
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Med. , 15 June 2022
Sec. Infectious Diseases – Surveillance, Prevention and Treatment
Volume 9 - 2022 | https://doi.org/10.3389/fmed.2022.855639
This article is part of the Research Topic Inflammation and Organic Damage in COVID-19: What Have We Learned 2 Years Into the Pandemic? View all 12 articles
 Emilia Roy-Vallejo1*‡
Emilia Roy-Vallejo1*‡ Laura Cardeñoso2‡
Laura Cardeñoso2‡ Ana Triguero-Martínez3Marta Chicot Llano4
Ana Triguero-Martínez3Marta Chicot Llano4 Nelly Zurita2
Nelly Zurita2 Elena Ávalos5Ana Barrios1Julia Hernando6Javier Ortiz7Sebastián C. Rodríguez-García3
Elena Ávalos5Ana Barrios1Julia Hernando6Javier Ortiz7Sebastián C. Rodríguez-García3 Marianela Ciudad Sañudo1
Marianela Ciudad Sañudo1 Celeste Marcos5
Celeste Marcos5 Elena García Castillo5Leticia Fontán García-Rodrigo2Begoña González4
Elena García Castillo5Leticia Fontán García-Rodrigo2Begoña González4 Rosa Méndez6Isabel Iturrate7
Rosa Méndez6Isabel Iturrate7 Ancor Sanz-García8Almudena Villa1Ana Sánchez-Azofra5Begoña Quicios4
Ancor Sanz-García8Almudena Villa1Ana Sánchez-Azofra5Begoña Quicios4 David Arribas6
David Arribas6 Jesús Álvarez Rodríguez1Pablo Patiño4Marina Trigueros4
Jesús Álvarez Rodríguez1Pablo Patiño4Marina Trigueros4 Miren Uriarte3Alexandra Martín-Ramírez2Cristina Arévalo Román1
Miren Uriarte3Alexandra Martín-Ramírez2Cristina Arévalo Román1 José María Galván-Román1
José María Galván-Román1 Rosario García-Vicuña3
Rosario García-Vicuña3 Julio Ancochea5
Julio Ancochea5 Cecilia Muñoz-Calleja9
Cecilia Muñoz-Calleja9 Elena Fernández-Ruiz10
Elena Fernández-Ruiz10 Rafael de la Cámara7Carmen Suárez Fernández1
Rafael de la Cámara7Carmen Suárez Fernández1 Isidoro González-Álvaro3§Diego A. Rodríguez-Serrano4†§ and the PREDINMUN-COVID Group
Isidoro González-Álvaro3§Diego A. Rodríguez-Serrano4†§ and the PREDINMUN-COVID GroupBackground: Interleukin 6 (IL6) levels and SARS-CoV-2 viremia have been correlated with COVID-19 severity. The association over time between them has not been assessed in a prospective cohort. Our aim was to evaluate the relationship between SARS-CoV-2 viremia and time evolution of IL6 levels in a COVID-19 prospective cohort.
Methods: Secondary analysis from a prospective cohort including COVID-19 hospitalized patients from Hospital Universitario La Princesa between November 2020 and January 2021. Serial plasma samples were collected from admission until discharge. Viral load was quantified by Real-Time Polymerase Chain Reaction and IL6 levels with an enzyme immunoassay. To represent the evolution over time of both variables we used the graphic command twoway of Stata.
Results: A total of 57 patients were recruited, with median age of 63 years (IQR [53–81]), 61.4% male and 68.4% Caucasian. The peak of viremia appeared shortly after symptom onset in patients with persistent viremia (more than 1 sample with > 1.3 log10 copies/ml) and also in those with at least one IL6 > 30 pg/ml, followed by a progressive increase in IL6 around 10 days later. Persistent viremia in the first week of hospitalization was associated with higher levels of IL6. Both IL6 and SARS-CoV-2 viral load were higher in males, with a quicker increase with age.
Conclusion: In those patients with worse outcomes, an early peak of SARS-CoV-2 viral load precedes an increase in IL6 levels. Monitoring SARS-CoV-2 viral load during the first week after symptom onset may be helpful to predict disease severity in COVID-19 patients.
One of the most feared complications of the disease caused by the coronavirus SARS-CoV-2 (COVID-19), is the development of an Acute Respiratory Distress Syndrome (ARDS), which can affect 15.6–31% of patients (1). Siddiqui and Mehra (2) proposed that ARDS is part of the final stage of the disease, in which clinical features are mainly the consequence of the host hyperinflammatory response and a cytokine storm; whereas the stage I (early infection) is mainly caused by viral replication and the early immune response. However, to the best of our knowledge, this proposal has not been validated.
Since the outbreak of the COVID-19 pandemic, many efforts have been made to find early risk factors and biomarkers able to predict the evolution toward the cytokine storm. In this sense, older age, obesity and comorbidities such as hypertension, diabetes and coronary heart disease have been associated with higher risk of death (3, 4). On the other hand, increased levels of C reactive protein (CRP), lactate dehydrogenase (LDH), and D-dimer, among others, have been shown to be related to the development of ARDS and mortality (3, 5, 6).
In this context, Interleukin 6 (IL6) has been described as one of the most useful biomarkers (7). In a previous work, we showed that IL6 could be a severity biomarker but also a guide to select COVID-19 patients who could benefit from treatment with tocilizumab, an inhibitor of the IL6 receptor (8). Another important biomarker is the presence of SARS-CoV-2 RNA in peripheral blood (viremia), which has been associated with disease severity and a hyperinflammatory state (9, 10). Saji et al. (11) showed that the combination of SpO2/FiO2, IL6 and the presence of SARS-CoV-2 viremia at admission had the highest accuracy to predict fatal outcomes. Bermejo et al. (12) and Myhre et al. (13) found that the presence of SARS-CoV-2 viremia at admission correlated with increased levels of IL6, CRP, and ferritin. In addition, a proteomic analysis showed that the expression of viral response and interferon/monocytic pathway proteins such as IL6 and one of its regulators, the Nicotinamide phosporibosyl transferase (NAMPT), were upregulated in patients with quantifiable SARS-CoV-2 viremia at admission, compared to those with undetectable viremia (14).
In a previous study of our group, we found that viremia was associated with Intensive Care Unit (ICU) admission and in-hospital death, and it was a better biomarker than IL6 (10). In this regard, since SARS-CoV-2 infection is involved in triggering IL6 expression, viremia as an indicator of the systemic viral shedding, could be related with the IL6 response and be useful as an early biomarker (phase of viral response). Nevertheless, the factors determining an IL6 increase in COVID-19 patients have not been well established yet and the association over time between SARS-CoV-2 viremia and IL6, has not been assessed in a prospective cohort with serial samples.
Considering our previous results, the aim of this study was to evaluate the relationship between the presence of SARS-CoV-2 viremia and the time evolution and IL6 levels in a prospective cohort of COVID-19 hospitalized patients.
This work is a secondary analysis of samples from a prospective observational cohort assembled to validate the predictive value of SARS-CoV-2 viremia (ongoing manuscript). The study included patients hospitalized for COVID-19 in Hospital Universitario La Princesa (HUP) between November 1st 2020 and January 15th 2021.
The inclusion criteria were: (a) positive Real-Time Reverse Transcription Polymerase Chain Reaction (rRT-PCR) for SARS-CoV-2 in nasopharyngeal and throat swabs at most 48 h prior to hospitalization; (b) acceptance to participate in the study and oral or written consent; (c) age older than 18 years. The exclusion criteria were: (a) patients without an initial viremia determination in the first 24–36 h after admission; (b) patients unlikely to be followed-up because they were candidates to be transferred to other health facilities.
Clinical, laboratory and therapeutic data were collected from electronic clinical records and included in an anonymized database. Baseline clinical and laboratory data are to those obtained at admission day.
The need for hospitalization was decided by the physicians at the emergency room based on clinical criteria, without the intervention of the research team. Patient’s treatment and management was decided by each attending physician based on the hospital protocols and their clinical judgment. Attending physicians were blind to the viremia results.
The sample size was estimated in 49 patients to validate the primary objective of the study “SARS-CoV-2 viremia as a biomarker of disease severity” (ongoing manuscript) based on the results of our previous retrospective studies (10, 15); nevertheless, 57 patients were finally included.
Serial plasma and serum samples were collected from admission until discharge. In the first week, samples were collected every 48 h, with the first sample in the first 24–36 h. Thereafter, samples were collected twice a week. All samples were frozen at –80°C and stored in the Microbiology Department facilities.
Firstly, a nucleic acid extraction of samples was performed by the automatic eMAG® Nucleic Acid Extraction System (Biomerieux, France). Detection of viremia was performed with rRT-PCR using TaqPath™ COVID-19 CE81 IVD RT-PCR Kit [Thermo Fisher Scientific, United States (TFS)], according to the manufacturer’s instructions, by a QuantStudio™ 5 Real Time PCR System (Applied Biosystems, United States). Amplification curves were analyzed with QuantStudio™ Design and Analysis software version 2.4.3 (Applied Biosystems, United States) and interpreted by a clinical microbiologist. To increase sensitivity, two wells were used for each sample. Two positive controls (one of 20,000 copies and another of 200 copies) and two negative controls were added in each run in duplicate.
A standard curve was established using a positive control with a known concentration (TaqPath Positive Control from TaqPath™ COVID-19 Control Kit) of 10,000 copies/μl of the SARS-CoV-2 genomic regions targeted by the TFS assay. Ten-fold serial dilutions of the positive control were made up to 1 copy. Nine wells of each of the concentrations and of the negative control were added to the run. The rRT-PCR was performed by QuantStudio™ 5 Real Time PCR System and a standard curve was obtained plotting DNA concentration against cycle threshold (Ct) values. The amplification curves were analyzed with QuantStudio™ Design and Analysis software version 2.4.3 (Applied Biosystems, United States). The results of the nine wells with 1 copy were omitted because they were widely dispersed.
Viral load was calculated from Ct values using the standard curve as reference and was expressed as copies/ml and the logarithm with base 10 (log10). Due to the variability and lack of accuracy obtained with the lower levels of SARS-CoV-2 viremia, only viremias > 1.3 log10 (20 copies/ml) were considered quantifiable.
Serum samples collected in the same extraction as the plasma used for SARS-CoV-2 viremia determinations were used to assess IL6 levels. IL6 levels were retrospectively quantified in triplicate with the Human IL6 Duoset enzyme-immunoassay from R&D Systems Europe Ltd. (Abingdon, United Kingdom), following the manufacturer’s instructions.
For analysis using viremia as a quantitative variable, all values were used. However, to define viremia as categorical, positive viremia was considered when values were higher than 1.3 log10 (namely 20 copies/ml, which was the threshold for quantifiable viremia) and negative when values were below this threshold. Persistent viremia was defined as more than one positive viremia in the first week of hospitalization.
Two different variables were used to evaluate IL6 levels: (a) a quantitative variable defined as IL6 concentration, expressed in pg/ml, (b) a dichotomic variable, which considered levels of IL6 as high when at least one IL6 determination was higher than 30 pg/ml or low if all determinations were below 30 pg/ml. This threshold was based on our previous study, where we showed that IL6 > 30 pg/ml was associated with poor respiratory outcomes (8). The average levels of IL6 and viral load were defined as the arithmetic mean of all their determinations in each patient.
We used Stata 14.0 for Windows (Stata Corp. LP, College Station, TX, United States) for all the analysis described below. Quantitative variables were represented as median and Interquartile Range (IQR), and the Mann Whitney or Kruskall Wallis tests were used to assess significant differences, since all quantitative variables followed a non-normal distribution. Qualitative variables were described as counts and proportions and Chi square or Fisher’s exact test was used for comparisons.
In order to comparatively show levels of IL6 and viral load through the two first weeks of follow-up, we used as time variable the number of days from the beginning of symptoms to collection of each sample. To represent the mean evolution over time of both variables we used the graphic command twoway from Stata with the option fractional polynomial prediction with 95% confidence interval (CI). Since it is well known that blockade of IL6 receptor with tocilizumab can result in an increase of IL6 serum levels (16), we decided to carry forward the last observation before tocilizumab treatment [last observation carried forward (LOCF) strategy] to replace IL6 values in the remaining visits of the first 2 weeks for those patients treated with tocilizumab in order to avoid the bias of excluding this important population (see comparative baseline characteristics in Supplementary Table 1). Furthermore, we also applied LOCT strategy for those patients who died or were discharged before the 5th visit (14th day after admission), in order to obtain a more homogeneous number of determinations all along the follow-up.
To determine which variables were associated with high levels of IL6, we performed a multivariable logistic regression analysis that was first modeled by adding all the variables with a p-value lower than 0.15 in the bivariable analysis. The final model was reached through backward stepwise removal of variables with p-value higher than 0.15.
This study was approved by the Research Ethics Committee of Hospital Universitario La Princesa, Madrid (register number 4267; 22-10-2020), and it was carried out following the ethical principles established in the Declaration of Helsinki. As proposed by AEMPS (Agencia Española de Medicamentos y Productos Sanitarios, The Spanish Agency for Medicines and Medical Devices), only oral consent was required due to the COVID-19 emergency (17). However, a written information sheet was also offered to all patients. After being informed about the study, all included patients (or their representatives) gave informed consent, which was registered in the electronic clinical chart.
This article was written following the STROBE initiative (Strengthening the Reporting of Observational studies in Epidemiology).
A total of 57 patients were recruited, with median age of 63 years (IQR 53–81), 61.4% were male, 68.4% Caucasian, and 75.4% had previous comorbidities. The median time from symptom onset to first sample was 8 days (IQR 4–10). Baseline clinical characteristics according to IL6 levels are shown in Table 1. During patients’ hospitalization, 301 serum samples were collected, with a median number of 3 samples per patient (IQR 2-5).
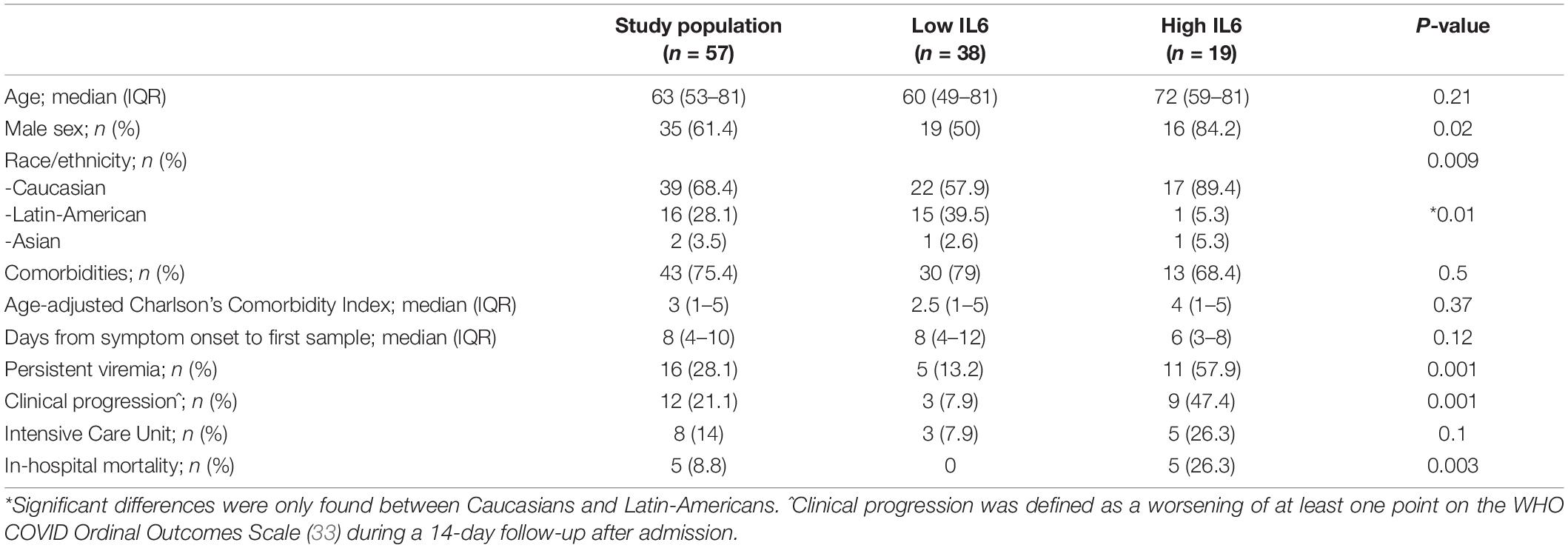
Table 1. Baseline clinical characteristics of the study population according to IL6 levels.
Nine patients were treated with tocilizumab, who on average, showed data suggesting a more severe disease, although differences did not reach statistical significance (Supplementary Table 1).
Most patients who progressed to a severe disease started this evolution 7–14 days after the symptoms onset. In addition, patients with a more benign course were discharged at the end of the first week after admission. For clinical consistency, we decided to analyze only the samples corresponding to the first 2 weeks of hospitalization, a maximum of 5 samples per patient. Thus, IL6 levels were measured in 228 samples, with a median of 3.6 pg/ml (IQR 0–21 pg/ml). Baseline clinical characteristics of patients depending on IL6 status are shown in Table 1. SARS-CoV-2 viremia was determined in 234 samples, with the highest percentage of positive viremia (36.8%) at admission (visit 1).
The average serum levels of IL6 and SARS-CoV-2 viral load were moderately but significantly correlated (r = 0.41, p = 0.0014; Supplementary Figure 1).
Figure 1A shows the evolution over time of IL6 and viremia analyzed using data from the whole population (including IL6 after tocilizumab treatment). The peak of viremia appeared early, at the first days after symptom onset (day 3–5), and quickly decreased. On the other hand, the highest levels of IL6 were found at day 20. The wide 95% CI suggested a high heterogeneity, especially at both extremes of the time course. Figure 1B shows the results when the LOCF strategy (see Statistical section for further information) was used to minimize the increase of IL6 induced by tocilizumab (see Supplementary Figure 2 for raw data in cases treated or not with tocilizumab). With LOCF strategy, the peak of IL6 was smaller, but the time course of IL6 production was quite similar to that obtained from raw data. Hereinafter, the relationship between IL6 and SARS-CoV2 viral load shown corresponds to results obtained with the LOCF strategy.
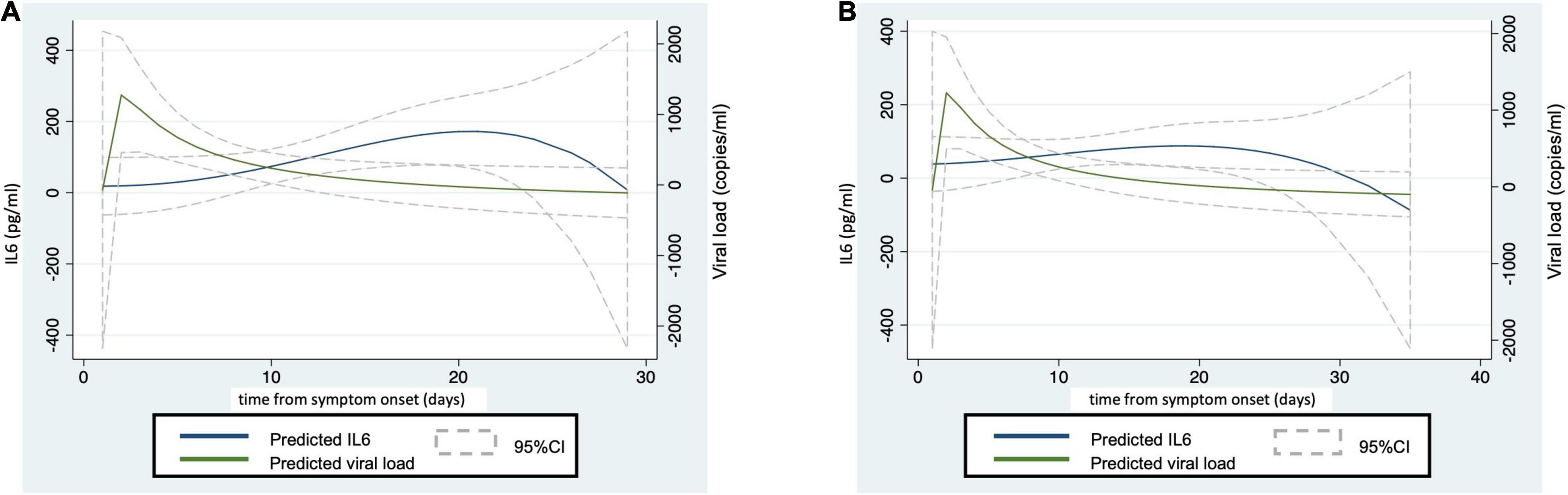
Figure 1. The peak of viral load precedes the IL6 increase. Graphic representation of time-course of IL6 levels and SARS-CoV-2 viral load from symptom onset. (A) representation of raw data. (B) Representation of data after applying the LOCF strategy. The fractional polynomial prediction was performed using the twoway command of Stata.
A total of 19 patients had high IL6 (Table 1), of them 11 (57.9%) had persistent viremia compared to 5 patients (13.2%) in the low IL6 group (p = 0.001), with an odds ratio of 9.1 (95%CI 2.5–32.6) (Figure 2E). In the graphic representation of IL6 and viral load according to high/low IL6 (Figures 2A,B), an early and minor peak of IL6 was found in the low IL6 group, together with a small peak of viremia at day 4. On the other hand, patients with at least one IL6 above 30 pg/ml had an early high viremia around day 3 and a progressive increase of IL6 especially after day 12.
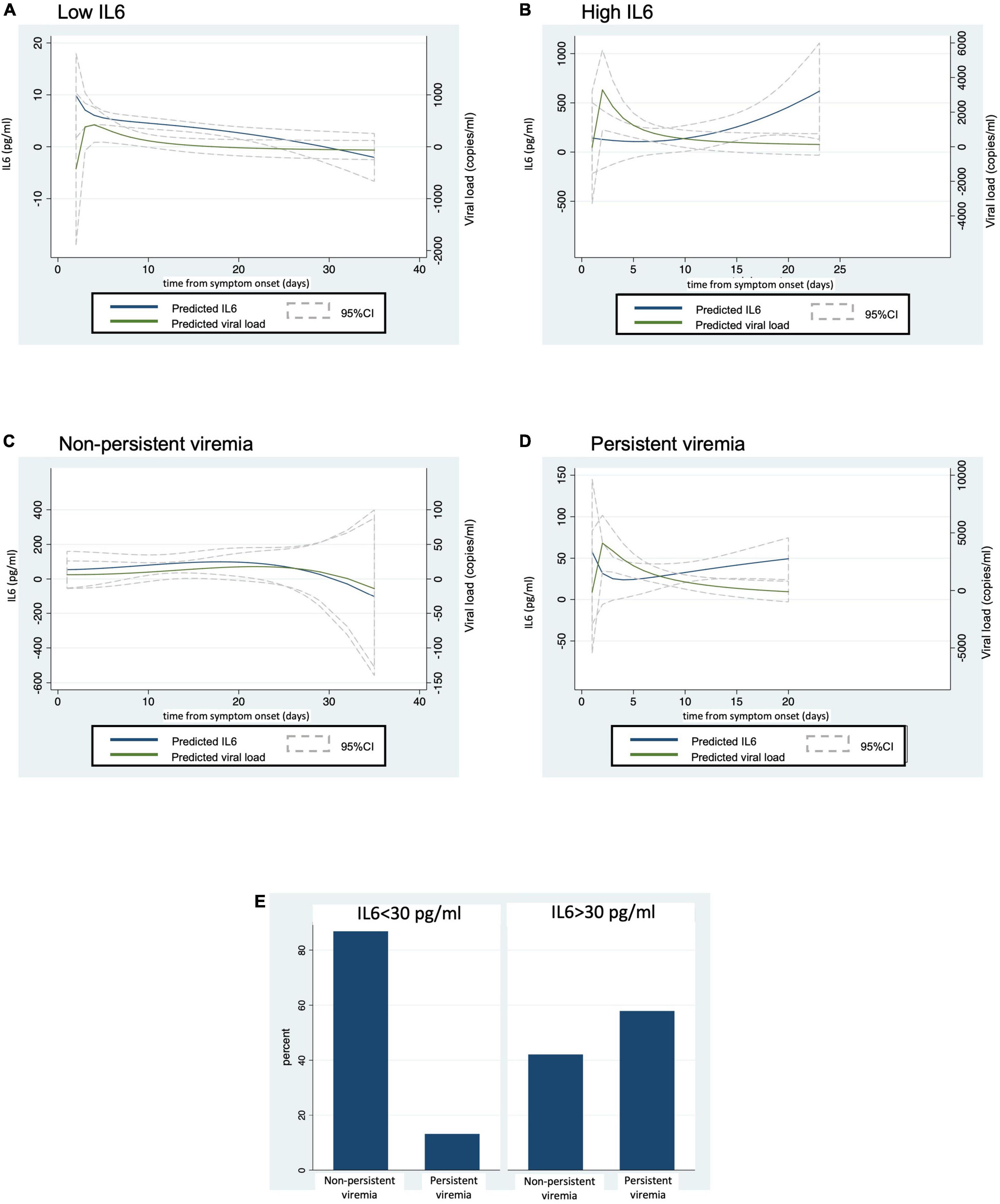
Figure 2. Patients with worse outcomes have an early peak of SARS-CoV-2 viral load before a prominent increase in IL6 levels. Graphic representation of IL6 levels and SARS-CoV-2 viral load from symptom onset in: (A) patients with low IL6; (B) patients with at least one IL6 > 30 pg/ml (high IL6); (C) non-persistent viremia; and (D) persistent viremia. (E) Represents the percentage of patients with persistent viremia according to IL6 levels (low vs. high). (A–D) The fractional polynomial predictions were performed using the twoway command of Stata.
When the prediction of IL6 and viral load was calculated according to persistent viremia status, remarkable differences were obtained (Figures 2C,D). In the persistent viremia group, viral load showed a peak around day 4, whereas IL6 had a two-phase increase: one at the first days from symptom onset and then a subsequent progressive increase after day 5. Regarding non-persistent viremia the increase of IL6 was slow from symptom onset until day 20. The median of the average levels of IL6 were 3.6 pg/ml (IQR 1.0–9.2 pg/ml) in the non-persistent viremia group and 21.4 pg/ml (IQR 12.3–44.9) in patients with persistent viremia (p < 0.001).
The effect of demographic factors on IL6 levels and SARS-CoV-2 viremia was also assessed. The median of the average IL6 concentration was significantly higher in males (11.3 pg/ml [IQR 3.3–27.5] than in females (2.5 pg/ml [IQR 0.7–9.2 pg/ml]; p = 0.005). In the group of patients with high IL6, 84.2% were male compared to 50% in the group with low IL6 (p = 0.02). No differences were found in the average viral load (11.1 copies/ml [IQR 0–197.3 copies/ml] vs. 2.3 copies/ml [IQR 0–6.8 copies/ml]; p = 0.08) or in the percentage of patients with persistent viremia (34.3% vs. 18.2%; p = 0.24) between males and females, respectively. However, predicting curves for IL6 and viral load were substantially different depending on sex (Figure 3A). In males, curves had a fast increase in viral load with a peak around day 2 from symptom onset and a later rise in IL6 levels until day 20, while women showed a small increase in viral load and IL6 between day 2 and 7 approximately.
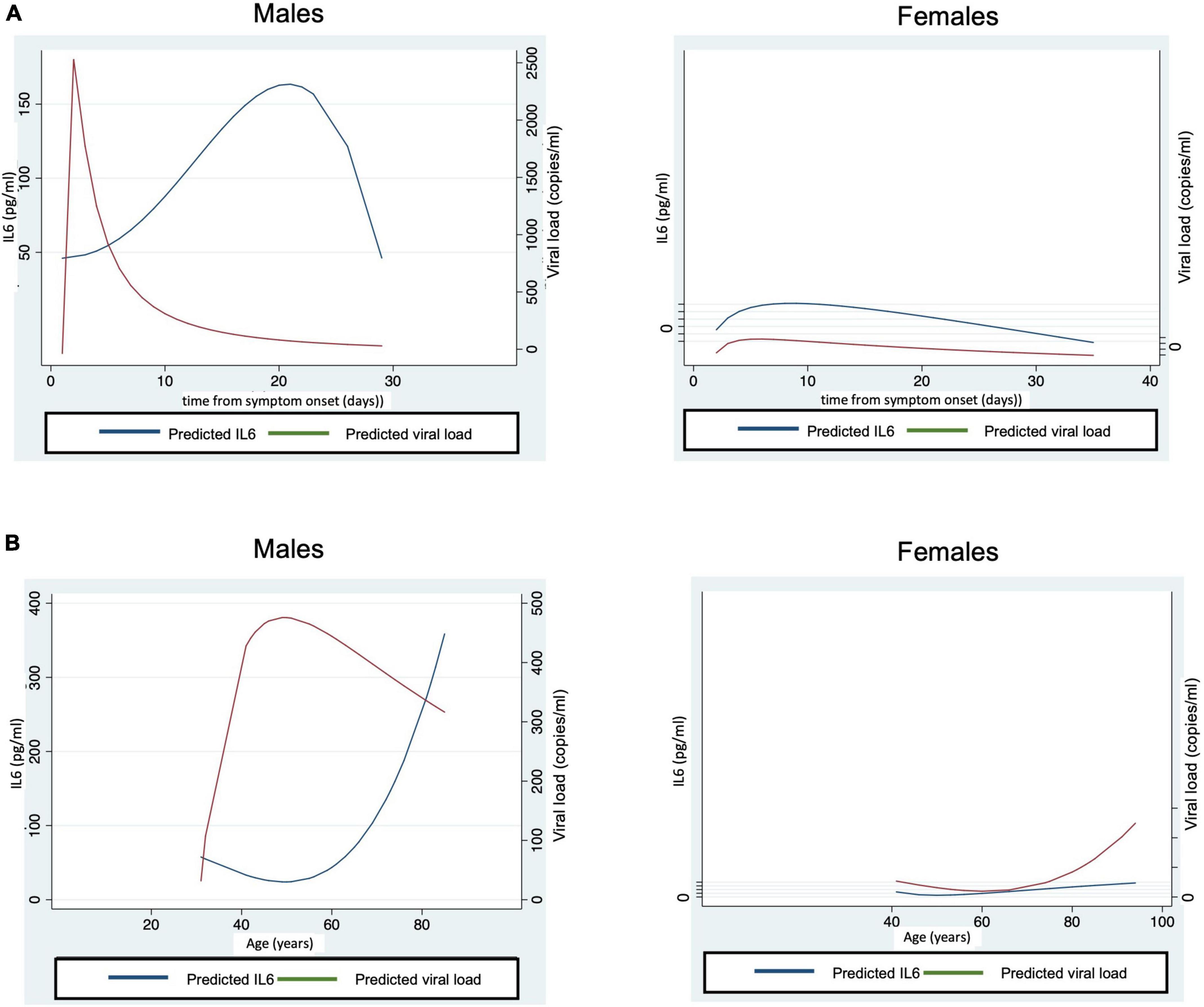
Figure 3. Males had more relevant increases of IL6 and viral load. (A) Represents the levels of IL6 and viral load from symptom onset by sex (both panels using the same scale), while (B) shows levels of IL6 and viral load by age and sex (both panels using the same scale). The fractional polynomial predictions were performed using the twoway command of Stata.
The effect of age on IL6 levels and viral load was also considered. The average levels of IL6 and viremia did not correlate with age (r = 0.21, p = 0.13; and r = 0.19, p = 0.16; respectively). Moreover, no differences were found when age was categorized as < 75 years and > 75 years (p = 0.57 and p = 0.88, for IL6 and viral load, respectively). In the group with high IL6, 31.6% of patients were older than 75 years, the same percentage as in the low IL6 group (p = 1). Regarding persistent viremia, the proportion of patients older than 75 years was 29.3% in the group with non-persistent viremia and 37.5% in those with persistent viremia (p = 0.55). In the prediction curves according to age and sex, all parameters increased with age except for viral load in males, which peaked between 40 and 50 years (Figure 3B).
Regarding ethnicity, there were only differences between Caucasians and Latin-Americans in the average IL6 levels (11.9 [IQR 2.9–35.2] vs. 2.9 [IQR 1.0–4.3]; p = 0.005), and the percentage of patients with high IL6 (89.5% vs. 5.3%, p = 0.01) (Table 1). No differences were found depending on ethnicity in the average viral load or the percentage of patients with persistent viremia.
Finally, a multivariable analysis showed that the presence of high IL6 was associated with persistent viremia (OR 10.0 [95%CI 2.0–49.5]; p = 0.005); conversely, female sex (OR 0.17 [0.03–0.9]; p = 0.04) and Latin-American origin (OR 0.06 [0.01–0.7]; p = 0.02) had a protective effect.
This study assessed the relationship between IL6 and SARS-CoV-2 viremia. The most relevant finding was the different time course of IL6 and viremia: the peak of viremia appeared shortly after symptom onset in patients with persistent viremia and also in those with at least one measure of IL6 > 30 pg/ml, in which it was followed days later by a progressive increase in IL6. Moreover, the presence of persistent viremia in the first week of hospitalization was associated with higher levels of IL6. Both IL6 and SARS-CoV-2 viral load were higher in males, with a progressive increase with age that occurred earlier in males.
Our findings are consistent with the COVID-19 phases first described by Siddiqui and Mehra (2). These authors described an early stage characterized by a viral response (SARS-CoV-2 viremia) and a final stage caused by a hyperinflammatory state characterized by increased levels of IL6. To date, only two studies have evaluated SARS-CoV-2 viremia and systemic cytokines in a longitudinal design, but none of them considered the different time course of the increase in viremia and IL6 (18, 19). Van Riel et al. (18) only included 20 patients and found that the levels of IL6 were associated with critical disease but not with the presence of viremia; while Brasen et al. (19) found and association between maximum viral load and IL6. Neither of them assessed the temporal course of both biomarkers. In our previous work (10), we described that the presence of relevant SARS-CoV-2 viremia was associated with higher risk of death and ICU admission. Furthermore, viremia was the most useful biomarker for these outcomes, being superior to IL6, lymphopenia and LDH. In the present study, we show that the SARS-CoV-2 viremia appears early in the course of the disease, standing out as a relevant, simple and early biomarker.
Since the beginning of the pandemic, CRP, and IL6 levels have been used as prognostic biomarkers in COVID-19; in addition, IL6 activity has been targeted for treatment by the anti-IL-6 receptor antibody but also to guide treatment and predict response to tocilizumab (8, 20, 21). Moreover, a previous study of our group showed that high levels of IL6 (above 30 pg/ml) were associated with worse prognosis of COVID-19, and also with a better response to tocilizumab, thereby suggesting a role of IL6 levels in guiding treatment and predicting response to this therapeutic agent (8). However, Ong et al. (22) and Liu et al. (23) showed that IL6 in COVID-19 patients peaked after the worsening of respiratory function, suggesting that when proinflammatory biomarkers rise, lung damage might be already established. In our cohort, 68.8% of patients with persistent viremia had at least one IL6 > 30 pg/ml in the later hyperinflammatory phase of the disease. Taking into account the high percentage of patients with persistent viremia who develop an hyperinflammatory response, these patients might be considered as candidates for intensive treatment and surveillance, or even for early treatment with IL6 blockade.
Nevertheless, these findings might not be extensive to all patients. A more severe course of COVID-19 and higher levels of IL6 have been previously described in older males (24). In this sense, genetic and hormonal factors have been proposed to be involved in age and sex related differences in COVID-19 (24, 25). One of the most studied SARS-CoV-2 related proteins is ACE2, the membrane receptor needed for the virus internalization, which is encoded by the gen of the same name located in the X chromosome (25, 26). ACE2 expression increases with age and in male sex in COVID-19 patients (27, 28). ACE2 expression also correlates with SARS-CoV-2 infectivity in cells of the respiratory tract (29) and with higher viral loads in nasopharyngeal swabs (30). Whether endothelial and vascular ACE2 is related to viral load in peripheral blood has not been assessed yet, but it is plausible that higher levels of systemic ACE2 lead to increased viremia. Another proposed mechanism to explain sex differences is the effect of Toll Like Receptor (TLR) pathways, especially TLR7. This receptor, which recognizes viral single strain RNA and enhances IL6 production, is also located in X chromosome. TLR7 was one of the most important susceptibility genes found in an Italian cohort of COVID-19 patients, where 6.3% of young males with life-threatening disease presented missense variants of this gene (31).
Regarding ethnicity, patients with a Latin-American origin had lower levels of IL6 in our cohort. In this sense, other cytokines and chemokines such as MCP-1, IL-10, IL-15, CXCL10, and CCL2 have been associated with SARS-CoV-2 viremia (12, 18). It is possible that the immune response of COVID-19 patients is enhanced by molecular pathways different from IL6, which may play a relevant role in patients without an IL6 increase. However, this hypothesis needs to be further evaluated with studies with bigger sample size than our cohort.
This study has several limitations. First of all, the sample size of our cohort was small, although it was sufficient to find different patterns in the kinetics of IL6 and viral load. Secondly, all patients included were hospitalized and their first sample was obtained at a median of 7 days after symptom onset, therefore, data from the first days of the disease were limited. In addition, information about different variants of SARS-CoV-2 in our cohort could not be obtained because viral sequencing was not available in our facilities. However, at the time our study was performed, the most prevalent variant in Madrid was the original strain (32).
In conclusion, in those patients with worse outcomes, an early peak of SARS-CoV-2 viral load precedes around 5–10 days a prominent increase in IL6 levels. This finding was very clear in males older than 40 years. Therefore, monitoring SARS-CoV-2 viral load during the first week after symptom onset may be helpful to stratify the severity of patients and predict those who are at high risk of developing hyperinflammatory syndrome and ARDS.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Research Ethics Committee of Hospital Universitario La Princesa, Madrid. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
ER-V, LC, IG-A, and DR-S designed the study and wrote the first draft of the manuscript. MCL, EÁ, AB, JH, JO, SR-G, MCS, CM, EG, BG, RM, II, AV, AS-A, DA, JÁ, PP, MT, MU, JG-R, RG-V, JA, RC, and CS included patients in the study and collected data. BQ, CA, CM-C, and EF-R extracted and processed samples. ER-V, AT-M, NZ, AM-R, and LF performed laboratory determinations. ER-V, AS-G, and IG-A analyzed the data. All authors reviewed the final draft.
This study was funded with grants: “Fondos Supera COVID19” by Banco Santander and CRUE to CS, RG-V, CM-C, and JÁ; RD16/0011/0012 and PI18/0371 to IG, from Ministerio de Economía y Competitividad (Instituto de Salud Carlos III) and co-funded by European regional development fund (ERDF) “A way to make Europe”; and co-financed by the Community of Madrid through the COVID-2019 Aid. The work of ER-V has been funded by a Rio-Hortega grant CM19/00149 from the Ministerio de Economía y Competitividad (Instituto de Salud Carlos III) and co-funded by the European Regional Development Fund (ERDF) “A way to make Europe.” SR-G was funded by the Spanish Rheumatology Foundation (grants for physicians-researchers 2018–2021). None of these sponsors have had any role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank our patients and relatives for agreeing with the use of pseudonymized clinical data and surpluses of clinical samples to perform this study, and Manuel Gomez Gutierrez, for his excellent editing assistance.
Internal Medicine-Infectious Diseases: Jesús Sanz1, Pedro Casado1, Ángela Gutiérrez1, Azucena Bautista1, Pilar Hernández1, Nuria Ruiz Giménez1, Berta Moyano1, Paloma Gil1, María Jesús Delgado1, Pedro Parra1, Beatriz Sánchez1, Carmen Sáez1, Marta Fernández Rico1.
Microbiology: Diego Domingo García2, Teresa Alarcón Cavero2, María Auxiliadora Semiglia Chong2, Ainhoa Gutiérrez Cobos2.
Rheumatology: Santos Castañeda3, Irene Llorente3, Eva G. Tomero3, Noelia García Castañeda3, Nuria Montes3.
Intensive Care Unit: Cristina Dominguez Peña4, David Jiménez Jiménez4, Pablo Villamayor4, Alfonso Canabal4.
Pneumology: Tamara Alonso5, Carolina Cisneros5, Claudia Valenzuela5, Francisco Javier García Pérez5, Rosa María Girón5, Javier Aspa5, Celeste Marcos5, M. del Perpetuo Socorro Churruca5, Enrique Zamora5, Adrián Martínez5, Mar Barrio Mayo5, Rosalina Henares Espi5.
Immunology: Francisco Sánchez-Madrid9, Enrique Martín Gayo9, Ildefonso Sánchez-Cerrillo9, Ana Marcos Jimenez9, Pedro Martínez-Fleta9, Celia López-Sanz9, Ligia Gabrie9, Luciana del Campo Guerola9, Reyes Tejedor9, Molecular Biology: Rosa Carracedo Rodríguez10.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2022.855639/full#supplementary-material
1. Li X, Ma X. Acute respiratory failure in COVID-19: is it “typical” ARDS? Crit Care. (2020) 24:198. doi: 10.1186/s13054-020-02911-9
2. Siddiqi HK, Mehra MR. COVID-19 illness in native and immunosuppressed states: a clinical-therapeutic staging proposal. J Heart Lung Transpl. (2020) 39:405–7. doi: 10.1016/j.healun.2020.03.012
3. Tian W, Jiang W, Yao J, Nicholson CJ, Li RH, Sigurslid HH, et al. Predictors of mortality in hospitalized COVID-19 patients: a systematic review and meta-analysis. J Med Virol. (2020) 92:1875–83. doi: 10.1002/jmv.26050
4. Gallo Marin B, Aghagoli G, Lavine K, Yang L, Siff EJ, Chiang SS, et al. Predictors of COVID -19 severity: a literature review. Rev Med Virol. (2021) 31:1–10. doi: 10.1002/rmv.2146
5. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. (2020) 395:1054–62. doi: 10.1016/S0140-6736(20)30566-3
6. Zhang JJY, Lee KS, Ang LW, Leo YS, Young BE. Risk factors for severe disease and efficacy of treatment in patients infected with COVID-19: a systematic review, meta-analysis, and meta-regression analysis. Clin Infect Dis. (2020) 71:2199–206. doi: 10.1093/cid/ciaa576
7. Mesas AE, Cavero-Redondo I, Álvarez-Bueno C, Sarriá Cabrera MA, Maffei de Andrade S, Sequí-Dominguez I, et al. Predictors of in-hospital COVID-19 mortality: a comprehensive systematic review and meta-analysis exploring differences by age, sex and health conditions. PLoS One. (2020) 15:e0241742. doi: 10.1371/journal.pone.0241742
8. Galván-Román JM, Rodríguez-García SC, Roy-Vallejo E, Marcos-Jiménez A, Sánchez-Alonso S, Fernández-Díaz C, et al. IL-6 serum levels predict severity and response to Tocilizumab in COVID-19: an observational study. J Allergy Clin Immunol. (2020) 147:72.e–80.e. doi: 10.1016/j.jaci.2020.09.018
9. Tang K, Wu L, Luo Y, Gong B. Quantitative assessment of SARS-CoV-2 RNAemia and outcome in patients with coronavirus disease 2019. J Med Virol. (2021) 93:3165–75. doi: 10.1002/jmv.26876
10. Rodríguez-Serrano DA, Roy-Vallejo E, Zurita Cruz ND, Martín Ramírez A, Rodríguez-García SC, Arevalillo-Fernández N, et al. Detection of SARS-CoV-2 RNA in serum is associated with increased mortality risk in hospitalized COVID-19 patients. Sci Rep. (2021) 11:13134. doi: 10.1038/s41598-021-92497-1
11. Saji R, Nishii M, Sakai K, Miyakawa K, Yamaoka Y, Ban T, et al. Combining IL-6 and SARS-CoV-2 RNAaemia-based risk stratification for fatal outcomes of COVID-19. PLoS One. (2021) 16:e0256022. doi: 10.1371/journal.pone.0256022
12. Bermejo-Martin JF, González-Rivera M, Almansa R, Micheloud D, Tedim AP, Domínguez-Gil M, et al. Viral RNA load in plasma is associated with critical illness and a dysregulated host response in COVID-19. Critic Care. (2020) 24:691. doi: 10.1186/s13054-020-03398-0
13. Myhre PL, Prebensen C, Jonassen CM, Berdal JE, Omland T. SARS-CoV-2 viremia is associated with inflammatory, but not cardiovascular biomarkers, in patients hospitalized for COVID-19. JAHA. (2021) 10:e019756. doi: 10.1161/JAHA.120.019756
14. Li Y, Schneider AM, Mehta A, Sade-Feldman M, Kays KR, Gentili M, et al. SARS-CoV-2 viremia is associated with distinct proteomic pathways and predicts COVID-19 outcomes. J Clin Investig. (2021) 131:e148635. doi: 10.1172/JCI148635
15. Martín Ramírez A, Zurita Cruz ND, Gutiérrez-Cobos A, Rodríguez Serrano DA, González Álvaro I, Roy Vallejo E, et al. Evaluation of two RT-PCR techniques for SARS-CoV-2 RNA detection in serum for microbiological diagnosis. J Virol Methods. (2022) 300:114411. doi: 10.1016/j.jviromet.2021.114411
16. Nishimoto N, Terao K, Mima T, Nakahara H, Takagi N, Kakehi T. Mechanisms and pathologic significances in increase in serum interleukin-6 (IL-6) and soluble IL-6 receptor after administration of an anti-IL-6 receptor antibody, tocilizumab, in patients with rheumatoid arthritis and Castleman disease. Blood. (2008) 112:3959–64. doi: 10.1182/blood-2008-05-155846
17. The Spanish Agency for Medicine and Health Products [Agencia Española de Medicamentos y Productos Sanitarios (AEMPS)]. Exceptional Measures Applicable to Clinical Trials to Manage Problems Arising from the COVID-19 Emergency. (2022). Available online at: https://www.aemps.gob.es/informa-en/exceptional-measures-applicable-to-clinical-trials-to-manage-problems-arising-from-the-covid-19-emergency/?lang=en (accessed January 11, 2022)
18. van Riel D, Embregts CWE, Sips GJ, van den Akker JPC, Endeman H, van Nood E, et al. Temporal kinetics of RNAemia and associated systemic cytokines in hospitalized COVID-19 patients. mSphere (2021) 6:e0031121. doi: 10.1128/mSphere.00311-21
19. Brasen CL, Christensen H, Olsen DA, Kahns S, Andersen RF, Madsen JB, et al. Daily monitoring of viral load measured as SARS-CoV-2 antigen and RNA in blood, IL-6, CRP and complement C3d predicts outcome in patients hospitalized with COVID-19. Clin Chem Lab Med. (2021) 59:1988–97. doi: 10.1515/cclm-2021-0694
20. The Spanish Agency for Medicine and Health Products - [Agencia Española de Medicamentos y Productos Sanitarios (AEMPS)]. Treatments Available for the Management of Respiratory Infection by SARS-CoV-2 - [Tratamientos Disponibles Para el Manejo de la Infección Respiratoria por SARS-CoV-2]. [Treatment Recommendations]. (2020). Available online at: https://www.aemps.gob.es/laAEMPS/docs/medicamentos-disponibles-SARS-CoV-2-16-4-2020.pdf (accessed April 17, 2020)
21. Abani O, Abbas A, Abbas F, Abbas M, Abbasi S, Abbass H, et al. Tocilizumab in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial. Lancet. (2021) 397:1637–45. doi: 10.1016/S0140-6736(21)00676-0
22. Ong EZ, Chan YFZ, Leong WY, Lee NMY, Kalimuddin S, Haja Mohideen SM, et al. A dynamic immune response shapes COVID-19 progression. Cell Host Microbe. (2020) 27:879.e–82.e. doi: 10.1016/j.chom.2020.03.021
23. Liu Z, Li J, Chen D, Gao R, Zeng W, Chen S, et al. Dynamic interleukin-6 level changes as a prognostic indicator in patients with COVID-19. Front Pharmacol. (2020) 11:1093. doi: 10.3389/fphar.2020.01093
24. Bonafè M, Prattichizzo F, Giuliani A, Storci G, Sabbatinelli J, Olivieri F. Inflamm-aging: why older men are the most susceptible to SARS-CoV-2 complicated outcomes. Cytokine Growth Factor Rev. (2020) 53:33–7. doi: 10.1016/j.cytogfr.2020.04.005
25. Rehman S, Ravinayagam V, Nahvi I, Aldossary H, Al-Shammari M, Amiri MSA, et al. Immunity, sex hormones, and environmental factors as determinants of COVID-19 disparity in women. Front Immunol. (2021) 12:680845. doi: 10.3389/fimmu.2021.680845
26. Zhang H, Penninger JM, Li Y, Zhong N, Slutsky AS. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: molecular mechanisms and potential therapeutic target. Intens Care Med. (2020) 46:586–90. doi: 10.1007/s00134-020-05985-9
27. Peng J, Sun J, Zhao J, Deng X, Guo F, Chen L. Age and gender differences in ACE2 and TMPRSS2 expressions in oral epithelial cells. J Transl Med. (2021) 19:358. doi: 10.1186/s12967-021-03037-4
28. Swärd P, Edsfeldt A, Reepalu A, Jehpsson L, Rosengren BE, Karlsson MK. Age and sex differences in soluble ACE2 may give insights for COVID-19. Crit Care. (2020) 24:221. doi: 10.1186/s13054-020-02942-2
29. Hou YJ, Okuda K, Edwards CE, Martinez DR, Asakura T, Dinnon KH, et al. SARS-CoV-2 reverse genetics reveals a variable infection gradient in the respiratory tract. Cell. (2020) 182:429.e–46.e. doi: 10.1016/j.cell.2020.05.042
30. Lieberman NAP, Peddu V, Xie H, Shrestha L, Huang M-L, Mears MC, et al. In vivo antiviral host transcriptional response to SARS-CoV-2 by viral load, sex, and age. PLoS Biol. (2020) 18:e3000849. doi: 10.1371/journal.pbio.3000849
31. Fallerini C, Daga S, Mantovani S, Benetti E, Picchiotti N, Francisci D, et al. Association of Toll-like receptor 7 variants with life-threatening COVID-19 disease in males: findings from a nested case-control study. Elife. (2021) 10:e67569. doi: 10.7554/eLife.67569
32. Dirección General de Salud Pública de la Comunidad de Madrid. Informe Semanal de Vigilancia Epidemiológica de la COVID-19. (2021). Available online at: https://www.comunidad.madrid/servicios/salud/coronavirus (accessed December 19, 2021)
33. World Health Organization. WHO R&D Blueprint. Novel Coronavirus COVID-19 Therapeutic Trial Synopsis. (2020). Available online at: https://www.who.int/blueprint/priority-diseases/key-action/COVID-19_Treatment_Trial_Design_Master_Protocol_synopsis_Final_18022020.pdf (accessed March 11, 2020)
Keywords: SARS-CoV-2, viremia, interleukin 6 (IL-6), prognosis, COVID-19
Citation: Roy-Vallejo E, Cardeñoso L, Triguero-Martínez A, Chicot Llano M, Zurita N, Ávalos E, Barrios A, Hernando J, Ortiz J, Rodríguez-García SC, Ciudad Sañudo M, Marcos C, García Castillo E, Fontán García-Rodrigo L, González B, Méndez R, Iturrate I, Sanz-García A, Villa A, Sánchez-Azofra A, Quicios B, Arribas D, Álvarez Rodríguez J, Patiño P, Trigueros M, Uriarte M, Martín-Ramírez A, Arévalo Román C, Galván-Román JM, García-Vicuña R, Ancochea J, Muñoz-Calleja C, Fernández-Ruiz E, de la Cámara R, Suárez Fernández C, González-Álvaro I, Rodríguez-Serrano DA and the PREDINMUN-COVID Group (2022) SARS-CoV-2 Viremia Precedes an IL6 Response in Severe COVID-19 Patients: Results of a Longitudinal Prospective Cohort. Front. Med. 9:855639. doi: 10.3389/fmed.2022.855639
Received: 15 January 2022; Accepted: 30 May 2022;
Published: 15 June 2022.
Edited by:
Luis Garcia De Guadiana-Romualdo, Santa Lucía University General Hospital, SpainReviewed by:
José Miguel Urra, Hospital General Universitario de Ciudad Real, SpainCopyright © 2022 Roy-Vallejo, Cardeñoso, Triguero-Martínez, Chicot Llano, Zurita, Ávalos, Barrios, Hernando, Ortiz, Rodríguez-García, Ciudad Sañudo, Marcos, García Castillo, Fontán García-Rodrigo, González, Méndez, Iturrate, Sanz-García, Villa, Sánchez-Azofra, Quicios, Arribas, Álvarez Rodríguez, Patiño, Trigueros, Uriarte, Martín-Ramírez, Arévalo Román, Galván-Román, García-Vicuña, Ancochea, Muñoz-Calleja, Fernández-Ruiz, de la Cámara, Suárez Fernández, González-Álvaro, Rodríguez-Serrano and the PREDINMUN-COVID Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emilia Roy-Vallejo, ZXJveXZhbGxlam9AZ21haWwuY29t
†Present address: Diego A. Rodríguez-Serrano, Intensive Care Unit, Hospital Universitario Príncipe de Asturias, Alcalá de Henares, Spain
‡These authors have contributed equally to this work and share first authorship
§These authors have contributed equally to this work and share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.