 Fan Zhang
Fan Zhang Hui Wang
Hui Wang Liuyan Huang
Liuyan Huang Yan Bai3
Yan Bai3
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Med. , 11 April 2022
Sec. Nephrology
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.861013
This article is part of the Research Topic Frailty and Sarcopenia in Various Cachectic Kidney Diseases, Volume II View all 9 articles
Objective: To examine the dose-response associations between total physical activity, different intensity of physical activity, and all-cause mortality in patients with chronic kidney disease (CKD).
Methods and Analysis: PubMed, Embase, Web of Science, and the Cochrane library will be searched from inception to June 2022. Only cohort studies assessing physical activity associations with all-cause mortality among CKD patients will be considered for inclusion. The quality of included cohort studies will be evaluated according to the Newcastle-Ottawa Scale (NOS). The robust error meta-regression (REMR) model will be used to establish dose-response relationships between physical activity and mortality. Additional statistical analysis including Egger's test, subgroup analysis, sensitivity analysis. The strengths of evidence will be evaluated with the Grading of Recommendation, Assessment, Development, and Evaluation approach.
Ethics and Dissemination: Ethics approval is not required as no private information from individuals is collected.
PROSPERO Registration Number: CRD 42021283630.
Chronic kidney disease (CKD) is a progressive lifelong disease that affects ~750 million people worldwide, and more than two million people have end-stage renal disease and require renal replacement therapy to stay alive (1, 2). In recent years, the life expectancy of CKD patients has increased with advances in dialysis or kidney transplantation techniques. Nevertheless, due to cardiovascular disease in more than 50% of CKD patients, the risk of premature death in CKD patients is 20 times higher than in the general population (3), placing a burden on individuals, families, and healthcare systems (4).
Physical activity is any physical movement produced by skeletal muscle that requires energy expenditure (5). Physical activity is the cornerstone of renal rehabilitation management in patients with CKD (6). There is evidence that even small increases in physical activity levels can improve exercise tolerance and cardiovascular responsiveness and improve quality of life in patients with CKD (7).
Intriguingly, a negative association between physical activity and all-cause mortality has been validated in the elderly (8) and other chronic disease populations such as cancer (9). To date, two meta-analyses have aimed to determine the association between physical activity and mortality risk in patients with CKD. These included a low number of studies (up to 11) or focused only on a certain stage of the CKD population (e.g., predialysis CKD or end-stage renal disease) (10, 11). Nevertheless, a dose-response relationship between physical activity levels and patients with full-spectrum CKD has not been established.
For this reason, we proposed to perform a dose-response meta-analysis of a cohort study of physical activity, all-cause mortality risk in CKD patients (including predialysis, peritoneal dialysis, hemodialysis, and kidney transplant recipients). We aim to elucidate the strength of this association, the shape of the dose-response relationship, potential sources of heterogeneity between studies, and the difference across activity domains.
This systematic review and meta-analysis will be performed according to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guideline (12). The protocol for the systematic review has been registered with the International Prospective Register of Systematic Reviews (CRD 42021283630).
Studies meeting the following inclusion criteria will be included: (1) patients aged over 18 years with chronic kidney disease and predialysis, peritoneal dialysis, hemodialysis, kidney transplant recipients will be eligible. (2) The relationship between physical activity and all-cause mortality outcomes in patients with CKD was reported; (3) adjusted effect sizes [hazard ratios (HRs), relative risks (RRs), odd ratios (ORs)] and corresponding 95% confidence intervals (CI) are provided; (4) reported physical activity doses in a metabolic equivalent task (MET)-h/week or other measures that can be used to calculate analytical values. (5) The study design was a cohort study. Exclusion criteria: (1) protocol, review, or without adequate information for analysis; (2) written in non-English.
This systematic review and meta-analysis will retrieve potential studies in the PubMed, Embase, Web of Science, and the Cochrane Library database based on keywords and medical subject heading (MeSH) terms such as “physical activity,” “chronic kidney disease,” and “mortality.” The detailed search strategy is listed in Supplementary File 1. The retrieval time is from inception to June 2022. To reduce the possibility of missing searches, we considered including “exercise” as a similar term to “physical activity.” In addition, we will also check references to similar systematic reviews to further identify potential studies.
Two authors (YB and HW) will perform the literature selection, and a third author (LH) will help resolve any discrepancies if encountered. First, the titles and abstracts of all retrieved articles will be independently reviewed, and studies that do not meet the inclusion criteria will be excluded. Then, to determine if the articles meet the inclusion criteria, each author will further review the full text of the remaining studies. The flowchart of the literature search and selection strategy is shown in Figure 1.
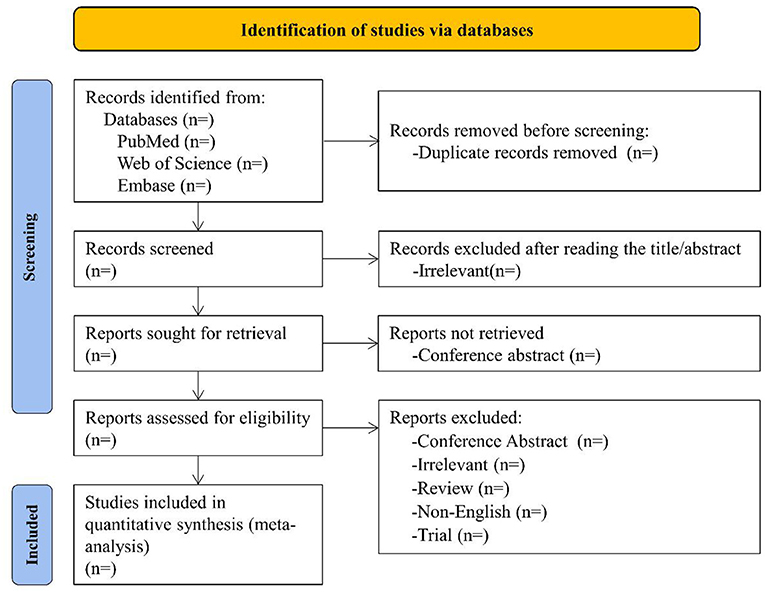
Figure 1. Flowchart showing the results of the selection process.
The Cohen kappa statistic (κ) was calculated during the screening process to assess the level of agreement of reviewers. Consistency was classified a priori as follows: substantial consistency: κ > 0.60; moderate consistency: 0.21 ≤ κ ≤ 0.60; slight consistency: κ < 0.21 (13).
Two authors (YB and HW) will extract data according to Table 1. Disagreements will be resolved by consensus or discussion with a third author (LH). The relevant data to be collected include baseline characteristics of the population (e.g., study design, data source, age, gender, and sample size), stage of CKD, number of deaths, follow-up time, physical activity measures, physical activity units (e.g., kilocalories/week, MET*h/week, or steps/day), covariates from multivariate models, and adjusted effect sizes (ORs/RRs/HRs) and 95% CI in each physical activity category. A total effect size will be collected if two or more adjusted effect sizes were reported in a study. This study proposes to use the Newcastle-Ottawa Scale (NOS) to assess the quality of cohort studies. The scale has three domains with a maximum possible score of nine: selection of the cohort (0–4), comparability of the cohort (0–2), and assessment of the outcome (0–3). A NOS score of ≥6 is considered medium to high quality. Otherwise, it is considered low quality.

Table 1. The characteristic of included studies.
First, we harmonized the group-level exposure estimates in MET*h/week to pool physical activity of different intensities and durations accumulated over the week. Physical activity was classified as low intensity (<3 METs), moderate-intensity (3–5.9 METs), and vigorous-intensity (≥6 METs) according to WHO classification criteria (14). When a study reported separate but uncombined results for different subgroups, we will use a fixed-effects model to combine the results for specific subgroups to obtain an overall estimate for the primary analysis. For studies that did not use the lowest category of physical activity as the reference category, we will recalculate the RRs using the method of Hamling et al. so that the lowest category becomes the reference (15).
When a study did not directly report physical activity, it was calculated by multiplying the median or midpoint duration of the reporting category with its assigned total MET value. The median or mean of the physical activity in each category was assigned to the corresponding RR for each study. For studies that reported physical activity, we estimated the midpoint of each category by calculating the mean of the lower and upper bounds. When the highest or lowest category was open-ended, we assumed that the length of the open interval was the same as the adjacent interval. For studies that reported physical activity at a weekly or monthly frequency, we converted frequency to hours per week or month by setting the dose of each activity at 45 min. If only the average duration of physical activity (e.g., walking) was reported, we assumed intensity of 4.5 METs. In addition, when studies reported kcal/week, we would convert between kcal/week (Y) and MET-h/week (X) using the following equation: X (MET*h)/Y (kcal) = 4.5 MET*2.5 h/550 kcal (16). The calculation of the dose distribution is shown in Table 2.

Table 2. Summary of MET*h/week assignment calculations for included studies.
In sensitivity analyses, the intensity of marginalized PA doses (MET-h/week) was considered by subtracting the resting metabolic rate of 1 MET from the original mean PA intensity (2, 3, 3.5, and 7 MET for mild physical activity, moderate physical activity, moderate to vigorous physical activity, and vigorous physical activity, respectively).
The primary outcome of this systematic review and dose-response meta-analysis will be all-cause mortality, and the secondary outcome will be cardiovascular mortality.
We will use a random-effects model to calculate the pooled RR and 95% CI for the highest vs. lowest physical activity level. We then used a robust error meta-regression (REMR) model to establish dose-response relationships between physical activity and mortality (17). The REMR model is a one-stage procedure that treats each study as a cohort and weights the effects of each study by its inverse variance while using robust variance to address the potential correlation of within-study effects. Considering that the dose-response relationship may be a non-linear pattern, we will use a restricted cubic spline function to fit the dose-response curve (18). This was done by setting three fixed nodes on the 5, 50, and 95 quartiles (19). The Wald test was used to test for non-linearity, with the null hypothesis that the coefficient of the non-linear term is equal to zero. All analyses will be carried out in Stata 12.0, and P < 0.05 was considered statistically significant.
Given the potential heterogeneity, a random effect model will assess the summary effect sizes. We will quantify statistical heterogeneity using the I2 statistic. The evaluation criteria are as follow: <25% means small; 25–50% represents moderate heterogeneity; ≥50% considers heterogeneity. Subgroup analysis and meta-regression were used to explore potential heterogeneity based on specific characteristics, such as region, follow-up time, gender, sample size, and disease stage. Funnel plots and Egger's tests will be conducted to investigate publication bias across studies.
If adequate data are available, we will perform subgroup analysis for the following: (1) region; (2) physical activity of different intensity (low-moderate vs. vigorous); (3) CKD stage (pre-dialysis vs. peritoneal dialysis vs. hemodialysis vs. kidney transplant); (4) follow-up duration [short term (1–3 months) vs. medium term (3–12 months) vs. long term (≥1 year)].
Sensitivity analysis will be performed to test the stability of the meta-analysis result, such as examining the effect of individual studies on the overall effect size by omitting one study.
We will use the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach (study limitations, consistency of effect, imprecision, indirectness, and publication bias) to determine the outcome's overall quality of the evidence (20). Furthermore, a summary of the findings table will be developed using the GRADEpro Tool (https://gradepro.org/).
Increasing physical activity levels may lead to improved physical function and, in turn, maintenance of independence and improved survival rates in patients with CKD (7). Therefore, most guidelines recommend 150 min of moderate intensity physical activity per week for CKD (21, 22). However, this recommendation is based on results from the general population, and the level of physical activity that would benefit people with chronic disease who have CKD is still unknown. The results of this study will address such clinical evidence.
This meta-analysis will present evidence related to all-cause mortality and physical activity in CKD patients. Nevertheless, some potential limitations need to be noted. First, different disease stages, gender, race, and other confounding factors may cause more significant heterogeneity in the results; therefore, if sufficient data are available, we will identify sources of heterogeneity through subgroup analysis and meta-regression and determine the stability of the results through sensitivity analysis. Second, the method of calculating physical activity dose according to the intensity or duration of physical activity exposure may distort the proper relationship between physical activity level and all-cause mortality. Third, the included studies contained self-reported physical activity, which may be prone to recall bias and overestimate effect values.
LH: conceptualization and writing—review and editing. FZ and YB: methodology. FZ and HW: writing—original draft. All authors contributed to the article and approved the submitted version.
This study was supported by Shanghai Key Clinical Specialty Construction Project-Chinese Medicine Nephropathy (Grant No: shslczdzk04201) and Longhua Hospital Shanghai University of Traditional Chinese Medicine (Grant No: YW.006.035).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.861013/full#supplementary-material
Supplementary File1. Search detail for the database.
1. Crews DC, Bello AK, Saadi G. Burden, access and disparities in kidney disease. Clin Kidney J. (2019) 12:160–6. doi: 10.1093/ckj/sfy128
2. Liyanage T, Ninomiya T, Jha V, Neal B, Patrice HM, Okpechi I, et al. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet. (2015) 385:1975–82. doi: 10.1016/S0140-6736(14)61601-9
3. Cozzolino M, Mangano M, Stucchi A, Ciceri P, Conte F, Galassi A. Cardiovascular disease in dialysis patients. Nephrol Dial Transplant. (2018) 33:iii28–iii34. doi: 10.1093/ndt/gfy174
4. GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2020) 395:709–33. doi: 10.1016/S0140-6736(20)30045-3
5. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. (1985) 100:126–31.
6. Hoshino J. Renal rehabilitation: exercise intervention and nutritional support in dialysis patients. Nutrients. (2021) 13:1444. doi: 10.3390/nu13051444
7. Zelle DM, Klaassen G, van Adrichem E, Bakker SJL, Corpeleijn E, Navis G. Physical inactivity: a risk factor and target for intervention in renal care. Nat Rev Nephrol. (2017) 13:152–68. doi: 10.1038/nrneph.2016.187
8. Hupin D, Roche F, Gremeaux V, Chatard J-C, Oriol M, Gaspoz J-M, et al. Even a low-dose of moderate-to-vigorous physical activity reduces mortality by 22% in adults aged ≥60 years: a systematic review and meta-analysis. Br J Sports Med. (2015) 49:1262–7. doi: 10.1136/bjsports-2014-094306
9. Ekelund U, Brown WJ, Steene-Johannessen J, Fagerland MW, Owen N, Powell KE, et al. Do the associations of sedentary behaviour with cardiovascular disease mortality and cancer mortality differ by physical activity level? A systematic review and harmonised meta-analysis of data from 850 060 participants. Br J Sports Med. (2019) 53:886–94. doi: 10.1136/bjsports-2017-098963
10. MacKinnon HJ, Wilkinson TJ, Clarke AL, Gould DW, O'Sullivan TF, Xenophontos S, et al. The association of physical function and physical activity with all-cause mortality and adverse clinical outcomes in nondialysis chronic kidney disease: a systematic review. Ther Adv Chronic Dis. (2018) 9:209–26. doi: 10.1177/2040622318785575
11. Martins P, Marques EA, Leal DV, Ferreira A, Wilund KR, Viana JL. Association between physical activity and mortality in end-stage kidney disease: a systematic review of observational studies. BMC Nephrol. (2021) 22:227. doi: 10.1186/s12882-021-02407-w
12. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. (2000) 283:2008–12. doi: 10.1001/jama.283.15.2008
13. McGinn T, Wyer PC, Newman TB, Keitz S, Leipzig R, For GG. Tips for learners of evidence-based medicine: 3. Measures of observer variability (kappa statistic). CMAJ. (2004) 171:1369–73. doi: 10.1503/cmaj.1031981
14. Bull FC, Al-Ansari SS, Biddle S, Borodulin K, Buman MP, Cardon G, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. (2020) 54:1451–62. doi: 10.1136/bjsports-2020-102955
15. Hamling J, Lee P, Weitkunat R, Ambühl M. Facilitating meta-analyses by deriving relative effect and precision estimates for alternative comparisons from a set of estimates presented by exposure level or disease category. Stat Med. (2008) 27:954–70. doi: 10.1002/sim.3013
16. Sattelmair J, Pertman J, Ding EL, Kohl HW, Haskell W, Lee IM. Dose response between physical activity and risk of coronary heart disease: a meta-analysis. Circulation. (2011) 124:789–95. doi: 10.1161/CIRCULATIONAHA.110.010710
17. Xu C, Doi SAR. The robust error meta-regression method for dose-response meta-analysis. Int J Evid Based Healthc. (2018) 16:138–44. doi: 10.1097/XEB.0000000000000132
18. Durrleman S, Simon R. Flexible regression models with cubic splines. Stat Med. (1989) 8:551–61. doi: 10.1002/sim.4780080504
19. Xu C, Liu Y, Jia P-L, Li L, Liu T-Z, Cheng L-L, et al. The methodological quality of dose-response meta-analyses needed substantial improvement: a cross-sectional survey and proposed recommendations. J Clin Epidemiol. (2019) 107:1–11. doi: 10.1016/j.jclinepi.2018.11.007
20. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. (2008) 336:924–6. doi: 10.1136/bmj.39489.470347.AD
21. Baker LA, March DS, Wilkinson TJ, Billany RE, Bishop NC, Castle EM, et al. Clinical practice guideline exercise and lifestyle in chronic kidney disease. BMC Nephrol. (2022) 23:75. doi: 10.1186/s12882-021-02618-1
Keywords: physical activity, chronic kidney disease, mortality, dose-response, meta-analysis
Citation: Zhang F, Wang H, Huang L and Bai Y (2022) Physical Activity and Mortality in Patients With Chronic Kidney Disease: A Protocol for Systematic Review and Dose-Response Meta-Analysis. Front. Med. 9:861013. doi: 10.3389/fmed.2022.861013
Received: 24 January 2022; Accepted: 07 March 2022;
Published: 11 April 2022.
Edited by:
Yoshiyuki Morishita, Jichi Medical University Saitama Medical Center, JapanReviewed by:
Tao-Hsin Tung, Taizhou Hospital of Zhejiang Province Affiliated to Wenzhou Medical University, ChinaCopyright © 2022 Zhang, Wang, Huang and Bai. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fan Zhang, ZmFuX3poYW5nMTk5M0AxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.