 Xiuhong Cao1†
Xiuhong Cao1† Qingsong Zhao
Qingsong Zhao Zhiqiang Liu
Zhiqiang Liu Zhendong Xu
Zhendong Xu- 1Department of Anesthesiology, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, China
- 2Department of Research and Education, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, China
- 3Department of Obstetrics, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, China
Background: In recent years, the incidence of postpartum hemorrhage has increased globally. Multiple pregnancies and cesarean sections are well-known risk factors for postpartum hemorrhage. No studies have evaluated the associations between fetal growth anomalies and postpartum hemorrhage in women with twin pregnancies undergoing cesarean section. This study aimed to identify the relationship between fetal growth anomalies and postpartum hemorrhage in women with twin pregnancies undergoing cesarean section.
Methods: This retrospective single-center study included 3,180 women with twin pregnancies at a tertiary hospital between August 2013 and July 2020. Singleton reference charts were used to assess fetal growth restriction at birth. Discordant growth was defined as an intertwin birth weight difference of ≥20%. Logistic regression analyses were used to evaluate the association between fetal growth anomalies and postpartum hemorrhage. Additionally, sensitivity analysis of abnormal placenta and stratification by twin chorionicity were conducted.
Results: The overall incidence of postpartum hemorrhage was 4.3%. Twin growth discordance, especially with fetal growth restriction, was associated with an increased risk of postpartum hemorrhage (adjusted odds ratio [AOR] = 1.62, 95% confidence interval [CI], 1.05–2.51, P = 0.031; AOR = 1.71; 95% CI, 1.08–2.70, P = 0.022; AOR = 1.98, 95% CI, 1.21–3.25, P = 0.006, respectively). After stratification, this relationship persisted in dichorionic twins (OR = 1.71, 95% CI, 1.04–2.82, P = 0.036; OR = 1.90, 95% CI, 1.13–3.21, P = 0.016; OR = 2.48, 95% CI, 1.41–4.38, P = 0.002, respectively). However, no significant association was observed in monochorionic twin pregnancies.
Conclusion: Growth discordance, especially complicated by fetal growth restriction, was associated with an increased risk of postpartum hemorrhage in women with twin pregnancies undergoing cesarean section, and was more evident in patients with dichorionic twins.
Introduction
In recent years, the number and rate of multiple gestations, especially twin gestations, have risen dramatically due to advanced maternal age and the rapid development of assisted reproductive technology (ART) (1, 2). Twin pregnancies are more commonly affected by abnormal fetal growth, as the human uterus has a weak ability to meet the needs of more than one fetus. The most common abnormal fetal growth in twin pregnancies is fetal growth restriction (FGR) (3–6). In twin pregnancies, the incidence of FGR, depending on the definition of growth restriction, ranges from 16 to 48% (4). Even without FGR, twin pregnancies may be complicated by twin growth discordance, which is defined as a birth weight difference of ≥20% (7). Both FGR and twin growth discordance are known risk factors for adverse perinatal outcomes (8–15).
Postpartum hemorrhage (PPH) is one of the most common adverse perinatal outcomes in twin pregnancies. Postpartum hemorrhage is the leading cause of maternal death and poses critical health care challenges globally (16); therefore, it is crucial to identify pregnant women who are at a higher risk of PPH and implement early preventive strategies. Recently, factors including advanced maternal age, placenta previa, placental abruption, gestational hypertension, previous cesarean delivery, and fetal macrosomia have been reported to be associated with PPH (17–25). However, no study has investigated the effects of abnormal fetal growth on PPH.
This study aimed to explore the associations between twin pregnancies complicated by FGR or twin growth discordance and the risk of PPH in a retrospective twin birth cohort study conducted in Shanghai, China. Additionally, we investigated whether twin chorionicity (dichorionic and monochorionic) altered the association between abnormal fetal growth and PPH.
Methods
Study Design and Population
This retrospective cohort study was conducted at the Shanghai First Maternity and Infant Hospital, which is one of the largest tertiary maternity hospitals in Shanghai, China, with over 20,000 deliveries annually. No special informed consent was obtained, and the hospital ethics committee approved the study (registration number: KS20279). Between August 2013 and July 2020, a total of 3,395 twin gestations were delivered via cesarean section in the hospital. We included patients who delivered after 22 weeks' gestation and had complete medical records available for review. The exclusion criteria included cases where: (1) one fetus died in utero; (2) a combined delivery was performed (vaginal delivery of the first twin followed by cesarean section of the second twin); and (3) fetal structural anomalies or aneuploidy were present. Finally, 3,180 twin gestations were analyzed.
Data Collection
We reviewed the obstetric records of all women with twin pregnancies undergoing cesarean section. We extracted the demographic information of the participants from a computerized database and double-checked the data. Data on potential risk factors for PPH were collected: maternal age, gravidity, parity, ART use, gestational age at delivery, pre-pregnancy body mass index (BMI), previous cesarean section, placenta previa, uterine myoma, hypertensive disorders, placental abruption, placenta accreta/increta/percreta, low-lying placenta, hematocrit, premature rupture of membranes, emergency cesarean delivery, age at menarche, prenatal fever, and thrombocytopenia. We also collected data on unique features of the twins, such as the sex of the twins, the individual and combined birth weight of the twins, and twin chorionicity.
Definition of Abnormal Fetal Growth
The definition of FGR in twin pregnancies is inconsistent in the literature, and two separate criteria have been applied: at least one fetus with a birth weight < the 10th percentile (4, 26, 27), or at least one fetus with a birth weight < the 3rd percentile (28–30). Based on the definition of selective fetal growth restriction (sFGR) in the recent Delphi Consensus Statement, we adapted the antenatal criteria of one of the following: (1) one twin with a birth weight < the 10th centile and a birth weight discordance of >25%, or (2) the solitary criterion of one twin with a birth weight < the 3rd percentile (28, 30, 31). Singleton reference charts were used to assess birth weight centiles (28). Growth discordance was defined as a twin birth weight difference of ≥20% (twin birth weight difference = (large fetal body weight – small fetal body weight) / large fetal body weight × 100%) (32, 33).
PPH Diagnosis
The primary outcome was PPH, which was identified in our dataset using the International Classification of Diseases, Eleventh Revision, Clinical Modification (ICD-11-CM) diagnosis codes JA43.1. Secondary outcomes included PPH with severe maternal morbidity (SMM) and PPH with hemostatic interventions. We used a combination of visual estimation and quantitative blood loss (QBL) measurement to qualify blood loss (34, 35). PPH was defined as blood loss of ≥1,000 ml following delivery (36, 37). PPH with SMM was a composite outcome defined as PPH associated with any of the following: transfusion of ≥4 units of packed red blood cells, hysterectomy, return to the operating room for exploratory laparotomy, and intensive care unit admission for invasive monitoring or treatment. PPH with hemostatic interventions was defined as PPH associated with uterine artery ligation, intrauterine balloon tamponade, or uterine compression suture.
Statistical Analysis
Statistical analysis was performed using SPSS (version 16.0, SPSS Inc., Chicago, IL, USA). Continuous variables with normal distributions are presented as mean ± standard deviation (SD), while categorical data are presented as percentages (%). Parametric t-tests and χ2 tests were used to compare the differences in demographic characteristics between women with PPH and women without PPH.
The associations of FGR or twin growth discordance with the risk of PPH were estimated using a multivariable logistic regression analysis, with odds ratios (ORs) corresponding to 95% confidence intervals (CIs) as risk measures. We adjusted for the following covariates that have been shown to be associated with PPH (17–25, 38): maternal age, pre-pregnancy BMI, gravidity, parity, gestational age at delivery, age at menarche, placental abruption, placenta previa, placenta accreta, placenta increta, low-lying placenta, premature rupture of membranes, hematocrit of <30%, reduced platelet count (<70,000/μL), gestational hypertension, the use of ART, emergency operation, previous cesarean section, gestational diabetes mellitus, uterine myoma, prenatal fever, and twin chorionicity.
In order to exclude the impact of placenta accreta and increta on the association between abnormal fetal growth and PPH, we conducted a sensitivity analysis by restricting all logistic regression analyses to participants without placenta accreta or increta. Further, to investigate the potential modification effect of twin chorionicity, we stratified the study population by twin chorionicity and assessed the association of abnormal fetal growth with PPH in dichorionic and monochorionic twins separately. All analyses were bilateral, and statistical significance was set at P < 0.05.
Results
Characteristics of the Study Participants
Altogether, 3,180 twin pregnancies were included in the final analysis. The overall incidence of PPH in this cohort was 4.3% (n = 138). The incidence of PPH with SMM and PPH with obstetric surgical procedures was 3.3% and 3.6%, respectively. Table 1 presents the participants' general characteristics. Women with PPH were significantly older than those without PPH (32.2 ± 3.8 vs. 31.5 ± 3.9, respectively, P = 0.043). The incidence of hypertensive disorders, hematocrit of <30%, and the use of ART were significantly higher in women with PPH than in women without PPH (P < 0.001, P = 0.021, P < 0.001, respectively). Moreover, the incidence of an abnormal placenta, such as placental abruption, placenta previa, placenta accreta, and placenta increta, was significantly different between the two groups (All values were P < 0.001).
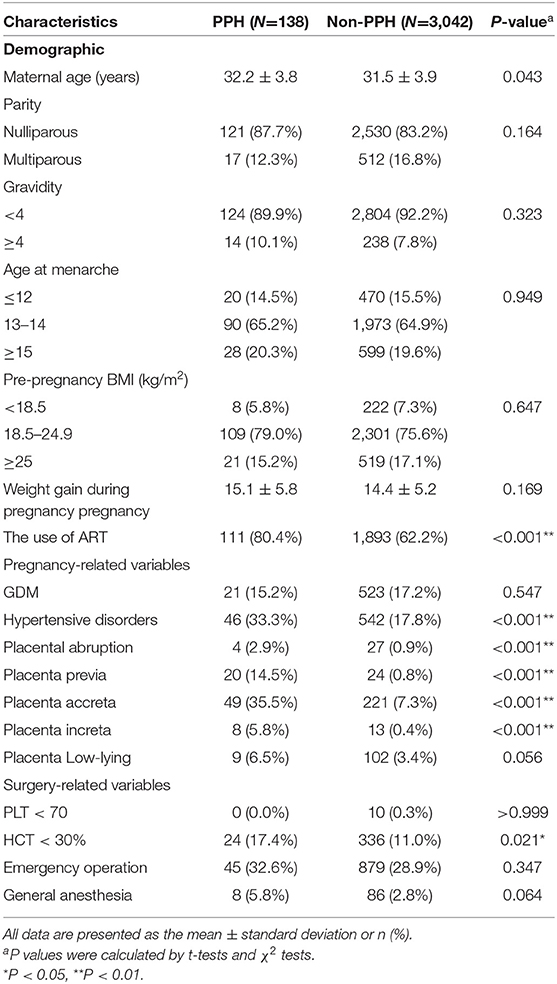
Table 1. Baseline characteristics of twin pregnancies complicated by PPH compared to non-PPH twin pregnancies.
Associations Between Abnormal Fetal Growth and Risk of PPH
The associations of FGR or twin growth discordance with the risk of PPH are shown in Table 2. In general, both FGR and sFGR were not associated with PPH, while twin growth discordance was significantly associated with an increased risk of PPH. In the adjusted model, compared to mothers of concordant growth twins, the odds of PPH increased by 62% (OR = 1.62, 95% CI, 1.05–2.51) for mothers of discordant twins. The co-presence of twin growth discordance and FGR was also significantly associated with an increased risk of PPH.

Table 2. Logistic regression analysis for the associations between twin growth discordance, fetal growth restriction (FGR), and risk of PPH.
Association Between Fetal Growth Anomalies and Secondary Outcomes
Table 3 presents the association of abnormal fetal growth with the risk of two secondary outcomes: PPH with SMM and PPH with hemostatic interventions. Similar to the results of PPH, both twin growth discordance and co-presence of twin growth discordance with FGR were associated with an increased risk of PPH with hemostatic interventions. In the adjusted model, compared to mothers of concordant growth twins, the odds of PPH with hemostatic interventions increased by 62% (OR = 1.62, 95% CI, 1.00–2.63) in mothers of discordant twins. For PPH with SMM, only the co-presence of twin growth discordance with FGR (birth weight <3rd percentile) was associated with an increased risk of PPH with SMM (OR = 2.07; 95% CI, 1.17–3.68).
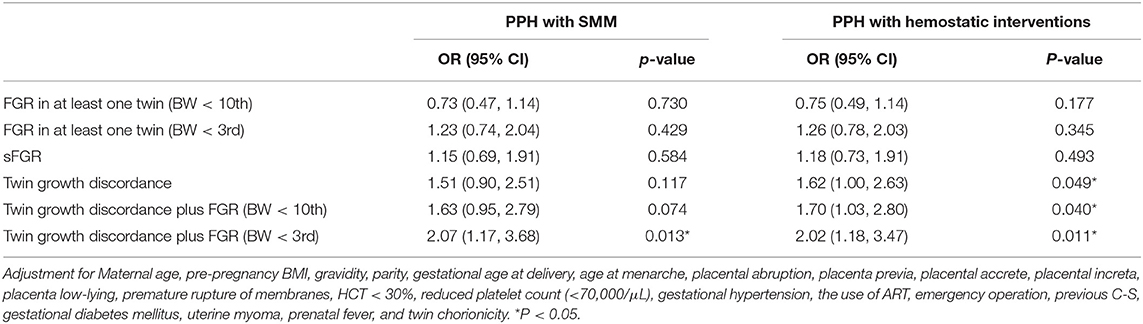
Table 3. The Associations between twin growth discordance, fetal growth restriction (FGR), and secondary outcomes.
Sensitivity Analysis
In the sensitivity analysis, when restricting the analysis to participating women without placenta accreta or placenta increta, the association between twin growth discordance or co-presence of twin growth discordance with FGR and PPH risk did not appreciably change. However, the 95% CIs for ORs became wider and the results were no longer statistically significant and the results were no longer statistically significant owing to a reduction in the sample size (Table 4).
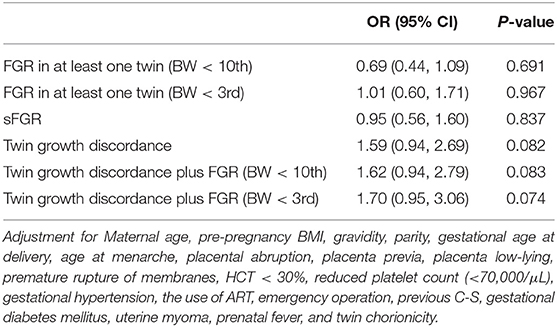
Table 4. The Association between intertwin growth discordance, fetal growth restriction (FGR), and PPH among participants without placenta accrete or placenta increta.
We further stratified the participants by twin chorionicity and estimated the association of abnormal fetal growth with PPH in dichorionic and monochorionic twins separately. As shown in Table 5, among mothers of dichorionic twins, twin growth discordance and co-presence of twin growth discordance with FGR was significantly associated with an increased risk of PPH. However, among mothers of monochorionic twins, no significance was found.
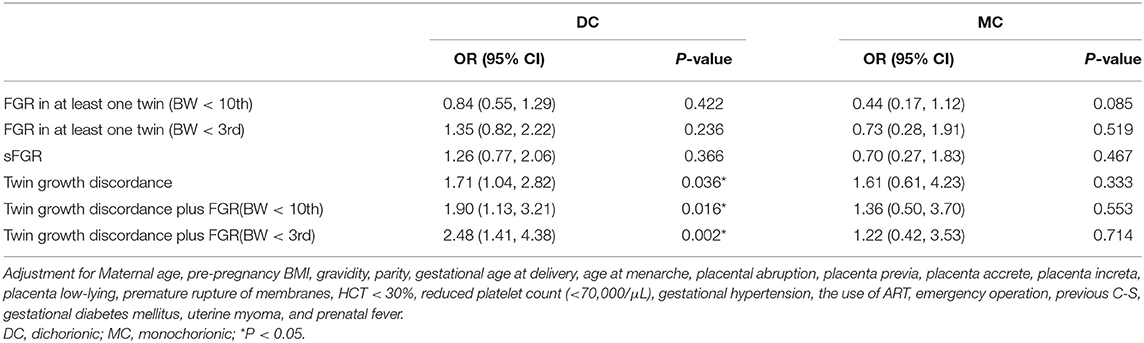
Table 5. The Association between intertwin growth discordance, fetal growth restriction, and PPH stratified by chorionicity.
Discussion
Principal Findings
Our findings demonstrated that twin growth discordance or twin growth discordance complicated by FGR was associated with an increased risk of PPH, and the associations were much more evident in mothers of dichorionic twins than in mothers of monochorionic twins. However, we found no association between FGR and PPH. Our findings suggest that twin growth discordance is an independent risk factor for PPH.
Interpretation of the Findings
PPH is one of the leading causes of maternal morbidity and mortality worldwide (39–42). Over the past few decades, many studies have focused on the predictors of PPH, and several factors have been reported to be associated with PPH (17–25). Several maternal risk-assessment tools, such as the California Maternal Quality Care Collaborative, the Association of Women's Health, Obstetric and Neonatal Nurses, and the New York Safety Bundle for Obstetric Hemorrhage, have also been developed to assess the risk of PPH (43). Compared to singleton gestations, PPH is more common in twin pregnancies, as uterine overdistention may impair the contraction of uterine muscles and increase the incidence of uterine atony after delivery (44). To date, no study has examined the association between FGR and PPH in twins. However, in singleton pregnancies, a study has reported that women with pregnancies complicated by both preeclampsia and FGR are more likely to experience abruption, have a higher rate of cesarean delivery, and undergo cesarean delivery for fetal heart rate abnormalities, but not for PPH (45).
Growth discordance is a proprietary feature of twin pregnancies, and it is one of the major determinants of perinatal outcomes in twin pregnancies (11, 12). Here, the overall incidence rate was approximately 16.9%, which is consistent with the results of previous studies (4, 11, 32). Higher degrees of discordance are known to be associated with perinatal mortality and morbidity (11, 13–15). A study has shown that a within-pair birth weight difference of >25% increases the risk of both intra-uterine death and neonatal death (13). However, whether there is a correlation between twin growth discordance and PPH remains unknown. To the best of our knowledge, this is the first report on the association between growth discordance and PPH in women with twin pregnancies.
The underlying mechanism between twin growth discordance and PPH is unclear. A potential mechanism may involve the notion that growth discordance increases the risk of preeclampsia or hypertension (28, 32), which are important risk factors for PPH (18, 22, 24). Interestingly, in our study, after adjusting for hypertensive disorders, we found that the association between twin growth discordance and PPH remained significant. Another possible explanation for the observed association is that twin growth discordance and PPH may have some common risk factors. Known risk factors for twin growth discordance are advanced maternal age and parity, conception by ART, maternal hypertensive disorders in pregnancy, opposite sex of twin fetuses, and exposure to air pollution during pregnancy (46–48). These can be categorized as maternal, fetal, placental, or environmental risk factors. Among these factors, advanced maternal age and parity, conception by ART, and maternal hypertensive disorders are also risk factors for PPH (17, 19, 20, 22, 24, 49). Other pathophysiological mechanisms include histological placenta and inflammatory responses (32, 50). Frequently, histological abnormalities in placentas were found among smaller twins of birth weight discordant pairs (50). Oxidative stress and apoptosis in the placenta may result from the increased demand imposed by twins and from placental ischemia/hypoxia, leading to growth discordance (51). Additionally, various active molecules released into the maternal circulation due to placental ischemia/hypoxia causes vasoconstriction and an increase in blood pressure, and this is due to generalized endothelial dysfunction and an exaggerated inflammatory response (32).
We also found that the relationship between growth discordance and PPH existed only among mothers of dichorionic twins but not among those with monochorionic twins. Fetal growth during gestation is generally determined by fetal, maternal, and uterine placental factors. Discordant growth among dichorionic twins may be due to the poor ability of the smaller twin to realize its growth potential, which commonly suggests a pathological condition, such as placental vascular dysfunction. For monochorionic twins, the cause of discordant growth is related to unequal distribution of uteroplacental blood flow between two fetuses, abnormal umbilical cord insertion site, and critically by twin-to-twin transfusion syndrome, while factors related to placental histology are rare (52–55). In a prospective study of 1,001 twin pairs, an association between abnormalities in placental histology and birth weight discordance was found in dichorionic twins, but not in monochorionic twins (50). Similarly, another study showed that excess placental apoptosis and changes in the synthesis of various trophoblastic proteins were found in discordant dichorionic twins (51). The incidence of preeclampsia in women with dichorionic pregnancies is much higher than that in women with monochorionic twins (56, 57). Qiao et al. reported that twin growth discordance was associated with a high risk of preeclampsia among women with dichorionic twins (32). All of the above factors may partially explain the relationship between growth discordance and PPH in the dichorionic twin group. Compared to singleton gestation, twin gestation increased the risk of placenta accreta spectrum (including placenta accreta, increta, and percreta) independent of measured risk factors (58). Besides, in twin pregnancies, the assisted reproductive technology is independently associated with placenta accreta spectrum (59). Based on the above reasons, the incidence of placenta accreta spectrum is higher in twins. This may explain why the association between twin growth discordance or twin growth discordance complicated by FGR and PPH was not apparent when we excluded these twins with placenta accreta spectrum.
Strengths and Limitations
This study is the first report on the relationship between growth discordance and PPH. Another strength of our study is the relatively large sample size from a single center. However, our study has several limitations. First, it only included twin pregnancies delivered via cesarean section. Due to physician counseling and maternal requirements for selective cesarean section to avoid combined delivery, the cesarean delivery rate of twin pregnancies has increased dramatically (60–62). In our center, nearly 90% of women with twin pregnancies undergo a cesarean section. During a cesarean section, the amniotic fluid is absorbed, and another aspirator is used to absorb blood, and this accurately measures the estimated amount of blood loss; however, it is impossible to accurately estimate the blood loss in vaginal deliveries. Second, due to the lack of unified international standard for the diagnosis of FGR in twins, we used the singleton birth weight standards as the diagnostic criteria of FGR. Recently, twin-specific charts were recommended when evaluating fetal growth in twin pregnancies in some studies (28, 30, 63). However, pathological growth tracks and at-risk fetuses may be obscured by twin-specific growth charts. Finally, although we adjusted for various confounders, some unmeasured confounders may invalidate the association between growth discordance and PPH.
Conclusions
We found that twin growth discordance, rather than FGR, was associated with an increased risk of PPH. Our findings suggest that twin growth discordance is an independent risk factor for PPH. This signals obstetricians and midwives to implement early preventative strategies for PPH among mothers of growth discordant twins.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee of Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
XC, YL, and SZ: full access to all of the data in the study, take responsibility for the integrity of the data, the accuracy of the data analysis, and drafting of the manuscript. XC and ZX: concept and design. XC, YL, SZ, XQ, and ZX: critical revision of the manuscript for important intellectual content. QZ and ZX: statistical analysis. YL, QZ, and XQ: administrative, technical, or material support. ZX and ZL: supervision. All authors: acquisition, analysis, or interpretation of data.
Funding
This work was supported by the grants of Pudong Health Committee of Shanghai (PW2021D-01 and PW2020D-13).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank Yan Zhao from the Department of Women & Children's Health Care, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University Shanghai, China, for the support provided in the statistical analysis.
Abbreviations
ART, assisted reproductive technology; FGR, fetal growth restriction; PPH, Postpartum hemorrhage; SMM, severe maternal morbidity; OR, odds ratio; CI, confidence interval; sFGR, selective fetal growth restriction.
References
1. Adashi EY, Gutman R. Delayed childbearing as a growing, previously unrecognized contributor to the national plural birth excess. Obstet Gynecol. (2018) 132:999–1006. doi: 10.1097/AOG.0000000000002853
2. Blondel B, Coulm B, Bonnet C, Goffinet F, Le Ray C, National National Coordination Group of the National Perinatal Surveys, et al. Trends in perinatal health in metropolitan France from 1995 to 2016: results from the French National Perinatal Surveys. J Gynecol Obstet Hum Reprod. (2017) 46:701–13. doi: 10.1016/j.jogoh.2017.09.002
3. Cleary-Goldman J, D'Alton ME. Growth abnormalities and multiple gestations. Semin Perinatol. (2008) 32:206–12. doi: 10.1053/j.semperi.2008.02.009
4. Fox N, Rebarber A, Klauser C, Roman A, Saltzman D. Intrauterine growth restriction in twin pregnancies: incidence and associated risk factors. Am J Perinatol. (2010) 28:267–72. doi: 10.1055/s-0030-1270116
5. Kibel M, Kahn M, Sherman C, Kingdom J, Zaltz A, Barrett J, et al. Placental abnormalities differ between small for gestational age fetuses in dichorionic twin and singleton pregnancies. Placenta. (2017) 60:28–35. doi: 10.1016/j.placenta.2017.10.002
6. Townsend R, Khalil A. Fetal growth restriction in twins. Best Pract Res Clin Obstet Gynaecol. (2018) 49:79–88. doi: 10.1016/j.bpobgyn.2018.02.004
7. Bagchi S, Salihu HM. Birth weight discordance in multiple gestations: occurrence and outcomes. J Obstet Gynaecol. (2006) 26:291–6. doi: 10.1080/01443610600594724
8. Gardosi J, Madurasinghe V, Williams M, Malik A, Francis A. Maternal and fetal risk factors for stillbirth: population based study. BMJ. (2013) 346:f108. doi: 10.1136/bmj.f108
9. S MK, Gardosi J. Perinatal mortality and fetal growth restriction. Best Pract Res Clin Obstet Gynaecol. (2004) 18:397–410. doi: 10.1016/j.bpobgyn.2004.02.009
10. Audette MC, Kingdom JC. Screening for fetal growth restriction and placental insufficiency. Semin Fetal Neonatal Med. (2018) 23:119–25. doi: 10.1016/j.siny.2017.11.004
11. Miller J, Chauhan SP, Abuhamad AZ. Discordant twins: diagnosis, evaluation and management. Am J Obstet Gynecol. (2012) 206:10–20. doi: 10.1016/j.ajog.2011.06.075
12. Harper LM, Weis MA, Odibo AO, Roehl KA, Macones GA, Cahill AG, et al. Significance of growth discordance in appropriately grown twins. Am J Obstet Gynecol. (2013) 208:393.e1–5. doi: 10.1016/j.ajog.2013.01.044
13. D'Antonio F, Odibo AO, Prefumo F, Khalil A, Buca D, Flacco ME, et al. Weight discordance and perinatal mortality in twin pregnancy: systematic review and meta-analysis. Ultrasound Obstet Gynecol. (2018) 52:11–23. doi: 10.1002/uog.18966
14. Di Mascio D, Acharya G, Khalil A, Odibo A, Prefumo F, Liberati M, et al. Birthweight discordance and neonatal morbidity in twin pregnancies: a systematic review and meta-analysis. Acta Obstet Gynecol Scand. (2019) 98:1245–57. doi: 10.1111/aogs.13613
15. ACOG Practice Bulletin No. 144. Multifetal gestations: twin, triplet, and higher-order multifetal pregnancies. Obstet Gynecol. (2014) 123:1118–32. doi: 10.1097/01.AOG.0000446856.51061.3e
16. Blitz MJ, Yukhayev A, Pachtman SL, Reisner J, Moses D, Sison CP, et al. Twin pregnancy and risk of postpartum hemorrhage. J Matern Fetal Neonatal Med. (2020) 33:3740–5. doi: 10.1080/14767058.2019.1583736
17. Ekin A, Gezer C, Solmaz U, Taner CE, Dogan A, Ozeren M, et al. Predictors of severity in primary postpartum hemorrhage. Arch Gynecol Obstet. (2015) 292:1247–54. doi: 10.1007/s00404-015-3771-5
18. Suzuki S, Hiraizumi Y, Miyake H. Risk factors for postpartum hemorrhage requiring transfusion in cesarean deliveries for Japanese twins: comparison with those for singletons. Arch Gynecol Obstet. (2012) 286:1363–7. doi: 10.1007/s00404-012-2461-9
19. Kramer MS, Berg C, Abenhaim H, Dahhou M, Rouleau J, Mehrabadi A, et al. Incidence, risk factors, and temporal trends in severe postpartum hemorrhage. Am J Obstet Gynecol. (2013) 209:449.e1–7. doi: 10.1016/j.ajog.2013.07.007
20. Borovac-Pinheiro A, Pacagnella RC, Cecatti JG, Miller S, El Ayadi AM, Souza JP, et al. Postpartum hemorrhage: new insights for definition and diagnosis. Am J Obstet Gynecol. (2018) 219:162–8. doi: 10.1016/j.ajog.2018.04.013
21. Butwick AJ, Abreo A, Bateman BT, Lee HC, El-Sayed YY, Stephansson O, et al. Effect of maternal body mass index on postpartum hemorrhage. Anesthesiology. (2018) 128:774–83. doi: 10.1097/ALN.0000000000002082
22. Merriam AA, Wright JD, Siddiq Z, D'Alton ME, Friedman AM, Ananth CV, et al. Risk for postpartum hemorrhage, transfusion, and hemorrhage-related morbidity at low, moderate, and high volume hospitals. J Matern Fetal Neonatal Med. (2018) 31:1025–34. doi: 10.1080/14767058.2017.1306050
23. Chen C, Liu X, Chen D, Huang S, Yan X, Liu H, et al. A risk model to predict severe postpartum hemorrhage in patients with placenta previa: a single-center retrospective study. Ann Palliat Med. (2019) 8:611–21. doi: 10.21037/apm.2019.09.04
24. Kebede BA, Abdo RA, Anshebo AA, Gebremariam BM. Prevalence and predictors of primary postpartum hemorrhage: an implication for designing effective intervention at selected hospitals, Southern Ethiopia. PLoS ONE. (2019) 14:e0224579. doi: 10.1371/journal.pone.0224579
25. Zhu C, Wang M, Niu G, Yang J, Wang Z. Obstetric outcomes of twin pregnancies at advanced maternal age: a retrospective study. Taiwan J Obstet Gynecol. (2018) 57:64–7. doi: 10.1016/j.tjog.2017.12.010
26. Gaccioli F, Aye I, Sovio U, Charnock-Jones DS, Smith GCS. Screening for fetal growth restriction using fetal biometry combined with maternal biomarkers. Am J Obstet Gynecol. (2018) 218:S725–37. doi: 10.1016/j.ajog.2017.12.002
27. ACOG Practice Bulletin No. 204: Fetal growth restriction. Obstet Gynecol. (2019) 133:e97-e109. doi: 10.1097/AOG.0000000000003070
28. Giorgione V, Bhide A, Bhate R, Reed K, Khalil A. Are twin pregnancies complicated by weight discordance or fetal growth restriction at higher risk of preeclampsia? J Clin Med. (2020) 9:3276. doi: 10.3390/jcm9103276
29. Gordijn SJ, Beune IM, Thilaganathan B, Papageorghiou A, Baschat AA, Baker PN, et al. Consensus definition of fetal growth restriction: a delphi procedure. Ultrasound Obstet Gynecol. (2016) 48:333–9. doi: 10.1002/uog.15884
30. Kalafat E, Abiola A, Thilaganathan B, Bhide A, Khalil A. The association between hypertension in pregnancy and preterm birth with fetal growth restriction in singleton and twin pregnancy: use of twin versus singleton charts. J Clin Med. (2020) 9:2518. doi: 10.3390/jcm9082518
31. Khalil A, Beune I, Hecher K, Wynia K, Ganzevoort W, Reed K, et al. Consensus definition and essential reporting parameters of selective fetal growth restriction in twin pregnancy: a delphi procedure. Ultrasound Obstet Gynecol. (2019) 53:47–54. doi: 10.1002/uog.19013
32. Qiao P, Zhao Y, Jiang X, Xu C, Yang Y, Bao Y, et al. Impact of growth discordance in twins on preeclampsia based on chorionicity. Am J Obstet Gynecol. (2020) 223:572.e1–8. doi: 10.1016/j.ajog.2020.03.024
33. Khalil A, Rodgers M, Baschat A, Bhide A, Gratacos E, Hecher K, et al. ISUOG practice guidelines: role of ultrasound in twin pregnancy. Ultrasound Obstet Gynecol. (2016) 47:247–63. doi: 10.1002/uog.15821
34. Bienstock JL, Eke AC, Hueppchen NA. Postpartum Hemorrhage. N Engl J Med. (2021) 384:1635–45. doi: 10.1056/NEJMra1513247
35. Prevention and management of postpartum haemorrhage: green-top guideline No. 52. BJOG. (2017) 124:e106–49. doi: 10.1111/1471-0528.14178
36. Lalonde A. International Federation of Gynecology and Obstetrics. Prevention and treatment of postpartum hemorrhage in low-resource settings. Int J Gynaecol Obstet. (2012) 117:108–18. doi: 10.1016/j.ijgo.2012.03.001
37. Practice Bulletin No. 183: Postpartum hemorrhage. Obstet Gynecol. (2017) 130:e168–86. doi: 10.1097/AOG.0000000000002351
38. Huang C, Deng J, Xu Y, Wu H, Peng C, Wu L, et al. Early age at menarche and risk of postpartum hemorrhage: a retrospective study in Chinese women. J Matern Fetal Neonatal Med. (2020) 35:2266–272. doi: 10.1080/14767058.2020.1784871
39. Haeri S, Dildy GA 3rd. Maternal mortality from hemorrhage. Semin Perinatol. (2012) 36:48–55. doi: 10.1053/j.semperi.2011.09.010
40. Nathan LM. An overview of obstetric hemorrhage. Semin Perinatol. (2019) 43:2–4. doi: 10.1053/j.semperi.2018.11.001
41. Kassebaum NJ, Barber RM, Bhutta ZA, Dandona L, Gething PW, Hay SI, et al. Global, regional, and national levels of maternal mortality, 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet. (2016) 388:1775–812. doi: 10.1016/S0140-6736(16)31470-2
42. Berg CJ, Harper MA, Atkinson SM, Bell EA, Brown HL, Hage ML, et al. Preventability of pregnancy-related deaths: results of a state-wide review. Obstet Gynecol. (2005) 106:1228–34. doi: 10.1097/01.AOG.0000187894.71913.e8
43. Kawakita T, Mokhtari N, Huang JC, Landy HJ. Evaluation of risk-assessment tools for severe postpartum hemorrhage in women undergoing cesarean delivery. Obstet Gynecol. (2019) 134:1308–16. doi: 10.1097/AOG.0000000000003574
44. Madar H, Goffinet F, Seco A, Rozenberg P, Dupont C, Deneux-Tharaux C, et al. Severe acute maternal morbidity in twin compared with singleton pregnancies. Obstet Gynecol. (2019) 133:1141–50. doi: 10.1097/AOG.0000000000003261
45. Sharma KJ, Esakoff TF, Guillet A, Burwick RM, Caughey AB. Pregnancies complicated by both preeclampsia and growth restriction between 34 and 37 weeks' gestation are associated with adverse perinatal outcomes. J Matern Fetal Neonatal Med. (2017) 30:2342–5. doi: 10.1080/14767058.2016.1248394
46. Bijnens EM, Derom C, Gielen M, Winckelmans E, Fierens F, Vlietinck R, et al. Small for gestational age and exposure to particulate air pollution in the early-life environment of twins. Environ Res. (2016) 148:39–45. doi: 10.1016/j.envres.2016.03.006
47. Mariet AS, Mauny F, Pujol S, Thiriez G, Sagot P, Riethmuller D, et al. Multiple pregnancies and air pollution in moderately polluted cities: is there an association between air pollution and fetal growth? Environ Int. (2018) 121:890–7. doi: 10.1016/j.envint.2018.10.015
48. Qiao P, Zhao Y, Cai J, van Donkelaar A, Martin R, Ying H, et al. Twin growth discordance in association with maternal exposure to fine particulate matter and its chemical constituents during late pregnancy. Environ Int. (2019) 133:105148. doi: 10.1016/j.envint.2019.105148
49. Nyflot LT, Sandven I, Oldereid NB, Stray-Pedersen B, Vangen S. Assisted reproductive technology and severe postpartum haemorrhage: a case-control study. BJOG. (2017) 124:1198–205. doi: 10.1111/1471-0528.14471
50. Kent EM, Breathnach FM, Gillan JE, McAuliffe FM, Geary MP, Daly S, et al. Placental pathology, birthweight discordance, and growth restriction in twin pregnancy: results of the ESPRiT study. Am J Obstet Gynecol. (2012) 207:220.e1–5. doi: 10.1016/j.ajog.2012.06.022
51. Hubinont C, Lewi L, Bernard P, Marbaix E, Debieve F, Jauniaux E, et al. Anomalies of the placenta and umbilical cord in twin gestations. Am J Obstet Gynecol. (2015) 213:S91–102. doi: 10.1016/j.ajog.2015.06.054
52. Breathnach FM, Malone FD. Fetal growth disorders in twin gestations. Semin Perinatol. (2012) 36:175–81. doi: 10.1053/j.semperi.2012.02.002
53. Lewi L, Devlieger R, De Catte L, Deprest J. Growth discordance. Best Pract Res Clin Obstet Gynaecol. (2014) 28:295–303. doi: 10.1016/j.bpobgyn.2013.12.003
54. Fick AL, Feldstein VA, Norton ME, Wassel Fyr C, Caughey AB, Machin GA, et al. Unequal placental sharing and birth weight discordance in monochorionic diamniotic twins. Am J Obstet Gynecol. (2006) 195:178–83. doi: 10.1016/j.ajog.2006.01.015
55. Cambiaso O, Zhao DP, Abasolo JI, Aiello HA, Oepkes D, Lopriore E, et al. Discordance of cord insertions as a predictor of discordant fetal growth in monochorionic twins. Placenta. (2016) 47:81–5. doi: 10.1016/j.placenta.2016.09.009
56. Sparks TN, Cheng YW, Phan N, Caughey AB. Does risk of preeclampsia differ by twin chorionicity? J Matern-Fetal Neonatal Med. (2013) 26:1273–7. doi: 10.3109/14767058.2013.777701
57. Bartnik P, Kosinska-Kaczynska K, Kacperczyk J, Ananicz W, Sierocinska A, Wielgos M, et al. Twin chorionicity and the risk of hypertensive disorders: gestational hypertension and pre-eclampsia. Twin Res Hum Genet. (2016) 19:377–82. doi: 10.1017/thg.2016.17
58. Miller HE, Leonard SA, Fox KA, Carusi DA, Lyell DJ. Placenta accreta spectrum among women with twin gestations. Obstet Gynecol. (2021) 137:132–8. doi: 10.1097/AOG.0000000000004204
59. Jiang F, Gao J, He J, Tang Y, Cao Y, Wang X, et al. Obstetric outcomes for twins from different conception methods—A multicenter cross-sectional study from China. Acta Obstet Gynecol Scand. (2021) 100:1061–7. doi: 10.1111/aogs.14116
60. Tal A, Zafran N, Peretz H, Garmi G, Romano S, Salim R, et al. Trend in cesarean delivery rate among twin pregnancies over a 20 years epoch and the accompanied maternal and perinatal outcomes. Eur J Obstet Gynecol Reprod Biol X. (2019) 3:100023. doi: 10.1016/j.eurox.2019.100023
61. Lee HC, Gould JB, Boscardin WJ, El-Sayed YY, Blumenfeld YJ. Trends in cesarean delivery for twin births in the United States: 1995-2008. Obstet Gynecol. (2011) 118:1095–101. doi: 10.1097/AOG.0b013e3182318651
62. Rissanen AS, Jernman RM, Gissler M, Nupponen I, Nuutila ME. Maternal complications in twin pregnancies in Finland during 1987-2014: a retrospective study. BMC Pregnancy Childbirth. (2019) 19:337. doi: 10.1186/s12884-019-2498-x
Keywords: chorionicity, cesarean section, fetal growth restriction, growth discordance, postpartum hemorrhage, twin pregnancy
Citation: Cao X, Luo Y, Zhou S, Zhao Q, Qin X, Liu Z and Xu Z (2022) Twin Growth Discordance and Risk of Postpartum Hemorrhage: A Retrospective Cohort Study. Front. Med. 9:876411. doi: 10.3389/fmed.2022.876411
Received: 15 February 2022; Accepted: 25 April 2022;
Published: 25 May 2022.
Edited by:
Depeng Zhao, Shenzhen Maternity and Child Healthcare Hospital, ChinaReviewed by:
Ferdinando Antonio Gulino, Azienda di Rilievo Nazionale e di Alta Specializzazione (ARNAS) Garibaldi, ItalySi Zeng, Sichuan Academy of Medical Sciences and Sichuan Provincial People's Hospital, China
Copyright © 2022 Cao, Luo, Zhou, Zhao, Qin, Liu and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhiqiang Liu, ZHJsaXV6aGlxaWFuZyYjeDAwMDQwOzE2My5jb20=; Zhendong Xu, YnR4emQxMjMmI3gwMDA0MDsxMjYuY29t
†These authors have contributed equally to this work and share first authorship