 Louise M. Allen1
Louise M. Allen1 Claire Palermo2*
Claire Palermo2*- 1Monash Centre for Professional Development and Monash Online Education, Monash University, Clayton, VIC, Australia
- 2Monash Centre for Scholarship in Health Education, Faculty of Medicine, Nursing and Health Sciences, Monash University, Clayton, VIC, Australia
Introduction/Objective: In resource poor environments, low cost methods are needed to review competency standards to ensure they remain reflective of the current health workforce. This study aims to show how document analysis can be used to inform the revision of competency frameworks and standards.
Methods: Altheide and Schneider's document analysis was modified to revise the National Competency Standards for Dietitians in Australia. This involved an eight-step process: (i) define the goal, (ii) identify documents for analysis, (iii) choose the analysis approach, (iv) engage with the documents and perform the analysis, (v) draft revisions, (vi) stakeholder engagement, (vii) final revisions, (viii) dissemination. Documents were sought through a combination of literature searches, review of document databases, and targeted document sourcing for documents relevant to contemporary dietetic practice. Framework analysis was used to analyse the data, with the thematic framework including four categories: (i) Aboriginal and Torres Strait Islander peoples, (ii) Consumer perspectives, (iii) Contemporary and future dietetic roles, and (iv) Contemporary wording and structure of competency. All included documents were indexed and charted which informed revisions to the standards.
Results: Sixty-seven documents were reviewed. Four new competency standards were added to address the skills and attributes required of dietitians to work effectively with Aboriginal and Torres Strait Islander peoples. One competency standard was modified to include an individualized approach as this was deemed important by consumers but not previously included in the standards. The revised standards also place greater emphasis on dietitian's role in teaching and learning. In addition, there are now multiple standards that refer to advocacy, sustainability is referenced multiple times, a new standard specific to advanced care planning has been included, and their structure and wording was revised to ensure it was contemporary.
Conclusion: Using document analysis to revise competency standards offers an efficient and low-cost method to update competency standards in a resource poor environment. This addresses a key issue with competency standards where unless revised frequently they can become rapidly out of date. Further research is needed to learn if document analysis can be used as a method to create rather than revise competency standards.
Introduction
A health workforce that has the necessary skills and qualities to address community and health systems needs is fundamental to improving health (1). Competency based approaches to preparation of the future health workforce are framed by competency frameworks that outline the key work roles, tasks and responsibilities of the health professional (2). While the aim of the competency movement is to focus on outcomes, key criticisms include their individual focus and inability to determine collective competence, the challenge of reflecting the complexity of care and health systems in the frameworks, and the inability for frameworks to keep up with current practice that evolves so regularly (3). Despite these criticisms' competency-based education and indeed competency frameworks dominate accreditation and drive curricula to prepare the health workforce for practice and health professions across the world.
A recent systematic scoping review of the methods and approaches to developing competency frameworks highlighted the range of methods and approaches used in the development of competency frameworks, and the lack of guidance on recommended approaches (4). A range of types of reviews and mapping exercises are used to identify existing competencies and inform the methods used to develop competency frameworks. Literature reviews, including systematic reviews, scoping reviews, focussed reviews, integrative reviews and environmental scans, were found to be one of the most common methods for the development of competency frameworks, used in 61% of included studies (4). However, the method of analysis of the literature and data used to inform standards development was not stated for many of the studies (4). In addition, the reasons for selecting the approaches used were rarely described. Key stakeholders engaged in the development of the standards were typically members of the profession themselves, with few approaches engaging patients or employers, despite evidence that significant involvement of patients or consumers in their healthcare or education has positive outcomes (5). Methods for developing and revising competency standards that capture multiple stakeholder perspectives should therefore be used moving forward. Document analysis is one method that allows this.
Document analysis involves a justifiable sampling approach for selecting documents followed by rigorous coding of documents and examination of codes for patterns. It is accepted and widely used in qualitative research as a method for data collection and subsequent analysis. Given its low cost, it provides a potential method for developing or revising competency frameworks for health professionals in resource poor environments (6, 7). While document analysis has been used largely as a complementary approach, it has also been used as a stand-alone method. When used as a stand-alone method, it can answer questions about policy, past events, cultural context, organizations, activities, groups, and more (6, 7). Document analysis provides an efficient and cost-effective way to obtain multiple perspectives from a range of stakeholders including consumers, employers, health professionals, and, professional and regulatory bodies.
Given that document analysis has not been articulated for the development or revision of competency frameworks to date, the authors sought to revise the National Competency Standards for Dietitians in Australia (8), using document analysis. The aim of this competency standards revision was to identify key gaps in the standards specific to the competency requirements of dietitians, and to revise the competency standards based on the findings of the document analysis. Using this example this paper aims to show how document analysis can be used to inform the revision of competency frameworks and standards.
Materials and methods
Study context
Dietitians were one of the first health professions to develop a competency framework in Australia (9). The competency standards were initially published in 1993 and were reviewed in 1998, 2005, 2009, 2015 (10, 11). Initially focused on entry-level dietitians they have evolved to describe the skills and attributes of all practicing dietitians. A range of different methods have been used to develop these frameworks typically involving the profession itself, including critical incident technique and new graduate interviews (10). The most recent revision in 2015 included the perspectives of employers of dietitians, but the development and subsequent revisions had never included the consumer perspective. Document analysis on its own has not informed previous development or revisions to the dietitians' standards. It was primarily chosen as a low-cost method as there was no resource to collect primary data, and document analysis allowed the incorporation of a range of stakeholder views, including consumers. In this resource poor environment, the need to update standards due to practice evolving was acknowledged. It was deemed essential to have competency standards that are contemporary and consider future practice (12).
Study design, data collection and data analysis
An interpretive approach to this research was taken whereby the researchers acknowledged their position as members of the profession and that standards were subjective. The approach to document analysis used in this research was adapted from Altheide and Schneider's process of qualitative document analysis (13). Altheide and Schneider's document analysis consists of five stages: (i) the problem and the unit of analysis, (ii) constructing a protocol, (iii) themes and frames, (iv) collecting the data, and (v) data analysis. With the five stages made up of 12 steps. For this research the 12 steps were condensed into an eight-step process that is specific to the revision of competency standards. A comparison of this eight-step process compared to Altheide and Schneider's 12 step process can be found in Supplementary Table 1. For each step a description has been provided in Table 1, as well as an example from the revision of the National Competency Standards to illustrate the steps.
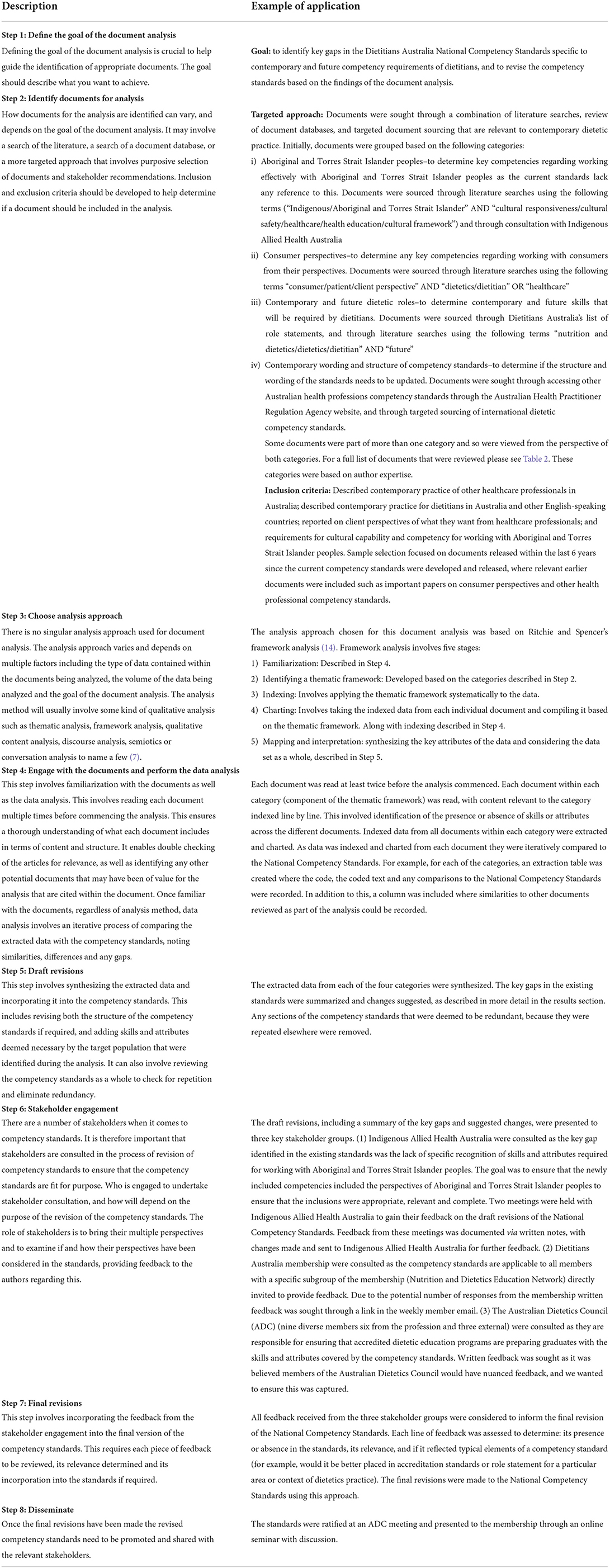
Table 1. Stepwise process for document analysis to inform revisions to the National Competency Standards for Dietitians in Australia.
Ethics approval
As this research did not involve direct involvement with human participants, ethics approval was not required.
Results
In total, 67 documents were reviewed. Twenty-six related to Aboriginal and Torres Strait Islander peoples (18 competency standards and eight frameworks and reports), 10 related to consumer perspectives (eight journal articles and two reports), 32 related to contemporary and future dietetic roles (19 role statements, six competency standards, five journal articles, and two letters), and 24 related to contemporary wording and structure of competency standards. A summary of the documents included in the analysis is included in Supplementary Table 2. Based on the four categories of documents, the key findings are described below and the changes made to the competency standards as a result are presented in Table 2.
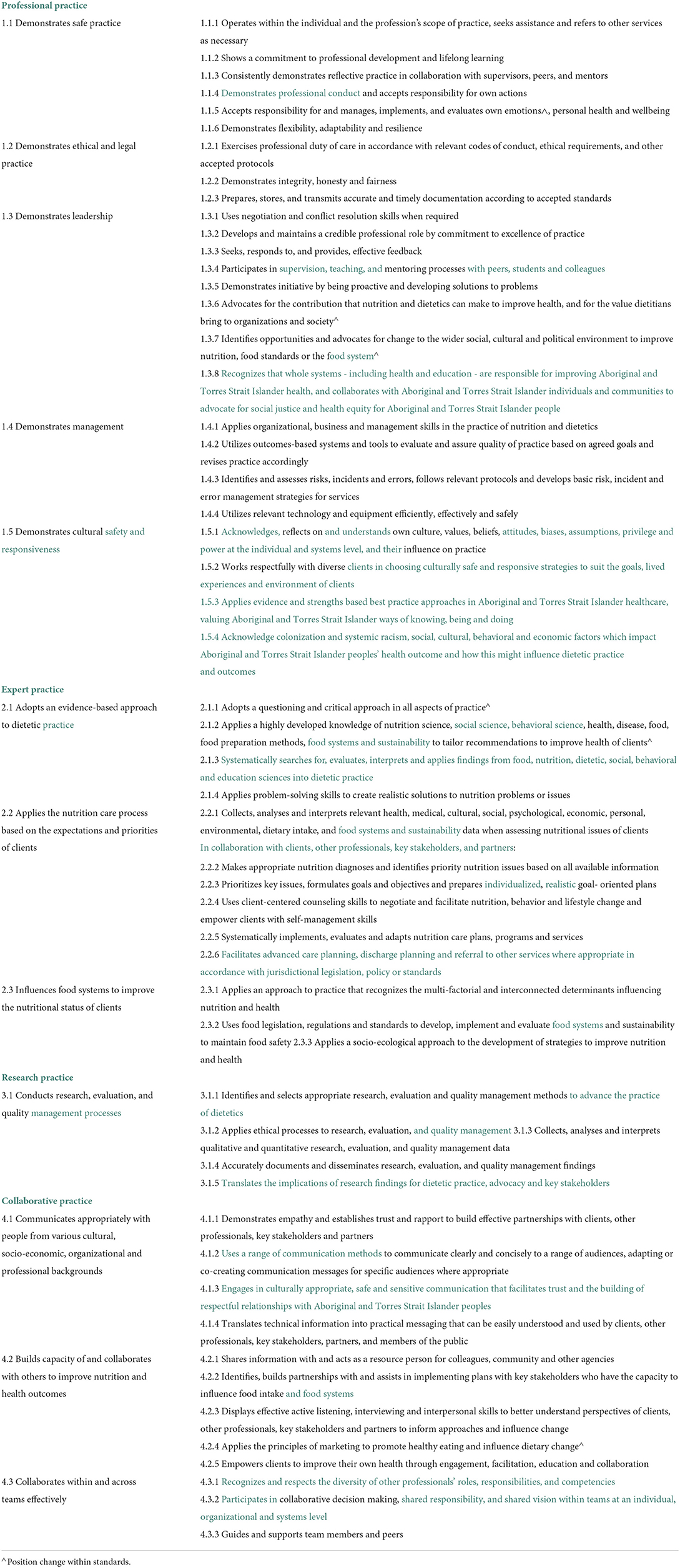
Table 2. National Competency Standards for Dietitians in Australia highlighting key changes in green font.
Aboriginal and Torres Strait Islander peoples
All Australian health professions competencies, excluding nurse practitioners and podiatrists, referred to Aboriginal and Torres Strait Islander peoples, with international dietetics competency standards also having competencies specific to their Indigenous populations where relevant. Therefore, the lack of reference to Aboriginal and Torres Strait Islander peoples and the specific skills and attributes required to work effectively in this space was a key gap in the National Competency Standards. Based on competencies identified from the document analysis as well as consultation with Indigenous Allied Health Australia four new competency standards were added to address the skills and attributes required of dietitians to work effectively with Aboriginal and Torres Strait Islander peoples (see standards 1.3.8, 1.5.3, 1.5.4, 4.1.8 Table 2). In addition to this, an acknowledgment of Aboriginal and Torres Strait Islander peoples was included in the front matter of the competency standards to reflect the professions commitment to improving practice with Aboriginal and Torres Strait Islander peoples.
Consumer perspectives
Only the occupational therapy, registered nursing, midwifery and nurse practitioner standards referenced the inclusion of consumer perspectives in the development of their competency standards. From the document analysis, the main points made by consumers in regards to dietetic care (and healthcare in general), included that dietitians are nutrition experts and deliver individualized care, gaining a holistic understanding of the patient, adapting to the patient's individual circumstances and considering their circumstances, ensuring strategies are appropriate, that there is shared decision-making, and supporting the patient in this process. In addition, consumers highlighted the importance of genuine relationships where the dietitian is supportive, respectful, non-judgemental, empathetic, compassionate, trustworthy, enthusiastic, positive, utilizes active listening, invested in the patient's wellbeing, communicates openly, facilitates behavior change and does not just provide information. Providing information that is clear, simple, understandable, actionable, available in a range of formats, caters to level of health literacy, available in English and other languages, and considers patient's culture is also important. The majority of these concepts were covered in the existing competency standards with one change regarding individualized and realistic goals made to ensure these consumer perspectives on what is important when it comes to healthcare were included (see standard 2.2.3 Table 2).
Contemporary and future dietetic roles
The key gaps identified from the document analysis relating to contemporary and future dietetic roles were: the narrow view of the dietitian's role in teaching and learning; limited emphasis on advocacy; lack of reference to environmental sustainability and; the lack of reference to the role of dietetic practice in advanced care planning. As a result, the revised standards place greater emphasis on dietitian's role in teaching and learning (see standard 1.3.4 Table 2) and the role in improving food systems and sustainability (see standards 2.1.2, 2.2.1, 2.3.2). In addition, there are now multiple standards that refer to advocacy and a new standard specific to advanced care planning has been included (standard 2.2.6 Table 2).
Contemporary wording and structure of competency standards
When reviewing the wording and structure of other competency standards, the name of the domains of the National Competency Standards were found to be inconsistent with other standards. This resulted in a simplification in the domain names. For example, “practices professionally” to “professional practice.” In addition, it was identified that the uncontemporary terminology of food supply was being used. To ensure the language within the National Competency Standards was contemporary, this was changed to food systems (Table 2). While reviewing the wording and structure of the standards, any redundancies noticed were discussed, and the standards streamlined as appropriate.
Discussion
The aim of this research was to use a document analysis method to identify key gaps in competency needs for dietitians in Australia to inform a revision of the competency standards. In doing so we also aimed to show how document analysis can be used as a low-cost solution to revising competency frameworks. We found that the current standards were mostly reflective of contemporary dietetic practice. However, there was an absence of reference to specific competencies relating to Aboriginal and Torres Strait Islander peoples. In addition, there was a narrow view of dietitian's role in teaching and learning, limited emphasis on advocacy, lack of reference to advanced care planning, some key terminology used by consumers such as individualized care not being specifically referred to, and food related language was not reflective of current understanding in this area in food systems and sustainability.
The lack of emphasis on Indigenous culture is perhaps reflective of the systemic racism within dietetics (15–17), and the previous lack of recognition of the pivotal role Indigenous people have in Australian history within the dietetics profession given the recognition many other professions have made in this area as demonstrated by this document analysis. It is well-established that in order to improve the health of Australia's Indigenous peoples non-Indigenous health professions must be culturally safe and responsive (18). Indigenous and non-Indigenous dietitians play a critical role in bridging the health equity gaps and improving nutritional health (19). Ensuring competency standards reflect the performance required of the profession is a key step to advancing practice that is culturally safe and responsive. In addition, Codes of Conduct and Codes of Ethics are key drivers of practice and reform (20). There have been calls to update all Codes of Conduct and Codes of Ethics to ensure cultural safety specifically relating to Aboriginal and Torres Strait Islander peoples is included (20). In line with these calls, Dietitians Australia updated their Code of Conduct at the same time that this review of the competency standards was conducted. Translating the revised standards and Code of Conduct into effective education in university programs that prepare dietitians for practice and upskilling dietitians already in practice is critical for ensuring dietitians are performing against these standards. There is a need for investment by the profession to develop the cultural safety and responsiveness of its members to ensure all dietitians demonstrate performance commensurate with the revised national performance standards.
Expanding the role of the dietitian in food systems and sustainability, and in advocacy is in line with recent evidence on the future of the nutrition and dietetics workforce (21). This recent work has argued that to truly improve nutritional health dietitians need to be system disruptors and work in areas where they may not have worked before. The critical capabilities identified as being needed to fulfill these future roles however align closely with the revised competency standards identified in this study, providing evidence that the standards reflect current and future performance requirements (19). The response of dietetics education providers and the profession to the developing the workforce will be critical in determining the success of the profession into the future and potentially enhancing secure employment which recent evidence suggests is limited among new graduates (22).
The results of this study may be limited if key documents relevant to dietetics practice have been missed as part of the document retrieval process. However, a large number of documents were included in this document analysis in an attempt to mitigate this. In addition, the use of secondary data to gather consumer perspectives may not fully represent their views on the roles and tasks of a dietitian. Competency frameworks should consider involving consumers in their development in the future (23). However, many of the steps used in this document analysis have been recommended as best practice in competency standards development (23). The positive response received from the profession to early drafts of the standards together with the final product provides reassurance that the process has met user needs.
Conclusion
Using document analysis to revise competency standards offers an efficient and low-cost method to update competency standards in a resource poor environment more frequently by incorporating the latest key documents. This addresses one of the key issues with competency standards that are updated infrequently that they are potentially out of date for some time, failing to reflect contemporary changes to practice. This paper has shown that document analysis can be a feasible component of a larger strategy for updating competency standards. We suggest that document analysis can be used at shortened intervals between the usual larger, more in-depth revisions that occur. Whether this method could develop standards as opposed to revising standards remains unknown, but for revisions such that they remain contemporary it is a useful method and should be considered by others in resource poor environments.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
CP conceptualized the study and supervised LA in the collection and analysis of data. Both authors contributed to the article and approved the submitted version.
Funding
This work was funded by the Australian Dietetics Council of Dietitians Australia.
Acknowledgments
We would like to acknowledge all of those involved in the stakeholder consultation including: Representatives from Indigenous Allied Health Australia, the Dietitians Australia Membership, the Australian Dietetics Council, Bree Murray, and Jo Leeson. Their contribution to this work was extremely valuable and ensured the revisions to the standards are fit for purpose.
Conflict of interest
Author CP is current chair of the Australian Dietetics Council and receives a small honorarium fee for this work. Author LA was employed by Dietitians Australia to complete this work. Author CP is associate editor for Frontiers in Medicine, Health Professions Education section. This manuscript has undergone independent peer review and CP excluded from the peer review process and all decision-making regarding this article.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.900636/full#supplementary-material
References
1. Frank JR, Snell LS, Cate OT, Holmboe ES, Carraccio C, Swing SR, et al. Competency-based medicial education: theory to practice. Med Teach. (2010) 32:638–45. doi: 10.3109/0142159X.2010.501190
2. Frank JR, Snell L, Sherbino J. CanMEDS 2015 Physician Competency Framework. Ottawa: Royal College of Physicians and Surgeons of Canada (2015).
3. Hodges BD, Lingard L editors. The Question of Competence: Reconsidering Medical Education in the Twenty-First Century. 1 ed. Ithaca, NY: Cornell University Press (2012).
4. Batt AM, Tavares W, Williams B. The development of competency frameworks in healthcare professions: a scoping review. Adv Health Sci Educ. (2020) 25:913–87. doi: 10.1007/s10459-019-09946-w
5. Bombard Y, Baker GR, Orlando E, Fancott C, Bhatia P, Casalino S, et al. Engaging patients to improve quality of care: a systematic review. Implement Sci. (2018) 13:98. doi: 10.1186/s13012-018-0784-z
6. Bowen GA. Document analysis as a qualitative research method. Qual Res J. (2009) 9:27–40. doi: 10.3316/QRJ0902027
7. Gross JMS. Document analysis. In: Frey BB, editor. The SAGE Encyclopedia of Education Research, Measurement, and Evaluation. Thousand Oaks, CA: SAGE Publications, Inc (2018).
8. Dietitians Association of Australia. National Competency Standards for Dietitians in Australia. Deakin: Dietitians Association of Australia (2015).
9. Ash S, Gonczi A, Hager P. Combining Research Methodologies to Develop Competency-Based Standards for Dietitians: A Case Study for the Professions. Canberra: Australian Government Publishing Service (1992).
10. Ash S, Palermo C, Gallegos D. The contested space: The impact of competency-based education and accreditation on dietetic practice in Australia. Nutr Diet. (2019) 76:38–46. doi: 10.1111/1747-0080.12430
11. Palermo C, Conway J, Beck EJ, Dart J, Capra S, Ash S. Methodology for developing competency standards for dietitians in Australia. Nurs Health Sci. (2016) 18:130–7. doi: 10.1111/nhs.12247
12. Aretz HT. Some thoughts about creating healthcare professionals that match what societies need. Med Teach. (2011) 33:608–13. doi: 10.3109/0142159X.2011.590389
13. Altheide D, Schneider C. Process of qualitative document analysis. In: Altheide D, Schneider C, editors. Qualitative Media Analysis. London: SAGE Publications, Ltd. (2013). p. 38–74.
14. Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Bryman A, Burgess B, editors. Analyzing Qualitative Data. London: Routledge (1994).
15. Delbridge R, Jovanovski N, Skues J, Belski R. Exploring the relevance of intersectionality in Australian dietetics: issues of diversity and representation. Sociol Health Illn. (2022) 44:919–35. doi: 10.1111/1467-9566.13471
16. Lassemillante ACM, Delbridge R. Do we dare ask if this is racism? Nutr Diet. (2021) 78:458–60. doi: 10.1111/1747-0080.12693
17. Boak R, Palermo C, Gallegos D. Towards 2030: Re-imagining the future of nutrition dietetics in Australia New Zealand. Report for the council of deans of nutrition dietetics, Australia New Zealand. (2021). Available online at: www.dieteticdeans.com
18. Jongen C, McCalman J, Bainbridge R. Health workforce cultural competency interventions: a systematic scoping review. BMC Health Serv Res. (2018) 18:232. doi: 10.1186/s12913-018-3001-5
19. Wynn E, Palermo C, Delbridge R, Wilson A. Long-term outcomes of a community of practice for dietitians working in Aboriginal and Torres Strait Islander health: a multimethod, follow-up study. J Contin Educ Health Prof. (2022) 42:e60–8. doi: 10.1097/CEH.0000000000000370
20. Milligan E, West R, Saunders V, Bialocerkowski A, Creedy D, Minniss FR, et al. Achieving cultural safety for Australia's first peoples: a review of the australian health practitioner regulation agency-registered health practitioners' codes of conduct and codes of ethics. Aust Health Rev. (2021) 45:398–406. doi: 10.1071/AH20215
21. Boak R, Palermo C, Beck EJ, Patch C, Pelly F, Wall C, et al. A qualitative exploration of the future of nutrition and dietetics in Australia and New Zealnad: implications for the workforce. Nutr Diet. (2022). doi: 10.1111/1747-0080.12734. [Epub ahead of print].
22. Blair M, Palermo C, Gibson S, Mitchell L. The Australian and New Zealand dietetics graduate outcomes survey: a cross-sectional study. Nutr Diet. (2022). doi: 10.1111/1747-0080.12739. [Epub ahead of print].
Keywords: document analysis, competency framework, competency standard, qualitative research, framework analysis
Citation: Allen LM and Palermo C (2022) Using document analysis to revise competency frameworks: Perspectives from the revision of competency standards for dietitians. Front. Med. 9:900636. doi: 10.3389/fmed.2022.900636
Received: 21 March 2022; Accepted: 19 July 2022;
Published: 04 August 2022.
Edited by:
Adrienne Forsyth, Australian Catholic University, AustraliaReviewed by:
Gina Trakman, La Trobe University, AustraliaAdam Walsh, Australian Catholic University, Australia
Copyright © 2022 Allen and Palermo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Claire Palermo, Y2xhaXJlLnBhbGVybW9AbW9uYXNoLmVkdQ==