 André Hajek
André Hajek Benedikt Kretzler
Benedikt Kretzler- Department of Health Economics and Health Services Research, University Medical Center Hamburg-Eppendorf, Hamburg Center for Health Economics, Hamburg, Germany
Background: Various studies have identified the prevalence of prefrailty and frailty among older adults in Germany. Nevertheless, there is no review systematically synthesizing these studies. Thus, our aim was to close this gap in knowledge. Moreover, another aim was to perform a meta-analysis to synthesize the pooled prevalence of prefrailty and frailty. A further aim was to explore potential sources of heterogeneity based on a meta-regression.
Methods: A number of three electronic databases (PubMed, PsycINFO, and CINAHL) were searched (plus an additional hand search). The observational studies that determine the prevalence of frailty among older adults aged 65 years and above in Germany were included, whereas disease-specific samples were excluded. Data extraction included the description of the sample, operationalization of frailty, statistical analysis, sample characteristics and main findings. The established Joanna Briggs Institute (JBI) standardized critical appraisal instrument for prevalence studies was used for evaluating the quality of the studies. Important steps were performed by two reviewers.
Results: In sum, a number of 12 studies were included. The prevalence of frailty varied from about 2.4 to 25.6%. The pooled prevalence of frailty was 13.7% (95% CI: 9.0 to 18.5%). There was a significant heterogeneity among the studies (I2 = 98.9%, p < 0.001). The pooled prevalence of prefrailty was 40.2% (95% CI: 28.3 to 52.1%; I2 = 99.6%, p < 0.001). Some evidence of a publication bias exists. Meta-regressions showed that some of the heterogeneity was explained by the tool to quantify frailty and the average age of the respective sample.
Conclusion: Particularly, the high prevalence of prefrailty should be highlighted since it is important to prevent individuals in old age from developing to frail status. This knowledge is important for the German society as a whole and for relevant stakeholders.
Systematic Review Registration: PROSPERO, identifier: CRD42021293648.
Introduction
Common attributes of frailty are a lack of physiological reserve and an increased vulnerability to stressors (1). Clegg et al. (2) defined it as “a state of vulnerability to poor resolution of homoeostasis after a stressor event” (p. 759).
Former research has demonstrated that frailty can increase the likelihood of institutionalization (3) and mortality (4, 5). Additionally, frailty can contribute to high economic costs (6). Against the backdrop of demographic aging, it is often assumed that the number of individuals with frailty will rise considerably (7). This underlines the importance of knowledge about the general prevalence of frailty.
For example, a recent systematic review and meta-analysis showed a pooled prevalence of frailty of 7.4% (95% confidence interval: 6.1–9.0%) among Japanese community-dwelling older people (8). While some studies also exist identifying the prevalence of prefrailty and frailty among older adults in Germany [e.g., among individuals aged 65 years and above: 2.8% were frail (9); among individuals aged 85 years and over: 31.7% of individuals were frail (10)]; a systematic review is lacking which systematically synthesizes the current evidence.
Thus, our first aim was to systematically summarize this evidence among older adults (i.e., 65 years and older) in Germany. Our second aim was to perform a meta-analysis to synthesize the pooled prevalence of frailty and also prefrailty among older adults in Germany—which can help to obtain more accurate prevalence rates of frailty. This is the important basic information for individuals involved in frailty research. Third, a meta-regression will be conducted to identify the impact of potentially moderating factors (such as tools used to quantify frailty). Our work may also help to identify knowledge gaps and can consequently inspire upcoming frailty research.
Methods
Our current work is in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines (11). Additionally, it has been registered in the International Prospective Register of Systematic Reviews (PROSPERO: CRD42021293648).
In December 2021, three electronic databases (MEDLINE, PsycINFO, and CINAHL) were searched. Our search strategy (MEDLINE) is displayed in Table 1.

Table 1. MEDLINE search algorithm.
Using two steps (title/abstract screening first and after that full-text screening), two reviewers (AH and BK) assessed the suitability. In addition, a hand search of the reference lists of retrieved papers was conducted. The discussions were used to resolve any discrepancies. This practice was also applied when there were any discrepancies in extracting the data or assessment of the study quality.
Main inclusion criteria for the screening included (i) cross-sectional and longitudinal observational studies identifying the prevalence of frailty among older adults (65 years and over) residing in Germany, (ii) studies adequately assessing frailty, (iii) studies published in peer-reviewed journals, (iv) and studies published in German or English language.
The cutoff for older adults (i.e., 65 years) was selected because in Germany, the age of 65 years was set in past years for retirement and commonly characterizes the transition from middle age to old age.
Main exclusion criteria included (i) the studies solely investigating samples with a specific disorder (e.g., individuals with mental disorders), (ii) the assessment of key variables (i.e., frailty) not appropriate (e.g., single item with two values to quantify frailty), and (iii) the studies not published in peer-reviewed journal.
Disease-specific samples were excluded since they may not be generalizable to the general population in late life.
No restrictions were applied with regard to the time and location of publication (except for Germany).
Prior to final eligibility criteria, a pretest was done (i.e., both reviewers screened a sample of 100 titles/abstracts and discussed their results). However, eligibility criteria were not refined.
With regard to the data extraction, while one reviewer (BK) extracted the data, a second reviewer (AH) checked the data extraction. The data extraction focused on the description of the sample, operationalization of frailty, statistical analysis, sample characteristics, and main findings.
To assess the quality of the studies, we used the established Joanna Briggs Institute (JBI) standardized critical appraisal instrument for prevalence studies (12). The resulting score ranged from 0 to 9 (higher values indicate higher study quality and less risk of bias).
Regarding meta-analysis, random-effect models were used to pool proportions across the studies. The underlying assumption of the random-effect models is that heterogeneity across studies exists. Following the recommendations, heterogeneity between studies was assessed using the I2 statistic [I2 values from 25 to 50%: low; 50 to 75%: moderate; 75% or more: high heterogeneity (13)]. The established “metaprop” (14) command was used to conduct the meta-analysis.
Regarding meta-regression (including these factors: mean age, assessment of frailty, and risk of bias score), the “meta regress” command from Stata 16 was used [more precisely, random-effects, with restricted maximum likelihood; moreover, Knapp-Hartung adjustment for the standard errors was used (15)]. The effect sizes were recalculated in a first step (16) because the coefficients are initially scaled as double arcsin values rather than proportions. Such meta-regressions were computed to examine the roots of heterogeneity (17).
A funnel plot and the Egger's test (p < 0.05 indicates publication bias) were applied to examine the publication bias. Stata 16.1 (College Station, TX, USA) was used for all analyses.
Results
Overview: Included Studies
In Figure 1 (11), the selection process is displayed. In sum, a number of 12 studies were included in our systematic review—and also in meta-analysis. In Table 2, a study overview that includes the main findings is given (10, 18, 20, 21, 23–30).
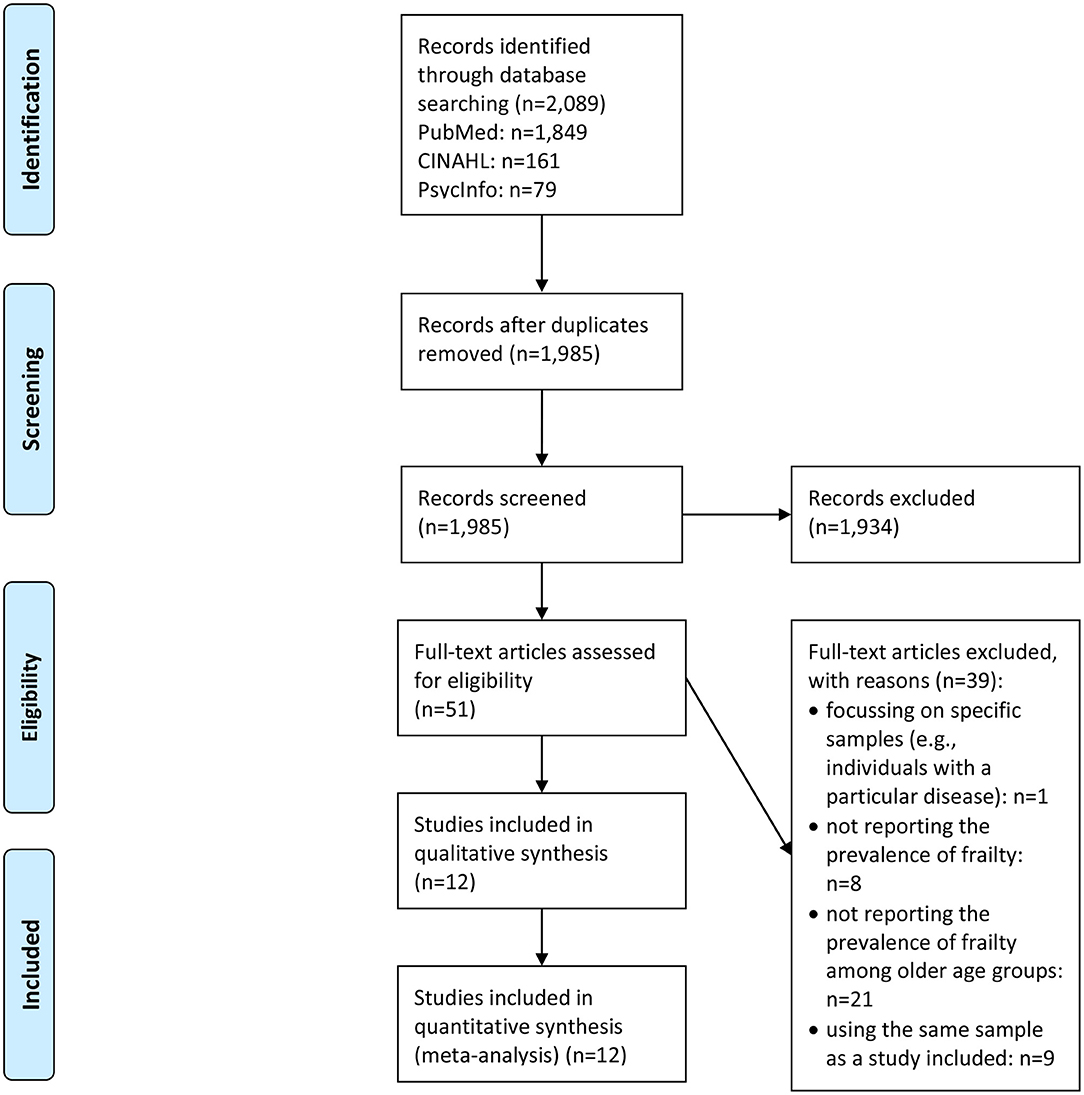
Figure 1. PRISMA flow diagram.
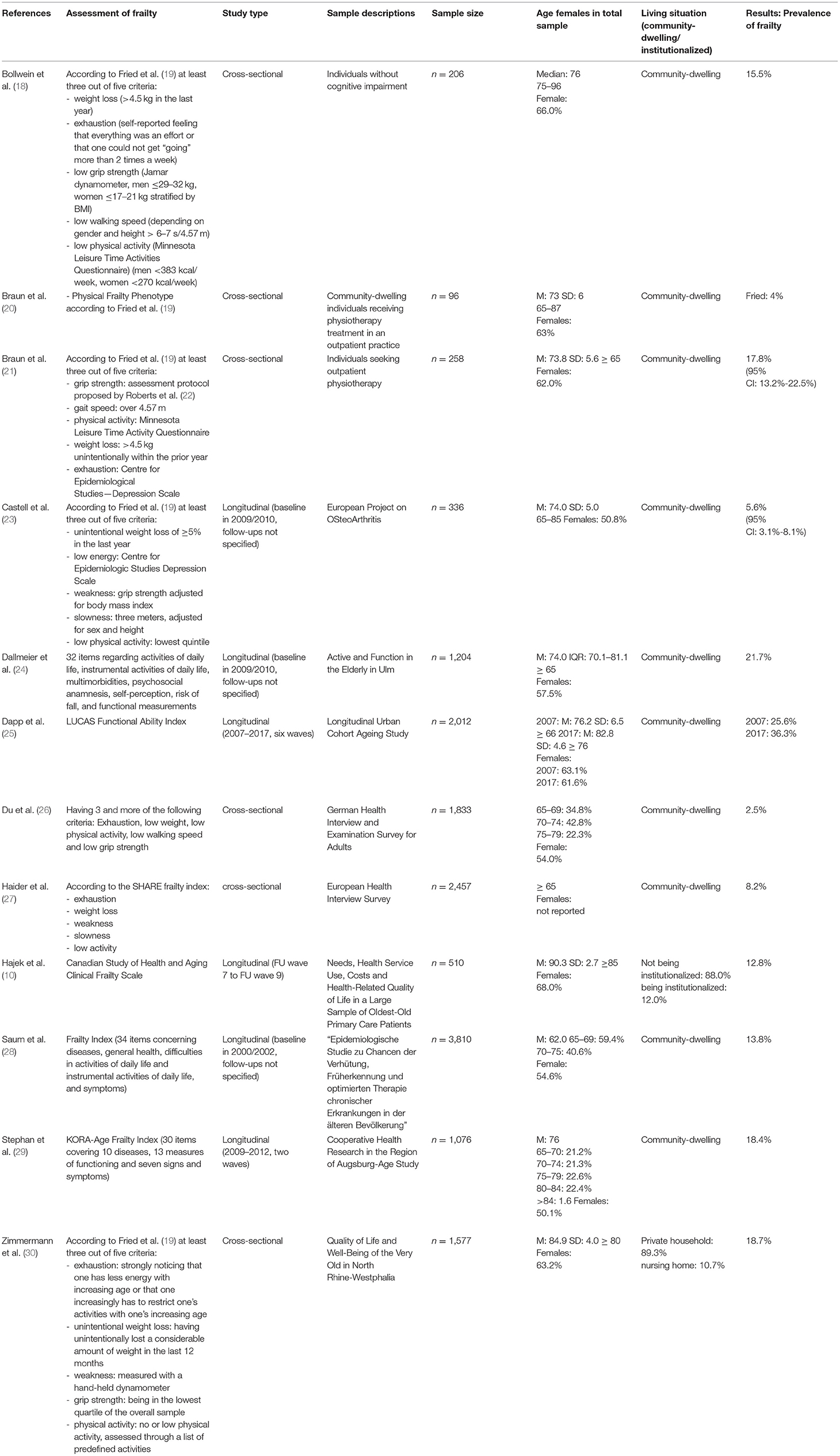
Table 2. Study overview and key findings.
A total of six studies were longitudinal (where we used the prevalence at baseline for meta-analysis) (10, 23–25, 28), whereas the other six studies were cross-sectional. Data were mainly used from the well-known German studies (e.g., “German Health Interview and Examination Survey for Adults” or “Quality of Life and Well-Being of the Very Old in North Rhine-Westphalia”). The sample size ranged from 96 (20) to 3,810 individuals (28). All the studies were published in the past 10 years (year 2013 onward).
Different tools were used to assess frailty [e.g., CSHA CFS (31) or according to the study of Fried et al. (19)]. The proportion of women ranged from 50 to 68%. Most samples had an average age of about 70 to 80 years. A number of ten studies solely used data from individuals residing in private households. More details are shown in Table 2.
Meta-Analysis and Meta-Regression
In total, the estimated overall prevalence of frailty was 13.7% (95% CI: 9.0 to 18.5%, Figure 2; ranging from 3.9 to 25.6%). There was a significant heterogeneity between the studies (I2 = 98.9%, p <0.001). The pooled prevalence of frailty was 15.9% (95% CI: 11.8 to 20.0%, ranging from 12.9 to 18.7%; I2 = 80.5%) when we only included samples with an average age of at least 80 years, whereas the pooled prevalence of frailty was 13.1% (95% CI: 7.5 to 18.6%, ranging from 3.9 to 25.6%; I2 = 99.1%) when we only included samples with an average age of below 80 years.
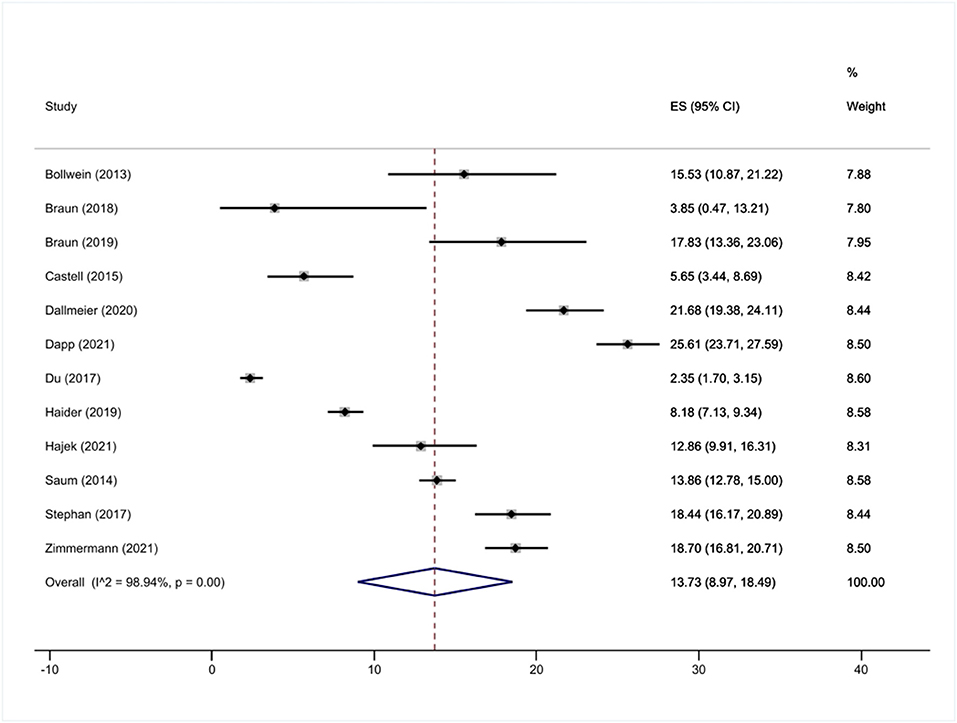
Figure 2. Meta-analysis (frailty).
Furthermore, the pooled prevalence of prefrailty was 40.2% (95% CI: 28.3 to 52.1%; ranging from 10.4 to 58.7%; I2 = 99.6%, p <0.001, Figure 3). The pooled prevalence of prefrailty was 44.0% (95% CI: 28.0 to 60.0%, ranging from 34.8 to 57.0%; I2 = 97.7%) when we only included samples with an average age of at least 80 years, whereas the pooled prevalence of frailty was 38.8% (95% CI: 25.2 to 52.4%, ranging from 10.4 to 58.7%; I2 = 99.7%) when we only included samples with an average age of below 80 years.
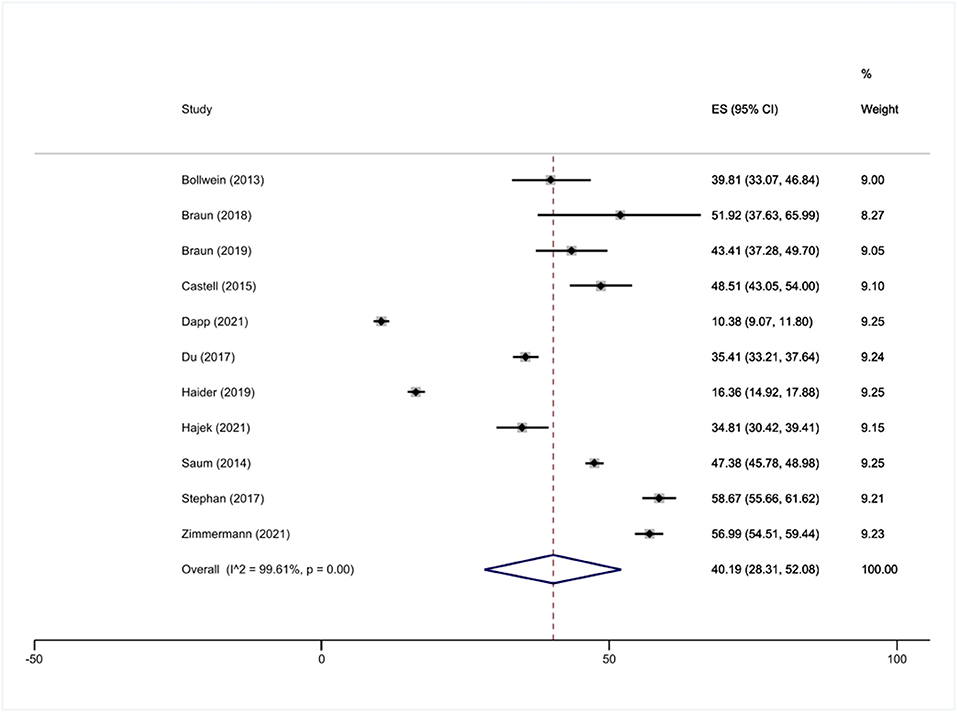
Figure 3. Meta-analysis (prefrailty).
Moreover, a meta-regression revealed that frailty prevalence was dependent of the average age in the sample and the assessment of frailty, whereas the risk of bias score did not achieve statistical significance (Table 3). The proportion of variance explained by these factors was 50.9%. The funnel plot (Figure 4) and the Egger's test (p = 0.06) partly suggested asymmetry of data—which implies a publication bias.
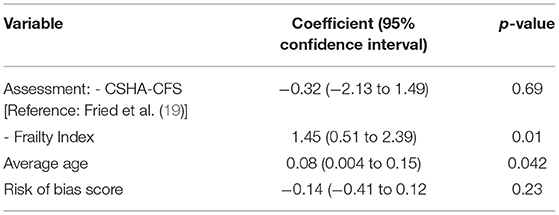
Table 3. Meta-regression analysis of factors affecting heterogeneity (prevalence of frailty).
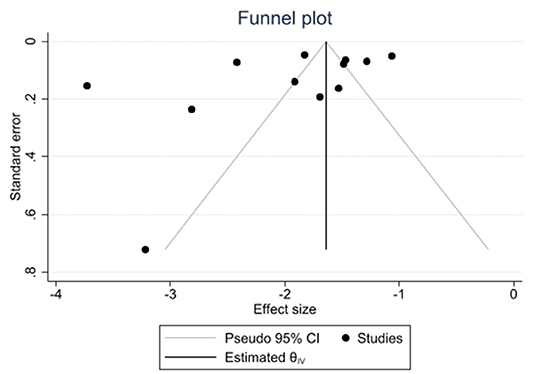
Figure 4. Funnel plot.
Quality Assessment or Risk of Bias Assessment
In Table 4, the risk of bias assessment or quality assessment is shown. In total, the scores varied from 4 to 9, with an average score of 7.3 (SD: 1.9). This reflects that the quality was rather high and the risk of bias was consequently quite small. Most often, limitations were the missing or inappropriate response rate (n = 8) and the missing or insufficient description or discussion of the model assumptions in these studies (n = 5). However, it should be acknowledged that some of these studies focused on reporting the prevalence and thus did not focus on the determinants of frailty in late life (and complex analytical models).
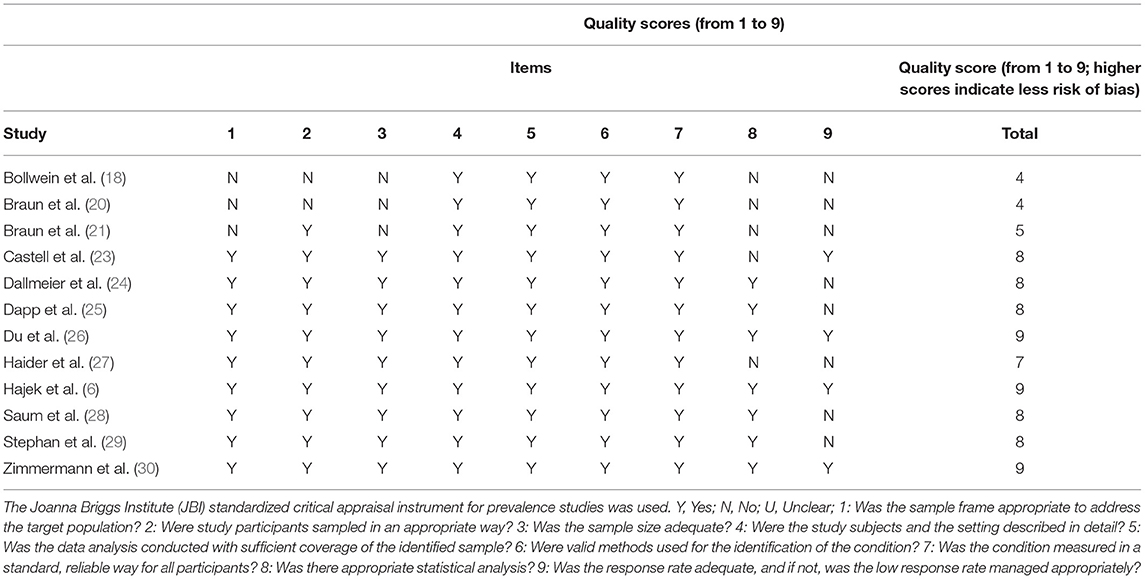
Table 4. Quality assessment/risk of bias assessment.
Discussion
Main Findings
Our aim was to determine the prevalence of frailty among older adults living in Germany. Another aim was to identify the potential sources of heterogeneity using a meta-regression.
The pooled prevalence of frailty was 13.7% (95% CI: 9.0 to 18.5%) and the pooled prevalence of prefrailty was 40.2% (95% CI: 28.3 to 52.1%). Considerable heterogeneity among the studies was determined. Some evidence of a publication bias exists. However, we think that more plausible explanations for the lack of publications could be that studies only had a small sample size or used data from convenience samples. Meta-regression showed that some of the heterogeneity can be explained by the tool to quantify the frailty and the average age. This appears very plausible. For example, Saum et al. showed that the prevalence of frailty was 4.5% among individuals aged 50 to 54 years, whereas the prevalence was 17.0% among individuals aged 70 to 75 years. Additionally, the prevalence of prefrailty was 32.5% among individuals aged 50 to 54 years, whereas the prevalence was 49.4% among individuals aged 70 to 75 years.
Comparability of the Included Studies
Substantial heterogeneity among the studies was identified. For example, the considerable higher prevalence rates of frailty were identified when the Frailty Index was used [compared to Fried et al. (19)]. It should be emphasized that no consensus exists on a single instrument for quantifying frailty (20).
It should be noted that a few studies exclusively used data from oldest old individuals (10, 30). This is worth noting because the prevalence of frailty commonly increases with age (8)—as noted above. Furthermore, while two studies also included individuals living in institutionalized settings (10, 30), the remaining studies explicitly examined community-dwelling individuals.
Study Quality
In total, a quite high quality of the studies included in our work was identified. For example, most of the studies used data from well-conducted samples. Frequent shortcomings were that the response rate was not clearly displayed or that the underlying assumptions of the analytical choice were not clearly described.
Gaps in Knowledge and Guidance for Future Studies
Our work identified some gaps in knowledge: First, far more research is required based on the samples which also include individuals residing in institutionalized settings. Moreover, more studies that examine the prevalence of frailty based on the representative samples and comparable assessments is required.
Beyond that, more longitudinal studies are required to determine the factors that lead to frailty in older adults in Germany. Additionally, since the existing longitudinal studies are mainly restricted in time span, more population-based longitudinal studies are required examining individuals over several decades (e.g., from middle age to highest age). These gaps may inspire future frailty research.
Strengths and Limitations
Our current work has some strengths and limitations. This is the first systematic review synthesizing the prevalence of frailty among older adults in Germany. Important procedures were done independently by two reviewers. An additional hand search was performed. Furthermore, a meta-analysis was conducted which can result in more accurate prevalence rates of frailty (when compared to individual empirical studies). Moreover, a meta-regression was done which can assist to clarify the influence of moderating factors. Due to the exclusion of non-peer-reviewed articles, some appropriate studies (e.g., gray literature) might be excluded. However, this choice was done to ensure a certain quality of the studies included in our work.
Conclusion
The pooled prevalence of frailty was 13.7% (95% CI: 9.0 to 18.5%) and the pooled prevalence of prefrailty was 40.2% (95% CI: 28.3 to 52.1%). Particularly, the high prevalence of prefrailty should be highlighted since it is important to prevent individuals in old age from developing to frail status. This knowledge is important for the German society as a whole and for relevant stakeholders. More longitudinal studies are required to reveal the factors contributing to frailty.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author Contributions
The study concept was developed by AH, BK, and H-HK. The manuscript was drafted by AH and critically revised by BK and H-HK. The search strategy was developed by AH and H-HK. The study selection, data extraction, and quality assessment were performed by AH and BK, with H-HK as a third party in case of disagreements (i.e., if clarification was still needed after discussion between AH and BK). Meta-analysis and meta-regressions were performed by AH, with critical assessment by BK and H-HK. All authors have approved the final version of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bergman H, Ferrucci L, Guralnik J, Hogan DB, Hummel S, Karunananthan S, et al. Frailty: an emerging research and clinical paradigm—issues and controversies. J Gerontol Ser A Biol Sci Med Sci. (2007) 62:731–7. doi: 10.1093/gerona/62.7.731
2. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. (2013) 381:752–62. doi: 10.1016/S0140-6736(12)62167-9
3. Hajek A, Brettschneider C, Lange C, Posselt T, Wiese B, Steinmann S, et al. Longitudinal predictors of institutionalization in old age. PLoS ONE. (2015) 10:e0144203. doi: 10.1371/journal.pone.0144203
4. Puts MT, Lips P, Deeg DJ. Sex differences in the risk of frailty for mortality independent of disability and chronic diseases. J Am Geriatr Soc. (2005) 53:40–47. doi: 10.1111/j.1532-5415.2005.53008.x
5. Wallis S, Wall J, Biram R, Romero-Ortuno R. Association of the clinical frailty scale with hospital outcomes. QJM. (2015) 108:943–9. doi: 10.1093/qjmed/hcv066
6. Hajek A, Bock J.-O., Saum K.-U., Matschinger H, et al. Frailty and healthcare costs—longitudinal results of a prospective cohort study. Age Ageing. (2017) 47:233–41. doi: 10.1093/ageing/afx157
7. Ahmed N, Mandel R, Fain MJ. Frailty: an emerging geriatric syndrome. Am J Med. (2007) 120:748–53. doi: 10.1016/j.amjmed.2006.10.018
8. Kojima G, Iliffe S, Taniguchi Y, Shimada H, Rakugi H, Walters K. Prevalence of frailty in Japan: a systematic review and meta-analysis. J Epidemiol. (2017) 27:347–53. doi: 10.1016/j.je.2016.09.008
9. Buttery AK, Busch MA, Gaertner B, Scheidt-Nave C, Fuchs J. Prevalence and correlates of frailty among older adults: findings from the German health interview and examination survey. BMC Geriatr. (2015) 15:22. doi: 10.1186/s12877-015-0022-3
10. Hajek A, Brettschneider C, Röhr S, Gühne U, Van der leeden C, Lühmann D, et al. Which factors contribute to frailty among the oldest old? Results of the multicentre prospective AgeCoDe and AgeQualiDe study. Gerontology. (2020) 66:460–6. doi: 10.1159/000508723
11. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
12. Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetc R, et al. Systematic reviews of etiology and risk. In: Aromataris E, Munn, editors. Joanna Briggs Institute Reviewer's Manual. Adelaide, SA: The Joanna Briggs Institute (2017). p. 219–26.
13. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
14. Nyaga VN, Arbyn M, Aerts M. Metaprop: a Stata command to perform meta-analysis of binomial data. Arch Public Health. (2014) 72:1–10. doi: 10.1186/2049-3258-72-39
15. Hartung J, Knapp G. On tests of the overall treatment effect in meta-analysis with normally distributed responses. Stat Med. (2001) 20:1771–82. doi: 10.1002/sim.791
16. Lipsey MW, Wilson DB. Practical Meta-Analysis. Thousand Oaks, CA: SAGE Publications, Inc. (2001).
17. Thompson SG, Higgins JP. How should meta-regression analyses be undertaken and interpreted? Stat Med. (2002) 21:1559–73. doi: 10.1002/sim.1187
18. Bollwein J, Volkert D, Diekmann R, Kaiser M, Uter W, Vidal K, et al. Nutritional status according to the mini nutritional assessment (MNA®) and frailty in community dwelling older persons: a close relationship. J Nutr Health Aging. (2013) 17:351–6. doi: 10.1007/s12603-013-0034-7
19. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol Ser A Biol Sci Med Sci. (2001) 56:M146–57. doi: 10.1093/gerona/56.3.M146
20. Braun T, Grüneberg C, Thiel C. German translation, cross-cultural adaptation and diagnostic test accuracy of three frailty screening tools. Zeitschr Gerontol Geriatr. (2018) 51:282–92. doi: 10.1007/s00391-017-1295-2
21. Braun T, Thiel C, Ziller C, Rasche J, Bahns C, Happe L, et al. Prevalence of frailty in older adults in outpatient physiotherapy in an urban region in the western part of Germany: a cross-sectional study. BMJ Open. (2019) 9:e027768. doi: 10.1136/bmjopen-2018-027768
22. Roberts HC, Denison HJ, Martin HJ, Patel HP, Syddall H, Coopper C, et al. A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age Ageing. (2011) 40:423–9. doi: 10.1093/ageing/afr051
23. Castell MV, Van Der Pas S, Otero A, Siviero P, Dennison E, Denkinger M, et al. Osteoarthritis and frailty in elderly individuals across six European countries: results from the European Project on OSteoArthritis (EPOSA). BMC Musculoskelet Disord. (2015) 16:1–8. doi: 10.1186/s12891-015-0807-8
24. Dallmeier D, Braisch U, Rapp K, Klenk J, Rothenbacher D, Denkinger M, et al. frailty index and sex-specific 6-year mortality in community-dwelling older people: the ActiFE Study. J Gerontol Ser A. (2020) 75:366–73. doi: 10.1093/gerona/glz051
25. Dapp U, Minder CE, Golgert S, Klugmann B, Neumann L, Von Renteln-Kruse W. The inter-relationship between depressed mood, functional decline and disability over a 10-year observational period within the Longitudinal Urban Cohort Ageing Study (LUCAS). J Epidemiol Community Health. (2021) 75:450–7. doi: 10.1136/jech-2020-214168
26. Du Y, Wolf I.-K., Knopf H. Association of psychotropic drug use with falls among older adults in Germany. Results of the German health interview and examination survey for adults 2008-2011 (DEGS1). PloS ONE. (2017) 12:e0182432. doi: 10.1371/journal.pone.0182432
27. Haider S, Grabovac I, Dorner TE. Fulfillment of physical activity guidelines in the general population and frailty status in the elderly population. Wien Klin Wochenschr. (2019) 131:288–293. doi: 10.1007/s00508-018-1408-y
28. Saum K.-U., Dieffenbach AK, Müller H, Holleczek B, Hauer K, et al. Frailty prevalence and 10-year survival in community-dwelling older adults: results from the ESTHER cohort study. Eur J Epidemiol. (2014) 29:171–9. doi: 10.1007/s10654-014-9891-6
29. Stephan AJ, Strobl R, Holle R, Meisinger C, Schulz H, Ladwig KH, et al. Male sex and poverty predict abrupt health decline: deficit accumulation patterns and trajectories in the KORA-Age cohort study. Prev Med. (2017) 102:31–8. doi: 10.1016/j.ypmed.2017.06.032
30. Zimmermann J, Hansen S, Wagner M. Home environment and frailty in very old adults. Zeitschr Gerontol Geriatr. (2021) 54:114–9. doi: 10.1007/s00391-021-01969-6
Keywords: frailty, Germany, prevalence, old age, systematic review, aged 80 and over
Citation: Hajek A, Kretzler B and König H-H (2022) Prevalence of Prefrailty and Frailty Among Older Adults in Germany: A Systematic Review, Meta-Analysis and Meta-Regression. Front. Med. 9:870714. doi: 10.3389/fmed.2022.870714
Received: 07 February 2022; Accepted: 08 March 2022;
Published: 22 April 2022.
Edited by:
Mario Ulises Pérez-Zepeda, Instituto Nacional de Geriatría, MexicoReviewed by:
Elena Vladimirovna Frolova, North Western State Medical University, RussiaSiti Setiati, University of Indonesia, Indonesia
Copyright © 2022 Hajek, Kretzler and König. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: André Hajek, YS5oYWplayYjeDAwMDQwO3VrZS5kZQ==