 Gulimire Muhetaer
Gulimire Muhetaer
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Med. , 22 July 2022
Sec. Nephrology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.876692
This article is part of the Research Topic Secondary Hyperparathyroidism: an Ongoing Challenge for the Nephrologist View all 10 articles
End-stage renal disease (ESRD) is a global health problem with a high incidence (1) and a steadily increasing prevalence (2). Secondary hyperparathyroidism (SHPT) is a common and serious complication of chronic renal failure (CRF) in dialysis patients (3). It is mainly manifested as parathyroid hyperplasia caused by abnormal calcium and phosphorus metabolism and active vitamin D resistance, resulting in excessive secretion of parathyroid hormone (PTH), which leads to complications such as bone deformity, osteoarthralgia, pruritus, ectopic calcification, and cardiovascular calcification in CKD patients, significantly reducing the quality of life in CKD patients (4, 5). In patients with chronic kidney disease, secondary parathyroid gland hyperplasia needs to be treated as early as possible (6). Currently, there are a variety of treatment options, including vitamin D receptor agonists, xenacax hydrochloride, parathyroidectomy and ablation techniques, etc. (7, 8). Medical treatment is the main choice among these treatments, but it is invalid in patients with severe hyperparathyroidism. So, parathyroidectomy is suggested to do in those patients (9). However, many dialysis patients who have severe cardiopulmonary dysfunction cannot tolerate the trauma caused by surgery as the concept of minimally invasive surgery has been gradually introduced into all fields of surgery and medical treatment. Traditional surgery is no longer the only option. Radiofrequency ablation has been widely applied due to its advantages of less trauma, simple operation, and good repeatability. It has been reported to achieve good effects in treating secondary hyperparathyroidism patients (8). This case reports that one severe secondary hyperparathyroidism patient gets good therapeutic results from parathyroid radiofrequency ablation.
This paper reported a case of secondary hyperparat hyroidism who underwent radiofrequency ablation to eliminate seven parathyroid glands hyperplasia. We report a 28-year-old male ESRD patient caused by primary glomerulonephritis, maintenance hemodialysis for 10 years, 3 times per week, intermittent bone pain for 2 years. Two years ago, he developed severe bone pain accompanied by a left-leaning spine and limited movement when sitting up and could not take care of herself. The blood level of PTH > 2500 pg/mL. Intermittent oral Rocaltrol implosive therapy and intermittent Cinacalcet therapy were used. His height was shortened by 28 cm in the past two years. A tumor appeared in the anterior part of the maxillary hard palate 6 months ago. The serum level of PTH > 2500 pg/ml, alkaline phosphatase 1284.00 U/L, calcium 1.99 mmol/L, inorganic phosphorus 1.54 mmol/L were rechecked. Five parathyroid tissues were detected by parathyroid B-ultrasound (Figure 1). The maximum one was 13 × 7.9 × 8.4 mm. He has a 10-year hypertension history, poor blood pressure control, admission blood pressure of 220/120 mmHg, a history of congenital heart disease, and a patent foramen ovale. The LVEF is 58%. Due to sequelae in 2006, children’s polio history underwent ’ left lower limb correction. CT findings: bilateral lung inflammation, heart shadow, pulmonary artery widening, pericardial effusion, thoracic scoliosis deformity. The pulmonary function examination showed severe restrictive pulmonary ventilation dysfunction. We conducted a multidisciplinary discussion. Refer to the guide, after discussion and communication, we decided to performed ultrasound-guided parathyroid radiofrequency ablation (bilateral) to this patient. In December 11, 2019, bilateral parathyroid radiofrequency ablation was performed. During the operation, local infiltration anesthesia was performed after dilution with 1% lidocaine, and physiological saline was used as isolation belt under the guidance of ultrasound to protect the trachea, skin and surrounding tissues. After that, the mass was isolated from the recurrent laryngeal nerve and bilateral paraproliferative glands were ablated by moving-shot ablation technique under the guidance of ultrasound, In addition to 5 parathyroid glands found by ultrasound, 2 parathyroid glands were detected buring surgery and total 7 parathyroid glands were eliminated (Figure 2), compression hemostasis was performed in the operation area. The patients without hoarseness, numbness of hands and feet, drinking cough and other discomfort complaints after operation. And the serum level of PTH reduced to 309 pg/mL. The paraproliferative gland was completely ablated reexamined by ultrasonography. After 3 days of symptomatic treatment such as calcium supplementation, the PTH level reduced to 96. 9 pg/mL, and discharged. During the follow-up, intermittent calcitriol, Caltrate and other medicines have been discontinued. On November 15,2021, the serum PTH level was 146.8 pg/ml, and the ALP level was 80 U/L. Bone pain disappeared. And the patients can basically stand on their own. The patient was followed up continuously.
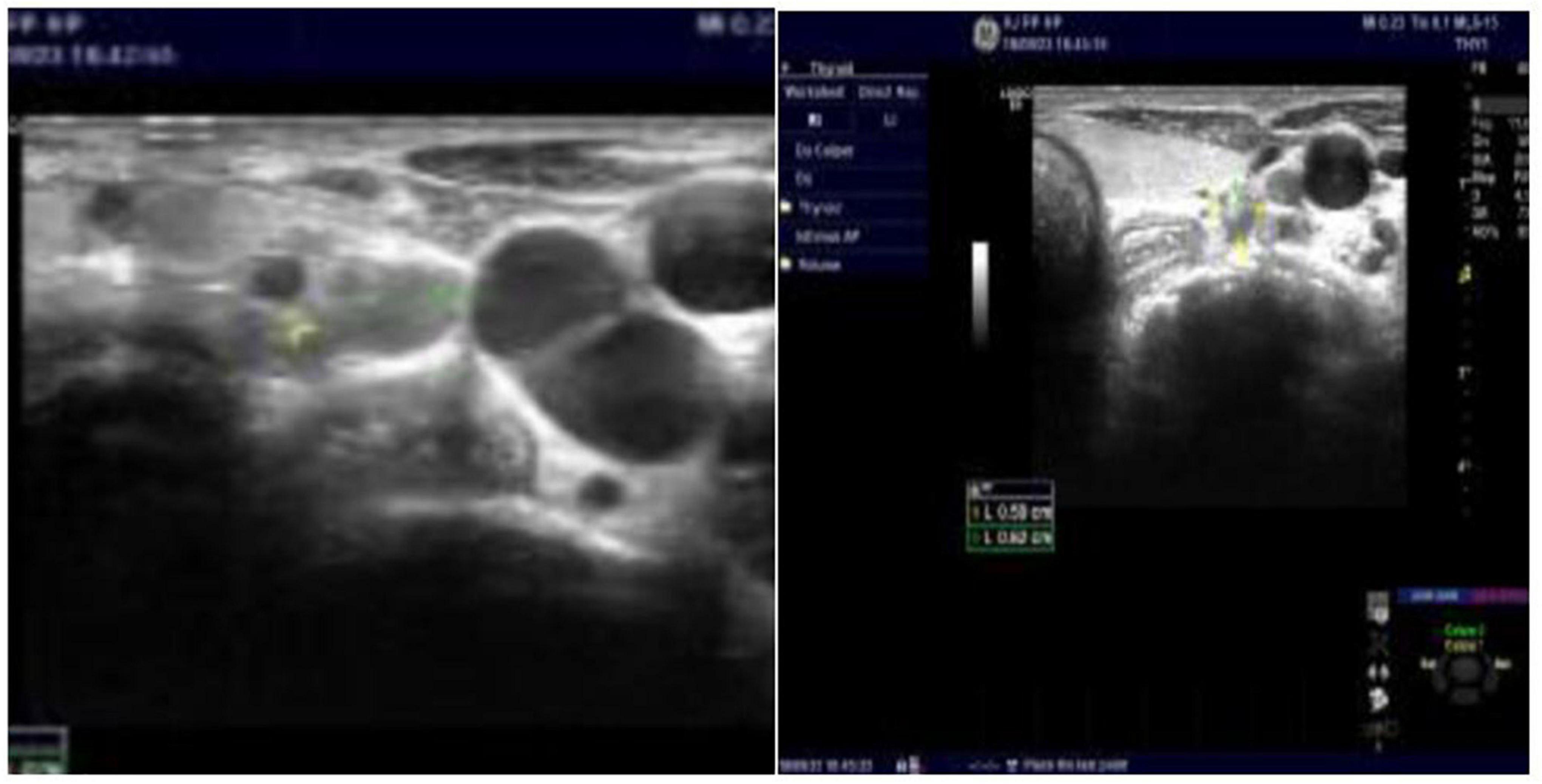
Figure 1. B-ultrasound image before parathyroid radiofrequency ablation.
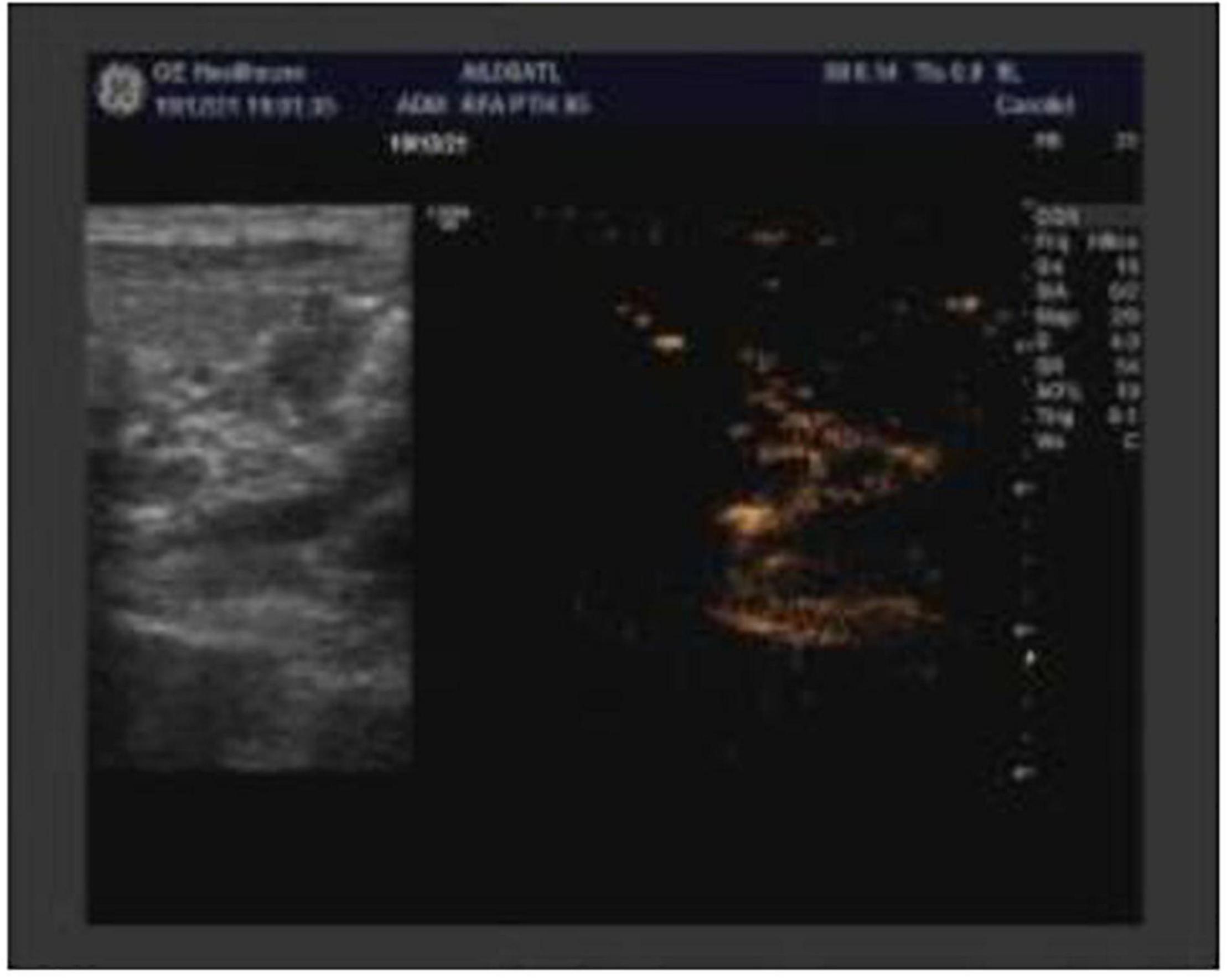
Figure 2. B-ultrasound image after parathyroid radiofrequency ablation.
SHPT is mainly characterized by calcium and phosphorus metabolism disorder, increased serum PTH secretion, and hyperparathyroidism. It is crucial to control the calcium, phosphorus, and PTH of patients with SHPT. The KDIGO guidelines suggest that PTH should be maintained at 2 ∼ 9 times the standard upper limit (9). It is recommended that patients with stage 5 CKD should use calcium analogs, calcitriol or vitamin D analogs, or combination treatment. This patient received intermittent administration of calcitriol and Sinakase oral. But the PTH level continued to rise. And multiple parathyroid glands were detected; the long diameter was more than 1cm of the largest one. Above mentioned reasons, combined with KDIGO’s recommendation, parathyroidectomy is recommended for CKD G3a ∼ G5D patients with severe hyperparathyroidism if medical treatment fails. However, many dialysis patients with cardiopulmonary dysfunction increase the risk of anesthesia complications and can’t stand the trauma caused by surgery. The clinical manifestations of this patient were bone pain, maxillary hard palate mass, shortening of height, and Poor cardiopulmonary function with malnutrition. Parathyroidectomy cannot be tolerated after evaluation, but traditional surgery is no longer the only option. Radiofrequency ablation has been widely used due to its advantages of less trauma, simple operation, and good repeatability. Radiofrequency ablation, laser ablation, and microwave ablation have been reported to have achieved good results in the treatment of secondary patients (8) and become an effective treatment method. Xu et al.’s study showed the iPTH and calcium levels controlled in 2 patients with SHPT by radiofrequency ablation (10). Although there are still controversies over surgical methods, efficacy, and safety, it is pointed out that there are still controversies over surgical techniques, effectiveness, and safety. However, radiofrequency ablation can also be regarded as an alternative therapy for patients with severe heart and lung function complications that increase general anesthesia risk and have achieved good efficacy (11). Therefore, we performed radiofrequency ablation for this patient. Seven parathyroid glands were eliminated during the operation. The PTH was also well reduced after the procedure. In SHPT patients, more glands may be affected, and the degree and number of glandular hyperplasia can seriously affect the prognosis of patients. The ectopic glands may exist in different locations, for example, the thyroid, cervical sheath, thymus, and upper mediastinum. Those glands cannot be approached by radiofrequency ablation adjacent to critical anatomical structures such as blood vessels or the esophagus. It will result in the failure of radiofrequency ablation and persistent SHPT after ablation. Studies have shown that the frequency of ectopic parathyroidosis in SHPT patients is about 15% (12). The proportion of patients with more than 4 glands is 2.5–30% (13). In this case, 5 parathyroids were detected by ultrasound. However, 7 parathyroids were seen in radiofrequency ablation operations. After another exploration, the ablated parathyroids were completely ablated. This shown that the positioning of instruments and doctors is particularly important, and experienced doctors can obtain better results through their own experience and repeated exploration to help find excess ectopic parathyroids. Alkaline phosphatase (ALP) is an indicator of osteogenesis, which reflects the high transport state of bone metabolism. Therefore, the higher level of ALP and the higher metabolic status of bone indicated the higher incidence of low level of serum calcium. Some studies have also pointed out that low calcium level after radiofrequency ablation is closely correlated with preoperative ALP (14). Higher ALP level before ablation will lead to more obvious postoperative hypocalcemia. In this patient, the level of ALP was very high before operation, and serum calcium decreased to 1.47 mmol/L after operation. Therefore, we actively supplement calcium and recheck PTH which also decreased compared with the first day after operation.
Although there are still some differences in surgical methods, efficacy, and safety in the clinical guidelines and related studies, radiofrequency ablation is an effective treatment for patients with severe hyperthyroidism who cannot tolerate surgery. In this case, the patient’s bone pain disappeared after radiofrequency ablation. At present, the level of PTH is maintained between 136–242 pg/ml (Figure 3). The patient can stand on their own, and the quality of his life has been improved significantly, also very satisfied with this treatment. Based on this patient’s experience, we consider that when patients suffer from cardiopulmonary dysfunction due to basic diseases, and can’t perform or endure the trauma caused by surgery, radiofrequency ablation can be widely used because of its advantages of small trauma, simple operation and repeatability, the levels of serum iPTH, calcium and phosphorus can also be effectively reduced after surgery, so as to achieve the effect similar to surgical resection. Of course, it also requires longer follow-up and clinical indicators to comprehensively determine the clinical efficacy. Therefore, it is very important to choose the most suitable treatment according to the individual differences of patients when choosing treatment plans.

Figure 3. Relevant clinical test values before and after parathyroid radiofrequency ablation Reference values: Ca (2.11–2.52 mmol/L); P (0.85–1.51 mmol/L); parathyroid hormone (PTH) (12–65 pg/ml); alkaline phosphatase (ALP) (45–125 U/L).
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
This work was supported by the Xinjiang Uygur Autonomous Region Project Application of bone disease information processing system in end-stage kidney disease (2020E02118) to HJ.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank the patients and their family for their participation in this study.
1. Saran R, Robinson B, Abbott KC, Agodoa LYC, Bhave N, Bragg-Gresham J, et al. US renal data system 2017 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis. (2018) 71:A7.
2. Ebert N, Jakob O, Gaedeke J, van der Giet M, Kuhlmann MK, Martus P, et al. Prevalence of reduced kidney function and albuminuria in older adults: the Berlin initiative study. Nephrol Dial Transplant. (2017) 32:997–1005.
3. Tajbakhsh R, Joshaghani HR, Bayzayi F, Haddad M, Qorbani M. Association between pruritus and serum concentrations of parathormone, calcium and phosphorus in hemodialysis patients. Saudi J Kidney Dis Transpl. (2013) 24:702–6. doi: 10.4103/1319-2442.113858
4. Naves-Díaz M, Passlick-Deetjen J, Guinsburg A, Marelli C, Fernández-Martín JL, Rodríguez-Puyol D, et al. Calcium, phosphorus, PTH and death rates in a large sample of dialysis patients from Latin America. The CORES Study. Nephrol Dial Transplant. (2011) 26:1938–47. doi: 10.1093/ndt/gfq304
5. Peng C, Zhang Z, Liu J, Chen H, Tu X, Hu R, et al. Efficacy and safety of ultrasound-guided radiofrequency ablation of hyperplastic parathyroid gland for secondary hyperparathyroidism associated with chronic kidney disease. Head Neck. (2017) 39:564–71. doi: 10.1002/hed.24657
6. Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Working Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder (CKD-MBD). Kidney Int Suppl. (2009) 113:S1–130.
7. Liaveri PG, Dikeos D, Ilias I, Lygkoni EP, Boletis IN, Skalioti C, et al. Quality of sleep in renal transplant recipients and patients on hemodialysis. J Psychosom Res. (2017) 93:96–101.
8. Zhao J, Qian L, Zu Y, Wei Y, Hu X. Efficacy of ablation therapy for secondary hyperparathyroidism by ultrasound guided percutaneous thermoablation. Ultrasound Med Biol. (2016) 42:1058–65. doi: 10.1016/j.ultrasmedbio.2015.08.021
9. Ketteler M, Block GA, Evenepoel P, Fukagawa M, Herzog CA, McCann L, et al. Executive summary of the 2017 KDIGO chronic kidney disease-mineral and bone disorder (CKD-MBD) guideline update: what’s changed and why it matters. Kidney Int. (2017) 92:26–36.
10. Zhuo L, Peng LL, Zhang YM, Xu ZH, Zou GM, Wang X, et al. US-guided microwave ablation of hyperplastic parathyroid glands: safety and efficacy in patients with end-stage renaldiseae – a pilot study. Radiology. (2017) 282:576–84.
11. Xu SY, Wang Y, Xie Q, Wu HY. Percutaneous sonography-guided radio-frequency ablation in the management of parathyroid adenoma. Singapore Med J. (2013) 54:e137–40. doi: 10.11622/smedj.2013092
12. Zhang L, Xing C, Shen C, Zeng M, Yang G, Mao H, et al. Diagnostic accuracy study of intraoperative and perioperative serum intact PTH level for successful parathyroidectomy in 501 secondary hyperparathyroidism patients. Sci Rep. (2016) 6:26841. doi: 10.1038/srep26841
13. Andrade JS, Mangussi-Gomes JP, Rocha LA, Ohe MN, Rosano M, das Neves MC, et al. Localization of ectopic and supernumerary parathyroid glands in patients with secondary and tertiary hyperparathyroidism: surgical description and correl ation with preoperative ultrasonography and Tc99m Sestamibi scintigraphy. Braz J Otorhinolaryngol. (2014) 80:29–34. doi: 10.5935/1808-8694.20140008
Keywords: hyperplastic parathyroid gland, radiofrequency ablation, secondary hyperparathyroidism, chronic kidney disease, parathyroid hormone
Citation: Muhetaer G, Liu G, Zhang L and Jiang H (2022) Severe secondary hyperparathyroidism in a chronic kidney disease patient treated with Radiofrequency ablation: One case report. Front. Med. 9:876692. doi: 10.3389/fmed.2022.876692
Received: 15 February 2022; Accepted: 15 June 2022;
Published: 22 July 2022.
Edited by:
Claudia Torino, Italian National Research Council, ItalyReviewed by:
Goce Spasovski, Saints Cyril and Methodius University of Skopje, North MacedoniaCopyright © 2022 Muhetaer, Liu, Zhang and Jiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hong Jiang, jangh-yt@163.com
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.