
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
GENERAL COMMENTARY article
Front. Med., 24 May 2022
Sec. Intensive Care Medicine and Anesthesiology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.884942
This article is part of the Research TopicPost COVID-19: Analysing and Addressing the Challenges Faced by Patients Following Intensive Care Treatment for COVID-19View all 16 articles
 Meiling Deng1
Meiling Deng1 Wangyuan Zou1,2*
Wangyuan Zou1,2*A Commentary on
Lung Recruitment, Individualized PEEP, and Prone Position Ventilation for COVID-19-Associated Severe ARDS: A Single Center Observational Study
by Sang, L., Zheng, X., Zhao, Z., Zhong, M., Jiang, L., Huang, Y., Liu, X., Li, Y., and Zhang, D. (2021). Front. Med. 7:603943. doi: 10.3389/fmed.2020.603943
The worldwide outbreak of “coronavirus disease 2019” (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has topped 5,916,373 deaths with more than 420 million diagnosed cases as of 24 February 2022 (1). Patients with acute hypoxemic respiratory failure or acute respiratory distress syndrome (ARDS) used to be treated with oxygen and ventilation (2). Approximately 3.2% of patients with COVID-19 required intubation and invasive ventilation in mainland China (2).
Early application of prolonged prone position ventilation provides a survival advantage with expected lower mortality in patients with severe ARDS (3) and has been widely used in Wuhan for critically ill patients with COVID-19 by improving mechanics and gas exchange (2). However, prone position ventilation was associated with an increased safety risk of displacement or dislocation of the endotracheal tube due to the gravity and the tape getting damp from oral secretion (4), especially in prolonged prone ventilation and patients with severe COVID-19 infection. In view of this, it is prudent to avoid unnecessary displacement or dislocation of the endotracheal tube in prone-position-ventilated patients with COVID-19 in order to avoid adverse events and unnecessary exposure of the virus to the environment.
In our previous study, we applied a custom-designed prone position tube (PPT) (Figure 1A) for patients undergoing prone position surgery (Figure 1B) (4, 5). Unlike those traditional tubes and tube-securing devices, the PPT tube and the fixation device are integrated with the following advantages: (1) it is designed with a fixture that attaches to the tube to keep the sides of the cord firm; (2) the fixation method is more effective and easier to manage, and the fixing effect is more reliable; (3) once fixed, the binding cord will not be affected by the sterilizing fluid, blood, or fluids leaking from the mouth; (4) the tube is reinforced with a steel wire to prevent patients from biting the tube; (5) the displacement rate of the tube in our previous research was lower compared with that of the Haider Tube-Guard reported by Buckley et al. (4, 6). We found that the application of PPT could significantly reduce the incidence of tube displacement compared to the conventional endotracheal tube. The tube and fixation ensure safe ventilation and simultaneously do not interfere with the procedure in the mouth or the airway, and this tube will be particularly beneficial for patients with COVID-19 who require prolonged ventilation in the prone position.
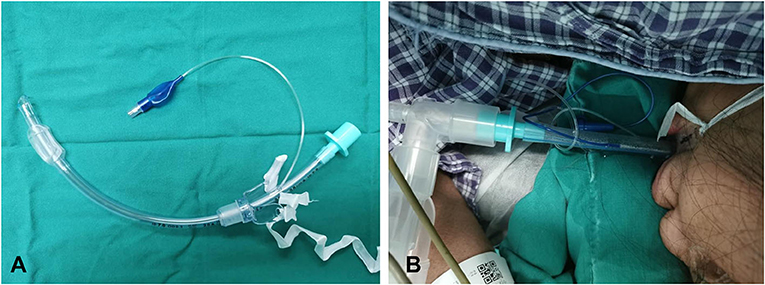
Figure 1. The prone position tube. (A) The prone position tube is designed as a whole unit with a fixture that is affixed to the tube to increase the stabilization. (B) The prone position tube was applied for a patient undergoing prone position surgery.
It is essential to guarantee a perfect hold of the prolonged prone position ventilation for the patients with COVID-19 to avoid possible displacement or dislocation of the endotracheal tube. According to our experience, the PPT can provide effective airway protection. Under the present emergency condition of COVID-19, we recommend that this PPT be used in prone position ventilation of patients with COVID-19.
MD and WZ wrote the paper. WZ revised the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by grants from the National Natural Science Foundation of China (81974172 ad 82171236 to WZ) and the Key Research and Development Program of Hunan Province (2021SK2018 to WZ).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Johns Hopkins University. 2019 Novel Coronavirus COVID-19 (2019-nCoV) Data Repository by Johns Hopkins CSSE. (2020). Available online at: https://www.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed February 24, 2022).
2. Meng L, Qiu H, Wan L, Ai Y, Xue Z, Guo Q, et al. Intubation and ventilation amid the COVID-19 outbreak: Wuhan's experience. Anesthesiology. (2020) 132:1317–32. doi: 10.1097/ALN.0000000000003296
3. Guérin C, Reignier J, Richard J-C, Beuret P, Gacouin A, Boulain T, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. (2013) 368:2159–68. doi: 10.1056/NEJMoa1214103
4. Zou W, Shao J, Liang X, Li L, He Z, Guo Q. A randomized comparison of the prone ventilation endotracheal tube versus the traditional endotracheal tube in adult patients undergoing prone position surgery. Sci Rep. (2017) 7:1769. doi: 10.1038/s41598-017-02006-6
5. Zou W, Zhang W, Li X, Guo Q. A randomized crossover comparison of the prone ventilation endotracheal tube versus the traditional endotracheal tube in pediatric patients undergoing prone position surgery. Paediatr Anaesth. (2013) 23:98–100. doi: 10.1111/pan.12068
6. Buckley JC, Brown AP, Shin JS, Rogers KM, Hoftman NN. A Comparison of the Haider Tube-Guard® endotracheal tube holder versus adhesive tape to determine if this novel device can reduce endotracheal tube movement and prevent unplanned extubation. Anesth Analg. (2016) 122:1439–43. doi: 10.1213/ane.0000000000001222
Keywords: COVID-19, prone position, endotracheal tube (ETT), ventilation, prone position tube (PPT)
Citation: Deng M and Zou W (2022) Commentary: Lung Recruitment, Individualized PEEP, and Prone Position Ventilation for COVID-19-Associated Severe ARDS: A Single Center Observational Study. Front. Med. 9:884942. doi: 10.3389/fmed.2022.884942
Received: 27 February 2022; Accepted: 15 April 2022;
Published: 24 May 2022.
Edited by:
Giuliana Scarpati, University of Salerno, ItalyReviewed by:
Sachit Anand, Kokilaben Dhirubhai Ambani Hospital and Medical Research Institute, IndiaCopyright © 2022 Deng and Zou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wangyuan Zou, d2FuZ3l1YW56b3VAY3N1LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.