufaki P, Mercer TH, Lindup H, Nugent E, Goldsmith D, et al. Long-term pulse wave velocity outcomes with aerobic and resistance training in kidney transplant recipients - A pilot randomised controlled trial. PLoS ONE. (2017) 12:e0171063. doi: 10.1371/journal.pone.0171063
17. Greenwood SA, Koufaki P, Mercer TH, Rush R, O'Connor E, Tuffnell R, et al. Aerobic or resistance training and pulse wave velocity in kidney transplant recipients: A 12-week pilot randomized controlled trial (the exercise in renal transplant [ExeRT] Trial). Am J Kidney Dis. (2015) 66:689–98. doi: 10.1053/j.ajkd.2015.06.016
18. Howden EJ, Leano R, Petchey W, Coombes JS, Isbel NM, Marwick TH. Effects of exercise and lifestyle intervention on cardiovascular function in CKD. Clin J Am Soc Nephrol: CJASN. (2013) 8:1494–501. doi: 10.2215/CJN.10141012
19. Mustata S, Groeneveld S, Davidson W, Ford G, Kiland K, Manns B. Effects of exercise training on physical impairment, arterial stiffness and health-related quality of life in patients with chronic kidney disease: a pilot study. Int Urol Nephrol. (2011) 43:1133–41. doi: 10.1007/s11255-010-9823-7
20. Kosmadakis GC, John SG, Clapp EL, Viana JL, Smith AC, Bishop NC, et al. Benefits of regular walking exercise in advanced pre-dialysis chronic kidney disease. Nephrol Dialysis Transplant. (2012) 27:997–1004. doi: 10.1093/ndt/gfr364
21. Headley S, Germain M, Wood R, Joubert J, Milch C, Evans E, et al. Short-term aerobic exercise and vascular function in CKD stage 3: a randomized controlled trial. Am J Kidney Dis. (2014) 64:222–9. doi: 10.1053/j.ajkd.2014.02.022
22. Greenwood SA, Koufaki P, Mercer TH, MacLaughlin HL, Rush R, Lindup H, et al. Effect of exercise training on estimated GFR, vascular health, and cardiorespiratory fitness in patients with CKD: a pilot randomized controlled trial. Am J Kidney Dis. (2015) 65:425–34. doi: 10.1053/j.ajkd.2014.07.015
23. Van Craenenbroeck AH, Van Craenenbroeck EM, Van Ackeren K, Vrints CJ, Conraads VM, Verpooten GA, et al. Effect of moderate aerobic exercise training on endothelial function and arterial stiffness in CKD stages 3-4: A randomized controlled trial. Am J Kidney Dis. (2015) 66:285–96. doi: 10.1053/j.ajkd.2015.03.015
24. Kirkman DL, Ramick MG, Muth BJ, Stock JM, Pohlig RT, Townsend RR, et al. Effects of aerobic exercise on vascular function in nondialysis chronic kidney disease: a randomized controlled trial. Am J Physiol Renal Physiol. (2019) 316:F898–905. doi: 10.1152/ajprenal.00539.2018
25. Toussaint ND, Polkinghorne KR, Kerr PG. Impact of intradialytic exercise on arterial compliance and B-type natriuretic peptide levels in hemodialysis patients. Hemodial Int. (2008) 12:254–63. doi: 10.1111/j.1542-4758.2008.00262.x
26. Koh KP, Fassett RG, Sharman JE, Coombes JS, Williams AD. Effect of intradialytic versus home-based aerobic exercise training on physical function and vascular parameters in hemodialysis patients: a randomized pilot study. Am J Kidney Dis. (2010) 55:88–99. doi: 10.1053/j.ajkd.2009.09.025
27. Cooke AB, Ta V, Iqbal S, Gomez YH, Mavrakanas T, Barré P, et al. The impact of intradialytic pedaling exercise on arterial stiffness: a pilot randomized controlled trial in a hemodialysis population. Am J Hyperten. (2018) 31:458–66. doi: 10.1093/ajh/hpx191
28. McGregor G, Ennis S, Powell R, Hamborg T, Raymond NT, Owen W, et al. Feasibility and effects of intra-dialytic low-frequency electrical muscle stimulation and cycle training: A pilot randomized controlled trial. PLoS ONE. (2018) 13:e0200354. doi: 10.1371/journal.pone.0200354
29. Oliveira ESVR, Stringuetta Belik F, Hueb JC, de Souza Gonçalves R, Costa Teixeira Caramori J, Perez Vogt B, et al. Aerobic exercise training and nontraditional cardiovascular risk factors in hemodialysis patients: results from a prospective randomized trial. Cardiorenal Med. (2019) 9:391–9. doi: 10.1159/000501589
30. Jeong JH, Biruete A, Tomayko EJ, Wu PT, Fitschen P, Chung HR, et al. Results from the randomized controlled IHOPE trial suggest no effects of oral protein supplementation and exercise training on physical function in hemodialysis patients. Kidney Int. (2019) 96:777–86. doi: 10.1016/j.kint.2019.03.018
31. Assawasaksakul N, Sirichana W, Joosri W, Kulaputana O, Eksakulkla S, Ketanun C, et al. Effects of intradialytic cycling exercise on daily physical activity, physical fitness, body composition, and clinical parameters in high-volume online hemodiafiltration patients: a pilot randomized-controlled trial. Int Urol Nephrol. (2021) 53:359–71. doi: 10.1007/s11255-020-02677-7
32. Greenwood SA, Koufaki P. Exercise programme to improve quality of life for patients with end-stage kidney disease receiving haemodialysis: the PEDAL RCT. Health Technol Assess. (2021) 25:1–52. doi: 10.3310/hta25400
33. Graham-Brown MPM, March DS, Young R, Highton PJ, Young HML, Churchward DR, et al. A randomized controlled trial to investigate the effects of intra-dialytic cycling on left ventricular mass. Kidney Int. (2021) 99:1478–86. doi: 10.1016/j.kint.2021.02.027
34. Riess KJ, Haykowsky M, Lawrance R, Tomczak CR, Welsh R, Lewanczuk R, et al. Exercise training improves aerobic capacity, muscle strength, and quality of life in renal transplant recipients. Appl Physiol Nutrit Metab. (2014) 39:566–71. doi: 10.1139/apnm-2013-0449
35. Temmar M, Liabeuf S, Renard C, Czernichow S, Esper NE, Shahapuni I, et al. Pulse wave velocity and vascular calcification at different stages of chronic kidney disease. J Hyperten. (2010) 28:163–9. doi: 10.1097/HJH.0b013e328331b81e
36. Ben-Shlomo Y, Spears M, Boustred C, May M, Anderson SG, Benjamin EJ, et al. Aortic pulse wave velocity improves cardiovascular event prediction: an individual participant meta-analysis of prospective observational data from 17,635 subjects. J Am College Cardiol. (2014) 63:636–46. doi: 10.1016/j.jacc.2013.09.063
37. Kim HL, Kim SH. Pulse wave velocity in atherosclerosis. Front Cardiovasc Med. (2019) 6:41. doi: 10.3389/fcvm.2019.00041
38. Blacher J, Safar ME, Guerin AP, Pannier B, Marchais SJ, London GM. Aortic pulse wave velocity index and mortality in end-stage renal disease. Kidney Int. (2003) 63:1852–60. doi: 10.1046/j.1523-1755.2003.00932.x
39. Vyas M, Izzo JL Jr, Lacourcière Y, Arnold JM, Dunlap ME, et al. Augmentation index and central aortic stiffness in middle-aged to elderly individuals. Am J Hyperten. (2007) 20:642–7. doi: 10.1016/j.amjhyper.2007.01.008
40. Nichols WW, Singh BM. Augmentation index as a measure of peripheral vascular disease state. Curr Opin Cardiol. (2002) 17:543–51. doi: 10.1097/00001573-200209000-00016
41. London GM, Blacher J, Pannier B, Guérin AP, Marchais SJ, Safar ME. Arterial wave reflections and survival in end-stage renal failure. Hypertension. (2001) 38:434–8. doi: 10.1161/01.HYP.38.3.434
42. Obara S, Hayashi S, Hazama A, Murakawa M, Katsuda S. Correlation between augmentation index and pulse wave velocity in rabbits. J Hyperten. (2009) 27:332–40. doi: 10.1097/HJH.0b013e32831ac951
43. Wilkinson IB, MacCallum H, Flint L, Cockcroft JR, Newby DE, Webb DJ. The influence of heart rate on augmentation index and central arterial pressure in humans. J Physiol. (2000) 525:263–70. doi: 10.1111/j.1469-7793.2000.t01-1-00263.x
44. Sprick JD, Mammino K, Jeong J. Aerobic exercise training improves endothelial function and attenuates blood pressure reactivity during maximal exercise in chronic kidney disease. J Appl Physiol. (2022) 132:785–93. doi: 10.1152/japplphysiol.00808.2021
45. Katulka EK, Hirt AE, Kirkman DL, Edwards DG, Witman MAH. Altered vascular function in chronic kidney disease: evidence from passive leg movement. Physiol Rep. (2019) 7:e14075. doi: 10.14814/phy2.14075
46. Heiwe S, Jacobson SH. Exercise training in adults with CKD: a systematic review and meta-analysis. Am J Kidney Dis. (2014) 64:383–93. doi: 10.1053/j.ajkd.2014.03.020
47. Pei G, Tang Y, Tan L, Tan J, Ge L, Qin W. Aerobic exercise in adults with chronic kidney disease (CKD): a meta-analysis. Int Urol Nephrol. (2019) 51:1787–95. doi: 10.1007/s11255-019-02234-x
48. Huang M, Lv A, Wang J, Xu N, Ma G, Zhai Z, et al. exercise training and outcomes in hemodialysis patients: systematic review and meta-analysis. Am J Nephrol. (2019) 50:240–54. doi: 10.1159/000502447
49. Chen G, Gao L. Effects of exercise training on cardiovascular risk factors in kidney transplant recipients: a systematic review and meta-analysis. Ren Fail. (2019) 41:408–18. doi: 10.1080/0886022X.2019.1611602
Keywords: chronic kidney disease, dialysis, exercise, vascular function, meta-analysis
Citation: Wang H, Xie D, Wu L and Zhao L (2022) Association of Exercise With Vascular Function in Patients With CKD: A Meta-Analysis of Randomized Controlled Trials. Front. Med. 9:904299. doi: 10.3389/fmed.2022.904299
Received: 25 March 2022; Accepted: 07 June 2022;
Published: 06 July 2022.
Edited by:
Li Zuo, Peking University People's Hospital, ChinaReviewed by:
Dorin Dragoş, Carol Davila University of Medicine and Pharmacy, RomaniaCopyright © 2022 Wang, Xie, Wu and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dengpiao Xie, Mjg3NjUyMjI1M0BxcS5jb20=; Liangbin Zhao, emxiMzE5Mjg4NTZAMTYzLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.