 Matthias L. Herrmann1,2*
Matthias L. Herrmann1,2* Cindy Boden2
Cindy Boden2 Christoph Maurer1,3
Christoph Maurer1,3 Felix Kentischer3
Felix Kentischer3 Eva Mennig4Sören Wagner5,6Lars O. Conzelmann7Bernd R. Förstner8
Eva Mennig4Sören Wagner5,6Lars O. Conzelmann7Bernd R. Förstner8 Michael A. Rapp8
Michael A. Rapp8 Christine A. F. von Arnim9
Christine A. F. von Arnim9 Michael Denkinger10,11
Michael Denkinger10,11 Gerhard W. Eschweiler2
Gerhard W. Eschweiler2 Christine Thomas2,4
Christine Thomas2,4- 1Department of Neurology and Neurophysiology, Medical Center-University of Freiburg, Freiburg, Germany
- 2Geriatric Center and Department of Psychiatry and Psychotherapy, Tübingen University Hospital, Tübingen, Germany
- 3Center for Geriatrics and Gerontology, University Medical Center Freiburg, Freiburg, Germany
- 4Department of Geriatric Psychiatry and Psychotherapy, Klinikum Stuttgart, Stuttgart, Germany
- 5Department of Anesthesiology, Klinikum Stuttgart, Stuttgart, Germany
- 6Department of Anesthesia, Critical Care and Pain Medicine, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, United States
- 7Helios Clinic for Cardiac Surgery, Karlsruhe, Karlsruhe, Germany
- 8Department of Social and Preventive Medicine, University of Potsdam, Potsdam, Germany
- 9Department of Geriatrics, University Medical Center Göttingen, Georg August University, Göttingen, Germany
- 10Geriatric Center, Agaplesion Bethesda Clinic Ulm, Ulm, Germany
- 11Institute for Geriatric Research, Ulm University Medical Center, Ulm, Germany
Introduction: Postoperative delirium (POD) is a common and serious adverse event of surgery in older people. Because of its great impact on patients' safety and quality of life, identification of modifiable risk factors could be useful. Although preoperative medication intake is assumed to be an important modifiable risk factor, the impact of anticholinergic drugs on the occurrence of POD seems underestimated in elective surgery. The aim of this study was to investigate the association between preoperative anticholinergic burden and POD. We hypothesized that a high preoperative anticholinergic burden is an independent, potentially modifiable predisposing and precipitating factor of POD in older people.
Methods: Between November 2017 and April 2019, 1,470 patients of 70 years and older undergoing elective orthopedic, general, cardiac, or vascular surgery were recruited in the randomized, prospective, multicenter PAWEL trial. Anticholinergic burden of a sub-cohort of 899 patients, who did not receive a multimodal intervention for preventing POD, was assessed by two different tools at hospital admission: The established Anticholinergic Risk Scale (ARS) and the recently developed Anticholinergic Burden Score (ABS). POD was detected by confusion assessment method (CAM) and a validated post discharge medical record review. Logistic regression analyses were performed to evaluate the association between anticholinergic burden and POD.
Results: POD was observed in 210 of 899 patients (23.4%). Both ARS and ABS were independently associated with POD. The association persisted after adjustment for relevant confounding factors such as age, sex, comorbidities, preoperative cognitive and physical status, number of prescribed drugs, surgery time, type of surgery and anesthesia, usage of heart-lung-machine, and treatment in intensive care unit. If a patient was taking one of the 56 drugs listed in the ABS, risk for POD was 2.7-fold higher (OR = 2.74, 95% CI = 1.55–4.94) and 1.5-fold higher per additional point on the ARS (OR = 1.54, 95% CI = 1.15–2.02).
Conclusion: Preoperative anticholinergic drug exposure measured by ARS or ABS was independently associated with POD in older patients undergoing elective surgery. Therefore, identification, discontinuation or substitution of anticholinergic medication prior to surgery may be a promising approach to reduce the risk of POD in older patients.
Introduction
Delirium is a neuropsychiatric syndrome defined by acute decline and fluctuation of attention, cognitive function, and disturbance of awareness (1). Especially in older patients, delirium is a common and serious adverse event of surgery (2) with an incidence ranging from 11 to 51% (3, 4). Postoperative delirium (POD) in older people is often associated with persistent cognitive dysfunction, dementia, higher rates of institutionalization, and increased morbidity and mortality (5, 6). Its etiology is believed to be multifactorial. Besides neuro-inflammation and blood-brain barrier leakage, a neurotransmitter disbalance in terms of acetylcholine deficiency and dopamine excess is thought to be involved in the pathogenesis of delirium (7). Electroencephalographic changes in delirium such as occipital slowing are also indicative of acetylcholine deficiency (8). Multiple pre- and perioperative risk factors are known to predispose to delirium. Preoperative factors comprise age, multimorbidity, frailty, polypharmacy, and deficits in cognitive, sensory, and mobility function (9, 10). Perioperative parameters that have been identified are, for example, type of surgery and anesthesia, surgery time and treatment in intensive care units (2, 9). Because delirium negatively affects patients' safety and quality of life, identifying modifiable risk factors could be of great relevance for its prevention, especially in older patients (11–13). In this regard, preoperative medication use is considered one of the most important potentially modifiable factors in the prevention of POD (14).
Assuming that delirium might be precipitated by an imbalance in cerebral neurotransmission specifically including acetylcholine deficiency (15), drugs with anticholinergic properties (DAPs) could have a significant impact on POD. DAPs are frequently prescribed in older people for a variety of indications such as minor and major depression, bladder disorders, or nausea (16). The cumulative effect of all DAPs taken regularly by an individual is often referred to as the anticholinergic burden (17). However, numerous studies indicated adverse effects of DAPs on cognitive and physical function (18, 19). Anticholinergic burden has been associated with delirium in several settings (18, 20, 21), although results were conflicting (22). Studies on the effect of DAPs on POD are less frequent, and their results were also inconsistent, with one positive (23) and two negatives studies (24, 25). Different results could be caused by the use of different scores calculating anticholinergic burden, small sample sizes, and different definitions of delirium. Therefore, in this study, we used the established Anticholinergic Risk Scale (ARS), which was most consistently associated with delirium (22). In addition, we applied a new, promising score developed in a very large sample of 250,000 participants to assess associations between long-term anticholinergic medication use and the risk of dementia (16). We hypothesized that a high preoperative anticholinergic burden is an independent, potentially modifiable predisposing and precipitating factor for POD in older people.
Methods
Study Design
This study is based on a secondary analysis of data collected from 1,470 patients between November 2017 and April 2019 for the PAWEL-Study (Patient safety, cost-effectiveness and quality of life: reduction of delirium risk and postoperative cognitive dysfunction after elective procedures in older adults). The complete protocol for this randomized, prospective, multicenter study has been described in detail previously (12). Briefly, inclusion criteria comprised patients aged 70 years and older scheduled for elective surgery with an expected duration of surgery of at least 60 min. Surgical procedures included orthopedic, general, cardiac, and vascular surgery conducted at five medical centers in the southwest of Germany. Exclusion criteria were life expectancy <15 months, insufficient knowledge of German language, and recently diagnosed severe dementia without a legal representative. We included the sub-cohort of 899 participants of the baseline group who did not receive a multimodal intervention for preventing POD analogous to the PAWEL risk factor study (10).
Data Collection in the Pre-, Peri-, and Postoperative Phase
Demographic and clinical data were collected at baseline, no more than 3 weeks before the scheduled surgery, including medical history by Charlson Comorbidity Index (26), cognitive screening by Montreal Cognitive Assessment [MoCA, (27)], preoperative physical status by classification of the American Society of Anesthesiologists [ASA, (28)], and functional status by Barthel Index (29) as well as nutritional condition by Body Mass Index. Preoperative depression and anxiety symptoms were assessed by the Patient Health Questionnaire (30). Perioperative data included premedication, surgical procedure with or without cardiopulmonary bypass, cut-to-suture time, and type of anesthesia. Parameters were collected from anesthesia and surgery protocols.
Anticholinergic Drug Exposure
Each patient's medication was analyzed on admission using the medication list and personal medical history. Long-term medications as well as “as-needed” (“PRN”) medication were included in the analysis if they were taken more than 3 days a week. In view of the high proportion of “over-the-counter”-drugs, the use of sleeping pills was explicitly queried. Preoperative anticholinergic burden was calculated for each patient using the Anticholinergic Risk Scale [ARS (31)]. Briefly summarized, the ARS is a weighted score developed by Rudolph et al. (31), which often has been used in studies investigating the association between anticholinergic burden and delirium in different study populations (21). It comprises 49 DAPs evaluated from 0 (no or low anticholinergic activity) to 3 (highest anticholinergic activity). The sum of all values provides the patient's individual anticholinergic burden. However, the ARS has not been updated since 2008 and the weights of different DAPs are a matter of debate (22). We therefore added the anticholinergic score recently published by Coupland et al. (16). This measure is primarily based on the score of Gray et al. (32) which comprises medications with strong anticholinergic properties identified by the American Geriatrics Society Beers Criteria Update Expert panel (33). Originally, this anticholinergic score was intended to assess the cumulative anticholinergic burden to evaluate associations between long-term anticholinergic drug exposure and the risk of dementia in a large cohort (16). Hereinafter, this score is called Anticholinergic Burden Score (ABS). The ABS includes 56 DAPs of different subgroups which previously have been described in detail (16). In contrast to the ARS, the ABS does not weigh anticholinergic properties of medications but counts the number of received DAPs. Therefore, in this study, we define the preoperative anticholinergic burden as the sum of all DAPs according to the ABS. We did not include the cumulative dosage of the identified DAPs. To our best knowledge, the ABS is used to investigate the association between anticholinergic burden and POD here for the first time.
Outcome Measures
Primary outcome measure was the occurrence of POD after elective surgery. POD was evaluated daily for up to 7 postoperative days by independent and previously trained assessors (10, 12) using the Confusion Assessment Method in a German operationalized version [CAM, (34, 35)]. Additionally, a chart review based on the DSM-V criteria for delirium (1) was conducted by experienced physicians at discharge. Similar to the SAGES Study (36), POD was defined if at least one of the methods indicated delirium (37).
Statistical Analysis
Differences between patients with and without POD were evaluated for categorical variables by χ2 test and for non-normally distributed continuous variables by Mann-Whitney U test. Logistic regression analysis was used to investigate the independent association of preoperative anticholinergic burden and the incidence of POD (Odds Ratios with 95% confidence intervals). First, univariate logistic regression was performed for both, ARS and ABS. In a second step, the model was adjusted for items that were found to be strong confounders in previous studies (2, 4, 10). These were age, sex, Charlson Comorbidity Index, preoperative cognitive status (MoCA), physical status (ASA), number of prescribed drugs, preoperative serum creatinine, surgery time, type of surgery and anesthesia, usage of heart-lung-machine, and treatment in intensive care unit. Missing data in confounding variables led to the exclusion of 53 patients from the adjusted multivariate analysis, which was finally performed on 846 patients. Data were analyzed with the software IBM SPSS Statistics Version 25 (IBM Corporation, Armonk, NY, USA). Results were considered statistically significant at a level of p < 0.05.
Results
Participants' Characteristics
The sociodemographic and clinical characteristics of all 899 patients aged 70 and older are described in Table 1. The mean age of the participants was 77.3 years (range 70–98 years), and 49.4% were female. According to the Charlson Comorbidity Index, 282 patients (31.4%) had at least three diseases. Participants were taking a median of six drugs with 56.6% taking ≥5 drugs. Most of the enrolled patients had orthopedic surgery (e.g., hip, knee, and spine, n = 474, 52.7%). Another group of 377 patients (37.5%) received cardiovascular interventions with or without cardiopulmonary bypass. The remaining 88 patients (9.8%) underwent general surgery (e.g., abdominal surgery). Surgeries were mostly performed under general anesthesia (n = 726, 80.8%).
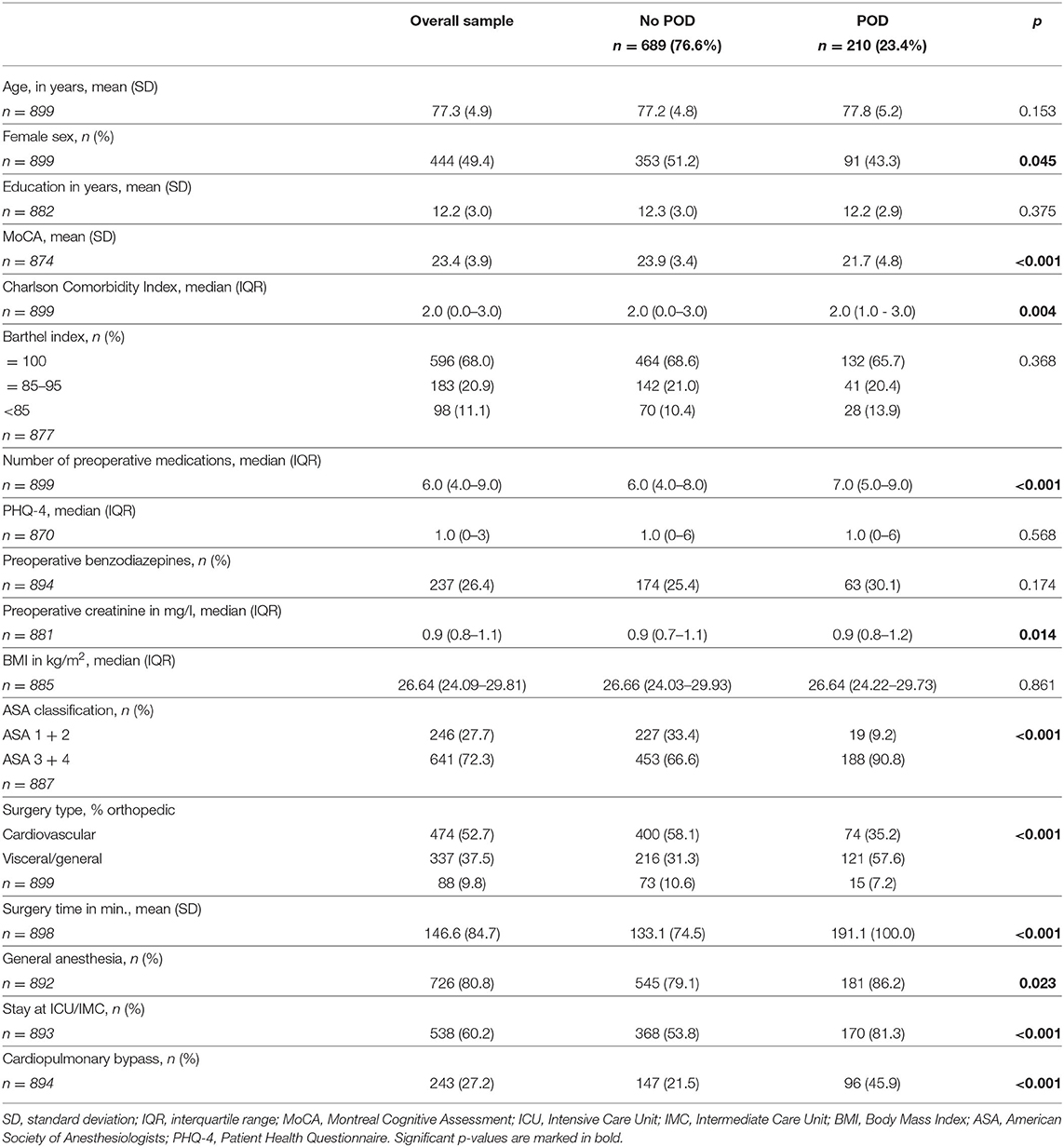
Table 1. Sociodemographic and clinical characteristics of enrolled patients.
POD was observed in 210 (23.4%) patients. Patients diagnosed with POD took significantly more medications (p < 0.001), had more comorbidities (p = 0.004), and revealed a lower MoCA level at baseline assessment (p < 0.001). Furthermore, patients with POD had a longer surgery time (p < 0.001), and were admitted to an intensive care unit more often (p < 0.001). POD occurred significantly more often in patients requiring cardiopulmonary bypass (p < 0.001). General anesthesia was performed more frequently in patients with POD (p = 0.023). POD and non-POD groups did not differ statistically in Body Mass Index, educational level, Barthel Index, preoperative depression, anxiety or treatment with benzodiazepines (see Table 1).
Association Between Preoperative Anticholinergic Burden and POD
Using the ARS score, 81 patients (9%) were taking at least one anticholinergic drug. Patients with POD had a significantly higher ARS value than patients without POD (p = 0.004). Evaluating medication according to ABS criteria, 71 patients (8%) were taking DAPs. Comparing the POD and non-POD groups, the rate of DAPs was significantly higher in patients with POD (ABS = 1: 6 vs. 11%, ABS = 2: 0 vs. 7%). The most frequently prescribed DAP in both groups (according the ABS criteria) was amitriptyline (n = 8 in each group) followed in the delirium group by doxepine (n = 4) and solifenacin (n = 3). In patients without POD, trospium (n = 7) and trimipramine (n = 6) were the most commonly used DAPs, in addition to amitriptyline. The top 10 DAPs prescribed are shown in Figure 1.
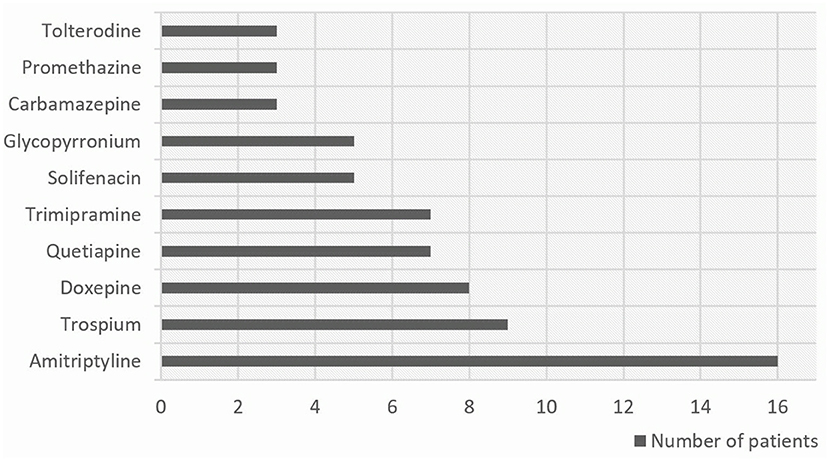
Figure 1. The ten most prescribed DAPs in our study population according to the Anticholinergic Burden Score (ABS).
Although the number of patients taking DAPs and the number of different DAPs (ARS: n = 22, ABS: n = 19) was relatively small in our study population, we found significant group differences. This was the case when ARS was used and when ABS criteria were applied. In the subgroup of 71 patients who received one or two ABS drugs, the POD rate was 42.3% (n = 30/71) and thus almost twice as high as in the group without ABS medication where POD occurred in only 21.7% (n = 180/828, see Table 2).
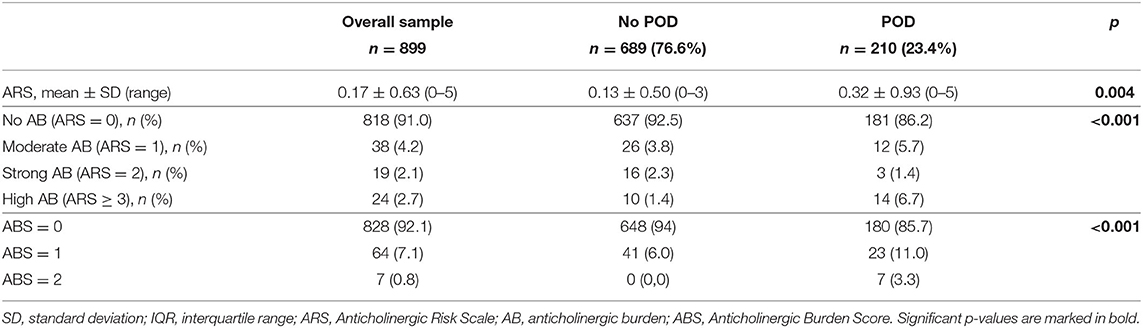
Table 2. Characteristics of anticholinergic burden according to ARS and ABS in patients with and without postoperative delirium.
Univariate logistic regression analysis revealed a positive association with the occurrence of POD for both scales, ARS and ABS. Odds ratios (ORs) and corresponding 95% confidence intervals (CI) are provided in Table 3. After adjustment for confounding variables, ORs changed only marginally and the positive association with the occurrence of POD persisted. Each additional point in the ARS was associated with a 1.5-fold higher risk of developing POD (OR = 1.54, 95% CI = 1.15–2.02). Applying the ABS criteria resulted in a 2.7 higher likelihood of POD (OR = 2.74, 95% CI = 1.55–4.94) for each additional DAP.
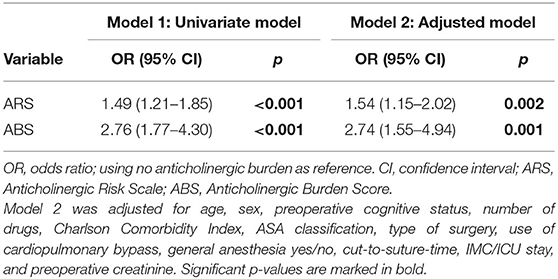
Table 3. Odds ratios for postoperative delirium according to ARS and ABS.
One of the confounding variables we included in the adjusted regression analysis (Table 3) was the ASA physical status classification, which is widely used to assess pre-anesthesia medical comorbidities. The Barthel Index is commonly applied to assess the functional status of older patients. Thus, we additionally performed an adjusted regression analysis using the Barthel Index instead of the ASA classification. The ORs for both, ARS (OR = 1.37, 95% CI = 1.04–1.81) and ABS (OR = 2.44, 95% CI = 1.39–4.28), changed only slightly. This result confirms that neither physical status (ASA) nor functional status (Barthel Index) accounted for the increase of POD with anticholinergic medication.
Discussion
Preoperative anticholinergic medication exposure was assessed by two different scales estimating the overall anticholinergic burden, the weighted ARS and the more recent ABS. The findings of this study suggest that anticholinergic medication usage might be an independent risk factor for POD in older population undergoing elective surgery. The reduction or omission of these drugs preoperatively might thus be beneficial for the prevention of POD.
Our results are in line with several previous studies, which reported an association between anticholinergic drug exposure measured with the ARS and the occurrence of delirium in older patients (38–41). A recently published systematic review by Egberts et al. showed that among the variety of existing anticholinergic drug scales, the Anticholinergic Risk Scale (ARS) was the only one found to be consistently associated with delirium (22). Also, our findings are in accordance with a published study by Mueller et al. who showed an independent association between preoperative anticholinergic burden and the occurrence of POD (prevalence 10%) in a sample of older cancer patients (mean age 71 years, n = 651) (23). Yet, in contrast to our study, this study used the Anticholinergic Drug Score (42) to determine the anticholinergic burden. Other studies did not find an association between anticholinergic burden and delirium (43, 44). Reasons for the inconsistent results of the studies are manifold. One reason could be that the measurement of the anticholinergic load has not yet been standardized (22). This leads to a large body of existing literature concerning DAPs and a lack of consensus on how to quantify the anticholinergic burden. In recent years, numerous different scales have been developed. However, they vary widely in their structure, focus, application, measurement of anticholinergic properties (serum vs. predefined) and association with outcomes (21). Therefore, comparability of individual study findings is limited, and an international consent on the most feasible instrument is strongly needed. The use of different tools to determine the anticholinergic burden is one explanation for the inconsistent findings of previous studies. Furthermore, there is a large heterogeneity in study populations comprising residents of nursing homes (38), Australian veterans (45), Taiwanese National Health Insurance database (46), palliative care inpatients (39) and acutely ill hospitalized patients (20, 40), making it even more difficult to compare results. Moorey et al. claimed that delirium is not associated with the anticholinergic burden in older patients on admission to an acute hospital (43). In contrast to our study, they used the Anticholinergic Cognitive Burden Scale (47) and the Anticholinergic Drug Score which were both not consistently associated with delirium (22). Pasina et al. also used the Anticholinergic Cognitive Burden Scale in their recently published study and did not find a clear association between anticholinergic burden and delirium in patients admitted to an acute geriatric ward (44). Also, in contrast to our findings, a recently published study by Heinrich et al. found no association between preoperative anticholinergic load and POD using the Anticholinergic Cognitive Burden Scale, the Anticholinergic Drug Score and the ARS (24). However, compared to our study, these patients were significantly younger (POD: 74 years, no POD: 71 years in median) and patients with more than mild cognitive impairment (Mini-Mental State Examination score ≤ 23 points) were excluded.
As mentioned above, to our best knowledge, this is the first study using the ABS to explore the effect of DAPs on delirium. In comparison to the ARS, ORs for occurrence of POD were clearly higher using the ABS than the ARS. Our results suggest a 2.7-fold risk of developing a POD for each drug included in the ABS. Therefore, our findings provide a strong argument for modifiable delirium risk assessment by ABS in older patients scheduled for surgery. The PAWEL study's intervention bundle AKTIVER (Alltags- und Kognitions-Training & Interdisziplinarität verbessert Ergebnis und mindert das Risiko [“everyday skills and cognition training and interdisciplinarity improves outcome and mitigates risk”]) has been shown to reduce delirium by 33% in patients undergoing elective orthopedic and abdominal surgery by daily application of individualized modules on activation, relaxation and diagnostic chaperonage during the hospital stay (37). In addition to those actions for delirium prevention, software programs, or an app could be implemented into the hospital clinical information system to raise awareness of detrimental drugs even before surgery of older patients to enable discontinuation or substitution prior to anesthesia to avoid postoperative delirium. In most cases, alternatives more appropriate for older people are available or medication is not crucial during the vulnerable perioperative period. However, further studies are required to validate ABS as a useful tool to reduce the risk of POD in older patients in addition to the AKTIVER bundle.
Limitations and Strengths
This study has several limitations. First, our approach to measure anticholinergic drug exposure did not include the dosages of DAPs. It is quite conceivable that higher dosages of DAPs have a stronger negative impact on the development of POD. Second, the ARS was developed in 2008 and was not updated since then. This could lead to an underestimation of anticholinergic burden due to an abandonment of newer DAPs. Third, we collected our information from patients' medication lists and verbal information but had little information about adherence to prescriptions prior to hospital admission. Finally, we did not consider delirium severity and duration in this study. The strengths of our study are the prospective multicenter study-design, the large number of patients and the usage of two different tools to measure anticholinergic burden. In addition to the established ARS as a weighted score, we used ABS as a quick and simple instrument to quantify anticholinergic burden in delirium patients for the first time. A further strength is the relatively high number of strong confounders like cognition included in our multivariable regression analysis.
Conclusion
This study of 899 older patients undergoing various elective surgical procedures shows that the preoperative anticholinergic burden, assessed by ARS or ABS, is an independent risk factor for POD in older patients. Delirium occurrence was more than 2.7 times higher if a patient took at least one of the 56 drugs listed in the ABS (16), even after controlling for the most known delirium risk factors. The POD rate increased from 21.7 to 42.3% in patients receiving one or two ABS drugs. Identifying DAPs prior to hospital admission might be an opportunity to terminate or substitute anticholinergic drugs preoperatively and prevent delirium after elective surgery.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
This study was approved by the Ethics Commission of the Faculty of Medicine of the Eberhard-Karls University and University Hospital Tübingen with number 233/2017BO1 on October 12, 2017 and by the Ethics Commission of the University of Potsdam with number 38/2017 on December 11, 2017. The study was registered on the German Clinical Trials Register (DRKS-ID: DRKS00012797) in July, 2017. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MH, CT, and GE designed this secondary analysis of the PAWEL-Study, planned the data collection, performed the statistical analysis, and prepared and revised the manuscript. CB, CM, FK, EM, SW, LC, BF, MR, CA, and MD were involved in data collection and critically revised the manuscript for final approval of the version to be published. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the Innovationsfonds (Fund of the Federal Joint Committee, Gemeinsamer Bundesausschuss, G-BA; AZ: VF1_2016-201), which had no role in the design of the study and had no role either during its execution, analyses of the data, or in the decision to submit any results. We acknowledge support by the Open Access Publication Fund of the University of Freiburg.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors thank all the patients and relatives, who were interviewed and assessed. They also thank all staff members at the recruiting centers and all members of the PAWEL Study group.
References
1. American Psychiatric A.ssociation. Diagnostic and Statistical Manual of Mental Disorders (5th Edn). (2013). doi: 10.1176/appi.books.9780890425596
2. Aldecoa C, Bettelli G, Bilotta F, Sanders RD, Audisio R, Borozdina A, et al. European Society of Anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur J Anaesthesiol. (2017) 34:192–214. doi: 10.1097/EJA.0000000000000594
3. Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. (2014) 383:911–22. doi: 10.1016/S0140-6736(13)60688-1
4. American Geriatrics Society. American Geriatrics Society abstracted clinical practice guideline for postoperative delirium in older adults. J Am Geriatr Soc. (2015) 63:142–50. doi: 10.1111/jgs.13281
5. Ansaloni L, Catena F, Chattat R, Fortuna D, Franceschi C, Mascitti P, et al. Risk factors and incidence of postoperative delirium in elderly patients after elective and emergency surgery. Br J Surg. (2010) 97:273–80. doi: 10.1002/bjs.6843
6. Witlox J, Eurelings LS, de Jonghe JF, Kalisvaart KJ, Eikelenboom P, van Gool WA. Delirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysis. JAMA. (2010) 304:443–51. doi: 10.1001/jama.2010.1013
7. Maldonado JR. Neuropathogenesis of delirium: review of current etiologic theories and common pathways. Am J Geriatr Psychiatry. (2013) 21:1190–222. doi: 10.1016/j.jagp.2013.09.005
8. Thomas C, Hestermann U, Kopitz J, Plaschke K, Oster P, Driessen M, et al. Serum anticholinergic activity and cerebral cholinergic dysfunction: an EEG study in frail elderly with and without delirium. BMC Neurosci. (2008) 9:86. doi: 10.1186/1471-2202-9-86
9. Guenther U, Riedel L, Radtke FM. Patients prone for postoperative delirium: preoperative assessment, perioperative prophylaxis, postoperative treatment. Curr Opin Anaesthesiol. (2016) 29:384–90. doi: 10.1097/ACO.0000000000000327
10. Eschweiler GW, Czornik M, Herrmann ML, Knauer YP, Forkavets O, von Arnim CAF, et al. Presurgical screening improves risk prediction for delirium in elective surgery of older patients: the PAWEL RISK study. Front Aging Neurosci. (2021) 13:679933. doi: 10.3389/fnagi.2021.679933
11. Martinez F, Tobar C, Hill N. Preventing delirium: should non-pharmacological, multicomponent interventions be used? A systematic review and meta-analysis of the literature. Age Ageing. (2015) 44:196–204. doi: 10.1093/ageing/afu173
12. Sanchez A, Thomas C, Deeken F, Wagner S, Kloppel S, Kentischer F, et al. Patient safety, cost-effectiveness, and quality of life: reduction of delirium risk and postoperative cognitive dysfunction after elective procedures in older adults-study protocol for a stepped-wedge cluster randomized trial (PAWEL Study). Trials. (2019) 20:71. doi: 10.1186/s13063-018-3148-8
13. Burton JK, Craig LE, Yong SQ, Siddiqi N, Teale EA, Woodhouse R, et al. Non-pharmacological interventions for preventing delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. (2021) 7:Cd013307. doi: 10.1002/14651858.CD013307.pub2
14. Kassie GM, Nguyen TA, Kalisch Ellett LM, Pratt NL, Roughead EE. Preoperative medication use and postoperative delirium: a systematic review. BMC Geriatr. (2017) 17:298. doi: 10.1186/s12877-017-0695-x
15. Collamati A, Martone AM, Poscia A, Brandi V, Celi M, Marzetti E, et al. Anticholinergic drugs and negative outcomes in the older population: from biological plausibility to clinical evidence. Aging Clin Exp Res. (2016) 28:25–35. doi: 10.1007/s40520-015-0359-7
16. Coupland CAC, Hill T, Dening T, Morriss R, Moore M, Hippisley-Cox J. Anticholinergic drug exposure and the risk of dementia: a nested case-control study. JAMA Intern Med. (2019) 179:1084–93. doi: 10.1001/jamainternmed.2019.0677
17. Tune LE. Anticholinergic effects of medication in elderly patients. J Clin Psychiatry. (2001) 62:11–4. Available online at: https://www.psychiatrist.com/read-pdf/833/
18. Fox C, Smith T, Maidment I, Chan WY, Bua N, Myint PK, et al. Effect of medications with anti-cholinergic properties on cognitive function, delirium, physical function and mortality: a systematic review. Age Ageing. (2014) 43:604–15. doi: 10.1093/ageing/afu096
19. Salahudeen MS, Duffull SB, Nishtala PS. Anticholinergic burden quantified by anticholinergic risk scales and adverse outcomes in older people: a systematic review. BMC Geriatr. (2015) 15:31. doi: 10.1186/s12877-015-0029-9
20. Egberts A, van der Craats ST, van Wijk MD, Alkilabe S, van den Bemt P, Mattace-Raso FUS. Anticholinergic drug exposure is associated with delirium and postdischarge institutionalization in acutely ill hospitalized older patients. Pharmacol Res Perspect. (2017) 5:e00310. doi: 10.1002/prp2.310
21. Welsh TJ, van der Wardt V, Ojo G, Gordon AL, Gladman JRF. Anticholinergic drug burden tools/scales and adverse outcomes in different clinical settings: a systematic review of reviews. Drugs Aging. (2018) 35:523–38. doi: 10.1007/s40266-018-0549-z
22. Egberts A, Moreno-Gonzalez R, Alan H, Ziere G, Mattace-Raso FUS. Anticholinergic drug burden and delirium: a systematic review. J Am Med Dir Assoc. (2021) 22:65–73.e64. doi: 10.1016/j.jamda.2020.04.019
23. Mueller A, Spies CD, Eckardt R, Weiss B, Pohrt A, Wernecke KD, et al. Anticholinergic burden of long-term medication is an independent risk factor for the development of postoperative delirium: a clinical trial. J Clin Anesth. (2019) 61:109632. doi: 10.1016/j.jclinane.2019.109632
24. Heinrich M, Muller A, Cvijan A, Morgeli R, Kruppa J, Winterer G, et al. Preoperative comparison of three anticholinergic drug scales in older adult patients and development of postoperative delirium: a prospective observational study. Drugs Aging. (2021) 38:347–54. doi: 10.1007/s40266-021-00839-5
25. Tillemans MPH, Butterhoff-Terlingen MH, Stuffken R, Vreeswijk R, Egberts TCG, Kalisvaart KJ. The effect of the anticholinergic burden on duration and severity of delirium in older hip-surgery patients with and without haloperidol prophylaxis: a post hoc analysis. Brain Behav. (2021) 11:e2404. doi: 10.1002/brb3.2404
26. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. (1987) 40:373–83. doi: 10.1016/0021-9681(87)90171-8
27. Nasreddine ZS, Phillips NA, Bedirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. (2005) 53:695–9. doi: 10.1111/j.1532-5415.2005.53221.x
28. Wolters U, Wolf T, Stutzer H, Schroder T. ASA classification and perioperative variables as predictors of postoperative outcome. Br J Anaesth. (1996) 77:217–22. doi: 10.1093/bja/77.2.217
29. Lubke N, Meinck M, Von Renteln-Kruse W. [The Barthel Index in geriatrics. A context analysis for the Hamburg Classification Manual]. Z Gerontol Geriatr. (2004) 37:316–26. doi: 10.1007/s00391-004-0233-2
30. Kroenke K, Spitzer RL, Williams JB, Lowe B. An ultra-brief screening scale for anxiety and depression: the PHQ-4. Psychosomatics. (2009) 50:613–21. doi: 10.1176/appi.psy.50.6.613
31. Rudolph JL, Salow MJ, Angelini MC, McGlinchey RE. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med. (2008) 168:508–13. doi: 10.1001/archinternmed.2007.106
32. Gray SL, Anderson ML, Dublin S, Hanlon JT, Hubbard R, Walker R, et al. Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Intern Med. (2015) 175:401–7. doi: 10.1001/jamainternmed.2014.7663
33. American Geriatrics Society. American Geriatrics Society 2019 Updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. (2019) 67: 674–94. doi: 10.1111/jgs.15767
34. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. (1990) 113:941–8. doi: 10.7326/0003-4819-113-12-941
35. Thomas C, Kreisel SH, Oster P, Driessen M, Arolt V, Inouye SK. Diagnosing delirium in older hospitalized adults with dementia: adapting the confusion assessment method to international classification of diseases, tenth revision, diagnostic criteria. J Am Geriatr Soc. (2012) 60:1471–7. doi: 10.1111/j.1532-5415.2012.04066.x
36. Schmitt EM, Saczynski JS, Kosar CM, Jones RN, Alsop DC, Fong TG, et al. The Successful Aging after Elective Surgery (SAGES) study: cohort description and data quality procedures. J Am Geriatr Soc. (2015) 63:2463–71. doi: 10.1111/jgs.13793
37. Deeken F, Sanchez A, Rapp MA, Denkinger M, Brefka S, Spank J, et al. Outcomes of a delirium prevention program in older persons after elective surgery: a stepped-wedge cluster randomized clinical trial. JAMA Surg. (2021) 157:e216370. doi: 10.1001/jamasurg.2021.6370
38. Landi F, Dell'Aquila G, Collamati A, Martone AM, Zuliani G, Gasperini B, et al. Anticholinergic drug use and negative outcomes among the frail elderly population living in a nursing home. J Am Med Dir Assoc. (2014) 15:825–9. doi: 10.1016/j.jamda.2014.08.002
39. Zimmerman KM, Salow M, Skarf LM, Kostas T, Paquin A, Simone MJ, et al. Increasing anticholinergic burden and delirium in palliative care inpatients. Palliat Med. (2014) 28:335–41. doi: 10.1177/0269216314522105
40. Wolters AE, Zaal IJ, Veldhuijzen DS, Cremer OL, Devlin JW, van Dijk D, et al. Anticholinergic medication use and transition to delirium in critically ill patients: a prospective cohort study. Crit Care Med. (2015) 43:1846–52. doi: 10.1097/CCM.0000000000001094
41. Hwang S, Jun K, Ah YM, Han E, Chung JE, Lee JY. Impact of anticholinergic burden on emergency department visits among older adults in Korea: a national population cohort study. Arch Gerontol Geriatr. (2019) 85:103912. doi: 10.1016/j.archger.2019.103912
42. Carnahan RM, Lund BC, Perry PJ, Pollock BG, Culp KR. The Anticholinergic Drug Scale as a measure of drug-related anticholinergic burden: associations with serum anticholinergic activity. J Clin Pharmacol. (2006) 46:1481–6. doi: 10.1177/0091270006292126
43. Moorey HC, Zaidman S, Jackson TA. Delirium is not associated with anticholinergic burden or polypharmacy in older patients on admission to an acute hospital: an observational case control study. BMC Geriatr. (2016) 16:162. doi: 10.1186/s12877-016-0336-9
44. Pasina L, Colzani L, Cortesi L, Tettamanti M, Zambon A, Nobili A, et al. Relation between delirium and anticholinergic drug burden in a cohort of hospitalized older patients: an observational study. Drugs Aging. (2019) 36:85–91. doi: 10.1007/s40266-018-0612-9
45. Kalisch Ellett LM, Pratt NL, Ramsay EN, Barratt JD, Roughead EE. Multiple anticholinergic medication use and risk of hospital admission for confusion or dementia. J Am Geriatr Soc. (2014) 62:1916–22. doi: 10.1111/jgs.13054
46. Huang KH, Chan YF, Shih HC, Lee CY. Relationship between Potentially Inappropriate Anticholinergic Drugs (PIADs) and adverse outcomes among elderly patients in Taiwan. J Food Drug Anal. (2012) 20:930–937+985. doi: 10.6227/jfda.2012200423
Keywords: delirium, acute encephalopathy, surgery, anticholinergic, geriatric, postoperative
Citation: Herrmann ML, Boden C, Maurer C, Kentischer F, Mennig E, Wagner S, Conzelmann LO, Förstner BR, Rapp MA, von Arnim CAF, Denkinger M, Eschweiler GW and Thomas C (2022) Anticholinergic Drug Exposure Increases the Risk of Delirium in Older Patients Undergoing Elective Surgery. Front. Med. 9:871229. doi: 10.3389/fmed.2022.871229
Received: 05 March 2022; Accepted: 29 March 2022;
Published: 06 May 2022.
Edited by:
Giuseppe Bellelli, University of Milano-Bicocca, ItalyReviewed by:
Angelique Egberts, Erasmus Medical Center, NetherlandsJoaquim Cerejeira, University of Coimbra, Portugal
Copyright © 2022 Herrmann, Boden, Maurer, Kentischer, Mennig, Wagner, Conzelmann, Förstner, Rapp, von Arnim, Denkinger, Eschweiler and Thomas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matthias L. Herrmann, bWF0dGhpYXMuaGVycm1hbm4ubmxvQHVuaWtsaW5pay1mcmVpYnVyZy5kZQ==