 Andraia R. Li
Andraia R. Li Laura Andrews
Laura Andrews Alexis Hilts
Alexis Hilts Manuel Valdebran
Manuel Valdebran
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Med., 09 June 2022
Sec. Dermatology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.868079
This article is part of the Research TopicAdvances in Evaluation and Management of Hair Loss DisordersView all 9 articles
Acupuncture is the practice of applying needles to target specific pressures points in the body. Since originating in China, acupuncture has been practiced for thousands of years to treat numerous conditions including chronic pain and mood disorders. Alopecia is a common dermatologic condition associated with psychological distress and decreased quality of life. Although it remains underexplored in western medicine, recent evidence suggests that acupuncture may be efficacious in the treatment of alopecia. In this review, we discuss the available evidence describing the efficacy of acupuncture or moxibustion alone (ACU) and in combination with other traditional and alternative interventions (ACU + TRAD) for hair loss. Additionally, the proposed physiologic mechanisms, targeted acupuncture points, and the benefits and barriers to treatment will be further described. An exploratory search using PubMed, EMBASE and Scopus databases was performed for studies that evaluated the effect of acupuncture and moxibustion on alopecia. In these studies, both ACU and ACU + TRAD were efficacious for numerous etiologies of hair loss including alopecia areata, androgenetic alopecia, and seborrheic alopecia. Given their ability to modulate the immune system, as well as neuronal networks associated with emotional cognition, the most frequently targeted acupoints were ST 36, GV 20, and LR 3. The proposed mechanistic effect is dependent upon disease etiology and is theorized to be twofold: reduction of inflammation and decrease in testosterone levels. The limited side effect profile of acupuncture makes it an advantageous treatment option, however, factors including cost, time, limited access, and aversion to needles may serve as barriers to treatment.
Acupuncture and moxibustion have been commonly practiced in traditional Chinese and Eastern medicine over the past three thousand years (1). Acupuncture is the practice of applying needles to target specific pressure points while moxibustion thermally stimulates these meridian points by burning dried mugwort herbs (2). Health benefits associated with acupuncture include alleviation of post-operative and chemotherapy-associated nausea and vomiting and post-operative dental pain (3). Acupuncture was not widely practiced in the United States until the 1970s and the acupuncture needle was not recognized as a medical device by the Food and Drug Administration (FDA) until 1996 (4, 5). Since then, acupuncture practice and research has rapidly advanced with recent evidence suggesting that acupuncture may also be efficacious in the treatment of alopecia (6).
Alopecia is a common dermatologic condition associated with psychological distress and decreased quality of life (7). Treatment of alopecia is dependent on etiology. Androgenetic alopecia is estimated to affect 50% of men by age 50, and 38% of women older than 70 years (8). Minoxidil and finasteride are currently the only FDA-approved treatments for androgenetic alopecia. Although both treatments have been shown to be effective in promoting hair growth in men with androgenetic alopecia, the efficacy of these treatments may be inflated considering publication bias (9). Potential side effects of low-dose minoxidil and finasteride include hypertrichosis and gynecomastia which may be prohibitive to their use (10, 11). Alopecia areata is a type of inflammatory and non-scarring hair loss that is estimated to affect 2% of the population worldwide with increasing prevalence over time (12). A variety of topical, systemic and injectable agents are used in the treatment of alopecia areata including corticosteroids and several immunosuppressive agents. Despite the array of treatment options, these methods produce variable outcomes, and no current treatment both induces and sustains remission in alopecia areata (12, 13).
The treatment of alopecia continues to prove challenging as results are inconsistent and efficacy is often limited by side effect profile. Given these challenges, the relative safety of acupuncture and the heterogeneity of previously published reports, we reviewed the evidence to assess the efficacy of acupuncture and moxibustion in the treatment of alopecia. We aimed to assess the most commonly targeted acupoints and the current understanding of the potential mechanism of action in order identify future directions for acupuncture in the treatment of hair loss.
An exploratory search using PubMed, EMBASE, and Scopus databases was performed to identify studies that evaluated the effect of acupuncture and moxibustion on hair loss. The search strategy was comprised of a combination of medical subject headings and keywords for acupuncture (e.g., acupressure, acupoint, electroacupuncture, laser acupuncture, moxibustion, and meridians) and hair loss (e.g., alopecia areata, seborrheic alopecia, androgenic alopecia, male pattern baldness, folliculitis decalvans, lichen planopilaris, telogen effluvium, traction alopecia, frontal fibrosing alopecia, and central centrifugal cicatricial alopecia). Case-reports, observational studies, and clinical trials assessing the efficacy of acupuncture alone (ACU) or in combination with other traditional therapies (ACU + TRAD) for the treatment hair loss were eligible for inclusion. Non-English studies and articles that did not report therapeutic outcomes in response to acupuncture were excluded.
The main findings of the 8 studies in acupuncture and hair loss are summarized in Table 1. These etiologies included alopecia areata, androgenetic alopecia, seborrheic dermatitis and perifolliculitis capitis abscedens et suffodiens (PCAS). Duration of needle retention ranged from 2 to 30 min while the number of total treatment sessions ranged from 3 to 50. Acupuncture was performed at least three times a week in 5 studies while the interval between treatments ranged from 1 to 4 weeks in the remaining 3 studies. The most commonly targeted acupoints were ST 36 (n = 4) (14–17), GV 20 (n = 3) (15, 17, 18), and LR 3 (n = 3) (15–17). Details of the study protocols and targets acupoints are summarized in Table 2.
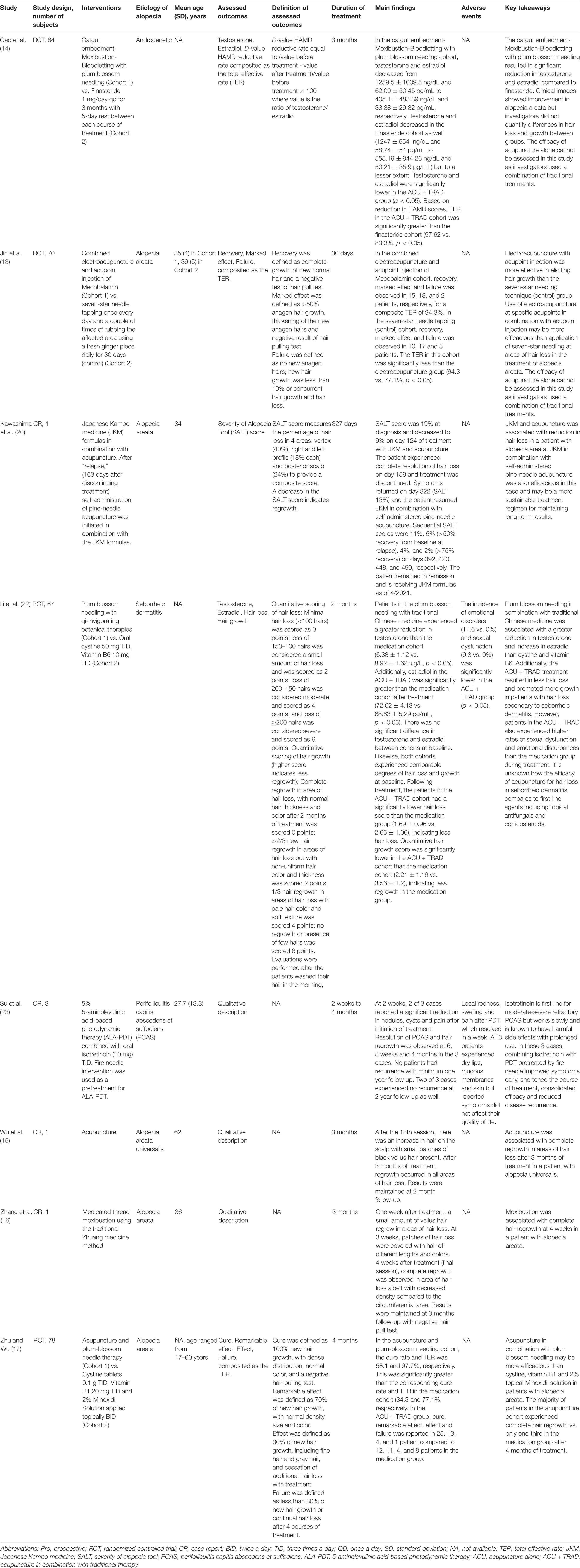
Table 1. Efficacy of acupuncture and moxibustion for alopecia.
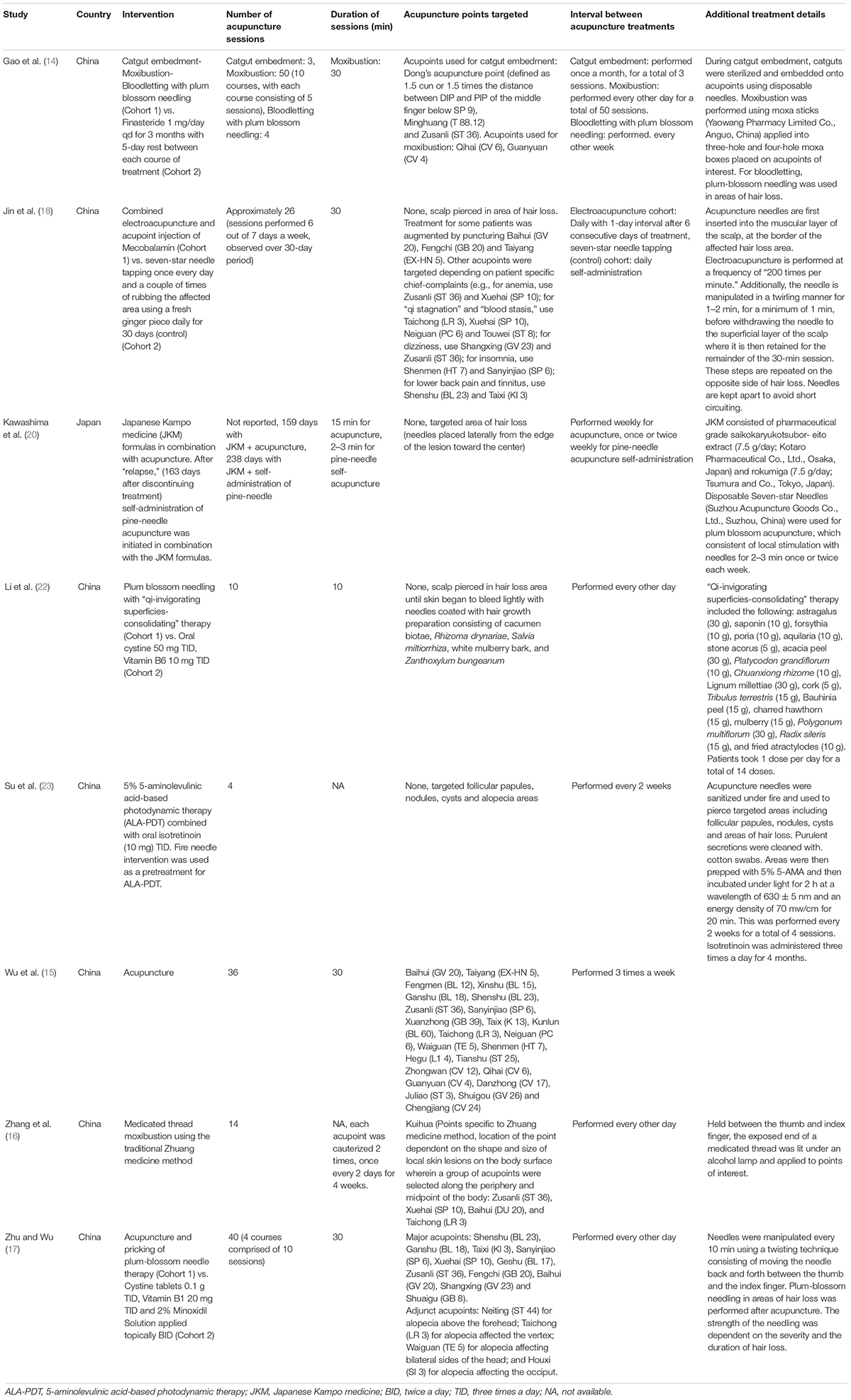
Table 2. Treatment specifications and details of eligible studies.
In a case report by Wu et al., acupuncture was associated with complete regrowth in areas of hair loss 3 months after treatment in a patient with alopecia areata universalis with results maintained at 2 months follow-up (15). In a randomized controlled trial (RCT) of 78 patients with alopecia areata, Zhu et al. found traditional acupuncture in combination with plum blossom needle acupuncture was associated with higher cure rates of alopecia areata than oral cystine with vitamin B6 and 2% topical minoxidil (58.1 vs. 77.1%, p < 0.05) after 4 months of treatment (17). Zhang et al. also reported of a case of alopecia areata where medicated-thread moxibustion using the traditional Zhuang medicine method was associated with hair regrowth appreciable after 1 week of treatment with complete regrowth at 4 weeks and results maintained at 3 months (16).
In a RCT by Gao et al., patients with androgenetic alopecia treated with moxibustion in combination with catgut embedment and bloodletting using plum blossom needling had significantly lower levels of testosterone (405.1 ± 483.39 vs. 555.19 ± 944.26 ng/dL, p < 0.05) and estradiol (33.38 ± 29.32 vs. 50.21 ± 35.9 pg/mL, p < 0.05) than patients in the finasteride cohort following treatment (14). Clinical images also showed improvement in alopecia areata in response to ACU + TRAD improvement, however, investigators failed to quantify differences in hair loss and growth between groups (14).
In a RCT of 70 patients with alopecia areata, Jin et al. found electroacupuncture in combination with acupoint injections of mecobalamin, a co-factor of vitamin B12 commonly used to treat peripheral neuropathy, was associated with a significantly greater total effective rate (TER) (94.3 vs. 77.1%, p < 0.05) than seven-star needle tapping in areas of hair loss after 30 days of treatment (18, 19).
Kawashima et al. report of a case of alopecia areata successfully treated with acupuncture in combination with Japanese Kampo medicine (JKM), a form of traditional Japanese herbal medicine (20, 21). Treatment resulted in reduction of Severity of Alopecia Tool (SALT) score from 19% at baseline to complete resolution of hair loss was observed on day 159 and treatment was discontinued. Symptoms returned on day 322 (SALT 13%) and the patient was directed to resume JKM in combination with self-administered pine-needle acupuncture in place of traditional acupuncture (20). On this regimen, the patient achieved >50% and >75% recovery from baseline at relapse on day 420 and day 490, respectively (20).
In a RCT of 87 patients with hair loss secondary to seborrheic dermatitis, Li et al. found plum blossom needling in combination with traditional Chinese medicine was associated with significantly less hair loss (1.69 ± 0.96 vs. 2.65 ± 1.06, p < 0.05) and more hair growth (2.21 ± 1.16 vs. 3.56 ± 1.2, p < 0.05) than oral cystine/vitamin B6 (22). Those in the ACU + TRAD group exhibited significantly lower levels of testosterone (6.38 ± 1.12 vs. 8.92 ± 1.62 μg/L, p < 0.05) and higher levels of estradiol (72.02 ± 4.13 vs. 68.63 ± 5.29 pg/mL, p < 0.05) compared to the medication group (22). Patients in the medication group reported higher rates of sexual dysfunction, which the authors defined as decreased sexual desire and erectile dysfunction (9.3 vs. 0%, p < 0.05), and emotional disturbances (11.6 vs. 0%, p < 0.05), than patients in the ACU + TRAD group during treatment (22).
Su et al. report of three cases of PCAS responding to acupuncture in combination with 5-aminolevulinic acid-based photodynamic therapy (ALA-PDT) and isotretinoin (23). Two of 3 cases reported a significant reduction nodules, cysts and pain at 2 weeks (23). For all 3 cases, symptoms resolved after 2–4 months of treatment with no patients experiencing disease recurrence at one year follow up (23). All 3 patients experienced dry lips and mucous membranes, which did not impact their quality of life. Additionally, patients experienced local redness, swelling and pain after PDT which all resolved within 1 week post-treatment.
There is evidence to suggest acupuncture or moxibustion alone or in combination with other treatment interventions may be efficacious for treating numerous etiologies of hair loss. Notably, all studies in this review reported benefits in hair loss and growth in response to treatment. However, the conclusion that can be drawn regarding acupuncture in hair loss are severely limited as the majority of studies did not evaluate acupuncture alone. Only a handful of controlled trials have been performed with the majority of evidence being in case-reports. The topic of acupuncture remains understudied in Western medicine with the majority of studies originating in Eastern countries. Nonetheless, published reports have overwhelmingly showed benefits associated with acupuncture as an adjuvant treatment to both traditional therapies and PDT, warranting further exploration of this treatment modality.
The limited side effect profile of acupuncture makes it an advantageous treatment option for alopecia. As previously mentioned, adverse effects associated with finasteride, a mainstay treatment for both seborrheic and androgenetic alopecia, include erectile dysfunction and decreased arousal secondary to decreased levels of sex hormones (24). Although its existence remains controversial, post-finasteride syndrome, a constellation of sexual, and psychological side effects that persist following cessation of the medication, has also been increasingly reported in the literature (25). As a result, this side effect profile may be prohibitive to its use, particularly in male patients. In contrast, acupuncture is widely viewed as a safe practice when performed by trained practitioners (26). The estimated prevalence of minor adverse events is 1.3 per 1000 treatments, with the most common side effects being nausea, syncope and pain and bruising at the site of application (27). However, a systematic review by Chan et al. showed serious adverse events, although incredibly rare, can include internal or soft tissue injury, infection, and spinal cord injury (28). There is also the potential for underreporting of adverse events in the literature as adverse events are not commonly evaluated in acupuncture studies (28). We found only 2 of the 8 studies assessed the rate of adverse events in their outcomes. Despite the need for better practice in reporting of adverse events, the relative safety of acupuncture has been overwhelmingly supported in the literature and makes it an increasingly appealing treatment option.
The potential mechanism of action behind the effect of acupuncture in alopecia may be disease dependent and stem from two different processes that lead to a reduction in inflammation and a decrease in testosterone. Alopecia areata is characterized by an immune-mediated attack on anagen hair follicles and inflammation-induced dystrophy of the hair follicle (29, 30). Like many other diseases in its class, the pathogenesis is theorized to stem from an interaction of genetic, environmental, and immune factors (29, 30). In a study using murine models for alopecia areata, stimulation of the ST 36 with electroacupuncture was associated with a significant reduction of mast cell degranulation around hair follicles and a phenotypical improvement in hair loss when compared to the untreated group (31). Preclinical studies have also shown acupuncture is able to modulate the balance between Th1 and Th2 CD4 + T-cells to obtund the Th1 response and subsequently decrease the release of pro-inflammatory cytokines including tumor necrosis factor (TNF)-alpha (32). Along these lines, a previously published pilot study assessing the role of acupuncture in rheumatoid arthritis, a Th1-predominant autoinflammatory disease, showed acupuncture significantly decreased disease activity with minimal adverse events (33). This relationship between acupuncture and immunomodulation could underlie the benefits associated with its use in alopecia areata.
Acupuncture may also be efficacious for the treatment of androgenetic alopecia through the reduction of testosterone. Androgens modulate the hair growth cycle by binding to receptors at the dermal papillae where testosterone is converted to the more potent dihydrotestosterone (DHT) via 5α-reductase (34). DHT is thought to be necessary to the pathogenesis of androgenetic alopecia as areas of hair loss express higher levels of androgen receptors and 5α-reductase. Moreover, individuals that lack 5α-reductase do not experience the hair loss phenotypical of androgenetic alopecia (34). This relationship also underlies the efficacy of finasteride in treating androgenetic hair loss (34). In a study of patients with seborrheic alopecia by Li et al. and a subsequent study of patients with androgenetic alopecia by Gao et al., both authors noted a significant reduction in testosterone in the ACU + TRAD group (14, 22). Similarly, results of a RCT assessing acupuncture vs. traditional Chinese medicine for polycystic ovary syndrome showed both interventions were associated with reduced total testosterone levels (35). This observed association between acupuncture and testosterone could provide a mechanistic explanation for the benefits of acupuncture in androgenetic alopecia if further validated.
Our review found the most commonly targeted acupoints in hair loss were ST 36 (14–17), GV 20 (15, 17, 18), and LR 3 (15–17). Throughout the practice of acupuncture, different acupoints have been implicated in the treatment of a variety of diseases and ailments. Interestingly, ST 36 and LR 3 are amongst the most commonly used acupoints across all diseases (36). GV 20 is associated with relief of headaches, stroke, insomnia, anxiety, and dizziness, through increasing nitric oxide (NO) production and increasing local circulation (37). Given GV 20’s location on the scalp, this enhancement of NO and increased local circulation may explain its positive impact in the treatment of hair loss. Subsequently, ST 36 is a commonly used treat various autoinflammatory conditions including rheumatoid arthritis (38). In addition to significantly reducing mast cell degranulation and alopecia in murine models, ST 36 has also been found to decrease levels of inflammatory cytokines including TNF-alpha, interleukin (IL)-1, and IL-6 (31, 39, 40). In vitro studies have demonstrated the role of TNF-alpha, IL-1 alpha, and IL-1 beta in the inhibition of hair growth through their distortion and disruption of the dermal papilla, matrix, and melanocytes. Consequently, these inflammatory cytokines are thought to mediate the pathological changes seen in alopecia areata (41). Lastly, LR 3 is thought to modulate emotion cognition, associative function, and visual function based on functional imaging studies (42). Emotional stress is often reported as a trigger for episodes of alopecia areata and thus, targeting acupoints associated with modulation of these neuronal networks associated with emotional cognition may help decrease hair loss in alopecia areata (43). Nonetheless, more research is needed to determine the specific acupoints most beneficial in treating alopecia and the identifying the etiologies that will have the best response to acupuncture.
Barriers to the use of acupuncture as a treatment remedy for hair loss are not insignificant and can include treatment costs, time requirements for treatment, limited access to resources and trained providers and patient aversion to needles (44). Cost of acupuncture ranges from $15 to $400 for an initial session and $15 to $300 for each follow up session, with the estimated annual cost spent by patients seeking acupuncture totaling $3.5 billion (45). These costs can be significant when considering the number of sessions ranged from 3 to 50 sessions for the treatment of hair loss. The time required for acupuncture treatment and follow up appointments is also considerably more intensive than the time needed for treatment with oral or topical medications (44). Moreover, the lack of trained physicians, staff, and space for equipment can contribute to difficulty scheduling appointments and accessing acupuncture treatment as well (44). Home treatment may represent a viable alternative to in-office treatment and provide a solution to the cost and time burden but self-administration of acupuncture poses significant training and safety barriers for patients. It should also be noted acupuncture not be an amendable treatment option for all patients, especially those with a phobia of needles (44). However, with the emergence of laser acupuncture, the practice of photonic stimulation of acupoints in absence of needles, serves as a non-invasive alternative to traditional acupuncture (46). Adverse events associated with laser acupuncture were mild and primarily included tingling, transient fatigue, and pain flare-ups which all resolved within 24 h of onset (46). Given the relative safety of laser acupuncture, it may be a safer form of acupuncture for patients in general if shown to be efficacious for hair loss and serve as an alternative for patients with aversion to needles (46).
Only eight clinical studies were identified, therefore the power of this review is limited by the small sample set. Language also served as a major limitation as studies in Chinese and South Korean, were not readily accessed and were not represented in our findings. This barrier is incredibly challenging considering the majority of research in acupuncture originate from Eastern countries. There is one published review focusing on alternative therapies for the treatment alopecia based on studies solely published in South Korean medical journals (47). Similar to our findings, the authors reported the most commonly used acupoints for alopecia included ST 36 and GV 20, which were used in 68 and 23% of eligible studies, respectively (48). Other common acupoints included EX-HN 1 and GB 5 (48). There was also significant heterogeneity in treatment interventions and measurement of outcomes and the absence of standardization of acupuncture techniques and clinical endpoints across the studies included in this review. The majority of studies examined other complementary and alternative medicine practices in combination with acupuncture, making it difficult to determine which treatment elicited improvement in hair loss. However, it should be noted that clinical improvements in hair loss was observed across all articles. Lastly, there were no studies comparing acupuncture with procedural interventions commonly used to treat alopecia including intralesional steroid injections and platelet rich plasma injections and therefore it is unknown how acupuncture compares to these procedural modalities.
Acupuncture may be an efficacious treatment for numerous etiologies of alopecia. Existing evidence remains limited and heterogenous in protocol and endpoints but overwhelmingly report of benefits associated with acupuncture. This alternative treatment modality continues to be understudied in Western medicine with no existing studies originating in the United States. Yet, given the beneficial side effect profile associated with acupuncture and notable improvements reported in the literature, it is a treatment modality that warrants further exploration. Future directions include performing randomized controlled studies assessing the efficacy of acupuncture alone in comparison to current first-line treatments for alopecia. Additionally, exploring methodologies for safer acupuncture practices, particularly with the application of laser acupuncture, an alternative and non-invasive practice compared to traditional acupuncture, could translate to more accessible treatment and may alleviate the large time and cost barriers needed to undergo acupuncture treatment. Although this acupuncture is viewed as generally safe practice, careful evaluation of adverse events is needed for a better understanding of the side effect profile associated with its practice.
AL designed the methodology, performed the data collection, prepared the initial draft, and critically reviewed the manuscript. LA performed the data collection and prepared the initial draft of the manuscript. AH prepared the initial draft of the manuscript. MV formulated the overarching research goals and aims and critically reviewed the manuscript. All authors reviewed the results and approved the final version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Jishun J, Mittelman M. Acupuncture: past, present, and future. Glob Adv Health Med. (2014) 3:6–8. doi: 10.7453/gahmj.2014.042
2. He XR, Wang Q, Li PP. Acupuncture and Moxibustion for Cancer-related Fatigue: a systematic review and meta-analysis. Asian Pac J Cancer Prev. (2013) 14:3067–74. doi: 10.7314/APJCP.2013.14.5.3067
4. Astin JA, Marie A, Pelletier KR, Hansen E, Haskell WL. A review of the incorporation of complementary and alternative medicine by mainstream physicians. Arch Intern Med. (1998) 158:2303–10. doi: 10.1001/archinte.158.21.2303
5. Meng X, Xu S, Lao L. Clinical acupuncture research in the West. Front Med. (2011) 5:134–40. doi: 10.1007/s11684-011-0135-9
6. Tan EK, Millington GWM, Levell NJ. Acupuncture in dermatology: an historical perspective. Int J Dermatol. (2009) 48:648–52. doi: 10.1111/j.1365-4632.2009.03899.x
7. Abedini R, Hallaji Z, Lajevardi V, Nasimi M, Karimi Khaledi M, Tohidinik HR. Quality of life in mild and severe alopecia areata patients. Int J Womens Dermatol. (2018) 4:91–4. doi: 10.1016/j.ijwd.2017.07.001
8. Phillips TG, Slomiany WP, Allison R. Hair Loss: common causes and treatment. Am Fam Physician. (2017) 96:371–8.
9. Adil A, Godwin M. The effectiveness of treatments for androgenetic alopecia: a systematic review and meta-analysis. J Am Acad Dermatol. (2017) 77:136–41.e5. doi: 10.1016/j.jaad.2017.02.054
10. Lee SW, Juhasz M, Mobasher P, Ekelem C, Mesinkovska NAA. Systematic review of topical finasteride in the treatment of androgenetic alopecia in men and women. J Drugs Dermatol. (2018) 17:457–63.
11. Vañó-Galván S, Pirmez R, Hermosa-Gelbard A, Moreno-Arrones ÓM, Saceda-Corralo D, Rodrigues-Barata R, et al. Safety of low-dose oral minoxidil for hair loss: a multicenter study of 1404 patients. J Am Acad Dermatol. (2021) 84:1644–51. doi: 10.1016/j.jaad.2021.02.054
12. Lee HH, Gwillim E, Patel KR, Hua T, Rastogi S, Ibler E, et al. Epidemiology of alopecia areata, ophiasis, totalis, and universalis: a systematic review and meta-analysis. J Am Acad Dermatol. (2020) 82:675–82. doi: 10.1016/j.jaad.2019.08.032
13. Strazzulla LC, Wang EHC, Avila L, Lo Sicco K, Brinster N, Christiano AM, et al. Alopecia areata: an appraisal of new treatment approaches and overview of current therapies. J Am Acad Dermatol. (2018) 78:15–24. doi: 10.1016/j.jaad.2017.04.1142
14. Gao JY, Liu HJ, Shi J, Yang Y, Ge CQ, Qie ZW, et al. Clinical efficacy of catgut embedment combined with moxibustion and bloodletting in the treatment of androgenic alopecia. World J Acupunct Moxibustion. (2015) 25:1–6. doi: 10.1016/S1003-5257(15)30001-5
15. Wu D, Zhang MR, Liu YC, Zhang SQ, Li Y, Zhou L, et al. Case of alopecia universalis. World J Acupunct Moxibustion. (2020) 30:320–2. doi: 10.1016/j.wjam.2020.11.003
16. Zhang YM, Liu CH, Wang YC, Teng HL, Meng XL, Han XJ. Medicated thread moxibustion for alopecia areata: a case report. Medicine. (2019) 98:e17793. doi: 10.1097/MD.0000000000017793
17. Zhu Q, Wu F. Clinical observation on acupuncture treatment of alopecia areata. J Acupunct Tuina Sci. (2011) 9:162–4. doi: 10.1007/s11726-011-0500-x
18. Jin Z, Yang F, Wang Y. Therapeutic effect observation on electroacupuncture plus acupoint injection for alopecia areata. J Acupunct Tuina Sci. (2011) 9:165–7. doi: 10.1007/s11726-011-0501-9
19. Sawangjit R, Thongphui S, Chaichompu W, Phumart P. Efficacy and Safety of Mecobalamin on Peripheral Neuropathy: a systematic review and meta-analysis of randomized controlled trials. J Altern Complement Med N Y N. (2020) 26:1117–29. doi: 10.1089/acm.2020.0068
20. Kawashima N, Hu X, Ishikawa N, Matsuhisa T, Sato J. A combination of herbal formulas, acupuncture, and novel pine-needle stimulation for recurrent alopecia areata: a case report. Medicine. (2021) 100:e26084. doi: 10.1097/MD.0000000000026084
21. Watanabe K, Matsuura K, Gao P, Hottenbacher L, Tokunaga H, Nishimura K, et al. Traditional Japanese Kampo medicine: clinical research between modernity and traditional medicine-the state of research and methodological suggestions for the future. Evid Based Complement Altern Med. (2011) 2011:513842. doi: 10.1093/ecam/neq067
22. Li Q, Xie Y, Zha X. The clinical effect of plum blossom needle acupuncture with qi-invigorating superficies-consolidating therapy on seborrheic alopecia. Ann Palliat Med. (2020) 9:1030–6. doi: 10.21037/apm-20-909
23. Su Y, Xu Q, Zhang C, Zhang C. Photodynamic therapy pre-treated by fire needle combined with isotretinoin in the treatment of refractory perifolliculitis capitis abscedens et suffodiens: case report. Photodiagnosis Photodyn Ther. (2021) 33:102103. doi: 10.1016/j.pdpdt.2020.102103
24. Irwig MS, Kolukula S. Persistent sexual side effects of finasteride for male pattern hair loss. J Sex Med. (2011) 8:1747–53. doi: 10.1111/j.1743-6109.2011.02255.x
26. White A. The safety of acupuncture – evidence from the UK. Acupunct Med. (2006) 24:53–7. doi: 10.1136/aim.24.Suppl.53
27. MacPherson H, Thomas K, Walters S, Fitter MA. Prospective survey of adverse events and treatment reactions following 34,000 consultations with professional acupuncturists. Acupunct Med. (2001) 19:93–102. doi: 10.1136/aim.19.2.93
28. Chan MWC, Wu XY, Wu JCY, Wong SYS, Chung VCH. Safety of acupuncture: overview of systematic reviews. Sci Rep. (2017) 7:3369. doi: 10.1038/s41598-017-03272-0
29. Gilhar A, Etzioni A, Paus R. Alopecia areata. N Engl J Med. (2012) 366:1515–25. doi: 10.1056/NEJMra1103442
30. Zafrir Y, Baum S, Greenberger S, Lyakhovitsky A, Barzilai A. [Alopecia areata]. Harefuah. (2016) 155:622–5.
31. Maeda T, Taniguchi M, Matsuzaki S, Shingaki K, Kanazawa S, Miyata S. Anti-inflammatory effect of electroacupuncture in the C3H/HeJ mouse model of alopecia areata. Acupunct Med J Br Med Acupunct Soc. (2013) 31:117–9. doi: 10.1136/acupmed-2012-010240
32. Kim SK, Bae H. Acupuncture and immune modulation. Auton Neurosci Basic Clin. (2010) 157:38–41. doi: 10.1016/j.autneu.2010.03.010
33. Lee H, Lee JY, Kim YJ, Kim S, Yin C, Khil JH, et al. Acupuncture for symptom management of rheumatoid arthritis: a pilot study. Clin Rheumatol. (2008) 27:641–5. doi: 10.1007/s10067-007-0819-3
34. Stough D, Stenn K, Haber R, Parsley WM, Vogel JE, Whiting DA, et al. Psychological effect, pathophysiology, and management of androgenetic alopecia in men. Mayo Clin Proc. (2005) 80:1316–22. doi: 10.4065/80.10.1316
35. Cao Y, Chen H, Zhao D, Zhang L, Yu X, Zhou X, et al. The efficacy of Tung’s acupuncture for sex hormones in polycystic ovary syndrome: a randomized controlled trial. Complement Ther Med. (2019) 44:182–8. doi: 10.1016/j.ctim.2019.04.016
36. Lee YS, Ryu Y, Yoon DE, Kim CH, Hong G, Hwang YC, et al. Commonality and specificity of acupuncture point selections. Evid Based Complement Alternat Med. (2020) 2020:2948292. doi: 10.1155/2020/2948292
37. Shen EY, Chen FJ, Chen YY, Lin MF. Locating the acupoint baihui (GV20) beneath the cerebral cortex with MRI reconstructed 3D neuroimages. Evid Based Complement Altern Med. (2011) 2011:362494. doi: 10.1093/ecam/neq047
38. Yang F, Gong Y, Yu N, Yao L, Zhao X, Hong S, et al. ST36 acupuncture alleviates the inflammation of adjuvant-induced arthritic rats by targeting monocyte/macrophage modulation. Evid Based Complement Alternat Med. (2021) 2021:9430501. doi: 10.1155/2021/9430501
39. Sun ZG, Pi YL, Zhang J, Wang M, Zou J, Wu W. Effect of acupuncture at ST36 on motor cortical excitation and inhibition. Brain Behav. (2019) 9:e01370. doi: 10.1002/brb3.1370
40. Villegas-Bastida A, Torres-Rosas R, Arriaga-Pizano LA, Flores-Estrada J, Gustavo-Acosta A, Moreno-Eutimio MA. Electrical stimulation at the ST36 acupoint protects against sepsis lethality and reduces serum TNF levels through vagus nerve- and catecholamine-dependent mechanisms. Evid Based Complement Altern Med. (2014) 2014:451674. doi: 10.1155/2014/451674
41. Ettefagh L, Nedorost S, Mirmirani P. Alopecia areata in a patient using infliximab: new insights into the role of tumor necrosis factor on human hair follicles. Arch Dermatol. (2004) 140:1012. doi: 10.1001/archderm.140.8.1012-a
42. Zheng Y, Wang Y, Lan Y, Qu X, Lin K, Zhang J, et al. Imaging of brain function based on the analysis of functional connectivity - imaging analysis of brain function by FMRI after acupuncture at LR3 in healthy individuals. Afr J Tradit Complement Altern Med. (2016) 13:90–100. doi: 10.21010/ajtcam.v13i6.14
43. Pratt CH, King LE, Messenger AG, Christiano AM, Sundberg JP. Alopecia areata. Nat Rev Dis Primer. (2017) 3:17011. doi: 10.1038/nrdp.2017.11
44. Ledford CJW, Fisher CL, Moss DA, Crawford PF. Critical factors to practicing medical acupuncture in family medicine: patient and physician perspectives. J Am Board Fam Med. (2018) 31:236–42. doi: 10.3122/jabfm.2018.02.170381
45. Fan AY, Wang DD, Ouyang H, Tian H, Wei H, He D, et al. Acupuncture price in forty-one metropolitan regions in the United States: an out-of-pocket cost analysis based on OkCopay.com. J Integr Med. (2019) 17:315–20. doi: 10.1016/j.joim.2019.06.003
46. Yang J, Mallory MJ, Wu Q, Bublitz SE, Do A, Xiong D, et al. The Safety of Laser Acupuncture: a systematic review. Med Acupunct. (2020) 32:209–17. doi: 10.1089/acu.2020.1419
47. Kaptchuk TJ. Acupuncture: theory, efficacy, and practice. Ann Intern Med. (2002) 136:374. doi: 10.7326/0003-4819-136-5-200203050-00010
Keywords: acupuncture-therapy, alopecia-etiology, alternative medicine (CAM), hair loss (alopecia), moxibustion acupuncture, acupoint, systematic review
Citation: Li AR, Andrews L, Hilts A and Valdebran M (2022) Efficacy of Acupuncture and Moxibustion in Alopecia: A Narrative Review. Front. Med. 9:868079. doi: 10.3389/fmed.2022.868079
Received: 02 February 2022; Accepted: 09 May 2022;
Published: 09 June 2022.
Edited by:
Linda Doan, UCI Health, United StatesReviewed by:
Francisco Jose Gomez Garcia, Hospital Universitario Reina Sofía, SpainCopyright © 2022 Li, Andrews, Hilts and Valdebran. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andraia R. Li, bGlAbXVzYy5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.