 Margaret Spottswood
Margaret Spottswood Christopher T. Lim3
Christopher T. Lim3 Hsiang Huang
Hsiang Huang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Med., 27 May 2022
Sec. Family Medicine and Primary Care
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.892205
Importance: Suicide prevention implementation in primary care is needed due to the increasing rate of suicide in the past few decades, particularly for young and marginalized people. Primary care is the most likely point of contact for suicidal patients in the healthcare system. Attention to the level of medical integration with behavioral health is vital to suicide prevention and is applied throughout this review.
Methods: A narrative review was performed.
Observations: Many interventions help improve suicide prevention care. PCP education, screening, safety planning/lethal means reduction, care transitions, psychotherapy, and medication management are all evidence-based strategies. Additionally, the pragmatic topics of financing suicide prevention, supporting providers, enacting suicide postvention, and preparing for future directions in the field at each level of primary care/behavioral health integration are discussed.
Conclusions and Relevance: The findings are clinically relevant for practices interested in implementing evidence-based suicide prevention strategies by attending to the behavioral health/medical interface. Leveraging the patient/provider relationship to allow for optimal suicide prevention care requires clinics to structure provider time to allow for emotionally present care. Defining clear roles for staff and giving attention to provider well being are also critical factors to supporting primary care-based suicide prevention efforts.
There is a pressing need for implementing evidence-based suicide prevention in primary care. There has been a 36.7% increase in the suicide rate within the past 20 years in the United States (1, 2). Suicide is the second leading cause of death in people ages 15–34 years and the tenth most common cause of death overall (3). Primary care is the most likely point of contact for suicidal patients in the healthcare system, with 77% of patients who die by suicide presenting to primary care in the year prior, and 45% presenting within the month prior to death (4). While the suicide prevention literature available is extensive, there remain few articles focused on the implementation of suicide prevention care in primary care systems that have varying degrees of behavioral health integration.
Compliance standards for suicide prevention mandates are increasing in healthcare (5). Fortunately, effective scalable practice interventions exist, and newer interventions show promise to improve suicide prevention (6). When one healthcare system mobilized multiple systemwide interventions with zero suicides as a goal, this rate was achieved and sustained for years (7). Suicide prevention strategies become easier to implement when primary care practices have the ability to track patients and collaborate with behavioral health providers.
To provide suicide preventive care in a primary care setting, some type of relationship with behavioral health specialists is critical. The suicide prevention literature thus far has not directly addressed how to provide preventive care considering the varying levels of behavioral health integration in practice. The relationships between primary care teams and behavioral health colleagues like psychologists, social workers, and psychiatric providers exist on a spectrum of informal to fully integrated. This article organizes achievable evidence-based interventions for primary care practices based on their current level of behavioral health integration.
There are six levels of identified mental health/primary care integration identified by the SAMHSA-HRSA Center for Integrated Health Solutions and summarized with permission in Table 1 (8). For the purposes of this article, we address three different levels of organization between primary care/mental health systems: (1) detached but with some coordination (“Informal Coordination”) (2) co-located (“Co-Location”) and (3) fully integrated (“Integration”).

Table 1. Levels of integrated healthcare framework.
The purpose of this article is to present and synthesize a comprehensive review of the literature on suicide prevention in primary care with different recommendations depending on the level of behavioral health integration. Many countries continue to operate behavioral health and medical services in a non-integrated fashion. In the United States today, with its fragmented healthcare reimbursement system, all three different levels of organization exist (Informal Coordination, Co-Location, and Integration). Efficient implementation for evidence-based interventions is recommended for these three levels of primary care/behavioral health collaboration. Financing of suicide prevention in the United States is discussed, as poor understanding of reimbursement is often an implementation barrier. Support for primary care providers asked to take a more active role in suicide prevention is presented as key to workforce sustainability. Finally, future directions for suicide prevention are discussed, focusing on how practices might prepare now for ensuing innovations. This paper should prove useful to clinic administrators such as medical directors and practice managers, primary care providers, and those involved in shaping suicide prevention policy. Additionally, suicide prevention resources are made available throughout the paper and in Appendices 1, 2.
A narrative review of the literature was conducted due to the broad scope of the topic. The search strategy involved identifying previously published clinical guidelines, systematic reviews, studies of novel primary care-based interventions, and other primary literature to answer the question of how to implement interventions to decrease the risk of suicide for primary care patients.
PubMed and Google Scholar were searched, focusing on seminal articles in the past 20 years with particular attention to recent evidence-based improvements in care. Searches included combinations of the following terms and variations thereof: “suicide,” “primary care,” “prevention,” “screening,” “technology.” Bibliographies of relevant articles were also reviewed to identify additional appropriate references and primary literature.
Studies were reviewed by authors MS, CTL, and HH, taking into consideration strengths and limitations of study designs, relevance to improving care provision and readiness for new innovations in the primary care setting. Articles were excluded if they did not suggest interventions feasible in a primary care population. Articles were included if they described evidence-based screening and suicide prevention interventions or added depth to understanding an important topic.
While some interventions will be more feasible to implement in practices with higher levels of integration, universal evidence-based standards are recommended for all practices. Standards include primary care provider (PCP) education and practice-wide implementation of screening and effective interventions to reduce risk. Risk reduction interventions include safety planning with removal of lethal means and providing caring contacts around higher-risk care transitions (e.g., following a psychiatric inpatient or emergency room discharge) (6). Evidence-based therapy, medications, and suggested financing for suicide prevention are also offered in this section.
In a recent meta-analysis, general practitioner and non-psychiatrist physician education on suicide prevention was found to be an effective suicide prevention intervention (6). In one older study, suicide was explored by primary care providers with only 36% of depressed patients (10). Physicians were more likely to inquire about suicide if they had had personal experience with depression, if the patient made a request for an antidepressant, or if the patient met criteria for major depressive disorder (10). Suicide care improves when systems improve, and one of the first steps is PCP education in suicide identification and management (11–13). Once PCPs feel sufficiently trained, they have increased clarity, job confidence, and positive attitudes about their efficacy in preventing suicide (14). Physicians receive effective one-time training in many topics, but standalone one-time training has been demonstrated to be insufficient for suicide prevention (9, 12, 15–18). Repeating educational sessions over years continued to correlate with a decrease in suicide (6, 9, 19). Training individual providers is an essential element in suicide prevention and educational efforts must be sustained to ensure continued impact.
PCP training should include the topics of screening and treatment of depression and substance use disorder (SUD), with psychiatrists available to supplement this treatment for more complex patients (6) (see Box 1).
Box 1. PCP education based on level of collaboration

The United States Preventive Service Taskforce (USPSTF) recommends universal depression screening for adults in primary care when paired with resources for diagnostic accuracy, treatment, and follow-up (20). Universal depression screening in primary care for adolescents ages 12+ is also recommended by the USPSTF and endorsed by the American Academy of Pediatrics (21). Data suggest that depression screening and treatment prevents suicide (6).
In 2014, the USPSTF found insufficient evidence to recommend for or against universal suicide screening in primary care for adolescents, adults, and older adults who lack a mental health diagnosis (22). A 10-year systematic review on suicide prevention strategies (23) and a review of U.S. Veteran primary care populations (24) resulted in the same conclusion. The case for universal suicide screening remains controversial within the suicide prevention community since suicidality can occur in the absence of identifiable risk factors (25, 26). One study found that only 39.5% of medically hospitalized adolescents (ages 10–21) who screened positive for suicidality also met criteria for depression (27).
However, screening for high-risk groups is agreed upon as the standard of care. High-risk groups in this context are those with any mental health or substance use disorder or taking a psychotropic medication (12, 28–31). In one cross-sectional study of 74 German primary care practices, additional predictors of suicidality included depression severity, male sex, and physical pain (32). More recent population analyses indicate rates increasing at a higher rate in Black and Asian or Pacific Islander youth, particularly female youth (33). Other recent population level data show that rates per sub-population vary significantly by geographic location (34).
The Perfect Depression Care Initiative in the Henry Ford Health System screens populations at risk, then stratifies patients into acute, high, moderate, and low risk for suicide based on screening, risk factors, and protective factors (7). Thereafter, the program immediately connects patients with targeted care based on these risk levels (35). Clinics should make sure patients who belong to populations with risk factors are screened.
Many evidence-based suicide self-report screeners are available to identify suicide risk and fulfill the current standard of care (36); clinics can take into account their patient population and provider workflow when selecting a screening instrument (37).
Because the PHQ-9 is already used in many health care systems for depression screening and contains question #9 (“thoughts that you would be better off dead, or thoughts of hurting yourself in some way”), many studies use question #9 to detect suicidal thoughts (38–41). When question 9 was examined in an observational analysis of data from a patient registry of a collaborative care program for safety-net primary care patients (n = 11,015), suicidal thoughts were present in 45.2% of patients on initial assessment (39). Of those with a positive question 9, 5.4% did not meet screening criteria for depression, and only 2.2% of people who indicated the highest score for question 9 would have been missed through PHQ-2 screening. Question 9 of this instrument has demonstrated effectiveness in predicting suicidal behavior across minority racial and ethnic groups (42).
While Question 9 of the PHQ-9 is a convenient suicide screening question, it is not precise, asking about two variables at once (self-harm and wanting to be dead), and does not directly assess whether a patient wants to kill themselves (27, 28, 38, 39, 43–47). Despite these limitations, because of the ubiquity of the PHQ-9 for depression screening and treatment response measurement, using question 9 as a suicide screening question with additional follow-up screening available for a positive screen is a pragmatic approach.
Suicide researchers examined the administrative burden of asking all hospitalized medical patients about suicide directly (48). Adding four suicide screening questions (to the PHQ-9) administered by nurses in a hospital setting took 2 min for a negative screening and 4 min for a positive screen with no patients in the study requiring acute intervention (48).
Created for use in primary care and specialty medical populations, this questionnaire is triggered when patients answer yes to having thoughts of hurting themselves (49). It helps the clinician evaluate past suicide attempts, suicide plan, probability of completing suicide, and preventive factors. It then stratifies risk into three categories: minimal, lower, and higher. In a study 0.4–1.6% of patients screened met criteria for higher risk, triggering emergency intervention (49). Preventive factors for those with high scores included faith, family, hope for the future, and fear of attempt failure (49).
The ASQ has been approved by the Joint Commission for youth and adults and has been studied in inpatient medical settings for adults (2-item version) (48) and outpatient settings for youth ages 10–24 (4-item screening version) (50). It has high sensitivity and negative predictive value (50–52).
Following a positive screen, the ASQ toolkit helps the team conduct a brief suicide safety assessment (BSSA) which determines next steps (acute positive screen with immediate intensive intervention or non-acute positive screen with brief suicide safety assessment to determine if full mental health assessment is needed), as well as providing all patients with a suicide prevention resource list (53).
In a recent retrospective analysis of patients aged 10–17 years given the ASQ (N = 91,580) across a safety-net public academic healthcare system, an emergency department, and 20 community outpatient clinics, universal screening resulted in 3% of patients being at any risk of suicide and acute positive screens in 1% of patients encounters (54). One in four patient encounters with a presenting psychiatric complaint resulted in a positive screen while only 2.7% of other encounters did.
Another suicide screening tool with a broad evidence base is the C-SSRS, which is validated for patients ages 12+ (55). It has been used extensively in research studies and can also be used by lay people, in healthcare settings, and in other community settings. A screening version is available that comprises two stem questions with four follow-up questions if the stem questions are positive, and one follow-up question if the stem question is negative. The triage points for primary care suggest three paths: (1) no intervention/referral needed, (2) non-urgent behavioral health referral or (3) urgent behavioral health consultation and patient safety precautions.
One qualitative study noted that heavy episodic drinking often occurred prior to unplanned suicide attempts (56). Alcohol use is not consistently assessed in primary care, and far fewer patients receive the recommended care for alcohol use disorder than for medical disorders (12, 57, 58).
Twenty percent of primary care patients have been found to drink in excess of National Institute on Alcohol Abuse and Alcoholism guidelines (59), resulting in the USPSTF recommendation that some level of screening for alcohol use be performed for each primary care patient >18 years old (60, 61). While a full discussion of screening and treatment for alcohol use is outside the scope of this narrative review, our recommendation includes using the 10-question Alcohol Use Disorders Identification Test (AUDIT) screen to further quantify alcohol use (60). Patients are provided increasing levels of support based on alcohol use risk scores (62). Recommended treatments include motivational interviewing and, for those with alcohol use disorder, behavioral treatment, support groups, pharmacotherapy (naltrexone, acamprosate, or disulfiram) and detoxification if needed (63).
Many primary care patients who subsequently die by firearm suicide will honestly answer screening questions about firearm access (64). Because of the high fatality linked to firearm ownership, recent evidence suggests that screening all primary care patients for firearms ownership with appropriate follow up care may prevent death from suicide for those who do not have a mental health or SUD diagnosis.
This is a pocket guide to help clinicians more thoroughly assess a higher risk patient to (1) identify risk factors; (2) identify protective factors; (3) conduct suicide inquiry; (4) determine risk level/intervention, and (5) perform documentation (65, 66). This resource aids behavioral health clinicians and medical providers in performing safety assessments.
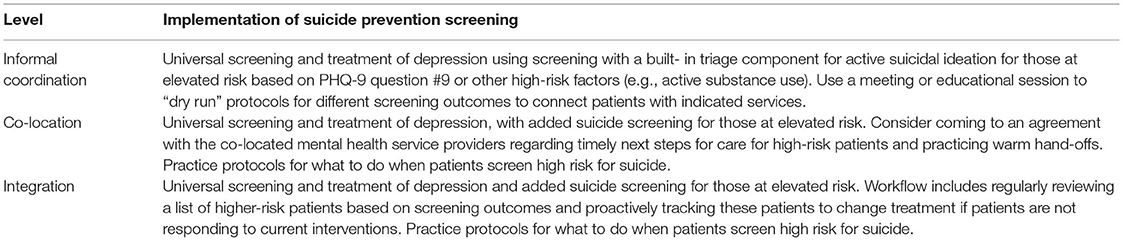
In summary, the best way to screen for suicidality by self-report continues to be an active research question and is dependent on the particular risk/benefit ratio based on specific primary care populations and how immediately available the behavioral health resources are in a specific primary care clinic. Universal depression screening and treatment is the standard of care and helps prevent suicide. Patients presenting with a mental health concern, with a mental health diagnosis, with a substance use disorder, or prescribed a psychotropic medication should be screened specifically for suicide risk in primary care. If the primary care population is a higher-risk population, it is recommended that 2–4 suicide screening questions are automatically administered following the PHQ (see Box 2).
Box 2. Suicide risk screening based on level of collaboration
Patients will be stratified by risk after screening. Those with acute risk should be transferred to a higher level of care such as a behavioral health specialist safety assessment and/or emergency services. Patients with non-acute risk should complete a brief suicide safety assessment to determine if, and how soon, a comprehensive mental health evaluation is needed (67). Interventions for non-imminent risk that can be provided in the primary care setting include safety planning, removing lethal means, and timely contacts targeting care transitions (36). Genuine emotional connection with clinic staff and providers is important throughout this process and is discussed further in the “support for providers” section.
After a patient is identified as being at elevated risk for suicide, immediate safety planning during the visit is recommended. When separate from ongoing psychotherapy, such safety planning is called a Safety Planning Intervention (SPI) (68). This consists of a written list of coping strategies and sources of support that are prioritized to help patients address a suicidal crisis; this brief intervention should be done at the PCP office as suicidal patients do not often follow up with behavioral health referrals (68–71).
Safety planning should not be confused with a “contract for safety/no-suicide contract,” which has been shown to be ineffective (73). Safety planning requires that practice managers designate a work-flow to accomplish this when needed, and allow for building in mental health support staff based on local resources (68); practices without behavioral health support should determine in advance who will create the safety plan with the patient (e.g., nursing staff, trained medical assistants, PCPs). The practice can review standardized forms like the safety plan script and resource list from the ASQ Toolkit (53) and the Brown-Stanley Safety Plan Template (71). Safety planning includes helping the patient write down warning signs, internal coping strategies like writing and self-soothing, external coping like distraction via people and social settings, individuals to call for help, professional resources to contact, and environmental lethal means reduction. Families and other social supports are important participants in safety planning, with the patient's permission. The Perfect Depression Care Initiative in the Henry Ford Health System provides a handout called “Understanding and Helping Someone Who is Suicidal” which includes information about warning signs and feelings, action steps, how to work with the treatment team, and whom to contact if a person feels suicidal (7). Suicide prevention literacy of providers, patients, and social supports drive success in brief contact interventions (74). Primary care practices can put in place protocols to enlist families and other social supports if the patient grants permission.
This is part of safety planning but addressed separately in this review as the nuances are such that primary care clinics may consider additional training for staff. Primary care clinics can endorse public health interventions like pharmacy/police collection boxes for extra medications and firearms as safety measures. Suicide attempts often occur during an acute crisis; 52% of completed suicides occur via firearms, 23% occur via suffocation, 18% via poisoning/overdose, 2% via jumps, 2% via cuts, and 4% via other means (75). Ninety percent of those who survive a first attempt do not subsequently die by suicide (76). When public health interventions target decreasing access to lethal means, fewer people complete suicide (77–80).
Broaching how to decrease access to lethal means with a patient is a specific skill set for integrated behavioral health clinicians or for medical clinicians and staff in practices without on-site behavioral health support. The Counseling on Access to Lethal Means (CALM) 2-h training course was created to provide this skill set. CALM focuses on the evidence behind reducing access to lethal means to prevent suicide, practicing strategies for conversations, off-site and in-home storage options for firearms and dangerous medications, and plan with patients and families to increase follow up and reduce access to lethal means (81).
The USPSTF has called for research focusing on behavioral health care transitions (22, 37). Transitions of care between the psychiatric inpatient unit or emergency room and outpatient care are times of increased risk for suicide (82). The above interventions as well as caring contacts (see below), timely follow-up visits, and contacting the patient if they miss a visit should be employed during these times of higher risk. Primary care offices should plan for “wraparound care” of those identified as at acute risk. If a care manager is part of the team, this can include frequent check-ins with the patient and coordination between any systems serving the patient (e.g., inpatient hospital, therapist, or crisis team) (see Box 3).
Box 3. Safety planning interventions and lethal means reduction based on level of collaboration

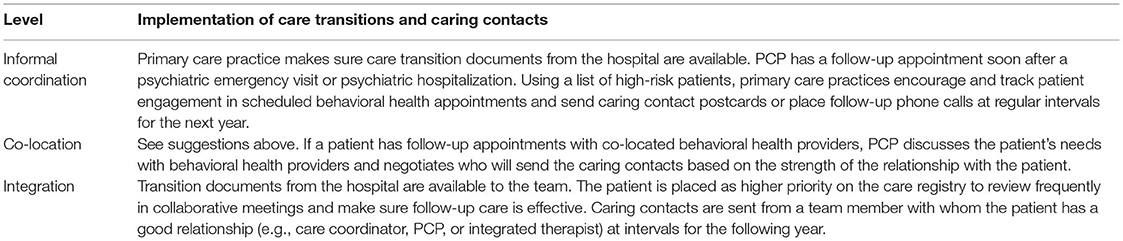
Once patients are identified as being at increased risk for suicide, reaching out at several specific times to provide brief, non-demanding communications voicing concern and care have shown to improve outcomes (83–88). This has been studied using postcards, telephone calls, and text messages. Systematic ways of implementing caring contacts can remove the burden of care from providers alone (83). Helping patients remember that they matter to providers leverages the patient-provider relationship against suicide. There are free examples of text for caring contacts available for clinics to implement this intervention (e.g., Caring Contacts Text and Scripts are available at nowmattersnow.org) (see Box 4).
Box 4. Care transitions and caring contacts based on level of collaboration
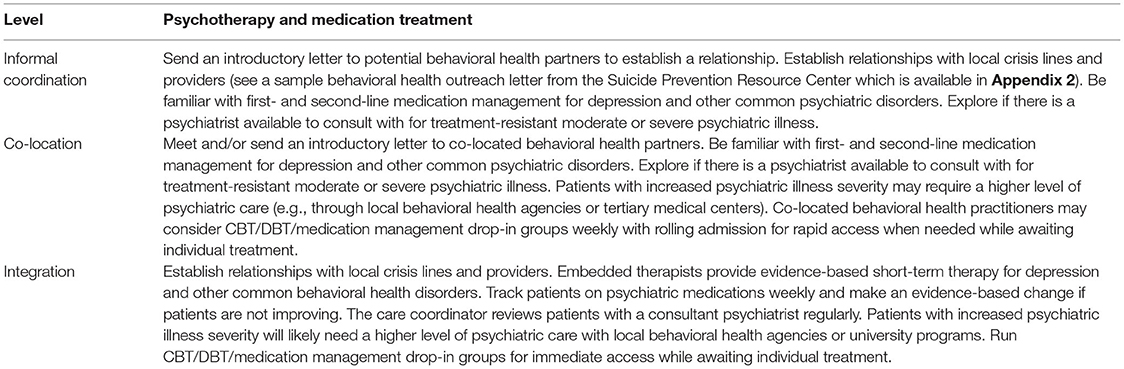
The Zero Suicide model recommends that primary care clinics without integrated behavioral health services establish relationships with local crisis lines, therapists, and other behavioral health partners. Therapies with evidence to help prevent suicide include cognitive therapy-suicide prevention (a form of cognitive behavioral therapy, or CBT) (6, 69, 89), dialectical behavior therapy (DBT) (6, 90), problem solving therapy (91), mentalization based treatment (92), and psychodynamic interpersonal therapy (93, 94). CBT and DBT are recommended as the most scalable options (6).
Psychotherapy, a relatively resource-intensive treatment, should be recommended to those with high suicide risk who do not currently require a higher level of behavioral health care (such as an intensive outpatient program or inpatient hospitalization). In order to provide immediate therapy and medication management for those at risk, the Perfect Depression Care Initiative in the Henry Ford Health System offered at least one 90-min weekly drop-in group at each outpatient clinic run by a psychiatrist and social worker for immediate access to evidence-based therapy and medication management (7). One meta-analysis demonstrated that general group treatment decreased suicides in one study, decreased suicidal ideation in half of studies, and had no effect on non-fatal suicide attempts (6). Groups can be offered as an immediate scalable intervention, but more robust research is needed regarding which patients most benefit from this treatment and which will need additional interventions.
Finding and treating the modifiable factors of suicidal ideation has been the standard of care, with particular attention given to depression care. Recent thinking around suicide prevention increasingly focuses on treating suicidal ideation in parallel to treating the presumed underlying disorder (95). Medications with the potential of lowering risk of suicide include lithium in patients with bipolar disorder (95, 96), ketamine in patients with severe major depression (95, 97), and clozapine in patients with schizophrenia (95, 98).
The combination of therapy and appropriate medication for identified psychiatric conditions has been demonstrated not to be superior to either alone for suicide prevention (6).
The following section on the financing of suicide prevention is specific to the United States. Country-specific literature regarding how different payment structures drive behavioral health/medical integration are required when examining this question for other systems of care.
In the United States, safety planning and caring contact follow up phone calls are relatively low intensity and have been demonstrated to be cost effective in fee-for-service primary care settings if the suicide risk prediction used has a specificity of >94% and sensitivity >16%, with a PPV of 1% or greater (99). More intensive intervention risk reduction included CBT or DBT therapy, which, to be cost effective, requires the suicide risk prediction method to have a specificity of 95% and a sensitivity 35% or greater, resulting in a PPV of 2%. A PPV of 2% is similar to other primary prevention risk thresholds with rare but high-cost negative outcomes (99, 100).
With the current fee-for-service reimbursement model in much of the United States, billing for suicide prevention is an important consideration. Comprehensive coding flow diagrams can be found for standalone primary care clinics and for integrated primary care/behavioral health clinics on the Zero Suicide website (101). See Table 2 for a summary of currently available codes (101) that are currently available (see Box 5).
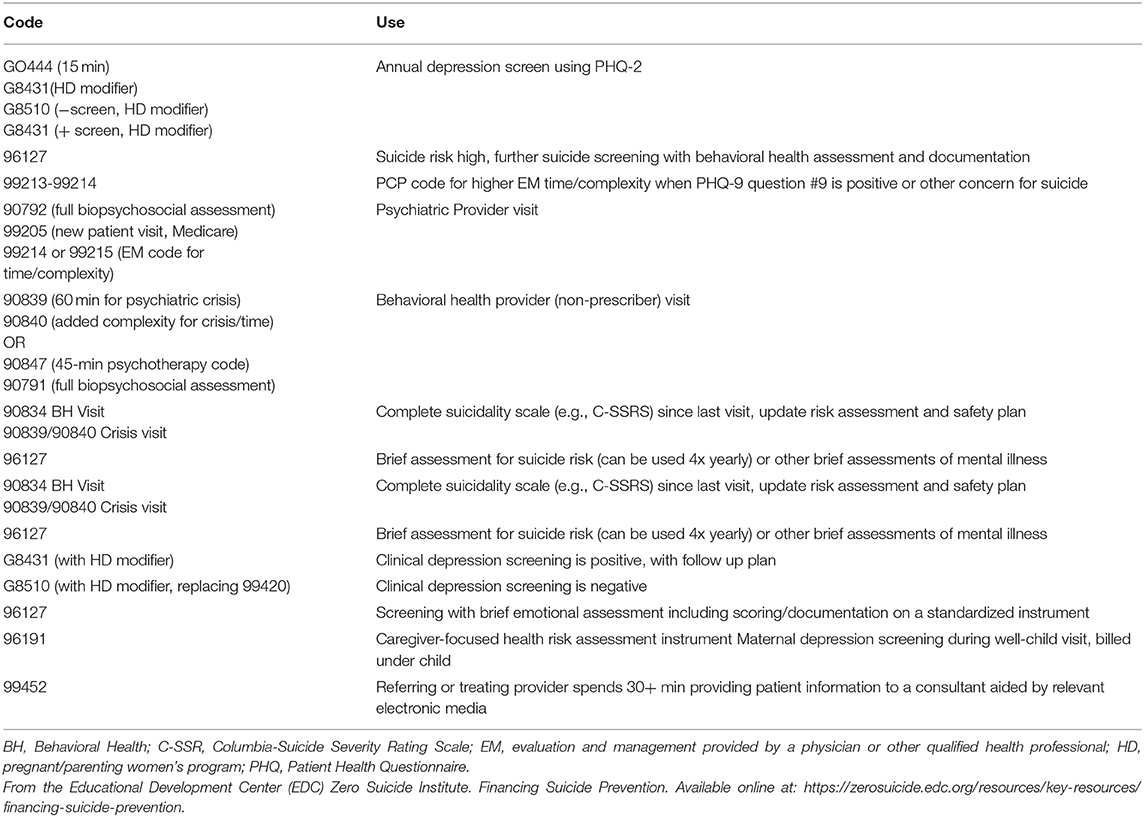
Table 2. United States reimbursement codes for any behavioral health integrated level.
Box 5. Psychotherapy and medication treatment based on level of collaboration
Primary care clinics that have implemented the Collaborative Care Model (CoCM) may have higher capacity to provide and follow up on rapid, targeted treatment for those with suicidal ideation and/or depression symptoms (12, 25, 29, 30, 39, 72, 102). Collaborative care is an integrated care model in which a team consisting of primary care providers, care coordinators/case managers, and psychiatric consultants work together providing screening, regular/proactive monitoring and treatment, and psychiatric caseload reviews, to target care to outcomes with evidence-based techniques (103). This has been shown to improve mental health outcomes (103).
Practices adopting CoCM still require the ability to refer the highest-risk and highest-complexity patients to community behavioral health providers for appropriate ongoing specialty services. CoCM does not address all behavioral health needs in a population but is designed to provide effective care in the primary care setting, thus enabling specialty behavioral health resources to be devoted to the highest-severity patients.
Reimbursement for team-based care and population health management programs is progressing at different rates across the United States. Accountable Care Organizations (ACOs) are one such model that incentivizes primary care clinics to take on population health management (104). To fully adopt these models, primary care-based data systems to measure per member per month utilization and cost are needed (104). However, there are billing codes for team-based population behavioral health care within the current fee-for-service system. New codes were introduced in 2017 and, in some U.S. states, integrated primary care/behavioral health can be reimbursed for work undertaken together (105–107).
Different types of practices may have different code availability, not all payers or states reimburse for each code, and the AIMS center and the CMS Medical Learning Network will provide the most up-to-date information as these codes evolve, see Table 3 (106, 107) (see Box 6).
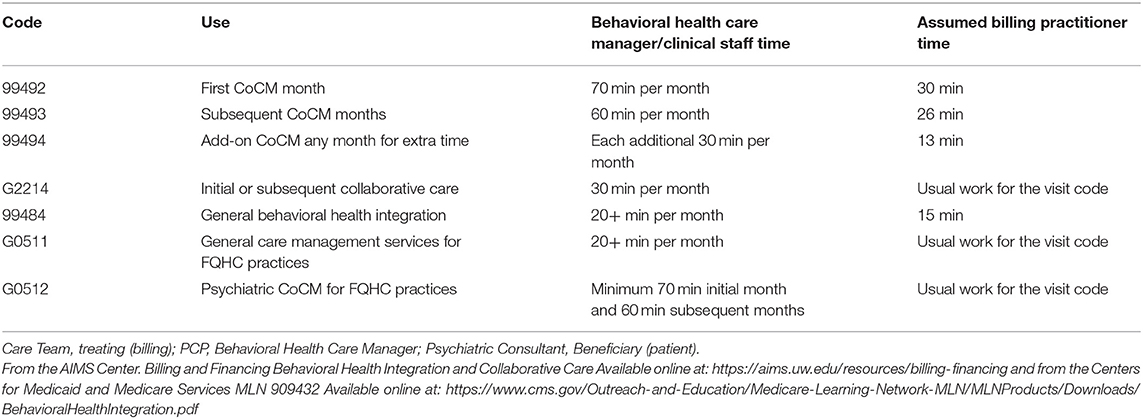
Table 3. United States integrated team-based reimbursement codes.
Box 6. Financing suicide prevention care based on level of collaboration

Physicians are at higher risk of suicide than the general population and female physicians are at higher risk relative to males (108–110). Poor medical health, depression, and work stressors demonstrate a stronger association with physician suicide than with non-physician suicide (110). In one academic medical center, a majority of physician respondents to a wellness survey met criteria for being at moderate or high risk of suicide or depression, and though only 15% of these at-risk respondents engaged in mental healthcare offered; those who did were satisfied with the care (111). Workplace cultures that include a healthy environment and increased mental health support for workers may be particularly beneficial to clinicians and staff who do not regularly engage in self-care.
Increasing support for PCPs enhances clinician-patient communication. Relationships with providers who are caring and listen help patients disclose suicidality; data indicate that patients believe it is appropriate for providers to ask about suicidality, report that provider overreaction is a deterrent from further disclosure, and note that, when disclosures occur, they want to be helped but are worried about negative consequences (56, 112). Although PCPs are increasingly called upon to provide mental health care, they typically do not have time built into their clinic to receive supervision and support to reflect on the emotional interactions they have with patients (113). In a qualitative study patients noted that, when the provider asked about suicide risk “like reading off a script and… checking boxes rather than I'm afraid for your safety,” it seemed that the provider was only asking out of obligation (56). Conversely, when providers expressed genuine listening and caring, it was easier to be honest about their experiences, and “expressions of listening and caring were more important than finding an immediate solution to their problems” (56).
One way to help clinicians convey the listening, empathy, and respect needed to promote communication and increase hope for individuals contemplating suicide is for clinicians themselves to feel heard, have empathy from, and feel respect within their workplaces. Workplace cultures that acknowledge the reality of healthcare being complex and support knowledge improvement and emotional healing for patients, families, staff, and communities at large may lead to improved overall wellbeing and improved provision of effective suicide care (114). Restorative Just Culture has been used in one public mental health system along with a Zero Suicide framework. This model shifts the focus of a post-suicide inquiry from who missed an opportunity to prevent the loss of life to what was responsible for a missed opportunity by asking who is hurt, what do they need, and who is responsible for meeting that need (114). Overall, work is a major social determinant of health, and public health literature suggests that work redesign can address conditions that lead to stress and burnout in general (115). While a comprehensive discussion on addressing physician burnout is outside the scope of this paper, several important approaches include training and employer support to improve social relations at work, increasing worker schedule control and voice, and adjusting job demands (115). This theme of having systems responsive to the emotional health of workers overlaps with inclusion of a Restorative Just Culture alongside suicide prevention efforts, a concept discussed in the next section.
One qualitative thematic analysis of provider perspectives regarding factors important to suicide risk assessment and management highlighted the importance of team-based care, patient-provider relationships built on trust, integrated behavioral health providers giving education to PCPs about suicide prevention, the ability for patients to access mental health care, and system-wide prevention efforts (116). In addition to improved medical and mental health care and outcomes for patients, one of the secondary benefits of integrated team-based models is that consultation about patient care through regular case review also appears to be associated with favorable PCP experience (117).
Just as suicide prevention improves with system culture change (7, 72, 114), provider well-being and resulting ability to participate in mental health work can be best addressed at a clinical systems level rather than an individual provider level (95, 115) (see Box 7).
Box 7. Support for provider wellbeing to improve clinician-patient communication based on level of collaboration

The Zero Suicide framework is both motivational and aspirational. With appropriate and rigorous care, suicides can dramatically decrease in populations (72). Tragically, just as with caring for ill medical patients who sometimes die, not every suicide can be prevented (114). Patient suicide has a profound impact on clinicians and healthcare workers (118–120). When suicide does occur, it is traumatic to providers, and trauma may lead people to isolate from one another (121). Because of suicide contagion, thoughtful suicide postvention may also serve as an antidote to this isolation and as suicide prevention for providers and others in the community.
One retrospective study found that PCPs feel grief, guilt, and self-scrutiny following a patient's death by suicide (122). Clinical staff can feel that they failed the patient and worry about their own clinical skills and choice of career (114, 123, 124). Amidst emotional loss, clinicians may fear or experience legal retribution, and possible loss of licensure, income, and reputation (114, 124–126). Most providers report turning to peers and colleagues for support following a patient's suicide (122).
Turner notes that, in the aftermath of a suicide, healthcare organizations may focus solely on documentation of risk prediction or lack thereof and overlook factors that have an equal or larger impact on suicide prevention (114, 126, 127). Helpful factors to examine include therapeutic relationships and instilling a sense of hope for future patients struggling with suicidal urges (114, 128). Primary care clinic administrators can help providers identify and go through the multiple elements of a comprehensive suicide postvention, including addressing emotional, professional, legal, and administrative consequences (129).
One model of organizational support (114, 128) for providers and other second victims like family/friends in suicide postvention is the TRUST acronym: just Treatment, Respect, Understanding and compassion, Supportive care, and Transparency/opportunity to contribute (114, 130). Postvention toolkits are available to provide evidence-based practices; toolkits include Texas' postvention toolkit, the Suicide Prevention Resource Center-endorsed practices, and the LOSS program (Loving Outreach to Survivors of Suicide program) (131) (see Box 8).
Box 8. Suicide postvention based on level of collaboration

There are numerous future directions for suicide prevention in primary care. For the purposes of this paper, we focus on the following: addressing underserved populations, improved detection/prediction, technology-based interventions, and shortening timelines of suicide risk detection and intervention.
Increasing identification and treatment engagement of underserved populations at risk of suicide should be prioritized. There is a pressing need to acknowledge and mitigate the social inequalities that impede provision of evidence-based treatment for those unjustly suffering the effects of systemic poverty and/or bias (95, 132). Suicide is increasing in Black youth (133, 134), and there are higher rates of suicide attempts among LGB people (135). Social adversity and clinician bias due to ethnicity contribute to screening and treatment gaps for higher-risk populations (136). Clinics can work to hire staff and providers that represent the demographics of the patient population served and to decrease attitudinal barriers for all staff by making sure suicide prevention and other trainings include opportunities to expand clinician and staff self-awareness around bias and anti-biased actions.
More research is needed to predict acute suicide risk; to date, only 0.1% of studies of suicide completion among those at elevated risk of suicide in the past 50 years have looked at suicide outcomes within 30 days, a clinically relevant timeframe, whereas most studies have assessed suicide completion over longer timelines (137). Interactive digital tools may activate patients to increase discussion of suicidal thoughts with PCPs (138). Such programs might be offered in waiting rooms or through social media algorithms to help with identification. Due to the need to improve interventions prior to the first suicide attempt and the waxing and waning nature of suicidality, digital phenotyping via smartphones also holds promise as a future intervention (139, 140). There is also ongoing research to identify the most effective treatment for each patient among those at risk of suicide (140, 141).
While self-report is an important method to identify suicidal ideation [>60% of people who attempt suicide seek help first (142, 143)], subjective markers of suicidality have limitations. People lack conscious awareness of factors that influence their behaviors (144, 145), they may have motivation to deny or conceal suicidal thoughts [78% deny these in their last communication prior to death (144, 146)], and suicidal thoughts are transient (147). An implicit association test (IAT) asking patients to pair “me”/“not me” and “life”/“death” has been tested in a variety of settings as a behavioral measure of suicide prediction. Results demonstrate difficulty differentiating between patients who have suicidal thoughts and those who will attempt suicide (144). There may be clinical utility using incremental prediction (145, 148) for this test when paired with other methods of suicide prediction, but more research is needed.
Machine learning algorithms to predict suicide risk can take into consideration known risk factors, such as treatment history, family history, general psychopathology, prior suicidal thoughts and behaviors, social factors, physical illness, demographics, externalizing and internalizing emotional experiences, psychosis, and biological factors (137). Novel risk factors can also be identified (149). Evidence exists for machine learning algorithms in the EMR paired with the PHQ-9 question 9 resulting in effective screening for suicide in a college student population (38). Digital phenotyping may also contribute to machine learning and contribute to suicide risk prediction (141, 142).
Separate from EMR data mining, Computer Adaptive Testing for Mental Health (CAT-MHTM, Adaptive Testing Technologies, Chicago, IL, www.adaptivetestingtechnologies.com) asks patients to fill out a set of questions, the answers to which change subsequent questions in real time, allowing for a short and precise screen that can be repeated over time using different questions (150, 151). In one pilot RCT of 20 patients, CAT-MH demonstrated greater association with gold-standard diagnostic tools such as the PHQ-9 and C-SSRS (151). More research is needed prior to scaling this intervention, but the benefits of improved screening through an adaptive algorithm may enhance suicide risk identification. If subsequent studies continue to support this method, CAT-MH may help with rigorous, efficient screening, freeing up provider time for therapeutic interventions.
Overall, studies suggest that targeted provider-initiated screening of higher-risk primary care patients combined with universal EMR mining may be the most thorough and accurate approach to timely suicide risk identification in primary care (23). In essence, no single strategy is best alone, so practices would need the ability to combine evidence-based algorithms in the future (23).
Regarding future directions for treatment, the current standard of care includes targeted caring contacts (99) and safety planning, lethal means reduction, and appropriate referral (36). Technology may improve engagement in treatment for suicidal ideation. However, one randomized clinical trial found that EMR online messaging by care managers did not change suicide or self-harm risk while the online delivery of dialectical behavior therapy skills was associated with a significant increase in risk of severe self-harm (death or hospitalization) (152). Engagement with mental health treatment apps can be high (153–157) but, between 10 days to months after download, the level of engagement may decrease, resulting in retention rates of 50% or lower (158–160). Primary care practices should be discerning regarding how care is delivered and which suicide prevention and depression apps are recommended.
Most mental health and suicide monitoring apps have not been systematically vetted for safety and effectiveness (157, 161, 162). Furthermore, apps may focus on engaging individuals alone rather than on engaging friends, family and clinicians (157). Martinengo suggests that the level of app governance should match the potential risk/benefit to users and concludes that suicide prevention apps do not meet this standard and often do not include best practices for suicide prevention (163). However, there are several evidence-based apps containing many best-practice features (including means safety, support, crisis line access, treatment, and safety plan) (157). The Koko App targets increasing treatment engagement for those at risk (164) by using machine learning from social media posts to identify those “online and in crisis” but reluctant to engage in treatment (165). Use of the app resulted in a 23% increase in crisis service engagement.
As another opportunity for collaboration with specialty mental health providers, if supported by future research, inpatient psychiatric units may begin to collect real-time data about dynamic changes in suicidal ideation during hospitalization to characterize risk post-hospitalization (166). Primary care practices and/or community mental health providers could then provide more intensive care transitions for those at highest risk.
Future research should focus on identifying suicide risk within shorter timelines (e.g., within 30 days) and continue to consider more effective screening and risk reduction interventions for participants without technological literacy (141). Clinics should be ready for a layered approach to incorporating self-report data, electronic medical record (EMR) data harvesting/machine learning, and enhancing provider awareness through means such as the Implicit Suicidal Cognition Association Test (IAT) to make identification result in effective and timely intervention in the future (141). If a dynamic model (i.e., one that synthesizes data from multiple methods) turns out to be the most powerful suicide predictor, and interventions can be more targeted, primary care practices will need stronger data systems and population health capacities (see Box 9).
Box 9. Clinical preparation for future directions

Current standards of suicide prevention rely heavily on effective coordination between primary care medical teams and behavioral health colleagues, making it essential that local levels of behavioral health integration (Table 1) are considered by practices during implementation efforts.
This review describes the evidence behind prevention strategies: PCP education, screening, safety planning/lethal means reduction, care transitions, psychotherapy, and medication management. We discuss how practices can finance suicide prevention, support providers, enact suicide postvention, and prepare for future directions in suicide prevention at each level of primary care/behavioral health integration. Based on this review, future directions in improving primary care-based suicide prevention include (1) implementation of evidence-based strategies in real-world settings, (2) increasing coordination between behavioral health and medical teams, and (3) prioritization of workforce (not simply individual) wellness to foster the genuine clinician-patient connection.
We identified that the existing literature either suggests all-encompassing clinic change (e.g., the Zero Suicide model) or individual provider-level change [e.g. (12)] but many lacked practical implementation strategies for real-world clinics. Recent literature shows that when social work is embedded into primary care practices, patients receive more rapid behavioral health treatment (167). Suicide prevention cannot wait for practices to adopt increasing levels of behavioral health integration, especially financial incentives are lacking. This review augments the existing literature by making implementation suggestions for practices based on level of current BH integration. The differences in training and implementation for practices with different levels of integration are vital. For example, with informal coordination, PCPs or adjacent staff will need the time and skills to complete the basics of suicide prevention (screening, safety assessment/lethal means reduction, care transitions and medication with access to rapid therapy referral). Alternatively, for fully integrated practices, embedded behavioral health providers may be able to take responsibility for care following a positive screen. With all levels of integration, seamless transitions between higher levels of care (i.e., emergency and inpatient) and outpatient primary care and behavioral health services should occur; however, roles may be performed by different staff, with a greater burden likely falling on PCPs for practices with lower behavioral health integration. Practices should place themselves on the spectrum of integration prior to implementing suicide prevention strategies to best assign and provide time for workload changes based on available staff. Future literature should focus more on the workings of the key relationships between PCPs, primary care practices, and behavioral health colleagues.
The literature indicates that greater integration of care between behavioral health and medical teams in real-world settings results in a range of benefits. Improving organization around care monitoring and delivery improves health outcomes. Without formalized integration, more suicide prevention work falls to PCPs. When feasible, we recommend integrated care and CoCM as part of population health management for depression (29) and suicide prevention (6, 12, 25, 30, 72, 102).
Greater integration of primary care and behavioral health care can enable efforts around primary care-based suicide prevention. On the one hand, some initiatives can be implemented regardless of the degree of integration, such as the provision of weekly drop-in DBT/CBT groups for at-risk patients identified in primary care, described in the Zero Suicide model (6, 90). By contrast, team-based approaches may facilitate clear designation of roles among the team, reducing PCP burden. Clinic models that track and respond to population health needs are more likely to have capacity to increase patient engagement, integrate new methods of screening (e.g., through application of machine learning algorithms to EMR data), and coordinate with behavioral health providers for monitoring of individuals at risk.
Finally, prioritizing workforce wellness to foster genuine clinician-patient connection is needed to support suicide prevention efforts. Without appropriate preparation and support, PCPs may under- or over-react to discussions about suicide. Suicide prevention requires staff and PCPs to have the emotional and temporal space to be present with patients. Providers and staff also deserve their own behavioral health support. Strategies to create healthy work environments have been identified in the public health literature (115) and overlap with those identified in the suicide prevention literature (114). Clinics can focus on changing the work environment to enable providers to have time for suicide prevention strategies, and for reflection to sustain this work over time. Future research should further explore the effect of healthy work environments on the connections with at-risk patients using evidence-based prevention strategies.
This paper focused on closing the gap in the current suicide prevention literature regarding behavioral health/medical interface, building on established knowledge. Limitations of this work include those of a narrative review including that the number of articles considered were not tracked and the strength/risk of bias of included articles were not evaluated. However, articles with strong methodologies including clinical guidelines, systematic reviews, and studies of novel primary care-based interventions were targeted for inclusion.
Extensive literature exists on the effective primary care-based screening of suicide risk, intervention, support for PCPs, and future directions for primary care-based suicide prevention. Current challenges in the field include the need for improved identification and treatment of those at risk and suboptimal funding incentives for suicide prevention care. This review represents a novel contribution to the literature by describing the ways suicide prevention strategies can be implemented in the primary care setting at different levels of behavioral health care integration (informal coordination, co-location, and integration). Given the importance of genuine connection for suicide prevention, we suggest that principles of workplace wellness be adopted to prevent staff burnout as suicide prevention becomes part of everyday practice workflow. This review highlights the need for more literature on real-world implementation focusing on how PCPs and behavioral health providers interact and the need for policy and financial strategies to incentivize greater primary care/behavioral health integration. While primary care practices should not wait for broad policy changes to implement elements of suicide prevention, we recommend that work toward more integrated practices is aligned with suicide prevention improvement. Investing in suicide prevention is an investment in saving lives as well as the basic tenets of good care; strategies needed for suicide prevention help practices connect better with patients and become more responsive to provider needs.
MS researched, wrote, and edited the manuscript. CL researched and edited the manuscript. DD and HH provided conceptual guidance and edited the manuscript. HH provided additional support tracking references. All authors contributed to the article and approved the submitted version.
This work was supported in part by the Four Pines Fund, a private fund focusing on suicide prevention.
MS has received support for one article in an MDEdge Child Psychiatry Consultation column on suicide prevention in primary care. CL has received consulting fees from Aetna Inc., CVS Health, and Lyra Health and HH has received research funding from Humana Inc.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Xu J, Murphy S, Kochanek K, Arias E. Mortality in the United States, 2015. National Center for Health Statistics Data Brief 2016 Available online: https://www.cdc.gov/nchs/products/databriefs/db267.htm (accessed September 8, 2021).
2. Curtin SC, Warner M, Hedegaard H. Increase in Suicide in the United States, 1999–2014. NCHS Data Brief. (2016) 1–8.
3. National Institute of Mental Health: Suicide Available online at: https://www.nimh.nih.gov/health/statistics/suicide (accessed August 15, 2021).
4. Luoma JB, Martin CE, Pearson JL. Contact with mental health and primary care providers before suicide: a review of the evidence. Am J Psychiatry. (2002) 159:909–16. doi: 10.1176/appi.ajp.159.6.909
5. Grumet JG, Hogan M, Chu A, Covington D, Johnson K. Compliance Standards Pave the Way for Reducing Suicide in Health Care Systems. J Health Care Compliance. (2019) 21:17–26.
6. Mann JJ, Michel CA, Auerbach RP. Improving suicide prevention through evidence-based strategies: a systematic review. Am J Psychiatry. (2021) 178:611–24. doi: 10.1176/appi.ajp.2020.20060864
7. Coffey CE. Building a system of perfect depression care in behavioral health. Jt Comm J Qual Patient Saf. (2007) 33:193–9. doi: 10.1016/S1553-7250(07)33022-5
8. SAMHSA-HRSA Center for Integrated Health Solutions. “CIHS' Standard Framework for Levels of Integrated Healthcare.” National Council for Mental Wellbeing, SAMHSA-HRSA Center for Integrated Health Solutions. (2020). Available online at: https://www.thenationalcouncil.org/wp-content/uploads/2020/01/CIHS_Framework_Final_charts.pdf?daf=375ateTbd56. (accessed August 15, 2021).
9. Szanto K, Kalmar S, Hendin H, Rihmer Z, Mann JJ, A suicide prevention program in a region with a very high suicide rate. Arch Gen Psychiatry. (2007) 64:914–20. doi: 10.1001/archpsyc.64.8.914
10. Feldman MD, Franks P, Duberstein PR, Vannoy S, Epstein R, Kravitz RL. Let's not talk about it: suicide inquiry in primary care. Ann Fam Med. (2007) 5:412–8. doi: 10.1370/afm.719
11. Mann JJ, Apter A, Bertolote J, Beautrais A, Currier D, Haas A, et al. Suicide prevention strategies: a systematic review. Jama. (2005) 294:2064–74. doi: 10.1001/jama.294.16.2064
12. McDowell AK, Lineberry TW, Bostwick JM. Practical suicide-risk management for the busy primary care physician. Mayo Clin Proc. (2011) 86:792–800. doi: 10.4065/mcp.2011.0076
13. Okolie C, Dennis M, Simon Thomas E, John A, A systematic review of interventions to prevent suicidal behaviors and reduce suicidal ideation in older people. Int Psychogeriatr. (2017) 29:1801–24. doi: 10.1017/S1041610217001430
14. Ramberg IL, Di Lucca MA, Hadlaczky G. The impact of knowledge of suicide prevention and work experience among clinical staff on attitudes towards working with suicidal patients and suicide prevention. Int J Environ Res Public Health. (2016) 13:195. doi: 10.3390/ijerph13020195
15. Roskar S, Podlesek A, Zorko M, Tavcar R, Dernovsek MZ, Groleger U, et al. Effects of training program on recognition and management of depression and suicide risk evaluation for Slovenian primary-care physicians: follow-up study. Croat Med J. (2010) 51:237–42. doi: 10.3325/cmj.2010.51.237
16. Rihmer Z, Belsö N, Kalmár S. Antidepressants and suicide prevention in Hungary. Acta Psychiatr Scand. (2001) 103:238–9. doi: 10.1034/j.1600-0447.2001.103003238.x
17. Rutz W, von Knorring L, Wålinder J. Frequency of suicide on Gotland after systematic postgraduate education of general practitioners. Acta Psychiatr Scand. (1989) 80:151–4. doi: 10.1111/j.1600-0447.1989.tb01318.x
18. Rutz W, von Knorring L, Wålinder J. Long-term effects of an educational program for general practitioners given by the Swedish Committee for the Prevention and Treatment of Depression. Acta Psychiatr Scand. (1992) 85:83–8. doi: 10.1111/j.1600-0447.1992.tb01448.x
19. Hegerl U, Mergl R, Havers I, Schmidtke A, Lehfeld H, Niklewski G, et al. Sustainable effects on suicidality were found for the Nuremberg alliance against depression. Eur Arch Psychiatry Clin Neurosci. (2010) 260:401–6. doi: 10.1007/s00406-009-0088-z
20. Siu AL, Bibbins-Domingo K, Grossman DC, Baumann LC, Davidson KW, Ebell M, et al. Screening for Depression in Adults: US Preventive Services Task Force Recommendation Statement. Jama. (2016) 315:380–7. doi: 10.1001/jama.2015.18392
21. Zuckerbrot RA, Cheung A, Jensen PS, Stein REK, Laraque D. Guidelines for Adolescent Depression in Primary Care (GLAD-PC): Part I. Practice Preparation, Identification, Assessment, and Initial Management. Pediatrics. (2018) 141:e20174081. doi: 10.1542/peds.2017-4081
22. LeFevre ML. Screening for suicide risk in adolescents, adults, and older adults in primary care: U. S Preventive Services Task Force recommendation statement Ann Intern Med. (2014) 160:719–26. doi: 10.7326/M14-0589
23. Zalsman G, Hawton K, Wasserman D, van Heeringen K, Arensman E, Sarchiapone M, et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry. (2016) 3:646–59. doi: 10.1016/S2215-0366(16)30030-X
24. Nelson HD, Denneson LM, Low AR, Bauer BW, O'Neil M, Kansagara D, et al. Suicide risk assessment and prevention: a systematic review focusing on veterans. Psychiatr Serv. (2017) 68:1003–15. doi: 10.1176/appi.ps.201600384
25. Raue PJ, Ghesquiere AR, Bruce ML. Suicide risk in primary care: identification and management in older adults. Curr Psychiatry Rep. (2014) 16:466. doi: 10.1007/s11920-014-0466-8
26. Horowitz L, Ballard E, Teach SJ, Bosk A, Rosenstein DL, Joshi P, et al. Feasibility of screening patients with nonpsychiatric complaints for suicide risk in a pediatric emergency department: a good time to talk? Pediatr Emerg Care. (2010) 26:787–92. doi: 10.1097/PEC.0b013e3181fa8568
27. Horowitz LM, Mournet AM, Lanzillo E, He JP, Powell DS, Ross AM, et al. Screening pediatric medical patients for suicide risk: is depression screening enough? J Adolesc Health. (2021) 68:1183–8. doi: 10.1016/j.jadohealth.2021.01.028
28. Uebelacker LA, German NM, Gaudiano BA, Miller IW. Patient health questionnaire depression scale as a suicide screening instrument in depressed primary care patients: a cross-sectional study. Prim Care Companion CNS Disord. (2011) 13:PCC.10m01027. doi: 10.4088/PCC.10m01027
29. Bostwick JM, Rackley S. Addressing suicidality in primary care settings. Curr Psychiatry Rep. (2012) 14:353–9. doi: 10.1007/s11920-012-0286-7
30. Weber AN, Michail M, Thompson A, Fiedorowicz JG. Psychiatric Emergencies: Assessing and Managing Suicidal Ideation. Med Clin North Am. (2017) 101:553–71. doi: 10.1016/j.mcna.2016.12.006
31. WHO. Preventing Suicide: A Global Imperative. (2014). Available from: https://apps.who.int/iris/bitstream/handle/10665/131056/9789241564779_eng.pdf?sequence=1. (accessed August 8, 2021).
32. Gensichen J, Teising A, König J, Gerlach FM, Petersen JJ. Predictors of suicidal ideation in depressive primary care patients. J Affect Disord. (2010) 125:124–7. doi: 10.1016/j.jad.2009.12.008
33. Ramchand R, Gordon JA, Pearson JL. Trends in Suicide Rates by Race and Ethnicity in the United States. JAMA Netw Open. (2021) 4:e2111563. doi: 10.1001/jamanetworkopen.2021.11563
34. Ivey-Stephenson AZ, Crosby AE, Hoenig JM, Gyawali S, Park-Lee E, Hedden SL. Suicidal Thought sand Behaviors Among Adults Aged ≥18 Years — United States, 2015–2019. MMWR Surveill Summ. (2022)71:1–19 Available online at: https://www.cdc.gov/mmwr/volumes/71/ss/ss7101a1.htm. (accessed January 23, 2022). doi: 10.15585/mmwr.ss7101a1
35. Henry Ford Zero Suicide Prevention Guidelines. Henry Ford Health System. 2001, (2018). Available online at: https://cdphe.colorado.gov/sites/cdphe/files/2021-05/zero_suicide_guidelines_final_feb_2019.pdf. (accessed October 9, 2021).
36. National Action Alliance for Suicide Prevention: Transforming Health Systems Initiative Work Group. Recommended standard care for people with suicide risk: Making health care suicide safe. Washington, DC: Education Development Center, Inc. (2018). Available online at: https://theactionalliance.org/sites/default/files/action_alliance_recommended_standard_care_final.pdf. (accessed August 8, 2021).
37. O'Connor E, Gaynes BN, Burda BU, Soh C, Whitlock EP. Screening for and treatment of suicide risk relevant to primary care: a systematic review for the U. s preventive services task force. Ann Intern Med. (2013) 158:741–54. doi: 10.7326/0003-4819-158-10-201305210-00642
38. Kim S, Lee HK, Lee K. Which PHQ-9 items can effectively screen for suicide? machine learning approaches. Int J Environ Res Public Health. (2021) 18:3339. doi: 10.3390/ijerph18073339
39. Bauer AM, Chan YF, Huang H, Vannoy S, Unützer J. Characteristics, management, and depression outcomes of primary care patients who endorse thoughts of death or suicide on the PHQ-9. J Gen Intern Med. (2013) 28:363–9. doi: 10.1007/s11606-012-2194-2
40. Denneson LM, Corson K, Helmer DA, Bair MJ, Dobscha SK. Mental health utilization of new-to-care Iraq and Afghanistan Veterans following suicidal ideation assessment. Psychiatry Res. (2014) 217:147–53. doi: 10.1016/j.psychres.2014.03.017
41. Mackelprang JL, Bombardier CH, Fann JR, Temkin NR, Barber JK, Dikmen SS. Rates and predictors of suicidal ideation during the first year after traumatic brain injury. Am J Public Health. (2014) 104:e100–7. doi: 10.2105/AJPH.2013.301794
42. Coleman KJ, Johnson E, Ahmedani BK, Beck A, Rossom RC, Shortreed SM, et al. Predicting Suicide Attempts for Racial and Ethnic Groups of Patients During Routine Clinical Care. Suicide Life Threat Behav. (2019) 49:724–34. doi: 10.1111/sltb.12454
43. Walker J, Waters RA, Murray G, Swanson H, Hibberd CJ, Rush RW, et al. Better off dead: suicidal thoughts in cancer patients. J Clin Oncol. (2008) 26:4725–30. doi: 10.1200/JCO.2007.11.8844
44. Louzon SA, Bossarte R, McCarthy JF, Katz IR. Does suicidal ideation as measured by the PHQ-9 predict suicide among VA patients? Psychiatr Serv. (2016) 67:517–22. doi: 10.1176/appi.ps.201500149
45. Razykov I, Hudson M, Baron M, Thombs BD. Utility of the patient health questionnaire-9 to assess suicide risk in patients with systemic sclerosis. Arthritis Care Res. (2013) 65:753–8. doi: 10.1002/acr.21894
46. Razykov I, Ziegelstein RC, Whooley MA, Thombs BD. The PHQ-9 versus the PHQ-8–is item 9 useful for assessing suicide risk in coronary artery disease patients? Data from the Heart and Soul Study. J Psychosom Res. (2012) 73:163–8. doi: 10.1016/j.jpsychores.2012.06.001
47. Mournet AM, Smith JT, Bridge JA, Boudreaux ED, Snyder DJ, Claassen CA, et al. Limitations of screening for depression as a proxy for suicide risk in adult medical inpatients. J Acad Consult Liaison Psychiatry. (2021) 62:413–20. doi: 10.1016/j.jaclp.2021.02.002
48. Horowitz LM, Snyder D, Ludi E, Rosenstein DL, Kohn-Godbout J, Lee L, et al. Ask suicide-screening questions to everyone in medical settings: the asQ'em quality improvement project. Psychosomatics. (2013) 54:239–47. doi: 10.1016/j.psym.2013.01.002
49. Dube P, Kurt K, Bair MJ, Theobald D, Williams LS. The p4 screener: evaluation of a brief measure for assessing potential suicide risk in 2 randomized effectiveness trials of primary care and oncology patients. Prim Care Companion J Clin Psychiatry. (2010)12:PCC.10m00978. doi: 10.4088/PCC.10m00978blu
50. Aguinaldo LD, Sullivant S, Lanzillo EC, Ross A, He JP, Bradley-Ewing A, et al. Validation of the ask suicide-screening questions (ASQ) with youth in outpatient specialty and primary care clinics. Gen Hosp Psychiatry. (2021) 68:52–8. doi: 10.1016/j.genhosppsych.2020.11.006
51. Horowitz LM, Bridge JA, Teach SJ, Ballard E, Klima J, Rosenstein DL, et al. Ask Suicide-Screening Questions (ASQ): a brief instrument for the pediatric emergency department. Arch Pediatr Adolesc Med. (2012) 166:1170–6. doi: 10.1001/archpediatrics.2012.1276
52. Horowitz LM, Snyder DJ, Boudreaux ED, He JP, Harrington CJ, Cai J, et al. Validation of the Ask Suicide-Screening Questions for adult medical inpatients: a brief tool for all ages. Psychosomatics. (2020) 61:713–22. doi: 10.1016/j.psym.2020.04.008
53. National Institute of Mental Health. Ask Suicide-Screening Questions (ASQ) Toolkit. Available online at: https://www.nimh.nih.gov/research/research-conducted-at-nimh/asq-toolkit-materials. (accessed August 8, 2021)
54. Roaten K, Horowitz LM, Bridge JA, Goans CRR, McKintosh C, Genzel R, et al. Universal pediatric suicide risk screening in a health care system: 90,000 patient encounters. J Acad Consult Liaison Psychiatry. (2021) 62:421–9. doi: 10.1016/j.jaclp.2020.12.002
55. Posner K, Brown GK, Stanley B, Brent DA, Yershova KV, Oquendo MA, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. (2011) 168:1266–77. doi: 10.1176/appi.ajp.2011.10111704
56. Richards JE, Whiteside U, Ludman EJ, Pabiniak C, Kirlin B, Hidalgo R, et al. Understanding why patients may not report suicidal ideation at a health care visit prior to a suicide attempt: a qualitative study. Psychiatr Serv. (2019) 70:40–5. doi: 10.1176/appi.ps.201800342
57. McGlynn EA, Asch SM, Adams J, Keesey J, Hicks J, DeCristofaro A, et al. The quality of health care delivered to adults in the United States. N Engl J Med. (2003) 348:2635–45. doi: 10.1056/NEJMsa022615
58. Hepner KA, Rowe M, Rost K, Hickey SC, Sherbourne CD, Ford DE, et al. The effect of adherence to practice guidelines on depression outcomes. Ann Intern Med. (2007) 147:320–9. doi: 10.7326/0003-4819-147-5-200709040-00007
59. Fleming MF, Manwell LB, Barry KL, Johnson K. At-risk drinking in an HMO primary care sample: prevalence and health policy implications. Am J Public Health. (1998) 88:90–3. doi: 10.2105/AJPH.88.1.90
60. Fleming MF. Screening and brief intervention in primary care settings. Alcohol Res Health. (2004) 28:57–62.
61. USPSTF Final Recommendation Statement. Unhealthy Alcohol Use in Adolescents and Adults: Screening and Behavioral Counseling Interventions. (2018). Available online at: https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/unhealthy-alcohol-use-in-adolescents-and-adults-screening-and-behavioral-counseling-interventions. (accessed October 16, 2021).
62. Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on early detection of persons with harmful alcohol consumption–II. Addiction. (1993) 88:791–804. doi: 10.1111/j.1360-0443.1993.tb02093.x
63. Patel AK, Balasanova AA. Treatment of alcohol use disorder. Jama. (2021) 325:596. doi: 10.1001/jama.2020.2012
64. Richards JE, Boggs JM, Rowhani-Rahbar A, Kuo E, Betz ME, Bobb JF, et al. Patient-reported firearm access prior to suicide death. JAMA Netw Open. (2022) 5:e2142204. doi: 10.1001/jamanetworkopen.2021.42204
65. Suicide Prevention Resource Center. Suicide Assessment Five-Step Evaluation Triage SAFE-T Pocket Card. (2009). Available online at: https://www.sprc.org/resources-programs/suicide-assessment-five-step-evaluation-and-triage-safe-t-pocket-card. (accessed September 14, 2021).
66. Rudd MD, Berman AL, Joiner TE. Jr., Nock MK, Silverman MM, Mandrusiak M, et al. Warning signs for suicide: theory, research, and clinical applications. Suicide Life Threat Behav. (2006) 36:255–62. doi: 10.1521/suli.2006.36.3.255
67. National Institute of Mental Health. COVID-19: Adult Suicide Risk Screening Pathway. Available online at: https://www.nimh.nih.gov/sites/default/files/documents/research/research-conducted-at-nimh/asq-toolkit-materials/inpatient/pdfs/covid-19_adult_suicide_risk_screening_pathway.pdf (accessed August 15, 2021).
68. Stanley B, Brown GK. Safety planning intervention: a brief intervention to mitigate suicide risk. Cogn Behav Pract. (2012) 19:256–64. doi: 10.1016/j.cbpra.2011.01.001
69. Brown GK, Ten Have T, Henriques GR, Xie SX, Hollander JE, Beck AT. Cognitive therapy for the prevention of suicide attempts: a randomized controlled trial. JAMA. (2005) 294:563–70. doi: 10.1001/jama.294.5.563
70. Stanley B, Brown G, Brent DA, Wells K, Poling K, Curry J, et al. Cognitive-behavioral therapy for suicide prevention (CBT-SP): treatment model, feasibility, and acceptability. J Am Acad Child Adolesc Psychiatry. (2009) 48:1005–13. doi: 10.1097/CHI.0b013e3181b5dbfe
71. Stanley B, Brown G. Safety planning intervention: Brief instructions. Washington, D.C.: United States Department of Veterans Affairs. Available from: https://www.mentalhealth.va.gov/docs/VA_Safety_planning_manual.doc. (accessed January 24, 2022).
72. Brodsky BS, Spruch-Feiner A, Stanley B. The zero suicide model: applying evidence-based suicide prevention practices to clinical care. Front Psychiatry. (2018) 9:33. doi: 10.3389/fpsyt.2018.00033
73. Bryan CJ, Mintz J, Clemans TA, Leeson B, Burch TS, Williams SR, et al. Effect of crisis response planning vs. contracts for safety on suicide risk in US Army Soldiers: A randomized clinical trial. J Affect Disord. (2017) 212:64–72. doi: 10.1016/j.jad.2017.01.028
74. Milner A, Spittal MJ, Kapur N, Witt K, Pirkis J, Carter G. Mechanisms of brief contact interventions in clinical populations: a systematic review. BMC Psychiatry. (2016) 16:194. doi: 10.1186/s12888-016-0896-4
75. Harvard School of Public Health (HSPH). Lethal Means Counseling and Means Matter: How Do Most People Commonly Complete Suicide. Available online at: https://www.hsph.harvard.edu/means-matter/basic-suicide-facts/how/. (accessed October 8, 2021).
76. Owens D, Horrocks J, House A. Fatal and non-fatal repetition of self-harm. Systematic review. Br J Psychiatry. (2002) 181:193–9. doi: 10.1192/bjp.181.3.193
77. Gunnell D, Eddleston M. Suicide by intentional ingestion of pesticides: a continuing tragedy in developing countries. Int J Epidemiol. (2003) 32:902–9. doi: 10.1093/ije/dyg307
78. Gunnell D, Fernando R, Hewagama M, Priyangika WD, Konradsen F, Eddleston M. The impact of pesticide regulations on suicide in Sri Lanka. Int J Epidemiol. (2007) 36:1235–42. doi: 10.1093/ije/dym164
79. Kreitman N. The coal gas story. United Kingdom suicide rates, 1960-71. Br J Prev Soc Med. (1976) 30:86–93. doi: 10.1136/jech.30.2.86
80. Hawton K. United Kingdom legislation on pack sizes of analgesics: background, rationale, and effects on suicide and deliberate self-harm. Suicide Life Threat Behav. (2002) 32:223–9. doi: 10.1521/suli.32.3.223.22169
81. Educational Development Center (EDC) Zero Suicide Institute. Counseling on Access to Lethal Means (CALM) Course Description. (2019). Available online at: https://zerosuicidetraining.edc.org/enrol/index.php?id=20. (accessed September 25, 2021).
82. Chung DT, Ryan CJ, Hadzi-Pavlovic D, Singh SP, Stanton C, Large MM. Suicide rates after discharge from psychiatric facilities: a systematic review and meta-analysis. JAMA Psychiatry. (2017) 74:694–702. doi: 10.1001/jamapsychiatry.2017.1044
83. Landes SJ, Kirchner JE, Areno JP, Reger MA, Abraham TH, Pitcock JA, et al. Adapting and implementing Caring Contacts in a Department of Veterans Affairs emergency department: a pilot study protocol. Pilot Feasibility Stud. (2019) 5:115. doi: 10.1186/s40814-019-0503-9
84. Motto JA. Suicide prevention for high-risk persons who refuse treatment. Suicide Life Threat Behav. (1976) 6:223–30.
85. Motto JA, Bostrom AG, A randomized controlled trial of postcrisis suicide prevention. Psychiatr Serv. (2001) 52:828–33. doi: 10.1176/appi.ps.52.6.828
86. Carter GL, Clover K, Whyte IM, Dawson AH, D'Este C. Postcards from the EDge project: randomised controlled trial of an intervention using postcards to reduce repetition of hospital treated deliberate self-poisoning. Bmj. (2005) 331:805. doi: 10.1136/bmj.38579.455266.E0
87. Carter GL, Clover K, Whyte IM, Dawson AH, D'Este C. Postcards from the EDge: 24-month outcomes of a randomised controlled trial for hospital-treated self-poisoning. Br J Psychiatry. (2007) 191:548–53. doi: 10.1192/bjp.bp.107.038406
88. Hassanian-Moghaddam H, Sarjami S, Kolahi AA, Carter GL. Postcards in Persia: randomised controlled trial to reduce suicidal behaviours 12 months after hospital-treated self-poisoning. Br J Psychiatry. (2011) 198:309–16. doi: 10.1192/bjp.bp.109.067199
89. Slee N, Garnefski N, van der Leeden R, Arensman E, Spinhoven P. Cognitive-behavioural intervention for self-harm: randomised controlled trial. Br J Psychiatry. (2008) 192:202–11. doi: 10.1192/bjp.bp.107.037564
90. Linehan MM, Comtois KA, Murray AM, Brown MZ, Gallop RJ, Heard HL, et al. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch Gen Psychiatry. (2006) 63:757–66. doi: 10.1001/archpsyc.63.7.757
91. Hatcher S, Sharon C, Parag V, Collins N. Problem-solving therapy for people who present to hospital with self-harm: Zelen randomised controlled trial. Br J Psychiatry. (2011) 199:310–6. doi: 10.1192/bjp.bp.110.090126
92. Bateman A, Fonagy P. Effectiveness of partial hospitalization in the treatment of borderline personality disorder: a randomized controlled trial. Am J Psychiatry. (1999) 156:1563–9. doi: 10.1176/ajp.156.10.1563
93. Guthrie E, Kapur N, Mackway-Jones K, Chew-Graham C, Moorey J, Mendel E, et al. Randomised controlled trial of brief psychological intervention after deliberate self-poisoning. Bmj. (2001) 323:135–8. doi: 10.1136/bmj.323.7305.135
94. Brown GK, Jager-Hyman S. Evidence-based psychotherapies for suicide prevention: future directions. Am J Prev Med. (2014)47(3 Suppl 2):S186–94. doi: 10.1016/j.amepre.2014.06.008
95. Stanley B, Mann JJ. The Need for Innovation in Health Care Systems to Improve Suicide Prevention. JAMA Psychiatry. (2020) 77:96–8. doi: 10.1001/jamapsychiatry.2019.2769
96. Müller-Oerlinghausen B, Lewitzka U. Lithium reduces pathological aggression and suicidality: a mini-review. Neuropsychobiology. (2010) 62:43–9. doi: 10.1159/000314309
97. Grunebaum MF, Galfalvy HC, Choo TH, Keilp JG, Moitra VK, Parris MS, et al. Ketamine for rapid reduction of suicidal thoughts in major depression: a midazolam-controlled randomized clinical trial. Am J Psychiatry. (2018) 175:327–35. doi: 10.1176/appi.ajp.2017.17060647
98. Meltzer HY, Alphs L, Green AI, Altamura AC, Anand R, Bertoldi A, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch Gen Psychiatry. (2003) 60:82–91. doi: 10.1001/archpsyc.60.1.82
99. Ross EL, Zuromski KL, Reis BY, Nock MK, Kessler RC, Smoller JW. Accuracy requirements for cost-effective suicide risk prediction among primary care patients in the US. JAMA Psychiatry. (2021) 78:642–50. doi: 10.1001/jamapsychiatry.2021.0089
100. Kessler RC. Clinical epidemiological research on suicide-related behaviors-where we are and where we need to go. JAMA Psychiatry. (2019) 76:777–8. doi: 10.1001/jamapsychiatry.2019.1238
101. Educational Development Center (EDC) Zero Suicide Institute. Financing Suicide Prevention. [Availableonline at: https://zerosuicide.edc.org/resources/key-resources/financing-suicide-prevention. (accessed 25 September 2021).
102. Mlinac ME, Smith RW, Siffert KJ, Richter LC, Steadman-Wood PL, Wetherell JL. Development of a suicide prevention toolkit for va home-based primary care teams. Home Healthc Now. (2021) 39:13–9. doi: 10.1097/NHH.0000000000000922
103. Unützer J, Harbin H, Schoenbaum M, Druss B. The Collaborative Care Model: An Approach for Integrating Physical and Mental Health Care in Medicaid Health Homes. Health Home Information Resource Center. (2013). Available online at: http://www.chcs.org/media/HH_IRC_Collaborative_Care_Model__052113_2.pdf. (accessed January 6s, 2022).
104. Corder JC. Population health management and ACOs: will they achieve their goals of better health and lower costs? Mo Med. (2018) 115:7–10.
105. Carlo AD, Unützer J, Ratzliff ADH, Cerimele JM. Financing for collaborative care - a narrative review. Curr Treat Options Psychiatry. (2018) 5:334–44. doi: 10.1007/s40501-018-0150-4
106. AIMS Center. Billing and Financing Behavioral Health Integration and Collaborative Care Available online at: https://aims.uw.edu/resources/billing-financing. (accessed 16 October, 2021).
107. Centers for Medicaid and Medicare Services MLN909432 Available online at: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/BehavioralHealthIntegration.pdf. (accessed October 16, 2021).
108. Dutheil F, Aubert C, Pereira B, Dambrun M, Moustafa F, Mermillod M, et al. Suicide among physicians and health-care workers: a systematic review and meta-analysis. PLoS Os. (2019) 14:e0226361. doi: 10.1371/journal.pone.0226361
109. Duarte D, El-Hagrassy MM, Couto TCE, Gurgel W, Fregni F, Correa H. Male and female physician suicidality: a systematic review and meta-analysis. JAMA Psychiatry. (2020) 77:587–97. doi: 10.1001/jamapsychiatry.2020.0011
110. Ye GY, Davidson JE, Kim K, Zisook S. Physician death by suicide in the United States: 2012-2016. J Psychiatr Res. (2021) 134:158–65. doi: 10.1016/j.jpsychires.2020.12.064
111. Sciolla AF, Haskins J, Chang CH, Kirshnit C, Rea M, Uppington J, et al. The suicide prevention, depression awareness, and clinical engagement program for faculty and residents at the University of California, Davis Health. Acad Psychiatry. (2021) 45:272–8. doi: 10.1007/s40596-021-01439-6
112. Richards JE, Hohl SD, Whiteside U, Ludman EJ, Grossman DC, Simon GE, et al. If You Listen, I Will Talk: the experience of being asked about suicidality during routine primary care. J Gen Intern Med. (2019) 34:2075–82. doi: 10.1007/s11606-019-05136-x
113. Abed Faghri NM, Boisvert CM, Faghri S. Understanding the expanding role of primary care physicians (PCPs) to primary psychiatric care physicians (PPCPs): enhancing the assessment and treatment of psychiatric conditions. Ment Health Fam Med. (2010) 7:17–25.
114. Turner K, Stapelberg NJ, Sveticic J, Dekker SW. Inconvenient truths in suicide prevention: Why a Restorative Just Culture should be implemented alongside a Zero Suicide Framework. Aust N Z J Psychiatry. (2020) 54:571–81. doi: 10.1177/0004867420918659
115. Lovejoy M, Kelly EL, Kubzansky LD, Berkman LF. Work redesign for the 21st century: promising strategies for enhancing worker well-being. Am J Public Health. (2021) 111:1787–95. doi: 10.2105/AJPH.2021.306283
116. Petrik ML, Miller BF, Matarazzo BB. Factors influencing suicide risk assessment and management in VA primary care clinics: a qualitative study of provider perspectives. Mil Behavs Health. (2018) 6:205–14. doi: 10.1080/21635781.2017.1379452
117. Katon WJ, Lin EH, Von Korff M, Ciechanowski P, Ludman EJ, Young B, et al. Collaborative care for patients with depression and chronic illnesses. N Engl J Med. (2010) 363:2611–20. doi: 10.1056/NEJMoa1003955
118. Alexander DA, Klein S, Gray NM, Dewar IG, Eagles JM. Suicide by patients: questionnaire study of its effect on consultant psychiatrists. BMJ. (2000) 320:1571–4. doi: 10.1136/bmj.320.7249.1571
119. Arancibia M, Martínez-Aguayo JC, Madrid E. Coping with a patient's suicide: the impact on physicians. Medwave. (2017) 17:e6986. doi: 10.5867/medwave.2017.06.6986
120. Midence K, Gregory S, Stanley R. The effects of patient suicide on nursing staff. J Clin Nurs. (1996) 5:115–20. doi: 10.1111/j.1365-2702.1996.tb00236.x
122. Saini P, Chantler K, While D, Kapur N. Do GPs want or need formal support following a patient suicide? a mixed methods study. Fam Pract. (2016) 33:414–20. doi: 10.1093/fampra/cmw040
123. Newman MC. The emotional impact of mistakes on family physicians. Arch Fam Med. (1996) 5:71–5. doi: 10.1001/archfami.5.2.71
124. Scott SD, Hirschinger LE, Cox KR, McCoig M, Brandt J, Hall LW. The natural history of recovery for the healthcare provider “second victim” after adverse patient events. Qual Saf Health Care. (2009) 18:325–30. doi: 10.1136/qshc.2009.032870
125. Joesten L, Cipparrone N, Okuno-Jones S, DuBose ER. Assessing the perceived level of institutional support for the second victim after a patient safety event. J Patient Saf. (2015) 11:73–8. doi: 10.1097/PTS.0000000000000060
126. Paparella S. Caring for the caregiver: moving beyond the finger pointing after an adverse event. J Emerg Nurs. (2011) 37:263–5. doi: 10.1016/j.jen.2011.01.001
127. Steeg S, Quinlivan L, Nowland R, Carroll R, Casey D, Clements C, et al. Accuracy of risk scales for predicting repeat self-harm and suicide: a multicentre, population-level cohort study using routine clinical data. BMC Psychiatry. (2018) 18:113. doi: 10.1186/s12888-018-1693-z
128. Scott SD, Hirschinger LE, Cox KR, McCoig M, Hahn-Cover K, Epperly KM, et al. Caring for our own: deploying a systemwide second victim rapid response team. Jt Comm J Qual Patient Saf. (2010) 36:233–40. doi: 10.1016/S1553-7250(10)36038-7
129. Al-Mateen CS, Jones K, Linker J, O'Keefe D, Cimolai V. Clinician response to a child who completes suicide. Child Adolesc Psychiatr Clin N Am. (2018) 27:621–35. doi: 10.1016/j.chc.2018.05.006
130. Denham CR, TRUST. The 5 rights of the second victim. J Patient Saf. (2007) 3:107–19. doi: 10.1097/01.jps.0000236917.02321.fd
131. Erlich MD, Rolin SA, Dixon LB, Adler DA, Oslin DW, Levine B, et al. Why we need to enhance suicide postvention: evaluating a survey of psychiatrists' behaviors after the suicide of a patient. J Nerv Ment Dis. (2017) 205:507–11. doi: 10.1097/NMD.0000000000000682
132. Castro-Ramirez F, Al-Suwaidi M, Garcia P, Rankin O, Ricard JR, Nock MK. Racism and poverty are barriers to the treatment of youth mental health concerns. J Clin Child Adolesc Psychol. (2021) 50:534–46. doi: 10.1080/15374416.2021.1941058
133. Lindsey MA, Sheftall AH, Xiao Y, Joe S. Trends of suicidal behaviors among high school students in the United States: 1991-2017. Pediatrics.(2019)144:e20191187. doi: 10.1542/peds.2019-1187
134. Bridge JA, Horowitz LM, Fontanella CA, Sheftall AH, Greenhouse J, Kelleher KJ, et al. Age-related racial disparity in suicide rates among US youths from 2001 through 2015. JAMA Pediatr. (2018) 172:697–9. doi: 10.1001/jamapediatrics.2018.0399
135. Hottes TS, Bogaert L, Rhodes AE, Brennan DJ, Gesink D. Lifetime prevalence of suicide attempts among sexual minority adults by study sampling strategies: a systematic review and meta-analysis. Am J Public Health. (2016) 106:e1–12. doi: 10.2105/AJPH.2016.303088a
136. Hunt IM, Richards N, Bhui K, Ibrahim S, Turnbull P, Halvorsrud K, et al. Suicide rates by ethnic group among patients in contact with mental health services: an observational cohort study in England and Wales. Lancet Psychiatry. (2021) 8:1083–93. doi: 10.1016/S2215-0366(21)00354-0
137. Franklin JC, Ribeiro JD, Fox KR, Bentley KH, Kleiman EM, Huang X, et al. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychol Bull. (2017) 143:187–232. doi: 10.1037/bul0000084
138. Shah R, Franks P, Jerant A, Feldman M, Duberstein P. Fernandez y, Garcia E, et al. The effect of targeted and tailored patient depression engagement interventions on patient-physician discussion of suicidal thoughts: a randomized control trial. J Gen Intern Med. (2014) 29:1148–54. doi: 10.1007/s11606-014-2843-8
139. Onnela JP. Opportunities and challenges in the collection and analysis of digital phenotyping data. Neuropsychopharmacology. (2021) 46:45–54. doi: 10.1038/s41386-020-0771-3
140. Kleiman EM, Turner BJ, Fedor S, Beale EE, Picard RW, Huffman JC, et al. Digital phenotyping of suicidal thoughts. Depress Anxiety. (2018) 35:601–8. doi: 10.1002/da.22730
141. Mou D, Kleiman EM, Nock MK. Proposed directions for suicide research: incorporating successful approaches from other disciplines. Br J Psychiatry. (2020) 217:659–60. doi: 10.1192/bjp.2020.58
142. Barnes LS, Ikeda RM, Kresnow MJ. Help-seeking behavior prior to nearly lethal suicide attempts. Suicide Life Threat Behav. (2001)32(1 Suppl):68–75. doi: 10.1521/suli.32.1.5.68.24217
143. Calear AL, Batterham PJ. Suicidal ideation disclosure: patterns, correlates and outcome. Psychiatry Res. (2019) 278:1–6. doi: 10.1016/j.psychres.2019.05.024
144. Glenn JJ, Werntz AJ, Slama SJ, Steinman SA, Teachman BA, Nock MK. Suicide and self-injury-related implicit cognition: a large-scale examination and replication. J Abnorm Psychol. (2017) 126:199–211. doi: 10.1037/abn0000230
145. Nock MK, Park JM, Finn CT, Deliberto TL, Dour HJ, Banaji MR. Measuring the suicidal mind: implicit cognition predicts suicidal behavior. Psychol Sci. (2010) 21:511–7. doi: 10.1177/0956797610364762
146. Busch KA, Fawcett J, Jacobs DG. Clinical correlates of inpatient suicide. J Clin Psychiatry. (2003) 64:14–9. doi: 10.4088/JCP.v64n0105
147. Kleiman EM, Turner BJ, Fedor S, Beale EE, Huffman JC, Nock MK. Examination of real-time fluctuations in suicidal ideation and its risk factors: Results from two ecological momentary assessment studies. J Abnorm Psychol. (2017) 126:726–38. doi: 10.1037/abn0000273
148. Randall JR, Rowe BH, Dong KA, Nock MK, Colman I. Assessment of self-harm risk using implicit thoughts. Psychol Assess. (2013) 25:714–21. doi: 10.1037/a0032391
149. Barak-Corren Y, Castro VM, Javitt S, Hoffnagle AG Dai Y, Perlis RH, et al. Predicting suicidal behavior from longitudinal electronic health records. Am J Psychiatry. (2017) 174:154–62. doi: 10.1176/appi.ajp.2016.16010077
150. Gibbons RD. deGruy FV. Without wasting a word: extreme improvements in efficiency and accuracy using Computerized Adaptive Testing for Mental Health Disorders (CAT-MH). Curr Psychiatry Rep. (2019) 21:67. doi: 10.1007/s11920-019-1053-9
151. Grunebaum MF, Mann JJ, Galfalvy HC, Gibbons RD. Computerized-adaptive vs. traditional ratings of depression and suicidal thoughts: an assay sensitivity pilot study in a ketamine clinical trial. Front Psychiatry. (2021) 12:602976. doi: 10.3389/fpsyt.2021.602976
152. Simon GE, Shortreed SM, Rossom RC, Beck A, Clarke GN, Whiteside U, et al. Effect of offering care management or online dialectical behavior therapy skills training vs usual care on self-harm among adult outpatients with suicidal ideation: a randomized clinical trial. JAMA. (2022) 327:630–8. doi: 10.1001/jama.2022.0423
153. Chandrashekar P. Do mental health mobile apps work: evidence and recommendations for designing high-efficacy mental health mobile apps. Mhealth. (2018) 4:6. doi: 10.21037/mhealth.2018.03.02
154. Bakker D, Kazantzis N, Rickwood D, Rickard N. Mental Health Smartphone Apps: review and evidence-based recommendations for future developments. JMIR Ment Health. (2016) 3:e7. doi: 10.2196/mental.4984
155. Chan S, Godwin H, Gonzalez A, Yellowlees PM, Hilty DM. Review of use and integration of mobile apps into psychiatric treatments. Curr Psychiatry Rep. (2017) 19:96. doi: 10.1007/s11920-017-0848-9
156. Fleming TM, Bavin L, Stasiak K, Hermansson-Webb E, Merry SN, Cheek C, et al. Serious games and gamification for mental health: current status and promising directions. Front Psychiatry. (2016) 7:215. doi: 10.3389/fpsyt.2016.00215
157. Wilks CR, Chu C, Sim D, Lovell J, Gutierrez P, Joiner T, et al. User engagement and usability of suicide prevention apps: systematic search in app stores and content analysis. JMIR Form Res. (2021) 5:e27018. doi: 10.2196/27018
158. Torous J, Lipschitz J, Ng M, Firth J. Dropout rates in clinical trials of smartphone apps for depressive symptoms: a systematic review and meta-analysis. J Affect Disord. (2020) 263:413–9. doi: 10.1016/j.jad.2019.11.167
159. Ng MM, Firth J, Minen M, Torous J. User engagement in mental health apps: a review of measurement, reporting, and validity. Psychiatr Serv. (2019) 70:538–44. doi: 10.1176/appi.ps.201800519
160. Baumel A, Muench F, Edan S, Kane JM. Objective user engagement with mental health apps: systematic search and panel-based usage analysis. J Med Internet Res. (2019) 21:e14567. doi: 10.2196/14567
161. Grist R, Porter J, Stallard P. Mental Health Mobile Apps for preadolescents and adolescents: a systematic review. J Med Internet Res. (2017) 19:e176. doi: 10.2196/jmir.7332
162. Wang K, Varma DS, Prosperi M, A systematic review of the effectiveness of mobile apps for monitoring and management of mental health symptoms or disorders. J Psychiatr Res. (2018) 107:73–8. doi: 10.1016/j.jpsychires.2018.10.006
163. Martinengo L, Van Galen L, Lum E, Kowalski M, Subramaniam M, Car J. Suicide prevention and depression apps' suicide risk assessment and management: a systematic assessment of adherence to clinical guidelines. BMC Med. (2019) 17:231. doi: 10.1186/s12916-019-1461-z
164. Koko app Available online at: https://www.kokocares.org/. (accessed January 6, 2022).
165. Jaroszewski AC, Morris RR, Nock MK. Randomized controlled trial of an online machine learning-driven risk assessment and intervention platform for increasing the use of crisis services. J Consult Clin Psychol. (2019) 87:370–9. doi: 10.1037/ccp0000389
166. Wang SB, Coppersmith DDL, Kleiman EM, Bentley KH, Millner AJ, Fortgang R, et al. A pilot study using frequent inpatient assessments of suicidal thinking to predict short-term postdischarge suicidal behavior. JAMA Netw Open. (2021) 4:e210591. doi: 10.1001/jamanetworkopen.2021.0591
167. Pfoh ER, Hohman JA, Alcorn K, Vakharia N, Rothberg MB. Linking primary care patients to mental health care via behavioral health social workers: a stepped-wedge study. Psychiatr Serv. 2022:appips202100322. doi: 10.1176/appi.ps.202100322
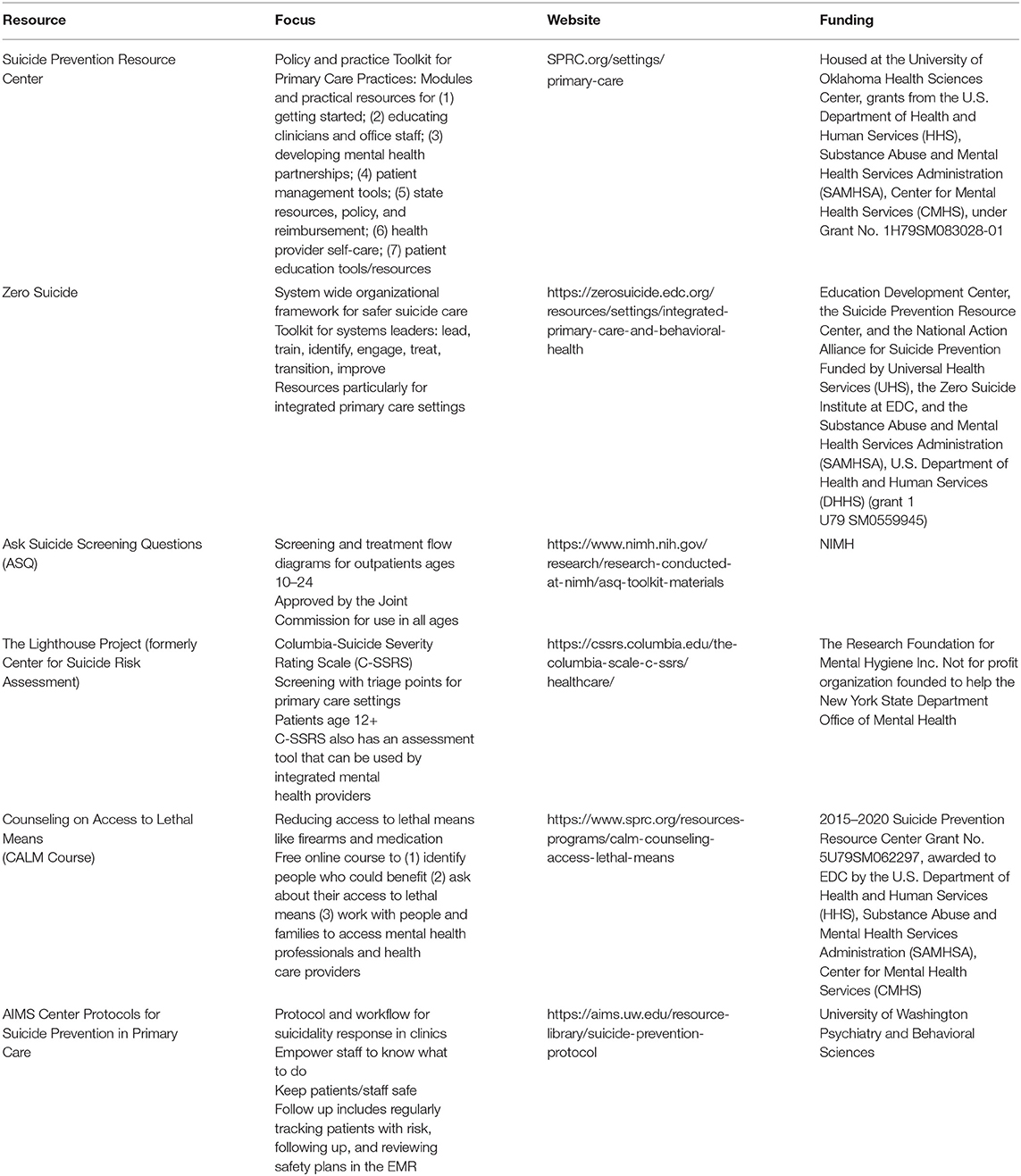
Appendix 1. Select tools for primary care practices.
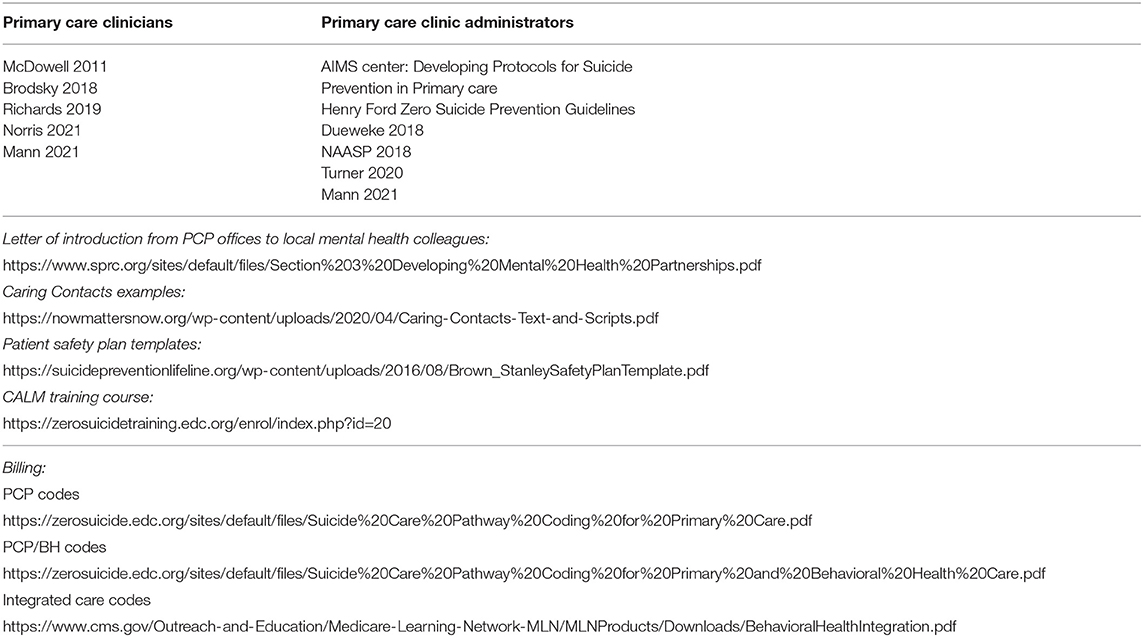
Appendix 2. Recommended reading and resources.
Keywords: suicide prevention, primary care, behavioral health integration, collaborative care, population health
Citation: Spottswood M, Lim CT, Davydow D and Huang H (2022) Improving Suicide Prevention in Primary Care for Differing Levels of Behavioral Health Integration: A Review. Front. Med. 9:892205. doi: 10.3389/fmed.2022.892205
Received: 08 March 2022; Accepted: 04 May 2022;
Published: 27 May 2022.
Edited by:
Dan Devoe, University of Calgary, CanadaReviewed by:
Harm Van Marwijk, Brighton and Sussex Medical School, United KingdomCopyright © 2022 Spottswood, Lim, Davydow and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Margaret Spottswood, bXNwb3R0c3dvb2RAY2hjYi5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.