 Ahsan Raquib1
Ahsan Raquib1 Radwan Raquib1,2
Radwan Raquib1,2 Safayet Jamil3
Safayet Jamil3 Ahmed Hossain4,5†
Ahmed Hossain4,5† Firoj al-Mamun1,6,7†
Firoj al-Mamun1,6,7† Mohammed A. Mamun1,6,7,8*†
Mohammed A. Mamun1,6,7,8*†- 1CHINTA Research Bangladesh, Dhaka, Bangladesh
- 2Faculty of Veterinary, Animal and Biomedical Sciences, Sylhet Agricultural University, Sylhet, Bangladesh
- 3Department of Pharmacy, Khwaja Yunus Ali University, Sirajgonj, Bangladesh
- 4Department of Public Health, North South University, Dhaka, Bangladesh
- 5Global Health Institute, North South University, Dhaka, Bangladesh
- 6Department of Public Health and Informatics, Jahangirnagar University, Dhaka, Bangladesh
- 7Department of Public Health, University of South Asia, Dhaka, Bangladesh
- 8Department of Public Health, Daffodil International University, Dhaka, Bangladesh
Background: Numerous studies on knowledge, attitude, and practice (KAP) about the prevention of COVID-19 infections are available in Bangladeshi contexts, with results that vary significantly. However, no earlier attempt has been made to analyze the available COVID-19 KAP studies in Bangladesh, which is incorporated in this meta-analysis for the first time.
Methods: Following the PRISMA guidelines, articles relevant to COVID-19 KAP that were conducted among the Bangladeshi population were found in databases such as PubMed, Scopus, CINAHL, Google Scholar, and ResearchGate. Random-effect meta-analysis was used to generate a pooled prevalence of knowledge, attitude, and practice level toward the prevention of COVID-19 infection.
Results: This review included 18 articles that were published between March 2020 and November 2021. Overall, 89.87% (95% CI: 67.71–97.40) understood about COVID-19 symptoms, 92.09% (95% CI: 84.32–96.18) knew about how it spreads, and 79.51% (95% CI: 59.38–91.15) knew about how to treat it. The public's perception of controlling COVID-19 is mixed, with only 44.16% (95% CI: 35.74–52.93) and 60.28% (95% CI: 49.22–70.38) believing the country would win the struggle against the pandemic and the infection will be successfully controlled, respectively. Although overall COVID-19 preventative practice was good, subgroup analysis found that men had a poor practice toward controlling the infection. The practice of avoiding crowded places (70.15%) and maintaining social distance (77.17%) was found to be satisfactory in institution-based studies.
Conclusion: The findings of this study revealed that the Bangladeshi population had a good awareness of COVID-19 symptoms, treatment, attitudes, and behaviors. The findings of this study are likely to aid Bangladeshi governments and policymakers in putting evidence into action by identifying gaps and emphasizing the importance of educating the less informed public about COVID-19 transmission.
Introduction
The COVID-19 pandemic caused by the SARS-CoV-2 virus has become the most public health concern affecting all aspects of life (1). The first case of COVID-19 was diagnosed in Wuhan, China, in late December 2019 (2, 3), by a patient with unexplained pneumonia etiology (4). However, as of November 22, 2021, approximately 258 million people are reported to be infected with the virus globally, whereas 5.15 million lost their lives. The World Health Organization declared it a pandemic due to its devastating effects on all aspects of health and the quality of life (5). The first COVID-19 case diagnosis in Bangladesh was reported on March 8, 2020 (6, 7). The country has been alleged to have poor healthcare facilities and skilled manpower to tackle any health emergencies. This situation worsened during the pandemic due to the overwhelming number of cases (8). As of November 22, 2021, 1.57 million Bangladeshi people have been tested positive for the virus, and the number of mortalities is 28,000. However, to mitigate the virus's rapid transmission, approaches to medication or therapeutic such as social movement restriction, lockdown, and quarantine have been imposed (9).
The impact of COVID-19 is severe among these people with chronic medical conditions such as diabetes, cancer, heart disease, and circulatory disorders, although general people are not escaping from the stressful situation created by the pandemic (10). Consequently, unwanted fear, panic, and worry related to being infected with the virus, loss of beloved ones, and economic crisis occur, whereas people have been reported at a higher risk of issues such as common mental health problems (i.e., depression, anxiety, and stress) and poor physical health along with inflammatory diseases (5, 11). Nearly half of the Bangladeshi people have been reported suffering from mental health problems (higher than the prevalence rates of mental disorders during the normal period), as estimated by a recent meta-analysis of the studies conducted during the COVID-19 pandemic (12). However, Bangladesh, like other countries, has implemented various safety precautions to mitigate the transmission, including pedestrianizing flow, confining them at home, allowing them to work from home, increasing awareness, disseminating information, closing schools, and providing other public assistance (13, 14).
It is said that public response to a disease is determined by knowledge and understanding of its etiology, signs and symptoms, treatment, and even prevention, which are expressed by their attitudes and practices toward the diseases (15, 16). The risk of disease-related adverse outcomes in a population increases if negative attitudes and practices are not possibly measured for modification. Therefore, assessing public understanding, perception, and experience related to COVID-19 is essential to visualize their preparedness for the pandemic (15, 16). This helps government and health authorities determine how to adopt the programs to control the outbreak. Therefore, many studies have been conducted to assess Bangladesh's knowledge, attitudes, and practice (KAP) toward COVID-19, but there is a lack of evidence generated from a systematic evaluation.
Given the nature of the COVID-19 pandemic, regular update of scientific literature is essential for initiating empirical evidence on interventions and strategies to tackle the COVID-19 pandemic more conveniently. For this purpose, a comprehensive and timely updated systematic evaluation of existing evidence is highly needed, whereas a few systematic review and meta-analysis has been published on the KAP of COVID-19 (15, 17–19). Notwithstanding, region- or country-based systematic reviews lack; for instance, Ethiopia (17, 20) and the United States (20) have reported publishing country-based systematic reviews on the KAP of COVID-19. Furthermore, knowledge and public perception being culture-based, interventions should focus on the data from the respective culture. Despite the global evidence, it is hard to achieve any policy directions and implement them due to cultural sensitivity. As a result, in order to better grasp the KAP for COVID-19 prevention in Bangladesh, a systematic review and meta-analysis is undertaken herein to better comprehend the infection's control.
Methods
Search Strategy
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol was used as a guideline for performing the present systematic review. To identify relevant studies for including in this review, a systematic literature search was conducted on the relevant databases like PubMed, Scopus, CINAHL, and Google Scholar between July 1, 2021, and July 10, 2021. In addition, random searches were done in ResearchGate to include missing literature. The search strategy included keywords in the combination of (i) knowledge OR attitude OR perception OR practice, (ii) corona virus OR novel coronavirus OR COVID-19 OR severe acute respiratory syndrome (iii) Bangladesh.
Eligibility Criteria
For inclusion of the literature, the following criteria were applied to the retrieved studies (i) being a cross-sectional observation study, (ii) having full-text access, (iii) being concerned with any of the KAP of COVID-19 related questions (Supplementary File), (iv) being published in a peer-reviewed journal in English, (iv) being conducted between March 2020 and November 2021, and (v) being conducted among Bangladeshi residents. In addition, literature like editorial, letter to the editor, commentary, perspective, preprint, and articles that failed to fulfill the aforementioned eligibility criteria were eliminated from this study.
Study Selection
To remove duplicate studies, articles (N = 2,110) retrieved from the database searches were exported to reference manager Zotero and Excel 2013. After carefully removing duplicate articles (n = 149), the title and abstracts of the remaining 1,923 studies were screened for pertinent studies, followed by a freely accessible study selection and relevant study selection based on eligibility criteria. Through title and abstract screening, 36 articles were left for full-text reading, and based on the eligible criteria, 18 articles were finally selected to be included in this review (Figure 1).
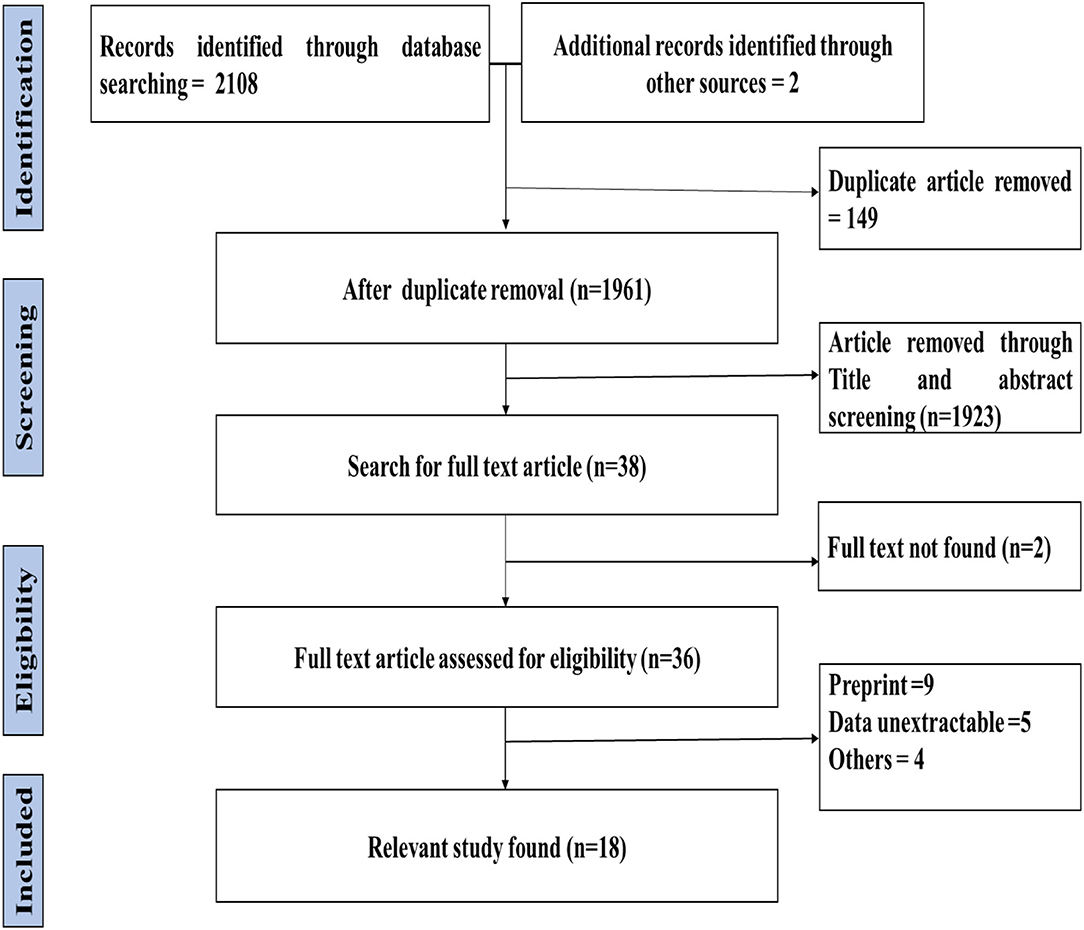
Figure 1. PRISMA flow diagram of literature search and study selection.
Quality Assessment
Risk of Bias Tool (RoBT) that was developed by Hoy et al. (21) was used to assess the risk of bias of all the included studies in this review. This assessment evaluated 10 items in which external validity (items one to four) and internal validity (items five to ten) were measured (Supplementary File). Each item of RoBT is scored “0” (risk of bias absent) or “1” (risk of bias present), where 10 is the highest score reflecting a greater risk of bias. However, based on the RoBT score, studies were classified as low risk (0–3), moderate risk (4–6), and high risk (7–10).
Data Extraction
From the eligible studies, the following information was retrieved in an excel file: first author, sample collection date, publication year, participant's characteristics (age, sex, education level, and occupation), focus group, study design, number of participants, and percentage of positive answers on each selected KAP (knowledge, attitude, and practice) questions.
Data Analysis
R studio version 4.1.0 was used to perform a meta-analysis of the data exported from an Excel spreadsheet. I2 (%) statistics were applied for the evaluation of study heterogeneity, where 25, 50, and 75% represented low, moderate, and severe heterogeneity, respectively. A random-effect model was employed to conduct the meta-analysis because of high heterogeneity, and the results were presented in forest plots. Additional subgroup analysis was conducted for study design and gender. Publication bias assessment was visualized by funnel plot and for rigorous assumptions egger's regression test was performed.
Results
Characteristics of the Included Studies
General Description of the Included Studies
All the selected studies (n = 18) comprised a total of 16,443 participants, where 8,523, 7,885, and 15 participants were male, female, and others, respectively, with a sample size range from 110 to 2,157. Twelve studies (6, 8, 9, 22–30) employed a community-based cross-sectional study design, and the other six (1, 2, 31–34) used an institutional-based cross-sectional study design. Among the included studies, 11 were published in 2020, and seven were published in 2021 (Table 1).
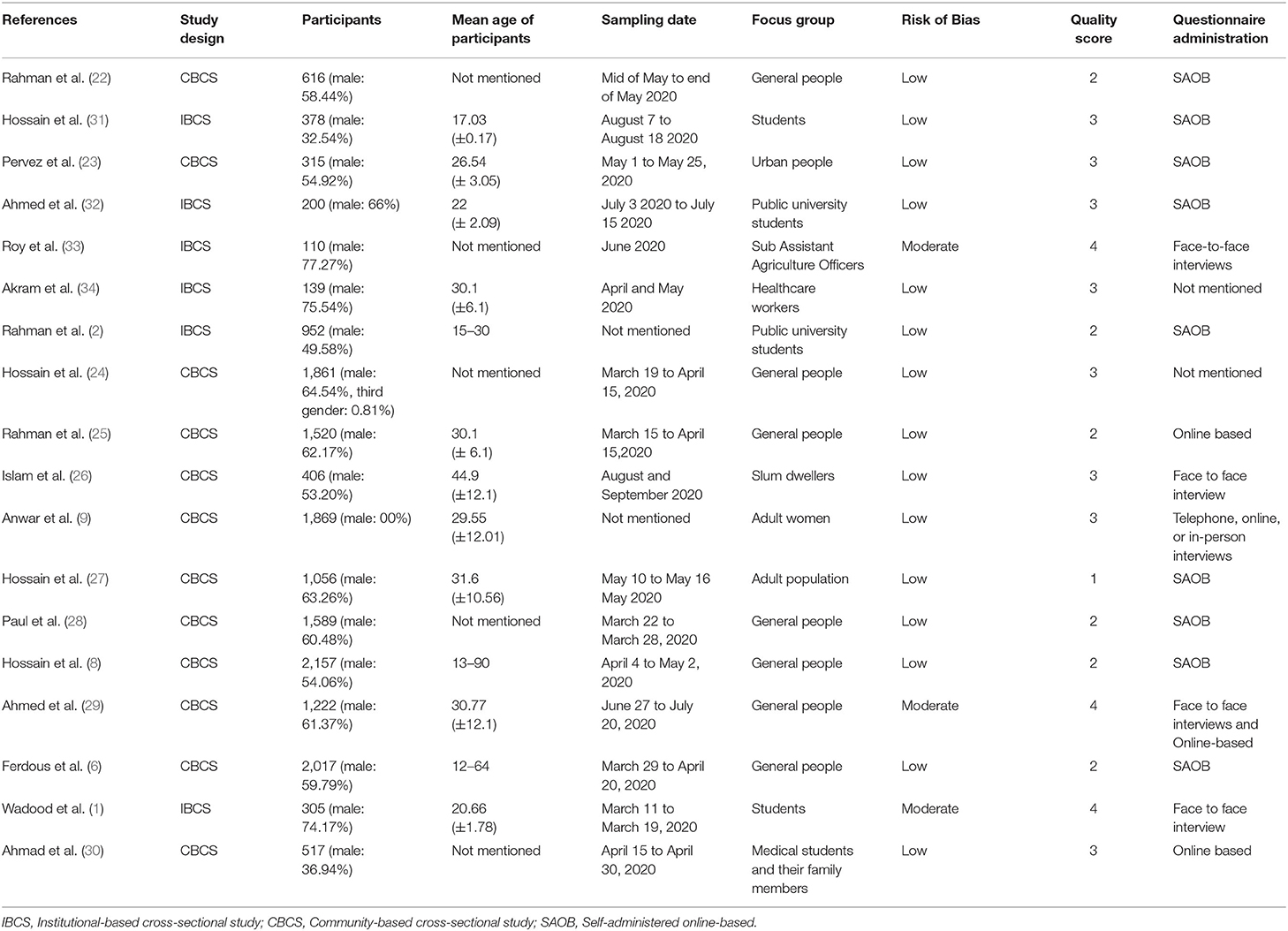
Table 1. Demographic characteristics of the participants.
Measurement Used in the Included Studies
Knowledge of COVID-19 was assessed by the domains of (i) symptoms (fever, dry cough, respiratory signs, weakness, diarrhea, headache, and sore throat), (ii) transmission (spread through respiratory droplet), and (iii) treatment (no specific treatment is available), whereas those items were responded using “Yes/No/Don't know,” or “True/False/Not sure” scheme in the included studies. In case of practices related to COVID-19 (wash hands regularly, maintain social distance, avoid the crowded place, and always wear a mask when going outside) and attitudes concerning COVID-19 (COVID-19 pandemic will be successfully controlled, and Bangladesh can win the battle against the COVID-19 pandemic), the included studies collected response using “Yes/No/Don't know” or “Strongly agree/Agree/Neutral/Disagree/Strongly disagree” items. The responses of “Yes,” “True,” or “Strongly agree/Agree” are considered positive responses for analysis herein.
Knowledge About COVID-19 Symptoms
Nine studies reported about overall knowledge of participants about COVID-19 symptoms, where 89.87% (95%, CI: 67.71–97.40%) participants had positive knowledge. In addition, six studies reported knowledge of fever, dry cough, and respiratory signs, where 93.54, 85.54, and 85.97% positive knowledge was encountered. Conversely, the lowest percentage of participants' knowledge was on diarrhea (39.24%, 95% CI: 19.10–63.85%) (Table 2). The forest is presented in Figure 2.
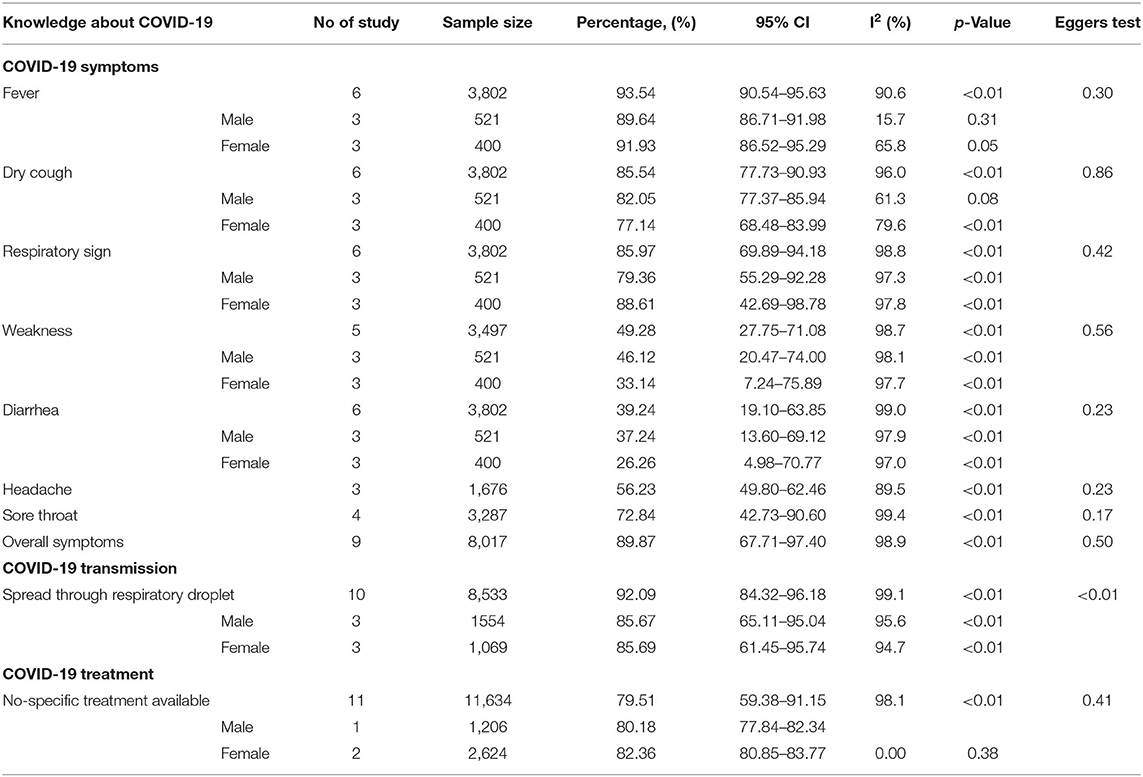
Table 2. Pooled prevalence of knowledge about COVID-19 among Bangladeshi residents.
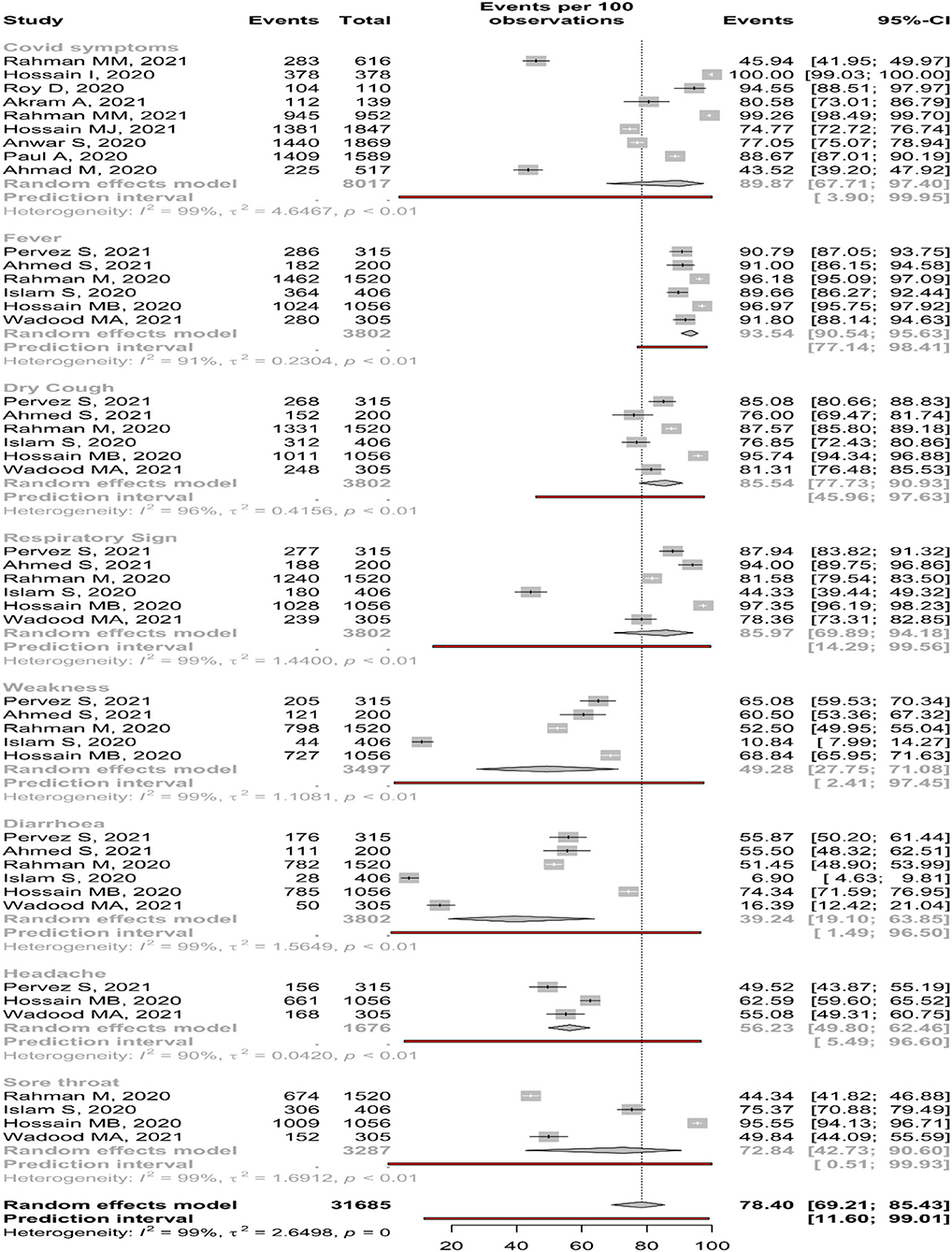
Figure 2. Knowledge about COVID-19 symptoms among Bangladeshi residents.
The subgroup meta-analysis of COVID-19 symptoms reveals that participants of the community-based studies had higher knowledge about fever, dry cough, diarrhea, headache, and sore throat than institution-based studies. In the case of gender, the male had higher knowledge of fever, dry cough, weakness, and diarrhea (Supplementary Material).
Knowledge About COVID-19 Transmission
Only 10 studies reported transmission, and random-effect meta-analysis estimated 92.09% (95% CI: 84.32–96.18%) participants were aware of the fact that COVID-19 can transmit through respiratory droplets. A substantial amount of study heterogeneity was identified (I2 = 99.1%), where Eggers tests showed a small-study effect (Table 2). The forest is presented in Figure 3.
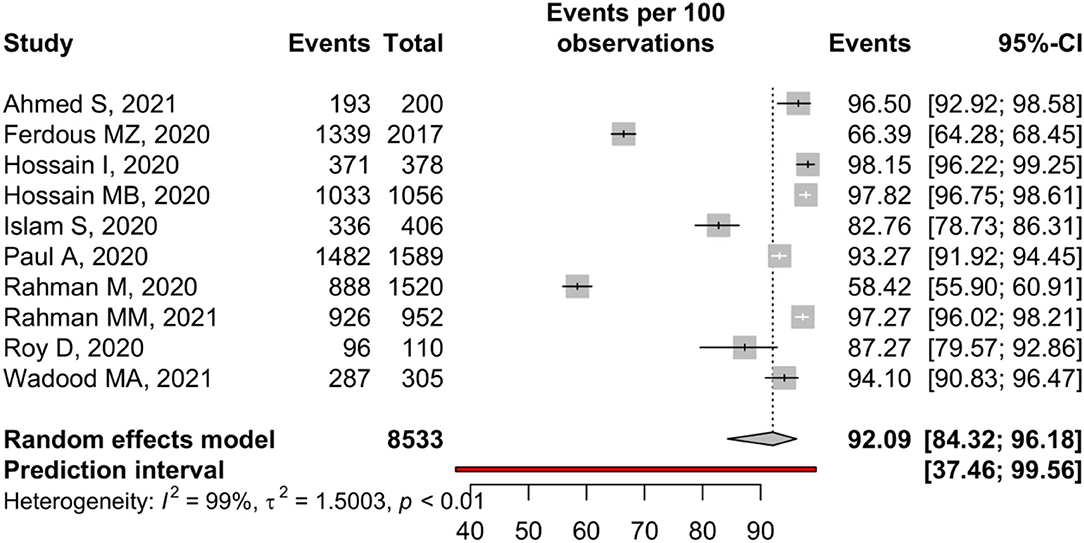
Figure 3. Knowledge about COVID-19 transmission among Bangladeshi residents.
In the subgroup analysis of gender, it was found that males (85.67%, 95% CI: 65.11–95.04%) and females (85.69%, 95% CI: 61.45–95.74%) had the almost same level of knowledge of COVID-19 transmission. Appropriate knowledge of transmission was estimated as 85.82 % (95%, CI: 66.41–94.88%) in CBCS and 95.82% (95%, CI: 92.50–97.70%) in IBCS (Supplementary Material).
Knowledge About COVID-19 Treatment
Eleven studies reported the treatment of COVID-19, and 79.51% (95%, CI: 59.38–91.15%) of participants know that COVID-19 has no specific treatment. A substantial amount of study heterogeneity was identified (I2 = 98.1%), whereas a small-study effect was absent based on the Eggers test (p = 0.41) (Table 2). The forest is presented in Figure 4.
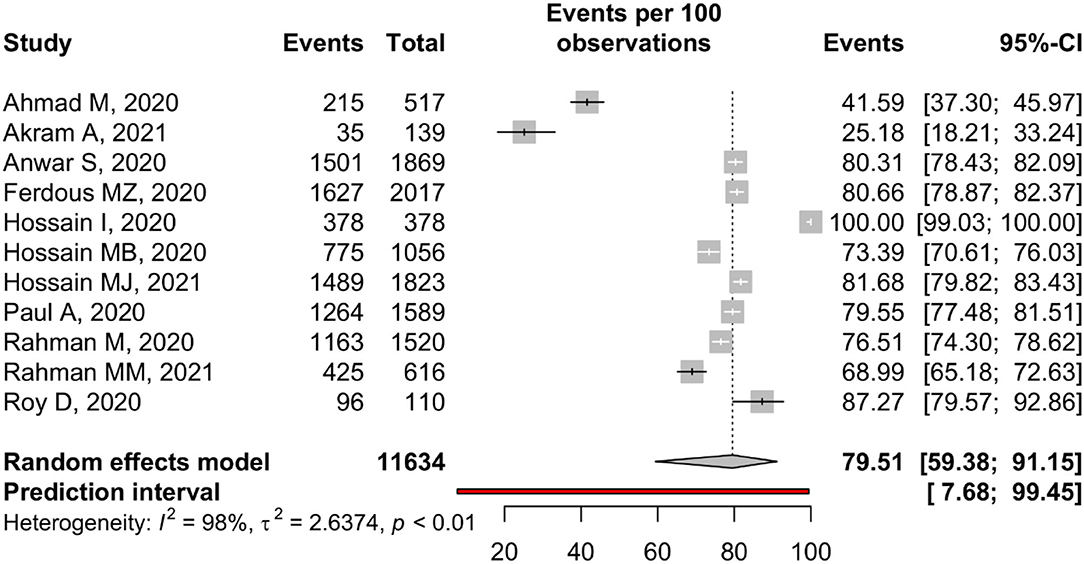
Figure 4. Knowledge about COVID-19 treatments among Bangladeshi residents.
Participants of IBCS (95.84%, 95% CI: 11.58–99.98%) had better knowledge of COVID-19 treatment than the participants of CBCS (74.01%, 95% CI: 65.83–80.80%). Higher percentage of female (82.36%, 95% CI: 80.85–83.77%) knew about the unavailability of specific treatment of COVID-19 than male (80.18%, 95% CI: 77.84–82.34%) (Supplementary Material).
Attitude Toward COVID-19
Five studies reported attitudes toward the control of COVID-19, and 60.28% (95%, CI: 49.22–70.38%) hold a positive attitude toward it (Table 3). In addition, three community-based and two institutional-based studies assessed this attitude among people with an estimated positive attitude of 58.47 and 63.06%, respectively (Supplementary Material). The forest is presented in Figure 5.

Table 3. Pooled prevalence of attitude toward COVID-19 among Bangladeshi residents.
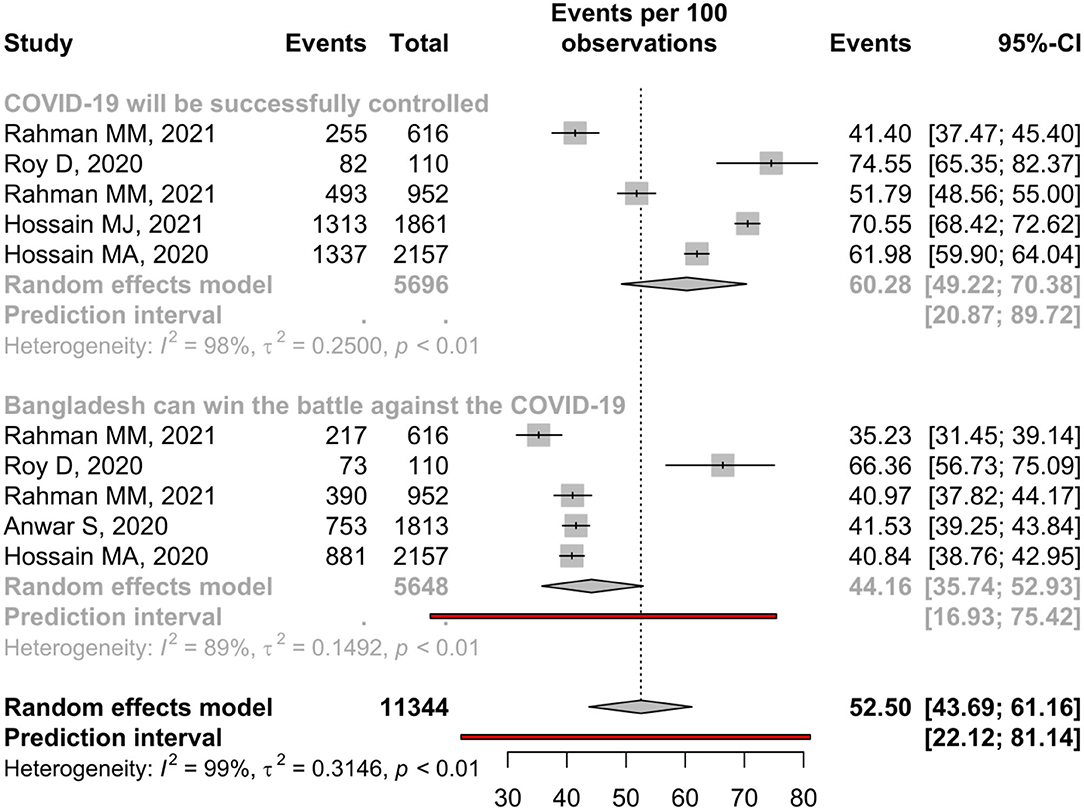
Figure 5. Attitude toward COVID-19 among Bangladeshi residents.
Only 44.16% of people believe Bangladesh can win the battle against COVID-19, and males (41.77%) and females (40.91%) hold almost similar levels of positive attitude toward this (Table 3). In contrast, participants of institutional-based studies (53.12%) had a better attitude than the participants of community-based studies (39.71%) (Supplementary Material).
Practice of COVID-19
Only 12 studies reported handwashing practice; random-effect meta-analysis estimated 93.79% (95%, CI: 87.21–97.10%) participants regularly do this practice. A substantial amount of study heterogeneity was identified (I2 = 96.8%), whereas no small-study effect was found based on the Eggers tests (p = 0.09) (Table 4). The forest is presented in Figure 6. Male (91.30%, CI: 78.96–96.71%) and participants of IBCS (96.17%, CI: 85.54–99.07%) used to do this practice more frequently than female (90.53%, CI: 75.53–96.74%) and participants of CBCS (91.71%, CI: 81.28–96.57%) (Supplementary Material).
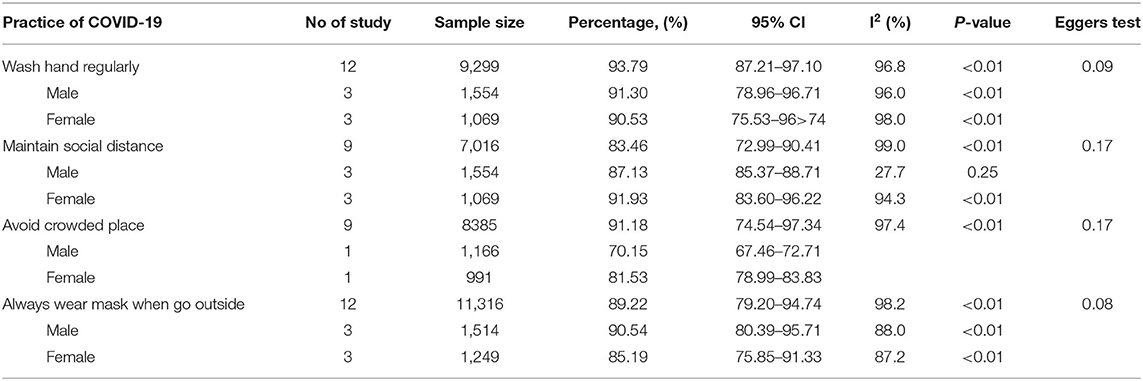
Table 4. Pooled prevalence of practice about COVID-19 among Bangladeshi residents.
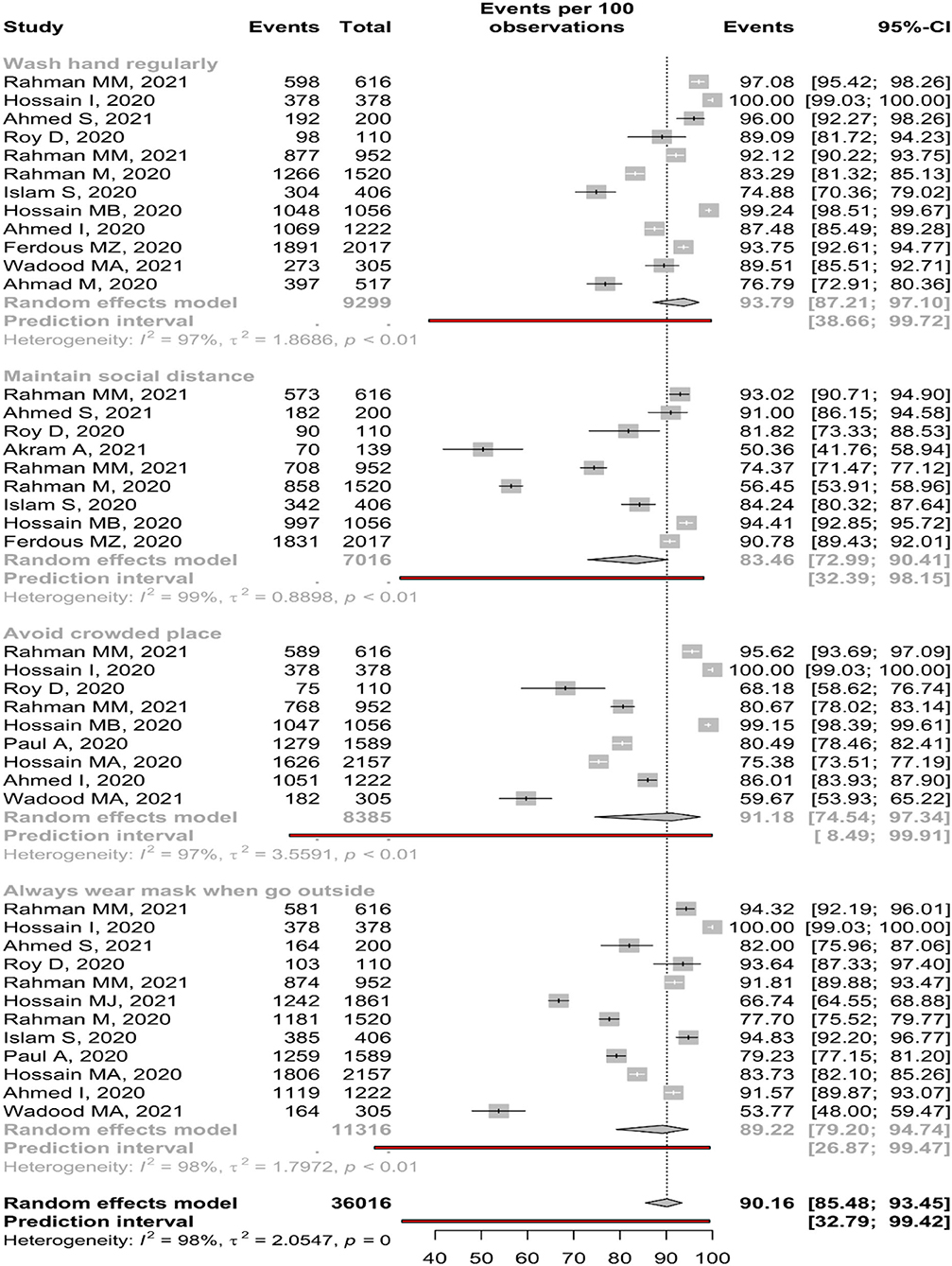
Figure 6. Practice about COVID-19 among Bangladeshi residents.
Nine studies reported about maintaining social distance, and only 83.46 % (95%, CI: 72.99–90.41%) participants found to do this practice (Table 4). The forest is presented in Figure 6. Female (91.93%, CI: 83.60–96.22%) and participants of CBCS (87.29%, CI: 75.28–93.94%) used to do this practice more frequently than male (87.13% CI: 85.37–88.71%) and participants of IBCS (77.17%, CI: 59.92–88.43%) (Supplementary Material).
Random-effect meta-analysis revealed 91.18 % (95% CI: 74.54–97.34%, p < 0.01) participants avoid crowded place. A substantial amount of study heterogeneity was identified (I2 = 97.4%). In the Eggers tests, no small-study effect was found (p = 0.17) (Table 4). The forest is presented in Figure 6. About 91.86 % and 92.10% of participants of CBCS and IBCS avoid crowded places, respectively (Supplementary Material).
About 89.22% (95% CI: 79.20–94.74%) participants from 12 reported studies always wear mask during going outside (Table 4). The forest is presented in Figure 6. Male (90.54%, CI: 80.39–95.71%) and participants of IBCS (93.78%, CI: 65.43–99.18%) used to do this practice more frequently than female (85.19%, CI: 75.85–91.33%) and participants of CBCS (86.40%, CI: 78.03–91.91%) (Supplementary Material).
Discussion
This systematic review and meta-analysis evaluated participants' overall knowledge of COVID-19 symptoms, transmission, treatment, and attitudes toward successfully controlling the COVID-19 pandemic. In addition, the COVID-19 control practices such as hand washing, wearing a mask, avoiding crowded places, and maintaining social distance were also evaluated in this study. The study included 18 articles, 12 of which used a community-based cross-sectional study design and six of which used an institutional-based cross-sectional study design.
Overall, a significant portion of the participants had knowledge about COVID-19 symptoms (89.87%, CI: 67.71–97.40%), whereas the symptoms like fever, dry cough, and respiratory signs were found to be known to the participants. But, less than half of the participants were not aware of diarrhea (39.24%) and weakness (49.28%) as the COVID-19 symptoms, and only 56.23% of people had positive knowledge about the headache; this may be due to those symptoms being less common among the COVID-19 infected individuals. In addition, a high percentage of participants were reported to know about COVID-19 transmission through respiratory droplets (92.09%) and the unavailability of its specific treatment (79.51%). In subgroup analysis, male gender had better knowledge than females, only in knowledge related to the symptom of dry cough, weakness, and diarrhea, while participants of the community-based studies were more informed about a sore throat, headache, diarrhea, dry cough, and fever as a symptom of COVID-19 than participants of the institutional-based studies. Those findings might denote that residents of Bangladesh have shallow and insufficient knowledge about some domains of the COVID-19 knowledge, where inappropriate and poor knowledge could potentially lead to a hover in the attempt to find medical support and, consequently, a hover in the early diagnosis and treatment (13, 14). Therefore, smattering knowledge about the disease impedes control and elimination due to negligence in disease prevention practices (33, 35). Therefore, it is suggested that the country's public health authority focuses on those knowledge aspects that are poorly reported while implementing health education programs.
Based on this review, it is found that only 44.16% of Bangladeshi residents thought that the country would win the battle against the COVID-19 pandemic. On the contrary, a higher level of positive attitude, that is, 72.39% of general people of Ethiopia, was enumerated in a meta-analysis of COVID-19 KAP studies (36), reflecting dissatisfaction about pandemic management in Bangladesh. Several challenges and probable poor management of the pandemic in the country can be the forces for driving such a poor attitude among the Bangladeshi residents (37). However, as the pandemic is new to the management authority of the country, such dissatisfaction can be resolved over time by growing up the competency of the respective authorities.
Regarding practice related to COVID-19, this study reveals that a significant portion of the participants maintained washing hands (93.79%), wearing a mask (89.22%), and avoiding crowded places (91.18%), but maintaining social distancing was not always possible for a large portion, especially for the participants of institution-based studies (77.17%). Furthermore, males more frequently wore masks than females, but females had other better prevention practices such as maintaining social distance and avoiding crowded places. This may be because males are more likely to visit outside the home, which leads them to wear a mask and wash hands more frequently than females. In addition, the higher mortality of COVID-19 rate among the Bangladeshi males (37, 38) could make them more concerned about following more precautious measures despite going outside (8).
Before concluding the importance and potential implications of this meta-analysis findings, several limitations are supposed to be noted. First of all, journal articles published in English were only taken into consideration, limiting other sources such as preprint articles. All of the included studies that were conducted in online data collection approaches, limiting the findings' generalizability to the entire country's population. Besides, some of the studies were excluded because of not meeting the inclusion criteria [e.g., ten-thousand nationwide data were collected in the study of Hosen et al. (16), which could help generate evidence based on such a wider-spaced population's findings]. Factors associated with the COVID-19 KAP were not considered in the present study. Despite those limitations, the potency of this meta-analysis lies in the compilation of the results of 18 papers, which accentuated the results of the individual studies and permitted to acquire a merged prevalence that generated a shred of stronger evidence about COVID-19 KAP among the general Bangladeshi population. The findings of this study are likely to aid Bangladeshi governments and policymakers in putting evidence into action by identifying gaps and emphasizing the importance of educating the less informed public about COVID-19 transmission.
Conclusion
A number of KAP studies were undertaken in Bangladesh with populations from various categories, with notable variation in terms of gender, geography, occupation, and education. As a result, the study gives an overall KAP scenario for COVID-19 prophylaxis. This research should be taken into account by policymakers to underline the necessity of educating the less informed people about COVID-19 to restrict the spread of infection.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
AR and MM conceptualized the study. AR and RR did data extraction, where AR and Fa-M performed formal analysis. AR and SJ wrote the first draft, which has been extensively reviewed and edited by MM. Later on, further review and subsequent edits were performed by AR, AH, Fa-M, and MM. AR, Fa-M, and MM contributed to the study's methodology. AR managed resources and software with the help of Fa-M. AR, AH, and MM supervised the project. All authors read and finally approved the submission for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.856156/full#supplementary-material
References
1. Wadood MA, Mamun A, Rafi MA, Islam MK, Mohd S, Lee LL, et al. Survey on knowledge, attitude, perception and practice among university students during the COVID-19 pandemic. Sci Medicine J. (2021) 3:67–79. doi: 10.28991/SciMedJ-2021-03-SI-9
2. Rahman MM, Jhinuk JM, Nabila NH, Yeasmin MTM, Shobuj IA, Sayma TH, et al. Knowledge, attitude, and practices towards COVID-19 during the rapid rise period: a cross-sectional survey among public university students of Bangladesh. Sci Medicine J. (2021) 3:116–28. doi: 10.28991/SciMedJ-2021-0302-4
3. Khan MHR, Hossain A. Machine learning approaches reveal that the number of tests do not matter to the prediction of global confirmed COVID-19 cases. Front Artif Intell. (2020) 3:90. doi: 10.3389/frai.2020.561801
4. Lu S, Wei N, Jiang J, Wu L, Sheng J, Zhou J, et al. First report of manic-like symptoms in a COVID-19 patient with no previous history of a psychiatric disorder. J Affect Disord. (2020) 277:337–40. doi: 10.1016/j.jad.2020.08.031
5. Al Mamun F, Hosen I, Misti JM, Kaggwa MM, Mamun MA. Mental disorders of Bangladeshi students during the COVID-19 pandemic: a systematic review. Psychol Res Behav Manag. (2021) 14:645. doi: 10.2147/PRBM.S315961
6. Ferdous MZ, Islam MS, Sikder MT, Mosaddek ASM, Zegarra-Valdivia JA, Gozal D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: an online-based cross-sectional study. PLoS ONE. (2020) 15:e0239254. doi: 10.1371/journal.pone.0239254
7. Khan MHR, Howlader T. Breaking the back of COVID-19: Is Bangladesh doing enough testing? J Biomed Anal. (2020) 3:25–35. doi: 10.30577/jba.v3i2.46
8. Hossain MA, Jahid MIK, Hossain KMA, Walton LM, Uddin Z, Haque MO, et al. Knowledge, attitudes, and fear of COVID-19 during the rapid rise period in Bangladesh. PLoS ONE. (2020) 15:e0239646. doi: 10.1371/journal.pone.0239646
9. Anwar S, Araf Y, Newaz Khan A, Ullah M, Hoque N, Sarkar B, et al. Women's knowledge, attitude, and perceptions toward COVID-19 in lower-middle-income countries: a representative cross-sectional study in Bangladesh. Front Public Health. (2020) 8:721. doi: 10.3389/fpubh.2020.571689
10. Ejaz H, Alsrhani A, Zafar A, Javed H, Junaid K, Abdalla AE, et al. COVID-19 and comorbidities: deleterious impact on infected patients. J Infect Public Health. (2020) 13:1833–9. doi: 10.1016/j.jiph.2020.07.014
11. Quadros S, Garg S, Ranjan R, Vijayasarathi G, Mamun MA. Fear of COVID 19 infection across different cohorts: a scoping review. Front Psychiatry. (2021) 12:708430. doi: 10.3389/fpsyt.2021.708430
12. Hosen I, Al-Mamun F, Mamun MA. Prevalence and risk factors of the symptoms of depression, anxiety, and stress during the COVID-19 pandemic in Bangladesh: a systematic review and meta-analysis. Glob Ment Health. (2021) 8:e47. doi: 10.1017/gmh.2021.49
13. Anwar S, Nasrullah M, Hosen MJ. COVID-19 and Bangladesh: challenges and how to address them. Front Public Health. (2020) 8:154. doi: 10.3389/fpubh.2020.00154
14. Ali M, Ahsan GU, Khan R, Khan HR, Hossain A. Immediate impact of stay-at-home orders to control COVID-19 transmission on mental well-being in Bangladeshi adults: patterns, explanations, and future directions. BMC Res Notes. (2020) 13:1–7. doi: 10.1186/s13104-020-05345-2
15. Saadatjoo S, Miri M, Hassanipour S, Ameri H, Arab-Zozani M. Knowledge, attitudes, and practices of the general population about Coronavirus disease 2019 (COVID-19): a systematic review and meta-analysis with policy recommendations. Public Health. (2021) 194:185–95. doi: 10.1016/j.puhe.2021.03.005
16. Hosen I, Pakpour AH, Sakib N, Hussain N, Al Mamun F, Mamun MA. Knowledge and preventive behaviors regarding COVID-19 in Bangladesh: a nationwide distribution. PLoS ONE. (2021) 16:e0251151. doi: 10.1371/journal.pone.0251151
17. Azene AG, Workie MS, Aragaw AM. Knowledge, attitude, and prevention practice towards Covid-19 in ethiopia: systematic review and meta-analysis. Curr Ther Res. (2021) 94:100633. doi: 10.1016/j.curtheres.2021.100633
18. Bekele F, Sheleme T, Fekadu G, Bekele K. Patterns and associated factors of COVID-19 knowledge, attitude, and practice among general population and health care workers: a systematic review. SAGE Open Med. (2020) 8:2050312120970721. doi: 10.1177/2050312120970721
19. Siddiquea BN, Shetty A, Bhattacharya O, Afroz A, Billah B. Global epidemiology of COVID-19 knowledge, attitude and practice: a systematic review and meta-analysis. BMJ Open. (2021) 11:e051447. doi: 10.1136/bmjopen-2021-051447
20. Sarria-Guzmán Y, Fusaro C, Bernal JE, Mosso-González C, González-Jiménez FE, Serrano-Silva N. Knowledge, attitude and practices (KAP) towards COVID-19 pandemic in America: a preliminary systematic review. J Infect Dev Ctries. (2021) 15:9–21. doi: 10.3855/jidc.14388
21. Hoy D, Brooks P, Woolf A, Blyth F, March L, Bain C, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol. (2012) 65:934–9. doi: 10.1016/j.jclinepi.2011.11.014
22. Rahman MM, Khan SJ, Sakib MS, Halim MA, Rahman F, Rahman MM, et al. COVID-19 responses among general people of Bangladesh: status and individual view toward COVID-19 during lockdown period. Cogent Psychol. (2021) 8:1860186. doi: 10.1080/23311908.2020.1860186
23. Pervez S, Naher S, Pranta MUR, Banik R, Rahman QM. Perception and experiences regarding COVID-19 pandemic among urban young adults in Bangladesh: a mixed-method study. J Public Health. (2021) 1–11. doi: 10.1007/s10389-021-01600-3
24. Hossain MJ, Kuddus MR, Rahman SA. Knowledge, attitudes, and behavioral responses toward COVID-19 during early phase in Bangladesh: a questionnaire-based study. Asia Pac J Public Health. (2021) 33:141–4. doi: 10.1177/1010539520977328
25. Rahman M, Karamehic-Muratovic A, Amrin M, Chowdhury AH, Mondol M, Haque U, et al. COVID-19 epidemic in Bangladesh among rural and urban residents: an online cross-sectional survey of knowledge, attitudes, and practices. Epidemiologia. (2021) 2:1–13. doi: 10.3390/epidemiologia2010001
26. Islam S, Emran GI, Rahman E, Banik R, Sikder T, Smith L, et al. Knowledge, attitudes and practices associated with the COVID-19 among slum dwellers resided in Dhaka City: a Bangladeshi interview-based survey. J Public Health. (2021) 43:13–25. doi: 10.1093/pubmed/fdaa182
27. Hossain MB, Alam MZ, Islam MS, Sultan S, Faysal MM, Rima S, et al. Do knowledge and attitudes matter for preventive behavioral practices toward the COVID-19? a cross-sectional online survey among the adult population in Bangladesh. Heliyon. (2020) 6:e05799. doi: 10.1016/j.heliyon.2020.e05799
28. Paul A, Sikdar D, Hossain MM, Amin MR, Deeba F, Mahanta J, et al. Knowledge, attitudes, and practices toward the novel coronavirus among Bangladeshis: implications for mitigation measures. PLoS ONE. (2020) 15:e0238492. doi: 10.1371/journal.pone.0238492
29. Ahmed I, Hasan M, Akter R, Sarkar BK, Rahman M, Sarker MS, et al. Behavioral preventive measures and the use of medicines and herbal products among the public in response to Covid-19 in Bangladesh: a cross-sectional study. PLoS ONE. (2020) 15:e0243706. doi: 10.1371/journal.pone.0243706
30. Ahmad M, Rahman FN, Rahman MZ, Ali MZ, Ali M. Knowledge, attitude and practices among medical students and their family members towards the COVID-19 pandemic: an online based cross-sectional study. KYAMC J. (2021) 11:166–70. doi: 10.3329/kyamcj.v11i4.51990
31. Hossain I, Ahmad SA, Khan MH, Rahman A. COVID-19 and changing behaviors: a cross-sectional online survey among students in Bangladesh. Eur J Pharm Med Res. (2020) 7:576–81.
32. Ahmed S, Ali Md M, Hasan J. Knowledge, attitudes, practices and perceptions on COVID-19 among university students in Bangladesh. J Contemp Stud Epidemiol Public Health. (2021). doi: 10.30935/jconseph/9366. [Epub ahead of print].
33. Roy D, Ghosh TK, Saha M, Sarker S. Assessing knowledge, attitude, and practice towards COVID-19 among sub assistant agriculture officers: an empirical study in Bangladesh. J Contemp Stud Epidemiol Public Health. (2020) 1:ep20009. doi: 10.30935/jconseph/9364
34. Akram A, Molla MMA, Yeasmin M, Nafisa T, Monir MBB, Islam J, et al. Knowledge, attitude and practices toward COVID-19 among healthcare workers in National Institute of Laboratory Medicine and Referral Center, Dhaka, Bangladesh. Microbes Infect Dis. (2021) 2:433–9. doi: 10.21608/mid.2021.68809.1134
35. Zhang N, Zhou H, Huang D-S, Guan P. Brucellosis awareness and knowledge in communities worldwide: a systematic review and meta-analysis of 79 observational studies. PLoS Negl Trop Dis. (2019) 13:e0007366. doi: 10.1371/journal.pntd.0007366
36. John K, Kazwala R, Mfinanga GS. Knowledge of causes, clinical features and diagnosis of common zoonoses among medical practitioners in Tanzania. BMC Infect Dis. (2008) 8:162. doi: 10.1186/1471-2334-8-162
37. Siam MHB, Hasan MM, Tashrif SM, Khan MHR, Raheem E, Hossain MS. Insights into the first seven-months of COVID-19 pandemic in Bangladesh: lessons learned from a high-risk country. Heliyon. (2021) 7:e07385. doi: 10.1016/j.heliyon.2021.e07385
Keywords: COVID-19 knowledge, COVID-19 preventive behaviors, knowledge, attitudes, practice (KAP), pandemic, systematic review and meta-analysis
Citation: Raquib A, Raquib R, Jamil S, Hossain A, al-Mamun F and Mamun MA (2022) Knowledge, Attitudes, and Practices Toward the Prevention of COVID-19 in Bangladesh: A Systematic Review and Meta-Analysis. Front. Med. 9:856156. doi: 10.3389/fmed.2022.856156
Received: 16 January 2022; Accepted: 26 April 2022;
Published: 06 June 2022.
Edited by:
Abu Reza Md. Towfiqul Islam, Begum Rokeya University, BangladeshReviewed by:
Leeberk Raja Inbaraj, National Institute of Research in Tuberculosis (ICMR), IndiaMd Hasinur Rahaman Khan, University of Dhaka, Bangladesh
Copyright © 2022 Raquib, Raquib, Jamil, Hossain, al-Mamun and Mamun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohammed A. Mamun, bWFtdW5waGk0NkBnbWFpbC5jb20=
†ORCID: Ahmed Hossain orcid.org/0000-0003-4575-1273
Firoj al-Mamun orcid.org/0000-0003-4611-9624
Mohammed A. Mamun orcid.org/0000-0002-1728-8966