 Tae-Hun Kim
Tae-Hun Kim Jung Won Kang3
Jung Won Kang3 Hye Won Lee
Hye Won Lee Myeong Soo Lee
Myeong Soo Lee
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med., 09 May 2022
Sec. Infectious Diseases: Pathogenesis and Therapy
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.884573
Background: Traditional, Complementary and Integrative Medicine (TCIM) has been reported to use for symptom management of coronavirus disease 2019 (COVID-19). The objective of this review was to identify the overall usage prevalence of TCIM interventions for COVID-19.
Methods: Surveys on the general population and observational studies on the COVID-19 patient chart review were located in the search of PubMed, EMBASE and Cochrane Central Register of Controlled Trials databases in September 2021. Observational studies, such as cross-sectional studies, surveys, cohort studies and hospital-based patient case reviews, published in any language, reporting the usage of TCIM in the patients with COVID-19 or the general population during the COVID-19 pandemic were included in this review. Data screening and extraction were performed independently by two reviewers. The reporting quality of the included studies was assessed with the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement. To conduct a meta-analysis of the usage prevalence of various TCIM interventions, the effect size of the proportion for each intervention was calculated with the inverse variance method. The main outcome was usage prevalence of TCIM interventions among patients with COVID-19 or the general population during the COVID-19 pandemic.
Results: A total of 62 studies were included in this review. The overall TCIM usage prevalence was estimated to be 0.64 (95% CI 0.54–0.73). The overall prevalence did not differ between the population-based survey (0.65, 95% CI 0.48–0.81) and the hospital-based patient case review (0.63, 95% CI 0.52–0.73). Statistical heterogeneity and comparatively low quality in reporting were observed, which should be cautiously considered when interpreting the results.
Conclusion: Various TCIM interventions were reported to be used with comparatively high frequency. Future international collaborative research might overcome the main limitation of this study, i.e., the heterogeneity of the included data.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=278452, identifier: CRD42021278452.
Coronavirus disease 2019 (COVID-19) is an acute upper respiratory tract infection which is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) newly identified in 2019 (1). Since the World Health Organization (WHO) declared a pandemic in March 2020, several variants have been appearing, and the pandemic continues. Treatment strategies have been gradually established based on accumulated clinical evidence for the acute treatment of COVID-19. In addition to the basic management principle that prioritizes the prevention of complications such as thrombosis, along with adequate oxygenation and hemodynamic support, antiviral agents such as remdesivir, antibody therapy and drug treatments such as dexamethasone are being used in clinical practice (2, 3). However, since knowledge about this disease is still incomplete and new mutated viruses continue to emerge, uncertainty is rising about the basis of treatment from a medical point of view. Additionally, symptoms that persist after the acute manifestation of COVID-19, called long COVID-19, should not be overlooked (4). Patients with severe clinical presentation of COVID-19 are likely to experience long-term respiratory system dysfunction or sequelae of complications, but the real problem is that a significant number of mild infections or asymptomatic COVID-19 patients have been presenting with long COVID symptoms for a long time (5). In addition, long COVID patients complain of symptoms of various spectra, such as fatigue, cognitive decline, respiratory difficulty, joint pain, loss of taste/smell and hair loss (4). From this perspective, a multidisciplinary approach is required for the prevention and management of COVID-19 from the acute stage through long COVID (3, 4).
Since the outbreak of COVID, Traditional, Complementary and Alternative Medicine (TCIM) has been adopted as an alternative strategy for the prevention and treatment of COVID-19 as the entire medical capacity of a country is mobilized at a national level to promote immunity and to protect against viral infection at both the national and individual levels. Clinical practice guidelines (CPGs) or therapeutic protocols for the management of COVID-19 have been published in various fields of TCIM, such as Traditional Chinese Medicine (TCM) (6, 7), Korean Medicine (8), and Ayurveda (9). In addition, according to a survey conducted on patients in quarantine in India, 25% of patients responded that they had experiences with TCIM-related products or home remedies (10). Judging from these data and recently published bibliometric studies (11–13). TCIM interventions are being used quite actively for the management of COVID-19 worldwide, although usage status might variations across countries might depending on the country's medical system. Considering each country's situation, reviewing the utilization prevalence of overall TCIM interventions by country and the utilization status of each intervention may provide insight into the impact of TCIM on global health in the COVID-19 pandemic period.
Therefore, we investigated the prevalence of TCIM use to prevent and treat COVID-19 around the world, identified the most frequently used specific TCIM treatments per country and suggested the overall proportion of CAM use worldwide to treat COVID-19 using systematic review methods.
This was a systematic review (SR) for observational studies that assessed the usage status of TCIM interventions worldwide. We located surveys of the general population to assess the usage status of TCIM interventions and hospital-based COVID patients' case review studies through electronic database searches. Overall and individual usage prevalence of diverse TCIM interventions were estimated through meta-analysis. This review protocol was registered in PROSPERO (https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=278452).
Review questions
1. How frequent are TCIM interventions used in the general population and COVID-19 patients worldwide?
2. How much is the difference in usage prevalence between different TCIM interventions?
We did not impose any limitations on the population if the study assessed the usage prevalence of TCIM interventions during the COVID-19 pandemic. Both healthy individuals and COVID-19 patients were included in this review.
In this review, we allowed any type of TCIM intervention based on the definition of the U.S. National Center for Complementary and Integrative Health (14). Interventions included nutrition (e.g., special diets, dietary supplements, herbs, probiotics, microbial-based therapies and botanical drugs), psychological treatment (e.g., meditation, hypnosis, music therapies, relaxation therapies, qigong, hypnotherapy, Feldenkrais method, Alexander technique, Pilates, Rolfing Structural Integration, and Trager psychophysical integration), physical therapies (e.g., acupuncture, massage and spinal manipulation), combinations such as psychological and physical methods (e.g., yoga, tai chi, dance therapies and some forms of art therapy), psychological and nutritional combinations (e.g., mindful eating), chiropractic and osteopathic manipulation or traditional medicine (e.g., Ayurvedic Medicine, Traditional Chinese Medicine, homeopathy, naturopathy and functional medicine).
We included observational studies, so most studies were not expected to have comparator groups. However, any kind of comparator intervention was allowed.
Usage prevalence of TCIM interventions among patients with COVID-19 or the general population during the COVID-19 pandemic was included.
Observational studies, such as cross-sectional studies, surveys, cohort studies and hospital-based patient case reviews, were included in this review.
Core databases, including PubMed, EMBASE and Cochrane Central Register of Controlled Trials (CENTRAL), were searched in September 2021. The search strategy was developed with COVID-19-related terms and keywords for TCIM for each database, and the PubMed search strategy was listed in the Supplementary Table 1.
Screening and selection of the studies for inclusion in this review were conducted manually by two authors (THK and SRJ) independently. Any disagreement was arbitrated by the third author (JWK). EndNote 20 (Philadelphia, PA) was used for the screening stage of this review. We uploaded a list of located publications and conducted a screening process with this software. The predefined extraction form included data regarding the type of study, population (healthy individuals or COVID-19 patients), type of TCIM interventions, country, time point for acquiring study data, information on the study population (age and sex), purpose of the usage of TCIM interventions and numbers of patients in hospital-based case reviews and survey respondents (numbers in the total population and those who used TCIM interventions).
For this review, observational patient case reviews for COVID-19 patients and surveys for the general population or COVID-19 patients were included. Therefore, items from the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement were selectively used for assessing the reporting quality of the included studies. We evaluated appropriateness of reporting for items including title and abstract, objectives, participants, variable, data sources, bias, study size, statistical methods, number of participants in each stage of the result section, result analysis, key results, limitations and funding (including conflicts of interest). Each item was evaluated with “A” if all the necessary points were appropriately suggested in the publication of the study and “I” if not. Two authors (THK and SRJ) independently assessed STROBE items and discussed them until they reached agreement.
To conduct a meta-analysis of the usage prevalence of various TCIM interventions, the effect size of the proportion for each intervention was calculated with the inverse variance method. When calculating the estimated proportion of TCIM usage, we used double arcsine transformation and back transformation methods, because some studies showed extreme proportions, such as close 0 or 1, which meant that the dataset was skewed and not normally distributed (15). A random effects model was adopted to calculate summary effect estimates of usage prevalence, because there could be potential clinical heterogeneity in the study methods and study population. Based on the study types (survey vs. hospital-based COVID patient case review), intervention types, study population (general population vs. hospitalized patients) and the country where the intervention was used, subgroup analysis was conducted. I2 statistics were used to assess statistical heterogeneity. In the subgroup analysis, the R2 index was calculated to quantify the amount of variance or how much of the total variance in the meta-analysis could be explained by the suspicious effect modifier (16). Publication bias was assessed through visual evaluation of funnel plots and Egger's test. The package “meta” and the function “metaprop” in R (ver 4.0.2) were used for meta-analysis of proportions in this study. The overall usage prevalence of TCIM interventions in each country was presented in the form of a world map using the “ggplot2” package.
From the electronic database search, a total of 62 studies were enrolled in this review (Figure 1) (10, 17–77). Thirty-nine studies were population-based surveys, and twenty-three studies were hospital-based COVID-19 patient case reviews. One study was a survey that included patient data from two regions, Hong Kong and mainland China, separately, so we analyzed the data separately (71). Twenty-two studies were conducted in China (27, 31–34, 37, 39, 40, 44, 47, 55, 62–65, 67, 69–73, 75–77), six in Saudi Arabia (18, 21–23, 25, 26), five in India (10, 41, 46, 60, 61), three in the United States (35, 42, 45) and three in Turkey (38, 49, 66), and these were the most frequent countries included in this review. Among the population-based survey studies, thirty-one were conducted through online surveys only (17, 18, 20, 22, 23, 25, 26, 28–31, 35, 42, 43, 45, 48–54, 57–62, 66, 68, 74), one was an in-person interview (56), three were telephone interviews (10, 21, 38), and two were both in-person and online surveys (19, 36). Among the included studies, usage status of the interventions, including TCM (n = 22) (27, 32–34, 37, 39, 40, 44, 47, 55, 63–65, 67, 69–73, 75–77), functional food (supplements) or herbs (n = 20) (17–24, 29, 36, 38, 43, 49–52, 57–59), mind-body practice or spiritual practice (n = 9) (28, 35, 42, 45, 48, 54, 60, 61, 74), Ayurveda (n = 2) (10, 41), homeopathy (n = 1) (46) and Ethiopian traditional medicine (n = 1) (56) was suggested. Only one study was conducted in 2021 (57). Most of the data for surveys or patient chart reviews were collected during 2020. In approximately half of the studies, TCIM interventions were used for prophylactic purposes (n = 28) (17–20, 22, 23, 25, 26, 28, 31, 35, 36, 38, 41, 42, 45, 48–54, 59, 61, 62, 66, 74), and the other half were used for therapeutic purposes (n = 27) (21, 24, 27, 32–34, 37, 39, 40, 44, 46, 47, 55, 58, 63–65, 67, 69–73, 75–77) (Table 1).
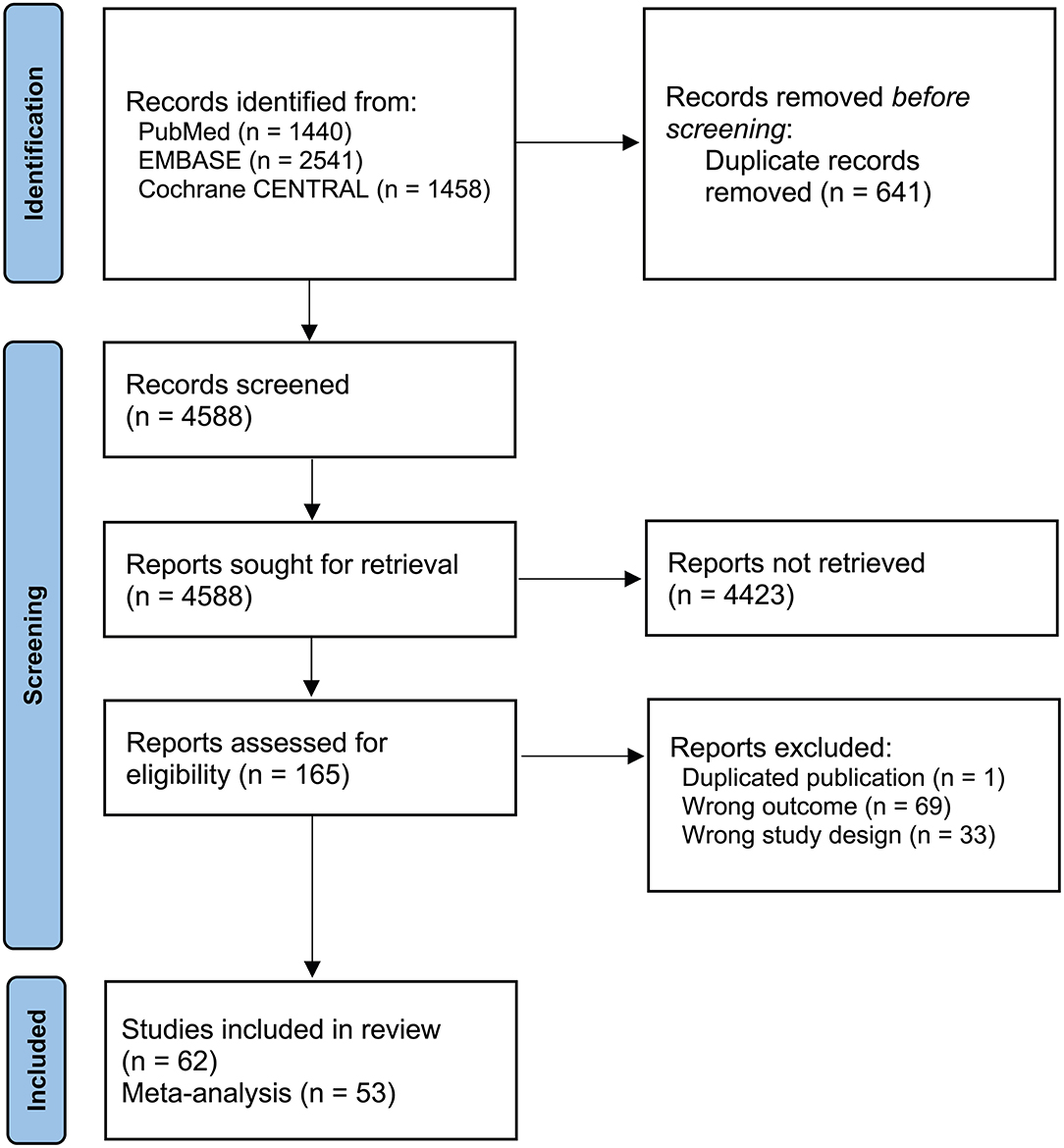
Figure 1. Study flow diagram.
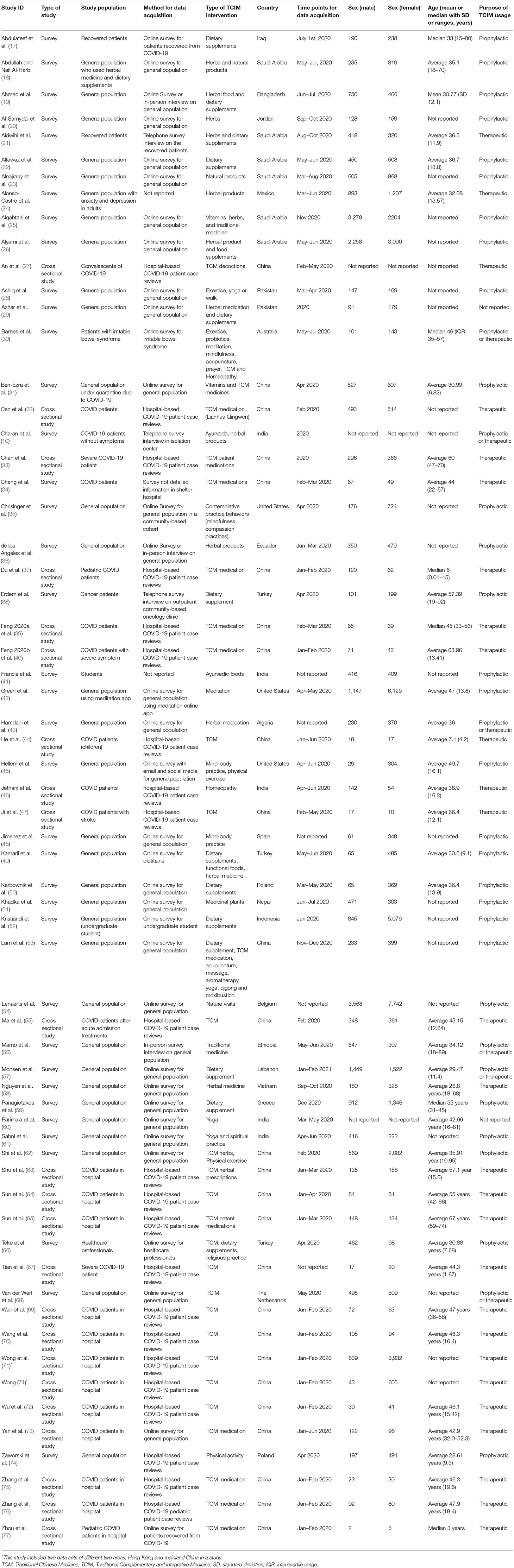
Table 1. Summary of the included studies.
When assessing reporting quality with STROBE statement items, most studies did not appropriately address all the necessary contents in the publications. The most poorly reported items are variables (including effect modifiers and confounders), potential bias, sample size calculation, statistical methods with adjustments of potential effect modifiers and detailed information on excluded participant numbers at each stage of the study (Supplementary Table 2).
From the included studies, 53 studies (n = 61,831) suggested a total number of respondents or patients who used TCIM interventions during the COVID pandemic period. The overall pooled prevalence of TCIM usage was estimated to be 0.64 (95% CI 0.54–0.73). The I2 statistic was 99.88%, which implied severe statistical heterogeneity among the included studies (Figure 2). In screening for outliers by evaluating the studentized residuals of the included studies, one study (71) was identified as a potential outlier (z = −2.6827, Supplementary Figure 1). When this study was excluded, the pooled prevalence was estimated to be 0.65 (95% CI 0.56–0.74). In the population-based survey, the overall prevalence of TCIM usage was 0.63 (95% CI 0.52–0.73), which did not show a severe difference when compared with findings from the hospital-based patient case review (overall prevalence 0.65, 95% CI 0.48–0.81, Figure 2).
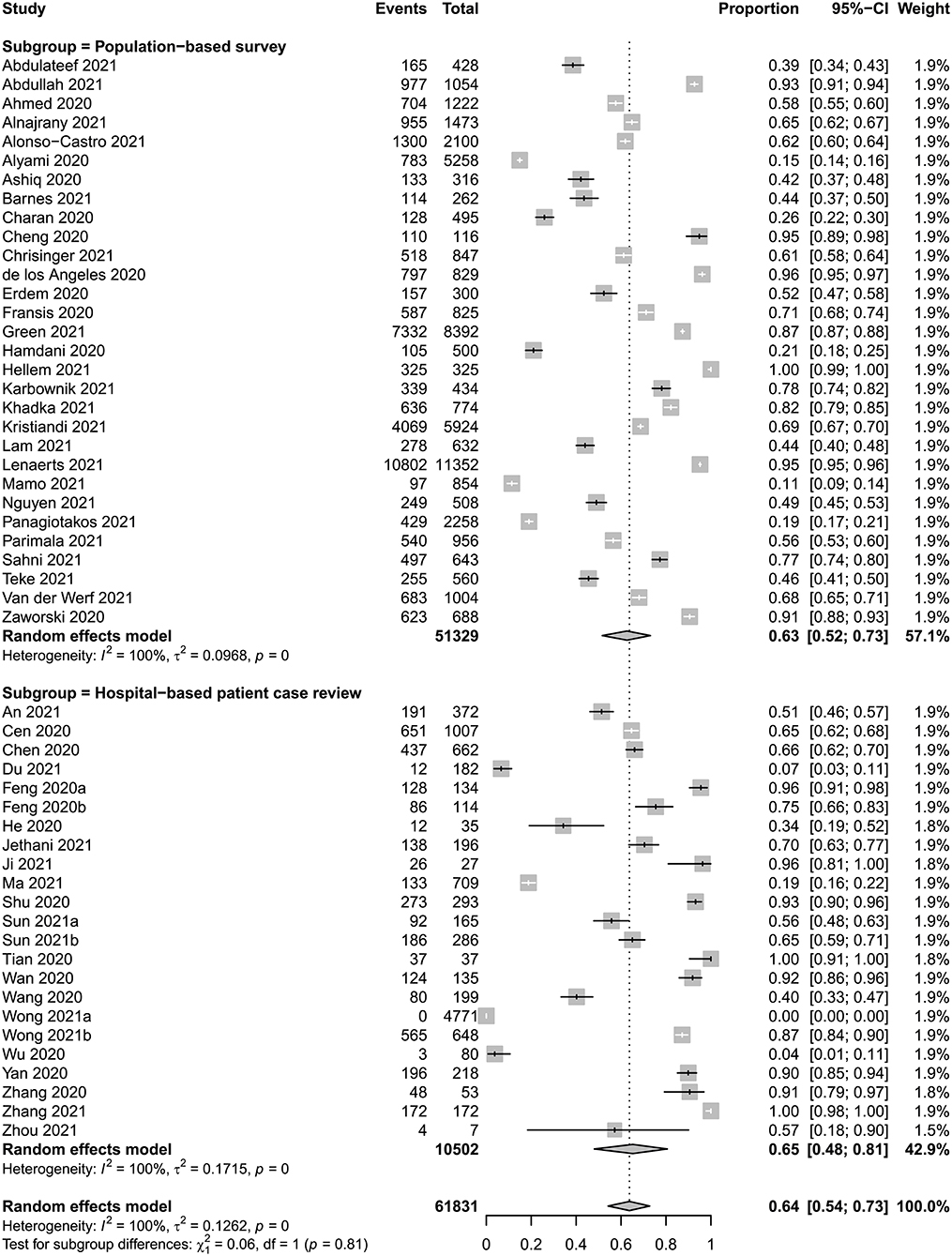
Figure 2. Meta-analysis of overall usage prevalence of TCIM interventions.
To analyze statistical heterogeneity among the included studies, subgroup analysis was conducted based on potential effect modifiers, including the type of studies (population-based survey vs. hospital-based COVID-19 patient case reviews), study population (general population vs. COVID-19 patients) and country of the study population (China vs. other countries). The R2 score for a potential effect modifier and the type of study was estimated to be 0%, which indicated that study type was not a strong effect modifier in this review. The study population (R2 score = 0%, Supplementary Figure 2) and country (R2 score = 1.03%, Supplementary Figure 3) could not explain the heterogeneity. In addition, a meta-regression test for the sample size of the included studies did not suggest that study size was an effect modifier (intercept: 0, P-value: 0.9108).
When comparing prevalence between countries, the country with the highest usage proportion of TCIM interventions was Ecuador (estimated proportion 0.9614, 95% CI 0.9471–0.9735), and Ethiopia showed the lowest proportion (0.1136, 95% CI 0.0931–0.1358, Table 2). There were no definitive regional trends in the usage proportion of TCIM interventions visually observed from the world map of proportion distribution (Supplementary Figure 4).
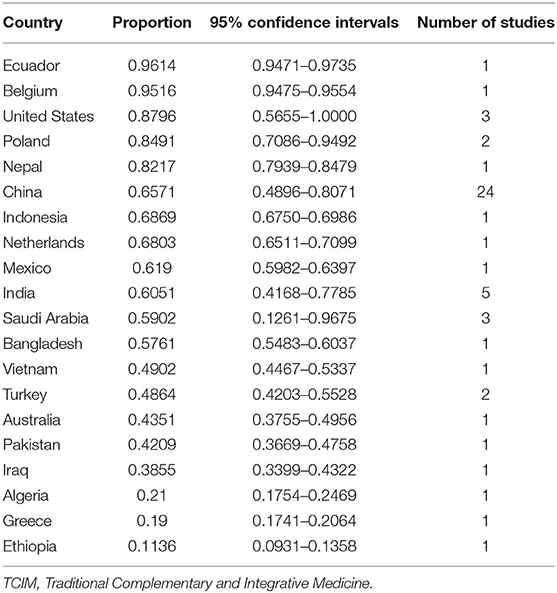
Table 2. Estimated proportion of TCIM usage in each country.
Twenty-five studies assessed the usage prevalence of TCM medication, and the synthesized proportion was estimated to be 0.62 (95% CI 0.45–0.78), which showed severe statistical heterogeneity (I2 = 100%, Supplementary Figure 5A). The usage proportions of Ayurveda (n = 2) and homeopathy (n = 2) were 0.44 (95% CI 0.04–0.91, Supplementary Figure 5B) and 0.30 (95% CI 0.00–0.97, Supplementary Figure 5C). The usage prevalence of yoga was suggested in 7 studies, and the estimated proportion was 0.53 (95% CI 0.27–0.78, Supplementary Figure 5D). Acupuncture was assessed in 3 studies, and the estimated prevalence was 0.20 (95% CI 0.00–0.58, Supplementary Figure 5E). Physical exercise was evaluated in 4 studies, and the estimated prevalence was 0.70 (95% CI 0.33–0.96, Supplementary Figure 5F). The proportion of dietary supplements, herbs or natural products used was estimated to be 0.58 (95% CI 0.42–0.73, Supplementary Figure 5G) from the meta-analysis of 14 studies. The usage prevalence of spiritual therapy (n = 3) and massage (n = 2) were 0.24 (95% CI 0.01–0.65, Supplementary Figure 5H) and 0.28 (95% CI 0.00–0.87, Supplementary Figure 5I), respectively.
To assess potential publication bias, visual inspection of funnel plots was conducted, and no obvious asymmetry was observed (Supplementary Figure 6). Egger's test results suggested that there was no significant publication bias (P = 0.6856).
From 62 studies, the overall prevalence of TCIM usage during the COVID-19 pandemic was estimated to be 0.64 (95% CI 0.54–0.73), which also showed severe statistical heterogeneity and poor reporting quality. When comparing the rates of TCIM use across countries, the estimated proportion showed very large differences from 0.6914 (95% CI 0.9471–0.9735) in Ecuador to 0.1136 (95% CI 0.0931 to 0.1358) in Ethiopia. Study types for data acquisition did not affect the overall prevalence of TCIM usage 0.63 (95% CI 0.52–0.73) in the population-based survey and 0.65 (95% CI 0.48–0.81) in the hospital-based patient case review (R2 index = 0%). Although we explored potential effect modifiers for assessing statistical heterogeneity of this review, we failed to identify any meaningful reasons. Type of studies, study population and country of the population could not explain the considerable statistical heterogeneity of this study result.
From this review, it was found that TCIM interventions have been used for preventive and therapeutic purposes. Why do people use TCIM interventions for COVID-19? Disease burden, previous TCIM experience and perception of TCIM efficacy are well-known determinants for the usage of TCIM interventions for disease management (78, 79). During the COVID-19 pandemic when some underdeveloped countries experienced shortage of medical resources and restricted access to medical institutions, TCIM interventions tended to be accepted as a panacea, and this kind of attitude is based on health-related beliefs and the desire for self-care to improve immunity from the viral infection with a holistic approach (26, 80, 81). China published TCM guidelines for COVID-19, which might be related to the high usage rate of TCM interventions for therapeutic purposes during the pandemic period (7, 82–84). Meanwhile, the prevalence of TCIM usage in Western countries, such as the United States, was as high as that in underdeveloped countries. This might be due to different reasons, including dissatisfaction with the quality of conventional healthcare services (85). In addition, TCIM interventions such as mind-body practice have been used to maintain psychosocial health in many countries during the pandemic (35, 42, 45). Regarding reasons for the use of TCIM interventions during the COVID-19 pandemic, it is necessary to evaluate the underlying reasons by region in future research in detail.
This study has limitations. First, we failed to identify meaningful effect modifiers to explain the statistical heterogeneity. The reasons for using TCIM interventions such as prophylactic purpose or therapeutic purpose might be related to the potential heterogeneity of this review result. Different economic statuses and the medical systems of each country might be closely related to the diverse usage status of TCIM interventions, but these factors could not be assessed due to the limited numbers of included studies. In addition, one of the most powerful suspicious factors is the study population of the included studies. Online surveys, which are the most frequent data acquisition methods for the general population, usually adopt convenient sampling or snowballing sampling methods; these methods are commonly used due to easy execution, but they cannot generate unbiased results due to generalizability issues (86). When looking at the process of online surveys in general, a link to the survey questionnaire is posted through the social network services, and interested people primarily participate in the survey. Since people interested in the interventions are more likely to participate in the survey, it is natural that the proportion of end users is high. As a way to solve this problem, it is necessary to use a survey that captures the entire population of interest or probability sampling methods, so that the overall opinion of the general population of interest can be reflected. Hospital-based COVID patient chart review data could also be biased because most studies were conducted in China, which is one of the few countries with published TCIM CPGs for COVID-19 (84, 87, 88). International cooperative surveys on the usage of TCIM interventions would be helpful to overcome the bias introduced by these limitations. Second, the definition of TCIM interventions varied from study to study, so the estimated usage prevalence derived from the meta-analysis of these studies could be inevitably biased. In addition, various study populations, such as the general population, COVID patients, physicians or practitioners of TCIM interventions, could have different perceptions and experiences of TCIM usage during the COVID-19 response. The initial purpose of this study was to suggest a crude prevalence of TCIM usage, so we did not consider these factors when conducting the meta-analysis, which is a critical limitation of this study. In this study, we did not search non-English DBs including China and Korea where TCIM is one of the main medical systems and many relevant studies are published. Therefore, we cannot be confident about locating all relevant data on this topic. Finally, data from the studies conducted mainly in the first half of 2020, shortly after the outbreak of COVID-19, were included in the analysis. The COVID-19 pandemic has been ongoing for nearly 2 years as of November 2021, and current TCIM usage patterns might be different than the initial patterns. An updated review that includes 2021 data is needed. Currently, an international survey on the prevention of and treatments for COVID-19 has been conducted, which might suggest more reliable data on the prevalence of TCIM interventions used worldwide (89).
In conclusion, various TCIM interventions were reported to be used at a comparatively high frequency, but this result should be interpreted carefully due to the heterogeneity and low reporting quality of the included studies. Future studies need to be updated to include global data through international collaborative research, which might overcome the main limitation of this study, i.e., the heterogeneity of the included data.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
ML and T-HK: conceptualization and writing—original draft. T-HK and S-RJ: methodology and investigation. T-HK: software and visualization. JK and HL: validation. T-HK and LA: formal analysis. T-HK and HL: resources. JK and LA: data curation. JK, S-RJ, LA, and HL: writing—review and editing. T-HK, ML, and JK: supervision. S-RJ and HL: project administration. ML: funding acquisition. All authors read and approved the final manuscript.
This study is funded by Korea Institute of Oriental Medicine (KSN20214115).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.884573/full#supplementary-material
1. Zhou T, Liu Q, Yang Z, Liao J, Yang K, Bai W, et al. Preliminary prediction of the basic reproduction number of the Wuhan novel coronavirus 2019-nCoV. J Evid Based Med. (2020) 13:3–7. doi: 10.1111/jebm.12376
2. Campos DMdO, Fulco UL, de Oliveira CBS, Oliveira JIN. SARS-CoV-2 virus infection: targets and antiviral pharmacological strategies. J Evid Based Med. (2020) 13:255–60. doi: 10.1111/jebm.12414
3. World Health Organization. COVID-19 Clinical Management: Living Guidance. Geneva: World Health Orgarnization (2021).
4. Crook H, Raza S, Nowell J, Young M, Edison P. Long covid-mechanisms, risk factors, and management. BMJ. (2021) 374:n1648. doi: 10.1136/bmj.n1648
5. Goertz YMJ, Van Herck M, Delbressine JM, Vaes AW, Meys R, Machado FVC, et al. Persistent symptoms 3 months after a SARS-CoV-2 infection: the post-COVID-19 syndrome? ERJ Open Res. (2020) 6:00542-2020. doi: 10.1183/23120541.00542-2020
6. Liang N, Ma Y, Wang J, Li H, Wang X, Jiao L, et al. Traditional Chinese medicine guidelines for coronavirus disease 2019. J Tradit Chin Med. (2020) 40:891–6. doi: 10.19852/j.cnki.jtcm.20200902.001
7. Ge L, Zhu H, Wang Q, Li M, Cai J, Chen Y, et al. Integrating Chinese and western medicine for COVID-19: a living evidence-based guideline (version 1). J Evid Based Med. (2021) 14:313–32. doi: 10.1111/jebm.12444
8. Lee BJ, Lee JA, Kim KI, Choi JY, Jung HJ. A consensus guideline of herbal medicine for coronavirus disease 2019. Integr Med Res. (2020) 9:100470. doi: 10.1016/j.imr.2020.100470
9. Pandit RD, Singh RK. COVID-19 Ayurveda treatment protocol of governments of Nepal and India: a review and perspective. App Sci Technol Ann. (2020) 1:72–80. doi: 10.3126/asta.v1i1.30276
10. Charan J, Bhardwaj P, Dutta S, Kaur R, Bist SK, Detha MD, et al. Use of complementary and alternative medicine (CAM) and home remedies by COVID-19 patients: a telephonic survey. Indian J Clin Biochem. (2020) 36:1–4. doi: 10.1007/s12291-020-00931-4
11. Ang L, Song E, Lee MS. Randomized controlled trials of traditional, complementary, and integrative medicine-based interventions for coronavirus disease 2019 (COVID-19): a bibliometric analysis and review of study designs. Integr Med Res. (2021) 10:100777. doi: 10.1016/j.imr.2021.100777
12. Ang L, Song E, Lee HW, Lee MS. Herbal medicine for the treatment of coronavirus disease 2019 (COVID-19): a systematic review and meta-analysis of randomized controlled trials. J Clin Med. (2020) 9:1583. doi: 10.3390/jcm9051583
13. Ng JY. Global research trends at the intersection of coronavirus disease 2019 (COVID-19) and traditional, integrative, and complementary and alternative medicine: a bibliometric analysis. BMC Complement Med Ther. (2020) 20:353. doi: 10.1186/s12906-020-03151-8
14. National Center for Complementary Integrative Health. Complementary, Alternative, or Integrative Health: What's In a Name? https://www.nccih.nih.gov/health/complementary-alternative-or-integrative-health-whats-in-a-name (accessed April 09, 2022).
15. Freeman MF, Tukey JW. Transformations related to the angular and the square root. Ann Math Stat. (1950) 21:607–11. doi: 10.1214/aoms/1177729756
16. Borenstein M, Hedges LV, Higgins JP, Rothstein HR. Introduction to Meta-Analysis. NJ: John Wiley & Sons; 2021. ISBN: 1119558387. doi: 10.1002/9781119558378
17. Abdulateef DS, Rahman HS, Salih JM, Osman SM, Mahmood TA, Omer SHS, et al. COVID-19 severity in relation to sociodemographics and vitamin D use. Open Med. (2021) 16:591–609. doi: 10.1515/med-2021-0273
18. Abdullah Alotiby A, Naif Al-Harbi L. Prevalence of using herbs and natural products as a protective measure during the COVID-19 pandemic among the Saudi population: an online cross-sectional survey. Saudi Pharm J. (2021) 29:410–7. doi: 10.1016/j.jsps.2021.04.001
19. Ahmed I, Hasan M, Akter R, Sarkar BK, Rahman M, Sarker MS, et al. Behavioral preventive measures and the use of medicines and herbal products among the public in response to Covid-19 in Bangladesh: a cross-sectional study. PLoS ONE. (2020) 15:e0243706. doi: 10.1371/journal.pone.0243706
20. Al-Samydai A, Hajleh MA, Akour A, Alabdallah N, Yousef M. Baqa‘in G, Al-Saadi A, Al-Halaseh LK, Aburjai T. Phytotherapeutic approaches and ethnopharmacological responses against COVID-19. Trop J Nat Prod Res. (2021) 5:1208–14. doi: 10.26538/tjnpr/v5i7.7
21. Aldwihi LA, Khan SI, Alamri FF, AlRuthia Y, Alqahtani F, Fantoukh OI, et al. Patients' behavior regarding dietary or herbal supplements before and during COVID-19 in Saudi Arabia. Int J Environ Res Public Health. (2021) 18:5086. doi: 10.3390/ijerph18105086
22. Alfawaz H, Yakout SM, Wani K, Aljumah GA, Ansari MGA, Khattak MNK, et al. Dietary intake and mental health among Saudi adults during COVID-19 lockdown. Int J Environ Res Public Health. (2021) 18:1653. doi: 10.3390/ijerph18041653
23. AlNajrany SM, Asiri Y, Sales I, AlRuthia Y. The Commonly utilized natural products during the COVID-19 pandemic in saudi arabia: a cross-sectional online survey. Int J Environ Res Public Health. (2021) 18:4688. doi: 10.3390/ijerph18094688
24. Alonso-Castro AJ, Ruiz-Padilla AJ, Ortiz-Cortes M, Carranza E, Ramírez-Morales MA, Escutia-Gutiérrez R, et al. Self-treatment and adverse reactions with herbal products for treating symptoms associated with anxiety and depression in adults from the central-western region of Mexico during the Covid-19 pandemic. J Ethnopharmacol. (2021) 272:113952. doi: 10.1016/j.jep.2021.113952
25. Alqahtani AH, Alqahtani SA, Alhodaib AS, Al-Wathinani AM, Daoulah A, Alhamid S, et al. Knowledge, attitude, and practice (Kap) toward the novel coronavirus (covid-19) pandemic in a saudi population-based survey. Int J Environ Res Public Health. (2021) 18:5286. doi: 10.3390/ijerph18105286
26. Alyami HS, Orabi MAA, Aldhabbah FM, Alturki HN, Aburas WI, Alfayez AI, et al. Knowledge about COVID-19 and beliefs about and use of herbal products during the COVID-19 pandemic: a cross-sectional study in Saudi Arabia. Saudi Pharm J. (2020) 28:1326–32. doi: 10.1016/j.jsps.2020.08.023
27. An YW, Yuan B, Wang JC, Wang C, Liu TT, Song S, et al. Clinical characteristics and impacts of traditional Chinese medicine treatment on the convalescents of COVID-19. Int J Med Sci. (2021) 18:646–51. doi: 10.7150/ijms.52664
28. Ashiq K, Ashiq S, Bajwa MA, Tanveer S, Qayyum M. Knowledge, attitude and practices among the inhabitants of lahore, pakistan towards the COVID-19 pandemic: an immediate online based cross-sectional survey while people are under the lockdown. Bangladesh J Med Sci. (2020) 19:S69–76. doi: 10.3329/bjms.v19i0.48169
29. Azhar H, Tauseef A, Usman T, Azhar Y, Ahmed M, Umer K, et al. Prevalence, attitude and knowledge of self medication during Covid-19 disease pandemic. Pakistan J Med Health Sci. (2021) 15:902–5. doi: 10.53350/pjmhs21155902
30. Barnes A, Andrews J, Spizzo P, Mountifield R. Medication adherence and complementary therapy usage in inflammatory bowel disease patients during the coronavirus disease 2019 pandemic. JGH Open. (2021) 5:585–9. doi: 10.1002/jgh3.12537
31. Ben-Ezra M, Sun S, Hou WK, Goodwin R. The association of being in quarantine and related COVID-19 recommended and non-recommended behaviors with psychological distress in Chinese population. J Affect Disord. (2020) 275:66–8. doi: 10.1016/j.jad.2020.06.026
32. Cen Y, Chen X, Shen Y, Zhang XH, Lei Y, Xu C, et al. Risk factors for disease progression in patients with mild to moderate coronavirus disease 2019-a multi-centre observational study. Clin Microbiol Infect. (2020) 26:1242–7. doi: 10.1016/j.cmi.2020.05.041
33. Chen G, Su W, Yang J, Luo D, Xia P, Jia W, et al. Chinese herbal medicine reduces mortality in patients with severe and critical Coronavirus disease 2019: a retrospective cohort study. Front Med. (2020) 14:752–9. doi: 10.1007/s11684-020-0813-6
34. Cheng F, Li Q, Han Y, Shi C, Wu S, Xu Q, et al. Analysis of influencing factors and pharmaceutical care of patients with COVID-19 in Fangcang Shelter Hospital. Infect Drug Resist. (2020) 13:3443–50. doi: 10.2147/IDR.S263961
35. Chrisinger BW, Rich T, Lounsbury D, Peng K, Zhang J, Heaney CA, et al. Coping with the COVID-19 pandemic: contemplative practice behaviors are associated with better mental health outcomes and compliance with shelter-in-place orders in a prospective cohort study. Prev Med Rep. (2021) 23:101451. doi: 10.1016/j.pmedr.2021.101451
36. de los Ángeles M, Minchala-Urgilés RE, Ramírez-Coronel AA, Aguayza-Perguachi MA, Torres-Criollo LM, Romero-Sacoto LA, et al. Herbal medicine as prevention and treatment against Covid-19. Arch Venez Farmacol Ter. (2020) 39:948–53. doi: 10.5281/zenodo.4543573
37. Du H, Dong X, Zhang JJ, Cao YY, Akdis M, Huang PQ, et al. Clinical characteristics of 182 pediatric COVID-19 patients with different severities and allergic status. Allergy. (2021) 76:51. doi: 10.22541/au.158920561.18059266
38. Erdem D, Karaman I. Awareness and perceptions related to COVID-19 among cancer patients: a survey in oncology department. Eur J Cancer Care. (2020) 29:e13309. doi: 10.1111/ecc.13309
39. Feng G, Huang WQ, Liu ML, Lin SC, Zhang XZ, Zhang Y, et al. Clinical features of COVID-19 patients in Xiaogan City. SN Compr Clin Med. (2020) 2:1717–23. doi: 10.1007/s42399-020-00465-z
40. Feng X, Li P, Ma L, Liang H, Lei J, Li W, et al. Clinical characteristics and short-term outcomes of severe patients with COVID-19 in Wuhan, China. Front Med. (2020) 7:491. doi: 10.3389/fmed.2020.00491
41. Francis J, Prof JP, Prof LP, Prof LA. Awareness of self-quarantine- a survey. Eur J Mol Clin Med. (2020) 7:2236–47.
42. Green J, Huberty J, Puzia M, Stecher C. The effect of meditation and physical activity on the mental health impact of covid-19-related stress and attention to news among mobile app users in the united states: cross-sectional survey. JMIR Mental Health. (2021) 8:e28479. doi: 10.2196/preprints.28479
43. Hamdani FZ, Houari N. Phytothérapie et Covid-19. Une étude fondée sur une enquête dans le nord de l'Algérie Phytothérapie. (2021) 18:248–54. doi: 10.3166/phyto-2020-0241
44. He M, Wang C, Xu L, Zhang H, Liu Y, Zhao Y, et al. Epidemiological and clinical characteristics of 35 children with COVID-19 in Beijing, China. Pediatr Investig. (2020) 4:230–5. doi: 10.1002/ped4.12230
45. Hellem T, Benavides-Vaello S, Taylor-Piliae R. National internet-based survey of the use, barriers, reasons and beliefs of mind-body practices during the early months of the COVID-19 pandemic. J Evid Based Integr Med. (2021) 26:2515690x211006332. doi: 10.1177/2515690X211006332
46. Jethani B, Gupta M, Wadhwani P, Thomas R, Balakrishnan T, Mathew G, et al. Clinical characteristics and remedy profiles of patients with COVID-19: a retrospective cohort study. Homeopathy. (2021) 110:86–93. doi: 10.1055/s-0040-1718584
47. Ji XY, Ma Y, Shi NN, Liang N, Chen RB, Liu SH, et al. Clinical characteristics and treatment outcome of COVID-19 patients with stroke in China: a multicenter retrospective study. Phytomedicine. (2021) 81:153433. doi: 10.1016/j.phymed.2020.153433
48. Jimenez O, Sanchez-Sanchez LC, Garcia-Montes JM. Psychological impact of COVID-19 confinement and its relationship with meditation. Int J Environ Res Public Health. (2020) 17:6642. doi: 10.3390/ijerph17186642
49. Kamarli Altun H, Karacil Ermumcu MS, Seremet Kurklu N. Evaluation of dietary supplement, functional food and herbal medicine use by dietitians during the COVID-19 pandemic. Public Health Nutr. (2021) 24:861–9. doi: 10.1017/S1368980020005297
50. Karbownik MS, Dobielska M, Paul E, Kowalczyk RP, Kowalczyk E. Health-, medication- and dietary supplement-related behaviors and beliefs relatively unchanged during the COVID-19 pandemic lockdown. Res Social Adm Pharm. (2021) 17:1501–6. doi: 10.1016/j.sapharm.2020.11.015
51. Khadka D, Dhamala MK, Li F, Aryal PC, Magar PR, Bhatta S, et al. The use of medicinal plants to prevent COVID-19 in Nepal. J Ethnobiol Ethnomed. (2021) 17:26. doi: 10.1186/s13002-021-00449-w
52. Kristiandi K, Yunianto AE, Darawati M, Doloksaribu TH, Anggraeni I, Pasambuna M, et al. Food consumption patterns of male and female undergraduate students in indonesia during new normal implementation of pandemic Covid-19 Era. Open Access Maced J Med Sci. (2021) 9:278–82. doi: 10.3889/oamjms.2021.5926
53. Lam CS, Koon HK, Chung VC, Cheung YT. A public survey of traditional, complementary and integrative medicine use during the COVID-19 outbreak in Hong Kong. PLoS ONE. (2021) 16:e0253890. doi: 10.1371/journal.pone.0253890
54. Lenaerts A, Heyman S, De Decker A, Lauwers L, Sterckx A, Remmen R, et al. Vitamin nature: how coronavirus disease 2019 has highlighted factors contributing to the frequency of nature visits in flanders, Belgium. Front Public Health. (2021) 9:646568. doi: 10.3389/fpubh.2021.646568
55. Ma X, Gao Y, Di L, Ma H, Mei B, Zhang J, Wang A, Feng K, Yang L, Chen Z. Characteristics of 1738 patients with coronavirus disease 2019 (COVID-19) in Wuhan, China. Disaster Med Public Health Prep. (2021) 1–5. doi: 10.1017/dmp.2021.129
56. Mamo A, Hassen MM, Adem A, Teferu Z, Kumbi M, Husen A, et al. Knowledge, attitude, and utilization of drugs toward COVID-19 pandemic among Bale Zone residents, Southeast Ethiopia. SAGE Open Med. (2021) 9:20503121211034384. doi: 10.1177/20503121211034384
57. Mohsen H, Yazbeck N, Al-Jawaldeh A, Bou Chahine N, Hamieh H, Mourad Y, et al. Knowledge, attitudes, and practices related to dietary supplementation, before and during the COVID-19 pandemic: findings from a cross-sectional survey in the lebanese population. Int J Environ Res Public Health. (2021) 18:8856. doi: 10.3390/ijerph18168856
58. Nguyen PH, Tran VD, Pham DT, Dao TNP, Dewey RS. Use of and attitudes towards herbal medicine during the COVID-19 pandemic: a cross-sectional study in Vietnam. Eur J Integr Med. (2021) 44:101328. doi: 10.1016/j.eujim.2021.101328
59. Panagiotakos D, Kosti RI, Pitsavos C. How will the way we live look different in the wake of the COVID-19 pandemic? A nutrition survey in Greece. Nutr Health. (2021) 2601060211009033. doi: 10.1177/02601060211009033
60. Parimala S, Kanchibhotla D. Association between yogic breathing practice with perceived impact of COVID-19: a cross-sectional study from India. Asia-Pac J Public Health. (2021) 33:157–9. doi: 10.1177/1010539520975282
61. Sahni PS, Singh K, Sharma N, Garg R. Yoga an effective strategy for self-management of stress-related problems and wellbeing during COVID19 lockdown: a cross-sectional study. PLoS ONE. (2021) 16:e0245214. doi: 10.1371/journal.pone.0245214
62. Shi Z, Qin Y, Chair SY, Liu Y, Tian Y, Li X, Hu W, Wang Q. Anxiety and depression levels of the general population during the rapid progressing stage in the coronavirus disease 2019 outbreak: a cross-sectional online investigation in China. BMJ Open. (2021) 11:e050084. doi: 10.1136/bmjopen-2021-050084
63. Shu Z, Zhou Y, Chang K, Liu J, Min X, Zhang Q, et al. Clinical features and the traditional Chinese medicine therapeutic characteristics of 293 COVID-19 inpatient cases. Front Med. (2020) 14:760–75. doi: 10.1007/s11684-020-0803-8
64. Sun F, Kou H, Wang S, Lu Y, Zhao H, Li W, et al. An analytical study of drug utilization, disease progression, and adverse events among 165 COVID-19 patients. Ann Transl Med. (2021) 9:306. doi: 10.21037/atm-20-4960
65. Sun QG, An XD, Xie P, Jiang B, Tian JX, Yang Q, et al. Traditional chinese medicine decoctions significantly reduce the mortality in severe and critically Ill patients with COVID-19: a retrospective cohort study. Am J Chin Med. (2021) 49:1063–92. doi: 10.1142/S0192415X21500518
66. Teke N, Özer Z, Bahçecioglu Turan G. Analysis of health care personnel's attitudes toward complementary and alternative medicine and life satisfaction due to COVID-19 pandemic. Holist Nurs Pract. (2021) 35:98–107. doi: 10.1097/HNP.0000000000000431
67. Tian S, Chang Z, Wang Y, Wu M, Zhang W, Zhou G, et al. Clinical characteristics and reasons for differences in duration from symptom onset to release from quarantine among patients with COVID-19 in Liaocheng, China. Front Med. (2020) 7:210. doi: 10.3389/fmed.2020.00210
68. van der Werf ET, Busch M, Jong MC, Hoenders HJR. Lifestyle changes during the first wave of the COVID-19 pandemic: a cross-sectional survey in the Netherlands. BMC Public Health. (2021) 21:1226. doi: 10.1186/s12889-021-11264-z
69. Wan S, Xiang Y, Fang W, Zheng Y, Li B, Hu Y, et al. Clinical features and treatment of COVID-19 patients in northeast Chongqing. J Med Virol. (2020) 92:797–806. doi: 10.1002/jmv.25783
70. Wang S, Chen Z, Lin Y, Lin L, Lin Q, Fang S, et al. Clinical characteristics of 199 discharged patients with COVID-19 in Fujian Province: a multicenter retrospective study between January 22nd and February 27th, 2020. PLoS ONE. (2020) 15:e0242307. doi: 10.1371/journal.pone.0242307
71. Wong CKH, Wan EYF, Luo S, Ding Y, Lau EHY, Ling P, et al. Clinical outcomes of different therapeutic options for COVID-19 in two Chinese case cohorts: a propensity-score analysis. EClinicalMedicine. (2021) 32:100743. doi: 10.1016/j.eclinm.2021.100743
72. Wu J, Liu J, Zhao X, Liu C, Wang W, Wang D, et al. Clinical characteristics of imported cases of coronavirus Disease 2019 (COVID-19) in Jiangsu Province: a multicenter descriptive study. Clin Infect Dis. (2020) 71:706–12. doi: 10.1093/cid/ciaa199
73. Yan X, Han X, Peng D, Fan Y, Fang Z, Long D, et al. Clinical characteristics and prognosis of 218 patients with COVID-19: a retrospective study based on clinical classification. Front Med. (2020) 7:485. doi: 10.3389/fmed.2020.00485
74. Zaworski K, Kubińska Z, Dziewulska A, Walasek O. Physical activity of Poles in the care for their health potential before and during the COVID-19 pandemic. Disaster Med Public Health Prep. (2020) 1–4. doi: 10.1017/dmp.2020.398
75. Zhang C, Li T, Wang X, Tian Y, Zhu X. Analysis of drug therapy of 53 patients with Corona Virus Disease-2019. Pharm Care Res. (2020) 20:423–57. doi: 10.5428/pcar20200606
76. Zhang Q, Wang Z, Lv Y, Zhao J, Dang Q, Xu D, et al. Clinical features and prognostic factors of patients with COVID-19 in Henan Province, China. Hum Cell. (2021) 34:419–35. doi: 10.1007/s13577-021-00499-y
77. Zhou L, Song X, Lu H, Mao Y, Liu C, Yuan Y, et al. Clinical analysis of seven pediatric patients with coronavirus disease 2019 (COVID-19) in Jingzhou, Hubei, China: a retrospective study. Transl Pediatr. (2021) 10:616–24. doi: 10.21037/tp-21-48
78. Chowdhuri PD, Kundu K. Factors determining choice of complementary and alternative medicine in acute and chronic diseases. J Complement Integr Med. (2020) 17. doi: 10.1515/jcim-2019-0105
79. Kretchy IA, Boadu JA, Kretchy J-P, Agyabeng K, Passah AA, Koduah A, et al. Utilization of complementary and alternative medicine for the prevention of COVID-19 infection in Ghana: a national cross-sectional online survey. Prev Med Rep. (2021) 24:101633. doi: 10.1016/j.pmedr.2021.101633
80. Peprah P, Agyemang-Duah W, Arthur-Holmes F, Budu HI, Abalo EM, Okwei R, et al. ‘We are nothing without herbs’: a story of herbal remedies use during pregnancy in rural Ghana. BMC Complement Altern Med. (2019) 19:65. doi: 10.1186/s12906-019-2476-x
81. Da'ar OB, Haji M, Jradi H. Coronavirus Disease 2019 (COVID-19): Potential implications for weak health systems and conflict zones in the Middle East and North Africa region. Int J Health Plann Manage. (2020) 35:1240–45. doi: 10.1002/hpm.2982
82. Ang L, Lee HW, Kim A, Lee MS. Herbal medicine for the management of COVID-19 during the medical observation period: a review of guidelines. Integr Med Res. (2020) 9:100465. doi: 10.1016/j.imr.2020.100465
83. Dai T, Zhang L, Dai X, Zhang X, Lu B, Zheng Y, et al. Multimode participation of traditional Chinese medicine in the treatment of COVID-19. Integr Med Res. (2021) 10:100781. doi: 10.1016/j.imr.2021.100781
84. Lu CL, Zheng RX, Xue X, Zhang XW, Liu XH, Jin XY, et al. Traditional Chinese medicine for COVID-19 pandemic and emerging challenges: an online cross-sectional survey in China. Integr Med Res. (2021) 10:100798. doi: 10.1016/j.imr.2021.100798
85. Laiyemo MA, Nunlee-Bland G, Adams RG, Laiyemo AO, Lombardo FA. Characteristics and health perceptions of complementary and alternative medicine users in the United States. Am J Med Sci. (2015) 349:140–4. doi: 10.1097/MAJ.0000000000000363
86. Jager J, Putnick DL, Bornstein MH. More than just convenient: the scientific merits of homogeneous convenience samples. Monogr Soc Res Child Dev. (2017) 82:13–30. doi: 10.1111/mono.12296
87. Ang L, Lee HW, Choi JY, Zhang J, Lee MS. Herbal medicine and pattern identification for treating COVID-19: a rapid review of guidelines. Integr Med Res. (2020) 9:100407. doi: 10.1016/j.imr.2020.100407
88. National Health Commission & National Administration of Traditional Chinese Medicine. Diagnosis and treatment protocol for COVID-19 patients (Tentative 8th Edition). Infect Dis Immun. (2021) 1:8–16. doi: 10.1097/01.ID9.0000733564.21786.b0
89. RTO-Covid-19. Retrospective Survey of Prevention, Treatment, Occurrence and Outcomes of Covid-19 in the Community. https://www.southampton.ac.uk/medicine/research/projects/rto-covid-19.page (accessed April 09, 2022).
Keywords: prevalence of usage, complementary and alternative medicine, systematic review, meta-analysis, STROBE statement, Traditional Complementary and Integrative Medicine, TCIM
Citation: Kim T-H, Kang JW, Jeon S-R, Ang L, Lee HW and Lee MS (2022) Use of Traditional, Complementary and Integrative Medicine During the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Front. Med. 9:884573. doi: 10.3389/fmed.2022.884573
Received: 26 February 2022; Accepted: 11 April 2022;
Published: 09 May 2022.
Edited by:
Yonggang Zhang, Sichuan University, ChinaReviewed by:
Kwabena F. M. Opuni, University of Ghana, GhanaCopyright © 2022 Kim, Kang, Jeon, Ang, Lee and Lee. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Myeong Soo Lee, ZHJtc2xlZUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.