
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Med. , 12 May 2022
Sec. Geriatric Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.877213
 Hélio José Coelho-Júnior1,2,3*
Hélio José Coelho-Júnior1,2,3* Riccardo Calvani3
Riccardo Calvani3 Francesco Panza4
Francesco Panza4 Riccardo F. Allegri5,6
Riccardo F. Allegri5,6 Anna Picca3
Anna Picca3 Emanuele Marzetti1,3†
Emanuele Marzetti1,3† Vicente Paulo Alves2†
Vicente Paulo Alves2†Objectives: The present study investigated the association between religious and spiritual (RS) practices with the prevalence, severity, and incidence of mental health problems in older adults.
Methods: We conducted a systematic review and meta-analysis of cross-sectional and longitudinal studies that investigated older adults aged 60+ years and assessed RS using valid scales and questions from valid scales, and mental health according to validated multidimensional or specific instruments. Studies were retrieved from MEDLINE, LILACS, SCOPUS, CINAHL, and AgeLine databases until July 31, 2021. The risk of bias was evaluated using the Newcastle-Ottawa Quality Assessment Scale (NOS). A pooled effect size was calculated based on the log odds ratio (OR) and Z-scores. This study is registered on PROSPERO.
Results: One hundred and two studies that investigated 79.918 community-dwellers, hospitalized, and institutionalized older adults were included. Results indicated that high RS was negatively associated with anxiety and depressive symptoms, while a positive association was observed with life satisfaction, meaning in life, social relations, and psychological well-being. Specifically, people with high spirituality, intrinsic religiosity, and religious affiliation had a lower prevalence of depressive symptoms. In relation to longitudinal analysis, most studies supported that high RS levels were associated with a lower incidence of depressive symptoms and fear of death, as well as better mental health status.
Conclusion: Findings of the present study suggest that RS are significantly associated with mental health in older adults. People with high RS levels had a lower prevalence of anxiety and depressive symptoms, as well as reported greater life satisfaction and psychological well-being, better social relations, and more definite meaning in life. Data provided by an increasing number of longitudinal studies have supported most of these findings.
Mental health is an integral and vital component of health that encompasses emotional, psychological, and social wellbeing (1). It refers to the way by which people behave, identify their selves, and cope with stressful events (1, 2), thereby affecting how they experience and understand life events (1, 2). In contrast, mental health decline is accompanied by a high frequency of persistent negative emotions, thoughts, and beliefs that influence the quality of life (3).
Older adults are highly susceptible to mental health problems (4). It is expected that one in five seniors will experience some form of mental illness during late life (1). Depression, anxiety, and substance abuse are the most common conditions found in older adults (5–8), although many other syndromes, such as sleep disorders, apathy, and agitation/aggression have also been frequently observed (9). The evolution of mental disorders is disastrous to patients and commonly involves disability and suicide (10–12), in addition to its high economic costs (12).
This scenario was noted by the World Health Organization (WHO) (2, 3), which established the maintenance of mental health in older adults as a priority for healthcare professionals and societies around the world. However, this topic is a relatively recent issue in medical and biological sciences and is still poorly addressed (13), impeding the creation and establishment of specific evidence-based treatments that effectively embrace all patients' needs.
Religious and spiritual (RS) beliefs are far from being just cultural traditions. Indeed, it involves numerous organizational, non-organizational, introspective, and community practices that might potentially influence human behavior (14). Concerning mental health, an increasing number of studies have observed better mental health status in people involved in RS activities (15–35). These results have been further confirmed by descriptive and systematic reviews (36–45). However, a specific pooled analysis based on a systematic search focused on the old population and incorporating a variety of religious and spiritual approaches is still needed (46).
Such research has important health and policy implications, given that older adults are highly involved in RS activities (47), and have frequently mentioned that they would feel better if health professionals could understand and take into consideration their personal beliefs (48, 49).
Based on these premises, the present study investigated the association between RS and the prevalence, severity, and incidence of mental health-related conditions in older adults by conducting a systematic review and meta-analysis.
This is a systematic review and meta-analysis of observational studies that investigated the cross-sectional and longitudinal associations between RS and mental health parameters in older adults. The study was fully performed by investigators and no librarian was part of the team. This study complies with the criteria of the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines (50) and the Cochrane Handbook for Systematic Reviews and Interventions (51). An a priori protocol was established and registered on PROSPERO, an international prospective register of systematic reviews [CRD42021292170].
Case-control, cross-sectional and longitudinal cohort studies that examined as a primary or secondary outcome the association between RS and mental health parameters in people aged 60+ years were included. Additional eligibility criteria consist of: (a) using valid scales or subscales (facets), questions from valid scales, and self-report devotion, identification, and/or adherence for measuring religiosity and/or spirituality; (b) mental health parameters assessed using valid multidimensional (e.g., Short Form Health Survey [SF-36]) or specific (Center for Epidemiological Studies-Depression [CES-D]) instruments; (c) published studies in English, Italian, Spanish or Portuguese languages. Studies that investigated patients with depression were included if they contained a non-depressive control group or presented depression severity scores. To be included in the meta-analysis, investigations should provide sample size of at least two groups divided according to mental health and RS. Alternatively, studies were incorporated into the pooled analysis if Pearson's correlation (r), Z-scores, Beta (β), or Odds Ratio (OR) values, as well as their corresponding confidence intervals (CI) or standard error (SE), for the association between RS and mental health parameters were presented. Studies designed to review the literature, investigate psychometric properties, validate and/or translate instruments were excluded. We also excluded studies that compared the prevalence of mental health parameters among different religious affiliations, but not provided comparisons with no religious identification or atheism.
Studies published on or before July 31, 2021, were retrieved from the following five electronic databases by one investigator: MEDLINE (PubMed interface), LILACS (Virtual Health Library interface), Scopus (EBSCO interface), AgeLine (EBSCO interface), CINAHL (EBSCO interface). Further eligible articles were identified by checking reference lists of systematic reviews and meta-analyses (Supplementary Material 1) and retrieved articles. In addition, citation searches on key articles were performed in Google Scholar and ResearchGate. Initially, a search strategy was designed using keywords, MeSH terms, and free text words, such as Religion, Mental Health, and Older Adults. Additionally, keywords and subject headings were exhaustively combined using Boolean operators. The complete search strategy used on PubMed is shown in Supplementary Material 2.
Titles and abstracts of retrieved articles were screened for eligibility by two researchers (HJCJ, RC). The full-text was consulted if the abstract did not provide enough information for final evaluation. Two reviewers (HJCJ, RC) extracted coded variables (i.e., methodological quality, risk of bias, and the characteristics of the studies) using a standardized coding form. A third researcher was consulted to solve disagreements (VP), if necessary. After extraction, data were divided into subcategories according to the type of religiosity and/or spiritual parameter and mental health aspects. To note, RS was examined as (a) Religious affiliation (yes/no), (b) Religious devotion (e.g., very much, not at all), (c) Religious index, (d) Organizational religious activities (ORA), (e) Non-organizational religious activities (NORA), and (f) Intrinsic religiosity (IR). ORA involved public religious practices, church/temple/cult/ritual attendance, and group-related religious activities (52); NORA included private activities, such as prayer, meditation, religious media, and scriptures studies (52); IR integrated personal commitment and/or motivation with the divine/deity (e.g., God). Spirituality was investigated alone and in combination with IR (52). Mental health parameters were divided into the following subcategories: (a) alcohol consumption, (b) anxiety, (c) death anxiety, (d) depressive symptoms, (e) hopelessness, (f) life satisfaction, (g) meaning in life, (h) psychological well-being, (i) self-esteem, (j) social relations, (k) suicidal ideation, and (l) tobacco use. A subcategory denominated general mental health was formed by studies that used composite scores that aggregate two or more mental health parameters or subscales of health survey questionnaires. The quality of reporting for each study was performed by two researchers (HJCJ, RC) using the Quality Assessment Tool for Observational Cohort and Cross-sectional of the National Institute of Health (53). This tool contains 14 questions that assess several aspects associated with the risk of bias, type I and type II errors, transparency, and confounding factors. Items 6, 7, and 13 do not refer to cross-sectional studies and were removed from the quality analysis. The maximum scores for cross-sectional and prospective studies were 8 and 14, respectively. The agreement rate for quality assessment between reviewers was 99%. The risk of bias was assessed using the Newcastle-Ottawa Quality Assessment Scale (NOS) (54, 55), according to Cochrane Collaboration Group' recommendation (56). NOS examines potential bin on selection, comparability, and outcome. The overall score ranges from 0 to 10 for cross-sectional studies, and from 0 to 9 for case-control and cohort studies. Scores ≤ 4 were identified as high risk of bias, scores 5–6 as moderate risk of bias, and scores ≥7 indicated a low risk of bias (57).
The meta-analysis was conducted using Revman 5.4.1 (Cochrane Collaboration, Copenhagen, Denmark) and STATA 13 (StataCorp, College Station, TX, USA). Effect sizes (ESs) were measured using OR, CI, Z-scores, and SE. When data were not made available by authors, they were calculated according to Cochrane guidelines (51). Specifically, SE was estimated according to the following formula: . OR were obtained from β coefficients or by calculating the number of participants allocated into high and low SR groups, and subsequently log-transformed (base 10) to be analyzed. Due to the variability of sample characteristics, a random-effect model was used to calculate the pooled logOR. Pearson's correlations were converted into Z-scores by calculating. Pooled Z-scores were calculated using the generic inverse variance (IV) method. A sensitivity analysis was performed based on the stratification technique according to RS aspects, including religious affiliation, religious devotion, religious index, service attendance, ORA, NORA, IR, and spirituality. Single pairwise comparisons were created when multiple studies referred to the same database using the formulas proposed by the Cochrane group (51). Publication bias was measured when at least ten studies investigated the same outcome (51) by examining funnel plots and the Egger's test for funnel plot asymmetry.
Forty-four thousand one hundred and eighty records were identified through database and hand searching. Of these, 43,863 records were excluded based on duplicate data, title, and abstract. Three hundred and seventeen studies were fully assessed for eligibility and 183 articles were excluded (Supplementary Material 3). Finally, 134 studies were included in the qualitative analysis and 62 studies provided data to be included in the pooled analysis. The flowchart of the present study is shown in Figure 1.
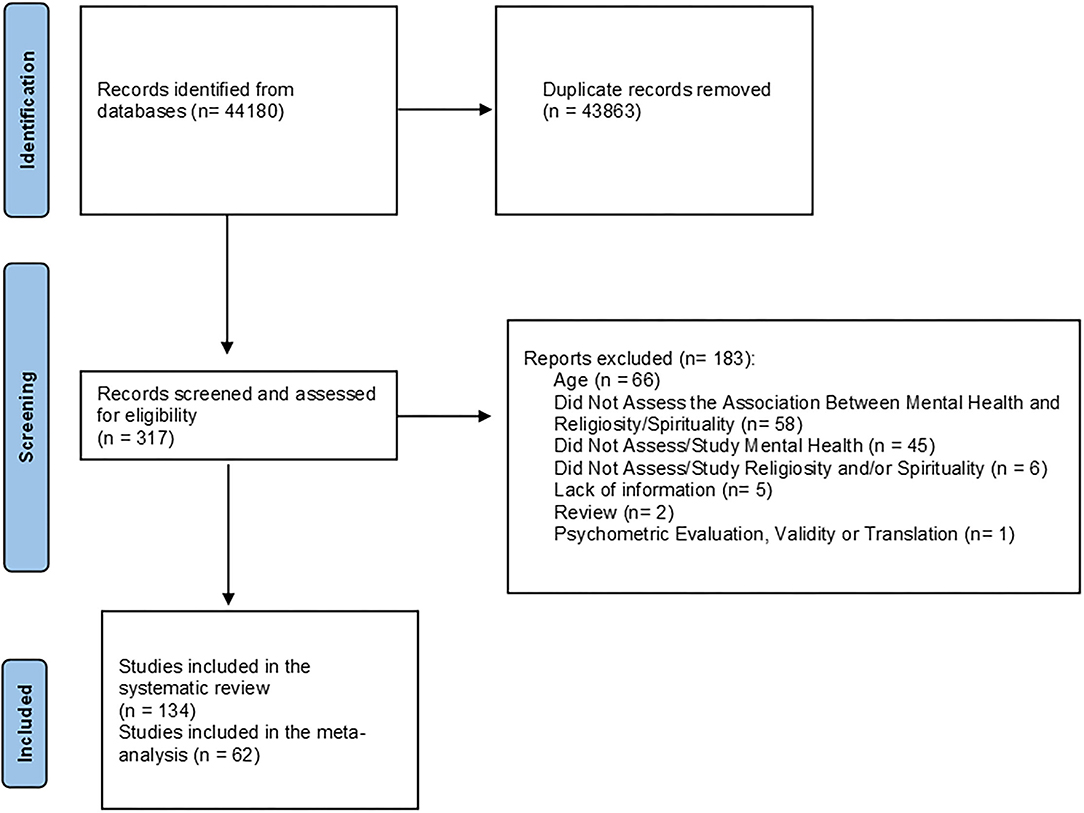
Figure 1. Flowchart of the present study.
A general description of the included cross-sectional and case-control studies that investigated religiosity is provided in Table 1. Religiosity was examined in one-hundred two studies (15–35, 46, 58–85, 87–90, 92–124, 126–136) that investigated 79,918 institutionalized, hospitalized, and community-dwellers with a mean age of ~73 years (from 60 to 90.3 years). Hospitalized patients included people with cancer, depression, and anxiety. Two studies involved older immigrants, one study investigated people who reported have experiencing trauma, and one study examined patients receiving home care nursing services. Investigations were conducted in Australia, Belgium, Brazil, Canada, Chile, China, Colombia, Egypt, Ghana, India, Iran, Italy, Japan, Korea, Lebanon, Malaysia, Mexican, Pakistan, Poland, Russia, Scotland, South Africa, South Korea, Spain, Sweden and Finland, Turkey, United Kingdom, and United States of America (USA) from 1977 to 2020. One study combined data from five different countries (i.e., England, Finland, Germany, Ireland, Netherland). The examined religious parameters included intrinsic and extrinsic religiosity, NORA, ORA, prayer, meditation, bible study, public religiosity, religious affiliation, religious behavior, religious coping, religious corporeity, religious devotion, religious doubt, religious engagement, religious index, religious involvement, religious knowledge, religious media, religious psychosocial resources, religious sentiment, religious support, service attendance, social religiosity, and private religious practices. Most studies (52.0%) assessed religiosity using self-developed scales, while 11.8% of the included studies used The Duke University Religion Index (DUREL), 5.9% The Religious Orientation Scale, 2.9% The Brief Multidimensional Measure Religiousness/Spirituality, 2.9% The Religious Coping Scale, 2% The Intrinsic Religiosity Scale, 2% The Religiosity index, and 2% The WHOQOL-SRPB. Other instruments, such as The Religious Attitudes Scale, The Religious Commitment Inventory, and The Religious Participation Questionnaire were only used in one study each. Mental health aspects included alcohol consumption, anger, anxiety, attachment to social relationships, cigarette smoking, coping strategies, death anxiety, depressive symptoms, emotional aspects limiting functioning, general psychological well-being, hopelessness, hostility, indirect life-threatening behavior, life satisfaction, meaning in life, optimism, satisfaction with life, self-esteem, social isolation, stress, suffering, and suicidal ideation. The majority of the mental health parameters were assessed using self-developed scales (26.5%) or specific instruments, including the GDS (21.6%), CES-D (12.7%), Hamilton Rating Scale for Depression (3.9%), Death Anxiety Scale (3.9%), Life Satisfaction Scale (2.9%), Beck Anxiety Inventory (2%), Suicidal Ideation Scale (2%), and Beck Hopelessness Scale (2%).
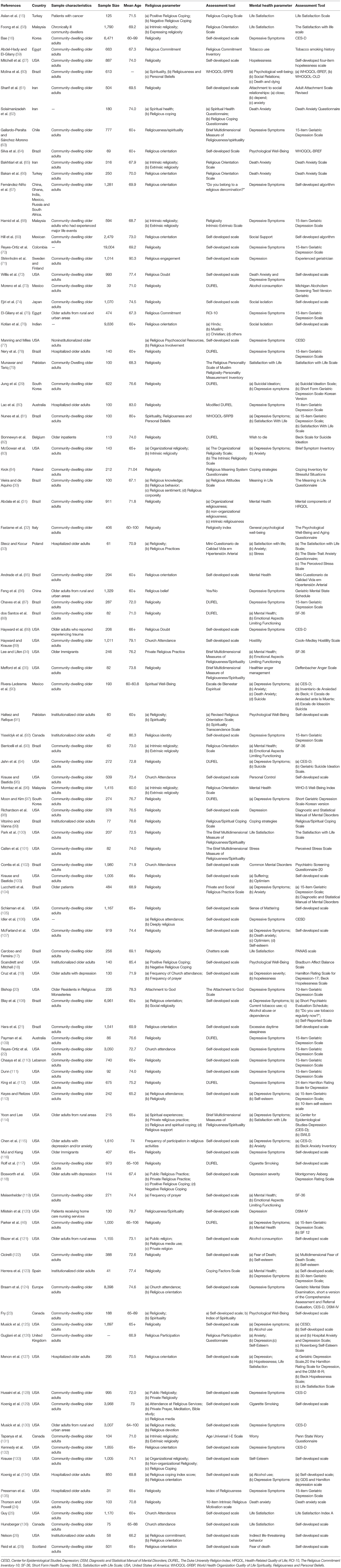
Table 1. Main characteristics of the cross-sectional and case-control studies that investigated the association between religious activities and mental health.
The main characteristic of the studies that investigated the association between spirituality and mental health is shown in Table 2. Twenty-seven studies investigated the association between spirituality and mental health parameters (63, 73, 100, 137–147, 149–161). Two investigations studied both religiosity and spirituality (63, 73). A total of 13,015 community-dwelling and institutionalized older adults with a mean age of 75.1 years (ranging from 70.3 to 83.1 years) from Belgium, Brazil, Bulgaria, Chile, England, Iran, Korea, Mexico, Pakistan, Portugal, Romani, Spain, Taiwan, Turkey, and the USA were studied. Native people and immigrants were investigated in one study each. Spirituality was assessed in 37.0% of the studies, spiritual well-being in 29.6%, RS in 26%, and spiritual belief in 7.4%. Spirituality was predominantly assessed using The Spiritual Well-being Scale (25.9%), followed by self-developed scales (18.5%), The Brief Multidimensional Measure of RS (18.5%), and The Spirituality Index of Well-Being (7.4%). Other scales were used in one study each. The studied mental health aspects included alcohol abuse, depressive symptoms, emotional aspects limiting functioning, happiness, hope, global mental health, optimism, fear of death and dying, positive mental well-being, psychological well-being, meaning in life, satisfaction with life, sense of suffering, and spiritual distress high heterogeneity was observed among the instruments used to assess mental health parameters. The most predominant scales were The CES-D, The GDS, The SF-36, seethe lf-developed scales, The Satisfaction with life scale, and The WHOQOL-BREF/WHOQOL-OLD.
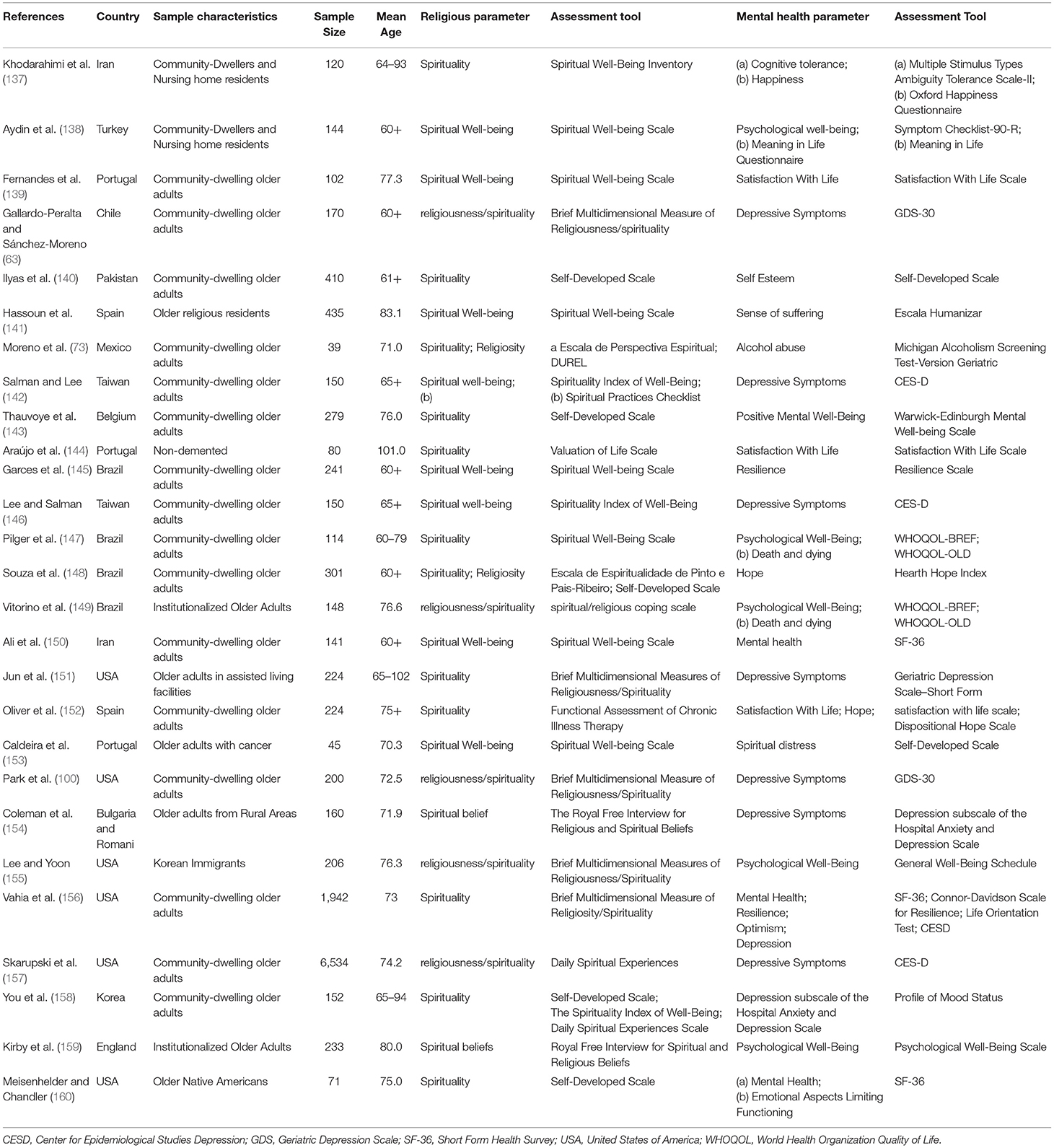
Table 2. Main characteristics of the cross-sectional studies that investigated the association between spiritual activities and mental health.
Table 3 provides the main characteristics of the included longitudinal studies. One study provided cross-sectional and longitudinal data (92). Eight studies (92, 162–168) that involved 12,067 community-dwelling older adults with a mean age of 72.3 years (ranging from 68.3 to 75.6 years) from Australia, England, Korea, Taiwan, and the USA were included. RS parameters included attachment to God, religious participation, religious identity, religious orientation, religious activities, religious coping, and church attendance. These parameters were assessed using self-developed scales and the DURAL index. The main outcome studied was depressive symptoms (75%), followed by death anxiety (12.5%) and mental health (12.5%). Mental health parameters were assessed using self-developed scales, CES-D, GDS, and the National Institute of Mental Health (NIMH) Diagnostic Interview Schedule.
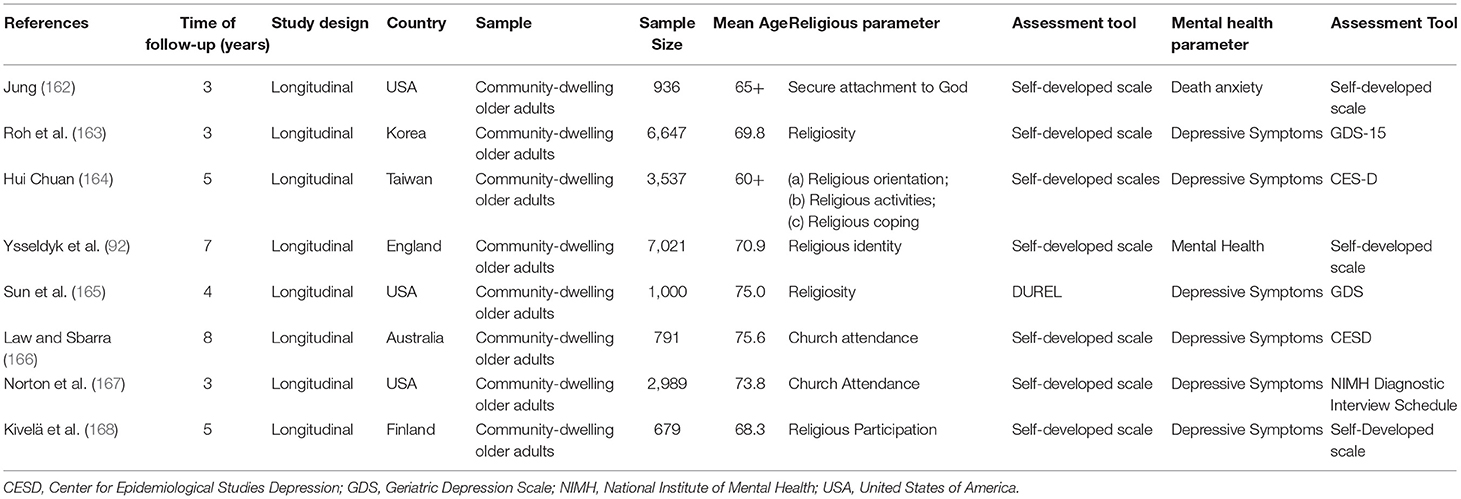
Table 3. Main characteristics of the longitudinal studies that investigated the association between religious/spiritual activities and mental health.
The overall quality assessment of cross-sectional studies is shown in Supplementary Material 4. Overall scores varied from 3 to 9. All studies defined the research question (item 1), clearly specified and defined the study population (item 2), and used valid and reliable instruments to assess RS (item 9) and mental health aspects (item 11). Most studies (58.7%) uniformly applied the eligibility criteria and recruited participants in the same population at the same period (item 4). On the other hand, different levels of exposition (35.7%; item 8) and sample size justification (15.1%; item 5) were only provided in some studies. Similarly, just 32.5% of the studies had a participation rate of at least 50% (item 3), while 30.2% adjusted results according to potential confounding variables (item 14), and only 1.6% of the investigations were conducted with assessors blinded to the exposure of participants (item 12). No studies assessed RS more than once (item 10). One study had a case-control design and received an overall quality score of 9 points.
The overall quality assessment of longitudinal studies is shown in Supplementary Material 5. Quality scores varied from 7 to 11. All studies defined the research question (item 1), clearly specified and defined the study population (item 2), measured the exposure of interest before the outcome being measured (item 6), used a sufficient timeframe to reasonably expect the development of the studied outcomes (item 7), and used valid and reliable instruments to assess RS (item 9) and mental health aspects (item 11). Most studies had a participation rate of at least 50% (63%; item 3), uniformly applied the eligibility criteria and recruited participants in the same population at the same period (88%; item 4), and measured different levels of exposition (63%; item 8). Results were adjusted according to potential confounding variables in 50% of the investigations (item 14). One study presented a loss to follow-up after baseline ≤ 20% (item 13). Neither of the studies justified the sample size (item 5) or assessed RS more than once (item 10). Any investigation described if assessors were blinded to exposure (item 12).
The detailed risk of bias assessment is shown in Supplementary Material 6. The overall risk of bias in cross-sectional studies ranged from 3 to 9 (low to high). As per protocol, all studies used validated or well-described tools to measure RS and mental health aspects. Insufficient sample size justification was the most prevalent bias (84.1%), followed by unsatisfactory statistical analysis (69.0%), insufficient description of respondents' rate (66.7%), and representativeness of the studied sample (42.1%). The case-control study had a mean risk of bias classified as moderate.
Cohort studies had a mean risk of bias that ranged from 5 to 8 points (good). All studies investigated sample representatives or somewhat representatives of the population, recruited participants of the non-exposed cohort from the same community, used a structured interview for assessing the exposure, demonstrated that the outcome of interest was not present at the start of the study, and used a follow-up long enough to allow the occurrence of study outcomes. However, only 25% of the investigations assessed study outcomes using an independent blind assessor, while most studies used self-report. Finally, most of the studies (87.5%) had a follow-up rate of <80% or did not provide a clear statement.
Five studies investigated the association between RS and alcohol consumption (73, 108, 121, 125, 134). Moreno et al. (73) observed that religiosity, but not spirituality, was negatively associated with alcohol consumption in Mexican older adults. In addition, Koenig et al. (134) observed that religious coping was negatively associated with alcohol abuse in old males. Musick et al. (125) noted that Baptists' older adults who lived in rural areas were less likely to drink alcohol than their counterparts from urban areas. According to the authors, these results occurred in function of higher service attendance levels. Analyzing the same cohort, Blazer et al. (121) expanded previous results by indicating that public religious activities were associated with alcohol abstinence in white and black Baptists. In contrast, Blay et al. (108) did not observe significant associations between religious affiliation, and social religiosity, have experienced religious changes, and have religion as an orienting-motivating force with alcohol abuse and dependency in Brazilian older adults.
The association between RS and anxiety is shown in Figure 2. The pooled analysis of six studies indicated a significant and negative association between RS and anxiety (Z-score = −0.057, 95 % CI = −0.111–0.003, P = 0.037).
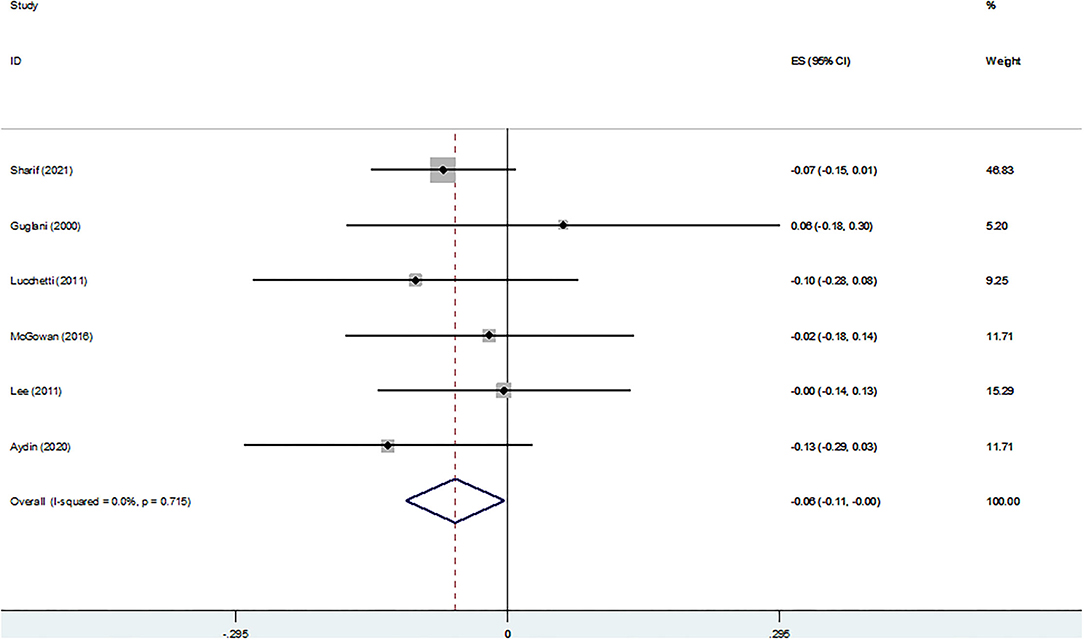
Figure 2. Z-scores for anxiety.
Figure 3 shows the association between religiosity and death anxiety. The pooled analysis of seven studies indicated a non-significant association (Z-score = −0.031, 95 % CI = −0.064–0.002, P = 0.067).
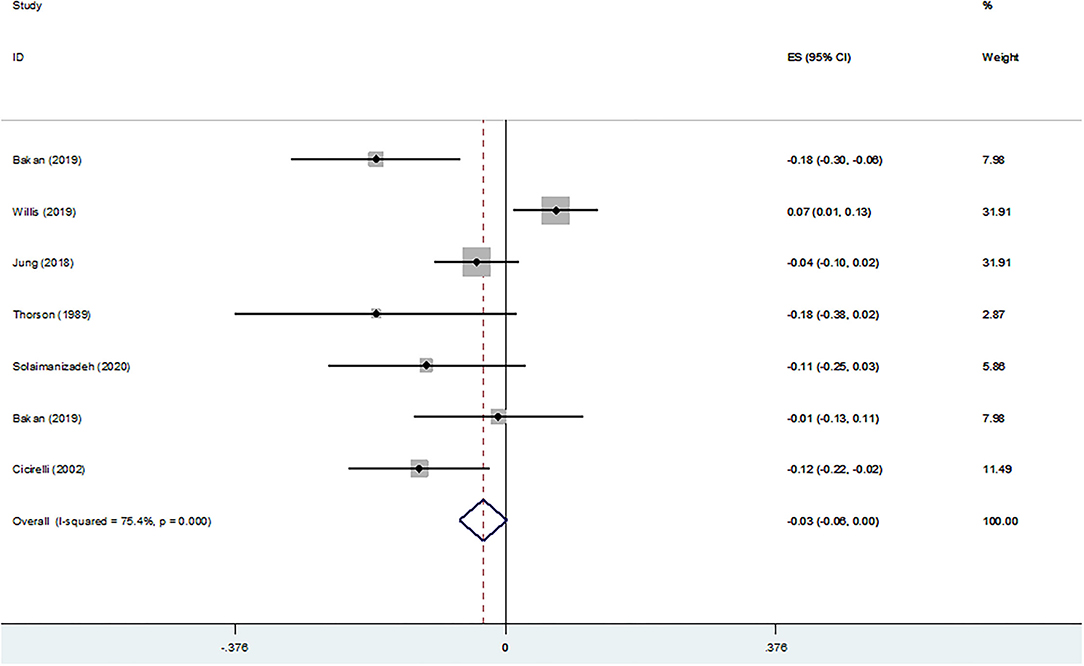
Figure 3. Z-scores for death anxiety.
Figure 4 shows the cross-sectional association between RS and depressive symptoms according to continuous data. A non-significant association between ORA (Z-score = −0.032, 95 % CI = −0.068–0.004, P = 0.079), ORA-based DUREL scores (Z-score = −0.042, 95 % CI = −0.087–0.002, P = 0.062), service attendance (Z-score = −0.013, 95 % CI = −0.073–0.047, P = 0.662), NORA (Z-score = −0.003, 95 % CI = −0.039–0.033, P = 0.889), NORA-based DUREL scores (Z-score = 0.003, 95 % CI = −0.042–0.049, P = 0.883), IR (Z-score = −0.024, 95 % CI = −0.057–0.008, P = 0.145), IR-based DUREL scores (Z-score = −0.010, 95 % CI = −0.052–0.033, P = 0.660), religious (Z-score = −0.044, 95 % CI = −0.092–0.004, P = 0.073), religious affiliation (Z-score = −0.039, 95 % CI = −0.110–0.031, P = 0.274), religious devotion (Z-score = −0.037, 95 % CI = −0.108–0.033, P = 0.297), and spiritual aspects (Z-score = −0.046, 95 % CI = −0.097–0.005, P = 0.080) and depressive symptoms was observed. In contrast, a significant and negative association was observed with spirituality (Z-score = −0.079, 95 % CI = −0.157–0.002, P = 0.045).

Figure 4. Z-scores for (A) ORA, (B) ORA-based DUREL scores, (C) service attendance, (D) NORA, (E) NORA-based DUREL scores, (F) IR, (G) IR-based DUREL scores, (H) religious, (I) religious, (J) religious devotion, (K) spiritual aspects, and (L) spirituality.
Figure 5 shows the cross-sectional association between RS and depressive symptoms according to binary data. No significant associations between NORA (OR = 1.54; 95 % CI = 0.53–4.51, P = 0.43; χ2 = 42.84, df = 4; I2 = 91%; P < 0.00001), service attendance (OR = 0.85; 95 % CI = 0.70–1.03, P = 0.10; χ2 = 0.77, df = 2; I2 = 0%; P = 0.68), ORA (OR = 0.98; 95 % CI = 0.92–1.03, P = 0.40; χ2 = 2.48, df = 5; I2 = 0%; P = 0.78), and private religious practice (OR = 0.95; 95 % CI = 0.86–1.04, P = 0.27; χ2 = 1.66, df = 2; I2 = 0%; P = 0.44) and depressive symptoms were observed. On the other hand, a lower prevalence of depressive symptoms was observed in older adults with high IR (OR = 0.86; 95 % CI = 0.76–0.97, P = 0.02; χ2 = 0.84, df = 3; I2 = 0%; P = 0.84) and those affiliated to any religion (OR = 0.82; 95 % CI = 0.70–0.95, P = 0.009; χ2 = 4.33, df = 4; I2 = 8%; P = 0.36).
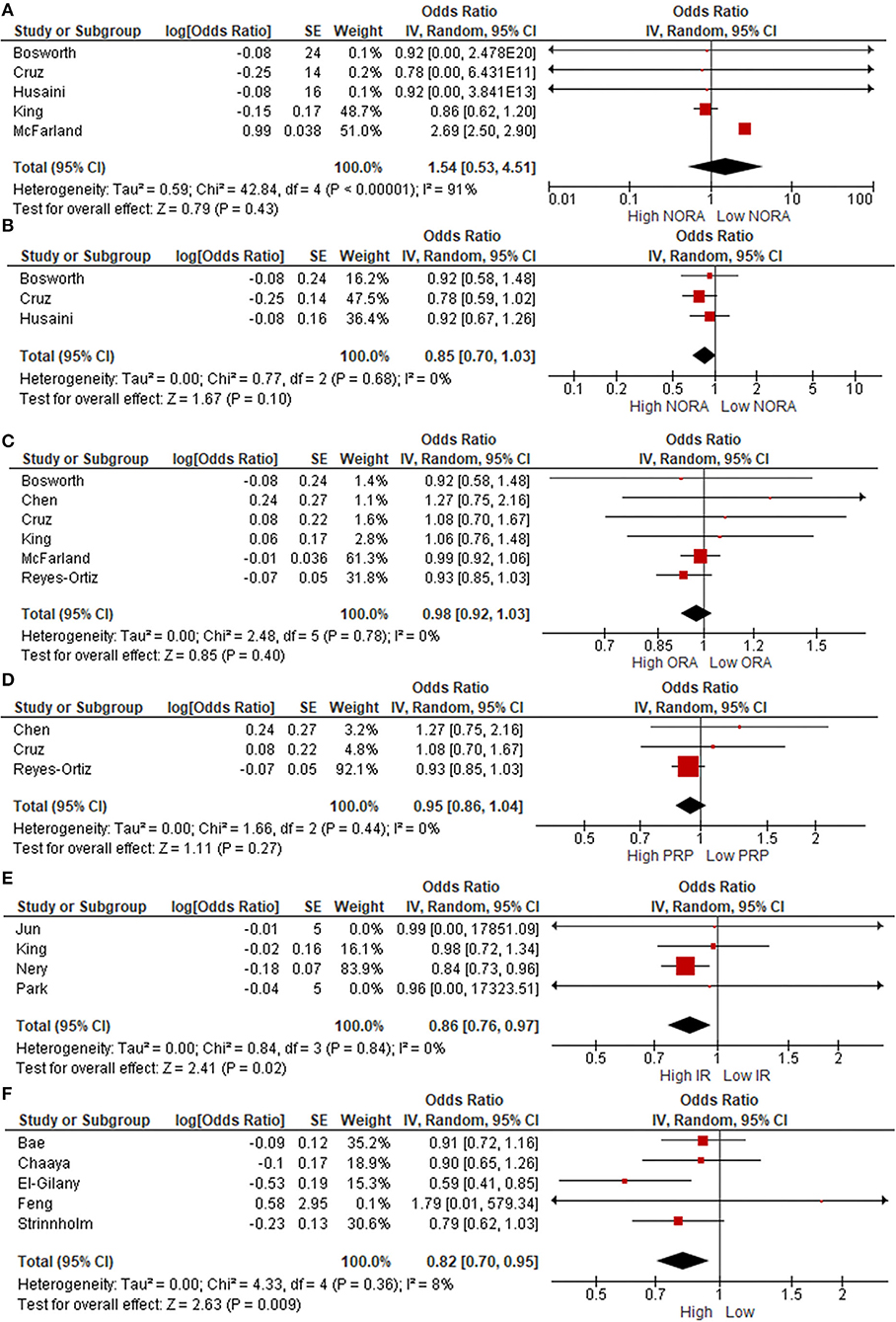
Figure 5. Odds Ratio (OR) for (A) NORA, (B) service attendance, (C) ORA, (D) private religious practices (PRP), (E) intrinsic religiosity, and (F) religious affiliation.
Three studies investigated the association between religious aspects and hopelessness. Menon et al. (127) observed a higher prevalence of hopelessness in male hospitalized older veterans with low religious levels. Cruz et al. (19) noted that prayer, but not church attendance, was significantly associated with a lower prevalence of hopelessness in older adults who attended geriatric inpatient units and outpatient clinics. More recently, Mitchell et al. (27) analyzed a cohort of 887 black men who participated in the Health and Retirement Study. The authors noted that participants with high religious attendance and religiosity had lower hopelessness levels.
Figure 6 shows the cross-sectional association between life satisfaction and religiosity. The pooled analysis of five studies indicated a positive and significant association (Z-score = 0.086, 95 % CI = 0.027–0.144, P = 0.004).
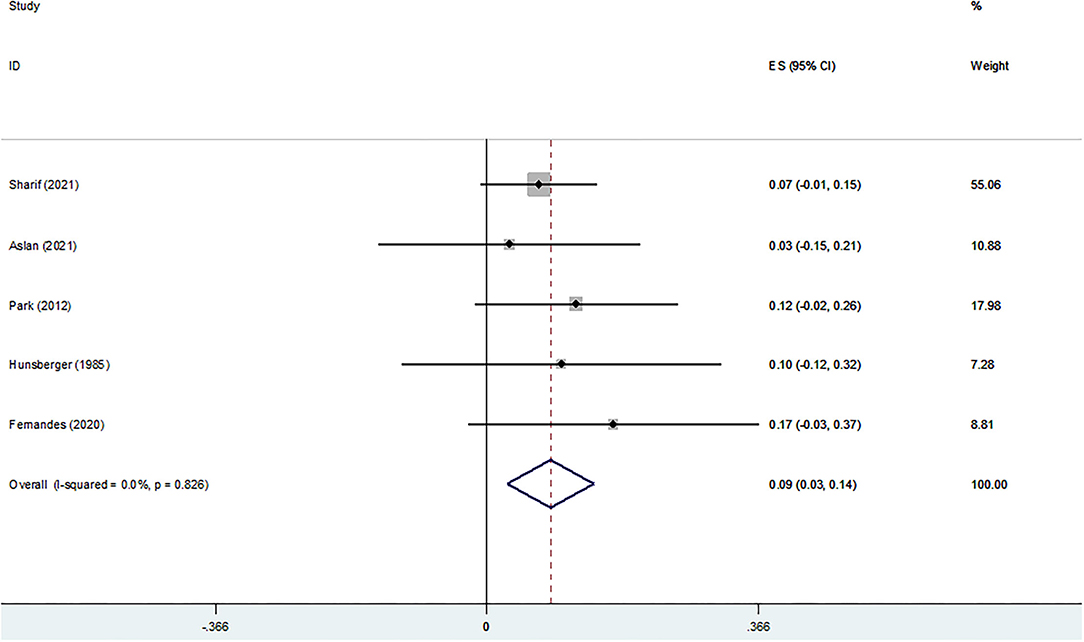
Figure 6. Z-scores for life satisfaction.
Figure 7 shows the association between RS and meaning in life. The pooled analysis was conducted with three studies and the results indicated a significant association (Z-score = 0.325, 95 % CI = 0.259–0.391, P = 0.0001).
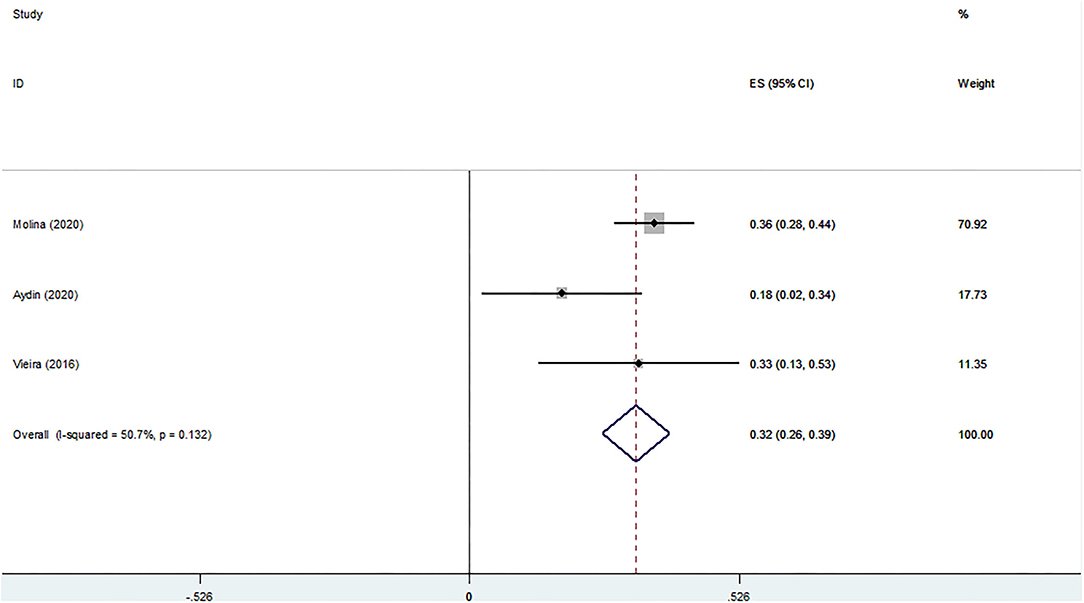
Figure 7. Z-scores for meaning in life.
Three studies investigated the association between RS and global mental health. Two studies assessed global mental health using the subscale of the SF-36 (160, 169), while one study used the subscale of the SF-12 (46). Meisenhelder and Chandler (160) reported a significant association between the frequency of prayer and the importance of faith with general mental in older native people. Parker et al. (46) noted a significant association between ORA, but not NORA and IR, and general mental health in community-dwelling older adults. Investigating older Korean immigrants, Lee et al. (169) reported that spiritual coping was negatively associated with general mental health. However, no significant relations were noted with private religious practice.
Figure 8 shows the association between psychological well-being and RS. A significant association was observed (Z-score = 0.108, 95 % CI = 0.054–0.162, P = 0.0001).

Figure 8. Z-scores for psychological well-being.
The association between self-esteem and RS was investigated in three studies. Guglani et al. (126) examined Asian Hindu grandmothers who lived in London and observed that religious participation was not significantly associated with self-esteem. Similar results were found by Krause et al. (133), who noted no effects of NORA and ORA on self-esteem. However, significant associations were observed with religious coping. Keyes et al. (113) supported these results by indicating that neither religious attendance nor religiosity, but religious identity, was associated with self-esteem.
Figure 9 shows the cross-sectional association between RS and social relations according to continuous data. The pooled analysis of four studies indicated a significant association (Z-score = 0.052, 95 % CI = 0.021–0.083, P = 0.001).
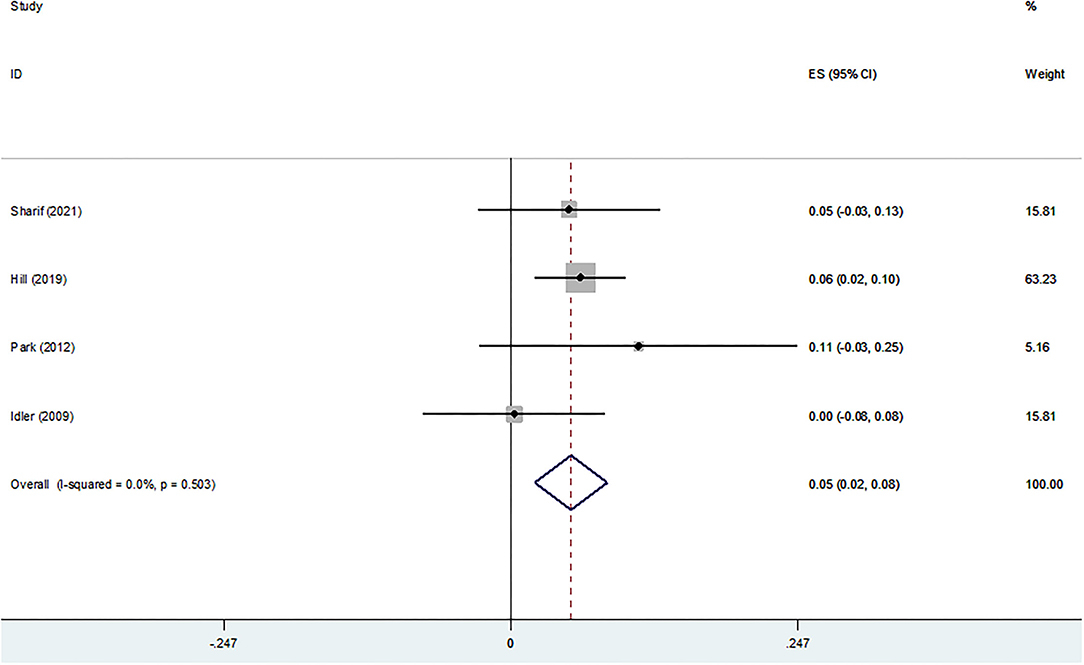
Figure 9. Z-scores for social relations.
Figure 10 shows the cross-sectional association between RS and social relations according to binary data. No significant associations between religious levels and social health were observed (OR = 0.78; 95 % CI = 0.58–1.05, P = 0.10; χ2 = 60.79, df = 2; I2 = 97%; P < 0.00001).

Figure 10. Odds Ratio (OR) for social relations.
The association between suicidal ideation and RS was investigated in four studies. Rivera-Ledesma and Montero-Lòpez Lena (90) noted that vital spirituality and dissatisfaction were associated with suicidal ideation in Pentecostal Mexican older adults. Moreover, Bonnewyn et al. (82) identified that private religiousness was associated with the wish to die in patients admitted to a psychiatry department. In contrast, Jahn et al. (94) did not observe significant relations between DUREL scores and the Geriatric Suicide Ideation Scale (GSIS). These results were partially supported by Jung et al. (29), who observed no significant effects of NORA and ORA on suicidal ideation, although a negative association was observed with IR.
Three studies investigated the association between tobacco use and religiosity. Abdel-Hady and El-Gilany (59) reported that low religiosity increased the likelihood of tobacco smoking use in Egyptian older adults. Lee Roff et al. (117) conducted an analysis according to religious aspects and noted that both NORA and ORA were negatively associated with cigarette smoking. Similarly, Blay et al. (108) observed a lower prevalence of tobacco users in participants who had experienced religious changes, have religion as an orienting-motivating force, have any religious affiliation and high social religiosity.
The funnel plot for depressive symptoms is shown in Supplementary Material 6. No publication bias was identified according to Egger's test (P = 0.836).
One study investigated the association between religiosity and death anxiety. Jung et al. (162) analyzed data from the Religion, Aging, and Health Survey and observed that secure attachment to God was associated with a lower risk of developing death anxiety 3 years later.
The longitudinal effects of religion on depressive symptoms were studied in six studies. Kivela et al. (168) investigated two waves (1984–1985 and 1989–1990) of Older Finns and noted that low religious participation increased the risk of depression in women, but not in men. These results were further expanded by Norton et al. (167), Law and Sbarra (166), Sun et al. (165), and Roh et al. (170) who observed that older adults with higher church attendance had a reduced risk of developing depression and depressive symptoms in a short-time-interval. Hui-Chuan (164) investigated the role of NORA on the severity of depressive symptoms over a 4-year follow-up period. Authors reported that prayer and reading the scriptures were associated with reduced depressive symptoms, whereas praying for calmness and praying for help were accompanied by a significant increase in depressive symptoms.
One study investigated the association between religion and mental health. In this investigation, Ysseldyk et al. (92) conducted a 6-year follow-up and observed that religious identity was significantly associated with better mental health.
RS is a social phenomenon that might be expressed across a plethora of activities, depending on individuals' desires, beliefs, motivation, needs, accessibility, availability, and recognition, to quote a few variables. Participation and adherence to religious practices might influence numerous health-related parameters, including mental health. This scenario is important because older adults are commonly very religious and particularly susceptible to mental health problems. However, until now, no prior investigations have provided a clearly evidence-based scenario on the association between RS and mental health in older adults.
Our results indicate that RS is significantly associated with many mental health parameters, including anxiety, depressive symptoms, life satisfaction, meaning in life, social relations, and psychological well-being. In addition, investigations provided encouraging longitudinal results regarding the effects of RS on death anxiety, depressive symptoms, and general mental health.
Results of the current study indicate that RS was negatively associated with anxiety. Numerous RS-related parameters might contribute to the attenuation of anxiety symptoms. Generalized and social anxiety, for example, are associated with loneliness in community-dwelling older adults (171, 172). In contrast, ORA is expected to provide a favorable environment for expanding the social network and creating intimate relationships. Experts in the field have suggested that religious communities might serve as an extension of the biological family (173, 174). Increased self-care is another possible candidate to explain the current results, given that anxiety is significantly associated with the prevalence of chronic diseases (175), whereas RS doctrine and philosophy are frequently concentrated on healthy lifestyle habits, avoiding the excessive consumption of tobacco, alcohol, and food (47). Notably, anxiety and depressive symptoms are usually observed simultaneously in older patients since they share many clinical symptoms and psychosocial and neurobiological mechanisms (176, 177). Hence, the possibility that changes in anxiety are secondary to improvements in depressive symptoms might not be ruled out. However, specific religious parameters were not investigated in the included studies hindering a better understanding of this scenario.
We observed that RS parameters were negatively associated with depressive symptoms. Particularly, older adults with high spirituality had fewer depressive symptoms in comparison to their counterparts. Furthermore, IR and religious affiliation were negatively associated with the prevalence of depressive symptoms. These results were supported by longitudinal studies, which reported that more religious and spiritual people had a lower risk of developing depression and worsening depressive symptoms. Taken together, these data indicate that approaching life according to the belief in the presence of the Divine (e.g., nature, energy, God) might be negatively associated with depressive symptoms in older adults.
The possibility that RS activities might contribute to coping with adverse life events has long been discussed in the literature, and many possible mediators have been suggested to explain this association. Giving meaning to suffering, for instance, can provide a cognitive framework to understand and manage negative life experiences (37, 178). Numerous religions explain suffering as an opportunity for purification, learning, and personal growth, in an attempt to escape from punishment and obtain awards in the current and/or in the afterlife (37, 178). This perspective was exhaustively discussed by Weber (14), who pointed out that this mechanism is similarly observed in the major religious groups worldwide.
RS might also reduce depressive symptoms by providing guidance and support in moments of frustration and despair. This scenario is based on the perception that the Divine is taking care of peoples' lives and that everything occurs according to a better purpose, even if sometimes humans cannot understand God's plan (37, 178). This scenario was well-illustrated in the discourse of a 61-year-old Peruvian Woman examined by Flores-Flores et al. (179), who explained that God was her psychologist and that she prayed to him every night to take her negative feelings away from her, and, according to her, little by little, they went away (179). In other cases, believing in the occurrence of spiritual experiences seemed to provide comfort and conciliation. Alaska native older adults who have experienced grieving mentioned that they constantly feel the presence of dead relatives by seeing lights or hearing voices and that these events contribute to coping with the losses (180).
Religious groups might also provide guidance and support by providing instructions of how people can go through difficult times and how religious communities can give support in these moments (37). The Jewish tradition is a good illustration of this scenario by describing structured, graduated, and linear periods by which people are likely to pass through in the course of mourning (181). Such perspective takes into consideration the numerous feelings that might be experienced during this period, and indicate the tasks that might be conducted by familiars to cope with the stages of grief (181). The Jewish community, in its turn, is advised about the best moments in which they can provide comfort and companionship (181).
Giving meaning to suffering is another potential mechanism by which RS can reduce depressive symptomatology (49, 178). Finding meaning in life is recognized as an important element in the maintenance of mental health by offering coherence in peoples' lives. This concept has been incorporated as a key component of the theoretical bases of many psychological schools. In logotherapy, the third Viennese school of psychotherapy, Frankl (182) proposed that finding meaning in life is the primary motor force of human beings. This perspective describes that people must take control and be responsible for all decisions concerning their lives, instead of acting passively, regardless of the circumstances. In contrast, the inability to identify meaning in life might trigger the development of numerous mental health problems, including depression. A complementary view is provided by Erikson (183), on his theory of psychosocial development. According to him, older adults that are unable to give meaning to their accomplishments in life tend to become desperate, hopeless, and depressive (183).
These premises also provide light to justify the significant association between death anxiety and religiosity (162), given that failure to understand life's meaning may produce a psychologically stressful environment that promotes an increase in death anxiety (184, 185). This point of view was explored by Becker (186) in the death deny theory. It describes that finding meaning in life has a vital role as a symbolic defense against the notion of mortality and consequently death anxiety (184, 185).
Finally, religious and spiritualist people might live their lives according to a transcendent approach, reducing the excessive focus on the self and changing the attention to other people with worse suffering (178). Focus on other people's well-being can increase the feeling of connection with high power and serve as a life purpose (178). Such attitude might impact depressive symptoms, given the close association between personality traits with a high self-conscious component and depression (187).
It is important to note that numerous other parameters might have impacted the negative association between IR and depression, such as NORA and ORA. However, the cross-sectional design of the included studies prevents us from making strong assumptions and points out the need for longitudinal studies.
Another major finding of the present study is that RS was significantly associated with numerous positive feelings, including life satisfaction, meaning in life, social relations, and psychological well-being. As no specific RS elements (e.g., NORA, ORA, IR) were investigated it is hard to suggest the main mechanisms underlying these associations. Nevertheless, social relations are predominately influenced by the feeling of belonging, worship and mutual spiritual support produced by ORA (188). In contrast, life satisfaction and meaning in life are affected by many variables, such as social, affective and psychological aspects (189).
Psychological well-being, in its turn, is a large multidimensional construct that dependents on the combination of emotional status, personality traits, and life experiences (188). Prior studies have suggested that RS might influence psychological well-being by modulating perceived control (190), positive emotions (191), social support (96), and coping mechanisms (192, 193). Furthermore, the impact of numerous indirect mechanisms associated with self-care might not be ruled out (41, 47).
Older patients' management is commonly based on pharmacological therapy and gerontologists have claimed that understanding the role of RS beliefs on peoples' health might contribute to better and more qualified care (194). Such criticism is based on the fact that older adults have mentioned that they would feel better if health professionals responsible for their care tried to include their personal beliefs in the treatment (48). However, most health professionals do not have basic knowledge in this field (48), although it might be essential in some contexts. Hospitalized patients, for example, often ask if their disease is a divine punishment and whether God will take care of them (195).
Our findings encourage health professionals to understand patients' beliefs and search for the best method to include RS elements in the therapeutic approach. Notably, NORA and ORA had a small direct impact on mental health parameters, whereas IR substantially influenced depressive symptomatology. These results might indicate that RS-based approaches to managing depressive symptoms in older adults should preferably allow patients to internalize, reflect, discuss, and solidify their personal beliefs than stimulate the adherence to religious events and the practice of private religious activities. In other cases, where was not possible to identify which RS elements were associated with better mental health status, such as anxiety, health professionals should try to distinguish which activities would make older adults feel more confident and comfortable.
The present study also detected important aspects that must be considered for future research. A fundamental observation is that most investigations have assessed RS using general scores and have not taken into consideration the importance of individual dimensions. This scenario limits the creation of more specific recommendations for health professionals responsible for the care of older adults. On the other hand, numerous dimensions have been tested against depressive symptoms, allowing us to indicate the most associated parameters. Hence, our results must be tested in large randomized clinical trials comparing RS-based treatments organized according to different dimensions (e.g., IR vs. NORA/ORA).
Another interesting point is that data from the systematic review suggested that most cross-sectional investigations showed that RS might be negatively associated with alcohol intake, tobacco use, and hopelessness. These findings are encouraging and suggest that RS might be a larger role in mental health status than those reported in the current study. However, the small number of evidence impeded us to conduct pooled and stratification analyses followed by heterogeneity and publication bias verification. In addition, not all investigations supported significant associations among the variables, indicating that conclusions must be taken carefully and that more studies are still necessary.
Numerous limitations restrict our findings. First, the majority of studies have a cross-sectional design and causality cannot be inferred. Second, results were predominately based on multidimensional scores and did not take into consideration specific RS elements. Third, the limited number of investigations impeded us to conduct pooled analysis for longitudinal studies and investigate publication bias and the sources of heterogeneity in other variables than depressive symptoms. Fourth, Z-scores were obtained by converting Pearson's correlation scores, which were not corrected according to possible covariables. Fifth, OR and Z-scores were not converted into a unique ES. Although we could have conducted this analysis using statistical methods, experts in the field have suggested that it is associated with a high risk of bias and might provide misleading results, mainly when studies provide low power and similar rates of cases and controls (51). Sixth, some ES were estimated by conversions. Seventh, many studies did not perform statistical regressions according to important covariables, including disease severity, drug treatment, physical activity levels, and dietary habits. Eight, the possible differences in mental health parameters among specific religious affiliations were not investigated. This aspect is important because a high prevalence of mental health problems has been observed in some religious contexts (196) due to the presence of rigid thinking, overdependence on laws and rules, and an emphasis on guilt and sin (37). Ninth, RS and mental health parameters were operationalized using different methods and they may have capture different dimensions. Tenth, we combined studies that have investigated alcohol and tobacco use and abuse. Eleventh, most studies involved community-dwelling older adults and our findings should be carefully extrapolated to hospitalized, institutionalized, and native people (119). Seventh, the present study investigated mental health parameters, and future studies are necessary to explore the association between RS with brain disorders and diseases. Finally, spirituality was poorly investigated.
Our findings suggest that RS activities are significantly associated with mental health in older adults. Specifically, people with high RS levels had lower anxiety and depressive symptoms, as well as higher life satisfaction, meaning in life, social relations, and psychological well-being. Data provided by an increasing number of longitudinal studies have supported most of these findings.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
HC-J, RC, FP, RA, AP, EM, and VA: conceived of the present idea and results interpretation. HC-J and RC: articles' search, qualitative analysis, and quantitative analysis. EM and VA: supervision. All authors discussed the results and commented on the manuscript.
This work was partially funded by an Intramural Research Grant from the Università Cattolica del Sacro Cuore (EM), the Fundação de Apoio a Pesquisa do Distrito Federal (FAPDF), and the nonprofit research foundation Centro Studi Achille e Linda Lorenzon (to AP, EM, HC-J, and RC).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.877213/full#supplementary-material
1. Center for Disease Control Prevention. About Mental Health. (2021). Available online at: https://www.cdc.gov/mentalhealth/learn/index.htm
2. World Health Organization. Mental Health of Older Adults. (2018). Available online at: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response
3. World Health Organization. Mental Disorders. (2019). Available online at: https://www.who.int/news-room/fact-sheets/detail/mental-disorders (accessed February 6, 2022).
4. Zarit SH, Zarit JM. Mental Disorders in Older Adults : Fundamentals of Assessment and Treatment. New York: Guilford Press. (2007).
5. McCombe G, Fogarty F, Swan D, Hannigan A, Fealy GM, Kyne L, et al. Identified mental disorders in older adults in primary care: a cross-sectional database study. Eur J Gen Pract. (2018) 24:84. doi: 10.1080/13814788.2017.1402884
6. Sinha P, Hussain T, Boora NK, Rao GN, Varghese M, Gururaj G, et al. Prevalence of common mental disorders in older adults: results from the National Mental Health Survey of India. Asian J Psychiatr. (2021) 55:102463. doi: 10.1016/j.ajp.2020.102463
7. Ausín B, Muñoz M, Santos-Olmo AB, Pérez-Santos E, Castellanos MA. Prevalence of mental disorders in the elderly in the community of Madrid: results of the mentdis_ICF65+ study. Span J Psychol. (2017) 20:E6. doi: 10.1017/sjp.2017.3
8. Andreas S, Schulz H, Volkert J, Dehoust M, Sehner S, Suling A, et al. Prevalence of mental disorders in elderly people: the European MentDis_ICF65+ study. Br J Psychiatry. (2017) 210:125–31. doi: 10.1192/bjp.bp.115.180463
9. Goldberg SE, Whittamore KH, Harwood RH, Bradshaw LE, Gladman JRF, Jones RG. The prevalence of mental health problems among older adults admitted as an emergency to a general hospital. Age Ageing. (2012) 41:80. doi: 10.1093/ageing/afr106
10. Kułak-Bejda A, Bejda G, Waszkiewicz N. Mental disorders, cognitive impairment and the risk of suicide in older adults. Front Psychiatry. (2021) 12:695286. doi: 10.3389/fpsyt.2021.695286
11. Mezuk B, Rock A, Lohman MC, Choi M. Suicide risk in long-term care facilities: a systematic review. Int J Geriatr Psychiatry. (2014) 29:1198–211. doi: 10.1002/gps.4142
12. The Lancet Global Health. Mental health matters. Lancet Glob Heal. (2020) 8:e1352. doi: 10.1016/S2214-109X(20)30432-0
13. Carpenter BD, Gatz M, Smyer MA. Mental health and aging in the 2020s. Am Psychol. (2021) doi: 10.1037/amp0000873
15. Aslan G, Bakan AB, Kilic D. An investigation of the relationship between religious coping and life satisfaction in oncology patients aged 65 and over. Psychogeriatrics. (2021) 21:279–87. doi: 10.1111/psyg.12661
16. Bae S-M. Factors associated with depressive symptoms among elderly Koreans: the role of health status, work ability, financial problems, living alone, and family relationships. Psychogeriatrics. (2020) 20:304–9. doi: 10.1111/psyg.12499
17. Cardoso MCS, Ferreira MC. Envolvimento religioso e bem-estar subjetivo em idosos TT - Implicación religiosa y bienestar subjetivo en los mayores TT - religious involvement and elderly subjective well-being. Psicol Cienc Prof. (2009) 29:380–93. doi: 10.1590/S1414-98932009000200013
18. Scandrett KG, Mitchell SL. Religiousness, religious coping, and psychological well-being in nursing home residents. J Am Med Dir Assoc. (2009) 10:581–6. doi: 10.1016/j.jamda.2009.06.001
19. Cruz M, Schulz R, Pincus HA, Houck PR, Bensasi S, Reynolds CF III. The association of public and private religious involvement with severity of depression and hopelessness in older adults treated for major depression. Am J Geriatr Psychiatry. (2009) 17:503–7. doi: 10.1097/JGP.0b013e31819d37a9
20. Bishop AJ. Stress and depression among older residents in religious monasteries: do friends and God matter? Int J Aging Hum Dev. (2008) 67:1–23. doi: 10.2190/AG.67.1.a
21. Hara C, Rocha FL, Costa É de C. e, Fuzikawa C, Uchoa E, Lima-Costa MF. Prevalence of excessive daytime sleepiness in Brazilian community-dwelling older adults with very low levels of schooling, and its association with sociodemographic characteristics and lifestyle: the Bambuí Health and Ageing Study (BHAS) TT – prevalência. J Bras Psiquiatr. (2008) 57:91–7. doi: 10.1590/S0047-20852008000200002
22. Reyes-Ortiz CA, Berges IM, Raji MA, Koenig HG, Kuo Y-F, Markides KS. Church attendance mediates the association between depressive symptoms and cognitive functioning among older Mexican Americans. J Gerontol A Biol Sci Med Sci. (2008) 63:480–6. doi: 10.1093/gerona/63.5.480
23. Fry PS. The unique contribution of key existential factors to the prediction of psychological well-being of older adults following spousal loss. Gerontologist. (2001) 41:69–81. doi: 10.1093/geront/41.1.69
24. Thorson JA, Powell FC. Death anxiety and religion in an older male sample. Psychol Rep. (1989) 64:985–6. doi: 10.2466/pr0.1989.64.3.985
25. Guy RF. Religion, physical disabilities, and life satisfaction in older age cohorts. Int J Aging Hum Dev. (1982) 15:225–32. doi: 10.2190/3C3M-CBVK-KTVH-BDNG
26. Nelson FL. Religiosity and self-destructive crises in the institutionalized elderly. Suicide Life Threat Behav. (1977) 7:67–74.
27. Mitchell UA, Gutierrez-Kapheim M, Nguyen AW, Al-Amin N. Hopelessness among middle-aged and older blacks: the negative impact of discrimination and protecting power of social and religious resources. Innov Aging. (2020) 4:igaa044. doi: 10.1093/geroni/igaa044
28. Reid WS, Gilmore AJ, Andrews GR, Caird FI. A study of religious attitudes of the elderly. Age Ageing. (1978) 7:41–5.
29. Jung J, Roh D, Moon YS, Kim DH. The moderating effect of religion on the relationship between depression and suicidal ideation in the elderly. J Nerv Ment Dis. (2017) 205:605–10. doi: 10.1097/NMD.0000000000000637
30. Vieira DCR, de Aquino TAA. Vitalidade subjetiva, sentido na vida e religiosidade em idosos: um estudo correlacional TT - Vitalidad subjetiva, sentido en la vida y religiosidad en los ancianos: un estudio correlacional. Temas Psicol. (2016) 24:483–94. doi: 10.9788/TP2016.2-05Pt
31. Abdala GA, Kimura M, Duarte YA de O, Lebrão ML, dos Santos B. Religiosidade e qualidade de vida relacionada à saúde do idoso. Rev Saude Publica. (2015) 49:77–98. doi: 10.1590/s0034-8910.2015049005416
32. Fastame MC, Hitchcott PK, Penna MP. Does social desirability influence psychological well-being: perceived physical health and religiosity of Italian elders? A developmental approach. Aging Ment Health. (2017) 21:348–53. doi: 10.1080/13607863.2015.1074162
33. Stecz P, Kocur J. Religiousness, religious coping with illness, and psychological function among Polish elderly patients with osteoarthritis undergoing arthroplasty. J Relig Health. (2015) 54:554–70. doi: 10.1007/s10943-014-9842-2
34. Lee T-F, Lifen W. God changed their lives: the value of religion in the elderly. J Christ Nurs. (2014) 31:36–9. doi: 10.1097/CNJ.0000000000000029
35. Mefford L, Thomas SP, Callen B, Groer M. Religiousness/Spirituality and anger management in community-dwelling older persons. Issues Ment Heal Nurs. (2014) 35:283–91. doi: 10.3109/01612840.2014.890472
36. Braam AW, Koenig HG. Religion, spirituality and depression in prospective studies: a systematic review. J Affect Disord. (2019) 257:428–38. doi: 10.1016/j.jad.2019.06.063
37. Dein S. Religion, spirituality and depression: implications for research and treatment. Prim Care Community Psychiatry. (2006) 11:67–72. doi: 10.1185/135525706X121110
38. Glas G. Anxiety, anxiety disorders, religion and spirituality. South Med J. (2007) 100:621–5. doi: 10.1097/SMJ.0b013e31805fe612
39. Koenig HG. Research on religion and mental health in later life: a review and commentary. J Geriatr Psychiatry. (1990) 23:23–53.
40. Koenig HG. Research on religion, spirituality and mental health: a review. Can J Psychiatry. (2009) 54:283–91. doi: 10.1177/070674370905400502
41. Koenig HG. Depression in chronic illness: does religion help? J Christ Nurs. (2014) 31:40–6. doi: 10.1097/CNJ.0000000000000016
42. McCullough ME, Larson DB. Religion and depression: a review of the literature. Twin Res. (1999) 2:126–36. doi: 10.1375/twin.2.2.126
43. Levin J. Religion and mental health: theory and research. Int J Appl Psychoanal Stud. (2010) 7:102–15. doi: 10.1002/aps.240
44. Rosmarin D, Koenig H. Handbook of Spirituality, Religion, and Mental Health. Cambridge: Academic Press. (2020).
45. Shreve-Neiger AK, Edelstein BA. Religion and anxiety: a critical review of the literature. Clin Psychol Rev. (2004) 24:379–97. doi: 10.1016/j.cpr.2004.02.003
46. Parker M, Roff LL, Klemmack DL, Koenig HG, Baker P, Allman RM. Religiosity and mental health in southern, community-dwelling older adults. Aging Ment Heal. (2003) 7:390–7. doi: 10.1080/1360786031000150667
47. Zimmer Z, Jagger C, Chiu C-T, Ofstedal MB, Rojo F, Saito Y. Spirituality, religiosity, aging and health in global perspective: a review. SSM Popul Heal. (2016) 2:373–81. doi: 10.1016/j.ssmph.2016.04.009
48. Ferreira AG de C, Duarte TM de M, Silva AF da, Bezerra MR. Concepções de Espiritualidade e Religiosidade e a Prática Multiprofissional em Cuidados Paliativos. Rev Kairós Gerontol. (2015) 18:227–44. doi: 10.23925/2176-901X.2015v18i3p227-244
49. Lee BY, Newberg AB. Religion and health. a review and critical analysis. Zygon®. (2005) 40:443–68. doi: 10.1111/j.1467-9744.2005.00674.x
50. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. (2000) 283:2008–12. doi: 10.1001/jama.283.15.2008
51. Green S, Higgins J. Cochrane Handbook for Systematic Reviews of Interventions. (2005). Available online at: http://www.rismes.it/pdf/Cochrane_handbook 2009.rtf (accessed July 21, 2018).
52. Koenig HG, Büssing A. The Duke University Religion Index (DUREL): a five-item measure for use in epidemological studies. Religions. (2010) 1:78–85. doi: 10.3390/rel1010078
53. Study Quality Assessment Tools. NHLBI, NIH. Available online at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed December 27, 2021).
54. Modesti PA, Reboldi G, Cappuccio FP, Agyemang C, Remuzzi G, Rapi S, et al. ESH working group on CV risk in low resource settings. Panethnic differences in blood pressure in Europe: a systematic review and meta-analysis. PLoS ONE. (2016) 11:e0147601. doi: 10.1371/journal.pone.0147601
55. Wells Shea, O'Connell, Peterson W. Ottawa Hospital Research Institute (2011). Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed May 25, 2021).
56. ROBINS-I Tool | Cochrane Methods. Available online at: https://methods.cochrane.org/methods-cochrane/robins-i-tool (accessed May 25, 2021).
57. Scarmeas N, Stern Y, Tang MX, Mayeux R, Luchsinger JA. Mediterranean diet and risk for Alzheimer's disease. Ann Neurol. (2006) 59:912–21. doi: 10.1002/ana.20854
58. Foong HF, Hamid TA, Ibrahim R, Haron SA. The association between religious orientation and life satisfaction in older adults living with morbidity and multimorbidity: a gender perspective in Malaysia. Psychogeriatrics. (2020) 20:891–9. doi: 10.1111/psyg.12614
59. Abdel-Hady D, El-Gilany A-H. Tobacco use and its associated factors among older people: a community-based study in Egypt. East Mediterr Heal J. (2020) 26:68–74. doi: 10.26719/2020.26.1.68
60. Molina NPFM, Tavares DM. dos S, Haas VJ, Rodrigues LR. Religiousity, spirituality and quality of life of elderly according to structural equation modeling. Texto e Contexto Enfermagem. (2020) 29:e20180468. doi: 10.1590/1980-265x-tce-2018-0468
61. Sharif S, Amiri M, Allen K-A, Sharif Nia H, Khoshnavay Fomani F, Hatef Matbue Y, et al. Attachment: the mediating role of hope, religiosity, and life satisfaction in older adults. Health Qual Life Outcomes. (2021) 19:57. doi: 10.1186/s12955-021-01695-y
62. Solaimanizadeh F, Mohammadinia N, Solaimanizadeh L. The relationship between spiritual health and religious coping with death anxiety in the elderly. J Relig Health. (2020) 59:1925–32. doi: 10.1007/s10943-019-00906-7
63. Gallardo-Peralta L, Sánchez-Moreno E. Espiritualidad, religiosidad y síntomas depresivos en personas mayores del norte de Chile TT - spirituality, religiosity, and depressive symptoms among elderly Chilean people in the north of Chile. Ter psicol. (2020) 38:169–87. doi: 10.4067/S0718-48082020000200169
64. Silva ATM, Tavares DMS, Molina NPFM, de Assunção LM, Rodrigues LR. Religiosidade e espiritualidade relacionadas às variáveis sociodemográficas, econômicas e de saúde entre idosos TT - Religiousity and spirituality related to the socio-demographic, economic and health variables in the older people TT - Religiosidad y es. REME Rev Min Enferm. (2019) 23:e–1221. doi: 10.5935/1415-2762.20190069
65. Bakhtiari A, Yadollahpur M, Omidvar S, Ghorbannejad S, Bakouei F. Does religion predict health-promoting behaviors in community-dwelling elderly people? J Relig Health. (2019) 58:452–64. doi: 10.1007/s10943-018-0710-3
66. Bakan AB, Arli SK, Yildiz M. Relationship between religious orientation and death anxiety in elderly individuals. J Relig Health. (2019) 58:2241–50. doi: 10.1007/s10943-019-00917-4
67. Fernández-Niño JA, Bojorquez I, Becerra-Arias C, Astudillo-Garcia CI. Religious affiliation and major depressive episode in older adults: a cross-sectional study in six low- and middle- income countries. BMC Public Health. (2019) 19:460. doi: 10.1186/s12889-019-6806-1
68. Hamid TA, Dzaher A, Ching SM. The role of social network, social support, religiosity and depression among elderly Malaysians who had experienced major life events. Med J Malaysia. (2019) 74:198–204.
69. Hill TD, Bradley CS, Dowd-Arrow B, Burdette AM. Religious attendance and the social support trajectories of older Mexican Americans. J Cross Cult Gerontol. (2019) 34:403–16. doi: 10.1007/s10823-019-09386-4
70. Reyes-Ortiz CA, Payan C, Altamar G, Gómez F, Koenig HG. Religiosity and self-rated health among older adults in Colombia. Colomb Med. (2019) 50:67–76. doi: 10.25100/cm.v50i2.4012
71. Strinnholm S, Gustafson Y, Niklasson J. Depressive disorders and religious engagement in very old people. Gerontol Geriatr Med. (2019) 5:2333721419846576. doi: 10.1177/2333721419846576
72. Willis KD, Nelson T, Moreno O. Death anxiety, religious doubt, and depressive symptoms across race in older adults. Int J Environ Res Public Health. (2019) 16:3645. doi: 10.3390/ijerph16193645
73. Moreno CAS, Alonso-Castillo MM, Gherardi-Donato EC da S, Armendáriz-García NA. Perspectiva espiritual, religiosidad y consumo de alcohol en adultos mayores TT - Spiritual perspective, religiousness and alcohol consumption in elderly TT - perspectiva espiritual, religiosidade e consumo de álcool em idosos. J Heal NPEPS. (2019) 4:155–66. doi: 10.30681/252610103688
74. Ejiri M, Kawai H, Fujiwara Y, Ihara K, Watanabe Y, Hirano H, et al. Social participation reduces isolation among Japanese older people in urban area: a 3-year longitudinal study. PLoS ONE. (2019) 14:e0222887. doi: 10.1371/journal.pone.0222887
75. El-Gilany A-H, Elkhawaga GO, Sarraf BB. Depression and its associated factors among elderly: a community-based study in Egypt. Arch Gerontol Geriatr. (2018) 77:103–7. doi: 10.1016/j.archger.2018.04.011
76. Kotian DB, Mathews M, Parsekar SS, Nair S, Binu VS, Subba SH. Factors associated with social isolation among the older people in India. J Geriatr Psychiatry Neurol. (2018) 31:271–8. doi: 10.1177/0891988718796338
77. Manning LK, Miles A. Examining the effects of religious attendance on resilience for older adults. J Relig Health. (2018) 57:191–208. doi: 10.1007/s10943-017-0438-5
78. Nery BLS, da Cruz KCT, Faustino AM, dos Santos CTB. Vulnerabilidades, depressão e religiosidade em idosos internados em uma unidade de emergência. Rev Gaúch Enferm. (2018) 39:e20170184. doi: 10.1590/1983-1447.2018.2017-0184
79. Munawar K, Tariq O. Exploring relationship between spiritual intelligence, religiosity and life satisfaction among elderly Pakistani Muslims. J Reli Heal. (2018) 57:781–95. doi: 10.1007/s10943-017-0360-x
80. Lac A, Austin N, Lemke R, Poojary S, Hunter P. Association between religious practice and risk of depression in older people in the subacute setting. Australas J Ageing. (2017) 36:E31–4. doi: 10.1111/ajag.12384
81. Nunes MGS, Leal MCC, Marques APO, Mendonça SS. Idosos longevos: avaliação da qualidade de vida no domínio da espiritualidade, da religiosidade e de crenças pessoais TT - Long-lived elderly: assessment of quality of life in the field of spirituality, religiousness and personal beliefs. Saúde Debate. (2017) 41:1102–15. doi: 10.1590/0103-1104201711509
82. Bonnewyn A, Shah A, Bruffaerts R, Demyttenaere K. Are religiousness and death attitudes associated with the wish to die in older people? Int Psychogeriatr. (2016) 28:397–404. doi: 10.1017/S1041610215001192
83. McGowan JC, Midlarsky E, Morin RT, Graber LS. Religiousness and psychological distress in Jewish and Christian older adults. Clin Gerontol. (2016) 39:489–507. doi: 10.1080/07317115.2016.1187696
84. Krok D. Sense of coherence mediates the relationship between the religious meaning system and coping styles in Polish older adults. Aging Ment Heal. (2016) 20:1002–9. doi: 10.1080/13607863.2015.1056772
85. Andrade JMO, Rios LR, Teixeira LS, Vieira FS, Mendes DC, Vieira MA, et al. Influência de fatores socioeconômicos na qualidade de vida de idosos hipertensos TT - influence of socioeconomic factors on the quality of life of elderly hypertensive individuals. Ciênc Saúde Coletiva. (2014) 19:3497–504. doi: 10.1590/1413-81232014198.19952013
86. Feng L, Li P, Lu C, Tang W, Mahapatra T, Wang Y, et al. Burden and correlates of geriatric depression in the Uyghur elderly population, observation from Xinjiang, China. PLoS ONE. (2014) 9:e114139. doi: 10.1371/journal.pone.0114139
87. Chaves ÉCL, Paulino CF, Souza VHS, Mesquita AC, Carvalho FS, Nogueira DA. Quality of life, depressive symptoms and religiosity in elderly adults: a cross-sectional study TT - Calidad de vida, síntomas depresivos y religiosidad en los adultos mayores: un estudio transversal TT - Qualidade de vida, sintomas depressivos e religi. Texto Context Enferm. (2014) 23:648–55. doi: 10.1590/0104-07072014001000013
88. dos Santos NC, Abdala GA. Religiosidade e qualidade de vida relacionada à saúde dos idosos em um município na Bahia, Brasil TT - religiosity and health-related quality of life of elderly in a city in Bahia, Brazil. Rev Bras Geriatr Gerontol. (2014) 17:795–805. doi: 10.1590/1809-9823.2014.13166
89. Hayward RD, Krause N. How religious doubt moderates depression symptoms following older adult bereavement. Death Stud. (2014) 38:217–23. doi: 10.1080/07481187.2012.742476
90. Rivera-Ledesma A, Montero-Lòpez Lena M. Ajuste psicológico y vida religiosa en adultos mayores TT - Psychological Adjustment and Religious Life in Elderly People. Univ Psychol. (2014) 13:895–906. doi: 10.11144/Javeriana.UPSY13-3.apvr
91. Hafeez A, Rafique R. Spirituality and Religiosity as Predictors of Psychological Well-Being in Residents of Old Homes. (2013).
92. Ysseldyk R, Haslam SA, Haslam C. Abide with me: religious group identification among older adults promotes health and well-being by maintaining multiple group memberships. Aging Ment Health. (2013) 17:869–79. doi: 10.1080/13607863.2013.799120
93. Barricelli ILFOBL, Sakumoto IKY, da Silva LHM, de Araujo CV. Influência da orientação religiosa na qualidade de vida de idosos ativos TT - influence of religious orientation in the quality of life of active elderly. Rev Bras Geriatr Gerontol. (2012) 15:505–15. doi: 10.1590/S1809-98232012000300011
94. Jahn DR, Poindexter EK, Graham RD, Cukrowicz KC. The moderating effect of the negative impact of recent life events on the relation between intrinsic religiosity and death ideation in older adults. Suicide Life Threat Behav. (2012) 42:589–601. doi: 10.1111/j.1943-278X.2012.00114.x
95. Krause N, Bastida E. Religion and health among older Mexican Americans: exploring the influence of making mandas. J Reli Heal. (2012) 51:812–24. doi: 10.1007/s10943-010-9389-9
96. Momtaz YA, Hamid TA, Ibrahim R, Yahaya N, Abdullah SS. Moderating effect of Islamic religiosity on the relationship between chronic medical conditions and psychological well-being among elderly Malays. Psychogeriatrics. (2012) 12:43–53. doi: 10.1111/j.1479-8301.2011.00381.x
97. Moon YS, Kim DH. Association between religiosity/spirituality and quality of life or depression among living-alone elderly in a South Korean city. Asia-Pacific Psychiatry. (2013) 5:293–300. doi: 10.1111/appy.12025
98. Richardson TM, Friedman B, Podgorski C, Knox K, Fisher S, He H, et al. Depression and its correlates among older adults accessing aging services. Am J Geriatr Psychiatry. (2012) 20:346–54. doi: 10.1097/JGP.0b013e3182107e50
99. Vitorino LM, Vianna LAC. Religious/spiritual coping in institutionalized elderly. Acta paul enferm. (2012) 25:136–42. doi: 10.1590/S0103-21002012000800021
100. Park J, Roh S, Yeo Y. Religiosity, social support, and life satisfaction among elderly Korean immigrants. Gerontologist. (2012) 52:641–9. doi: 10.1093/geront/gnr103
101. Callen BL, Mefford L, Groër M, Thomas SP. Relationships among stress, infectious illness, and religiousness/spirituality in community-dwelling older adults. Res Gerontol Nurs. (2011) 4:195–206. doi: 10.3928/19404921-20101001-99
102. Corrêa AAM, Moreira-Almeida A, Menezes PR, Vallada H, Scazufca M, Meneze PR, et al. Investigating the role played by social support in the association between religiosity and mental health in low income older adults: results from the São Paulo Ageing & Health Study (SPAH) TT - investigando o papel do suporte social na associação ent. Rev Bras Psiquiatr. (2011) 33:157–64. doi: 10.1590/S1516-44462010005000028
103. Krause N, Bastida E. Religion, suffering, and self-rated health among older Mexican Americans. J Gerontol B Psychol Sci Soc Sci. (2011) 66:207–16. doi: 10.1093/geronb/gbq086
104. Lucchetti G, Lucchetti AG, Badan-Neto AM, Peres PT, Peres MFP, Moreira-Almeida A, et al. Religiousness affects mental health, pain and quality of life in older people in an outpatient rehabilitation setting. J Rehabil Med. (2011) 43:316–22. doi: 10.2340/16501977-0784
105. Schieman S, Bierman A, Ellison CG. Religious involvement, beliefs about God, and the sense of mattering among older adults. J Sci Study Reli. (2010) 49:517–35. doi: 10.1111/j.1468-5906.2010.01526.x
106. Idler EL, McLaughlin J, Kasl S. Religion and the quality of life in the last year of life. J Gerontol B Psychol Sci Soc Sci. (2009) 64:528–37. doi: 10.1093/geronb/gbp028
107. McFarland MJ, Uecker JE, Regnerus MD. The role of religion in shaping sexual frequency and satisfaction: evidence from married and unmarried older adults. J Sex Res. (2011) 48:297–308. doi: 10.1080/00224491003739993
108. Blay SL, Batista AD, Andreoli SB, Gastal FL. The relationship between religiosity and tobacco, alcohol use, and depression in an elderly community population. Am J Geriatr Psychiatry. (2008) 16:934–43. doi: 10.1097/JGP.0b013e3181871392
109. Payman V, George K, Ryburn B. Religiosity of depressed elderly inpatients. Int J Geriatr Psychiatry. (2008) 23:16–21. doi: 10.1002/gps.1827
110. Chaaya M, Sibai AM, Fayad R, El-Roueiheb Z. Religiosity and depression in older people: evidence from underprivileged refugee and non-refugee communities in Lebanon. Aging Ment Health. (2007) 11:37–44. doi: 10.1080/13607860600735812
111. Dunn KS. Predictors of self-reported health among older African-American central city adults. Holist Nurs Pract. (2007) 21:237–43. doi: 10.1097/01.HNP.0000287987.94472.d7
112. King DA, Lyness JM, Duberstein PR, He H, Tu XM, Seaburn DB. Religious involvement and depressive symptoms in primary care elders. Psychol Med. (2007) 37:1807–15. doi: 10.1017/S0033291707000591
113. Keyes CLM, Reitzes DC. The role of religious identity in the mental health of older working and retired adults. Aging Ment Health. (2007) 11:434–43. doi: 10.1080/13607860601086371
114. Yoon DP, Lee E-KO. The impact of religiousness, spirituality, and social support on psychological well-being among older adults in rural areas. J Gerontol Soc Work. (2007) 48:281–98. doi: 10.1300/J083v48n03_01
115. Chen H, Cheal K, McDonel Herr EC, Zubritsky C, Levkoff SE. Religious participation as a predictor of mental health status and treatment outcomes in older persons. Int J Geriatr Psychiatry. (2007) 22:144–53. doi: 10.1002/gps.1704
116. Mui AC, Kang S-Y. Acculturation stress and depression among Asian immigrant elders. Soc Work. (2006) 51:243–55. doi: 10.1093/sw/51.3.243
117. Roff LL, Klemmack DL, Simon C, Cho GW, Parker MW, Koenig HG, et al. Functional limitations and religious service attendance among African American and white older adults. Heal Soc Work. (2006) 31:246–55. doi: 10.1093/hsw/31.4.246
118. Bosworth HB, Park K-S, McQuoid DR, Hays JC, Steffens DC. The impact of religious practice and religious coping on geriatric depression. Int J Geriatr Psychiatry. (2003) 18:905–14. doi: 10.1002/gps.945
119. Meisenhelder JB. Gender differences in religiosity and functional health in the elderly. Geriatr Nurs. (2003) 24:343–7. doi: 10.1016/j.gerinurse.2003.10.005
120. Milstein G, Bruce ML, Gargon N, Brown E, Raue PJ, McAvay G. Religious practice and depression among geriatric home care patients. Int J Psychiatry Med. (2003) 33:71–83. doi: 10.2190/MUP1-DFB4-23KK-XPCF
121. Blazer DG, Hays JC, Musick MA. Abstinence versus alcohol use among elderly rural Baptists: a test of reference group theory and health outcomes. Aging Ment Health. (2002) 6:47–54. doi: 10.1080/13607860120101086
122. Cicirelli VG. Fear of death in older adults: predictions from terror management theory. J Gerontol B Psychol Sci Soc Sci. (2002) 57:P358–66. doi: 10.1093/geronb/57.4.P358
123. Herrera CG, Rodríguez Testal JF. Afrontamiento del estrés institucional en la vejez TT - coping of the institutional stress in the elderly. Geriátrika. (2002) 18:179–96.
124. Braam AW, Van den Eeden P, Prince MJ, Beekman AT, Kivelä SL, Lawlor BA, et al. Religion as a cross-cultural determinant of depression in elderly Europeans: results from the EURODEP collaboration. Psychol Med. (2001) 31:803–14. doi: 10.1017/S0033291701003956
125. Musick MA, Blazer DG. Hays JC. Religious activity, alcohol use, and depression in a sample of elderly baptists. Res Aging. (2020) 22:91–116. doi: 10.1177/0164027500222001
126. Guglani S, Coleman PG, Sonuga-Barke EJ. Mental health of elderly Asians in Britain: a comparison of Hindus from nuclear and extended families of differing cultural identities. Int J Geriatr Psychiatry. (2000) 15:1046–53. doi: 10.1002/1099-1166(200011)15:11<1046::AID-GPS229>3.0.CO;2-C
127. Menon AS, Campbell D, Ruskin P, Hebel JR. Depression, hopelessness, and the desire for life-saving treatments among elderly medically ill veterans. Am J Geriatr Psychiatry. (2000) 8:333–42. doi: 10.1097/00019442-200011000-00010
128. Husaini BA, Blasi AJ, Miller O. Does public and private religiosity have a moderating effect on depression? A bi-racial study of elders in the American South. Int J Aging Hum Dev. (1999) 48:63–72. doi: 10.2190/F5MT-RTYH-7XR1-TFQU
129. Koenig HG, Pargament KI, Nielsen J. Religious coping and health status in medically ill hospitalized older adults. J Nerv Ment Dis. (1998) 186:513–21. doi: 10.1097/00005053-199809000-00001
130. Musick MA, Koenig HG, Hays JC, Cohen HJ. Religious activity and depression among community-dwelling elderly persons with cancer: the moderating effect of race. J Gerontol B Psychol Sci Soc Sci. (1998) 53:S218–27. doi: 10.1093/geronb/53B.4.S218
131. Tapanya S, Nicki R, Jarusawad O. Worry and intrinsic/extrinsic religious orientation among Buddhist (Thai) and Christian (Canadian) elderly persons. Int J Aging Hum Dev. (1997) 44:73–83. doi: 10.2190/ENQG-HNV4-5G0D-CQ88
132. Kennedy GJ, Kelman HR, Thomas C, Chen J. The relation of religious preference and practice to depressive symptoms among 1,855 older adults. J Gerontol B Psychol Sci Soc Sci. (1996) 51:P301–8. doi: 10.1093/geronb/51B.6.P301
133. Krause N. Religiosity and self-esteem among older adults. J Gerontol B Psychol Sci Soc Sci. (1995) 50:P236–46. doi: 10.1093/geronb/50B.5.P236
134. Koenig HG, Cohen HJ, Blazer DG, Pieper C, Meador KG, Shelp F, et al. Religious coping and depression among elderly, hospitalized medically ill men. Am J Psychiatry. (1992) 149:1693–700. doi: 10.1176/ajp.149.12.1693
135. Pressman P, Lyons JS, Larson DB, Strain JJ. Religious belief, depression, and ambulation status in elderly women with broken hips. Am J Psychiatry. (1990) 147:758–60. doi: 10.1176/ajp.147.6.758
136. Hunsberger B. Religion, age, life satisfaction, and perceived sources of religiousness: a study of older persons. J Gerontol. (1985) 40:615–20. doi: 10.1093/geronj/40.5.615
137. Khodarahimi S, Ghadampour E, Karami A. The roles of spiritual well-being and tolerance of uncertainty in prediction of happiness in elderly TT - los roles del bienestar espiritual y la tolerancia a la incertidumbre en la predicción de la felicidad en los ancianos. An psicol. (2021) 37:371–7. doi: 10.6018/analesps.446871
138. Aydin A, Işik A, Kahraman N. Mental health symptoms, spiritual well-being and meaning in life among older adults living in nursing homes and community dwellings. Psychogeriatrics. (2020) 20:833–43. doi: 10.1111/psyg.12613
139. Fernandes AM, Sousa C de, Valentim O, Sousa L, Vinagre H, Carvalho JC. Bem-estar e espiritualidade em adultos seniores TT - well-being and spirituality in senior adults. Rev Rol enferm. (2020) 43:414–9.
140. Ilyas Z, Shahed S, Hussain S. An impact of perceived social support on old age well-being mediated by spirituality, self-esteem and ego integrity. J Reli Heal. (2020) 59:2715–32. doi: 10.1007/s10943-019-00969-6
141. Hassoun H, Bermejo JC, Villacieros M, Millán Asín MÁ, Arenas Antúnez A. Relación entre bienestar espiritual, calidad de vida y sentido del sufrimiento en una población de ancianos religiosos residentes en centros españoles TT - relation between spiritual wellbeing, quality of life and sense of suffering in a population of el. Gerokomos. (2019) 30:124–9.
142. Salman A, Lee Y-H. Spiritual practices and effects of spiritual well-being and depression on elders' self-perceived health. Appl Nurs Res. (2019) 48:68–74. doi: 10.1016/j.apnr.2019.05.018
143. Thauvoye E, Vanhooren S, Vandenhoeck A, Dezutter J. Spirituality and well-being in old age: exploring the dimensions of spirituality in relation to late-life functioning. J Relig Health. (2018) 57:2167–81. doi: 10.1007/s10943-017-0515-9
144. Araújo L, Ribeiro O, Paúl C. The role of existential beliefs within the relation of centenarians' health and well-being. J Relig Health. (2017) 56:1111–22. doi: 10.1007/s10943-016-0297-5
145. Garces SBB, Figueiró MF, Hansen D, Rosa CB, Brunelli AV, do Bianchi PD, et al. Resiliência entre mulheres idosas e sua associação com o bem-estar espiritual e o apoio social TT - Resilience among older women and its association with spiritual well-being and social support. Estud Interdiscip Envelhec. (2017) 22:9–30. doi: 10.22456/2316-2171.43412
146. Lee Y-H, Salman A. The mediating effect of spiritual well-being on depressive symptoms and health-related quality of life among elders. Arch Psychiatr Nurs. (2018) 32:418–24. doi: 10.1016/j.apnu.2017.12.008
147. Pilger C, Santos ROP. dos, Lentsck MH, Marques S, Kusumota L. Spiritual well-being and quality of life of older adults in hemodialysis TT - bienestar espiritual y calidad de vida de ancianos en tratamiento de hemodiálisis TT - bem estar espiritual e qualidade de vida de idosos em tratamento hemodialítico. Rev Bras Enferm. (2017) 70:689–96. doi: 10.1590/0034-7167-2017-0006
148. Souza EN, Oliveira NAD, Luchesi BM, Gratão ACM, Orlandi FDS, Pavarini SCI. Relação entre a esperança e a espiritualidade de idosos cuidadores. Texto & Contexto-Enfermagem. (2017).
149. Vitorino LM, Lucchetti G, Santos AEO, Lucchetti ALG, Ferreira EB, Adami NP, et al. Spiritual religious coping is associated with quality of life in institutionalized older adults. J Reli Heal. (2016) 55:549–59. doi: 10.1007/s10943-015-0148-9
150. Ali J, Marhemat F, Sara J, Hamid H. The relationship between spiritual well-being and quality of life among elderly people. Holist Nurs Pr. (2015) 29:128–35. doi: 10.1097/HNP.0000000000000081
151. Jun JS, Lee KH, Bolin BL. Stress and spirituality on the depressive symptoms of older adults in assisted living: gender differences. J Evid Informed Soc Work. (2015) 12:588–600. doi: 10.1080/15433714.2014.966229
152. Oliver A, Galiana L, Sancho P, Tomás JM. Espiritualidad, esperanza y dependencia como predictores de la satisfacción vital y la percepción de salud: efecto moderador de ser muy mayor TT - spirituality, hope and dependence as predictors of satisfaction with life and perception of health: the mod. Aquichan. (2015) 15:228–38. doi: 10.5294/aqui.2015.15.2.7
153. Caldeira S, de Carvalho EC, Vieira M. Between spiritual wellbeing and spiritual distress: possible related factors in elderly patients with cancer. Rev Lat Am Enfermagem. (2014) 22:28–34. doi: 10.1590/0104-1169.3073.2382
154. Coleman PG, Carare RO, Petrov I, Forbes E, Saigal A, Spreadbury JH, et al. Spiritual belief, social support, physical functioning and depression among older people in Bulgaria and Romania. Aging Ment Health. (2011) 15:327–33. doi: 10.1080/13607863.2010.519320
155. Lee KH, Yoon DP. Factors influencing the general well-being of low-income Korean immigrant elders. Soc Work. (2011) 56:269–79. doi: 10.1093/sw/56.3.269
156. Vahia I V, Depp CA, Palmer BW, Fellows I, Golshan S, Thompson W, et al. Correlates of spirituality in older women. Aging Ment Health. (2011) 15:97–102. doi: 10.1080/13607863.2010.501069
157. Skarupski KA, Fitchett G, Evans DA, de Leon CFM. Daily spiritual experiences in a biracial, community-based population of older adults. Aging Ment Health. (2010) 14:779–89. doi: 10.1080/13607861003713265
158. You KS, Lee H-O, Fitzpatrick JJ, Kim S, Marui E, Lee JS, et al. Spirituality, depression, living alone, and perceived health among Korean older adults in the community. Arch Psychiatr Nurs. (2009) 23:309–22. doi: 10.1016/j.apnu.2008.07.003
159. Kirby SE, Coleman PG, Daley D. Spirituality and well-being in frail and nonfrail older adults. J Gerontol B Psychol Sci Soc Sci. (2004) 59:P123–9. doi: 10.1093/geronb/59.3.P123
160. Meisenhelder JB, Chandler EN. Faith, prayer, and health outcomes in elderly Native Americans. Clin Nurs Res. (2000) 9:191–203. doi: 10.1177/105477380000900207
161. Gonçalves JS, da Silva LL, Abdala GA, Meira MDD, Santos ACM, da Silva MFF. Religiosidade e os transtornos mentais comuns em adultos TT - religiosity and common mental disorders in adults. Rev Enferm UFPE Line. (2017) 11:1708–15. doi: 10.5205/1981-8963-v11i4a15268p1708-1715-2017
162. Jung JH. Attachment to god and death anxiety in later life: does race matter? Res Aging. (2018) 40:956–77. doi: 10.1177/0164027518805190
163. Roh HW, Hong CH, Lee Y, Oh BH, Lee KS, Chang KJ, et al. Participation in physical, social, and religious activity and risk of depression in the elderly: a community-based three-year longitudinal study in Korea. PLoS ONE. (2015) 10:e0132838. doi: 10.1371/journal.pone.0132838
164. Hsu HC. Effects of religiousness on depressive symptoms among elderly persons in Taiwan. Clin Gerontol. (2014) 37:446–57. doi: 10.1080/07317115.2014.937549
165. Sun F, Park NS, Roff LL, Klemmack DL, Parker M, Koenig HG, et al. Predicting the trajectories of depressive symptoms among southern community-dwelling older adults: the role of religiosity. Aging Ment Heal. (2012) 16:189–98. doi: 10.1080/13607863.2011.602959
166. Law RW, Sbarra DA. The effects of church attendance and marital status on the longitudinal trajectories of depressed mood among older adults. J Aging Health. (2009) 21:803–23. doi: 10.1177/0898264309338300
167. Norton MC, Singh A, Skoog I, Corcoran C, Tschanz JT, Zandi PP, et al. Church attendance and new episodes of major depression in a community study of older adults: the Cache County Study. J Gerontol B Psychol Sci Soc Sci. (2008) 63:P129–37. doi: 10.1093/geronb/63.3.P129
168. Kivelä SL, Köngäs-Saviaro P, Laippala P, Pahkala K, Kesti E. Social and psychosocial factors predicting depression in old age: a longitudinal study. Int Psychogeriatr. (1996) 8:635–44. doi: 10.1017/S1041610296002943
169. Lee KH, Hwang MJ. Private religious practice, spiritual coping, social support, and health status among older Korean adult immigrants. Soc Work Public Heal. (2014) 29:428–43. doi: 10.1080/19371918.2013.858234
170. Roh S, Brown-Rice KA, Lee KH, Lee YS, Lawler MJ, Martin JI. Stressors, coping resources, and depressive symptoms among rural American Indian older adults. Soc Work Public Health. (2015) 30:345–59. doi: 10.1080/19371918.2015.1019174
171. Hoffman YSG, Grossman ES, Bergman YS, Bodner E. The link between social anxiety and intimate loneliness is stronger for older adults than for younger adults. Aging Ment Health. (2021) 25:1246–53. doi: 10.1080/13607863.2020.1774741
172. Rashedi V, Pachana NA, Khademi MJ, Sajadi S, Gheshlaghi SM. Anxiety and loneliness in the Iranian older adults. Int J Psychol Behav Sci. (2015) 2015:49–52. doi: 10.5923/j.ijpbs.20150502.01
173. Bailly N, Martinent G, Ferrand C, Agli O, Giraudeau C, Gana K, et al. Spirituality, social support, and flexibility among older adults: a five-year longitudinal study. Int Psychogeriatr. (2018) 30:1745–52. doi: 10.1017/S1041610218000029
174. VanderWeele TJ Yu J, Cozier YC, Wise L, Argentieri MA, Rosenberg L, Palmer JR, et al. Attendance at religious services, prayer, religious coping, and religious/spiritual identity as predictors of all-cause mortality in the black women's health Study. Am J Epidemiol. (2017) 185:515–22. doi: 10.1093/aje/kww179
175. Himmelfarb S, Murrell SA. The prevalence and correlates of anxiety symptoms in older adults. J Psychol. (1984) 116:159–67. doi: 10.1080/00223980.1984.9923632
176. Schaub RT, Linden M. Anxiety and anxiety disorders in the old and very old–results from the Berlin Aging Study (BASE). Compr Psychiatry. (2000) 41:48–54. doi: 10.1016/S0010-440X(00)80008-5
177. Van Balkom AJLM, Beekman ATF, De Beurs E, Deeg DJH, Van Dyck R, Van Tilburg W. Comorbidity of the anxiety disorders in a community-based older population in The Netherlands. Acta Psychiatr Scand. (2000) 101:37–45. doi: 10.1034/j.1600-0447.2000.101001037.x
178. Hodges S. Mental health, depression, and dimensions of spirituality and religion. J Adult Dev. (2002) 9:109–15. doi: 10.1023/A:1015733329006
179. Flores-Flores O, Zevallos-Morales A, Carrión I, Pawer D, Rey L, Checkley W, et al. “We can't carry the weight of the whole world”: illness experiences among Peruvian older adults with symptoms of depression and anxiety. Int J Ment Health Syst. (2020) 14:49. doi: 10.1186/s13033-020-00381-8
180. Dennis MK, Washington KT. Ways of grieving among Ojibwe elders: “They're All Around Us. They're Always”. Omega. (2018) 78:107–19. doi: 10.1177/0030222816679661
181. Levine E. Jewish views and customs on death. Death and Bereavement Across Cultures. (2003) 106–38. doi: 10.4324/9780203435199-9
182. Frankl VE. Man's Search for Meaning. Available online at: https://www.amazon.com/gp/product/B009U9S6FI/ref=dbs_a_def_rwt_hsch_vapi_tkin_p1_i0 (accessed February 4, 2022).
183. Erikson EH. The Life Cycle Completed (Extended Version): A Review. Available online at: https://www.amazon.com/Life-Cycle-Completed-Extended-Version-ebook/dp/B00CJQ2GRI/ref=sr_1_2?crid=2CJ34TVVCANES&keywords=erik+erikson&qid=1643977512&s=digital-text&sprefix=erik+erikson%2Cdigital-text%2C185&sr=1-2 (accessed February 4, 2022).
184. Tomer A, Eliason GT, Wong PTP. Existential and Spiritual Issues in Death Attitudes. Hove: Psychology Press. (2013).
185. Neimeyer RA Death Anxiety Handbook: Research, Instrumentation, Application. (2005). Available online at: https://books.google.es/books?hl=en&lr=&id=ziZACwAAQBAJ&oi=fnd&pg=PA121&dq=info:qTs8OXiYStgJ:scholar.google.com&ots=7YMNjfYCJy&sig=uj9mQVZQCX5mLyqGDea5zdBUmgI&redir_esc=y#v=onepage&q&f=false (accessed February 4, 2022).
187. Hakulinen C, Elovainio M, Pulkki-Råback L, Virtanen M, Kivimäki M, Jokela M, et al. Individual participant meta-analysis of 10 cohort studies. Depress Anxiety. (2015) 32:461–70. doi: 10.1002/da.22376
188. Hayward RD, Krause N. Religion, mental health, and well-being: social aspects. Relig Personal Soc Behav. (2013) 255–80.
189. Villani D, Sorgente A, Iannello P, Antonietti A. The role of spirituality and religiosity in subjective well-being of individuals with different religious status. Front Psychol. (2019) 10:1525. doi: 10.3389/fpsyg.2019.01525
190. Jackson BR, Bergeman CS. How does religiosity enhance well-being? The role of perceived control. Psycholog Relig Spiritual. (2011) 3:149. doi: 10.1037/a0021597
191. Van Cappellen P, Toth-Gauthier M, Saroglou V, Fredrickson BL. Religion and well-being: the mediating role of positive emotions. J Happiness Stud. (2014) 17:485–505. doi: 10.1007/s10902-014-9605-5
192. Meanley S, Pingel ES, Bauermeister JA. Psychological well-being among religious and spiritual-identified young gay and bisexual men. Sex Res Social Policy. (2016) 13:35–45. doi: 10.1007/s13178-015-0199-4
193. Butler-Barnes ST, Martin PP, Hope EC, Copeland-Linder N, Lawrence Scott M. Religiosity and coping: racial stigma and psychological well-being among African american girls. J Relig Health. (2018) 57:1980–95. doi: 10.1007/s10943-018-0644-9
194. Guerrero-Castañeda RF, Menezes TMO, do Prado ML, Galindo-Soto JA. Spirituality and religiosity for the transcendence of the elderly being. Rev Bras Enferm. (2019) 72:259–65. doi: 10.1590/0034-7167-2018-0840
195. Peteet JR, Zaben F. Al, Koenig HG. Integrating spirituality into the care of older adults. Int Psychogeriatr. (2018) 31:1–8. doi: 10.1017/S1041610218000716
Keywords: religion, mental disorder (disease), depression, anxiety, elderly
Citation: Coelho-Júnior HJ, Calvani R, Panza F, Allegri RF, Picca A, Marzetti E and Alves VP (2022) Religiosity/Spirituality and Mental Health in Older Adults: A Systematic Review and Meta-Analysis of Observational Studies. Front. Med. 9:877213. doi: 10.3389/fmed.2022.877213
Received: 16 February 2022; Accepted: 19 April 2022;
Published: 12 May 2022.
Edited by:
Tzvi Dwolatzky, Technion Israel Institute of Technology, IsraelReviewed by:
Nicolas Roussiau, Université de Nantes, FranceCopyright © 2022 Coelho-Júnior, Calvani, Panza, Allegri, Picca, Marzetti and Alves. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hélio José Coelho-Júnior, Y29lbGhvanVuaW9yQGhvdG1haWwuY29tLmJy
†These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.